Back to Journals » International Journal of Nanomedicine » Volume 20
Deep Eutectic Solvents in Chronic Wound Management: Current Developments and Future Prospects
Received 4 October 2025
Accepted for publication 3 December 2025
Published 12 December 2025 Volume 2025:20 Pages 14955—14973
DOI https://doi.org/10.2147/IJN.S572066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. RDK Misra
Rakesh Bastola,1 Raj Kumar Thapa1,2
1Pharmacy Program, Gandaki University, Pokhara, Kaski, Nepal; 2Research Center, Invention and Innovation Center, Gandaki University, Pokhara, Kaski, Nepal
Correspondence: Raj Kumar Thapa, Email [email protected]
Abstract: Chronic wounds pose a significant and growing global health challenge, affecting millions of individuals and often leading to prolonged suffering and increased healthcare costs. A major barrier to effective healing is wound infection, which disrupts the natural repair process and contributes to the chronicity. Therefore, innovative strategies for infection control are urgently required. Deep Eutectic Solvents (DESs) have recently gained attention as promising drug delivery systems owing to their multifunctional properties. In addition to serving as penetration enhancers that improve drug permeation, DESs exhibit intrinsic antimicrobial and antibiofilm activities, making them attractive candidates for managing infected wounds. This review highlights the fundamentals of DESs in the context of chronic wound management. It provides an overview of the wound healing process, pathophysiology of chronic wounds, and the role of biofilms in persistent infections. It further explores the dual role of DESs as penetration enhancers and antibiofilm agents, summarizing the recent DES-based formulations under investigation. Finally, this review discusses the current challenges and future prospects of integrating DESs into clinical practice. Collectively, DESs represent novel and versatile therapeutic platforms that have the potential to transform the treatment landscape of chronic wound healing.
Keywords: antibiofilm agent, chronic wound, deep eutectic solvent, penetration enhancer, wound healing
Introduction
Injuries caused by surgery, pathological conditions (eg, diabetes and vascular diseases), or extrinsic factors (eg, cuts, burns, and pressure) that compromise the structure and integrity of the skin are defined as acute and/or chronic wounds.1,2 Acute wounds typically heal within 4–6 weeks with complete restoration of functional and anatomical skin integrity.3 However, chronic wounds take longer to heal, typically requiring more than 6 weeks,3 due to pathological conditions such as venous stasis, autoimmune diseases and diabetes.2 Prior infections, tumors, and inflammation may also result in chronic wounds. Delays in the healing process provide opportunities for bacterial infection and growth, thereby hindering optimal and functional restoration of skin integrity.2 Diabetic foot ulcers are one of the most common chronic wounds, and have been estimated to affect 9.1–26.1 million people annually.4 Basic treatment strategies for chronic wounds include sharp debridement, surgical drainage of abscesses, debridement of osteomyelitis, and antimicrobial therapy.5 Wound dressings can be used to create and maintain a moist environment to enhance wound healing. A moist wound environment reduces pain and scarring, facilitates autolytic debridement and activates collagen synthesis.6 It also boosts the migration of keratinocytes to the surface of the wound and supports the function of growth factors, nutrients, and other soluble mediators in the wound microenvironment. Moist wound dressings include foams, films, hydrogels, hydrocolloids and alginates.6
The stratum corneum (SC) is the outermost layer of skin that is non-living in nature. This renders the skin impermeable and hinders the drug permeation.7,8 Only a few drug molecules can permeate intact skin. Specifically, molecules with low molecular weight (<500 Da) and optimal lipophilicity (logP = 1–3) can penetrate the skin.8 Therefore, chemical penetration enhancers (CPEs) such as azone, terpenoids, ethanol, sulfoxide, and glycosides are used to enhance drug permeation.9 CPEs enable drug molecules to permeate and accumulate in deeper skin regions,10 resulting in an increased drug concentration at the site of injury including the biofilms, thereby enhancing wound healing.
Biofilm formation can occur in wounds. A biofilm contains microorganisms entrenched in extracellular polymeric substances (EPS). It is comprised of bacteria, fungi, viruses, proteins, extracellular DNA, and other biogenic factors.11 Biofilms are more common in chronic wounds than in acute wounds, and are attributed to delayed wound healing.12 This hinders effective treatment of skin and soft tissue infections.13 Antibiofilm agents disrupt and prevent biofilm formation,14 thereby enhancing chronic wound healing. Antibiofilm agents include antibiotics, surfactants, antimicrobial peptides, bacteriophages, quorum sensing inhibitors, nanoparticles and hydrogels.15
Deep eutectic solvents (DESs) are eutectic mixtures of two or three compounds associated with hydrogen bond interactions.16 The melting point of DES is lower than that of each individual component. Usually, DES exists in the liquid state at room temperature.16 DES can act as penetration enhancer17 and antibiofilm agent15 for chronic wound healing. However, few studies have been conducted to explore the properties of DES as penetration enhancers and antibiofilm agents.
This review provides a brief overview of DES, the physiology of wound healing, the features of chronic wounds, and biofilm formation. Here, we examine the role of DES as both a penetration enhancer and antibiofilm agent for chronic wound healing. Additionally, this review provides an insight into current DES-based formulations, and discusses the obstacles and future perspectives associated with the use of DES for chronic wound healing.
Deep Eutectic Solvents
A DES contains two or three components that interact with each other through hydrogen bonding to form a eutectic mixture.16 The DES exhibits a melting point that falls below that of each constituent compound. The characteristic feature of DES is a very large depression of the freezing point, resulting in a liquid state of the mixture at temperatures below 150°C.16 Typically, DESs are prepared by mixing a quaternary ammonium salt with metal salts or a hydrogen bond donor that has the potential to form a complex by interacting with the halide ion present in the quaternary ammonium salt.16,18
DESs are considered a new class of ionic liquids (IL) because of their many characteristic similarities. DESs and ILs are two different types of solvents; however, they have been used interchangeably in literature. ILs are composed of one type of discrete anion and cation, whereas DESs are formed from a eutectic mixture of Lewis or Brønsted acids and bases containing a variety of cationic and/or anionic species.19 High thermal stability, low volatility, low vapor pressure, and tunable polarity are some of the general characteristics of both DESs and ILs. DESs are biodegradable, inexpensive, non-toxic, and easy to prepare; however, ILs are non-biodegradable, expensive, and highly toxic.20
As a pioneer, Abbott et al illustrated significantly deep melting point depression of eutectic mixture of hydrogen bond donors (HBDs) and acceptors (HBAs).21 A 1:2 mole fraction combination of choline chloride (melting point = 302°C) and urea (melting point = 133°C) resulted in a eutectic composition (melting point = 12°C), which is a liquid at ambient temperature.21 Urea, glycerol, l-lactic acid, and d-fructose are commonly used HBDs to prepare DES, whereas examples of HBAs include choline chloride, nicotinic acid, l-alanine, and methyltriphenylphosphonium bromide.22
Classification of DESs
DESs are prepared by mixing HBD and HBA at a certain molar ratio, which results in depression of the melting point of the solvent.23 The DESs were classified into four categories, as listed in Table 1.19,24 DESs can be represented by general formula19 as follows:
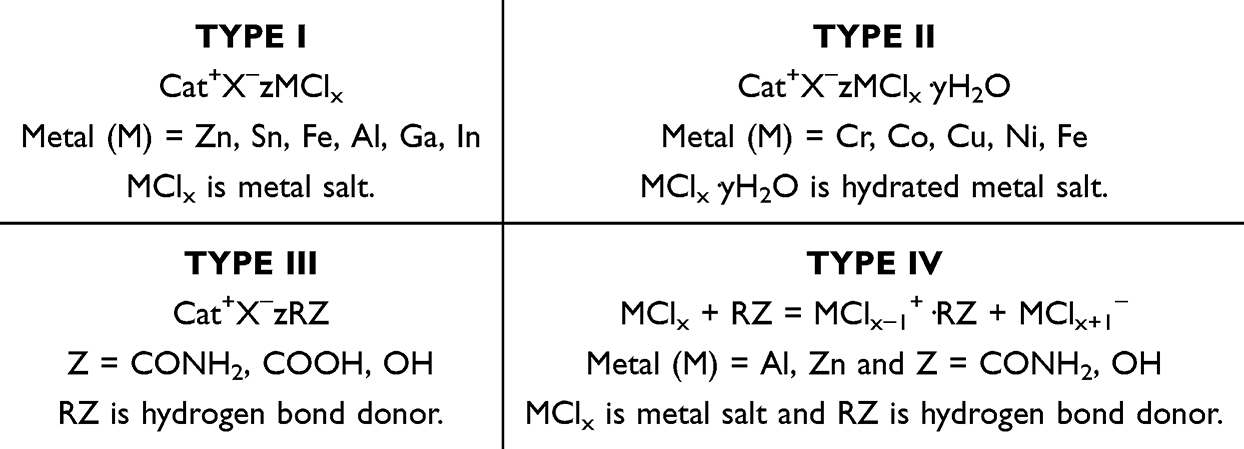 |
Table 1 Classification of DESs into Four categories19,24 Cat+ is Generally a Phosphonium, Ammonium, or Sulfonium Cation; X is a Lewis Base, That is Usually a Halide Anion; and z Represents the Number of Molecules Interacting with Anion That Can Be Metal Salt, Hydrated Metal Salt or Hydrogen Bond Donor |

where Cat+ is generally a phosphonium, ammonium, or sulfonium cation; X is a Lewis base, which is usually a halide anion; Y is a Lewis or Brønsted acid; and z represents the number of Y molecules interacting with the anion.
Type I DESs consist of quaternary ammonium salts and metal chlorides, whereas Type II DESs contain quaternary ammonium salts and hydrated metal chlorides.25 Type I DESs have a high melting point owing to the presence of non-hydrated metal halides. Type III DESs consist of quaternary ammonium salts and HBDs, whereas Type IV DESs are composed of metal chlorides and HBDs (eg, ethylene glycol and urea).25 Recently, new types of DESs have been proposed as Type V, which are composed of non-ionic HBAs and HBDs.26
Among the different categories, Type III DESs have been extensively studied and are usually based on choline chloride and various hydrogen-bond donors.23,24 Choline chloride is inexpensive, biodegradable, and non-toxic, making it a natural additive for several animal species.24
Based on their aqueous solubility, Type III DESs can be further classified as hydrophilic and hydrophobic DESs.27 Hydrophilic DESs are prepared from small quaternary ammonium salts (eg, choline chloride) and HBDs (eg, urea, ethylene glycol, glycerol, and small organic acids). They are highly hygroscopic, have a relatively low viscosity and reasonable conductivity.27 Hydrophobic DESs are composed of hydrophobic compounds, such as thymol, menthol, tetrabutylammonium bromide, and fatty acids as HBAs, along with carboxylic acids and long-alkyl-chain alcohols as HBDs.24 These solvents are promising for the extraction of natural compounds and metals from aqueous solutions. Compared to hydrophilic DESs, hydrophobic DESs have higher viscosities and low conductivity.27
Active pharmaceutical ingredients (APIs) such as lidocaine, ibuprofen, and phenylacetic acid can be used to prepare DES; in such cases, DESs are referred to as therapeutic DESs (THEDES).24 A DES, which consists of a polymerizable monomer and conductive ion salt along with other components, and possesses the capability to undergo polymerization reactions, is known as a polymerizable DES (PDES). In general, PDESs are used to prepare gel-based formulations.28
Type III DES are sometimes referred to as natural DES (NADES).24 NADESs mostly contain natural primary metabolites such as sugars, sugar alcohols, amines, organic acids, and amino acids, along with water at specific molar ratios.29 Depending on the nature of the components, NADESs have been categorized into five major groups:24,30
- Ionic liquids (prepared from an acid and a base)
- Neutral liquids (composed of sugars only, or sugars with other polyalcohols)
- Neutral liquids with acids (composed of sugars/polyalcohols and organic acids)
- Neutral liquids with bases (composed of sugars/polyalcohols and organic bases)
- Amino acid-containing NADES (composed of amino acids and organic acids/sugars)
Preparation and Characterization of DESs
Common methods used for the preparation of DES include heating and stirring, grinding, vacuum evaporation, and freeze-drying.31 In the heating and stirring method, the compounds are mixed and heated under constant stirring until a homogenous liquid is obtained. The temperature ranges between 50–100°C because at high temperatures, degradation of the DES may occur due to esterification reaction.24 A mortar and pestle is used for the grinding method, where the compounds are mixed and crushed at room temperature to form a clear liquid.24 In the evaporation method, the components are dissolved in water, then most of the water is evaporated under vacuum at 50°C, and finally dried in a desiccator until a constant weight is achieved.31 In the freeze-drying method, an aqueous solution of DES or the individual compounds used for DES preparation are freeze-dried to sublimate water to obtain a pure form of solvent.32
Methods assisted by microwaves and ultrasound have been used to prepare DES. The microwave-assisted method is ultra-fast because, in this method, individual components (ingredients) are mixed in glass bottles and exposed to microwaves for a few seconds (< 30s).32 In the ultrasound (US)-assisted method, various concentrations (10%, 30%, 75%) of components are prepared in distilled water, then kept in glass vials fitted with screw cap and finally exposed to US waves (37 KHz, 30 W) at 50°C until homogenous liquids are obtained.32
Various tools and techniques have been employed to characterize DESs. Intermolecular interactions between DES components (or between drug and DES components in THEDES) can be identified using Fourier transform infrared spectroscopy (FTIR).33 Moreover, proton and carbon nuclear magnetic resonance (NMR) spectroscopy can confirm the chemical structure and purity of the DESs and drug-DES systems.33 Differential scanning calorimetry (DSC)33 and thermogravimetric analysis (TGA)34 can be employed to identify the phase transformation and determine the thermal decomposition behavior of the DESs respectively.
UV-Vis spectroscopy25,33 and high-performance liquid chromatography (HPLC)25 are commonly employed to identify the concentration of API (drug) dissolved in the DESs, which in turn helps to determine the drug solubility and release profile. Likewise, a pycnometer can be used to determine the density and a viscometer to determine the viscosity of the DESs.25 A conductivity meter,35 pH meter,35 Du Noüy ring method,36 and refractometer36 can be employed to determine the electrical conductivity, pH, surface tension, and refractive index of the DESs, respectively.
Chronic Wound
Physiology of Wound Healing
Wound healing is achieved through four overlapping and highly coordinated phases: hemostasis, inflammation, proliferation and remodeling.37 Table 2 shows the phases of wound healing and the key events.
 |
Table 2 Phases of Wound Healing with Key Events |
Hemostasis
Hemostasis is initiated when the integrity of the skin is compromised. Vasoconstriction occurs to prevent blood loss and clot formation seals the vessel. Platelet aggregates result in the formation of an initial hemostatic plug, and initiate coagulation and complement cascades. Prothrombin is activated to form thrombin within the tissue, which, in turn, cleaves fibrinogen to generate fibrin, forming a clot with platelets and plasma fibronectin. In addition, various mediators are released to attract macrophages and fibroblasts to the injury site.37,38
Inflammatory Phase
The inflammatory phase is triggered by the release of mediators from injured capillaries and tissue cells, activated platelets (along with their cytokines), and other by-products of hemostasis. Neutrophils migrate to the injury site and initiate wound repair by activating the fibroblasts and epithelial cells. In addition, monocytes, lymphocytes, and plasma cells arrive at the site of injury.39 Local vessels dilate as a result of coagulation and complement cascades during the hemostasis phase. Bradykinin (generated by the coagulation cascade) and anaphylatoxins, such as C3a and C5a (generated by the complement cascade), increase the permeability of blood vessels and facilitate the migration of inflammatory cells at the wound site.37 Monocytes differentiate into macrophages, which results in the formation of phagocytic cells. They ingest surviving microorganisms, fibrin clots, dead neutrophils, and other cellular debris. In addition, they synthesize NO (nitric oxide) and secrete cytokines that initiate wound repair.39
Proliferative Phase
Degradation of the initial fibrin-platelet matrix and invasion of endothelial cells and fibroblasts occur at the beginning of the proliferative phase. This phase overlaps with the inflammatory phase. Cellular migration through the fibrin clot and provisional matrix is facilitated by the secretion of proteases belonging to serine, cystine, and matrix metalloproteinase (MMP) families.37 The major events in this phase include covering the wound surface with new skin (re-epithelialization), restoration of vascular integrity (neovascularization), and filling of defective tissue with new connective tissue (granulation).39
Keratinocytes completely cover the defective skin surface and initiate re-epithelialization. Locally released growth factors stimulate keratinocyte proliferation. New keratinocytes migrate to the repair site, which requires a fluid environment. Migration involves complex steps that are directed by a chemotactic gradient created by various growth factors. Keratinocytes secrete proteolytic enzymes in the absence of a fluid surface, which enable them to find the moisture necessary for migration.38,39
Neovascularization, or angiogenesis, is the process of re-establishing vascular network.42 This event is stimulated by tissue hypoxia and growth factors. A hypoxic wound environment is created by closure of the wound surface. The fibrin clot formed in the hemostasis phase temporarily covers the wound surface, thereby creating a closed system for angiogenesis to proceed.39 Hypoxia induces secretion of angiogenic growth factors by macrophages. Additionally, angiogenesis is stimulated by lactic acidosis.39 Furthermore, fibroblasts and vascular endothelial growth factors stimulate angiogenesis along the edges of wounds.37,39
Replacement of the fibrin clot scaffold with new tissue rich in hyaluronic acid, fibronectin, and other extracellular matrices (ECM) results in granulation tissue.37,39 Such tissue is metabolically active, highly vascular, and supports the proliferation of a variety of cells and proteins, thereby resulting in a pinkish-red appearance.39 Fibroblasts (dermal cells) are the predominant cell types found in the granulation tissue. Fibroblasts produce collagen, along with other substances that comprise the ECM.39,43 ECM consists of fibronectin (promotes adhesion and migration), hyaluronan (promotes tissue hydration), collagens/elastin (provides tissue resiliency and strength), and chondroitin sulfate (involves in the regulation, storage, migration, and expression of a variety of substances, including enzymes, growth factors, and coagulation proteins).39
Remodeling Phase
During the remodeling phase, wound contraction contributes to the successful closure of full-thickness wounds enhancing the cosmetic appearance.37,41 It also strengthens the scar because the newly formed epithelium that lacks glandular, follicular, nervous, and vascular components, has to cover a smaller area of the wound. Therefore, a high degree of contraction is desirable for wound healing.41
At the end of wound contraction, myofibroblasts disappear by apoptosis or revert to a quiescent fibroblastic phenotype because of reduced tension within the ECM. The components of the ECM change to ascertain the integrity, strength, and function of the replacement tissue during the remodeling phase. The final phase of wound repair involves the conversion of the ECM from granulation to scar tissue, which is referred to as maturation. Proteoglycans replace hyaluronan, supporting the aggregation and deposition of collagen fibers, which in turn provides tensile strength to the wound.41 ECM remodeling depends on the presence of proteolytic enzymes produced by mesenchymal and inflammatory cells,41 such as matrix metalloproteinases (MMPs),44 cathepsins, and serine.41 Wound remodeling may continue for up to two years, and during this period, collagen content does not increase; however, under the influence of local mechanical factors, collagen fibers rearrange themselves into a more organized lattice-like structure, thereby increasing the tensile strength of scar tissue.41
Features of Chronic Wounds
Disruption of the normal wound healing process results in the development of chronic wounds, which pose a significant challenge to patients, healthcare professionals, and the overall healthcare system.45 Chronic wounds do not follow the predictable stages. The three major etiologies include venous, diabetic, and pressure ulcers.46 Venous ulcers occur in the legs and are primarily caused by dysfunctionalization of valves. Diabetic ulcers start as small scratches that usually go unnoticed due to impaired nerves in the lower extremities. However, they may become seriously infected due to poor circulation, compromised immune systems, and damaged capillaries. Pressure ulcers can affect bedridden patients who have limited mobility.46 Although different chronic wounds have different etiologies at the molecular level, they express some common features, such as persistent infections, and deficiency of stem cells that are often dysfunctional, along with elevated levels of proinflammatory cytokines, reactive oxygen species (ROS), senescent cells, and proteases.5
Microorganisms, repeated tissue injury, and platelet-derived factors such as transforming growth factor-β (TGF-β) or ECM fragment molecules result in a constant influx of immune cells, which in turn amplifies the proinflammatory cytokine cascade, leading to higher levels of proteases.5 Proteases are regulated by their inhibitors in acute wounds; however, in chronic wounds, protease levels increase in comparison with the levels of their respective inhibitors, which subsequently results in the destruction of ECM and degradation of growth factors.5,47 The proteolytic destruction of the ECM attracts inflammatory cells and prevents the proliferative phase of wound healing, thereby magnifying the inflammation cycle.5
ROS produced by immune cells at low concentrations can protect microorganisms. However, in chronic wounds, hypoxic and inflammatory environments lead to uncontrolled ROS production, which damages ECM proteins and cause cell damage.5,48 Moreover, the presence of senescent cells with impaired proliferative and secretory capacities is a characteristic feature of chronic wounds, which makes them unresponsive to typical wound-healing signals. Oxidative stress in senescent cells leads to DNA damage-related cell cycle arrest and unusual metabolic changes in patients with diabetes, resulting in defects in intracellular biochemical pathways.5
The environment of chronic wounds is alkaline, with pH ranging from 7.2 to 8.9.46,49 However, acidic environments are essential for fibroblast proliferation, collagen formation, oxygenation, angiogenesis, and macrophage activity. An alkaline environment affects these key processes and prevents healing by further colonization by pathogenic bacteria. Therefore, the occurrence of biofilms is higher in chronic wounds, making them more resistant to biocides.46
Biofilm Formation
A bacterial biofilm consists of microorganisms embedded in extracellular polymeric substances (EPS) that adhere to living or inert surface.11 Biofilms contain not only bacterial cells, but also fungi, viruses, extracellular DNA, proteins, and other biogenic factors. They help bacterial growth by providing a protective environment. Biofilm-producing infections are highly polymicrobial, which further increase virulence and complicate the treatment.11
Biofilm formation occurs in five stages, as illustrated in Figure 1.50 In the first stage, there is reversible attachment of microbes to the surface via flagella, pili, or other surface appendages. The second stage includes irreversible attachment facilitated by EPS secretion. The third stage is characterized by cell proliferation and microcolony formation. Growth and differentiation occur in the fourth stage, resulting in a mature biofilm with features, such as water channels and towering clusters of cells. In the fifth (final) stage, active and/or passive detachment results in the dispersion of biofilm cells.11,51
 |
Figure 1 Stages of biofilm formation. Reproduced with permission from Liu et al.50 |
DESs as Penetration Enhancers for Chronic Wound Treatment
Transdermal drug delivery offers advantages such as improved patient compliance owing to its non-invasive nature, avoidance of first pass metabolism, sustained and controlled drug delivery, reduced side effects, and direct access to target sites.52 Low permeability of the skin is a major challenge in the development of topical and transdermal drug delivery systems.8 Skin barriers protect the organs from foreign toxins and prevent water loss. The outermost non-living layer of the skin, that is, the stratum corneum (SC), hinders permeation of drugs.52 Drug molecules with properties such as low molecular weight (<500 Da) and optimum lipophilicity (logP= 1–3) can easily penetrate the skin. Therefore, only a limited number of molecules can permeate an intact skin.8
The “bricks and mortar” model is generally used to depict the SC, which is the main barrier to transdermal permeation of molecules.53 Figure 2 shows the brick-and-mortar model of the SC.54 In this model, SC morphologically and functionally represent a two-compartment system consisting of corneocytes (bricks) and intercellular matrix (mortar). Corneocytes are primarily composed of fibrous protein networks, whereas intercellular matrix is mainly composed of neutral lipid.55 While penetrating the SC, molecules are transported via either the transcellular pathway (corneocytes) or intercellular pathway (tortuous lipid).53
 |
Figure 2 Bricks and mortar model of the SC. Corneocytes are considered bricks and intercellular matrix as mortar. Reproduced with permission from Banas et al.54 |
The low solubility and permeability of oral drugs render them unsuitable for topical and transdermal delivery systems.9 Various physical, pharmaceutical, and chemical methods have been developed to address these issues. The most common method employed to enhance skin permeability is the use of chemical penetration enhancers (CPEs) such as ethanol, terpenoids, glycosides, sulfoxides, and azones. CPEs act by modifying SC fluidity, increasing the drug’s skin disruption coefficient, and generating hydrophilic pores in the SC to establish drug reservoir.9 Indeed, CPEs enable drug molecules such as antibiotics, analgesics, and anti-inflammatory agents to penetrate tissues and accumulate in deeper skin regions,10 thereby increasing the local drug concentration at the wound site and promoting wound healing.
Understanding the mechanisms of action of DES will aid in designing DES-based formulations for the treatment of chronic wounds. DESs penetrate SC primarily through mechanisms, such as liquid modification, protein modification, and lipid exchange.9 DESs play a crucial role in liquid modification of SC. Hydrophilic DESs act by opening tight junctions and facilitating intercellular transport, whereas hydrophobic DESs act by increasing the transport channels and facilitating transcellular transport.9 In contrast, amphiphilic DESs can pass through the lipid bilayer and destroy the lipid membrane, resulting in increased skin permeability.9,56 DESs can interact with keratin and disrupt its ordered arrangement in the SC, inducing conformational changes in the protein molecules.57,58 In addition, DESs can denature keratin to form vacuoles, thereby enhancing drug penetration.9 When used as drug solvents, DES enhances the penetration of macromolecular drugs through a mechanism known as “lipid exchange.” DESs selectively dissolve and replace lipids and facilitate the diffusion of drug molecules into the deeper layers of the skin.9
Sakuragi et al reported that DES facilitates lysozyme penetration by interacting with lipids in the SC, thereby exhibiting the property of DES as a skin penetration enhancer for proteins.59 Additionally, Boscariol et al demonstrated that DES can promote the transdermal permeation of bioactive macromolecules by disrupting the skin.60 In this study, DES promoted the passage of molecules through the intercellular (composed of lamellar lipids) and transcellular (composed of corneocyte lipid envelopes) routes. Molecules slipped around the lamellar lipids in the intercellular route; however, in the transcellular route, small transient openings were created to allow molecules to pass through.60 Similarly, in a study by Li et al, DESs enhanced the skin penetration of molecules such as oxymatrine and quercetin.61 This study showed that DESs are safe for promoting skin permeability.61 Song et al demonstrated that DES enhanced the skin permeability of L-ascorbic acid.62 The increased solubility of DES in skin lipids (SC) facilitated the penetration of L-ascorbic acid.62 Furthermore, in a recent study, Czyrski et al showed that DES enhanced permeation mainly by loosening lipid packing and increasing lipid and protein mobility.57 In this study, a blend of propylene glycol and DES enhanced the transition of keratin’s secondary structure from α-helix to β-sheet conformation.57
Owing to the lack of understanding regarding toxicity and safety, only a small number of CPEs have been used for commercial purposes. Therefore, there is an urgent need for novel biodegradable and biocompatible skin-penetration enhancers. DESs can be used as CPE alternatives to harmful organic solvents in the treatment of chronic wounds. In addition, DESs can be used as solubilizing agents, drug reservoirs, stabilizing agents and surfactants.9
Chronic wounds are open and lack an intact SC. However, when penetration enhancers such as DESs are used to treat open wounds, they increase the permeation of drugs through the partially intact surrounding skin for localized effect and promote wound healing.63 Additionally, DESs can penetrate the biofilms in the wounds which is essential to disrupt them and control wound infections.13
DESs as Antibiofilm Agents for Chronic Wound Healing
Biofilm formation hinders the treatment of skin and soft tissue infections. A biofilm is a three-dimensional matrix consisting of microbial cells entrenched in an EPS.13 EPS is primarily made of proteins, polysaccharides, and/or extracellular DNA. The biofilm matrix enhances microorganism survival when exposed to antibiotics, resulting in antimicrobial tolerance and treatment failure.13 Biofilm formation, which is common in chronic wounds, prevents wound contracture and epithelialization, induces chronic inflammation, prevents normal epidermal differentiation following healing, and disrupts host immune response.12
An agent that prevents and disturbs biofilm formation in wounds is commonly known as an antibiofilm agent.64 Antibiofilm agents target various stages of biofilm formation, such as initial attachment, irreversible attachment, microcolony formation, maturation, and dispersal, to enhance wound healing.15 Such agents act by targeting cell surface-associated adhesins such as proteins, appendages, and EPS, thereby interrupting the attachment of microorganisms to the wound surface. EPS production and cellular division are also targeted to inhibit the early stages of biofilm development.14 Disruption of biofilm formation can be achieved through various means, such as physical removal of the biofilm, elimination of dormant cells, targeting social interactions (particularly in polymicrobial biofilms), and degradation of the EPS matrix.14 Additionally, antibiofilm agents can achieve biofilm dispersion by inducing EPS matrix remodeling and activating dispersal mechanisms.14 Various approaches are available for managing chronic wound biofilms (Table 3).
 |
Table 3 Approaches for the Management of Chronic Wound Biofilms |
DES disrupts biofilm structure and enhances biofilm removal. DES can solubilize proteins and polysaccharides that are part of the biofilm and other components present in the biofilm matrix.73 DES can restrain microbial adhesion and proliferation and promote biofilm detachment and removal. Moreover, it can control inflammatory cascade associated with wounds and decrease cell stress by inhibiting the production of reactive oxygen species.74
Wikene et al illustrated that the hydrophobic photosensitizer-solubilizing property of DES coupled with photodynamic therapy presented potential for antimicrobial activity.76 A DES containing a hydrophobic compound (curcumin) photo inactivated Escherichia coli at a relatively low concentration of curcumin, ie 1.25 µM.76 Nystedt et al have demonstrated the antibiofilm properties of neutral DES. In a pre-established bacterial biofilm, neutral DES demonstrated bactericidal activity against P. aeruginosa and S. aureus.13 Moreover, biofilm formation by both bacterial species was inhibited by DES at or below 0.5 times the minimum inhibitory concentration (MIC) (sub-MIC levels).13 In a recent study, Swebocki et al showed that DESs eradicated methicillin-resistant Staphylococcus aureus (MRSA) and Escherichia coli biofilms at concentrations below 1% v/v, thereby exhibiting antibiofilm activity.75 DES induced significant morphological changes in both strains. Moreover, in the study, DES exhibited antifungal activity against Candida albicans and Candida auris.75
The hygroscopic and chaotropic effects of DES can modify proteins and disorganize slough, thereby enhancing wound healing of wounds.77 The slough is devitalized or dead proteinaceous host tissue attached to viable tissue. In contrast, biofilms are viable and made of bacteria-derived tissues, where bacteria are embedded in an EPS matrix primarily composed of polysaccharides.78
DESs possess cytotoxic properties and play a significant role in the extraction and purification of virus-like particles.79 Hydrophilic DES can pass through the cell membrane and exhibit toxic effects by disrupting both the pH and the anion pool of the cytoplasm. An increase in internal acidity (lowering pH) adversely affects the integrity of purines, resulting in enzyme denaturation and oxidative stress, thereby affecting microbial cell viability.80,81 In a recent study, Shaw et al demonstrated the antifungal properties of DES against the pathogenic fungal species Candida albicans, suggesting that DES acts as an antibiofilm agent.82 DES interacted with cell wall components, primarily β-glucans, chitin, and glycoproteins, and blocked the uptake of nutrients and other compounds, thereby resulting in cell death due to starvation.82 However, this study did not include data on the effects of DESs on fibroblasts. Other studies, nevertheless, have reported that DESs exhibit good biocompatibility with murine fibroblasts,83 along with excellent viability and proliferation of both fibroblasts and keratinocytes.84
DES-Based Formulations for Chronic Wound Treatment
Different DESs- and DES-based formulations have been used to treat chronic wounds. DESs are primarily used as penetration enhancers and antibiofilm agents in the treatment of chronic wounds. They are also used for therapeutic purposes, wound dressing, and debridement. Examples of DES used for chronic wound healing are presented in Table 4.
 |
Table 4 DES-Based Formulations for Wound Healing |
Challenges and Future Perspectives
DESs are increasingly being recognized as promising drug delivery systems, particularly for the treatment of chronic wounds. Various classes of DES, such as THEDES, NADES, PDES, and conventional DES, have shown potential for enhancing wound healing. Some formulations primarily function as permeation enhancers, facilitating drug penetration into the skin layers and thereby accelerating the repair process. Others exhibit intrinsic biological activities, including antimicrobial and antibiofilm properties, which play critical roles in the reduction of wound-associated infections. In addition, several DES formulations have demonstrated synergistic effects such as stimulating cell migration, promoting angiogenesis, and supporting overall tissue regeneration.
As wound healing is a highly complex and dynamic process, a thorough evaluation of DES toxicity is essential to avoid harmful effects on damaged tissues. Rigorous in vitro and in vivo investigations are required to confirm the safety and therapeutic efficacy of each newly developed DES in human applications. To date, most studies have focused on topical or transdermal applications, with a limited exploration of alternative routes of administration for internal wound management. Although the preliminary findings are encouraging, comprehensive preclinical and clinical studies are necessary to establish DES-based therapies as viable clinical options. Furthermore, such studies will require adherence to strict regulatory standards, including FDA evaluations, before any formulation reaches the market.
Combination approaches represent a promising direction, in addition to stand-alone DES formulations. DES may be incorporated into advanced delivery systems, such as spray-dried or freeze-dried formulations, into lipid nanocarriers or can be used to form microemulsions, creams, or gels to enhance stability and therapeutic performance. Similarly, combining DES with established excipients or delivery platforms can generate synergistic systems that maximize healing outcomes.
Future research should prioritize the design of novel DES using biocompatible and safe excipients with the goal of identifying alternatives that minimize toxicity while maximizing therapeutic benefits. Mechanistic studies are also essential to elucidate the pathways through which DES exerts antimicrobial, antibiofilm, and wound-healing effects. Finally, attention to formulation stability, scalability, and shelf life is critical for translating DES-based systems from laboratory research into market-ready products capable of addressing the global burden of chronic wounds.
Conclusion
DESs have emerged as innovative alternatives for the management of chronic wounds. Their intrinsic antimicrobial, antibiofilm, and wound healing properties highlight their potential as therapeutic candidates in this field. Although chronic open wounds lack an intact SC, the penetration enhancing properties of DES-based formulations facilitate deep drug permeation through the surrounding partially intact skin. This, in turn, promotes wound healing by enabling effective biofilm penetration, disruption, and infection control. Moreover, the incorporation of DES in advanced delivery systems or combination formulations can further enhance their safety, stability, and efficacy while providing synergistic benefits for tissue repair and regeneration. Despite encouraging preliminary findings, extensive preclinical and clinical investigations are essential to validate their safety, elucidate their mechanisms of action, and establish regulatory approval pathways. Overall, DES represent a promising platform for drug delivery and hold significant potential for translation into market-ready therapies aimed at improving the outcomes of chronic wound care.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tottoli EM, Dorati R, Genta I, et al. Skin wound healing process and new emerging technologies for skin wound care and regeneration. Pharmaceutics. 2020;12(8):735. doi:10.3390/pharmaceutics12080735
2. Kolimi P, Narala S, Nyavanandi D, et al. Innovative treatment strategies to accelerate wound healing: trajectory and recent advancements. Cells. 2022;11(15):2439. doi:10.3390/cells11152439
3. Schultz GS, Barillo DJ, Mozingo DW, et al. Wound bed preparation and a brief history of TIME. Int Wound J. 2004;1(1):19–32. doi:10.1111/j.1742-481x.2004.00008.x
4. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
5. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care. 2015;4(9):560–582. doi:10.1089/wound.2015.0635
6. Nuutila K, Eriksson E. Moist wound healing with commonly available dressings. Adv Wound Care. 2021;10(12):685–698. doi:10.1089/wound.2020.1232
7. Prausnitz MR, Mitragotri S, Langer R. Current status and future potential of transdermal drug delivery. Nat Rev Drug Discov. 2004;3(2):115–124. doi:10.1038/nrd1304
8. Emami S, Shayanfar A. Deep eutectic solvents for pharmaceutical formulation and drug delivery applications. Pharm Dev Technol. 2020;25(7):779–796. doi:10.1080/10837450.2020.1735414
9. Wang J, Li M, Duan L, et al. Deep eutectic systems as novel vehicles for assisting drug transdermal delivery. Pharmaceutics. 2022;14(11):2265.
10. Abdelfattah S, Nasr M, Ali A, et al. Vesicular systems used for wound healing. Arch Pharm Sci Ain Shams Univ. 2021;5(1):184–203.
11. Clinton A, Carter T. Chronic wound biofilms: pathogenesis and potential therapies. Lab Med. 2015;46(4):277–284. doi:10.1309/LMBNSWKUI4JPN7SO
12. Weigelt MA, McNamara SA, Sanchez D, et al. Evidence-based review of antibiofilm agents for wound care. Adv Wound Care. 2021;10(1):13–23. doi:10.1089/wound.2020.1193
13. Nystedt HL, Grønlien KG, Rolfsnes RR, et al. Neutral natural deep eutectic solvents as anti-biofilm agents. Biofilm. 2023;5:100114. doi:10.1016/j.bioflm.2023.100114
14. Koo H, Allan RN, Howlin RP, et al. Targeting microbial biofilms: current and prospective therapeutic strategies. Nat Rev Microbiol. 2017;15(12):740–755. doi:10.1038/nrmicro.2017.99
15. Thapa RK, Kim JO, Kim J. Antimicrobial strategies for topical biofilm-based wound infections: past, present, and future. J Pharm Investig. 2023;53(5):627–641. doi:10.1007/s40005-023-00628-9
16. Zhang Q, Vigier KDO, Royer S, et al. Deep eutectic solvents: syntheses, properties and applications. Chem Soc Rev. 2012;41(21):7108–7146. doi:10.1039/c2cs35178a
17. Lv J, Wu P, Fang Y, et al. Deep eutectic solvents based on L-arginine and 2-hydroxypropyl-β-cyclodextrin for drug carrier and penetration enhancement. AAPS Pharm Sci Tech. 2023;24(7):187. doi:10.1208/s12249-023-02638-0
18. Kovács A, Neyts EC, Cornet I, et al. Modeling the physicochemical properties of natural deep eutectic solvents. ChemSusChem. 2020;13(15):3789–3804. doi:10.1002/cssc.202000286
19. Smith EL, Abbott AP, Ryder KS. Deep eutectic solvents (DESs) and their applications. Chem Rev. 2014;114(21):11060–11082. doi:10.1021/cr300162p
20. Hansen BB, Spittle S, Chen B, et al. Deep eutectic solvents: a review of fundamentals and applications. Chem Rev. 2021;121(3):1232–1285. doi:10.1021/acs.chemrev.0c00385
21. Abbott AP, Capper G, Davies DL, et al. Novel solvent properties of choline chloride/urea mixtures. Chem Commun. 2003;(1):70–71. doi:10.1039/b210714g
22. Perna FM, Vitale P, Capriati V. Deep eutectic solvents and their applications as green solvents. Curr Opin Green Sustain Chem. 2020;21:27–33. doi:10.1016/j.cogsc.2019.09.004
23. Dwamena AK. Recent advances in hydrophobic deep eutectic solvents for extraction. Separations. 2019;6(1):9. doi:10.3390/separations6010009
24. El Achkar T, Greige-Gerges H, Fourmentin S. Basics and properties of deep eutectic solvents: a review. Environ Chem Lett. 2021;19(4):3397–3408. doi:10.1007/s10311-021-01225-8
25. Mekuriaw TA, Tizazu BZ. Deep eutectic solvents for lignin isolation. In: Pizzi A, editor. Advanced Lignin Technologies. London, UK: IntechOpen; 2024:1–32.
26. Abranches DO, Martins MAR, Silva LP, et al. Phenolic hydrogen bond donors in the formation of non-ionic deep eutectic solvents: the quest for type V DES. Chem Commun. 2019;55(69):10253–10256. doi:10.1039/C9CC04846D
27. Kivela H, Salomaki M, Vainikka P, et al. Effect of water on a hydrophobic deep eutectic solvent. J Phys Chem B. 2022;126(2):513–527. doi:10.1021/acs.jpcb.1c08170
28. Zhang C, Li X, Wu X, et al. Polymerizable deep eutectic solvent-gels synthesized in situ under molecular engineering control exhibit excellent adhesion, freeze resistance, as well as stretching and humidity sensing capabilities. J Colloid Interface Sci. 2025;679:245–253. doi:10.1016/j.jcis.2024.10.070
29. Dai Y, Witkamp G-J, Verpoorte R, et al. Tailoring properties of natural deep eutectic solvents with water to facilitate their applications. Food Chem. 2015;187:14–19. doi:10.1016/j.foodchem.2015.03.123
30. González CG, Mustafa NR, Wilson EG, et al. Application of natural deep eutectic solvents for the “green” extraction of vanillin from vanilla pods. Flavour Fragr J. 2018;33(1):91–96. doi:10.1002/ffj.3425
31. Zhang X, Zhu P, Li Q, et al. Recent advances in the catalytic conversion of biomass to furfural in deep eutectic solvents. Front Chem. 2022;10:911674. doi:10.3389/fchem.2022.911674
32. Negi T, Kumar A, Sharma SK, et al. Deep eutectic solvents: preparation, properties, and food applications. Heliyon. 2024;10(7):e28784. doi:10.1016/j.heliyon.2024.e28784
33. Trombino S, Siciliano C, Procopio D, et al. Deep eutectic solvents for improving the solubilization and delivery of dapsone. Pharmaceutics. 2022;14(2):333. doi:10.3390/pharmaceutics14020333
34. Kumar AK, Parikh BS, Pravakar M. Natural deep eutectic solvent mediated pretreatment of rice straw: bioanalytical characterization of lignin extract and enzymatic hydrolysis of pretreated biomass residue. Environ Sci Pollut Res. 2016;23(10):9265–9275. doi:10.1007/s11356-015-4780-4
35. Jablonsky M, Majova V, Ondrigova K, et al. Preparation and characterization of physicochemical properties and application of novel ternary deep eutectic solvents. Cellulose. 2019;26(5):3031–3045. doi:10.1007/s10570-019-02322-2
36. Hayyan A, Mjalli FS, AlNashef IM, et al. Glucose-based deep eutectic solvents: physical properties. J Mol Liq. 2013;178:137–141. doi:10.1016/j.molliq.2012.11.025
37. Thiruvoth FM, Mohapatra DP, Kumar D, et al. Current concepts in the physiology of adult wound healing. Plast Aesthet Res. 2015;2(5):250–256. doi:10.4103/2347-9264.158851
38. Broughton G, Janis JE, Attinger CE. The basic science of wound healing. Plast Reconstr Surg. 2006;117(7S):12S–34S. doi:10.1097/01.prs.0000225430.42531.c2
39. Strodtbeck F. Physiology of wound healing. Newborn Infant Nurs Rev. 2001;1(1):43–52. doi:10.1053/nbin.2001.23176
40. Bowers S, Franco E. Chronic wounds: evaluation and management. Am Fam Physician. 2020;101(3):159–166.
41. Theoret C. Physiology of wound healing. In: Theoret C, Schumacher J, editors. Equine Wound Management.
42. Ellis S, Lin EJ, Tartar D. Immunology of wound healing. Curr Dermatol Rep. 2018;7(4):350–358. doi:10.1007/s13671-018-0234-9
43. Gonzalez A, Costa TF, Andrade Z, et al. Wound healing - a literature review. An Bras Dermatol. 2016;91(5):614–620. doi:10.1590/abd1806-4841.20164741
44. Gill SE, Parks WC. Metalloproteinases and their inhibitors: regulators of wound healing. Int J Biochem Cell Biol. 2008;40(6–7):1334–1347. doi:10.1016/j.biocel.2007.10.024
45. Izadi K, Ganchi P. Chronic wounds. Clin Plast Surg. 2005;32(2):209–222. doi:10.1016/j.cps.2004.11.011
46. Kathawala MH, Ng WL, Liu D, et al. Healing of chronic wounds: an update of recent developments and future possibilities. Tissue Eng Part B Rev. 2019;25(5):429–444. doi:10.1089/ten.teb.2019.0019
47. Tan MLL, Chin JS, Madden L, et al. Challenges faced in developing an ideal chronic wound model. Expert Opin Drug Discov. 2023;18(1):99–114. doi:10.1080/17460441.2023.2158809
48. Schreml S, Szeimies RM, Prantl L, et al. Oxygen in acute and chronic wound healing. Br J Dermatol. 2010;163(2):257–268. doi:10.1111/j.1365-2133.2010.09804.x
49. Bennison LR, Miller CN, Summers RJ, et al. The pH of wounds during healing and infection: a descriptive literature review. Wound Pract Res J Aust Wound Manag Assoc. 2017;25(2):63–69.
50. Liu HY, Prentice EL, Webber MA. Mechanisms of antimicrobial resistance in biofilms. Npj Antimicrob Resis. 2024;2(1):27. doi:10.1038/s44259-024-00046-3
51. Stoodley P, Sauer K, Davies DG, et al. Biofilms as complex differentiated communities. Annu Rev Microbiol. 2002;56(1):187–209. doi:10.1146/annurev.micro.56.012302.160705
52. Brown MB, Martin GP, Jones SA, et al. Dermal and transdermal drug delivery systems: current and future prospects. Drug Deliv. 2006;13(3):175–187. doi:10.1080/10717540500455975
53. Chen L, Lian G, Han L. Use of “bricks and mortar” model to predict transdermal permeation: model development and initial validation. Ind Eng Chem Res. 2008;47(17):6465–6472. doi:10.1021/ie701711v
54. Banas K, Banas AM, Pastorin G, et al. Sensing the changes in stratum corneum using Fourier transform infrared microspectroscopy and hyperspectral data processing. Sensors. 2024;24(21):7054. doi:10.3390/s24217054
55. Elias PM. Structure and function of the stratum corneum permeability barrier. Drug Dev Res. 1988;13(2‐3):97–105. doi:10.1002/ddr.430130203
56. Jing B, Lan N, Qiu J, et al. Interaction of ionic liquids with a lipid bilayer: a biophysical study of ionic liquid cytotoxicity. J Phys Chem B. 2016;120(10):2781–2789. doi:10.1021/acs.jpcb.6b00362
57. Czyrski GS, Qie R, Sparr E, et al. Impact of propylene glycol, menthol: thymol deep eutectic solvent, and their blends on structure and molecular mobility of stratum corneum components. Int J Pharm. 2025;678:125723. doi:10.1016/j.ijpharm.2025.125723
58. Qi QM, Duffy M, Curreri AM, et al. Comparison of ionic liquids and chemical permeation enhancers for transdermal drug delivery. Adv Funct Mater. 2020;30(45):2004257. doi:10.1002/adfm.202004257
59. Sakuragi M, Maeda E, Kusakabe K. Penetration process of a hydrated deep eutectic solvent through the stratum corneum and its application as a protein penetration enhancer. ChemistryOpen. 2020;9(9):953–958. doi:10.1002/open.202000114
60. Boscariol R, Caetano ÉA, Silva EC, et al. Performance of choline geranate deep eutectic solvent as transdermal permeation enhancer: an in vitro skin histological study. Pharmaceutics. 2021;13(4):540. doi:10.3390/pharmaceutics13040540
61. Li B, Xiao T, Guo S, et al. Oxymatrine-fatty acid deep eutectic solvents as novel penetration enhancers for transdermal drug delivery: formation mechanism and enhancing effect. Int J Pharm. 2023;637:122880. doi:10.1016/j.ijpharm.2023.122880
62. Song J-E, Jun S-H, Ryoo J-Y, et al. Formulation of ascorbic acid and betaine-based therapeutic deep eutectic system for enhanced transdermal delivery of ascorbic acid. Pharmaceutics. 2024;16(5):687. doi:10.3390/pharmaceutics16050687
63. Hooshmand SE, Alavioon SI, Mohajer F, et al. Deep eutectic solvents for wound healing: a leading-edge trajectory. J Drug Deliv Sci Technol. 2025;111:107129. doi:10.1016/j.jddst.2025.107129
64. Asma ST, Imre K, Morar A, et al. An overview of biofilm formation–combating strategies and mechanisms of action of antibiofilm agents. Life. 2022;12(8):1110. doi:10.3390/life12081110
65. Percival SL, Mayer D, Malone M, et al. Surfactants and their role in wound cleansing and biofilm management. J Wound Care. 2017;26(11):680–690. doi:10.12968/jowc.2017.26.11.680
66. Lei J, Sun L, Huang S, et al. The antimicrobial peptides and their potential clinical applications. Am J Transl Res. 2019;11(7):3919–3931.
67. Thapa RK, Diep DB, Tønnesen HH. Topical antimicrobial peptide formulations for wound healing: current developments and future prospects. Acta Biomater. 2020;103:52–67. doi:10.1016/j.actbio.2019.12.025
68. Sen CK, Roy S, Mathew-Steiner SS, et al. Biofilm management in wound care. Plast Reconstr Surg. 2021;148(2):275e–288e. doi:10.1097/PRS.0000000000008142
69. Goswami AG, Basu S, Banerjee T, et al. Biofilm and wound healing: from bench to bedside. Eur J Med Res. 2023;28(1):157. doi:10.1186/s40001-023-01121-7
70. Darvishi S, Tavakoli S, Kharaziha M, et al. Advances in the sensing and treatment of wound biofilms. Angew Chem Int Ed. 2022;61(13):e202112218. doi:10.1002/anie.202112218
71. Finnegan S, Percival SL. Clinical and antibiofilm efficacy of antimicrobial hydrogels. Adv Wound Care. 2015;4(7):398–406.
72. Ali AA, Al Bostami RD, Al-Othman A. Nanogel-based composites for bacterial antibiofilm activity: advances, challenges, and prospects. RSC Adv. 2024;14(15):10546–10559. doi:10.1039/D4RA00410H
73. Nava-Ocampo MF, Al Fuhaid L, Verpoorte R, et al. Natural deep eutectic solvents as biofilm structural breakers. Water Res. 2021;201:117323. doi:10.1016/j.watres.2021.117323
74. Oliveira F, Silva E, Matias A, et al. Menthol-based deep eutectic systems as antimicrobial and anti-inflammatory agents for wound healing. Eur J Pharm Sci. 2023;182:106368. doi:10.1016/j.ejps.2022.106368
75. Swebocki T, Kocot AM, Cieminska K, et al. Breaking through microbial defenses – organic acid-based deep eutectic solvents as a neoteric strategy in bacterial biofilm, persister, and fungal control. ACS Appl Bio Mater. 2025;8(10):8980–8990.
76. Wikene KO, Bruzell E, Tønnesen HH. Characterization and antimicrobial phototoxicity of curcumin dissolved in natural deep eutectic solvents. Eur J Pharm Sci. 2015;80:26–32. doi:10.1016/j.ejps.2015.09.013
77. Schuh CM, Ezquer F, Mamani S, et al. A natural deep eutectic solvent as an effective material for dual debridement and antibiofilm effects in chronic wound treatment. Int J Pharm. 2024;663:124553. doi:10.1016/j.ijpharm.2024.124553
78. Metcalf DG, Bowler PG. Biofilm delays wound healing: a review of the evidence. Burns Trauma. 2013;1(1):2321–3868. doi:10.4103/2321-3868.113329
79. Bedair HM, Samir TM, Mansour FR. Antibacterial and antifungal activities of natural deep eutectic solvents. Appl Microbiol Biotechnol. 2024;108:198.
80. de Morais P, Goncalves F, Coutinho JAP, et al. Ecotoxicity of cholinium-based deep eutectic solvents. ACS Sustainable Chem Eng. 2015;3(12):3398–3404. doi:10.1021/acssuschemeng.5b01124
81. Correia ECF. Biofilm disinfection with choline-based eutectic solvents [Master dissertation]. Porto, Portugal, The University of Porto; 2022.
82. Shaw ZL, Awad MN, Gharehgozlo S, et al. Deep eutectic solvent eutectogels for delivery of broad-spectrum antimicrobials. ACS Appl Bio Mater. 2024;7(3):1429–1434. doi:10.1021/acsabm.3c00971
83. Silva JM, Carvalho JPF, Teixeira MC, et al. Xylan-chitosan based films with deep eutectic solvents for wound healing applications. Int J Biol Macromol. 2025;320:145482.
84. Yang J-Y, Zhou E-Y, Cheng T-H, et al. Injectable deep eutectic solvent-based ionic gel with rapid gelation and broad hemostatic functionality. Adv Healthcare Mater;2025. e03038. doi:10.1002/adhm.202503038
85. Silva JM, Pereira CV, Mano F, et al. Therapeutic role of deep eutectic solvents based on menthol and saturated fatty acids on wound healing. ACS Appl Bio Mater. 2019;2(10):4346–4355. doi:10.1021/acsabm.9b00598
86. Grønlien KG, Pedersen ME, Tønnesen HH. A natural deep eutectic solvent (NADES) as potential excipient in collagen-based products. Int J Biol Macromol. 2020;156:394–402. doi:10.1016/j.ijbiomac.2020.04.026
87. Wang Y, Zhang Y, Su J, et al. Preparation of a multifunctional wound dressing based on a natural deep eutectic solvent. ACS Sustainable Chem Eng. 2020;8(37):14243–14252. doi:10.1021/acssuschemeng.0c05754
88. Zhang Q, Lin Z, Zhang W, et al. Fabrication of green poly(vinyl alcohol) nanofibers using natural deep eutectic solvent for fast-dissolving drug delivery. RSC Adv. 2021;11:1012–1021.
89. Che Zain MS, Yeoh JX, Lee SY, et al. Integration of choline chloride-based natural deep eutectic solvents and macroporous resin for green production of enriched oil palm flavonoids as natural wound healing agents. Antioxidants. 2021;10(11):1802. doi:10.3390/antiox10111802
90. Li W, Zhao X, Huang T, et al. Preparation of sodium hyaluronate/dopamine/AgNPs hydrogel based on the natural eutetic solvent as an antibaterial wound dressing. Int J Biol Macromol. 2021;191:60–70. doi:10.1016/j.ijbiomac.2021.09.056
91. Bardsley TA, Evans CL, Greene JR, et al. Integration of choline geranate into electrospun protein scaffolds affords antimicrobial activity to biomaterials used for cutaneous wound healing. J Biomed Mater Res B Appl Biomater. 2021;109(9):1271–1282. doi:10.1002/jbm.b.34788
92. Zhu J, Li X, Wu X, et al. Nanocomposite of Ag nanoparticles and deep eutectic solvent-derived carbon dots with oxidase mimicking activity as synergistic bactericidal agent. Lett Appl Microbiol. 2022;74(5):684–694. doi:10.1111/lam.13654
93. Zhu G, Zhang J, Huang J, et al. Self-healing, antibacterial, and 3D-printable polymerizable deep eutectic solvents derived from tannic acid. ACS Sustainable Chem Eng. 2022;10(24):7954–7964. doi:10.1021/acssuschemeng.2c01328
94. Alkhawaja B, Al-Akayleh F, Al-Khateeb A, et al. Deep eutectic liquids as a topical vehicle for tadalafil: characterisation and potential wound healing and antimicrobial activity. Molecules. 2023;28(5):2402.
95. Sulthan R, Sambhudevan S, Greeshma S, et al. Extraction of β-chitin using deep eutectic solvents for biomedical applications. Mater Today Proc. 2023;94:44–48. doi:10.1016/j.matpr.2023.05.521
96. Shah SWH, Imran F, Ahmad HS, et al. Allantoin eutectics with choline chloride and zinc chloride: interactions and wound healing applications. J Taibah Univ Sci. 2023;17(1):2208727. doi:10.1080/16583655.2023.2208727
97. Li B, Zhou M, Xu X, et al. Preparation and properties of β-CD/P(AM-co-AA) composite hydrogel by frontal polymerization of ternary deep eutectic solvent. Polym Int. 2023;72(7):664–670. doi:10.1002/pi.6523
98. Sun X, Yu J, Wei Q, et al. Construction of chitosan-based supramolecular biofilm material for wound dressing based on natural deep eutectic solvents. Int J Biol Macromol. 2023;236:123768. doi:10.1016/j.ijbiomac.2023.123768
99. Sun X, Yang Y, Yu J, et al. Chitosan-based supramolecular aerogel with “skeletal structure” constructed in natural deep eutectic solvents for medical dressings. Int J Biol Macromol. 2024;254:127720. doi:10.1016/j.ijbiomac.2023.127720
100. Huang T, Zhang Y, Zhao L, et al. Sodium hyaluronate hydrogel for wound healing and human health monitoring based on deep eutectic solvent. Int J Biol Macromol. 2024;257:128801. doi:10.1016/j.ijbiomac.2023.128801
101. Parsana N, Seoud OE, Al-Ghamdi A, et al. Deep eutectic solvent and poly (vinyl alcohol) based self-healable, injectable and adhesive “eutectogel”: an emerging drug delivery vehicle. ChemistrySelect. 2024;9(1):e202304157. doi:10.1002/slct.202304157
102. Liu Y, Wang D, Lai Y, et al. Deep eutectic solvents for essential-oil delivery and bacterial-infected wound healing. Langmuir. 2024;40(45):23766–23779. doi:10.1021/acs.langmuir.4c02736
103. Tian Y, Jiang F, Xie H, et al. Conductive hyaluronic acid/deep eutectic solvent composite hydrogel as a wound dressing for promoting skin burn healing under electrical stimulation. Adv Healthcare Mater. 2024;13(17):2304117. doi:10.1002/adhm.202304117
104. Vakili S, Mohamadnia Z, Ahmadi E. Self-healing, electrically conductive, antibacterial, and adhesive eutectogel containing polymerizable deep eutectic solvent for human motion sensing and wound healing. Biomacromolecules. 2024;25(12):7704–7722. doi:10.1021/acs.biomac.4c00960
105. Yusakul G, Jomrit J, Bacabac RG, et al. 3D printed personalized wound dressings using a hydrophobic deep eutectic solvent (HDES)-formulated emulgel. RSC Adv. 2024;14(46):34175–34191. doi:10.1039/D4RA05456C
106. Liu S, Zhan J, Liu Z, et al. Versatile poly (deep eutectic solvents) electroactive chitosan eutectogel for infected wound healing and monitoring administration. Carbohydr Polym. 2025;352:123192. doi:10.1016/j.carbpol.2024.123192
107. Zhou R, Zhang W, Wu J, et al. Polyvinyl alcohol/chitosan hydrogel based on deep eutectic solvent for promoting methicillin-resistant Staphylococcus aureus-infected wound healing. Int J Biol Macromol. 2025;297:139916. doi:10.1016/j.ijbiomac.2025.139916
108. Ren R-Y, Zhao T-G, Li L-X, et al. Immunomodulatory all-natural kelp decellularized scaffold prepared using deep eutectic solvent with angiogenic properties for accelerating diabetic wound healing. ACS Biomater Sci Eng. 2025;11(4):2306–2320. doi:10.1021/acsbiomaterials.4c02420
109. Shanmugapriya K, Kang HW. Natural deep eutectic solvents (NADES)-based chitosan hydrogel for enhanced photoimmunomodulation treatment on various wounds. Int J Biol Macromol. 2025;321:146591. doi:10.1016/j.ijbiomac.2025.146591
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Vibration Therapy for Hard-to-Heal Wounds in Clinical Study: A Scoping Review
Haba D, Itabashi M, Tamai N, Tobe H, Sanada H, Nakagami G
Chronic Wound Care Management and Research 2024, 11:1-12
Published Date: 3 February 2024
Effects of Oral Cholecalciferol on Chronic Wound Healing in Patients with Vitamin D Insufficiency or Deficiency
Zhao H, Wu X, Li H, Lan Y
Journal of Multidisciplinary Healthcare 2025, 18:6887-6900
Published Date: 24 October 2025