")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Demand of and Access to Health Messages Through Mass Media in the Rural Community of Eastern Ethiopia: A Mixed Method Study
Authors Aliyi B, Dassie Y, Deressa A , Debella A , Birhanu A , Gamachu M , Eyeberu A , Mamo Ayana G , Fekredin H , Mussa I
Received 10 July 2023
Accepted for publication 8 September 2023
Published 13 September 2023 Volume 2023:16 Pages 1859—1874
DOI https://doi.org/10.2147/RMHP.S429712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Bushra Aliyi,1 Yadeta Dassie,2 Alemayehu Deressa,2 Adera Debella,3 Abdi Birhanu,4 Mulugeta Gamachu,4,5 Addis Eyeberu,3 Gelana Mamo Ayana,2 Hamdi Fekredin,2 Ibsa Mussa2
1Zonal Health Office, Eastern Hararghe, Oromia, Ethiopia; 2School of Public Health, CHMS, Haramaya University, Harar, Ethiopia; 3School of Nursing and Midwifery, CHMS, Haramaya University, Harar, Ethiopia; 4School of Medicine, CHMS, Haramaya University, Harar, Ethiopia; 5Departments of Public Health, Rift Valley University, Harar, Ethiopia
Correspondence: Alemayehu Deressa, School of Public Health, CHMS, Haramaya University, PO Box 235, Harar, Ethiopia, Tel +251917841709, Fax +251256668081, Email [email protected]
Background: The demand for health-related information has increased dramatically in recent years. Media is crucial in reaching health messages to audiences, especially those who are distant and rural. Therefore, the study aimed to assess demands, access, and factors associated with access to health messages through mass media in the rural community of Kersa District of East Hararghe, Eastern Ethiopia.
Methods: A mixed-methods study was conducted from October 15 to November 20, 2020. A quantitative cross-sectional and a qualitative phenomenological study design were applied. A total of 578 participants were included by using a systematic sampling technique. Collected data were entered into Epidata version 3.1 and analyzed using SPSS version 22.0. A multivariate logistic regression analysis model was used and reported using an adjusted odds ratio (AOR) with a 95% confidence interval (CI). Statistical significance was set at p < 0.05. For qualitative, six-focused group discussions (FGDs) were used and then analyzed thematically.
Results: Overall, the demand of and access to health messages through mass media was 32.5% (95% CI=28.5– 34.2%) and 26.6% (95% CI=24.6– 28.7%), respectively. Factors such as having electric services (AOR=2.36, 95% CI=2.13– 5.41), having a mobile phone (AOR=4.56, 95% CI=4.32– 8.73), exposure to TV (AOR=4.73, 95% CI=1.03– 11.62), and exposure to social media and printed media (AOR=5.24, 95% CI=1.07– 15.63), a preference for programs such as news, current affairs, entertainment, health and educational were 2.37, 9.47, 4.75 and 7.55 times more likely to access health messages (AOR=2.37, 95% CI=1.00– 5.61; AOR=9.47, 95% CI=3.54– 25.34; AOR=4.75, 95% CI=1.23– 18.38; and AOR=7.55, 95% CI=3.12– 8.66, respectively). Qualitative findings, participants demand for health messages from health workers, radio, and the main source for accessing the message was the radio.
Conclusion: Approximately one in every three and one in every four rural communities in the study area had demand, and access to health messages through mass media, respectively. As a result, all stakeholders should emphasize and strengthen expanding methods of reaching health messages using mass media.
Keywords: health message, media, access, rural community, Eastern Ethiopia
Introduction
Health communication is an approach to communicating information with the purpose of improving health outcomes by encouraging behavioral modification and societal change along a spectrum of knowledge, beliefs, attitudes, and actions.1–3 Health communication strategies that use mass media (television, print, and the Internet) have been linked to health attitudes and behaviors.4,5 Health promotion is a process that allows for greater control over the determinant of health status.6,7 According to the health-promotion approach, health communication is both an art and a technology for informing, influencing, and motivating people, institutions, and the general public about important health concerns. It strives to enhance behavior by maintaining the continuity of information, faith, and attitude with conduct and to promote health in the long run by supporting societal reforms.4,8
The demand for health communication and information services has grown exponentially in recent years.9,10 The media are an important part of any public health situation.11,12 Local and international media play a vital role as links between health workers and the larger public.13 Health workers educate and entrust critical health information to the media, which is subsequently communicated to the public in easily accessible formats through media outlets.14,15 The media assists health professionals in broadening their audience reach, which is critical given that face-to-face communication methods sometimes take too many human resources and reach only a limited number of individuals in large, underserved rural areas.6,13
Health message can be transmitted through verbal and written strategies to influence and empower individuals, populations, and communities to make healthier choices and to promote positive changes in knowledge, attitudes, and behaviors.16,17 To bring this change, most of the time, the health education professionals develop materials such as brochures, billboards, newspaper articles, television and radio broadcasts, public service announcements, newsletters, pamphlets, awareness creating videos, digital tools, case studies, group discussions, health fairs, and field trips as a media outlet.2,18 Such like media serves as a bridge between rural population and health educators during critical health information dissemination.19,20 There are different types of mass medias that can be used to reach out rural communities, particularly mobile, radio and television, play a pivotal role for persuading target audiences to adopt new habits, bring a health behavior, and to remind individuals about important health topics.21,22 Moreover, they can not only notify the public about new health ailments and where to receive health care but also, these medias are helpful to keep the public up to date about health issues, especially during pandemic and other health and health-related disasters.3,6,23,24
For several years, health professionals have recognized the increasing necessity of incorporating mass media methods into their health promotion practices.25 The ever-changing technological environment and increased reliance on mass communication have strengthened the prominence of mass media.26 The immense potential of mass media resources to reach specific audiences and affect health-related habits has long been recognized.27–29 Despite these facts, it is said that the health profession has been slow to recognize, accommodate, and accept such practices. As a result, incorporating health-related mass media activities within a health-promotional role remains elusive.7,25,30,31
Different studies showed individuals are currently dependent on mass media, that of an appropriate way and have an enormous advantage in reaching health topics for targeted audiences.11,13,32 Media demand and accessed of health message can be determined by the level of education, residents, wealth index, trustfulness of the source of health, and marital status.33–35 Social media is altering how people obtain information and interact with others.36 Public health professionals may utilize social media to analyze health needs, develop policies, and convey health problems as they work to safeguard and improve the health of the community. Traditional health message efforts are projected to reach < 10% of the target population.7,37
According to the findings of the 2016 EDHS, the level of exposure to mainstream media in Ethiopia is low. Radio was the most accessible type of medium for both men and women (17% and 29%, respectively), followed by television (16% and 21%, respectively). Because of the low literacy rate, men (9%) and women (4%) read the printed materials. The majority of respondents (74% women and 62% men) had no access to any of the three media platforms at least once a week. However, women and men’s media exposure has shifted since 2011. For example, the proportion of women who listened to the radio at least once a week decreased from 22% to 17%. The proportion of men decreased from 38% to 32%.38
Despite the commitment of the government and various stakeholders, access to health messages in rural communities has been hampered by several factors. Moreover, as far as the knowledge of investigators is concerned, there is a paucity of documented evidence and information regarding demands, access, and associated factors at the country level, particularly in the study area using both quantitative and qualitative data. Thus, this study aimed to assess the demand, access, and associated factors among rural communities in the rural areas of Kersa District of East Hararghe, Eastern Ethiopia through mixed study design.
Methods and Materials
Study Design, Area, and Period
A mixed-method study design, such as a quantitative cross-sectional study design and qualitative phenomenology, was carried out from October 15 to November 20, 2020, among rural households in Kersa District of East Hararghe, Eastern Ethiopia. The district is situated in eastern Ethiopia, 483 km from Addis Ababa, a country’s capital city. Dega (18%), Weynadega (77%), and Kola (5%) were the three climatic zones in Kersa District, which consisted of 35 rural and three urban kebeles (the lowest administrative system). Thirty-seven health posts and seven health centers serve the district’s estimated 243,170 population, and 11 of the 35 rural kebeles, which account for approximately 18% of the total population, have access to electricity. Additionally, the district’s TV transmission services depend on satellite dishes and network coverage, and every kebele has access to these services, with the exception of a few outlying kebele districts. There were 106 public schools, five private schools, two preparatory schools, three high schools, with the remaining being primary schools.
Study Participants and Eligibility Criteria
All rural households in Kersa District were the source population, whereas randomly selected rural household members who were present at home throughout the data collection period were the study population. The study included a sample of households with individuals ranging in age from 13 to 70 years; however, household members with vision, hearing, or other developmental problems were excluded.
Sample Size Determination
The quantitative sample size was determined based on the specific objectives of access to media from a relevant study that was conducted on the impact of mass media on the improvement of women’s reproductive health in Ethiopia, considering 37% of rural women had frequent access to radio, TV, and magazines/newspapers.39 Therefore, using the single population formula,  , at a 95% CI, d=0.04, p=0.37 =3.84139 (0.37×0.63)/(0.04)2, n=560. Using a 5% non-response rate, the final sample size was 588. The final sample size was calculated after calculating each media demand and access-associated factor, all of which were less than the final sample size.
, at a 95% CI, d=0.04, p=0.37 =3.84139 (0.37×0.63)/(0.04)2, n=560. Using a 5% non-response rate, the final sample size was 588. The final sample size was calculated after calculating each media demand and access-associated factor, all of which were less than the final sample size.
For qualitative data, six Focus Group Discussions (FGDs) with ten participants from different groups (community leader, religious leader, respective kebele administrators, and female developmental army leaders) were conducted based on information saturation. The information saturation and diversity of ideas among the subgroups were therefore taken into consideration when determining the sample size.
Sampling Procedures, Data Collections Methods, and Procedures
For quantitative analysis, there were 35 kebeles in Kersa District, and six kebeles were randomly selected to include the total number of households in each kebele. Based on the list of household heads who registered for long-lasting impregnated net (LLIN) distribution in 2019, a total of households in each kebele was listed, depending on their LLIN registration order. Proportional allocation was then used, depending on the total number of households in each kebele. Finally, systematic random sampling was used to divide the total number of households by the sample size to determine the interval and the nth household head serial number and list all the names of the households in the nth interval; 588 samples were distributed for the six kebeles: Sodu (146), Adele (121), Wichiro (102), Dolu Salama (89), Burka water (69), and Gale mirga (61), listed and distributed for the data collectors (Figure 1). The data was collected using a validated interview-administered semi-structured questionnaire adapted from different related literatures. The customized questionnaires were adjusted and contextualized to match the local circumstances and study objectives, and the interviewer-administered questionnaires were used for the study. Data were collected by trained health extension workers and supervised by a BSc nurse. Data completeness and consistency were also assessed.
 |
Figure 1 Diagrammatic presentation of the sampling procedures of demand and access to health messages through mass media among the rural community in Kersa District, Eastern Ethiopia, in 2020. |
Purposive sampling was used for the qualitative study, considering maximal variability with the assumptions of getting “rich” information. Data were collected by public health professionals using the FGD interview guide. To gather the data, interview instructions created after reviewing several pieces of evidence were used. Data were collected using a tape recorder and notes were recorded. Additionally, field notes were taken that covered situations, behaviors, difficulties, decisions made in the field, and reflections on daily tasks with the supervisor.
Data Quality Control and Assurance
Before receiving the completed questionnaire from each data collector, the investigators and supervisors provided a thorough review of clarity, accuracy, and consistency. Prior to actual data collection, pretesting was carried out outside the study area with 5% of the respondents. The questionnaires were cleaned and categorized appropriately during data collection.
Focused group discussions (FGD) were audio-recorded to ensure qualitative data quality. The Focus group discussion facilitation guide was developed in line with the objective of the study. The discussion was conducted by an experienced and trained facilitator. The facilitator and note-takers documented impressions from each discussion session. The information generated from all focus group discussion was recorded in a notebook as well as on a memory card, then recorded information was transcribed verbatim and translated to English language by language expert. The FGD member reviewed the interviews data by summarizing the key points and checking the originality of their discussions. Debriefing and discussion sessions each day during the entire fieldwork were conducted to encourage and deal with any emerging issues for the consecutive discussion. Finally, in order to ensure that the interpretation of the finding made sense, debriefing and member checking were conducted.
Data Processing and Analysis
Quantitative data were checked for completeness and consistency by cross-checking, entered into Epi Data version 3.1, and exported to SPSS version 22.0. Descriptive statistics, such as mean and standard deviation, were calculated and presented using frequency tables, figures, and graphs. Binary logistic regression analysis was performed to identify the factors associated with access to the health message. Variables with a p-value less than 0.25 in the bi-variable logistic regression were considered for the multivariable binary logistic regression analysis to control for possible confounding factors. In the final multivariable binary logistic regression, the odds ratio, along with the 95% confidence interval, was used to present the association between the explanatory and outcome variables at a p-value of less than 0.05. The goodness of model fit was checked using the Hosmer-Lemeshow statistic. Multi-collinearity tests were carried out to determine the correlation between independent variables and checked using standard error and collinearity statistics (variance inflation factors >10 and standard error >2), which were considered suggestive of Multi Collinearity.
To obtain qualitative data, audio records and field notes were transcribed in Afaan Oromo and translated into English. Atlas software version 7.1.4 was used to analyze the translate documents. Coding and related codes were grouped (into a single family). Once more, related families were grouped into a superfamily, which ultimately formed themes using both inductive reasoning and specified study concepts and objectives. In addition, extracts from the participants’ statements that best illustrated important concepts were used directly throughout the analysis and interpretation. Finally, the thematically analyzed findings from the qualitative data were triangulated with the quantitative results and discussion.
Results
Socio Economic and Demographic Characteristics
A total of 578 study participants age 14 to 73 years were involved, yielding a response rate of 98.3%. The mean age of the study participants was 36 (SD=±6.3). Nearly a quarter of the study participants (140; 24.2%) were aged 32–37 years. The majority of the study participants were male (374; 64.7%), 272 (47.1%) were unable to read and write, and 171 (29.7%) were housewives by occupation. The majority of the participant’s (501; 86.67%) belonged to the Oromo ethnic group, and 453 (78.56%) were Muslims. The majority of the study participants (504; 87.21%) were in the middle-wealth quintile (Table 1).
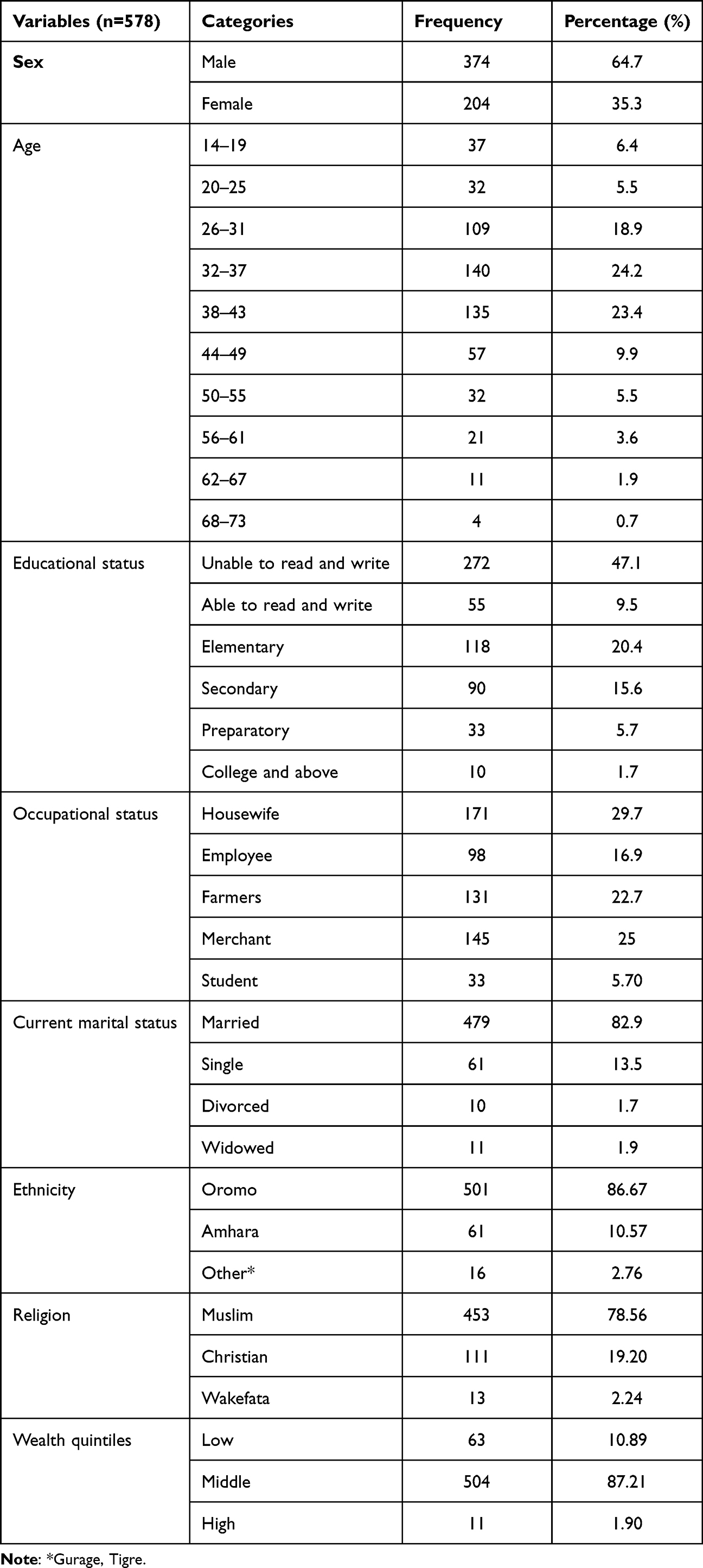 |
Table 1 Sociodemographic Characteristics of the Participants with Access to Health Messages Through Mass Media in the Rural Community of Kersa District, Eastern Ethiopia, 2020 |
Distribution of Media Across Sex of the Study Participants
As shown in Figure 2, of the total study participants, 332 (88.8%) were exposed to media, whereas 116 (56.8%) females had media exposure (Figure 2).
 |
Figure 2 The distribution of media exposure across the sexes of the study participants (n=578). |
Mass Media-Related Factors
According to this study, out of the total 578 study participants, 376 (65%) of the respondents had access to electric services. Nearly four out of five (79.58%) owned media devices, half of whom owned a radio (50.86%). In terms of media exposure, 448 (77.50%) participants were exposed to media, and the majority of study participants were exposed to radio. A total of 214 (37%) respondents replied that they preferred news programs. Regarding the timing and frequency of access to health messages, almost one-fifth of the study participants (19.20%) were advised to access the health message at night, and (20.04%) tended to access it each month (Table 2).
 |
Table 2 Media-Related Feature of the Participants with Access to Health Messages Through Mass Media in the Rural Community of Kersa District, Eastern Ethiopia, 2020 |
Demand and Access of Health Message
According to this study, the overall demand for health messages through mass media of the study population was 188 (32.5%) and access to health messages through mass media was 154 (26.6%) (Figure 3).
 |
Figure 3 Access of health messages through mass media among the rural community in Kersa District, Eastern Ethiopia, in 2020. |
Qualitative Findings
Six FGDs were conducted, and the demand for and access to health message theme concepts emerged as follows:
Demand for Health Messages
As they responded, there are two main sources of health information: health extension workers/ health professionals, and radio. These two sources were preferred differently, most of the elders and women responded to health extension workers or health professionals as their source of health information and youths responded to radio as their source of health information. This means it does not mean no one of the elders or women were not had a piece of information from the radio or from both sources.
Participants require information depending on their circumstances and conditions, according to the discussant of FGD regarding the demand for health information, a 43-year man said the following:
Despite slight differences on the issue of health among the groups they were interested to know about, communicable diseases like COVID-19, malaria, and the causes of under-five deaths, and services like reproductive health.
Participants need the health message as peer the program type, and credible sources of information, Similarly, one of the focus group discussants said:
I have got information about the cause of under-five death from Fana FM radio frequently and similarly from the health professional who came from Haramaya University to implement the CHAMPS program.
Participants require health messages from health extension workers who make house and house visit and focused on child health, this was strengthened and supported by other discussants:
We have got health messages from the health extension workers, during their home visits and health service delivery program like vaccination, nutritional screening, and community meetings. [Woman, aged 44]
I have trained on the issue of the CHAMPS to know the cause of under-five death, so I follow the program regarding the issue transmitted through Fana FM regularly. We have got health information from a radio program that has been transmitted from Haramaya University community radio. [Man, aged 42]
According to the participants, the motivation or purpose for demanding information is to widen their desired knowledge on many issues, because they perceptive information is critical for individuals to know and grasp about a variety of topics, one of the focused group discussants, a 38-year dweller of Kersa district reported that:
I need information most of the time and I have tried my best to know about current events of all from local to global issues based on the level of my understanding.
Another person said that:
Most of us need information on different issues such as health, agriculture, and security as to me and most women need information about legal issues and justice.
Regarding the reason for the need for information, participants considered individuals require messages to overcome their living situation, and particularly young groups, require information to make decision about their future life, one of the leaders of the community stated that:
Information is very important for human beings to overcome the living condition, whereas most of us especially youth groups need information to decide about our future live so decisions could be based on information and knowledge.
In a similar vein, one of the local religious leaders added that:
As our livelihood is based on agriculture, we need information on agricultural knowledge and agricultural inputs.
Most participants need message from radio, phone and peer communication, this was strengthened by a 59-year-old head of community leader:
Most of us follow the radio to get information as we have mentioned about security on daily events, we share information and ask each other about the issue we want to know about, especially news and current affairs. Someone of us gets information through the phone to call somebody who knows about the information we want to know, the information about the market issue especially Chat, we have got through the phone.
Access to Mass Media
Most people owned and used radios, and because there was insufficient access to electricity, few people could watch TV. Young people can use and run social media, especially Facebook. The majority of family radio access depends on males returning home at night with radio after working primarily in agricultural fields. Therefore, this is implied that access to health information on a variety of health topics may occur accidentally rather than on purpose.
Regarding access to mass media, most of participants had access to and owned radios, but shortage of energy was a problem to access to television, Social media was the most accessed for youths, one of the focused group discussants reported that:
Most of us accessed and owned the radio, but access to TV has limited due to electric service even in the same kebele. Social media is accessible to used and operated by the youths but the information from social media especially face book has been disseminated to most of the rural community whether it is rumor or tangible. As a result, quantitative printing media was not demanded as a source of any type of concerned issues.
Radio is the most commonly accessed media by males, while females access it when men return home for relaxation and chewing chat after working hours.
The mass media we have access to is radio, most of the time the male take a radio with them to the place where they have worked mostly in agricultural fields, and came back home at night, so our exposure to radio and health messages through radio if disseminated at the time. It depends on the came back condition of the male at home sometimes they are late due to the ceremony coming together at one place called “shikifi” meaning take rest and chewing chat after working time. [Woman, aged 41]
Participants accessed and gathered health information on a variety of topics through coincidence rather than intent, this is supported by Woman, aged 40.
We have got health information on different issue by chance not deliberately, for example, there is a TV show on OBN which call hello doctor as I am watching this show and somebody came to the place where I am watching the TV and change the channel to other show or program I could never respond to the person who changed the channel, rather simply I continue to with the opened channel. This is the same is true for all of us.
Access of Health Message Through Media and Its Associated Factors
In the bivariate analysis, predictor variables such as having access to electric services; being the owner of media devices; type of device owned; exposure to Radio, TV, social media, and printing media; and those who preferred media programs such as news, current affairs, health, and education were significantly associated with access to health messages.
However, in the final model of the multivariable logistic regression analysis, predictor variables such as having access to electric services; having a mobile phone; type of device owned; exposure to TV, social media, and printing media; and those who preferred media programs such as news, current affairs, health, and education were significantly associated with access to health messages.
Accordingly, respondents who had electric services were 2.36 times more likely to access health messages than their counterparts (AOR=2.36, 95% CI=2.13–5.41). Similarly, study participants who had a mobile phone were 4.56 times more likely to access health messages than their counterparts (AOR=4.56, 95% CI=4.32–8.73).
Moreover, those study participants who had exposure of TV and social media and printing media were 4.73 and 5.24 times more likely to access health messages than those who had exposure to radio (AOR=4.73, 95% CI=1.03–11.62; and AOR=5.24, 95% CI=1.07–15.63, respectively).
Likewise, those study participants who had a preference for programs such as news, current affairs, entertainment, health and educational were 2.37, 9.47, 4.75 and 7.55 times more likely to access health messages as compared to their counterparts (AOR=2.37, 95% CI=1.00–5.61) and (AOR=9.47, 95% CI=3.54–25.34; AOR=4.75, 95% CI=1.23–18.38; and AOR=7.55, 95% CI=3.12–8.66, respectively).
Furthermore, the odds of accessed to health messages were 79% less likely among rural community who preferred to attend the media on weekend time than those who preferred to attend the media in the special program (AOR=0.21, 95% CI=0.06–0.72) (Table 3).
 |
Table 3 Bi-Variable and Multivariable Logistic Regression Analysis of Factors Associated with Access to Health Messages Among the Rural Community in Kersa District, Eastern Ethiopia, 2020 |
Discussion
This study was conducted to assess the demand, access, and factors influencing access to health messages through mass media among rural communities in Kersa district of East Hararghe, Eastern Ethiopia. According to this study, the overall demand of health messages through mass media from the quantitative result was 32.5% (95% CI=28.5–34.2%) and as it was also realized from the qualitative results, most of them were interested in interpersonal sources of health messages. The study also depicted that the overall access to health messages through mass media was 26.6% (95% CI=24.6–28.7%). The final model of multivariable logistic regression analysis indicated that predictors such as having access to electric services; having a mobile phone; type of device owned; exposure to TV, social media, and printed media; and those who preferred media programs such as news, current affairs, health and education were significantly associated with access to health messages.
This study found that the demand for health messages in rural communities was 32.5%. Findings from a study conducted in Ethiopia revealed that 20.8% of the population demanded antiretroviral treatment.40 On the other hand, a study conducted in Sierra Leon explicitly showed that 86% of people wanted to receive more information on health for themselves and their families, on a range of health issues, and were particularly interested in receiving information on health issues that they already had some knowledge of (29% mentioned that they wanted information on malaria and typhoid), and 11% wanted to receive information on health topics that they currently did not know much about.41 Thus, in one or another way, sorts of information vividly related to the type of topic discussed, when the topic to be discussed is related to the current issues, the chance of being demanded among the study participants would dramatically and drastically increase. In addition, health message communicators should take into consideration the factors that vividly increase the demand for health messages when plan to communicating with the target population because health message demand can be based on perceived or actual health problems, preferences, values, and expectations of individuals.42
According to this study, access to health messages through mass media accounted for 26.6% of the total. Thus, 25.9% of the study participants had access to health messages through radio (25.9%), had access to TV (63.2%), mobile phones (52%), and had access to more than one type of media (11.3%). This is in line with the findings from the EDHS analysis, where 32.5% of households had a radio and 4.9% had a TV, but 39.1% were exposed to radio and 18.5% to TV. Thus, our study clearly showed that, regardless of the type of information, those who utilize a combination of radio, TV, and mobile phones have a higher level of exposure to information.35,40 It is fact that, access to the health messages depend on the accessibility, affordability, acceptability, and appropriateness of the communication sources, channels, and content media; therefore, without such access, media communication is regarded as speaking into space because target audiences may not receive the message that health communicators intended to deliver to the target audiences.43
This study pointed out that having electric services is statistically significant for accessing health messages through the mass media. Thus, those who had electric services were 2.36 times more likely to have access to health messages than their counterparts. This is explicitly related to the fact that electric light and power must be available to render media devices functional and workable. Moreover, the majority of those rural communities did not have dry cell batteries and did not use solar energy to charge their mobile phones to replace radio and use them for dual functions.35 Another possible explanation was electric power can increase health message access by providing electricity supply for healthcare facilities, which can improve their services, equipment, and communication, and also enable the use of digital technologies such as mobile phones, the Internet, and telemedicine, which can improve the health information and awareness deliverances for the targeted population.
This study showed that having a mobile phone is statistically significant for accessing health messages through the mass media. Thus, the study participants who had a mobile phone were 4.56 times more likely to access health messages than their counterparts. This is consistent with studies conducted in different settings worldwide.3,13,23 The most likely reason for this could be the easy and simple portability of these devices and their dual functionality. Moreover, mobile devices allow users and customers to easily trace and access health messages whenever they want. Furthermore, Mobile phones can increase access to health messages by enabling people to use patient portals, the hello doctor program, and text messages from the Ministry of Health, which help people in preventing communicable diseases, to get the innovative health information and receive advice from health message Communicators or health care providers. It also gives health messages to aid people in preventing and controlling non-communicable diseases (NCDs) and mobile devices uses to improve public health and healthcare delivery through frequent reminding the audiences.
Moreover, our study revealed that those who had an exposure to TV and social media and printing were 4.73 and 5.24 times more likely to access health messages than those who had exposure to radio (AOR=4.73, 95% CI=1.03–11.62; and AOR=5.24, 95% CI=1.07–15.63, respectively). This is in line with a study conducted in Iran, where those exposed to TV and social media were more likely to have ample health messages than their counterparts.44 Television has the potential to increase the accessibility of health messages by quickly disseminating up-to-date and correct information to a wide range of viewers. It may also utilize social media to improve audience engagement and participation with health message if it covers health issues objectively and without bias.45,46 One possible explanation could be related to the facts that there is a pre-planned weekly program related to health that is clearly disseminated through the aforementioned media. Thus, everybody had prior notice through advertisements of what kind of health-related message and when, which in turn provided them with a golden opportunity to set and arrange their time so as not to miss the program. Moreover, many expert opinions can be readily distributed in detail through the media.
Furthermore, program preferences among the study participants clearly indicated access to health messages. Those study participants who preferred programs such as news, current affairs, health and education were 2.37, 9.47, 4.75, and 7.55 times more likely to access health messages as compared to their counterparts. This is in line with studies conducted in different settings worldwide.7,13,23,24,39,44 Preferences for channels and programs increase how a health message program operates and is delivered to target populations, if audiences preferred with health topic program it can increase the reach of health message that makes health information more understandable and accessible to people who need it and also help health message communicator reaching their message as they intended to be communicated.34,47 One of the possible justifications related to this was that people have unreserved and unwavering tendencies toward pre-sated, pre-planned, and current programs. Moreover, expert-entrained issues include breath-taking and eye-catching tendencies of the audience or target population. Hence, the likelihood of devoting time and accessing is likely to be high.
Finally, the odds of access to health messages were 79% less likely during the weekend. This could be related to the fact that weekends would be where the majority of people engage in different activities and tasks linked to social life other than that of media, which in turn deters them from being actively involved in accessing health messages.
Strength and Limitation of the Study
Caution should be exercised when interpreting survey results. This cross-sectional design prevents straightforward establishment of cause-and-effect linkages. We employed a mixed-method study design that addressed the qualitative and quantitative aspects of the problems. One of the notable limitations of the study is the social desirability bias, as household reports conform to larger audiences detaching from reality. Hence, we strongly recommend that researchers implement observational tools to address these problems. The Delphi method to retrieve data from experts will also be required to more mature the future finding.
Conclusions
The findings from this study indicated that more than a quarter of the study participants had access to health messages in the rural community of Kersa District, whereas the overall demand for health messages was 32.5%. Factors such as having access to electric services; having a mobile phone; type of device owned; exposure to TV, social media, and printing media; and those who preferred media programs such as news, current affairs, health and education were significantly associated with access to health messages. Thus, concerned entities should pay attention to and have a strong emphasis on enhancing preplanned health-related programs that directly address health-related issues of the community. In addition, health message communicators would be more successful if they worked together with local institutions, partners, and communities when designing and establishing communication strategies to enhance demand for and access to health messages. Furthermore, research-based strategies, and address communication barriers when disseminating health information to the target population are also enormous.
Data Sharing Statement
All data generated and analyzed during this study are available from the corresponding author upon reasonable request.
Ethical Approval
The study was carried out in accordance with the Helsinki Declaration, and ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the Haramaya University College of Health and medical Sciences. Support letters from the College of Health Sciences were submitted to the kebeles where the study was conducted. After obtaining all permission letters from the responsible body, informed voluntary, and written consent, was signed by study participants and informed consent was taken from a parent or legal guardian of participants under 18 years of age. Confidentiality was maintained by using codes instead of the participant’s name. Participants were also informed that they have full right to refuse participation or withdraw any time from the research and the participants informed consent included publication of anonymized responses.
Acknowledgment
The authors would like to thank the Haramaya University College of Health and Medical Science for their kind cooperation in this study. The authors would also like to express their gratitude to the study participants in the district for their genuine cooperation during the data collection and throughout the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bettinghaus EP. Health promotion and the knowledge-attitude-behavior continuum. Prev Med. 1986;15(5):475–491. doi:10.1016/0091-7435(86)90025-3
2. Schiavo R. Health Communication: From Theory to Practice. John Wiley & Sons; 2013.
3. Yinimi G, Atutiga PP, Banleman K. The role of mass communication in ghana’s rural development: a case study of wa west district. New Med Mass Commun. 2016;55:1.
4. Redmond N, Baer HJ, Clark CR, Lipsitz S, Hicks LS. Sources of health information related to preventive health behaviors in a national study. Am J Prev Med. 2010;38(6):620–627.e2. doi:10.1016/j.amepre.2010.03.001
5. Colon-Ramos U, Atienza AA, Weber D, Taylor M, Uy C, Yaroch A. Practicing what they preach: health behaviors of those who provide health advice to extensive social networks. J Health Commun. 2009;14(2):119–130. doi:10.1080/10810730802659111
6. Avcı K, Çakır T, Avşar Z, Üzel Taş H. Examination of the mass media process and personal factors affecting the assessment of mass media-disseminated health information. Glob Health Promot. 2015;22(2):20–30. doi:10.1177/1757975914536912
7. Li X, Liu Q. Social media use, eHealth literacy, disease knowledge, and preventive behaviors in the COVID-19 pandemic: cross-sectional study on Chinese Netizens. J Med Inter Res. 2020;22(10):e19684. doi:10.2196/19684
8. Mahmud AJ, Olander E, Eriksén S, Haglund BJ. Health communication in primary health care -A case study of ICT development for health promotion. BMC Med Inform Decis Mak. 2013;17:13.
9. Fenton SH, Low S, Abrams KJ, Butler-Henderson K. Health information management: changing with time. Yearb Med Inform. 2017;26(1):72–77. doi:10.15265/iy-2017-021
10. Alireza G. Demand for Health and Healthcare. In: Amit A, Srinivas K, editors. Healthcare Access. IntechOpen; 2021:3.
11. Anwar A, Malik M, Raees V, Anwar A. Role of mass media and public health communications in the COVID-19 pandemic. Cureus. 2020;12(9):e10453. doi:10.7759/cureus.10453
12. Tumpey AJ, Daigle D, Nowak G. Communicating during an outbreak or public health investigation. CDC Field Epidemiol Manual. 2018;2018:243–259.
13. Naveena N. Importance of mass media in communicating health messages: an analysis. IOSR J Humanit Soc Sci. 2015;20(2):36–41. doi:10.9790/0837-20253641
14. Evans WD, Thomas CN, Favatas D, Smyser J, Briggs J. Digital segmentation of priority populations in public health. Health Educ Behav. 2019;46(2_suppl):81S–89S. doi:10.1177/1090198119871246
15. Van Dijck J, Alinejad D. Social media and trust in scientific expertise: debating the Covid-19 pandemic in the Netherlands. Soc Med Soc. 2020;6(4):2056305120981057.
16. Cislaghi B, Denny EK, Cissé M, et al. Changing social norms: the importance of “organized diffusion” for scaling up community health promotion and women empowerment interventions. Prev Sci. 2019;20:936–946. doi:10.1007/s11121-019-00998-3
17. Health UDo, Services H. Theory at a Glance: A Guide for Health Promotion Practice. Lulu. com; 2018.
18. Hostiuc MF, Radu G, Solomon M, Purcarea VL. Preventive medicine through the efficiency of marketing communication and promotional materials; 2017.
19. Greenberg AJ, Haney D, Blake KD, Moser RP, Hesse BW. Differences in access to and use of electronic personal health information between rural and urban residents in the United States. J Rural Health. 2018;34:s30–s38. doi:10.1111/jrh.12228
20. Benham-Hutchins M, Staggers N, Mackert M, Johnson AH, DeBronkart D. “I want to know everything”: a qualitative study of perspectives from patients with chronic diseases on sharing health information during hospitalization. BMC Health Serv Res. 2017;17(1):1–10. doi:10.1186/s12913-017-2487-6
21. Sheeran P, Klein WM, Rothman AJ. Health behavior change: moving from observation to intervention. Ann Rev Psychol. 2017;68:573–600. doi:10.1146/annurev-psych-010416-044007
22. Van Cappellen P, Rice EL, Catalino LI, Fredrickson BL. Positive affective processes underlie positive health behaviour change. Psychol Health. 2018;33(1):77–97. doi:10.1080/08870446.2017.1320798
23. Durkin S, Brennan E, Wakefield M. Mass media campaigns to promote smoking cessation among adults: an integrative review. Tob Control. 2012;21(2):127–138. doi:10.1136/tobaccocontrol-2011-050345
24. Keller-Hamilton B, Stevens EM, Villanti AC, Leshner G, Wagener TL, Mays D. Messaging to prevent and reduce young adults’ waterpipe tobacco smoking: a randomized trial. Addict Behav. 2023;138:107546. doi:10.1016/j.addbeh.2022.107546
25. Whitehead D. Using mass media within health-promoting practice: a nursing perspective. J Adv Nurs. 2000;32(4):807–816. doi:10.1046/j.1365-2648.2000.01544.x
26. Kumar KJ. Mass Communication in India. Jaico publishing house; 2020.
27. Ngigi S, Busolo DN. Behaviour change communication in health promotion: appropriate practices and promising approaches. Inter J Innov Res Develop. 2018;7(9):84–93. doi:10.24940/ijird/2018/v7/i9/SEP18027
28. Hefler M, Kerrigan V, Henryks J, Freeman B, Thomas DP. Social media and health information sharing among Australian Indigenous people. Health Promo Inter. 2019;34(4):706–715. doi:10.1093/heapro/day018
29. Al-Dmour H, Masa’deh R, Salman A, Al-Dmour R, Abuhashesh M. The role of mass media interventions on promoting public health knowledge and behavioral social change against COVID-19 Pandemic in Jordan. Sage Open. 2022;12(1):21582440221082125. doi:10.1177/21582440221082125
30. Hackett AJ. Risk, its perception and the media: the MMR controversy. Comm Practit. 2008;81(7):22–25.
31. O’Hara SK, Smith KC. Presentation of eating disorders in the news media: what are the implications for patient diagnosis and treatment? Patient Educ Couns. 2007;68(1):43–51. doi:10.1016/j.pec.2007.04.006
32. Merchant RM, South EC, Lurie N. Public health messaging in an era of social media. JAMA. 2021;325(3):223–224. doi:10.1001/jama.2020.24514
33. Ethiopia ED. Demographic and health survey 2016: key indicators report. The DHS Program ICF; 2016.
34. Asfaw S, Morankar S, Abera M, et al. Talking health: trusted health messengers and effective ways of delivering health messages for rural mothers in Southwest Ethiopia. Archiv Public Health. 2019;77(1):8. doi:10.1186/s13690-019-0334-4
35. Tsehay AK, Zegeye DT, Yilma TM. Impact of mass media exposure on family planning: analysis of the Ethiopian demography and health Survey. J Health Inform Dev Ctries. 2017;3(2):405–441.
36. Anand S, Gupta M, Kwatra S. Social media and effective health communication. Inter J Soc Sci Interdiscip Res. 2013;2(8):39–46.
37. Smith M-K, Denali DL. Social media in health education, promotion, and communication: reaching rural Hispanic populations along the USA/Mexico border region. J Racial Ethnic Health Disparit. 2014;1:194–198. doi:10.1007/s40615-014-0025-3
38. Ethiopian Demeographic health survey EDHS; 2016. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.
39. Etana D, Gurmu E. The Effect of Mass Media on Women’s Reproductive Health Behavior in Ethiopia. East Afr Socl Sci Res Rev. 2018;34(2):37–58. doi:10.1353/eas.2018.0013
40. Tafesse M. Investigating the Impact of Media Advocacy in Framing Accessibility of Antiretroviral Treatment in Ethiopia: a Social Work Perspective. J HIV AIDS Soc Serv. 2007;10(2):174–193. doi:10.1080/15381501.2011.572742
41. Wittels A. Exploring the role of communication in community health in Sierra Leone; 2016.;
42. Rodriguez Santana I, Mason A, Gutacker N, Kasteridis P, Santos R, Rice N. Need, demand, supply in health care: working definitions, and their implications for defining access. Health Econom Policy Law. 2023;18(1):1–13. doi:10.1017/S1744133121000293
43. Ghio D, Lawes-Wickwar S, Tang MY, et al. What influences people’s responses to public health messages for managing risks and preventing infectious diseases? A rapid systematic review of the evidence and recommendations. BMJ Open. 2021;11(11):e048750. doi:10.1136/bmjopen-2021-048750
44. Saei MH, Valadi S, Karimi K, Khammarnia M. The role of mass media communication in public health: the impact of Islamic Republic of Iran broadcasting health channel on health literacy and health behaviors. Med J Islam Repub Iran. 2021;35:54. doi:10.47176/mjiri.35.54
45. Sharma MSK, Gupta YK. Impact of mass media on health-seeking behaviour of an individual (A Study in the State of Rajasthan). Available from: https://www.academia.edu/34938583/Impact_of_Mass.
46. Sharma S, Gupta Y. Mass media for health education (a study in the state of Rajasthan). Multidiscip Int J. 2017;1:26–39.
47. Zallman L, Bearse A, West C, Bor D, McCormick D. Patient preferences and access to text messaging for health care reminders in a safety-net setting. Inform Health Soc Care. 2017;42(1):32–42. doi:10.3109/17538157.2015.1113177
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.