Back to Journals » International Journal of General Medicine » Volume 15
Demographic, Clinical, and Co-Morbidity Characteristics of COVID-19 Patients: A Retrospective Cohort from a Tertiary Hospital in Kenya
Authors Shah R ![]() , Shah J, Kunyiha N, Ali SK, Sayed S, Surani S, Saleh M
, Shah J, Kunyiha N, Ali SK, Sayed S, Surani S, Saleh M
Received 9 February 2022
Accepted for publication 12 April 2022
Published 21 April 2022 Volume 2022:15 Pages 4237—4246
DOI https://doi.org/10.2147/IJGM.S361176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Reena Shah,1 Jasmit Shah,1 Nancy Kunyiha,1 Sayed K Ali,1 Shahin Sayed,2 Salim Surani,3 Mansoor Saleh4
1Department of Medicine, Aga Khan University, Nairobi, Kenya; 2Department of Pathology, Aga Khan University, Nairobi, Kenya; 3Department of Medicine & Pharmacology, Texas A&M University, College Station, TX, USA; 4Department of Hematology and Oncology, Aga Khan University, Nairobi, Kenya
Correspondence: Reena Shah, Department of Medicine, Aga Khan University, East Tower Block, 3 rd Parklands Avenue, P.O. Box 30270 – 00100, Nairobi, Kenya, Tel +254 735 338003, Email [email protected]
Introduction: The first documented case of COVID-19 in Kenya was recorded March of 2020. Co-morbidities including hypertension and diabetes have been associated with increased morbidity, hospitalization, and mortality among COVID-19 patients. This retrospective study describes the clinical characteristics, disease severity, and outcomes among the patient population at a tertiary hospital in Kenya.
Methods: This was a retrospective descriptive study of COVID-19 patients who were admitted between March 2020 and December 2020 at the Aga Khan University Hospital in Nairobi, Kenya. Data collected include patient demographic and baseline characteristics. Differences between patients who were known to have diabetes and hypertension during admission were compared for statistical significance. Difference between those who survived and those who died were also compared for statistical significance.
Results: A total of 913 records of patients were studied with a mean age of 51.2 years (SD = 16.7), 66.5% were male and 80.8% were of African origin. History of diabetes, hypertension, and HIV status were at 27.3%, 33.1%, and 2.3%, respectively. At presentation, 33.1% (302/913) of patients had known hypertension by history, and following admission, this proportion increased to 37.7% (344/913). At presentation, 27.3% (249/913) of patients had known diabetes. During hospital stay, 20.8% (190) more patients were found to have diabetes, raising the overall percent to 48.1% (439/913). When comparing diabetes and hypertension at baseline versus at the end of admission, diabetes increased by 20.8% (p < 0.001) and hypertension by 4.6% (p = 0.049). HIV co-infection was 2.3%, and no patient had tuberculosis.
Conclusion: This study showed a high incidence of co-morbidities in patients infected with COVID-19. Diabetes was most common, followed by hypertension. All patients admitted with COVID-19 infection should routinely be tested for diabetes with HbA1c and have regular blood pressure monitoring in order to diagnose occult diabetes and hypertension. Adverse outcomes were found in patients with these co-morbidities and should be monitored and treated appropriately.
Keywords: COVID-19, diabetes, hypertension, sub-Saharan Africa
Introduction
In December 2019, a novel coronavirus (SARS-CoV-2) emerged in China and spread globally within months, creating global havoc. This new infectious disease was named “COVID-19” in March 2020.1 As of January 8th, 2022, there have been over 306 million confirmed cases and 5.5 million deaths globally.2 The first documented case in Kenya was in March 2020, with initial cases reported in the capital, Nairobi. As of 2022, Kenya has had over 310,000 confirmed cases with over 5500 deaths.2 High poverty rates, limited access to healthcare, and high prevalence of chronic communicable diseases such as HIV and TB, likely affects the burden of COVID-19 and disease severity in low and middle-income countries (LMICs).3
Although the SARS-CoV-2 virus predominantly targets the respiratory system, its associated mortality involves multiple organ systems.4 A better understanding of the pathophysiology of the disease and the introduction of specific diagnostic, therapeutic, and clinical care measures throughout the pandemic have led to a reduction in in-hospital mortality rates, especially in well-resourced and high-income countries (HICs).5–7 Characterizing populations at increased risk of COVID-19 mortality is important for prioritizing interventions, particularly in low and middle-income countries (LMICs) where resources are limited. However, available data on risk factors for severe COVID-19 disease, including mortality, are mostly from HICs. In contrast, in-hospital mortality remains relatively high in LMICs, especially in Africa. This has been attributed to later presentation, the burden of underlying comorbidities, resource deficits, and fragile health care systems in Africa.8 This likely affects the burden of COVID-19 and disease severity in LMICs.9
Reports globally have indicated that certain factors, such as increasing age,10–12 male gender, comorbidities including cardiovascular disease, diabetes,10,13,14 chronic kidney disease, and increased body mass index15,16 are associated with adverse outcomes. In addition, low oxygen saturation, mechanical ventilation,11–13,17 and laboratory parameters such as a high CRP > 200, troponin >1, and D-dimer level >2500 have been associated with a critical illness.18 Diabetes has been associated with increased morbidity, hospitalization, and mortality among COVID-19 patients. In Africa, the prevalence of diabetes is significantly under-recognized due to inadequate screening and inadequate access to testing as a diagnostic priority. For patients with COVID-19, it can be important due to the high incidence of hospitalization in diabetics. Studies have shown that reduced expression of the Angiotensin-converting enzyme 2 (ACE 2) is thought to have a modulatory and antioxidant effect within the lung and is postulated as a mechanism for the exacerbation of lung disease in COVID-19 infected individuals with type-2 diabetes.19 Diabetes is correlated with increased rates of ARDS, poor outcomes, and an increase in mortality.20 The medications used for COVID-19, especially steroids in moderate and critical patients, can account for hyperglycaemia and overt diabetes developing in individuals with previously undiagnosed pre-diabetes.
Hospitals in Kenya’s various regional health services are categorized into different complexity levels depending on their size, technological resources, and the higher or lower availability of different clinical departments. Therefore, in ascending order of complexity, we have primary, secondary, and tertiary level hospitals. Tertiary hospitals often have specific clinical departments that provide high-level comprehensive specialized care. The Aga Khan University Hospital, Nairobi (AKUHN) is a tertiary referral hospital with 280 beds, including 36 in the critical care area. It serves the population of Nairobi and has referrals from within Kenya as well as in East and Central Africa. The patient population within this region often suffers from unique communicable diseases (such as human immunodeficiency virus (HIV), tuberculosis, malaria, and other infectious diseases), which do not normally infect individuals in high-income and high-resource regions. For example, the HIV prevalence in Kenya is estimated at about 4.9%.21
In the initial months of the pandemic, it was mandated by the Ministry of Health in Kenya to isolate all patients in health facilities for management and care due to the rising number of COVID-19 cases. This was later changed to admit only those who required supplemental oxygen and presented with comorbidities. Therefore, the severity of disease in hospitalized patients evolved with the pandemic, with patients ranging from asymptomatic to severe in initial months, to only severe/critical and those with co-morbidities in later months.
Limited information is available to describe characteristics, complications, and mortality due to COVID-19 infection among hospitalized patients in Kenya. This retrospective study describes the clinical characteristics, severity, and types of treatments, in addition to identifying risk factors associated with outcomes among patients hospitalized with COVID-19 at AKUHN.
Materials and Methods
Study Design and Participants
This study was a single center retrospective cohort study of patients admitted to the COVID-19 units over a 9-month time frame from March to December 2020. Ethical approval for this study was obtained from the Institutional Ethics Review Committee at AKUHN. A waiver for informed consent was obtained for this retrospective study. All related procedures were followed in accordance with the Declaration of Helsinki. No patient identifiers were used, and data was abstracted from medical chart records into the REDCap platform. The basis for this study is patient data collected through a retrospective review of hospital. Patients were included if they had a positive SARS-CoV-2 polymerase-chain-reaction (PCR) test through a nasopharyngeal or throat swab. As per hospital management protocol, all patients had history and physical examinations, vital signs recorded, routine labs on admission, which include hemogram, renal and liver function tests, CRP, HbA1c, and oxygen saturation monitoring. HIV testing was conducted for those who gave consent.
Data Management and Statistical Analysis
Data was obtained from medical records at AKUHN. The admission registry was used to identify the patients, and both their electronic and paper-based files were retrieved from medical records. Data was collected and managed through the Research Electronic Data Capture (REDCap) platform (Vanderbilt and National Institute of Health).22,23 Patient demographic data, medical history, baseline comorbidities, symptoms, and signs both at admission and during follow-up, laboratory findings, treatment strategy used for COVID-19, complications, and outcome data were collected.
Data was summarized using frequency tables and percentages for categorical data, whereas, for continuous data, means and standard deviations or medians and interquartile ranges were reported. Univariate analysis was performed using the nonparametric Kruskal–Wallis test to compare the continuous variables, and Fisher's exact test to compare the categorical variables between the outcome of the patients. To assess mortality risk, a multivariate logistic regression analysis was performed, and the associations between risk factors and outcomes were presented as odds ratios (ORs) and 95% confidence intervals after adjustment for confounders, including age, gender, race, and comorbidities including diabetes, hypertension, and COVID-19 severity as appropriate. Data analysis was performed using SPSS statistical software version 20.0 (IBM Corp). The significance level was set at α = 0.05, and all statistical tests performed were two-tailed.
Results
Demographic Data
During the study period, 913 patients who met our study inclusion criteria were included in the analysis. The mean age of the cohort was 51.2 years (SD=16.7), with the mean age of male patients at 52.7 years (SD=15.9) and the female patients at 48.11 years (SD=12.6). More than half of the patients were males (66.5%) and of African origin (80.8%). Travel during COVID-19 was significantly low, with 860 (94.2%) patients reporting not having travelled during this period, compared to 5.8% of patients who did report a history of travel before infection. Table 1 summarizes the overall demographic and baseline characteristics of patients presenting at admission. Out of all the counties present in the study (n=895), Nairobi County had the largest group of patients, with 85.1% admitted for COVID-19 infections. At presentation, 33.1% (302/913) of patients had known hypertension, and following admission, 4.6% additional patients were found to have hypertension, totalling 37.7% (344/913). Additionally, 27.3% (249/913) of patients had known diabetes at presentation, and following admission, 20.8% of additional patients were found to have diabetes, totalling 48.1% (439/913). HIV co-infection was 2.3%, and no patient had tuberculosis. When comparing hypertension and diabetes at baseline based on patient history as well as at the end of admission, hypertension and diabetes increased by 4.8% and 20.8%, respectively. Both measurements were statistically significant with p-value <0.05 (Table 2), revealing that a significant number of patients were unaware of their diabetes and hypertension.
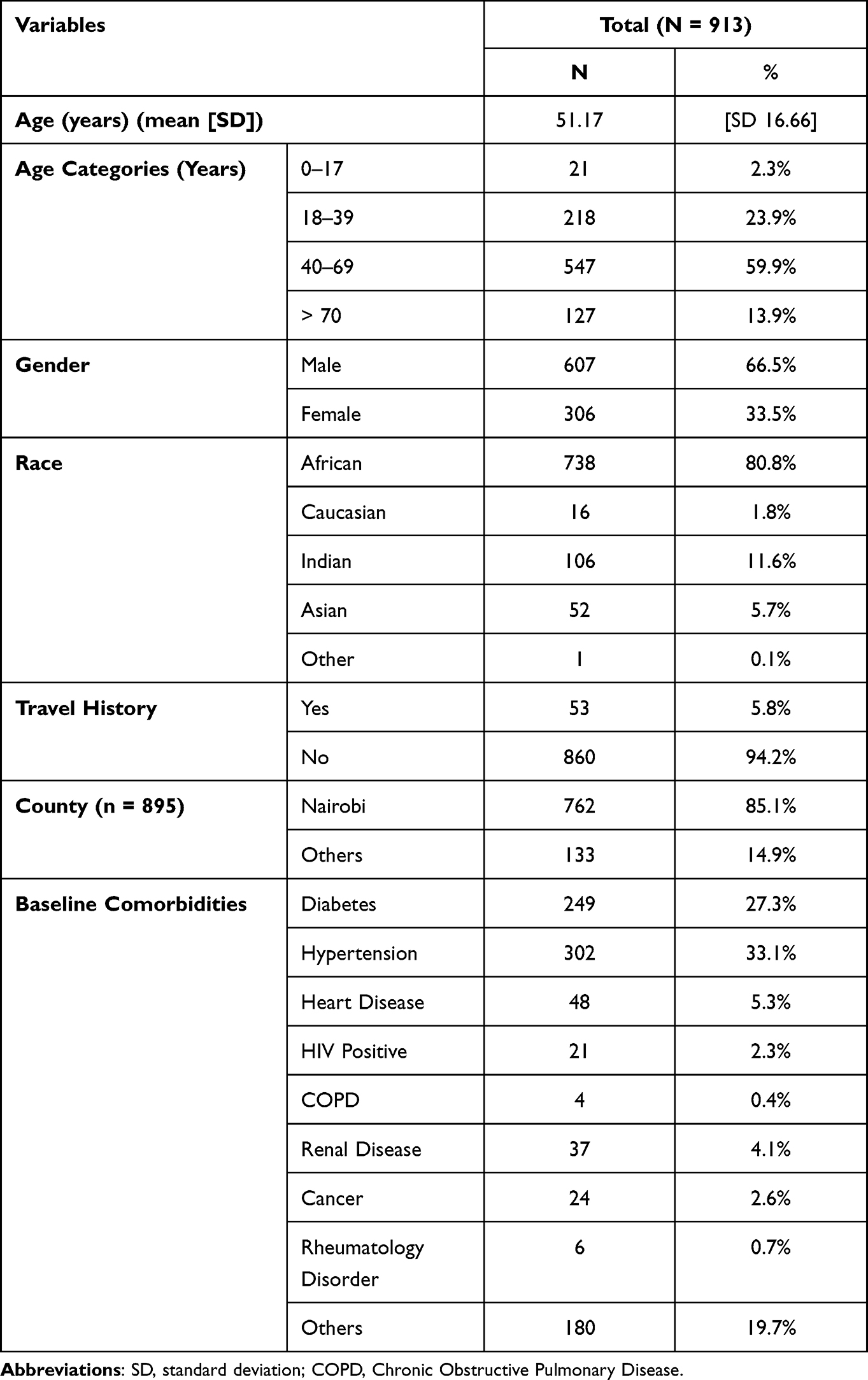 |
Table 1 Overall Demographic and Baseline Characteristics Presented at Admission |
 |
Table 2 Comparison of Diabetes and Hypertension Among History and During Admission to Outcome, Also Stratified by Gender |
Symptoms and Signs
More than half of the patients, 56.6%, had a cough on presentation, 42.6% of patients presented with fevers, 8.7% with vomiting, 7.3% with diarrhea, and 14.3% with headache. Additional details are provided in Table 3.
 |
Table 3 Symptoms and Vitals at Presentation During Admission and Stratified by Gender |
COVID-19 Severity
On day 1, the majority (87.4%) of admitting locations were from general COVID-19 isolation wards, followed by the ICU (intensive care unit) at 7.3%, and HDU (high dependency unit) at 5.3%. During hospital stays, 14.3% of hospitalized patients were in ICU and 7.8% in HDU. Details are shown in Table 4.
 |
Table 4 Patient Management, COVID-19 Severity and Treatment Characteristics |
At presentation, 43.4% of patients were on oxygen, 2.2% were on mechanical ventilation, and 0.1% were on ionotropic support. Overall, during their hospitalization, 8.3% of the patients were on mechanical ventilation, and 1% of patients were on ionotropic support. In this population, 46.7% had severe COVID-19, 3% had critical COVID-19, and 3.9% had moderate COVID-19.24
Mortality Comparison
The number of patients who survived was 834 (91%) and died was 79 (8.65%). The average age of patients who recovered was 49.8 years (SD =15.82), and those who died had a mean age of 65.7 years (SD =18.30), p<0.001. Male patients had higher mortality at 78.5%, compared to female patients at 21.5%, p=0.024. Patients who had diabetes and hypertension on presentation had higher mortality at 44.3% and 51.9%, respectively, compared to patients without diabetes and hypertension on presentation at 25.7% and 31.1%, respectively (p <0.001). Based on COVID-19 severity, 57% of the patients who had severe disease and 24.1% of the patients who had critical disease died. Details are shown in Table 5.
 |
Table 5 Comparison of Variables Based on Outcome (Recovered vs Died) |
A multivariate logistics regression analysis adjusted for age, gender, race, diabetes, hypertension, and COVID-19 severity was performed to determine the potential risk factors for mortality and the associations between risk factors and outcomes. The adjusted odds ratios of moderate, severe, and critical COVID-19 were 9.69 (95% CI =3.11–30.13), 4.76 (95% CI = 2.15 to 10.54), and 81.69 (95% CI = 25.07 to 266.19) p<0.001 respectively. The adjusted odds ratios (95% CI) of diabetes were 1.98 (95% CI = 1.10 to 3.57) p= 0.023, and hypertension was 0.84 (95% CI = 0.47 to 1.50) p=0.549, respectively (Table 6).
 |
Table 6 Multivariate Logistic Regression Analysis (Outcome = Recovered vs Dead) |
Discussion
This study showed a high incidence of co-morbidities in patients infected with COVID-19. Diabetes (48%) was the most common, followed by hypertension at 37.7%. When comparing diabetes and hypertension at baseline and at during admission, diabetes increased by 20.8% and hypertension by 4.6%, and both differences were statistically significant. Most studies in this region have shown hypertension as the most common co-morbidity, and a preprint from South Africa found hypertension at 37.4% and diabetes at 27.4%.25 Rathmann et al in their study of 35,865 patients with COVID-19 found an increase in incidence of diabetes with an incidence rate ratio (IRR) for type 2 diabetes of 1.28.26 In study by Barrett et al, they found the new diabetes diagnoses were 166% (based on IQVIA) and 31% (based on HealthVerity) more likely in patients with COVID-19 than among those without COVID-19.27
The prevalence of diabetes in Africa based on data from the International Diabetes Federation data is 2.2%.28 This is probably due to inadequate screening and lack of registries in these countries, and it is presumed that these numbers are a gross underestimation of the real situation. Diabetes Federation and WHO recognize that in Africa, 50% of those living with diabetes and pre-diabetes are undiagnosed, so it is not surprising to find a high number of patients during illness with overt diabetes. The WHO estimates the prevalence of diabetes in Africa to be 3.3%.29,30 Although the prevalence of diabetes is allegedly low, a surprisingly high number of patients with diabetes were admitted with COVID-19 to the facility (48%). Undiagnosed diabetes is usually asymptomatic, and additional stress hyperglycaemia with attendant COVID-19 in this situation may account for the large number of individuals diagnosed during admission, despite such low national prevalence rates. This was attributed to appropriate screening for diabetes on presentation. The percentage of patients known to have diabetes on admission was 27.3%. Meanwhile, HbA1c screening increased the number of diabetic patients following admission to 48.1%.
Diabetes mellitus has been shown to worsen COVID-19 outcomes, and there is evidence that COVID-19 also worsens dysglycaemia in diabetes through various mechanisms.31 The WHO has reported that 18.3% of COVID-19 deaths in the African region occur among individuals with diabetes.32 In our study, diabetic patients had an odds ratio of 1.98 for mortality with a p-value of 0.02. We advocate that all patients presenting with COVID-19 should have an HbA1c at admission to help diagnose diabetes. Pre-diabetes (HbA1c 5.8–6.4) would also alert clinicians to monitor patients who may develop diabetes with COVID-19 coinfection and following steroid treatment. Patients in the study had HbA1c done at presentation, and therefore, high numbers of diabetes are not attributable to steroid use alone.
Given the novelty of this illness and accepted best practices for its management, the mortality rate in the initial phase was very high, especially for patients who were older and immunocompromised. The overall mortality rate was 8.65% in our patient population. This was much lower than mortality rates observed in Tanzania and China, where the mortality was 31.8% and 28%, respectively.33,34 This low mortality may have been due to the high percentage of hospital admission rates for individuals testing positive for COVID-19, regardless of whether they required oxygen supplementation, as part of the government requirement in the initial duration of the pandemic they needed to be admitted. The mortality among critically ill patients has varied significantly among different studies and has ranged from 24–54%.35–39 In Tanzania, the mortality in severe and critically ill patients with COVID-19 was 26% and 68%. Severe and critical COVID-19 patients’ mortality in our population was 57% and 24.1% mortality, respectively, with the odds ratio of 4.76 and 81.69, respectively. Mortality rates among patients with severe and critical COVID-19 illness in our population is comparable to other African countries and developed countries. Among 503,409 patients who were admitted in hospital, patients with SARS-CoV-2 had higher mortality compared to patients who were negative for SARS-CoV-2. Moreover, the mortality increased with age.40
In the International Viral Infection and Respiratory Illness Universal Study Registry group (VIRUS), the COVID-19 patients’ overall mortality rate was 19%. The mortality rate for patients not receiving organ support was 8.2%, whereas it was a high of 49.8% in patients receiving mechanical ventilation.35 The percentage of patients receiving mechanical ventilation was much lower in our study than in the VIRUS group study (8.3% vs 24.3%), which could have been the reason for the difference in the overall mortality rates.35 In addition, lower mortality rates seen in our population may also be due to the younger patient population in our study as well as a lower admission threshold compared to other European and Northern American populations. In our study, the mortality was >50% in patients greater than 70 years of age, which is consistent with other studies.34,35 The average age of patients who died in our study was 65.7, and the average age of patients who survived in our study was 49.7.
This is one of the first studies reporting demographics, mortality, and morbidity risk factors from a tertiary center in Kenya. A retrospective study has its own set of limitations, and this study is not immune from those limitations. In the initial months of the pandemic, per government regulations, everyone who was positive for COVID-19 on PCR was admitted, falsely giving a very low overall mortality compared to other countries. The variation in therapeutic regimen among patients lacks details of patients on mechanical ventilation as well as information about steroid dosages given to patients. Moreover, the majority of patients admitted were from Nairobi, so this study may not accurately reflect the population of the entirety of Kenya or East Africa.
Conclusion
All patients admitted with COVID-19 infection should routinely be tested for diabetes with HbA1c and have regular glucose and blood pressure monitoring. In resource-challenged settings where HBA1c is not available, initial glucose is recommended with follow-up glucose levels during admission. Adverse outcomes were found in patients with these co-morbidities and should be monitored and treated appropriately.
The overall mortality was lower in the Kenyan population due to a variety of factors, such as the young population admission criteria, whereas the mortality among COVID-19 patients who were critically ill was consistent with other studies. The high prevalence of diabetes in patients admitted with COVID-19 (48%) (when compared to a national prevalence of 2.2%) raises a concern and an opportunity to protect and vaccinate those vulnerable individuals as a priority group to help further decrease the mortality rate. Despite several limitations of this study, this study offers insight into the disease-specific to the Kenyan population and provides opportunities to improve preventative and treatment measures in patients at risk of COVID-19. This is the first study to our knowledge presenting the demographic information of the patients at a tertiary hospital with COVID-19 in the Kenyan population.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gorbalenya AE, Baker SC, Baric RS, et al. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;5(4):536–544. doi:10.1038/s41564-020-0695-z
2. World Health Organization. WHO Coronavirus Disease (COVID-19) dashboard. Available from: https://covid19.who.int/.
3. Enos M, Sitienei J, Ong’ang’o J, et al. Kenya tuberculosis prevalence survey 2016: challenges and opportunities of ending TB in Kenya. PLoS One. 2018;13(12):e0209098. doi:10.1371/journal.pone.0209098
4. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
5. Dennis JM, McGovern AP, Vollmer SJ, Mateen BA. Improving survival of critical care patients with Coronavirus disease 2019 in England: a National Cohort Study, March to June 2020. Crit Care Med. 2021;49(2):209–214. doi:10.1097/CCM.0000000000004747
6. Horwitz LI, Jones SA, Cerfolio RJ, et al. Trends in COVID-19 risk-adjusted mortality rates. J Hosp Med. 2021;16(2):90–92. doi:10.12788/jhm.3552
7. Anesi GL, Jablonski J, Harhay MO, et al. Characteristics, outcomes, and trends of patients with COVID-19-related critical illness at a learning health system in the United States. Ann Intern Med. 2021;174(5):613–621. doi:10.7326/M20-5327
8. Biccard BM, Gopalan PD, Miller M. Patient care and clinical outcomes for patients with COVID-19 infection admitted to African high-care or intensive care units (ACCCOS): a multicentre, prospective, observational cohort study. Lancet. 2021;397(10288):1885–1894. doi:10.1016/S0140-6736(21)00441-4
9. Walker PGT, Whittaker C, Watson OJ, et al. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science. 2020;369(6502):413–422. doi:10.1126/science.abc0035
10. Wu Z, McGoogan JM. Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
11. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area. JAMA. 2020;323(20):2052–2059. doi:10.1001/jama.2020.6775
12. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. 2020;323(18):1775–1776. doi:10.1001/jama.2020.4683
13. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi:10.1136/bmj.m1966
14. Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–436. doi:10.1038/s41586-020-2521-4
15. Lighter J, Phillips M, Hochman S, et al. Obesity in patients younger than 60 years is a risk factor for COVID-19 hospital admission. Clin Infect Dis. 2020;71(15):896–897. doi:10.1093/cid/ciaa415
16. Tartof SY, Qian L, Hong V, et al. Obesity and mortality among patients diagnosed with COVID-19: results from an integrated health care organization. Ann Intern Med. 2020;173(10):773–781. doi:10.7326/M20-3742
17. Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. doi:10.1136/bmj.m1091
18. Castro VM, McCoy TH, Perlis RH. Laboratory findings associated with severe illness and mortality among hospitalized individuals with Coronavirus Disease 2019 in Eastern Massachusetts. JAMA Netw Open. 2020;3(10):e2023934. doi:10.1001/jamanetworkopen.2020.23934
19. Tikellis C, Thomas MC. Angiotensin-converting enzyme 2 (ACE2) is a key modulator of the renin angiotensin system in health and disease. Int J Pept. 2012;2012:256294. doi:10.1155/2012/256294
20. Huang I, Lim MA, Pranata R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia - A systematic review, meta-analysis, and meta-regression. Diabetes Metab Syndr. 2020;14(4):395–403. doi:10.1016/j.dsx.2020.04.018
21. Ministry of Health. Kenya HIV Estimates: report 2018; 2018. Available from: https://nacc.or.ke/wp-content/uploads/2018/11/HIV-estimates-report-Kenya-20182.pdf.
22. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
23. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
24. National Institutes of Health. Clinical spectrum of SARS-CoV-2 infection; 2021. Available from: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/.
25. Jassat W, Cohen C, Tempia S, et al. A national cohort study of COVID-19 in-hospital mortality in South Africa: the intersection of communicable and non-communicable chronic diseases in a high HIV prevalence setting. medRxiv. 2021. doi:10.1101/2020.12.21.20248409
26. Rathmann W, Kuss O, Kostev K. Incidence of newly diagnosed diabetes after Covid-19. Diabetologia. 2022:1–6. doi:10.1007/s00125-022-05670-0
27. Barrett CE, Koyama AK, Alvarez P, et al. Risk for newly diagnosed diabetes >30 days after SARS-CoV-2 infection among persons aged <18 years - United States, March 1, 2020-June 28, 2021. MMWR Morb Mortal Wkly Rep. 2022;71(2):59–65. doi:10.15585/mmwr.mm7102e2
28. International Diabetes Federation. Diabetes around the world in 2021. 2019. Available from: https://diabetesatlas.org/.
29. Ministry of Public Health and Sanitation. Kenya National Diabetes Strategy 2010–2015; 2010. Available from: https://www.worlddiabetesfoundation.org/sites/default/files/WDF09-436%20Kenya%20National%20Diabetes%20Strategy%202010-2015%20%20-%20Complete.pdf.
30. Chege MP. Risk factors for type 2 diabetes mellitus among patients attending a rural Kenyan hospital. Afr J Prim Health Care Fam Med. 2010;2(1):096. doi:10.4102/phcfm.v2i1.96
31. Pal R, Bhansali A. COVID-19, diabetes mellitus and ACE2: the conundrum. Diabetes Res Clin Pract. 2020;162:108132. doi:10.1016/j.diabres.2020.108132
32. World Health Organization. COVID-19 more deadly in Africans with diabetes; 2021. Available from: https://www.afro.who.int/news/covid-19-more-deadly-africans-diabetes.
33. Kassam N, Aghan E, Aziz O, et al. Factors associated with mortality among hospitalized adults with COVID-19 pneumonia at a private tertiary hospital in Tanzania: a retrospective cohort study. Int J Gen Med. 2021;14:5431–5440. doi:10.2147/IJGM.S330580
34. Weiss P, Murdoch DR. Clinical course and mortality risk of severe COVID-19. Lancet. 2020;395(10229):1014–1015. doi:10.1016/S0140-6736(20)30633-4
35. Domecq JP, Lal A, Sheldrick CR, et al. Outcomes of patients with Coronavirus disease 2019 receiving organ support therapies: the international viral infection and respiratory illness universal study registry. Crit Care Med. 2021;49(3):437–448. doi:10.1097/CCM.0000000000004879
36. Grasselli G, Greco M, Zanella A, et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med. 2020;180(10):1345–1355. doi:10.1001/jamainternmed.2020.3539
37. Wendel Garcia PD, Fumeaux T, Guerci P, et al. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine. 2020;25:100449. doi:10.1016/j.eclinm.2020.100449
38. Gupta S, Hayek SS, Wang W, et al. Factors associated with death in critically ill patients with Coronavirus disease 2019 in the US. JAMA Intern Med. 2020;180(11):1436–1447. doi:10.1001/jamainternmed.2020.3596
39. Xie J, Wu W, Li S, et al. Clinical characteristics and outcomes of critically ill patients with novel coronavirus infectious disease (COVID-19) in China: a retrospective multicenter study. Intensive Care Med. 2020;46(10):1863–1872. doi:10.1007/s00134-020-06211-2
40. Finelli L, Gupta V, Petigara T, Yu K, Bauer KA, Puzniak LA. Mortality among US patients hospitalized with SARS-CoV-2 infection in 2020. JAMA Netw Open. 2021;4(4):e216556. doi:10.1001/jamanetworkopen.2021.6556
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.