Back to Journals » Psychology Research and Behavior Management » Volume 16
Demoralization and Suicidal Ideation in Chronic Pain Patients
Authors Chytas V ![]() , Costanza A
, Costanza A ![]() , Mazzola V, Luthy C, Bondolfi G
, Mazzola V, Luthy C, Bondolfi G ![]() , Cedraschi C
, Cedraschi C ![]()
Received 13 April 2022
Accepted for publication 30 January 2023
Published 5 March 2023 Volume 2023:16 Pages 611—617
DOI https://doi.org/10.2147/PRBM.S367461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Vasileios Chytas,1,* Alessandra Costanza,2,3,* Viridiana Mazzola,1 Christophe Luthy,4,5 Guido Bondolfi,1,2 Christine Cedraschi5,6
1Department of Psychiatry, Service of Liaison Psychiatry and Crisis Intervention, Geneva University Hospitals, Geneva, Switzerland; 2Department of Psychiatry, Faculty of Medicine, University of Geneva, Geneva, Switzerland; 3Faculty of Biomedical Sciences, Università della Svizzera Italiana (USI), Lugano, Switzerland; 4Division of General Medical Rehabilitation, Geneva University Hospitals, Geneva, Switzerland; 5Department of Geriatrics and Rehabilitation, Faculty of Medicine, University of Geneva, Geneva, Switzerland; 6Division of Clinical Pharmacology & Toxicology, Multidisciplinary Pain Centre, Geneva University Hospitals, Geneva, Switzerland
*These authors contributed equally to this work
Correspondence: Vasileios Chytas, Department of Psychiatry, Service of Liaison Psychiatry and Crisis Intervention, Geneva University Hospitals, Rue Gabrielle-Perret-Gentil 4, Geneva, 1205, Switzerland, Tel +41 79 553 41 55, Fax +41 22 372 38 55, Email [email protected]
Abstract: The literature has clearly stressed that patients suffering from chronic pain are at high risk of suicidal behavior (SB). Hence the need to improve the characterization of this behavior risk profile in these patients. Some findings indicate a possible relationship between demoralization and pain, with functional disability found to be correlated with demoralization. The primary objective of this study was to investigate the relationship between demoralization and suicidal ideation (SI) in patients with chronic pain. The secondary objective was to verify whether demoralization can occur independently of depression in these patients. Inclusion criteria were patients with chronic pain, with SI or not, matched for age and gender, aged > 18 years. Seventy patients with SI and 70 patients without SI were included. Between-group difference was statistically significant (F=1.064; t= 7.21, p< 0.001, d=1.22), confirming the presence of numerous and intense depressive symptoms in the patients of the SI group. Regarding the Demoralization Scale (DS), the difference between the two groups was statistically highly significant (F=1.49; t=9.44; p< 0.001, d=1.6). There was also a strong positive correlation between DS and Beck Depression Inventory (BDI-II) (R=0.749; p< 0.001 for the study group and R=0.704; p< 0.001 for the control group). Furthermore, there was a strong positive correlation between the DS and the Scale for Suicide Ideation (SSI) in the SI patients group, meaning that high demoralization is associated with higher suicidal ideation as well. Our findings did not allow us to distinguish between the notions of depression and demoralization, since the two constructs show almost the same strong positive correlation with suicidal thoughts, the two also being strongly correlated with each other.
Keywords: demoralization, suicidal ideation, chronic pain, depression
Introduction
Chronic pain conditions have been associated with an elevated risk of suicidal behavior (SB). Indeed, prevalence rates of suicidal ideation (SI) are as high as 20% to 40%, and suicidal attempts (SA) have a lifetime prevalence of 5%-14%. Further, the risk of death by suicide is doubled in patients suffering from chronic pain as compared to controls.1–4
The literature shows that associations between chronic pain and SB are robust even after adjusting for socio-demographic and clinical variables, including in particular depressive conditions.5–11 Various conditions modulating the risk of SB in patients suffering from chronic pain have been investigated. This includes in particular pain characteristics, functional interference, illness beliefs, but also access to opioids.1,3,12 Yet, the necessity to further explore other possible risk and protection factors is clearly emerging, so as to better describe the suicidal risk profile in these patients.3
Demoralization is one such factor. This construct was introduced by Frank as resulting from persistent failure to cope with internally or externally induced stresses that the persons and those close to them expect them to handle, and characterized by feelings of impotence, isolation, and despair.13 Fava introduced the demoralization construct in the psychosomatic domain.14–17 In Kissane and Clarke’s theoretical model, constitutive components of demoralization are loss of meaning in life, hopelessness or disheartenment, helplessness, sense of failure, and dysphoria.18,19 To capture the specific dimensions of demoralization as well its intensity, these authors developed the Demoralization Scale (DS).20 The demoralization is distinguished with the different depressive disorders which are characterized by sadness severe enough or persistent enough to interfere with function and often by decreased interest or pleasure in activities according to the Diagnostic and Statistical Manual of Mental Disorders (DSM). Additionally, de Figuereido21 emphasized that the main problem in demoralization is the subjective incompetence experienced by the person, caused by uncertainty about the appropriate direction of action, while the major concern in depression is a decreased motivation, even when the appropriate direction of action is known.
Some findings indicate a possible relationship between demoralization and the pain experience, with functional disability found to be correlated with demoralization in a sample of inpatients independently of illness severity.22,23
SB in demoralization was specifically addressed by Kissane, who emphasized a predictable progression to a desire to die or to commit suicide in a number of medically ill patients and psychiatrically ill patients who were not developing a clinical depression but were demoralized.18,19,24
The issue is to examine the relationship between demoralization and depression in individuals presenting with SB. Most of the studies admitted that demoralization is an independent condition distinguishable from depression, focusing on their phenomenological differentiation.18,21,25,26 In patients with cancer20,27–30 and other medical diseases,17 there may be a frequent overlap between demoralization and depression, but demoralization can occur independently of depression and the two conditions are not necessarily connected by a hierarchical connection.
Within this framework, the primary objective of this study was to investigate the relationship between demoralization and SI in patients with chronic pain. The secondary objective was to verify whether demoralization can occur independently of depression in patients with chronic pain. We expect to observe a higher score on the Demoralization Scale (DS) for patients with SI as identified by the Beck Depression Inventory (BDI-II) and the Scale for Suicidal Ideation (SSI). We also expect that patients with SI as measured by the BDI-II and SSI have a higher score on the DS but not necessarily a higher score on the BDI-II. Indeed, according to the literature, both depression and demoralization seem to play a mediating role in suicidality with the latter having a greater effect, even when considered together in the mediation model.31
Materials and Methods
Design
The details of the procedure have been presented extensively elsewhere.32 Briefly, the present project is an observational study, conducted at the Geneva University Hospitals, and more specifically at the Multidisciplinary Pain Center in collaboration with the Service of Liaison Psychiatry and Crisis Intervention.
Research Sample
Inclusion criteria were patients affected by chronic pain, referred to the pain center, either presenting with SI as or not presenting with SI, as identified by the question 9 of the BDI-II, matched for age and gender, aged > 18 years and providing a written informed consent. Exclusion criteria were patients with an insufficient comprehension of the French language, affected by dementia, psychotic disorder or borderline personality disorder.
Instruments
The following instruments were used: a) The question 9 of the Beck Depression Inventory, BDI-II33 allowed to identify the presence or absence of suicidal ideation. As a reminder, question 9 of the BDI-II presents the following items: 0- I never think about kill myself, 1- I sometimes think about killing myself but I probably never will, 2- I would like to kill myself and 3- I would kill myself if I had the chance. In addition, the BDI-II allowed to establish the severity of the depressive symptomatology (0–10 no depressive symptoms, 11–19 mild depressive symptoms, 20–29 moderate depressive symptoms and> 30 severe depressive symptoms); b) The French version 5.0.0 of the international neuropsychiatric structured diagnostic mini interview (MINI)34 to screen for possible psychiatric diagnoses according to the DSM IV, and to establish the presence of depression; c) The Scale for Suicide Ideation.35 This is a scale designed to assess the characteristics and severity of SI. It has 19 items with scores ranging from 0–2 and a maximum score of 38. High scores indicate high suicidal ideation and a score ≥6 is used as the cut-off for this scale, indicating clinically significant suicidal ideation;36–38 d) The Demoralization Scale (DS) which has 24 items, with scores varying between 0 (never) and 4 (all the time).20 The maximum score is 96 and the higher the DS score, the higher the degree of demoralization. The scale was developed and validated in a population of cancer patients benefiting from palliative care in different countries, with average scores around 30, which was used as a “cut-off” in our study.20
Statistical Analyses
Data from the questionnaires were manually entered into an ad-hoc database devised through SPSS (Inc., 2009, Chicago, USA). We tried and minimized entry errors by using double data entry. As for the analysis, SPSS22 was used. Descriptive statistical analyses were conducted to calculate means and standard deviations (SD) for all numeric variables and frequencies (%) for categorical variables. The chi-square test was used for categorical variables as well as to check for correspondence between groups, with respect to sociodemographic variables (eg age, sex and years of education). In order to test our main hypothesis, that is to investigate any significant interaction between the variables DS and SI, we computed a nonparametric statistical dependence measure (Spearman’s rho) or a Pearson correlation coefficient. Missing values analysis was performed across all questionnaire scores to look for significant trends. Random missing values have been replaced with the mean.
Ethical Issues
The Ethics Committee of the Canton of Geneva approved the protocol (project No. 2017–02138; decision dated January 25, 2018) that has been carried out in accordance with the research plan and Swiss legal and regulatory requirements, which is in agreement with the principles stated in the current version of the Declaration of Helsinki. We obtained written informed consent from all patients.
Participants
Seventy patients with suicidal ideation (ie patients who responded> 0 to question 9 of the BDI-II – the SI group), and 70 patients not presenting suicidal ideation (who answered 0 to question 9 of the same questionnaire (ie control group). These patients were recruited between March 2018 and November 2019, ie, over a 20 month-period. Eight patients declined participation in the study and 4 patients were not included because they did not understand the French language well enough. Table 1 and Table 2 present the characteristics of the participants, showing that the SI and control groups are very satisfactorily comparable with regard to their socio-demographic and clinical characteristics.
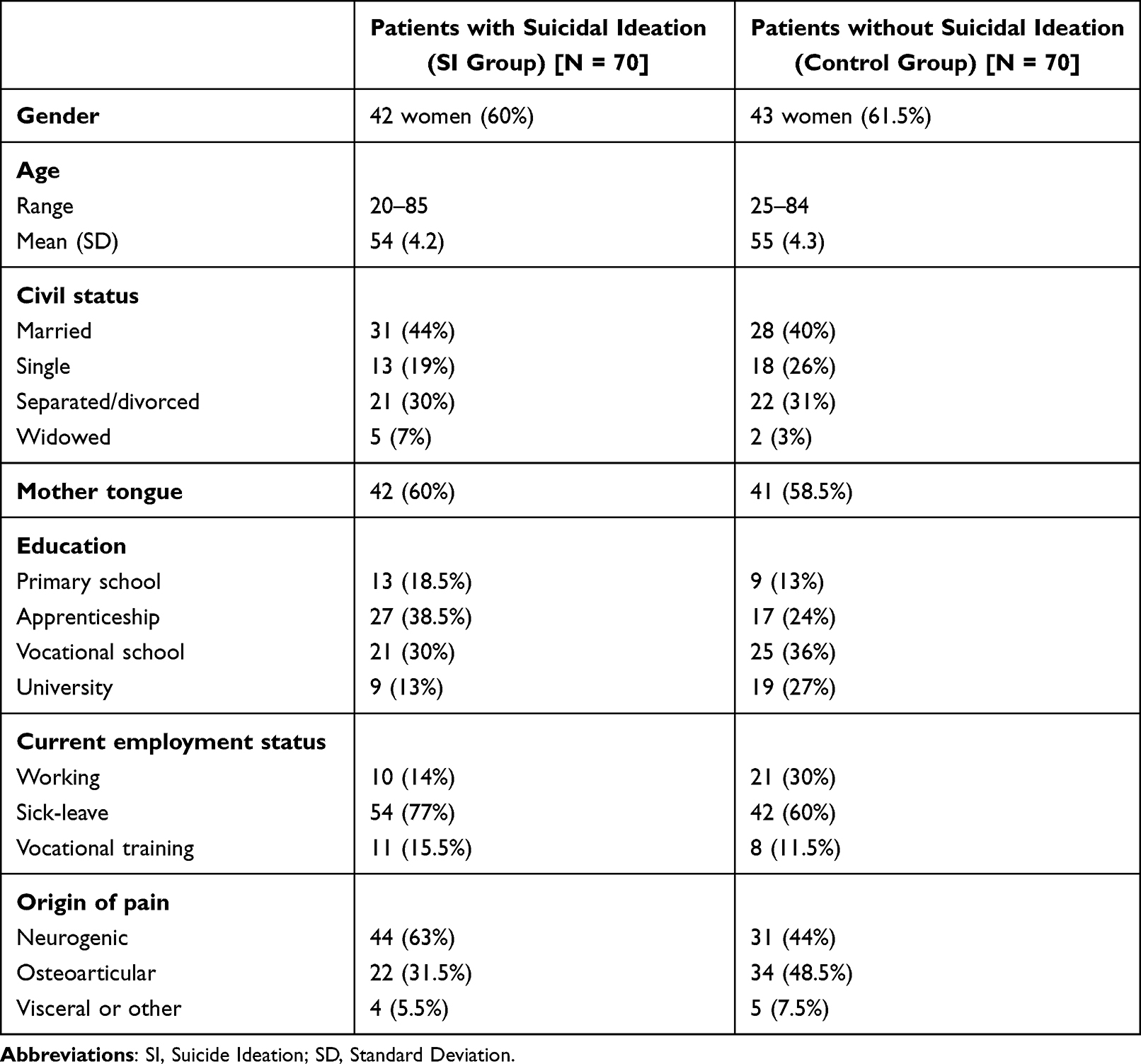 |
Table 1 Descriptive of the Sociodemographic and Origin of Pain Data |
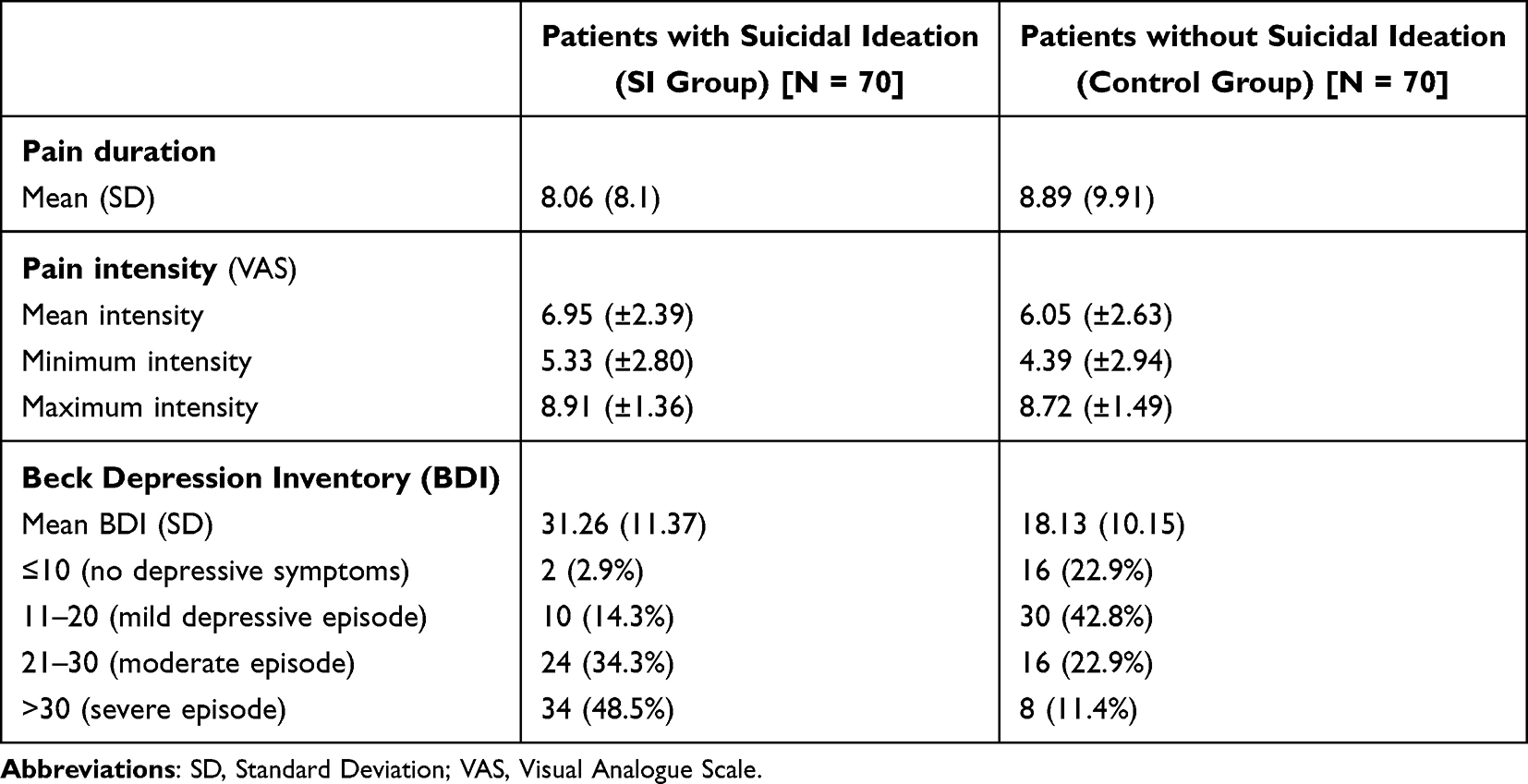 |
Table 2 Mean and Standard Deviation of Pain and Depression in Both Groups |
Results
Results Concerning BDI and SSI
As expected, the difference between the two groups on the BDI-II was statistically very significant (F=1.064; t=7.21 df=138; p<0.001, d=1.22), which confirms the presence of more numerous and intense depressive symptoms in the patients of the SI group as compared to the control group.
Much in the same line, in the SI group, depression and severity of suicidal ideation, as measured by the Scale for Suicide Ideation (SSI) were strongly and positively correlated (R= 0.575; p<0.001).
The MINI structured clinical interview conducted with the SI group confirmed the relevance of the inclusion of the patients in this group, since the interview confirmed a depressive episode in most patients (68/70, or 97.1%).
Results Concerning DS and SSI
In this study, we initially examined the relationship of the demoralization construct and its relationship to suicidal ideation. In the SI group, the mean score on the DS was 38.36 (SD±15.84). In contrast, in the control group, the mean score on the DS was 12.07 (SD±6.98). The difference between the two groups, SI and control, was statistically highly significant (F=1.49; t=9.44; df=137; p<0.001) with a large effect size (d=1.6).
In addition, in patients with high demoralization (with a DS score≥30) in the two groups, the difference between the SI and control group was very significant (F=9.04; t=2.9; df=63; p=0.005) with a large effect size too (d=1.02).
Furthermore, the DS and SSI were positively correlated in the patients of the SI group (R= 0.498; p<0.001). There was also a strong positive correlation between the DS and the BDI-II in the two groups, SI and control, as assessed with the BDI scale (R=0.749; p<0.001 for the SI group and R=0.704; p<0.001 for the control group).
Discussion
The primary aim of this study was to investigate the relationship between suicidal ideation and demoralization in patients suffering from chronic pain. The results first highlight a statistically significant difference on the demoralization scale (DS) between the SI group and the control group. In addition, we found a significant difference between the patients of the two groups (SI and control) who had a high DS score (≥30). On the other hand, when considering those patients with a lower degree of demoralization (<30), the between-group difference was also very significantly different with the patients of the control group displaying lower scores on the DS.
Furthermore, there is a strong positive correlation between the DS score and the SSI score in the SI group patients, meaning that high demoralization is associated with higher suicidal ideation as well. These results confirm the association between demoralization and suicidal ideation (both in terms of presence and intensity). This confirmation of our hypothesis is in line with the data in the literature, especially in patients suffering from physical illnesses,18,19,24 as well as in cancer patients.29,30 These findings also confirm those of a previous study indicating that one of the component of demoralization, loss of meaning in life, has a strong impact on suicidal ideation in this population.39
Our findings did not allow us to distinguish between the notions of depression compared to that of demoralization, since the two constructs show almost the same strong positive correlation with suicidal thoughts, the two also being strongly correlated with each other. While demoralization and depression may be worth considering as to different theoretical concepts, the necessity to separate them in the clinical practice seems less relevant.
Limitations of the Study
The limitations of the study need to be acknowledged. First, the size of the study sample. As the sample is small, it precludes the construction of subgroups using the participants’ sociodemographic and clinical characteristics; consequently, the results can only be considered as preliminary and as the initial step of an on-going study. Furthermore, the participants recruited were only those patients who self-reported SI by the BDI-II. Indeed, response bias may be induced by both under-reporting symptoms as a means of concealing them40 and over-reporting symptoms as a way of attracting attention or making a plea for getting help.41
Conclusion
Our study formally confirms the association between depression, demoralization and suicidal ideation in patients with chronic pain and thus the importance of considering demoralization and its components when taking care of these patients. A better understanding of these components could allow to further assess depression and target its various modes of expression. Finally, the issue may not be to separate depression and demoralization, but rather to address the patient’s profound psychological distress. Such specifically-designed patient-centered care could contribute to reduce the risk of suicide in this population by soothing at least part of the mental suffering related to the chronic pain experience. Further studies should address the complex relationship between these dimensions and provide new perspectives on the care of these patients.
Acknowledgments
We would like to thank the patients who spent time on our questionnaires and so accepted to contribute to our study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tang NK, Crane C. Suicidality in chronic pain: a review of the prevalence, risk factors and psychological links. Psychol Med. 2006;36(5):575–586. doi:10.1017/S0033291705006859
2. Fishbain DA, Lewis JE, Gao J. The pain suicidality association: a narrative review. Pain Med. 2014;15(11):1835–1849. doi:10.1111/pme.12463
3. Hassett AL, Aquino JK, Ilgen MA. The risk of suicide mortality in chronic pain patients. Curr Pain Headache Rep. 2014;18(8):436. doi:10.1007/s11916-014-0436-1
4. Calati R, Laglaoui Bakhiyi C, Artero S, Ilgen M, Courtet P. The impact of physical pain on suicidal thoughts and behaviors: meta-analyses. J Psychiatr Res. 2015;71:16–32. doi:10.1016/j.jpsychires.2015.09.004
5. Ilgen MA, Kleinberg F, Ignacio RV, et al. Noncancer pain conditions and risk of suicide. JAMA Psychiatry. 2013;70(7):692–697. doi:10.1001/jamapsychiatry.2013.908
6. Kikuchi N, Ohmori-Matsuda K, Shimazu T, et al. Pain and risk of completed suicide in Japanese men: a population-based cohort study in Japan (Ohsaki Cohort Study). J Pain Symptom Manage. 2009;37(3):316–324. doi:10.1016/j.jpainsymman.2008.03.012
7. Ratcliffe GE, Enns MW, Belik SL, Sareen J. Chronic pain conditions and suicidal ideation and suicide attempts: an epidemiologic perspective. Clin J Pain. 2008;24(3):204–210. doi:10.1097/AJP.0b013e31815ca2a3
8. Braden JB, Sullivan MD. Suicidal thoughts and behavior among adults with self-reported pain conditions in the national comorbidity survey replication. J Pain. 2008;9(12):1106–1115. doi:10.1016/j.jpain.2008.06.004
9. Ilgen MA, Zivin K, McCammon RJ, Valenstein M. Pain and suicidal thoughts, plans and attempts in the United States. Gen Hosp Psychiatry. 2008;30(6):521–527. doi:10.1016/j.genhosppsych.2008.09.003
10. Campbell G, Darke S, Bruno R, Degenhardt L. The prevalence and correlates of chronic pain and suicidality in a nationally representative sample. Aust N Z J Psychiatry. 2015;49(9):803–811. doi:10.1177/0004867415569795.
11. Smith MT, Edwards RR, Robinson RC, Dworkin RH. Suicidal ideation, plans, and attempts in chronic pain patients: factors associated with increased risk. Pain. 2004;111(1–2):201–208. doi:10.1016/j.pain.2004.06.016
12. Racine M, Choinière M, Nielson WR. Predictors of suicidal ideation in chronic pain patients: an exploratory study. Clin J Pain. 2014;30(5):371–378. doi:10.1097/AJP.0b013e31829e9d4d
13. Frank JD. Psychotherapy: the restoration of morale. Am J Psychiatry. 1974;131(3):271–274. doi:10.1176/ajp.131.3.271
14. Fava GA, Freyberger HJ, Bech P, et al. Diagnostic criteria for use in psychosomatic research. Psychother Psychosom. 1995;63(1):1–8. doi:10.1159/000288931
15. Fava GA, Fabbri S, Sirri L, Wise TN. Psychological factors affecting medical condition: a new proposal for DSM-V. Psychosomatics. 2007;48(2):103–111. doi:10.1176/appi.psy.48.2.103
16. Grassi L, Caruso R, Sabato S, Massarenti S, Nanni MG; The UniFe Psychiatry Working Group Coauthors. Psychosocial screening and assessment in oncology and palliative care settings. Front Psychol. 2015;5:1485. doi:10.3389/fpsyg.2014.01485
17. Mangelli L, Fava GA, Grandi S, et al. Assessing demoralization and depression in the setting of medical disease. J Clin Psychiatry. 2005;66(3):391–394. doi:10.4088/jcp.v66n0317
18. Clarke DM, Kissane DW. Demoralization: its phenomenology and importance. Aust N Z J Psychiatry. 2002;36(6):733–742. doi:10.1046/j.1440-1614.2002.01086.x
19. Kissane DW, Clarke DM, Street AF. Demoralization syndrome--a relevant psychiatric diagnosis for palliative care. J Palliat Care. 2001;17(1):12–21. doi:10.1177/082585970101700103
20. Kissane DW, Wein S, Love A, Lee XQ, Kee PL, Clarke DM. The Demoralization Scale: a report of its development and preliminary validation. J Palliat Care. 2004;20(4):269–276. doi:10.1177/082585970402000402
21. de Figueiredo JM. Distress, demoralization and psychopathology: diagnostic boundaries. Eur J Psychiatry. 2013;27(1):61–73. doi:10.4321/s0213-61632013000100008
22. Marchesi C, Maggini C. Socio-demographic and clinical features associated with demoralization in medically ill in-patients. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):824–829. doi:10.1007/s00127-007-0230-z
23. Block AR. Demoralization, patient activation, and the outcome of spine surgery. Healthcare. 2016;4(1):11. doi:10.3390/healthcare4010011
24. Robinson S, Kissane DW, Brooker J, Hempton C, Burney S. The relationship between poor quality of life and desire to hasten death: a multiple mediation model examining the contributions of depression, demoralization, loss of control, and low self-worth. J Pain Symptom Manage. 2017;53(2):243–249. doi:10.1016/j.jpainsymman.2016.08.013.
25. Schildkraut JJ, Klein DF. The classification and treatment of depressive disorders. In: Shader RI, editor. Manual of Psychiatric Therapeutics: Practical Psychopharmacology & Psychiatry. Boston, MA: Little, Brown & Company; 1975:39–61.
26. Kissane DW. Distress, demoralization and depression in palliative care. Curr Ther. 2000;41(6):14–19.
27. Angelino AF, Treisman GJ. Major depression and demoralization in cancer patients: diagnostic and treatment considerations. Support Care Cancer. 2001;9(5):344–349. doi:10.1007/s005200000195
28. Jacobsen J, Vanderwerker L, Block S, Friedlander R, Maciejewski P, Prigerson H. Depression and demoralization as distinct syndromes: preliminary data from a cohort of advanced cancer patients. Indian J Palliat Care. 2006;12(1):8. doi:10.4103/0973-1075.25913
29. Fang CK, Chang MC, Chen PJ, et al. A correlational study of suicidal ideation with psychological distress, depression, and demoralization in patients with cancer. Support Care Cancer. 2014;22(12):3165–3174. doi:10.1007/s00520-014-2290-4.
30. Tang PL, Wang HH, Chou FH. A systematic review and meta-analysis of demoralization and depression in patients with cancer. Psychosomatics. 2015;56(6):634–643. doi:10.1016/j.psym.2015.06.005
31. Costanza A, Vasileios C, Ambrosetti J, et al. Demoralization in suicide: a systematic review. J Psychosom Res. 2022;157:110788. doi:10.1016/j.jpsychores.2022.110788
32. Costanza A, Chytas V, Mazzola V, et al. The role of demoralization and meaning in life (DEMIL) in influencing suicidal ideation among patients affected by chronic pain: protocol of a single-center, observational, case-control study. JMIR Res Protoc. 2020;9(11):e24882. doi:10.2196/24882
33. Bourque P, Beaudrette D. Etude psychométrique du questionnaire de dépression de Beck auprès d’un échantillon d’étudiants universitaires francophones. Rev Can Sci Comport. 1982;14(3):211–218.
34. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33;quiz 34–57.
35. Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the scale for suicide ideation. J Consult Clin Psychol. 1979;47(2):343–352. doi:10.1037//0022-006x.47.2.343
36. Sokero TP, Melartin TK, Rytsälä HJ, Leskelä US, Lestelä-Mielonen PS, Isometsä ET. Suicidal ideation and attempts among psychiatric patients with major depressive disorder. J Clin Psychiatry. 2003;64(9):1094–1100. doi:10.4088/jcp.v64n0916
37. de Beurs DP, Fokkema M, O’Connor RC. Optimizing the assessment of suicidal behavior: the application of curtailment techniques. J Affect Disord. 2016;196:218–224. doi:10.1016/j.jad.2016.02.033
38. Baertschi M, Costanza A, Canuto A, Weber K. The dimensionality of suicidal ideation and its clinical implications. Int J Methods Psychiatr Res. 2019;28(1):e1755. doi:10.1002/mpr.1755
39. Costanza A, Chytas V, Piguet V, et al. Meaning in life among patients with chronic pain and suicidal ideation: mixed methods study. JMIR Form Res. 2021;5(6):e29365. doi:10.2196/29365
40. Schnyder U, Valach L, Bichsel K, Michel K. Attempted suicide. Gen Hosp Psychiatr. 1999;21(1):62–69. doi:10.1016/s0163-8343(98)00064-4
41. Racine M. Chronic pain and suicide risk: a comprehensive review. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):269–280. doi:10.1016/j.pnpbp.2017.08.020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Resilience and Depressive Symptoms Mediated Pathways from Social Support to Suicidal Ideation Among Undergraduates During the COVID-19 Campus Lockdown in China
Zhang X, Liu X, Mi Y, Wang W, Xu H
Psychology Research and Behavior Management 2022, 15:2291-2301
Published Date: 23 August 2022
Loneliness and Pain Catastrophizing Among Individuals with Chronic Pain: The Mediating Role of Depression
Wilson JM, Colebaugh CA, Meints SM, Flowers KM, Edwards RR, Schreiber KL
Journal of Pain Research 2022, 15:2939-2948
Published Date: 16 September 2022
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Prevalence and Factors Associated with Suicidal Ideation Among Older People with Visual Impairments Attending an Eye Center During the COVID-19 Pandemic: A Hospital-Based Cross-Sectional Study
Tantirattanakulchai P, Hounnaklang N, Pongsachareonnont PF, Khambhiphant B, Win N, Tepjan S
Clinical Ophthalmology 2023, 17:917-930
Published Date: 19 March 2023
The Interconnection Between Social Support and Emotional Distress Among Individuals with Chronic Pain: A Narrative Review
Franqueiro AR, Yoon J, Crago MA, Curiel M, Wilson JM
Psychology Research and Behavior Management 2023, 16:4389-4399
Published Date: 27 October 2023