Back to Journals » International Medical Case Reports Journal » Volume 15
Delayed Infection 34 Months After IntraSPINE® Dynamic Internal Insertion
Received 19 June 2022
Accepted for publication 1 September 2022
Published 7 September 2022 Volume 2022:15 Pages 479—483
DOI https://doi.org/10.2147/IMCRJ.S376437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Ngoc Quyen Nguyen,1 Trong Hau Phan2
1Department of Outpatient Clinic, 108 Military Central Hospital, Hanoi City, Vietnam; 2Department of Spinal Surgery, 108 Military Central Hospital, Hanoi City, Vietnam
Correspondence: Ngoc Quyen Nguyen, Department of Outpatient Clinic, 108 Military Central Hospital, No. 1, Tran Hung Dao Street, Ha Ba Trung District, Hanoi City, 113000, Vietnam, Tel +84-989052288, Email [email protected]
Introduction: Postoperative surgical site infection remains one of the major complications after spinal surgery. IntraSPINE® (intraspine) is a dynamic intralaminar device introduced by Cousin Biotech and is indicated for the surgical treatment of lumbar spine disorders. There are no reports on delayed surgical site infection (SSI) after lumbar surgery using this device.
Case Presentation: A 29-year-old male patient was admitted to our department with complaints of moderate pain and chronic subcutaneous abscess with purulent flow from his old surgical scar. Thirty-four months ago, he underwent a traditional open bilateral L4 laminotomy without discectomy and intraspine insertion for the treatment of L4-5 central lumbar spinal stenosis at another hospital. The patient was discharged 4 days after surgery without radiating pain, and the surgical wound was well healed. He gradually returned to his normal activity and work. However, he experienced moderate pain, redness and swelling of his old surgical scar approximately one month before coming to our hospital, but he did not receive any treatment. One month later, he had a mass with purulent discharge at the surgical scar site, and he visited our hospital on December 29th, 2020. Based on the physical examination and MRI findings, delayed -SSI was diagnosed. The patient underwent removal of the intraspine device, debridement and wound closure with closed drainage. The wound healed satisfactorily, and the patient had no complaints more than 2 years later.
Conclusion: A delayed surgical site infection following intraspine insertion may have occurred.
Keywords: postoperative surgical infection, artificial device, lumbar disc herniation
Introduction
Postoperative surgical site infection (SSI) remains one of the major complications after spinal surgery. The rate of SSI after spinal surgery with implantation has been reported to range from 2.2 to 20%.1–6 Postoperative SSI is divided into three groups according to the onset of infection signs: acute (<2 weeks), subacute (2–4 weeks), and chronic (delayed infection) (>4 weeks), among which the prevalence of delayed infection is the lowest.7 A delayed infection after spinal implantation may be difficult to diagnose because of its low incidence and variety of clinical manifestations.8,9
IntraSPINE® is a dynamic intralaminar device introduced by Cousin Biotech and is indicated for the surgical treatment of lumbar spine disorders. It is made from medical dimethyl siloxane with a polyethylene terephthalate covering, and the anterior part is designed to perfectly fit the intralaminar space. According to the manufacturer, the indication of this artificial device is “chronic low back pain in black disc with facet-syndrome, soft and/or dynamic stenosis and foraminal stenosis after operations for large expelled disc hernias in young patients in order to prevent the collapse of the disc and subsequent chronic lower back pain, and insufficiency of the supra-spinal fibrous complex”. ref10 At present, the application of this device is not widespread. The published literature mainly includes studies of its clinical efficacy10,11 or case reports.12,13 To our knowledge, there are no reports on delayed SSI after lumbar surgery using this artificial device. Here, the author presents a case with delayed SSI 34 months following intraspine internal fixation for the treatment of lumbar disc herniation.
Case Presentation
A 29-year-old male patient was admitted to our department on December 29th, 2020 with complaints of moderate pain and chronic subcutaneous abscess with purulent flow from his old surgical scar on the lower back.
Thirty-four months before admission, the patient underwent a traditional open bilateral L4 laminotomy without discectomy and intraspine device insertion for the treatment of L4-5 central lumbar spinal stenosis at another hospital. The patient was discharged 4 days after surgery without radiating pain, and the surgical wound was well healed. He gradually returned to his normal activity and work. However, he had moderate pain, redness and swelling of his old surgical scar approximately one month before coming to our hospital, but he did not receive any treatment. One month later, he had a mass at his old surgical scar site with purulent discharge (Figure 1), and he visited our hospital.
 |
Figure 1 A chronic subcutaneous abscess. |
A chronic subcutaneous abscess (Figure 1) and normal neurological findings were found by physical examination. The erythrocyte sedimentation rate (ESR) was 2 mm/h, and the white blood cell (WBC) count was 6.550/mm3. Magnetic resonance imaging (MRI) of the lumbar spine was performed on the day of the visit and showed a chronic subcutaneous abscess connected to the artificial device (Figure 2). No evidence of lumbar discitis or epidural abscess was detected on MRI (Figure 2).
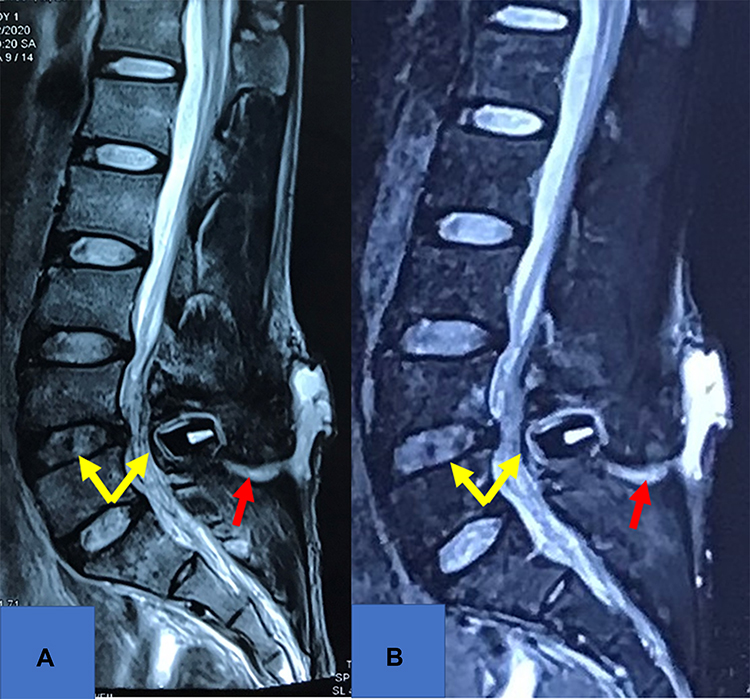 |
Figure 2 Sagittal T2-weighted MRI (A) and sagittal T2-weighted MRI with gadolinium enhancement (B) showed a chronic subcutaneous abscess connected to the artificial device (red arrows) and no evidence of lumbar discitis or epidural abscess (yellow arrows). |
Staphylococcus aureus was found in cultures of purulent flow from the chronic subcutaneous abscess, and cefoxitin 4 gr/day was initiated according to the sensitivity tests. The artificial implant was removed, debridement of the soft tissue and L4 and L5 spinous processes was performed, and closed drainage and wound closure were achieved. Pathological examination of the surgical material was consistent with chronic nonspecific infection, and Staphylococcus aureus was detected again in cultures.
The wound healed satisfactorily, and the patient was discharged on the 10th postoperative day. He had no complaints more than 2 years later.
Discussion
Diagnosis of a delayed SSI after spinal implantation is not easy because of the variety of clinical symptoms and the low incidence.8,9,14,15 The clinical symptoms that have been described include surgical site pain and a feeling of malaise, but spontaneous drainage seems to be the most common.8,9,16 Only a few patients had fever,8 and pain might not be present.14 The diagnosis of this case was not difficult; although the patient did not have a fever, he had moderate pain at the surgical site, and a chronic subcutaneous abscess was found at the site of the old surgical scar. Because the placement of the intraspine device was between the interlumbar laminae and its posterior aspect was under the supraspinous ligament, which was close to the subcutaneous tissue, the bacteria developed near the artificial device and were transferred to the subcutaneous tissue, and the purulent exudate formed the chronic abscess.
Takahashi et al17 reported that infection markers, including C-reactive protein, ESR, and WBC, are present at substantially greater levels in patients with spinal implantation than in patients without implantation. The levels of these markers started increasing 6 hours post-operatively and peaked on the 2nd and 3rd days after surgery. Generally, normal levels are found between the 5th and 21st postoperative days. Elevated infection markers after this period may be considered a warning of SSI. Nevertheless, the ESR and WBC count in this delayed infection case were normal.
MRI may be helpful for the diagnosis of postoperative spinal infection.9 The spread of infection to implants, epidural space, vertebral bodies and soft tissues can be seen on MRI. Abscesses or drainage material are typically contiguous with the implant in postoperative infection cases and are usually connected with the artificial device.8,9 The MRI of this patient showed a typical connection between the subcutaneous abscess and the artificial device.
Removal of the implant, irrigation and debridement, and antibiotherapy are effective treatments for delayed SSI after spinal implantation. The artificial device is usually the source of infection, and only removal of the implant will eradicate the bacteria.8 However, if the removal of the implant may cause further spinal problems, such as spinal instability, or the patient is asymptomatic after intravenous antibiotic therapy and the ESR is reduced, the implant may remain, and irrigation and debridement can be used successfully.8,18,19 In recent years, management with vacuum-assisted wound closure has also been recommended to treat deep SSIs following spinal implantation. Mehbod et al20 treated 20 patients with deep infection after spinal implantation using this method, and all patients achieved a clean closed wound without removal of the implant at a minimum follow-up of 6 months. The artificial devices should be removed if the infection is detected to be contiguous with the implant or the implant is believed to be the cause of the infection.8,9 In this patient, the intraspine device was removed because of infection around the implant that connected with the subcutaneous abscess. In addition, device removal is believed not to cause any problems after surgery.
Conclusions
At present, the application of the intraspine device is not widespread, and it is still necessary to evaluate the efficacy and complications of this implant in the treatment of lumbar spine disorders. One of the late-onset troublesome complications of using this artificial implant may be a delayed SSI, which should be monitored whenever this device is used.
Abbreviations
SSI, surgical site infection; ESR, erythrocyte sedimentation rate; WBC, white blood cell count; MRI, magnetic resonance imaging.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
Institutional review board (IRB) approval for this study was not required. The patient provided consent for the case details and images to be published, and the guidelines outlined in the Declaration of Helsinki were followed.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aydinli U, Karaeminoğullari O, Tişkaya K. Postoperative deep wound infection in instrumented spinal surgery. Acta Orthop Belg. 1999;65(2):182–187.
2. Pull ter Gunne AF, Cohen DB. Incidence, prevalence, and analysis of risk factors for surgical site infection following adult spinal surgery. Spine. 2009;34(13):1422–1428. doi:10.1097/BRS.0b013e3181a03013
3. Pull ter Gunne AF, Mohamed AS, Skolasky RL, van Laarhoven CJHM, Cohen DB. The presentation, incidence, etiology, and treatment of surgical site infections after spinal surgery. Spine. 2010;35(13):1323–1328. doi:10.1097/BRS.0b013e3181bcde61
4. Pull ter Gunne AF, van Laarhoven CJHM, Cohen DB. Incidence of surgical site infection following adult spinal deformity surgery: an analysis of patient risk. Eur Spine J. 2010;19(6):982–988. doi:10.1007/s00586-009-1269-1
5. Schimmel JJP, Horsting PP, de Kleuver M, Wonders G, van Limbeek J. Risk factors for deep surgical site infections after spinal fusion. Eur Spine J. 2010;19(10):1711–1719. doi:10.1007/s00586-010-1421-y
6. Nota SPFT, Braun Y, Ring D, Schwab JH. Incidence of surgical site infection after spine surgery: what is the impact of the definition of infection? Clin Orthop Relat Res. 2015;473(5):1612–1619. doi:10.1007/s11999-014-3933-y
7. Kuo C-H, Wang S-T, Yu W-K, et al. Postoperative spinal deep wound infection: a six-year review of 3230 selective procedures. J Chin Med Assoc. 2004;67(8):398–402.
8. Bose B. Delayed infection after instrumented spine surgery: case reports and review of the literature. Spine J. 2003;3(5):394–399. doi:10.1016/s1529-9430(03)00023-8
9. Guzey FK, Guzey D, Seyithanoglu MH, Alatas I. Delayed infection 6 years after spinal instrumentation: a case report. Turk Neurosurg. 2007;2014:116.
10. Gelder CL, Drozda M, Spink G. Lumbar microdiscectomy with Intraspine® - A case series. Coluna Columna. 2020;19(3):201–204. doi:10.1590/S1808-185120201903207243
11. Co-Minh D. Surgical outcomes of patients with degenerative lumbar disc disease post-IntraSPINE® device fixation: three-year prospective study. Int J Clin Case Report Rev. 2021;8(1):01–10. doi:10.31579/2690-4861/130
12. Yeh KL, Wu SH, Wu SS. Application of the IntraSPINE® interlaminar device in patients with osteoporosis and spinal stenosis: two case reports. J Int Med Res. 2021;49(10):030006052110499. doi:10.1177/03000605211049961
13. Feng S, Fan Z, Ni J, Yang Y, Fei Q. New combination of IntraSPINE device and posterior lumbar interbody fusion for rare skipped-level lumbar disc herniation: a case report and literature review. J Int Med Res. 2020;48(8):030006052094976. doi:10.1177/0300060520949764
14. Clark CE, Shufflebarger HL. Late-developing infection in instrumented idiopathic scoliosis. Spine. 1999;24(18):1909–1912. doi:10.1097/00007632-199909150-00008
15. Viola RW, King HA, Adler SM, Wilson CB. Delayed infection after elective spinal instrumentation and fusion. A retrospective analysis of eight cases. Spine. 1997;22(20):2441–2444. doi:10.1097/00007632-199710150-00023
16. de la Hera B, Sánchez-Mariscal F, Gómez-Rice A, et al. Deep surgical-site infection following thoracolumbar instrumented spinal surgery: the experience of 25 years. Int J Spine Surg. 2021;15(1):144–152. doi:10.14444/8019
17. Takahashi J, Ebara S, Kamimura M, et al. Early-phase enhanced inflammatory reaction after spinal instrumentation surgery. Spine. 2001;26(15):1698–1704. doi:10.1097/00007632-200108010-00014
18. Ido K, Shimizu K, Nakayama Y, et al. Suction/irrigation for deep wound infection after spinal instrumentation: a case study. Eur Spine J. 1996;5(5):345–349. doi:10.1007/BF00304351
19. Naderi S, Acar F, Mertol T. Is spinal instrumentation a risk factor for late-onset infection in cases of distant infection or surgery? Case report. Neurosurg Focus. 2003;15(3):E15. doi:10.3171/foc.2003.15.3.15
20. Mehbod AA, Ogilvie JW, Pinto MR, et al. Postoperative deep wound infections in adults after spinal fusion: management with vacuum-assisted wound closure. J Spinal Disord Tech. 2005;18(1):14–17. doi:10.1097/01.bsd.0000133493.32503.d3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.