Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Defining “Adequately Treated”: A Post Hoc Analysis Examining Characteristics of Patients with Schizophrenia Successfully Transitioned from Once-Monthly Paliperidone Palmitate to Once-Every-3-Months Paliperidone Palmitate
Authors O'Donnell A, Rao S, Turkoz I ![]() , Gopal S
, Gopal S ![]() , Kim E
, Kim E ![]()
Received 10 September 2020
Accepted for publication 26 November 2020
Published 6 January 2021 Volume 2021:17 Pages 1—9
DOI https://doi.org/10.2147/NDT.S278298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Amy O’Donnell,1 Sanjai Rao,2 Ibrahim Turkoz,3 Srihari Gopal,3 Edward Kim1
1Janssen Scientific Affairs, LLC, Titusville, NJ, USA; 2Department of Psychiatry, University of California, San Diego, La Jolla, CA, USA; 3Janssen Research and Development, LLC, Titusville, NJ, USA
Correspondence: Ibrahim Turkoz
Janssen Research and Development, LLC, Titusville, NJ, USA
Tel +1 609-730-7719
Fax +1 609-730-3232
Email [email protected]
Purpose: Paliperidone palmitate once every 3 months (PP3M) is indicated in adults with schizophrenia adequately treated with once-monthly paliperidone palmitate (PP1M) for at least 4 months, in whom the last two consecutive doses are the same. The decision of when to transition to PP3M is based on the patient’s symptom status while receiving PP1M.
Patients and Methods: In a double-blind relapse–prevention study (NCT01529515), patients who met Positive and Negative Syndrome Scale (PANSS) score stabilization criteria after 4 months of PP1M were eligible for transition to PP3M; those who continued to meet stabilization criteria after 12 weeks following an open-label PP3M dose were randomized to receive PP3M or placebo. We compared (post hoc) PANSS, Clinical Global Impression–Severity (CGI-S), and Personal and Social Performance (PSP) scores during the pre-randomization, open-label phase in patients in randomized versus non-randomized groups using analysis of variance or chi-square tests.
Results: Of 506 patients enrolled, 305 were randomized. After 4 months’ PP1M treatment, PANSS and CGI-S scores were significantly lower and PSP scores significantly higher in randomized patients versus non-randomized patients (least squares means [95% CI]: 57.1 [55.7, 58.6] vs 62.2 [60.0, 64.3], 2.9 [2.8, 3.1] vs 3.3 [3.1, 3.4], and 67.0 [65.7, 68.3] vs 64.5 [62.6, 66.4], respectively); changes from baseline between groups differed significantly (all P ≤ 0.009).
Conclusion: Confirming adequate stabilization with PP1M prior to transitioning to PP3M is critical in maximizing treatment response; clinicians should consider transitioning patients to PP3M only if patients respond well to PP1M for at least 4 months and their last two consecutive doses are the same.
Keywords: treatment outcome, administration and dosage, neuropsychiatric symptoms, psychosocial functioning, stabilization, long-acting injectable antipsychotic
Plain Language Summary
Paliperidone palmitate once every 3 months (PP3M) is indicated in adults with schizophrenia adequately treated with paliperidone palmitate once-monthly (PP1M) for at least 4 months (with the same dose for the last two consecutive months); however, the meaning of “adequately” is subjective and may differ among clinicians. To provide clinicians with a better understanding of the clinical characteristics of a patient who is considered “adequately treated” with PP1M, we conducted a post hoc analysis of a double-blind, placebo-controlled, relapse–prevention study, wherein only patients who met protocol-defined stabilization criteria after five doses of open-label PP1M received PP3M. Those patients who received PP3M and subsequently continued to meet protocol-defined stabilization criteria at week 29 were then randomized to either double-blinded PP3M or placebo. Thus, meeting protocol-defined criteria for randomization after the transition to PP3M served as a proxy for a successful transition from PP1M to PP3M. Our results showed that patients who were ultimately randomized were generally more stable than patients who were not randomized at all time points. Furthermore, we identified that there is a subgroup of patients who may need longer than 4 months of treatment with PP1M to assure stability prior to transitioning to PP3M. Our findings provide useful clinical information that should further assist clinicians in managing the transition of adult patients with schizophrenia from PP1M to PP3M.
Introduction
Suboptimal levels of adherence and persistence with antipsychotic therapy are ongoing challenges in the treatment of schizophrenia.1,2 As reported by the American Psychiatric Association, poor adherence is associated with poor outcomes, including increased risks of relapse, rehospitalization, suicidal and aggressive behaviors, and mortality.2 Because of their long pharmacokinetic half-lives, long-acting injectable (LAI) formulations of antipsychotic medications allow for less-frequent treatment administration and can reduce the treatment burden associated with having to remember to take a medication every day.3 Paliperidone palmitate once every 3 months (PP3M) is an LAI antipsychotic indicated for the treatment of adult patients with schizophrenia who have been adequately treated with once-monthly paliperidone palmitate (PP1M) for at least 4 months.4–6 A PP1M treatment period of at least 4 months is required to ensure that the patient’s symptoms are stable and to optimize the dose for each patient before switching to PP3M.7 Once the PP1M dose has been optimized and the patient has received the same PP1M dose for two consecutive doses, PP3M can be initiated at the next scheduled injection visit at a dose that is a 3.5-fold multiple of the immediately preceding PP1M dose.7
The decision of when to transition a patient from PP1M to PP3M is based primarily on clinical judgment.8 Stabilization on PP1M is critical to maximize treatment response to PP3M. If a long-term optimally effective PP1M dose is not achieved, patients may receive a PP3M dose that is too low, potentially increasing the risk of a relapse, or a PP3M dose that is too high, which may increase the risk of adverse events.7 The selection and optimization of the PP1M dose is based on the severity of schizophrenia symptoms, the ability of the patient to tolerate PP1M, and knowledge of prior antipsychotic doses.4 After 4 months of treatment with PP1M, blood levels approach that of steady state based on population pharmacokinetic models,9 but it may take longer than 4 months to identify the optimal dose at steady state for individual patients and to reach a point where the patient has received the same optimal PP1M dose for two consecutive doses. Moreover, the apparent half-life of PP1M is dose-dependent, with higher doses associated with longer half-lives and hence a longer time until steady state is achieved.10
To aid clinicians in identifying patients who are “adequately treated” on PP1M and ready to transition to PP3M, we analyzed data from the pre-randomization open-label phase of a double-blind, placebo-controlled, relapse–prevention study that evaluated the efficacy and safety of PP3M compared with placebo in delaying time to relapse of schizophrenia symptoms.4 In this study, only PP1M-treated patients who met protocol-defined stabilization criteria based on the Positive and Negative Syndrome Scale (PANSS) scores in the open-label phase were transitioned to PP3M at an equivalent paliperidone palmitate dose; those who continued to meet stabilization criteria after another 12 weeks were randomly assigned to receive PP3M or placebo in the double-blind phase. Therefore, for this post hoc analysis, meeting the criteria for randomization in the double-blind phase served as a proxy for having had a successful transition from PP1M to PP3M. In this analysis, we compared responses to PP1M at various time points before randomization in patients who met stabilization criteria (randomized) versus those who did not (non-randomized) to obtain further insights into what constitutes clinical stability.
Patients and Methods
Patients
Full methodology of this study (NCT01529515) has been published previously.4 Briefly, patients (aged 18 to 70 years) who were diagnosed with schizophrenia (based on criteria of The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision [DSM-IV-TR]) at least 1 year before screening and who had a PANSS total score <120 at screening and baseline were enrolled. Major exclusion criteria included primary, active DSM-IV-TR diagnosis other than schizophrenia, significant risk of suicidal behavior, history of substance dependence within 5 months before screening, and involuntary status in a psychiatric hospital at screening. The study was approved by an independent ethics committee or institutional review board at each site and conducted in accordance with the Declaration of Helsinki and Good Clinical Practices. A full list of participating study sites is provided in Supplementary Table 1. All patients provided written informed consent.
Study Design
After a 3-week screening period, eligible patients received once-monthly doses of PP1M (78, 117, 156, or 234 mg) during a flexible-dose, 17-week, open-label phase (Figure 1). At week 17, patients who met stabilization criteria, defined as a PANSS total score of <70, received a single dose of PP3M (3.5 times the stabilized dose of PP1M). At week 29, patients who continuously met stabilization criteria, defined as a PANSS total score of <70 and scores of ≤4 for the PANSS items P1 (delusions), P2 (conceptual disorganization), P3 (hallucinatory behavior), P6 (suspiciousness/persecution), P7 (hostility), G8 (uncooperativeness), and G14 (poor impulse control), at weeks 21, 25, and 29 were randomly assigned to receive either a fixed dose of PP3M or placebo once every 3 months during the double-blind phase.
 |
Figure 1 Study design showing randomized and non-randomized patient populations. aAt week 17, the stabilization criterion for transition from PP1M to PP3M was PANSS total score <70. bAt week 29, the stabilization criteria for randomization (to be met at weeks 21, 25, and 29) were PANSS total score <70 and scores of ≤4 for the PANSS items P1 (delusions), P2 (conceptual disorganization), P3 (hallucinatory behavior), P6 (suspiciousness/persecution), P7 (hostility), G8 (uncooperativeness), and G14 (poor impulse control). cPatients received PP1M 78, 117, 156, or 234 mg. dPatients received PP3M 3.5 times the stabilized dose of PP1M. Abbreviations: PANSS, Positive and Negative Syndrome Scale; PP1M, once-monthly paliperidone palmitate; PP3M, once-every-3-months paliperidone palmitate. |
Assessments
Neuropsychiatric symptoms of schizophrenia were assessed with the 30-item PANSS scale, which consists of 7 items assessing positive symptoms, 7 items assessing negative symptoms, and 16 general psychopathology items. Each item was rated 1 (symptoms absent) to 7 (extreme), and a total scale score was calculated (range, 30–210 for the 30-item scale).11
Psychosocial functioning was assessed using the Personal and Social Performance (PSP) scale, a 100-point single-item rating scale that examines four domains of behavior: (1) socially useful activities, (2) personal and social relationships, (3) self-care, and (4) disturbing and aggressive behavior.12 Scores of 71 to 100 indicate a mild degree of dysfunction; scores of 31 to 70 indicate varying degrees of difficulty; and scores ≤30 indicate poor function that requires intensive supervision.13
The patient’s overall clinical condition was assessed with Clinical Global Impression–Severity (CGI-S), a 7-point scale ranging from 1 (not ill) to 7 (extremely ill).14
Analysis
In this post hoc analysis, randomized patients were defined as those assigned to PP3M or placebo after continuously meeting stabilization criteria at weeks 17, 21, 25, and 29. Non-randomized patients were defined as those who did not meet stabilization criteria at all assessments at weeks 17, 21, 25, and 29 or who were withdrawn during weeks 17 to 29 for other reasons.
Demographic and baseline characteristics were summarized using descriptive statistics and compared between the groups using analysis of variance or chi-square test. Comparisons between randomized and non-randomized patients in PANSS, PSP, and CGI-S scores were made at baseline and before transitioning to PP3M. Between-group comparisons for PANSS total score, CGI-S score, and PSP score were examined using analysis of covariance models with factors for randomization group and country, and with baseline scores as a covariate.
Results
Patient Disposition and Demographics
Of 506 patients who received PP1M in the open-label phase, 379 received one dose of PP3M in the pre-randomization open-label phase of the study. Of these, 305 patients continued to meet stabilization criteria and were randomly assigned to PP3M or placebo in the double-blind phase (PP3M, n = 160; placebo, n = 145). Overall, 201/506 enrolled patients were not randomized into the double-blind phase owing to withdrawal of consent (n = 66), lack of efficacy (n = 28), adverse event (n = 26), loss to follow up (n = 24), other (n = 17), exposure to prohibited medications (n = 14), failed randomization criteria (n = 13), failed criteria to enter next study phase (n = 10), study terminated by sponsor (n = 2), and death (n = 1) (Figure 1). The results of the double-blind phase of the study have been previously reported4 and this analysis focuses on data during the open-label phase based on subsequent randomization categorization.
At baseline of the open-label phase, patients who were randomized had a shorter duration of illness, lower total PANSS score and CGI-S score, and higher PSP score than non-randomized patients (Table 1).
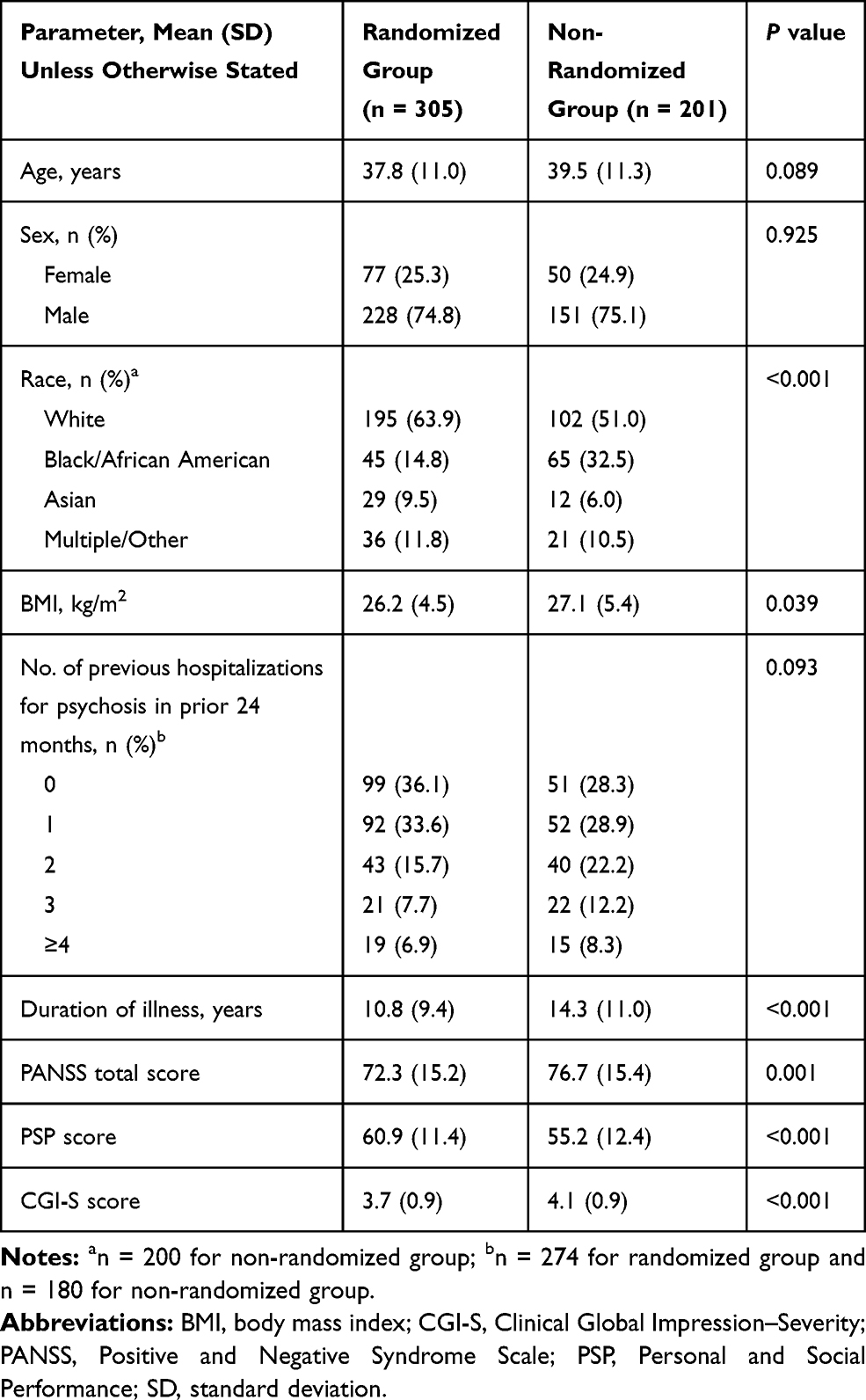 |
Table 1 Open-Label Baseline Demographics and Disease Characteristics by Randomization Status |
Assessment of Symptoms, Functioning, and Clinical Condition
During the 17-week, flexible-dose phase when patients received PP1M, measures of symptoms, psychosocial functioning, and overall clinical condition improved in both the randomized and the non-randomized groups, with effects as early as week 5 (Figure 2A–C; Figure 3).
 |
Figure 2 Least squares mean (A) PANSS total score, (B) PSP scores, and (C) CGI-S scores during open-label PP1M and PP3M treatment in randomized and non-randomized patients. *P < 0.01, **P < 0.001 versus non-randomized. Abbreviations: CGI-S, Clinical Global Impression–Severity; LS, least squares; PANSS, Positive and Negative Syndrome Scale; PP1M, once-monthly paliperidone palmitate; PP3M, once-every-3-months paliperidone palmitate; PSP, Personal and Social Performance; SE, standard error. |
 |
Figure 3 Percentage of patients with stabilization (either PANSS total score <70 alone or PANSS total score <70 and scores of ≤4 for the PANSS items P1 [delusions], P2 [conceptual disorganization], P3 [hallucinatory behavior], P6 [suspiciousness/persecution], P7 [hostility], G8 [uncooperativeness], and G14 [poor impulse control]) over time. **P < 0.001 versus non-randomized (chi squared test). Abbreviation: PANSS, Positive and Negative Syndrome Scale. |
At all time points from baseline to week 17, PANSS scores were significantly lower in randomized patients compared with non-randomized patients. At baseline, least squares (LS) mean PANSS total scores were 67.1 in randomized patients and 73.0 in non-randomized patients. At week 17, after 4 monthly doses of PP1M, LS mean PANSS total scores had decreased to 57.1 in randomized patients and 62.2 in non-randomized patients. The LS mean differences in PANSS total score between randomized and non-randomized patients were –6.0 (95% confidence interval [CI]: –8.6, –3.3) at baseline and –5.1 (95% CI: –7.2, –2.9) at week 17 (Figure 2A).
PSP total scores were significantly higher in randomized patients compared with non-randomized patients at all time points (Figure 2B). At week 17, LS mean PSP scores increased to 67.0 (95% CI: 65.7, 68.3) in randomized patients (from 62.6 [95% CI: 60.8, 64.3] at baseline), and to 64.5 (95% CI: 62.6, 66.4) in non-randomized patients (from 57.7 [95% CI: 55.6, 59.8] at baseline).
From baseline to week 17, CGI-S scores were significantly lower in the randomized group compared with the non-randomized group at all time points (Figure 2C). At week 17, prior to PP3M, LS mean CGI-S scores decreased to 2.9 (borderline ill; 95% CI: 2.8, 3.1) in randomized patients (from 3.5 [mildly ill; 95% CI: 3.4, 3.7] at baseline), and to 3.3 (mildly ill; 95% CI: 3.1, 3.4) in non-randomized patients (from 3.9 [mildly ill; 95% CI: 3.8, 4.1] at baseline).
After the single dose of PP3M at week 17, improvements in total PANSS, PSP, and CGI-S scores were maintained in the randomized group to week 29: by week 29, the LS mean total PANSS score had decreased further to 54.2 (95% CI: 52.9, 56.1; Figure 2A), the LS mean PSP score was 67.7 (95% CI: 66.3, 69.1; Figure 2B) and LS mean CGI-S score was 2.8 (95% CI: 2.7, 2.9; Figure 2C). In non-randomized patients, improvements in total PANSS, PSP, and CGI-S scores achieved by week 17 were not maintained to week 29: LS mean total PANSS score was 66.6 (95% CI: 62.5, 70.7; Figure 2A), LS mean PSP score was 62.3 (95% CI: 59.6, 64.9; Figure 2B), and LS mean CGI-S score was 3.4 (95% CI: 3.1, 3.7; Figure 2C).
Of randomized patients (who by definition had a PANSS total score <70 by week 17, and subsequently maintained a total score <70 and scores of ≤4 for each of the requisite PANSS items at weeks 21, 25, and 29 following PP3M), 171/305 (56.1%) had actually achieved and maintained a PANSS total score <70 since week 5 and following a single dose of PP1M (Figure 3). The majority of these patients (165/171) also had scores ≤4 for the requisite PANSS items since week 5.
Discussion
Schizophrenia is a chronic, lifelong condition that is best managed when patients have consistent continuous antipsychotic medication therapy.2 Although LAIs are a treatment option that can provide such predictable long-term exposure, their extended elimination half-lives require careful dose selection and extended monitoring to ensure that the dose is effective and tolerated at steady-state concentrations. Unlike oral antipsychotics, for which the effects of dose adjustments may be seen within days or weeks, it may take months for LAIs to achieve steady state. The elimination half-life of PP1M ranges from 25 to 49 days, depending on the dose.10 Therefore, steady state may not be reached until as late as 9 months after initiation of treatment. Premature transition to PP3M may result in a non-optimal dose and suboptimal outcomes. The pivotal study for PP3M required that decisions regarding transitioning to PP3M be made according to a fixed protocol-defined timeframe, resulting in a recommendation that patients be treated for at least 4 months with PP1M before switching to PP3M.5 No data are available regarding whether patients treated for more than 4 months on PP1M could have had better outcomes as a result of having greater time for dose optimization.
To provide clinicians with a better understanding of the clinical characteristics of a patient who is considered “adequately treated” with PP1M, we conducted a post hoc analysis of a double-blind, placebo-controlled, relapse–prevention study, wherein only patients who met protocol-defined stabilization criteria after five doses of open-label PP1M received PP3M. Those patients who received PP3M and subsequently continued to meet protocol-defined stabilization criteria at week 29 were then randomly assigned to either double-blinded PP3M or placebo. Thus, meeting protocol-defined criteria for randomization after the transition to PP3M served as a proxy for a successful transition from PP1M to PP3M.
This analysis showed that patients who were ultimately randomized were generally more stable than non-randomized patients at all time points. Specifically, all patients who received PP3M at week 17 had a PANSS total score of <70 after 4 months of treatment with PP1M; however, a subgroup of these patients did not achieve the stabilization criteria required to continue into the randomization phase. In clinical practice, this could translate to patients receiving PP1M who narrowly meet stabilization criteria and then transition to PP3M prematurely, only to find that improvements cannot be maintained and PP3M is discontinued. Optimal stabilization prior to transitioning to PP3M is especially important since dose adjustment with PP3M can be made only once every 3 months and, owing to the long half-life of PP3M, the patient’s response to an adjusted dose will not be apparent for several months.7
Findings from this post hoc analysis may help clinicians to better identify patients currently treated with PP1M who are suitable candidates for transition to PP3M. Although few clinicians routinely use standardized scales such as the PANSS or PSP in practice, they can focus on evaluating their patients for overall severity and stability of symptoms and functioning over the entire PP1M treatment period, whether for 4 months or even longer. Clinicians should demonstrate special caution when considering transitioning patients with higher levels of baseline symptoms and disease severity and with lower functioning as well as those with comparatively longer disease duration, and/or those in whom symptomatic control has only recently been achieved. Such patients may benefit particularly from a longer treatment duration of PP1M before transitioning to PP3M, especially if they are on higher doses, where it may take longer than 4 months to achieve steady state. Patients who are not clinically stable on PP1M, patients who have not been treated continuously with PP1M for 4 months or more, and patients for whom the last two doses were not the same should not be considered candidates for transitioning to PP3M. In a recent analysis of patients treated in the United States, patients received an average of 8.9 PP1M claims prior to transitioning to PP3M, indicating they had been receiving treatment with PP1M for between 8 and 9 months prior to transitioning.3 Although this is significantly longer than the 4 months in the current trial, it is consistent with the principle of ensuring that the dose of PP1M is optimal and stable at steady state prior to transitioning to PP3M.
Note that in our analysis, the assessment of clinical stability was based on PANSS scores, whereas, in clinical practice, the assessment of clinical stability with PP1M and whether a patient is ready to transition to PP3M is based on multiple factors. However, we also looked at CGI-S and PSP scores, although they were not a requirement for meeting randomization criteria, and they were consistent with the PANSS scores. We also acknowledge that some patients were not randomized to treatment because of study-related criteria such as withdrawal of consent, lack of efficacy, and adverse events rather than PANSS total scores. However, these reasons are still consistent with poor patient candidacy for transition to PP3M, as the patient’s willingness to commit to the treatment and PP1M efficacy and tolerability should all be part of the assessment in determining whether a patient receiving PP1M is an appropriate candidate to transition from PP1M to PP3M. In addition, our findings are based on a post hoc analysis, since the study itself was not designed to assess readiness for transition from PP1M to PP3M, and we acknowledge that the necessary design, with patients categorized retrospectively, introduces an inherent selection bias. As expected, smaller numbers of participants were available in the non-randomized group in later visits. Despite these limitations, our results provide useful clinical information that should further assist clinicians in managing the transition of adult patients with schizophrenia from PP1M to PP3M.
Conclusion
There is a subgroup of patients who may need longer than 4 months of treatment with PP1M to assure stability prior to transitioning to PP3M. Based on our analysis, these patients may have higher levels of baseline symptoms and disease severity, lower functioning, longer disease duration, and/or only recent attainment of symptomatic control. We can conclude that confirming adequate stabilization with PP1M prior to transitioning patients to PP3M is critical in maximizing treatment response and that clinicians should consider transitioning patients to PP3M only if they respond well to PP1M for at least 4 months and if the last two consecutive doses of PP1M have been the same.
Abbreviations
BMI, body mass index; CGI-S, Clinical Global Impression–Severity; CI, confidence interval; DSM-IV-TR, the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; LAI, long-acting injectable; LS, least squares; PANSS, Positive and Negative Syndrome Scale; PP1M, once-monthly paliperidone palmitate; PP3M, paliperidone palmitate once every 3 months; PSP, Personal and Social Performance; SD, standard deviation; SE, standard error.
Data Sharing Statement
The data sharing policy of Janssen Pharmaceutical Companies of Johnson & Johnson is available at https://www.janssen.com/clinical-trials/transparency. As noted on this site, requests for access to the study data can be submitted through Yale Open Data Access (YODA) Project site at https://yoda.yale.edu.
Acknowledgments
The authors thank Sarah Feeny, BMedSci, and Bettina Seri, PhD, of ApotheCom (London, UK), and Lynn Brown, PhD, of ApotheCom (Yardley, PA, USA) for editorial and writing assistance, which was funded by Janssen Scientific Affairs, LLC. The authors are entirely responsible for the scientific content of the paper. The authors would also like to thank the staff at the study sites and the patients involved in the study on which this analysis is based. These data were previously presented in poster form at the 32nd Annual Psych Congress, October 3–6, 2019, San Diego, CA.
Author Contributions
All authors made significant contributions to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by Janssen Scientific Affairs, LLC.
Disclosure
AO and EK were affiliated with Janssen at the time the study was conducted. IT and SG are employees of Janssen and stockholders of Johnson & Johnson, Inc. SR is a speaker for Janssen, Alkermes, Sunovion, Neurocrine, and Otsuka (for non-branded talks). The authors report no other conflicts of interest in this work.
References
1. Patel C, Emond B, Lafeuille MH, et al. Real-world analysis of switching patients with schizophrenia from oral risperidone or oral paliperidone to once-monthly paliperidone palmitate. Drugs Real World Outcomes. 2020;7(1):19–29. doi:10.1007/s40801-019-00172-9
2. American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia.
3. Joshi K, Lafeuille MH, Brown B, et al. Baseline characteristics and treatment patterns of patients with schizophrenia initiated on once-every-three-months paliperidone palmitate in a real-world setting. Curr Med Res Opin. 2017;33(10):1763–1772. doi:10.1080/03007995.2017.1359516
4. Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):830–839. doi:10.1001/jamapsychiatry.2015.0241
5. INVEGA TRINZA® (paliperidone palmitate) extended-release injectable suspension for intramuscular use. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2019.
6. Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. 2016;19(7):pyw018. doi:10.1093/ijnp/pyw018
7. Gopal S, Vermeulen A, Nandy P, et al. Practical guidance for dosing and switching from paliperidone palmitate 1 monthly to 3 monthly formulation in schizophrenia. Curr Med Res Opin. 2015;31(11):2043–2054. doi:10.1185/03007995.2015.1085849
8. Magnusson MO, Samtani MN, Plan EL, et al. Dosing and switching strategies for paliperidone palmitate 3-month formulation in patients with schizophrenia based on population pharmacokinetic modeling and simulation, and clinical trial data. CNS Drugs. 2017;31(4):273–288. doi:10.1007/s40263-017-0416-1
9. Magnusson MO, Samtani MN, Plan EL, et al. Population pharmacokinetics of a novel once-every 3 months intramuscular formulation of paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinet. 2017;56(4):421–433. doi:10.1007/s40262-016-0459-3
10. INVEGA SUSTENNA® (paliperidone palmitate) extended-release injectable suspension, for intramuscular use. Titusville, NJ: Janssen Pharmaceuticals Inc.; 2019.
11. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
12. Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV social and occupational functioning assessment scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323–329. doi:10.1034/j.1600-0447.2000.101004323.x
13. Patrick DL, Burns T, Morosini P, et al. Reliability, validity and ability to detect change of the clinician-rated Personal and Social Performance scale in patients with acute symptoms of schizophrenia. Curr Med Res Opin. 2009;25(2):325–338. doi:10.1185/03007990802611919
14. Guy W. ECDEU Assessment Manual for Psychopharmacology Revised, 1976. Rockville, Maryland: US Department of Health Educatuion and Welfare; 1976.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.