Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Demographic variables, clinical aspects, and medicolegal implications in a population of patients with adjustment disorder
Authors Anastasia A, Colletti C, Cuoco V, Quartini A, Urso S, Rinaldi R, Bersani G ![]()
Received 18 July 2015
Accepted for publication 16 November 2015
Published 1 April 2016 Volume 2016:12 Pages 737—743
DOI https://doi.org/10.2147/NDT.S92637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Annalisa Anastasia,1 Chiara Colletti,1 Valentina Cuoco,1 Adele Quartini,1 Stefania Urso,2 Raffaella Rinaldi,2 Giuseppe Bersani1
1Department of Medical-Surgical Sciences and Biotechnologies, Faculty of Pharmacy and Medicine, Sapienza University of Rome, 2Department of Anatomical, Istological, Forensic and Locomotor System Sciences, Sapienza University of Rome, Rome, Italy
Introduction: Although adjustment disorder (AD) is considered as residual diagnosis and receives little attention in research, it plays an important role in clinical practice and also assumes an increasingly important role in the field of legal medicine, where the majority of diagnostic frameworks (eg, mobbing) often refer to AD. Our study aimed to look for specific stressor differences among demographic and clinical variables in a naturalistic setting of patients with AD.
Methods: A restrospective statistical analysis of the data of patients diagnosed with AD from November 2009 to September 2012, identified via manual search from the archive of the outpatient setting at the University Unit of Psychiatry “A. Fiorini” Hospital, Terracina (Latina, Italy), was performed.
Results: The sample consisted of 93 patients (46 males and 47 females), aged between 26 and 85, with medium–high educational level who were mainly employed. In most cases (54.80%), a diagnosis of AD with mixed anxiety and depressed mood was made. In all, 72% of the sample reported a negative family history for psychiatric disorders. In 22.60%, a previous history of psychopathology, especially mood disorders (76.19%), was reported. The main stressors linked to the development of AD were represented by working problems (32.30%), family problems (23.70%), and/or somatic disease (22.60%) with significant differences with respect to age and sex. Half of the patients were subjected to a single first examination; 24.47% requested a copy of medical records.
Conclusion: Confirming previous data from previous reports, our results suggest that AD may have a distinct profile in demographic and clinical terms. Increased scientific attention is hoped, particularly focused on addressing a better definition of diagnostic criteria, whose correctness and accuracy are critical, especially in situations with medicolegal implications.
Keywords: adjustment disorder, diagnostic criteria, stressor, mobbing, medicolegal
Introduction
Talking about adjustment disorder (AD) immediately leads to a simple first observation: the discrepancy between its common use in clinical setting and, at the same time, its poor consideration in the field of research. Moreover, there are critical issues about this diagnosis, not only in nosological terms but also, with increasing relevance, in the field of legal medicine.
Over the last few decades, a few studies have dealt with AD. Within these studies, the most shared concept is that diagnostic criteria are vague and not so helpful in clinical practice.1,2 AD has been regarded as one of the most ill-defined mental disorders.3 Conceptually, it is an intermediate category between healthy normal responses to stress and affective conditions such as anxiety and mood disorders.4,5 At present, it is included in the “Trauma and Stress Related Disorder” category of Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). Noteworthy, the first DSM-5 criterion of AD is its temporal relationship to an identifiable stressor or stressors. Unfortunately, what is a “stressor” is not clearly defined and only its effects can identify this. Moreover, the impact of a stressor depends on both its duration and intensity, both of which, in view of the lack of qualifiable and quantifiable criteria, are difficult to measure to date.2 The second DSM-5 criterion of AD is the presence of clinically significant symptoms in excess with respect to what would be expected. Even in this case, there is no method to assess that distress is out of proportion to the intensity of the stressor and what constitutes a normal response varies widely across cultures and social groups.1 To note, this latter aspect has been taken into account in the current version of DSM; however, the same widespread uncertainty remains.
Probably because of the poor definition and the absence of a reliable and valid diagnostic tool, AD is actually a minor object of research compared to other disorders.5–7 It is often described as the “wastebasket” of the psychiatric classification.1–3,8 As a matter of fact, in clinical practice, AD has been mostly used as a residual category for patients who do not meet the diagnostic criteria for depressive or anxiety disorders or as a provisional diagnosis when it is not yet defined whether or not a posttraumatic or mood disorder will emerge.3 One of the consequences of considering it as a subclinical category is that it is viewed as mild in comparison to other full-blown conditions, particularly with respect to suicidal behavior.6 In this regard, it has been found that suicidal behavior seems to be present among people with this diagnosis, certainly representing an important potential aftermath of AD diagnosis.9 Moreover, a shorter interval (<1 month) between suicidal intent communication and act in AD has been reported in comparison to other disorders (depression 3 months, bipolar disorder 30 months, and schizophrenia 47 months).1,4
Apart from prognostic and therapeutic purposes, the necessity of a correct diagnosis is also important for medicolegal implications. In this field, the majority of diagnostic frameworks (eg, mobbing, bullying, damage mourning, posttrauma biological damage) refer to this nosological entity. AD is the most frequent consequence of bullying at work, described at higher level of prevalence in specific occupations, above all associated with recurrent sickness absence involving a significant cost in terms of social security support and missed workdays.10 Since it has been perceived as a mild diagnosis, one of its uses is to enable treatment of patients not otherwise diagnosed who require financial support from health care insurance companies.5 Thus, being deliberately provocative, AD would seems to play a starring role, a sort of big box in which all those situations requiring compensation for many different reasons are included. Hence, more than ever, there is a strong need to define precise criteria for AD diagnosis, such as to ensure the rigor, which is a characteristic of the medicolegal discipline. Some argue that a psychopathological revision of the current nosological concept of AD should be taken into consideration, given the high prevalence rates of this disorder and its scientific neglect.11–13 At the same time, many pitfalls in diagnostic criteria need to be addressed.1 First, what is a stressor and how can it be measured? What types of stressors cause AD? Furthermore, which processes underlie the interaction between the individual and the stressor? Which factors determine the result of this interaction? Is there a liability for the disorder? Can individuals at risk be characterized?2
Taken the former into consideration, our study aimed to look for specific stressor differences among demographic and clinical variables in a naturalistic setting of a population of patients diagnosed with AD.
Methods
Subjects diagnosed with AD from November 2009 to September 2012 were identified via manual search from the archive of the outpatient setting at the University Unit of Psychiatry – “A. Fiorini” Hospital, Terracina (Latina, Italy). Ethical approval was granted by the ethics committee of A. Fiorini Hospital, Terracina (Latina, Italy). Written informed consent was obtained for all the patients recruited. A retrospective analysis of the data collected by a senior psychiatrist during the usual assessment of the patient and periodic visits carried out on the base of individual needs was performed.
The following were selected to be used in this study:
- Demographic variables: sex, age, educational level, and occupation.
- Clinical variables: diagnosis and diagnostic subtypes according to Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR) criteria for AD; family history of psychiatric disorders; and previous history of personal psychopathology, comorbidity, and life stressors, leading to the development of the disorder.
- Medicolegal-related variables: number of visits and requests for medical record.
Statistical analysis
Statistical analysis was performed using SPSS version 16 (SPSS Inc., Chicago, IL, USA). Once subdivided all subjects in groups with respect to sex (male [M]/female [F]), age (15–34/35–54/55–74/75–90), educational level (primary school/secondary school/high school/university), occupation (yes/no), family history of psychiatric disorders (yes/no), past and/or current psychiatric disorders (yes/no), somatic diseases (yes/no), and/or life stressors (jobs related/family related/bereavement/casualty/somatic diseases/others), independent t-tests, Pearson’s chi-square tests, and univariate analyses of variance were carried out (as appropriate) to attempt comparisons between M and F subjects, with regard to age and specific life stressors, among the various life stressors, with regard to age, and also among the various AD subtypes, with regard to age and sex. The significant threshold was set at P≤0.05.
Results
Demographic variables
The sample consisted of 93 patients (46 M [49.5%] and 47 F [50.50%]), aged between 26 years and 85 years (mean age 52.58±13.18). The age group 35–54 was the most represented (45 patients [48.40%]), followed by the group 55–74 (33 patients [35.50%]), the 15–34 (eight patients [8.60%]), and the 75–90 (six patients [6.50%]) groups. Overall, our sample shows a medium–high educational level (47 patients – high school diploma or higher [50.6%], 27 patients – secondary school [29.0%], and 14 patients – primary school [15.10%]). Most patients were in regular work (65 patients [69.90%]), while only a minority of them resulted jobless (29 patients [29.0%]).
Clinical variables
In most cases, a diagnosis of AD with mixed anxiety and depressed mood was made (51 patients [54.80%]). The rest of the subjects received a diagnosis of AD with depressed mood (25 patients [26.90%]), with anxiety (15 patients [16.10%]), or else with conducts disorder (two patients [2.20%]). About the medical history, 67 patients (72.00%) reported a negative family history for psychiatric disorders, with only 17 patients (18.30%) reporting some sort of psychiatric familiarity, at the same time with 64 patients (68.8%) denying a previous history of psychiatric disorders, with the remaining 21 patients (22.60%) reporting a previous history of psychopathology, especially mood disorders (76.19%). The majority of subjects developed an AD in response to stressful events in the workplace (30 patients [32.30%]). For a good percentage of the sample, the main stressor was instead represented by family problems (22 patients [23.70%]), followed by organic, degenerative, or neoplastic diseases (21 patients [22.60%]), bereavement (six patients [6.50%]), or casualties (five patients [5.40%]) (Figure 1). Comparing the two sex groups, no significant differences were found between M and F subjects with respect to age (F=53.87±13.57 vs M=53.87±13.57: t(90)=0.964, P=0.338), age group, χ2(3)=1.419, P=0.701; AD subtypes, χ2(3)=5.511, P=0.138; family history of psychiatric disorders, χ2(1)=0.026, P=0.872; past and/or current psychiatric disorders, χ2(1)=8.41, P=0.004 and/or χ2(1)=0.098, P=0.754, respectively; and/or somatic diseases, χ2(1)=0.000, P=0.988. Educational level was also similar between the two sex groups, χ2(3)=4.104, P=0.250. With respect to the various life stressors at the base of the diagnosis of AD, however, interesting sex differences were found among M subjects, job-related problems were chiefly reported (Figure 2) and among F subjects, family problems seemed to prevail, χ2(1)=8.41, P=0.004 (Figure 3). Noteworthy, an additional comparison between M and F subjects with respect to occupational level revealed a greater proportion of F subjects jobless as compared to M, χ2(1)=4.246, P=0.39. With respect to age, significant differences were found in the mean age of subjects reporting specific life stressors, F(5, 45)=4.061, P=0.002. Post hoc tests revealed younger ages in subjects reporting casualties as compared to those reporting job, family, and/or somatic problems (P=0.010, P=0.004, and P=0.000, respectively), at the same time revealing older ages among subjects reporting somatic diseases as compared to those reporting job problems and also as compared to those reporting bereavements (P=0.012 and P=0.014, respectively). In subjects subdivided with respect to sex, while no significant differences emerged in the mean age of F subjects reporting specific life stressors, still, mean age of M subjects reporting casualties resulted lower as compared to that of subjects reporting job problems, bereavements, and/or somatic diseases (P=0.009, P=0.047, and P=0.000, respectively), at the same time, with subjects reporting somatic diseases resulting older as compared to those reporting job and family problems (P=0.026 and P=0.048) (Figure 4). With regard to the diagnosis of AD, no significant differences emerged among the various AD subtypes with respect to age, F(3, 92)=0.581, P=0.629, and/or sex, χ2(3)=5.511, P=0.138.
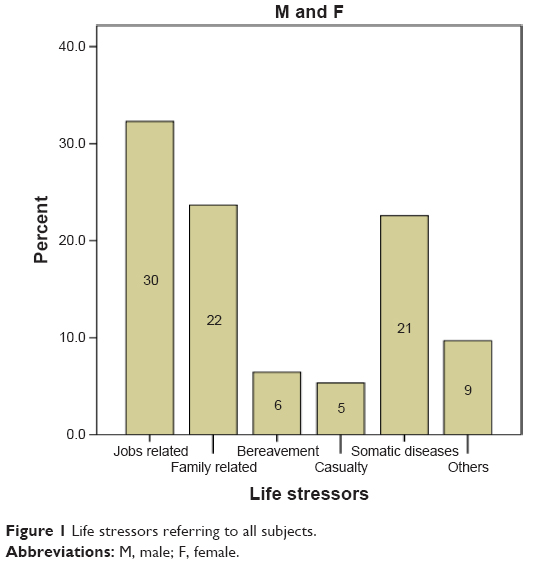 | Figure 1 Life stressors referring to all subjects. |
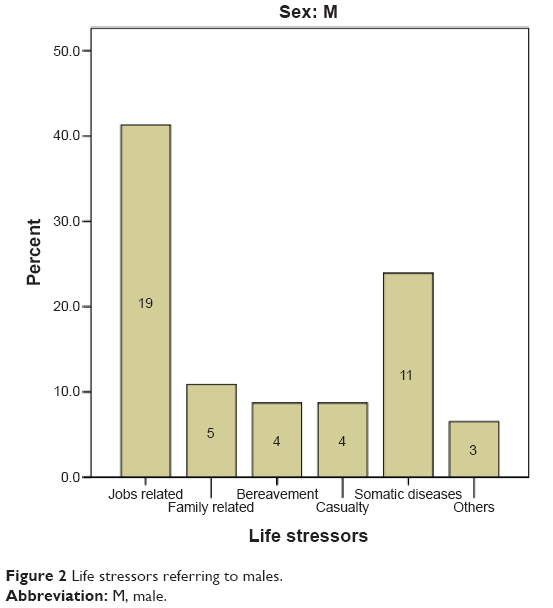 | Figure 2 Life stressors referring to males. |
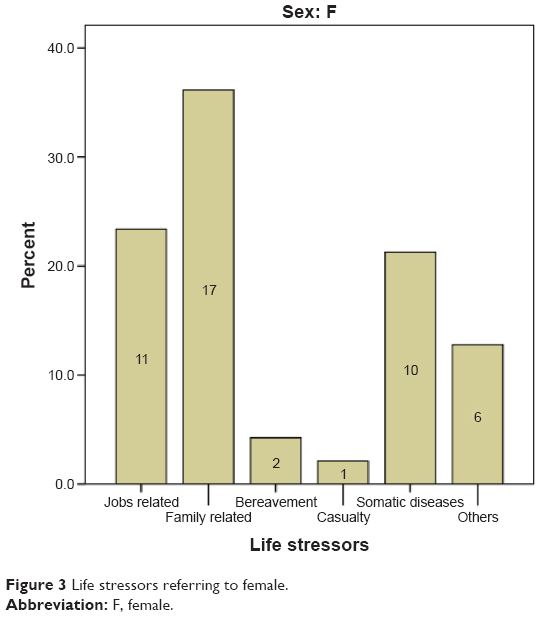 | Figure 3 Life stressors referring to female. |
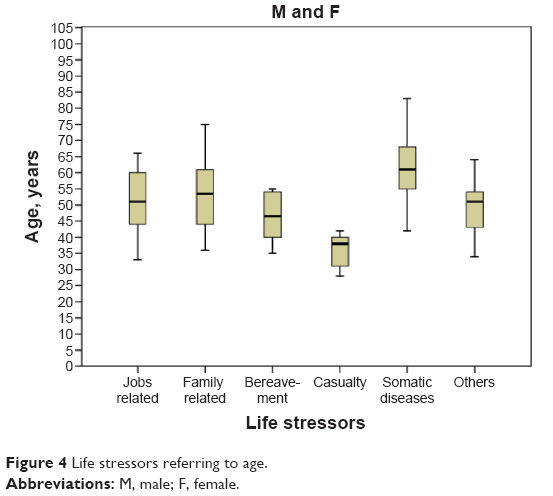 | Figure 4 Life stressors referring to age. |
Medicolegal-related variables
Interestingly, 50% (47 patients) of the sample was subjected to a single first examination and then did not continue the course of treatment over the considered period, while 24.47% of the subjects made request for medical records due to medicolegal reasons.
Discussion
In our outpatient service, people diagnosed with AD represent ~14% of all outpatients. Exploring demographic variables, the outline of a profile begins to take shape. Considering the entire sample, our results show that AD is diagnosed in M and in F with a comparable frequency, mainly in the age group 35–54 and 55–74. People affected by this disorder are mostly employed with a medium–high educational level. Considering the two sex groups, no significant differences with regard to these aspects were found, except for occupational level, which is higher in M than in F.
About the clinical variables, our results show that AD with mixed anxiety and depressed mood prevails, followed by AD with depressed mood and AD with anxiety. These data are consistent with the findings in literature.1,14,15 Noteworthy, differences in diagnostic subtypes do not seem to be relevant for treatment selection and are not associated with prognosis. Moreover, there are no substantial differences in patients’ demographic and clinical profiles with regard to the various AD subtypes.15,16 Indeed, also in our sample, no significant differences (with respect to age and sex) emerged among the different AD subtypes. However, the prevalence of these subtypes is one of the major problems of this diagnosis, that is to say, the overlap with subthreshold clinical manifestations of mood and anxiety disorders.17 This significant symptomatic overlap, especially considering a depressive episode, commonly leads to diagnostic difficulties.15 In this regard, some argue that a concept should be stressed: AD is a diagnosis based on the longitudinal course of symptoms, while a diagnosis of major depression is cross-sectional one, based on symptom numbers.18 Nevertheless, the fact remains that between AD and major depression, a severity distinction is made despite the potential fatal consequences of AD mentioned in the “Introduction”.
About the various life stressors in our total sample, the main events linked to the development of AD are represented by job-related problems, followed by family related problems and finally by somatic diseases. Our data are consistent with those reported in the literature, interestingly, with very similar percentages.19,20 With respect to this variable, additionally, interesting sex differences were found: among M, job-related problems were chiefly reported, among F, family problems prevailed. It is also true that in our sample, there are a greater proportion of jobless F subjects compared to M subjects. With respect to age, significant differences were found in the mean age of subjects reporting specific life stressors: patients reporting somatic diseases resulted older as compared to those reporting job and family problems. In Figure 5, a Venn diagram illustrating potential relationship among the most significant variables is provided. Far from the medicalization of life events, the analysis of the stressors underlying the development of AD points out a critical issue. AD and depression are frequently work-related mental problems, and the number of employees with psychiatric disorders, leading to the suspension of jobs, is increasing.21 Harassment and bad relationships in the workplace, job loss, and unemployment are factors that most often induce AD.20,22 This issue seems to gain increasing relevance, especially in medicolegal context. Regarding this, in our clinical sample, 50% of subjects underwent a single first examination, and then did not continue the course of treatment; at the same time, 24.47% of the subjects requested a copy of medical records for medicolegal reasons. In our opinion, these data are worthy of attention. In fact, the main issues surrounding AD diagnosis have clear implication from a medicolegal perspective, particularly concerning the application of the general forensic criteria, carefully taking into account that juridical realities may vary across different countries. The need for better-defined criteria, especially in terms of symptomatology severity rating, which is still lacking, is required, especially among those who are requested to adequately respond to forensic questions concerning single cases and to assess the outcome of a psychic trauma. The correlation between a given stressful event and clinical response connected to this is another issue, which assumes particular emphasis in legal medicine. In determining clinical response to a stressful event, it is very likely that different causal factors may act together.17 In addition to the stressor characteristics, one of these causal factors may be identified in premorbid individual characteristics. Our results show that only a minority of patients had a previous history of psychopathology and, among these, mood disorders prevailed. Other authors reported positive psychiatric disorders history in a higher percentage (53.8% of the cases, mostly anxiety disorder) among people suffering from AD.19 Personality seems to also be an important factor for successful adjustment in stressful situations. Because of the retrospective nature of the present study, the investigation of personality aspects could not be done. However, some research13,16,23 investigated this aspect and found that patients with AD with depressed mood had significantly higher scores on harm avoidance and lower scores on self-directedness, cooperativeness, and self-transcendence than healthy controls; moreover, there was a high frequency of comorbid somatic and mental disorders, especially of personality disorders (15%–73%). Patients came to our attention as a result of the occurrence of stressful events to which they were not able to cope with an effective and adaptive reaction, and then with unavoidable affective or behavioral changes in their lives. About that, another contributing factor may be represented by the individual social support system, which seems to play a crucial role.2
 | Figure 5 Venn diagram of the potential relationship among the most significant variables studied. |
Hence, it is actually very difficult for psychiatrists to deal with subjects with AD (including false-positive cases) and some argue that more realistic and useful methods should be taken into consideration. An enhancing cooperation or interaction between occupational health physicians and psychiatrists is desirable as well.21 Even with clear limitations, mainly due to the sample size and retrospective data analysis, the present study was carried out in the attempt to study in depth AD. In terms of future perspectives, future studies should investigate the relationship between other factors contributing to the AD development, including personality aspects. Moreover, the design of a system for defining severity level of symptomatology could be very useful, especially for medicolegal purposes.
Conclusion
AD is a psychiatric diagnosis that falls between normal behavior and the major psychiatric disorders, and thus produces diagnostic and taxonomical dilemmas1 that have clinical and legal impact. In DSM-5, it has been classified under Trauma and Stress Related Disorders but the main issues about diagnostic criteria remain unsolved. The data currently available in the literature, to which our results can be added, suggest that AD might have a distinct profile in demographic and clinical terms. Overall, this study highlights the need for an increased attention about AD from researchers and clinicians toward a better definition of diagnostic criteria, whose correctness and accuracy are critical, especially in those situations with medicolegal implications.
Disclosure
The authors report no conflicts of interest in this work.
References
Patra BN, Sarkar S. Adjustment disorder: current diagnostic status. Indian J Psychol Med. 2013;35(1):4–9. | ||
Gur S, Hermesh H, Laufer N, Gogol M, Gross-Isseroff R. Adjustment disorder: a review of diagnostic pitfalls. Isr Med Assoc J. 2005;7:726–731. | ||
Maercker ACR, Brewin RA, Bryant M, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11. World Psychiatry. 2013;12:198–206. | ||
Fernandez A, Mendive JM, Salvador-Carulla L, et al. Adjustment disorders in primary care: prevalence, recognition and use of services. Br J Psychiatry. 2012;201:137–142. | ||
Gil T. From crisis to adjustment disorder: a medicalization of a concept? Turk J Psychiatri Derg. 2013;24:50–54. | ||
Casey P, Doherty A. Adjustment disorder: implications for ICD-11 and DSM-5. Br J Psychiatry. 2012;201:90–92. | ||
Cornelius LR, Brouwer S, de Boer MR, Groothoff JW, van der Klink JJ. Development and validation of the diagnostic interview adjustment disorder (DIAD). Int J Methods Psychiatr Res. 2014;23(2):192–207. | ||
Strain JJ, Diefenbacher A. The adjustment disorders: the conundrums of the diagnoses. Compr Psychiatry. 2008;49(2):121–130. | ||
Gradus JL, Qin P, Lincoln AK, Miller M, Lawler E, Lash TL. The association between adjustment disorder diagnosed at psychiatric treatment facilities and completed suicide. Clin Epidemiol. 2010;2:23–28. | ||
Catalina-Romero C, Pastrana-Jiménez JI, Tenas-López MJ, et al. Long-term sickness absence due to adjustment disorder. Occup Med. 2012;62:375–378. | ||
Baumeister H, Kufner K. It is time to adjust the adjustment disorder category. Curr Opin Psychiatry. 2009;22(4):409–412. | ||
Baumeister H, Maercker A, Casey P. Adjustment disorder with depressed mood: a critique of its DSM-IV and ICD-10 conceptualisations and recommendations for the future. Psychopathology. 2009;42(3):139–147. | ||
Jäger M, Frasch K, Becker T. Adjustment disorders – nosological state and treatment options. Psychiatr Prax. 2008;35(5):219–225. | ||
Ferrer L, Kirchner T. Suicidal tendency in a sample of adolescent outpatients with adjustment disorder: gender differences. Compr Psychiatry. 2014;55(6):1342–1349. | ||
Zimmerman M, Martinez JH, Dalrymple K, Martinez JH, Chelminski I, Young D. Is the distinction between adjustment disorder with depressed mood and adjustment disorder with mixed anxious and depressed mood valid? Ann Clin Psychiatry. 2013;25(4):257–265. | ||
Doherty AM, Jabbar F, Kelly BD, Casey P. Distinguishing between adjustment disorder and depressive episode in clinical practice: the role of personality disorder. J Affect Disord. 2014;168:78–85. | ||
Semprini F, Fava GA, Sonino N. The spectrum of adjustment disorders: too broad to be clinically helpful. CNS Spectr. 2010;15(6):382–388. | ||
Casey P. Adjustment disorder: epidemiology, diagnosis and treatment. CNS Drugs. 2009;23(11):927–938. | ||
Semaan W, Hergueta T, Bloch J, et al. Cross-sectional study of the prevalence of adjustment disorder with anxiety in general practice. Encephale. 2001;27(3):238–244. | ||
Golinowska D, Florkowski A, Juszczak D. Analysis of the causes and determinants of reaction to severe stress and adjustment disorder patients on mental health clinics. Pol Merkur Lekarski. 2010;28(167):387–394. | ||
Nakamura J. Early detection and intervention for adjustment disorder and depression in the work place. Seishin Shinkeigaku Zasshi. 2012;114(9):1093–1099. | ||
Maercker A, Forstmeier S, Pielmaier L, Spangenberg L, Brähler E, Glaesmer H. Adjustment disorders: prevalence in a representative nationwide survey in Germany. Soc Psychiatry Psychiatr Epidemiol. 2012;47(11):1745–1752. | ||
Na KS, Oh SJ, Jung HY, et al. Temperament and character of young male conscripts with adjustment disorder: a case-control study. J Nerv Ment Dis. 2012;200(11):973–977. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.