Back to Journals » Clinical Ophthalmology » Volume 19
Demographic and Socioeconomic Factors, Including Workers’ Compensation, as Predictors of Monocular Blindness After Open Globe Injuries
Authors Chen C ![]() , Malek DA, Greenfield JA
, Malek DA, Greenfield JA ![]() , Yuan Z
, Yuan Z ![]() , Cavuoto KM
, Cavuoto KM
Received 21 March 2025
Accepted for publication 23 June 2025
Published 21 July 2025 Volume 2025:19 Pages 2405—2412
DOI https://doi.org/10.2147/OPTH.S529646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Constance Chen, Davina A Malek, Jason A Greenfield, Zhuochen Yuan, Kara M Cavuoto
Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Kara M Cavuoto, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, 900 NW 17th Street, Miami, FL, 33136, USA, Tel +1 305 326 6324, Fax +1 305 547 3675, Email [email protected]
Objective: To investigate the effect of demographic factors in predicting monocular blindness in patients after open globe injury (OGI) in a large tertiary ophthalmology center.
Methods: A retrospective chart review of patients with OGI. Clinical data collected were visual acuity, presence of globe rupture, perforating injury, and rapid afferent pupillary defect. Demographic factors included race, sex, time to follow-up, and insurance status. Primary outcome is monocular blindness with visual acuity worse than 20/200 at the last follow-up visit. Logistic regression models and univariable and multivariable analysis were performed to examine the effect of demographic characteristics.
Results: Four hundred and forty-three patients (mean age: 48 ± 22.5 years) were included and the majority (348, 78%) were male. Patients of Black race and females were approximately twice as likely to have monocular blindness (OR: 1.9 [1.2– 3.0]; p = 0.005 and OR: 2.0 [1.3– 3.2]; p = 0.003, respectively). Older individuals were more likely (OR: 1.3 [1.2– 1.4]; p < 0.001) to have worse visual outcomes per each decade of life. Patients with workers’ compensation were almost half as likely to have monocular blindness (OR: 0.41 [0.21– 0.79]; p = 0.008), and also had significantly greater number of clinic visits (mean: 15.7 visits) than those without (mean: 11.7 visits, p = 0.02).
Conclusion: Black race, older patients, and females were more likely to experience monocular blindness. Patients with workers’ compensation and being Hispanic or Latino race were associated with decreased risk of monocular blindness. Combined racial and ethnic analyses showed persistent effects of non-Hispanic Blacks experiencing poor outcomes. These findings emphasize the need for a multifactorial approach in evaluating ocular trauma.
Keywords: open globe injury, visual outcome, demographic, insurance, workers’ compensation, ocular trauma score
Introduction
Open globe injury (OGI) is a full-thickness injury to the eyeball due to perforation, foreign body, globe rupture, or trauma.1 OGIs have an incidence of 4.49 per 100,000 population, with expenditures totaling to $793 million in an 8-year span.2 For younger individuals, OGIs are commonly caused by assault, recreational or occupational injuries, while the etiology in older individuals is more commonly falls.2–4
Several demographic features such as race, sex, and age have been shown to influence visual outcome.4 Patients of Black race or Hispanic ethnicity have the highest OGI incidence4,5 with Black race more likely to experience monocular blindness as a result.6 In terms of sex, females are more likely than males to exhibit worse outcomes.4,5 Lastly, older patients were found to have poorer visual outcomes after OGI.6 For these patients already in a more vulnerable position, visual impairment can extend beyond physical disability, impacting psychological, social, and economic well-being.7 Deeper understanding of these demographic influences can improve care for patients with ocular injuries.
The Ocular Trauma Score (OTS) is a widely used prognostic model for estimate visual outcomes in patients with open globe injuries.3,8 The presenting visual acuity (VA) is assigned a raw score, which is then adjusted for ocular comorbidities such as the presence of an afferent pupillary defect, a ruptured globe, perforating injury, endophthalmitis, or retinal detachment.9 Finally, raw scores are stratified from a range of 1 to 5, with a score of 1 representing the worst visual prognosis.9 This risk stratification model effectively incorporates various presenting factors and can guide decision-making for vision preservation strategies.
There is a high prevalence of work-related OGI.7,10,11 Thousands of people are blinded yearly because of work-related injuries,11 yet one factor that remains unexplored in OGI outcomes is the effect of workers’ compensation. The Workers’ Compensation Act, commonly known as workers’ compensation (WC), is an employer-provided insurance that offers financial support for job-related injuries or illnesses. This insurance is distinct from general health insurance, and patients can have one or both types of coverage.12 Previous research has shown that patients with workers’ compensation have more frequent clinical visits compared to those with other insurance types.13 This suggests that financial incentives may lead to increased engagement with health-care providers, enabling closer monitoring of medical conditions and facilitating more timely interventions. In the context of OGI, workers’ compensation coverage may encourage more consistent follow-up, potentially leading to better visual outcomes. However, no prior study has established whether workers’ compensation is independently associated with the risk of monocular blindness after OGI.
This study aims to fill that gap by evaluating the role of workers’ compensation alongside demographic, socioeconomic and clinical risk factors in predicting long term monocular blindness after OGI. By evaluating how these diverse factors contribute to the prediction of monocular blindness in patients who sustain OGI, we can identify high risk populations and guide interventions in follow-up care.
Methods
This was a retrospective study of patients with OGI treated at a single tertiary ophthalmology center from 2018 to 2021. The study was approved under the Institutional Review Board (IRB) at the University of Miami, # 20200719. Patients were identified based on International Classification of Diseases (ICD) or Current Procedural Terminology (CPT) codes (Appendix A). Patients included in the study had at least 3 visits: one initial presentation and two follow-up visits to ensure the observed effects were not transient, with a minimum of 3 months of follow-up. The best corrected visual acuity (BCVA) at each clinical visit was collected and was selected from the following visual acuity measurements: with correction, pinhole, or without correction, in that order. In cases of bilateral OGI, the right eye was selected for analysis due to a high prevalence of right eye dominance.14 BCVA was then transformed to corresponding Logarithm of the Minimum Angle of Resolution (LogMAR) values. Additional data collected included the presence of globe rupture, perforating injury, and relative afferent pupillary defect at presentation. The demographic characteristics recorded were age, sex, race, ethnicity, time to follow-up, and insurance type.
A modified OTS was calculated by assigning a raw score of up to 100 points based on presenting VA. In accordance to the original OTS calculation, points were deducted if globe rupture, perforating injury, or relative afferent pupillary defect were present.9 However, due to incomplete clinical documentation, the modified calculation did not deduct points for presence of concurrent endophthalmitis or retinal detachment, and these factors were excluded to reduce bias. Raw scores were then standardized using z-score distributions and classified into a modified OTS ranging from 1–5. Despite the omissions, the modified OTS has previously been shown to be a strong predictor of poor visual outcome, reinforcing its reliability for analysis.6
The primary outcome measure was the presence of monocular blindness at the last follow-up. It was classified as a binary variable where a VA worse than 20/200 (1.00 LogMAR) was indicative of poor outcome. The 20/200 threshold was chosen because it is considered as the criteria for legal blindness by the Social Security Administration due to the functional limitations,15 and it serves as an internationally accepted benchmark for severe vision impairment.
Univariable logistic regressions was performed to examine the effect of demographic characteristics on the presence of monocular blindness. It was followed by multivariable logistic regression models to analyze statistically significant associations identified in univariable analysis. We conducted an additional sensitivity analysis by grouping race and ethnicity into a single mutually exclusive variable to capture intersectionality and its effect on monocular blindness. Statistical software used was Stata software (version 18, StataCorp LP, College Station, TX). The significance level was established at 0.05 for all statistical calculations.
Results
The patient demographic data are included in Table 1. Of the 443 patients (mean age: 48 ± 22.5 years), the majority (348 patients, 78%) were male. Although females comprised less than a quarter of the patients (98 patients, 22%), they were twice as likely (OR: 2.0 [1.3–3.2]; p = 0.003) than males to have worse visual outcomes at follow-up (Table 2). Patients of Black race represented 27% of this cohort and were almost two times (OR: 1.9 [1.2–3.0]; p = 0.005) more likely to have monocular blindness than White patients. On the contrary, Hispanic patients were half as likely (OR: 0.47 [0.32–0.69]; p < 0.001) to have adverse visual outcomes. When race and ethnicity were grouped together, non-Hispanics Whites were almost twice as likely (OR: 1.8 [1.1–2.8]; p = 0.017) than Hispanic Whites to have worse visual outcomes (Table 3). Furthermore, non-Hispanic Blacks were nearly three times more likely (OR: 2.7 [1.6–4.5]; p < 0.001) than White Hispanics to experience monocular blindness.
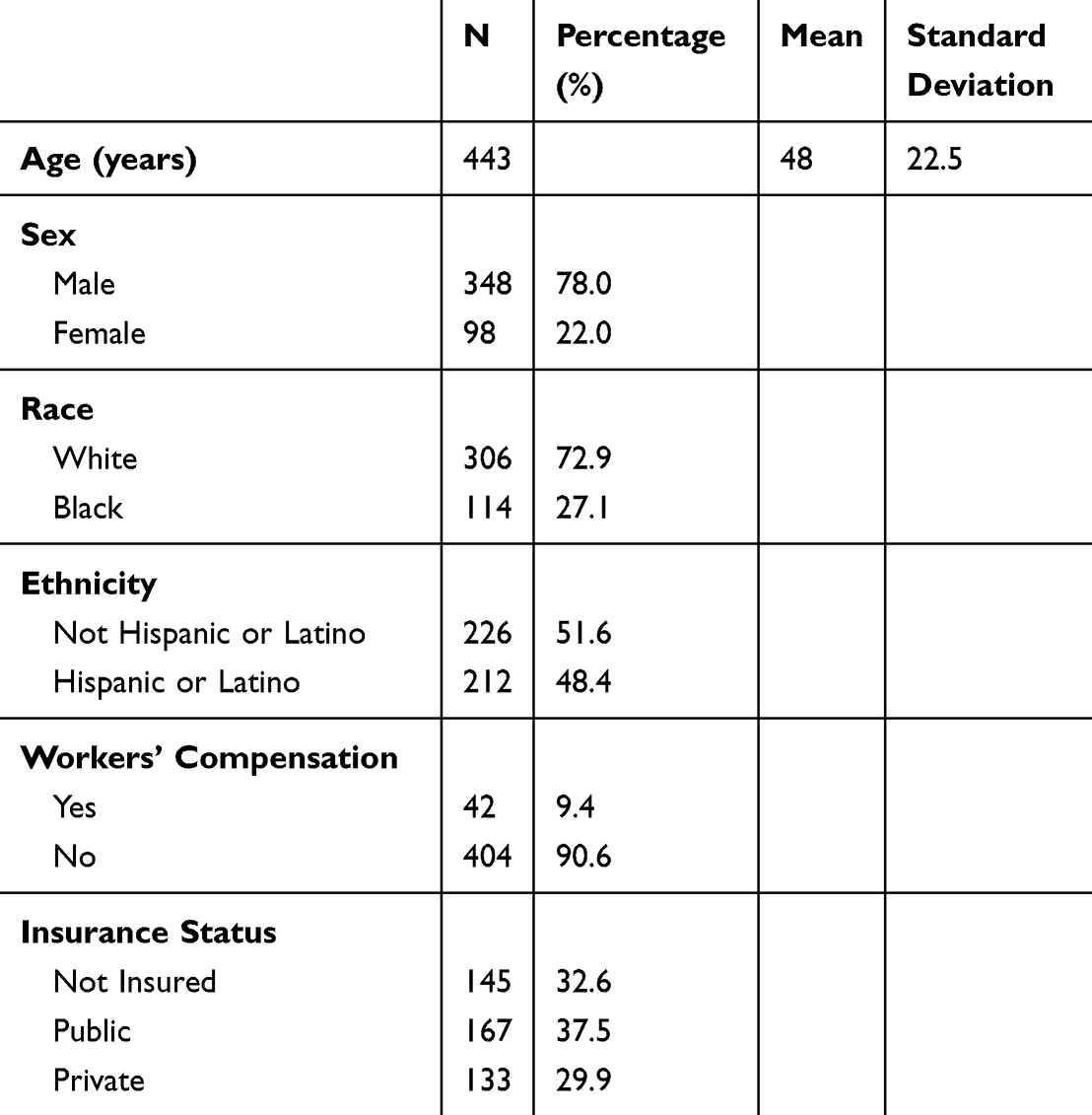 |
Table 1 Patient Demographics |
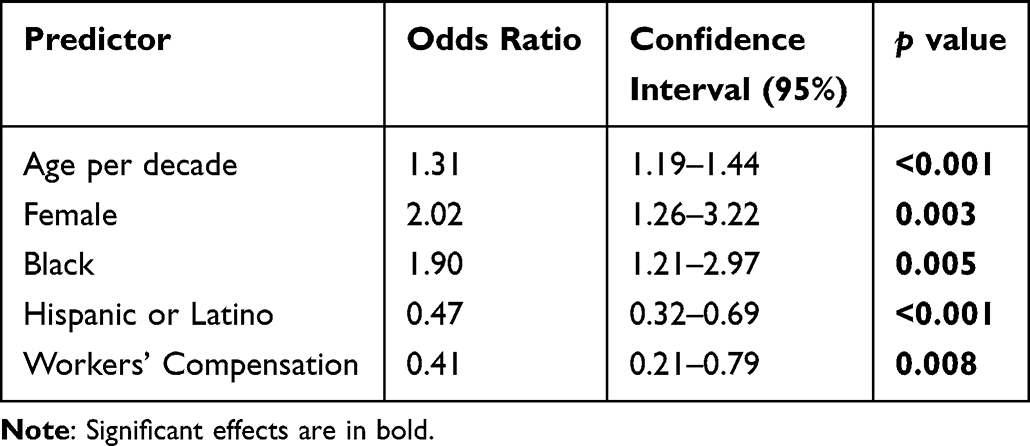 |
Table 2 Logistic Regressions |
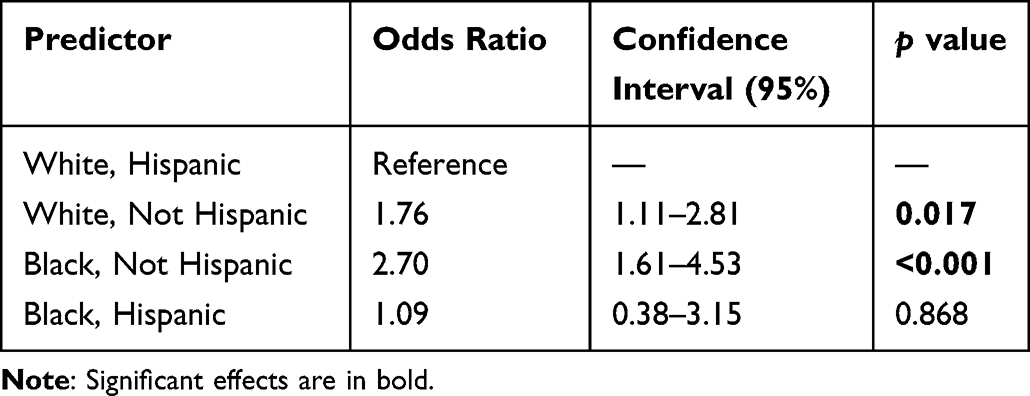 |
Table 3 Race and Ethnicity Groupings |
Older individuals were more likely (OR: 1.3 [1.2–1.4]; p < 0.001) to have worse visual outcomes than younger individuals per each decade of life. The most common cause is due to falls, which was almost three times more likely than other causes (OR: 2.7 [1.04–7.1]; p = 0.041). Workers’ compensation acted as a protective factor, as these patients were almost half as likely to have a poor visual outcome (OR: 0.41 [0.21–0.79]; p = 0.008). Patients with workers’ compensation also had significantly more frequent clinic visits (mean: 15.7 visits) than those without workers’ compensation (11.7, p = 0.02). When comparing other insurance types to workers’ compensation, patients with public insurance (OR: 3.8 [1.8–7.8]; p < 0.001) and private insurance (OR: 2.1 [1.8–7.7]; p < 0.001) had greater risk of experiencing monocular blindness. There was no difference between having no insurance and having workers’ compensation (p > 0.05) (Table 4).
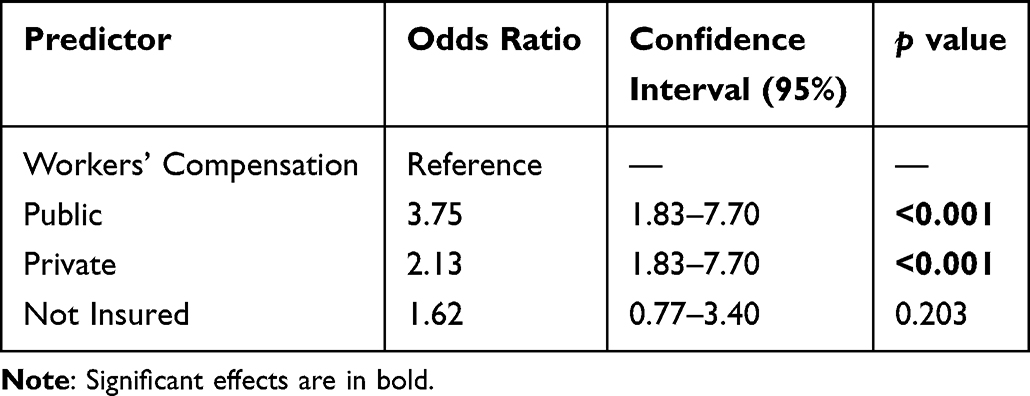 |
Table 4 Insurance Comparison |
Multivariable regression analysis demonstrated a significant association between lower OTS classification and the presence of monocular blindness at last follow-up (OTS class 1 OR: 21 [7.3–63.1]; p < 0.001), indicating that the modified OTS is a reliable prognostic tool for poorer visual outcomes (Table 5). Older age was associated with worse visual outcomes (OR: 1.2 per decade older [1.1–1.4]; p < 0.001), and Black non-Hispanic patients were found to be twice as likely to experience monocular blindness (OR: 2.1 [1.0–4.2]; p = 0.049) as compared to White non-Hispanic patients. No significant effect was observed when sex and age were combined (p = 0.957).
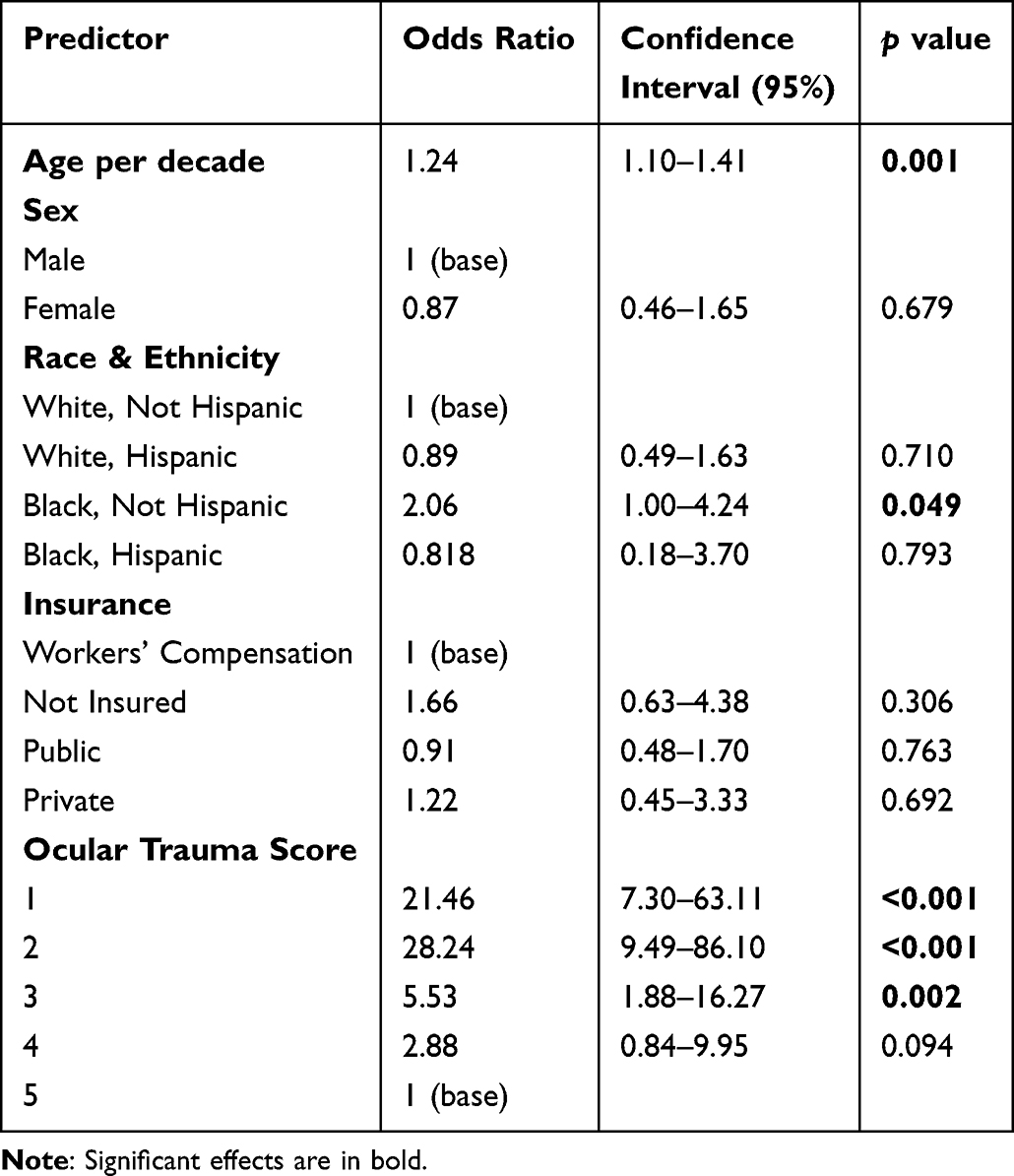 |
Table 5 Multivariable Regressions with Racial and Ethnic Grouping |
Discussion
In this study, we investigated the demographic, clinical, and socioeconomic factors associated with monocular blindness following open-globe injury in patients presenting to a large tertiary ophthalmology center. These findings highlight the multidimensional challenges in predicting visual prognosis at presentation and emphasize the need for a holistic approach to care and risk assessment. Our research has the potential to enhance prognostic models and provide more personalized care for high-risk populations.
Sociodemographic status has been shown to play a significant role in shaping visual outcomes after OGI and may reflect broader social and systemic factors.5 Consistent with previous studies, we found that Black patients faced nearly twice the risk of monocular blindness compared to White patients.4,6 This disparity may be attributed to systemic barriers to care, socioeconomic inequalities, or differences in injury severity.16 Interestingly, we found that the Hispanic patients were half as likely to experience monocular blindness and that the Hispanic race may act as a protective factor. The positive outcomes indicate an extension of the Hispanic paradox in OGI, which is often attributed to strong support from the cultural community.17 Emerging data suggests that acculturation can moderate disease risk by buffering economic and environmental stressors commonly faced by this population.18 This group has also been found to have lower rates of anxiety and better mental health overall.19 Given that OGIs are generally traumatic experiences, the social support and resilient mindset associated with this community may be critical in the recovery process.
We further compared visual outcomes across groups by analyzing race and ethnicity together. As expected, White Hispanic patients exhibited the best visual outcomes, which may reflect a combined protective effect of both White racial and Hispanic ethnic backgrounds. In contrast, non-Hispanic White and non-Hispanics Black patients demonstrated significantly higher risk of poor visual outcomes. This is notable because White race is generally considered protective when analyzed alone, yet it exhibited similar outcomes to patients Black race when ethnicity was incorporated. These results suggest that the Hispanic ethnicity may offer an even stronger influence than previously recognized. Interestingly, Hispanic Black patients, who often have a sociodemographic profiles similar to non-Hispanic Blacks,20 did not experience the same level of adverse outcome in our study. This finding may further support the idea that Hispanic ethnicity provides some protection in the setting of ocular trauma. Recommendation for future studies would be to investigate race and ethnicity as a combined group to better understand these effects.
Age and sex were also strongly associated with visual outcomes.5 We found that older individuals and female sex were associated with worse visual outcomes, which have been previously demonstrated in literature.4–6 In patients over 65 years of age, the most common cause of injury was due to falls, consistent with prior studies.2–4,21 The result is further corroborated by the data presented in Table 4 comparing the various insurance types, as individuals with Medicare (for those aged 65 and older) exhibited a significantly higher risk of monocular blindness. For females, falls were also the most common cause of injury, with the majority occurring in the home. Research indicates that females are 1.5 times more likely to experience falls as compared to males,21 and this risk increases with age.22 We also hypothesize that intimate partner violence (IPV) among women, which predominantly takes place in domestic settings, could be another potential contributing factor. Approximately 30.6% of females experience IPV23 and nearly 45% of these encounters involve ocular trauma, including OGI.24 Based on these findings, female patients presenting with OGI should be screened for IPV during their treatment, as IPV may indirectly contribute to the poor visual outcomes observed in this group.
Patients with workers’ compensation had significantly better visual outcomes following OGI.4 This result contrasts with findings from patients with orthopedic or spinal conditions who have reported worse health outcomes and greater dissatisfaction with care.13,25 The negative outcomes have been attributed to difficulty navigating the compensation system, which can lead to mental stress and physical harm.26 In our patient sample, one possible explanation for the positive findings is that patients with workers’ compensation had significantly more frequent clinical visits as compared to other insurance types. Increased clinical visits have been previously associated with decreased rates of mortality following an Emergency Department discharge.27 While physicians dictate the level of follow-up care, financial barriers may limit patient adherence. Workers’ compensation may reduce this burden by providing more comprehensive financial support, including wage replacement, which may encourage patients to comply with follow-up care without financial strain.28 In addition, given the nature of vision-threatening injuries, patients may also receive greater social work support in claiming compensation, as societal support is more robust in promoting independence for those with visual disability as compared to physical.29 The protective effects of WC is especially notable when compared to the other health insurance statuses, as both public and private insurance were associated with higher odds of monocular blindness. However, no difference was observed for the uninsured group. While seemingly counterintuitive, it could reflect our sampling criteria requiring at least 3 visits for inclusion. Patients without insurance who completed at least 3 visits likely represented a healthier and more motivated subgroup, which would explain the observed relationship.
When sociodemographic variables and ocular trauma severity were analyzed together, age, non-Hispanic Blacks and OTS remained predictive of visual outcomes. The age-related outcomes can be attributed to an increased risk of falls and subsequent injury in older individuals. The OTS reflects that recovery prognosis is largely dependent on the severity of the initial presenting symptoms. However, the borderline significance of race and ethnicity presented an interpretation challenge because these results suggest a possible interaction between demographic and socioeconomic risk factors, which may confound each other. This finding underscores the importance of considering intersectionality, rather than analyzing them as entirely independent variables. Our results emphasize the importance of considering latent interactions and highlight the need for a multifactorial approach in evaluating ocular trauma. Such an approach would allow a more accurate understanding of how sociodemographic and clinical variables influence visual prognosis.
Several limitations should be noted. This was a retrospective study conducted at a single site, which may introduce biases and limit the generalizability of the results. In addition, patients were required to have a minimum number of follow-up visits and a specified follow-up duration, which may have introduced selection bias by excluding those with rapidly deteriorating or markedly improving injuries. Given the lack of pre-injury ophthalmic records for most patients, we assumed that visual function prior to trauma was normal and that the unaffected eye reflects the patient’s baseline visual potential. Our study also used a modified OTS that excluded endophthalmitis and retinal detachment, which were part of the original criteria and can affect the predictive power of the scoring system. Finally, the data in this study were recorded from electronic health records and patient-reported information, which may introduce potential biases. Variations in treatment of care were not systematically documented, which could influence the visual outcomes.
Conclusion
In this study from Miami, Florida, we explored the effect of various sociodemographic factors on monocular blindness after OGI. We found that Black race, advanced age, and females were more likely to experience monocular blindness. Workers’ compensation and Hispanic ethnicity, however, appeared to serve as protective factors. Combined analyses highlighted the complex interplay between demographic, socioeconomic, and clinical risk factors in predicting visual outcomes. These interactions may not be immediately apparent and could contribute to disparities in recovery and prognosis following OGI. These findings emphasize the importance of a holistic evaluations at the time of OGI presentation, including detailed stratification of insurance status with specific attention to workers’ compensation coverage. Additionally, future studies should incorporate interpersonal violence assessments to better understand its potential impact on visual outcomes. Additional research is needed to understand the underlying mechanisms driving disparities in recovery with the goal of identifying and mitigating the factors contributing to worse outcomes among high-risk populations.
Institutional Review Board Statement
This study received Institutional Review Board approval from the University of Miami, #20200719. Patient consent was not required due to the retrospective nature of the review, and the data was maintained with confidentiality. The study adhered to the tenets of the Declaration of Helsinki.
Funding
NIH Center Core Grant P30EY014801 (Institution, KC).
Disclosure
All authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
1. Mayer CS, Reznicek L, Baur ID, Khoramnia R. Open globe injuries: classifications and prognostic factors for functional outcome. Diagnostics. 2021;11(10):1851. doi:10.3390/diagnostics11101851
2. Mir TA, Canner JK, Zafar S, Srikumaran D, Friedman DS, Woreta FA. Characteristics of open globe injuries in the United States from 2006 to 2014. JAMA Ophthalmol. 2020;138(3):268–275. doi:10.1001/jamaophthalmol.2019.5823
3. Zhou Y, DiSclafani M, Jeang L, Shah AA. Open Globe Injuries: review of evaluation, management, and surgical pearls. Clin Ophthalmol. 2022;16:2545–2559. doi:10.2147/OPTH.S372011
4. Ojuok E, Uppuluri A, Langer PD, Zarbin MA, Thangamathesvaran L, Bhagat N. Demographic trends of open globe injuries in a large inpatient sample. Eye. 2021;35(8):2270–2276. doi:10.1038/s41433-020-01249-4
5. Tomaiuolo M, Woreta F, Li A, et al. Open Globe Repairs in the United States 2014–2018: incidence, risk factors and visual outcomes - an IRIS® registry (intelligent research in sight) analysis. Invest Ophthalmol Visual Sci. 2022;63(7):4249.
6. Greenfield JA, Malek DA, Anant S, et al. A multi-center analysis of visual outcomes following open globe injury. Sci Rep. 2024;14(1):16638. doi:10.1038/s41598-024-67564-y
7. Schulz M, Bonnell AC, Chee YE, Feng S, Chen PP, Bojikian KD. Associations between socioeconomic status and open globe injury. Eye. 2024;39:986–991. doi:10.1038/s41433-024-03537-9
8. Shah MA, Shah SM, Applewar A, Patel C, Shah S, Patel U. OcularTrauma Score: a useful predictor of visual outcome at six weeks in patients with traumatic cataract. Ophthalmology. 2012;119(7):1336–1341. doi:10.1016/j.ophtha.2012.01.020
9. Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmol Clin North Am. 2002;15(2):163–5,vi. doi:10.1016/s0896-1549(02)00007-x
10. Patel A, Berkowitz S, Sridhar J, Durrani A, Patel S. Trends in Workplace-Related Eye Injuries in the United States From 2011 Through 2020. J Vitreoretin Dis. 2023;7(1):49–56. doi:10.1177/24741264221117418
11. El-Hadidy SS, Hashish AM. Proportion of occupational eye injuries and their risk factors: a single-center study. Egypt J Occup Med. 2024;48:91–105. doi:10.21608/ejom.2024.271473.1327
12. Himmelstein J, Buchanan JL, Dembe AE, Stevens B. Health services research in workers’ compensation medical care: policy issues and research opportunities. Health Serv Res. 1999;34(1 Pt 2):427–437.
13. Compton J, Glass N, Fowler T. The effect of workers’ compensation status on the patient experience. Open Access. 2019;4(2):e0003. doi:10.2106/JBJS.OA.19.00003
14. Lopes-Ferreira D, Neves H, Queiros A, Faria-Ribeiro M, Peixoto-de-matos SC, Gonzalez-Meijome JM. Ocular dominance and visual function testing. Biomed Res Int. 2013;2013:238943. doi:10.1155/2013/238943
15. Lee SY, Gurnani B, Mesfin FB. Blindness. StatPearls. 2025.
16. DeAngelis RT, Hargrove TW, Hummer RA. Skin tone and the health returns to higher status. Demography. 2022;59(5):1791–1819. doi:10.1215/00703370-10191675
17. Castaneda E, Smith B, Vetter E. Hispanic health disparities and housing: comparing measured and self-reported health metrics among housed and homeless Latin individuals. J Migr Health. 2020;1–2:100008. doi:10.1016/j.jmh.2020.100008
18. Ruiz JM, Steffen P, Smith TB. Hispanic mortality paradox: a systematic review and meta-analysis of the longitudinal literature. Am J Public Health. 2013;103(3):e52–60. doi:10.2105/AJPH.2012.301103
19. Teruya SA, Bazargan-Hejazi S. The immigrant and Hispanic paradoxes: a systematic review of their predictions and effects. Hisp J Behav Sci. 2013;35(4):486–509. doi:10.1177/0739986313499004
20. Cuevas AG, Dawson BA, Williams DR. Race and skin color in Latino health: an analytic review. Am J Public Health. 2016;106(12):2131–2136. doi:10.2105/AJPH.2016.303452
21. Li Y, Hou L, Zhao H, Xie R, Yi Y, Ding X. Risk factors for falls among community-dwelling older adults: a systematic review and meta-analysis. Front Med. 2022;9:1019094. doi:10.3389/fmed.2022.1019094
22. Jin J. Prevention of falls in older adults. JAMA. 2024;332(1):84. doi:10.1001/jama.2024.9713
23. Slentz DH, Joseph AW, Joseph SS. Intimate partner violence-related oculofacial injuries during the COVID-19 pandemic. JAMA Ophthalmol. 2021;139(7):789–790. doi:10.1001/jamaophthalmol.2021.1543
24. Baldwin G, Miller JB. Ocular injuries and intimate partner violence: a review of the literature. Clin Ophthalmol. 2025;19:119–127. doi:10.2147/OPTH.S489585
25. Russo F, De Salvatore S, Ambrosio L, et al. Does workers’ compensation status affect outcomes after lumbar spine surgery? A systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(11):6165. doi:10.3390/ijerph18116165
26. Wadhwa S, Taouk Y, Spittal MJ, King T. Workplace injury compensation and mental health and self-harm outcomes: a systematic review. New Solut. 2024;34(2):71–82. doi:10.1177/10482911241254836
27. Lin MP, Burke RC, Orav EJ, Friend TH, Burke LG. Ambulatory follow-up and outcomes among medicare beneficiaries after emergency department discharge. JAMA Netw Open. 2020;3(10):e2019878. doi:10.1001/jamanetworkopen.2020.19878
28. Robertson J, Corro D. Workers compensation vs group health: a comparison of utilization. Available from: https://www.ncci.com/Articles/Pages/II_Research-wc-vs-group-health.pdf.
29. Cimarolli VW, Wang SW. Differences in social support among employed and unemployed adults who are visually impaired. J Vision Impairment Blindness. 2006;100. doi:10.1177/0145482X0610000906
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.