Back to Journals » Patient Preference and Adherence » Volume 17
Dental Anxiety Among Physicians: Relationship with Oral Problems, Dental Visits, and Socio-Demographic Factors
Authors Alkuwaiti E ![]() , Alshubaili R, AlZahrani N, Khusheim S, AlMunif R, Alharbi N, Nazir M
, Alshubaili R, AlZahrani N, Khusheim S, AlMunif R, Alharbi N, Nazir M ![]()
Received 27 January 2023
Accepted for publication 7 April 2023
Published 20 April 2023 Volume 2023:17 Pages 1107—1116
DOI https://doi.org/10.2147/PPA.S406105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Elaf Alkuwaiti,1 Rand Alshubaili,1 Nada AlZahrani,1 Sarah Khusheim,1 Raghad AlMunif,1 Nawal Alharbi,1 Muhammad Nazir2
1College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, 31441, Saudi Arabia; 2Department of Preventive Dental Science, College of Dentistry Imam Abdulrahman Bin Faisal University, Dammam, 31441, Saudi Arabia
Correspondence: Muhammad Nazir, Tel +966-543579615, Email [email protected]
Purpose: The purpose of study was to investigate dental anxiety (DA) and its relationship with oral health problems, dental visits, and socio-demographic factors among physicians.
Patients and Methods: This cross-sectional study was conducted on physicians working in Dhahran, Khobar, Dammam, and Qatif cities of the kingdom of Saudi Arabia. The study included physicians (general practitioners, residents, specialists, and consultants) working in the public and private sectors. Modified Dental Anxiety Scale and World Health Organization’s Oral Health Questionnaire for Adults were used to evaluate DA, oral health problems, and dental attendance.
Results: The study included data from 355 participants with a mean age of 40.13 ± 10.45 years. There were 57.2% of non-Saudi and 42.8% of Saudi participants in the study. Bad dental experience in the previous dental visit was reported by 40% of participants, which was significantly related to DA (P = 0.002). Only 9.60% of participants had no DA, whereas 41.10% demonstrated low DA, 23.4% moderate DA, 18.9% high DA, and 7% extreme DA. Common oral problems included tooth sensitivity (65.40%), tooth cavities (45.90%), bleeding gums (43.10%), and bad breath (36.90%). More than half of participants (58.3%) visited the dentist during the last year and dental pain was the most common reason for dental visits (31.3%). Saudi participants demonstrated significantly increased DA than non-Saudis (P = 0.019). DA was significantly related to tooth sensitivity (P = 0.001), tooth cavities (P = 0.002), dry mouth (P = 0.044), and bad breath (P = 0.005). The participants with difficulty in biting foods (P > 0.001) and feeling embarrassed due to the appearance of teeth (P < 0.001) demonstrated significantly higher DA.
Conclusion: This sample of physicians showed a high prevalence of DA, oral problems, and dental visits due to pain. DA was significantly related to physicians’ negative dental experience, tooth sensitivity, dental decay, dry mouth, and bad breath.
Keywords: physicians, dental anxiety, dental attendance, oral health
Introduction
Oral conditions remain one of the most prevalent diseases affecting billions of people worldwide.1,2 It is known that oral health plays an important role and, in many ways, is interlinked with overall general health and well-being.3 Many oral diseases have systemic manifestations, and many systemic diseases have oral manifestations. This shows how critical is oral health for physicians.4 Physicians can play an important role in the early diagnosis of oral conditions, oral health education of patients, oral health promotion, and quality of life.3 According to the American Academy of Pediatrics, children visit pediatricians 8 times in the first year of birth and 13 times by the age of three years.5 While only 2% of children visit the dentist in the first year of birth and less than 25% by the age of three years.6 According to the Ministry of Health (2018), Saudi nationals’ visits to primary healthcare clinics were 16 times more than visits to dental clinics.7
Dental visits are important for the evaluation of soft and hard tissues, and early detection, prevention, and treatment of oral health problems. Individuals who regularly visit the dentist showed improved oral health status.8 Also, not having a recent dental visit is one of the main factors associated with multiple oral health complaints.9 A study in New Zealand found that positive oral health outcomes in adults were associated with regular dental attendance in childhood.10
Dental anxiety (DA) is a reaction to uneasiness or danger in the dental clinic and is associated with poor dental health. Even with the advances in dental instruments and equipment, DA and fear are common in dental practice.11 A study revealed that patients who have high DA rarely visit the dentist and as a result, they have more missing and decayed teeth.12 DA can start a vicious cycle that can lead patients not to visit the clinic until their dental conditions require invasive treatment, and this can further add to their dental fear.13 Dentally anxious patients also demonstrate impaired oral health-related quality of life and body image disturbances.14,15
Periodontal diseases are strongly linked with cardiovascular disease, diabetes, negative pregnancy outcomes, and respiratory disease.16 These interconnections between oral health and systemic health underscore the need to explore DA, oral health problems, and dental attendance patterns among physicians because the awareness of oral disease can help prevent oral problems among physicians and improve their oral health. Physicians are known to play a role in screening oral diseases, educating patients about the importance of oral health, and referring them to the dentist. However, DA among physicians may not only discourage them to visit the dentist but may also not support oral health promotion among their patients by not referring them to the dentist. There is a high burden of oral disease in the populations; however, data are scant on DA and oral health problems among physicians. The aim of this study was to investigate dental anxiety, oral health problems, and dental visits among physicians in the Eastern province of Saudi Arabia. This investigation may help improve oral health and access to dental care services for physicians.
Materials and Methods
Study Design and Participants
We conducted a cross-sectional study on physicians in Dhahran, Khobar, Dammam, and Qatif cities in the kingdom of Saudi Arabia. The study included physicians (general practitioners, residents, specialists, and consultants) working in primary healthcare centers and hospitals in the public sector, and private clinics and hospitals. Physicians who at least have one year of clinical experience and work either in the public or private sector in the selected cities were eligible for this study. The assumptions for sample size estimation included: 5% margin of error, 95% confidence level, 50% response distribution, population size (N ≈ 2000), and 80% of the power of the study. These calculations yielded a sample of 377 physicians. Physicians were selected using a convenience sampling technique.
Study Instrument
DA, oral health problems, and dental attendance of physicians were broadly evaluated using a self-completion questionnaire. The Modified Dental Anxiety Scale (MDAS) was used to assess DA among physicians.17 The scale evaluated the physician’s fear of dental care, and it consists of five questions using a 5-point Likert scale (“1” being not anxious, “2” slightly anxious, “3” fairly anxious, “4” very anxious, “5” extremely anxious). These questions were about the participant’s feelings related to dental treatment the next day, feelings in the waiting room before dental treatment, feelings about tooth drilling during dental treatment, feelings regarding tooth scaling, and feelings related to the local anesthetic injection. The score of the MDAS scale ranges from 5 to 25, with higher values indicating greater DA. The MDAS score of 5 denotes no dental anxiety; 6–10 low dental anxiety; 11–14 moderate dental anxiety; 15–18 high dental anxiety; and 19–25 extreme dental anxiety.18 A previous study confirmed the reliability and validity of the MDAS scale in Saudi adults.19 In the present study, internal consistency of MDAS scale was evaluated by using Cronbach's alpha and its score (0.89) showed good level of reliability.
The questions about the time since the last dental visit and the reasons for dental attendance and oral health status were derived from the Oral Health Questionnaire for Adults by the World Health Organization.20 Additionally, the questionnaire included physicians’ demographic details such as gender, age, nationality, marital status, place of work (private or government sector), monthly income, physician’s qualifications, and years of experience. The questionnaire in English language was pilot tested among Saudi and non-Saudi physicians who can fully understand the English. The pilot testing on 20 physicians was conducted for clarity and understanding of questions and examining the validity of the questionnaire. Piloting was done about one month before the start of data collection. No changes/modifications were indicated in the questionnaire as a result of pilot testing.
Ethical Considerations
The research ethical approval (IRB 2022–02-341) was obtained from the Deanship of Scientific Research, Imam Abdulrahman Bin Faisal University, Dammam. The participation of physicians in the study was voluntary, and they were ensured about anonymity, privacy, and confidentiality of their data. The purpose, details, and expected benefits of the study were explained to all participants, and those who agreed to participate were asked to provide written informed consent before questionnaire administration. Ethical guidelines expressed in the Declaration of Helsinki were followed during the conduct of the study.
Procedure/Survey Administration
The researchers themselves collected the data by visiting physicians in their clinics and hospitals. Hard copies of self-administered questionnaire were provided to 377 participating physicians in their clinics/hospitals who provided their responses by filling up these questionnaires and returned them to researchers in the same or next visit. A maximum of three visits were performed when the physicians were unable to provide their responses in the first or second visit.
Statistical Analysis
Data were screened for the completion of information before statistical analysis. Frequencies and proportions of categorical variables (gender, qualification, place of work, etc.) and means and standard deviations of continuous variables (age, score of DA, etc.) were calculated. Shapiro–Wilk test (P = 0.08) was performed to assess the normality of the MDAS scale, and accordingly, Student’s t-test and one-way ANOVA test were performed to compare the mean score of MDAS in two (eg, male and female physicians) or more than two categories of physicians (eg, general physicians, specialists, consults), respectively. Similarly, one-way ANOVA test was used to evaluate MDAS score among categories based on reasons for dental visits and time since last dental visit. Statistical Package for Social Science (SPSS Statistics for Windows, Version 22.0, Armonk, NY: IBM Corp) was used for statistical analysis. A value of <0.05 was considered statistically significant.
Results
The study included data from 355 physicians because 22 questionnaires were discarded due to missing/incomplete information. The mean age of the participants was 40.13 ± 10.45 years and the age ranged from 24 to 68 years. More than half of the sample consisted of males (67%), were non-Saudi (57.2%), and worked in the government sector (63.9%). Dental pain or discomfort during the past 12 months was reported by 58.3% of participants and 40% faced bad dental experience in the previous dental visit. The mean DA score of the sample was 11.36 ± 4.53. The mean DA score was significantly higher among non-Saudi (11.85 ± 4.39) than Saudi participants (10.70 ± 4.65) (P = 0.019). The participants with dental pain or discomfort demonstrated greater DA (12.15 ± 4.61) than those without pain or discomfort (10.34 ± 4.19) (P < 0.001). Similarly, the participants who faced a bad dental experience showed significantly higher DA score (12.29 ± 4.75) than those without bad dental experience (10.74 ± 4.28) (P = 0.002). (Table 1).
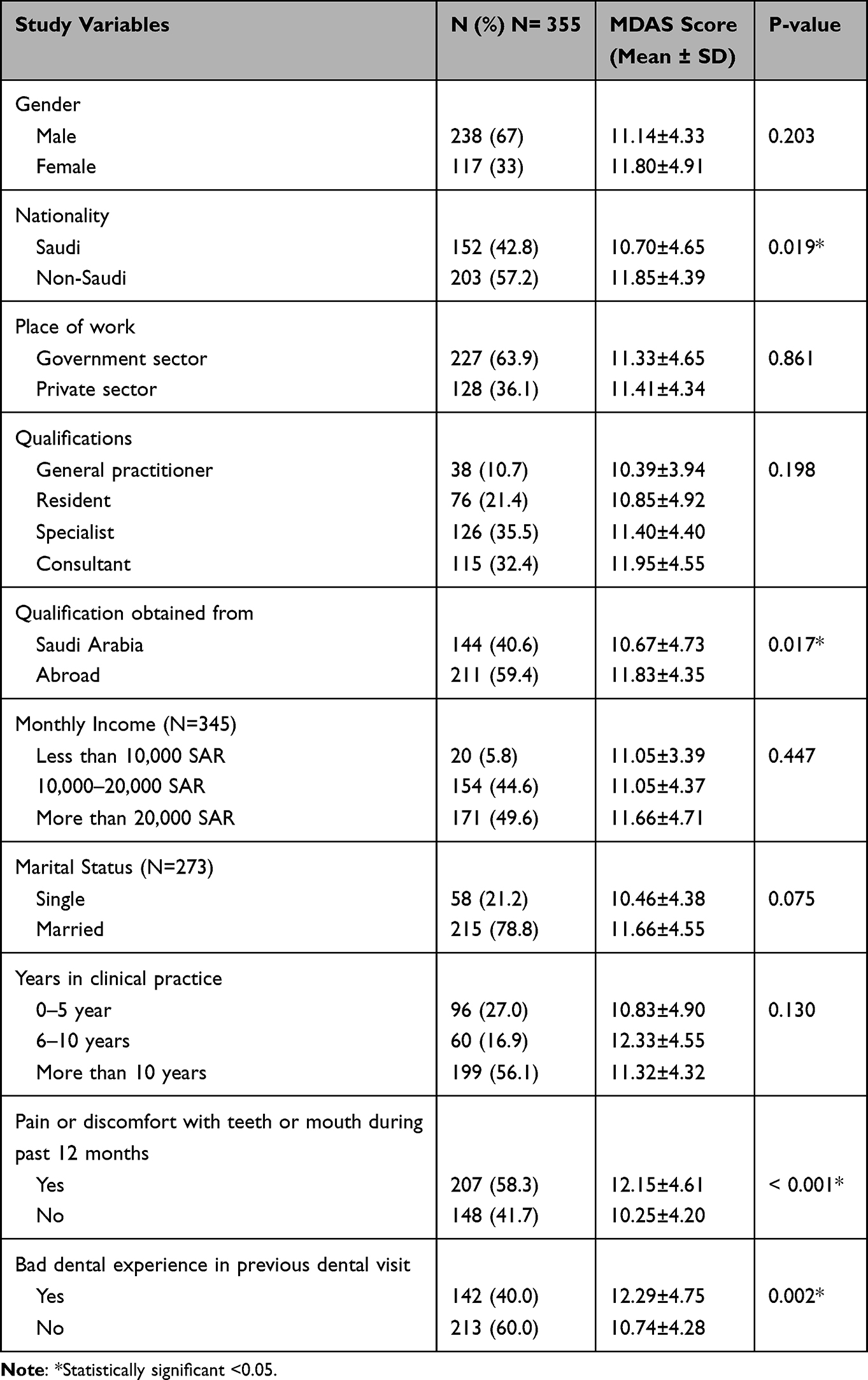 |
Table 1 Distribution of Socio-Demographic Factors and Their Relationship with DA Among Study Participants |
Figure 1 shows the distribution of self-reported oral problems among participants. Tooth sensitivity (65.40%) was the most common oral problem among participants. This was followed by tooth cavities (45.90%), bleeding gums (43.10%), and bad breath (36.90%). Table 2 displays the mean score of each item of the MDAS questionnaire. The item “Feelings about tooth drilling” secured the highest mean score (2.74 ± 1.18) and this was followed by “Feelings about local anesthetic injection” (2.62 ± 1.15). On the other hand, “Feelings while sitting in waiting room” showed the lowest mean score (1.94 ± 0.99) (Table 2). Only 9.60% of participants had no DA, whereas 41.10% of participants demonstrated low DA, 23.4% moderate DA, 18.9% high DA, and 7% extreme DA (Figure 2).
 |
Table 2 DA According to MDAS Questionnaire Items Among Physicians |
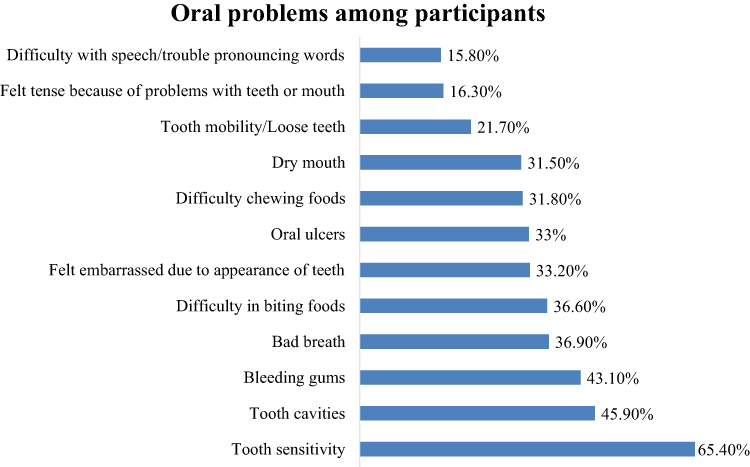 |
Figure 1 Distribution of oral problems among participants. |
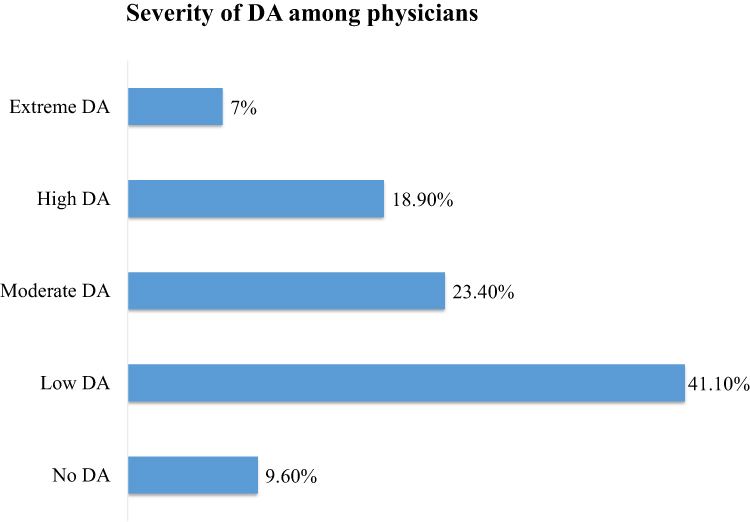 |
Figure 2 Distribution of severity of DA among study participants. |
Pain or trouble with teeth, gums or mouth was the most common reason for dental visits (31.3%), followed by treatment/follow-up treatment (26.2%). More than half participants (58.3%) visited the dentist during the last year. The study found a statistically significant relationship between reasons of dental visits and DA (P = 0.002) and participants who visited due to pain or trouble with teeth, gums or mouth showed the highest DA (12.71 ± 4.79). The participants who visited the dental office after 5 years or more demonstrated the highest DA (12.07 ± 5.53); however, time since the last dental visit showed no statistically significant relationship with DA (P = 0.494) (Table 3).
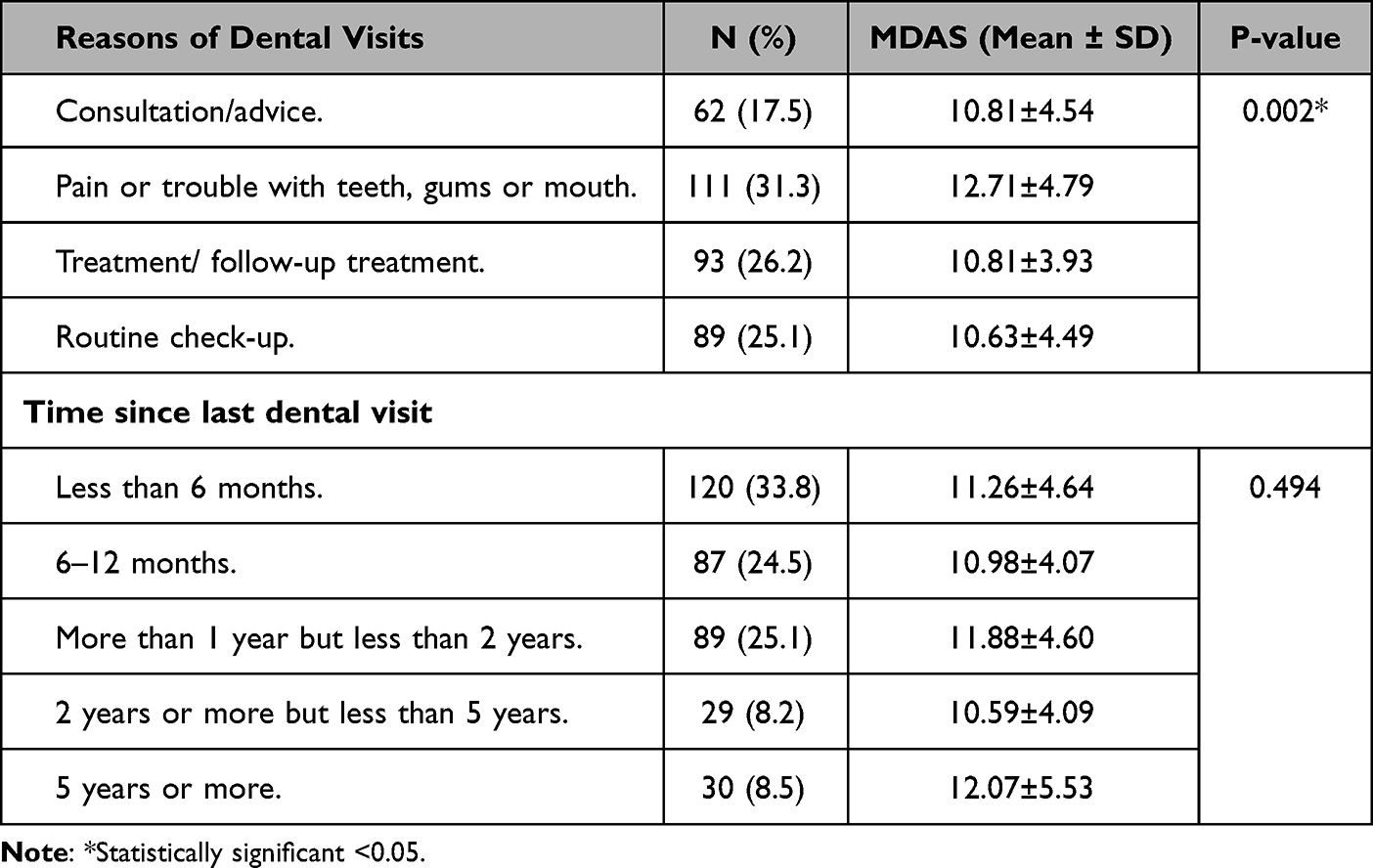 |
Table 3 Relationship Between Reasons of Dental Visits and Time Since Last Dental Visits with DA Among Study Participants |
Table 4 illustrates the relationship between DA and oral health problems. The participants with difficulty biting foods (P > 0.001), difficulty chewing foods (P = 0.011), and dry mouth (P = 0.044) demonstrated significantly higher DA than those without these problems. Similarly, DA was significantly related to bad breath (P = 0.005), tooth sensitivity (P = 0.001), tooth cavities (P = 0.002), and feeling embarrassed due to the appearance of teeth (P < 0.001).
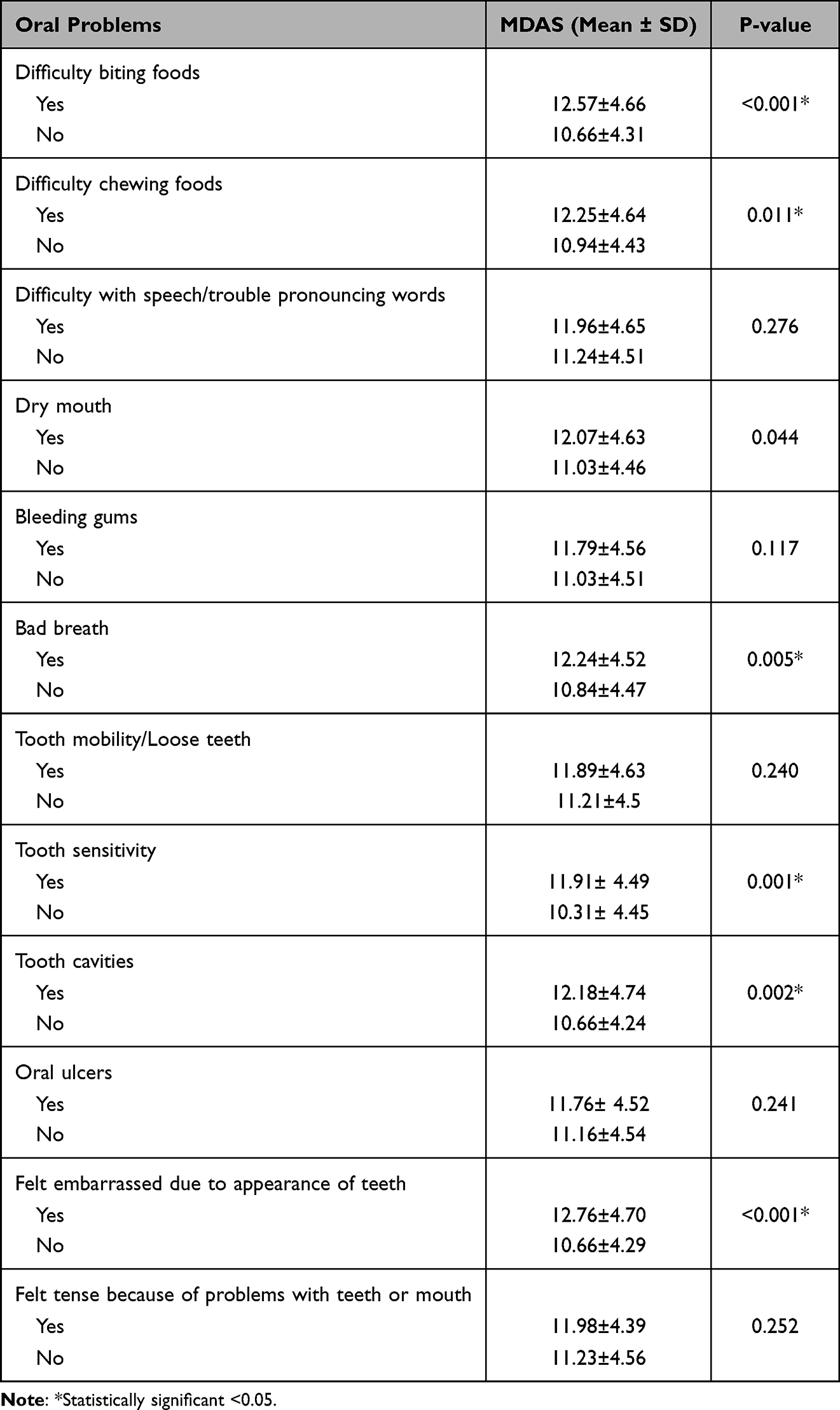 |
Table 4 Relationship Between DA and Oral Problems Among Study Participants |
Discussion
This study evaluated DA, oral health problems, and dental visits among physicians which could be relevant to their values about oral health of their patients. Our study found that half of the participants showed no or low DA (50.7%), whereas 18.9% showed high DA and 7% extreme DA. According to three previous studies in Saudi Arabia, the prevalence of DA was 52% in Al-Jouf,21 31.9–50% in Jeddah,22,23 and 22.7% in Dammam.23 In Jeddah and Al-Jouf, 22–30% of the participants were moderately anxious, 11–17% were highly anxious, and 9–12% were extremely anxious.21,22 A recent systematic review and meta-analysis estimated that the global prevalence of DA in adults was 13.8%, and 11.2% had high DA and 2.6% severe DA.24
Having a negative experience during a dental appointment was found to be one of the main reasons for DA when looking at the studies conducted in the USA and India.25,26 About 40% of the participants in our study had a negative dental experience, which was significantly associated with DA. A previous study in Saudi Arabia showed that 34.8% of participants with extreme DA had previously experienced bad dental visits.23 Our study also demonstrated that DA was significantly associated with dental pain within the last 12 months. One of the reasons could be that subjects with DA are more likely to delay their dental appointments, deteriorate oral health status, and more likely to experience dental pain.27
In the present study, there was a high prevalence of tooth sensitivity, tooth cavities, and bleeding gums among physicians. These findings corroborate a high distribution of oral conditions among people in the country. The loss of hard tissue (tooth wear) is one of the main causes of tooth sensitivity.28 A study by Al-Khalifa revealed that 83.5% of the adult population had tooth wear in the eastern province of Saudi Arabia.29 According to a review by Al-Ansari, the general population in Saudi Arabia had a high prevalence and severity of caries with an alarming increase in DMFT rates.30 Bleeding gums are affected by systematic and local factors such as oral hygiene, smoking, and diabetes, and studies in eastern Saudi Arabia discussed the relationship between bleeding gums and smoking and diabetes.31,32 It is crucial that public health measures should focus on preventing oral problems, reducing the burden of oral diseases, and maintaining the optimal oral health of physicians in order for them to fully appreciate an excellent oral health for their patients.
Among our sample of physicians, the highest MDAS scores were for the drilling of teeth and this was followed by local anesthetic injection. According to patients in the cities of Dammam and Jeddah, the local anesthetic injection was the most anxious procedure followed by drilling of teeth.23 Similar results were reported in two previous studies from Saudi Arabia where authors found the highest DA related to local anesthetic injections and drilling of teeth.33,34 A study from Pakistan also showed that injection of local anesthesia was the most anxious procedure.35 Contrary to most studies in the literature, the participants in our study showed the highest DA related to the drilling of teeth as opposed to local anesthetic injection which could be explained by the fact that physicians have more knowledge about local anesthesia and may practice injecting it on their patients which may lower their perception of DA related to local anesthesia.
High DA could lead to avoiding dental treatment resulting in higher caries risk and a greater need for oral rehabilitation. A German study showed a positive correlation between dental fear and the number of carious and missing teeth.36 Another epidemiological study from Australia found a significantly greater number of decayed teeth among anxious patients.37 Likewise, the researchers demonstrated that DA was significantly related to increased caries and worse periodontal health among adult populations in Hong Kong, China.38 These findings support our results, which showed that physicians with decayed teeth, tooth sensitivity, dry mouth, and bad breath demonstrated significantly higher DA. Our study also showed that DA was significantly related to biting and chewing of food and feeling embarrassment due to the appearance of teeth. Our study shows that DA adversely affects physicians’ oral health. Medical education should include emphasis on the importance of oral health and its robust connection with systemic health. The physicians should improve their oral health by following oral hygiene guidelines including visiting dentists for routine dental care. The results of our study also highlight the significance of further exploring the relationship between DA and oral problems using a large population in a cohort study.
Our results showed that dental pain was the most frequent reason for visiting the dentist among physicians. This is supported by the findings of a study by Almutlaqah et al, who showed that emergency visits were the most common reason for visiting the dentist in Saudi Arabia.39 In contrast, conservative treatment was found to be the most common reason for visiting the dental office among Polish populations.40 Similar results were reported among Indian patients who visited the dentist most frequently for esthetic reasons, while toothache was the third concern for visiting the dentist.41 On the other hand, those who visit the dentist more frequently were found to be less anxious because they get treated before the dental problems lead to a painful experience.19 Dental visits due to pain among our sample of physicians could be explained by a high prevalence of oral problems. It is also possible that physicians may not be fully aware of proper oral hygiene instructions and the importance of maintaining good oral health.
This is the first study to report DA among physicians and its relationship with oral health status and dental attendance. A validated MDAS instrument and WHO oral health questionnaire were used to report reliable statistics on this important topic. However, there are some limitations to this study. The generalizability of study findings may be limited because physicians from eastern Saudi Arabia participated in the study. Moreover, self-administered questionnaires are prone to inaccuracies in recalling and reporting the information and misunderstandings and not responding to some questions. The clinical oral examination provides more accurate information about caries, periodontal health, bleeding gums, dry mouth, etc. An important consideration in future research about physicians’ DA would be to judge the effect physicians’ dental anxiety has on their values and discussions about oral health among their patients compared with physician who have no or low dental anxiety. Future studies should also investigate if physicians with better oral health more frequently screen oral diseases, educate more patients about oral health, and more often refer patients to dental office than those with poor oral health status.
Conclusion
In conclusion, the study revealed a high prevalence of DA among physicians. Most physicians demonstrated DA from low to extreme levels. Common oral problems included tooth sensitivity, tooth cavities, bleeding gums, and bad breath. A majority of physicians visited the dental office during the last year mostly due to dental pain. DA was significantly related to physicians’ bad dental experience. The physicians with tooth sensitivity, tooth cavities, dry mouth, and bad breath demonstrated significantly higher DA. Dental anxiety among physicians is important because it may impact physicians’ values about oral health. It is important that physicians should be provided more education about oral problems including dental anxiety, oral hygiene measures, and the importance of regular dental visits for their optimal oral health. They should also play their vital role in promoting the oral health of their patients through oral health education and referral to dentists.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Marcenes W, Kassebaum NJ, Bernabé E, et al. Global burden of oral conditions in 1990–2010: a systematic analysis. J Dent Res. 2013;92(7):592–597. doi:10.1177/0022034513490168
2. Peres MA, Macpherson LMD, Weyant RJ, et al. Oral diseases: a global public health challenge. Lancet. 2019;394(10194):249–260. doi:10.1016/S0140-6736(19)31146-8
3. Aggelidou Galazi A, Siskou O, Karagkouni I, et al. Investigating physicians’ and patients’ oral health knowledge: a field needed interdisciplinary policy making approach. Int J Health Promot Educ. 2019;57(6):343–354. doi:10.1080/14635240.2019.1638813
4. Rabiei S, Mohebbi SZ, Patja K, Virtanen JI. Physicians’ knowledge of and adherence to improving oral health. BMC Public Health. 2012;12:855. doi:10.1186/1471-2458-12-855
5. American Academy of Pediatric. Committee on practice and ambulatory medicine recommendations for preventive pediatric health care. Pediatrics. 2000;105(3):645–646.
6. Chi DL, Momany ET, Jones MP, et al. Relationship between medical well baby visits and first dental examinations for young children in Medicaid. Am J Public Health. 2013;103(2):347–354. doi:10.2105/AJPH.2012.300899
7. Ministry of Health. Statistical Yearbook. Ministry of Health; 2018.
8. Almoznino G, Aframian DJ, Sharav Y, et al. Lifestyle and dental attendance as predictors of oral health-related quality of life. Oral Dis. 2015;21(5):659–666. doi:10.1111/odi.12331
9. Al-Shammari KF, Al-Ansari JM, Al-Khabbaz AK, Dashti A, Honkala EJ. Self-reported oral hygiene habits and oral health problems of Kuwaiti adults. Med Princ Pract. 2007;16(1):15–21.
10. Crocombe LA, Broadbent JM, Thomson WM, Brennan DS, Poulton R. Impact of dental visiting trajectory patterns on clinical oral health and oral health-related quality of life. J Public Health Dent. 2012;72(1):36–44. doi:10.1111/j.1752-7325.2011.00281.x
11. Yildirim TT. Evaluating the relationship of dental fear with dental health status and awareness. J Clin Diagn Res. 2016;10(7):Zc105–Zc109. doi:10.7860/JCDR/2016/19303.8214
12. Schuller AA, Willumsen T, Holst D. Are there differences in oral health and oral health behavior between individuals with high and low dental fear? Community Dent Oral Epidemiol. 2003;31(2):116–121. doi:10.1034/j.1600-0528.2003.00026.x
13. Armfield JM, Stewart JF, Spencer AJ. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health. 2007;7:1. doi:10.1186/1472-6831-7-1
14. Shacham M, Greenblatt-Kimron L, Hamama-Raz Y, et al. Unveiling the association between body image dissatisfaction and dental anxiety. Surgeries. 2022;3(2):92–100. doi:10.3390/surgeries3020011
15. Mehrstedt M, John MT, Tönnies S, Micheelis W. Oral health‐related quality of life in patients with dental anxiety. Community Dent Oral Epidemiol. 2007;35(5):357–363. doi:10.1111/j.1600-0528.2007.00376.x
16. Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci. 2017;11(2):72–80.
17. Humphris G, Freeman R, Campbell J, Tuutti H, D’souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000;50(6):367–370. doi:10.1111/j.1875-595X.2000.tb00570.x
18. Giri J, Pokharel PR, Gyawali R, Bhattarai B. Translation and validation of modified dental anxiety scale: the Nepali version. Int Sch Res Notices. 2017;2017. doi:10.1155/2017/5495643
19. Bahammam MA, Hassan MH. Validity and reliability of an Arabic version of the modified dental anxiety scale in Saudi adults. Saudi Med J. 2014;35(11):1384–1389.
20. World Health Organization. Oral Health Surveys: Basic Methods. World Health Organization; 2013.
21. Fayad MI, Elbieh A, Baig MN, Alruwaili SA. Prevalence of dental anxiety among dental patients in Saudi Arabia. J Int Soc Prev Community Dent. 2017;7(2):100–104. doi:10.4103/jispcd.JISPCD_19_17
22. Ibrahim NK, Al-Jdani M, Al-Aamoudi N, Sukkar S. Anxiety due to dental procedures and treatment among adult patients attending outpatient clinics in King Abdulaziz University Hospital, Jeddah, Saudi Arabia. J Med Res. 2016;2(2):35–40. doi:10.31254/jmr.2016.2206
23. Al-Khalifa KS. Prevalence of dental anxiety in two major cities in the kingdom of Saudi Arabia. Saudi J Med Sci. 2015;3(2):135. doi:10.4103/1658-631X.156421
24. Silveira ER, Cademartori MG, Schuch HS, Armfield JA, Demarco FF. Estimated prevalence of dental fear in adults: a systematic review and meta-analysis. J Dent. 2021;108:103632. doi:10.1016/j.jdent.2021.103632
25. White AM, Giblin L, Boyd LD. The prevalence of dental anxiety in dental practice settings. J Dent Hyg. 2017;91(1):30–34.
26. Appukuttan D, Subramanian S, Tadepalli A, Damodaran LK. Dental anxiety among adults: an epidemiological study in South India. N Am J Med Sci. 2015;7(1):13–18. doi:10.4103/1947-2714.150082
27. Armfield JM. What goes around comes around: revisiting the hypothesized vicious cycle of dental fear and avoidance. Community Dent Oral Epidemiol. 2013;41(3):279–287. doi:10.1111/cdoe.12005
28. Warreth A, Abuhijleh E, Almaghribi MA, Mahwal G, Ashawish A. Tooth surface loss: a review of literature. Saudi Dent J. 2020;32(2):53–60. doi:10.1016/j.sdentj.2019.09.004
29. Al-Khalifa KS. The prevalence of tooth wear in an adult population from the Eastern Province of Saudi Arabia. Clin Cosmet Investig Dent. 2020;12:525–531. doi:10.2147/CCIDE.S286500
30. Al-Ansari AA. Prevalence, severity, and secular trends of dental caries among various Saudi populations: a literature review. Saudi J Med Sci. 2014;2(3):142. doi:10.4103/1658-631X.142496
31. AlTuraiki AM, Jaemal HM, Alamer AA, et al. Oral health and patterns of dental visits among diabetic patients in the Eastern Province of Saudi Arabia. Clin Cosmet Investig Dent. 2021;13:513–520. doi:10.2147/CCIDE.S340579
32. Al-Qurashi H, Al-Farea M, Al-Qurai T, et al. Comparison of oral hygiene practices and oral health problems among smoker and non-smoker male adolescents in the Eastern Province of Saudi Arabia. Saudi J Dent Res. 2016;7(2):106–111. doi:10.1016/j.sjdr.2016.04.002
33. Sghaireen MG, Zwiri AM, Alzoubi IA, Qodceih SM, Al-Omiri MK. Anxiety due to dental treatment and procedures among university students and its correlation with their gender and field of study. Int J Dent. 2013;2013:647436. doi:10.1155/2013/647436
34. Muhammad UN, Rajan JS. A cross-sectional study to assess the level of dental anxiety prevailing in undergraduate dental students in Riyadh Elm University. Saudi J Oral Sci. 2020;7(1):35. doi:10.4103/sjos.SJOralSci_32_19
35. Ali S, Farooq I, Khan SQ, et al. Self-reported anxiety of dental procedures among dental students and its relation to gender and level of education. J Taibah Univ Med Sci. 2015;10(4):449–453. doi:10.1016/j.jtumed.2015.06.002
36. Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety--an epidemiological study on its clinical correlation and effects on oral health. J Oral Rehabil. 2006;33(8):588–593. doi:10.1111/j.1365-2842.2005.01589.x
37. Armfield JM, Slade GD, Spencer AJ. Dental fear and adult oral health in Australia. Community Dent Oral Epidemiol. 2009;37(3):220–230. doi:10.1111/j.1600-0528.2009.00468.x
38. Ng SK, Leung WK. A community study on the relationship of dental anxiety with oral health status and oral health-related quality of life. Community Dent Oral Epidemiol. 2008;36(4):347–356. doi:10.1111/j.1600-0528.2007.00412.x
39. Almutlaqah MA, Baseer MA, Ingle NA, Assery MK, Al Khadhari MA. Factors affecting access to oral health care among adults in Abha City, Saudi Arabia. J Int Soc Prev Community Dent. 2018;8(5):431–438. doi:10.4103/jispcd.JISPCD_205_18
40. Michalak E, Łoboda J, Chomyszyn-Gajewska M. Reasons for patients’ visits in the dental offices of Cracow in the years 2005–2006 and 2013–2014. Przegl Epidemiol. 2015;69(4):787–794.
41. Jeddy N, Nithya S, Radhika T, Jeddy N. Dental anxiety and influencing factors: a cross-sectional questionnaire-based survey. Indian J Dent Res. 2018;29(1):10–15. doi:10.4103/ijdr.IJDR_33_17
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.