Back to Journals » Journal of Pain Research » Volume 14
Decreased Opioid Consumption and Durable Pain Relief in Patients Treated with 10 kHz SCS: A Retrospective Analysis of Outcomes from Single-Center
Authors Feng H, Doherty P, Rotte A ![]()
Received 29 March 2021
Accepted for publication 30 June 2021
Published 24 August 2021 Volume 2021:14 Pages 2593—2600
DOI https://doi.org/10.2147/JPR.S312932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Honghui Feng,1 Patrick Doherty,1 Anand Rotte2
1Lawrence and Memorial Hospital, Yale New Haven Healthcare, New London, CT, USA; 2Nevro Corp., Redwood City, CA, USA
Correspondence: Honghui Feng Email [email protected]
Background: Chronic pain is frequently treated with opioid analgesics, but there is limited evidence for efficacy for chronic use of opioids and the drugs pose significant risks to patients’ physical and mental health. Spinal cord stimulation delivered at a frequency of 10,000 Hertz (10 kHz SCS) is a minimally invasive therapy with demonstrated efficacy and safety in treating chronic pain that has also been associated with decreased opioid use.
Objective: To evaluate opioid reduction and pain relief in real-world cohort.
Study Design: Retrospective review.
Setting: Single center.
Patients and Methods: Consecutive patients who were implanted with 10 kHz SCS devices from December 1, 2015, to June 30, 2020 for the treatment of chronic pain in the trunk or lower limbs were included. Changes in opioid use following 10 kHz SCS treatment were extracted from electronic medical records, and patient-reported pain relief, improvement in function and sleep were extracted from manufacturer’s database. Responder rate was defined as the proportion of patients with at least 50% pain relief. Anonymised results from descriptive analysis of the data are reported.
Results: At last follow-up (median 21.4 months), mean daily opioid dose fell by 48.4 morphine milligram equivalents (MME), and fewer patients used opioids. Mean pain relief in these patients was 57% ± 4%, and responder rate was 68% at last recorded follow-up. Interestingly, pain relief (66%) and responder rate (86%) were higher in patients with 1 year or more. Finally, 50% of patients reported improved sleep, and 73% reported improvement in function at last recorded follow-up after treatment with 10 kHz SCS.
Conclusion: These results support 10 kHz SCS as a safe and effective treatment of chronic pain in real-world patients with secondary benefits to opioid consumption and measures of patients’ quality of life.
Keywords: spinal cord stimulation, chronic pain, opioid analgesics, failed back surgery syndrome
Introduction
Chronic pain was estimated to affect 50 million Americans in 2016, or about 20% of the adult population,1 and opioid analgesics are often used to treat cases of chronic pain not adequately controlled by non-steroidal anti-inflammatory drugs (NSAIDS).2 However, the ongoing opioid epidemic has created urgency around meeting the need for safe and effective chronic pain relief.3 In addition, the Centers for Disease Control and Prevention (CDC) issued a guideline in 2016 that discourages the use of opioid analgesics in cases of nonterminal, noncancer chronic pain, instead recommending nonopioid therapies wherever possible and using the lowest effective dose possible when required.4 Spinal cord stimulation (SCS) is a minimally invasive form of neuromodulation used since the 1980s for treating chronic pain in which the pain is reduced by spinal stimulation using epidural electrodes and an implantable pulse generator (IPG).5
High-frequency SCS delivered at a frequency of 10,000 Hz (10 kHz SCS) produces paresthesia-free pain relief and has been shown to be superior to conventional SCS in reducing chronic low back and leg pain in SENZA-RCT, a pivotal randomized controlled study.6 The results of SENZA-RCT and other prospective studies7–9 have established 10 kHz SCS as a safe and effective therapy for the treatment of chronic pain, particularly low back and leg pain.
Data from these trials also show that the use of 10 kHz SCS for treating chronic pain is associated with reduced opioid consumption, and that this reduction is observed in patients on high-dose opioids at baseline, in addition to those taking lower initial doses.10 These results suggest that the use of 10 kHz SCS could have a doubly beneficial impact in cases of chronic, intractable pain by both reducing both pain levels and opioid use. However, it is unclear whether these results are generalizable to real-world patients who were not treated under the carefully controlled circumstances of a prospective trial. This retrospective study of real-world patients treated at a single institution was conducted to evaluate the effects of 10 kHz SCS treatment for chronic, intractable pain on opioid consumption and pain levels.
Materials and Methods
This real-world, single-center, retrospective study was conducted using data derived from electronic medical records (EMR) for patients who were permanently implanted with a 10 kHz SCS device (Nevro Corp., Redwood City, Ca) to treat chronic pain in the trunk and/or limbs from December 1, 2015, to June 30, 2020, at Lawrence and Memorial Hospital, Yale New Haven Healthcare (New London, Ct, USA). As the study was retrospective and involved analyzing privately collected, observational information (non-interventional) for an on-label indication; did not involve re-identifying patients and reaching out to patients for additional information; did not generate identifiable results and also because of the secondary nature of the research, 45 CFR part 46 regulating human research was considered not applicable and the study was considered exempt under 45 CFR part 46104 (d) 4.11
Procedures
Trial stimulation and implant procedures have been previously described.12 Briefly, patients were implanted with octapolar leads in the epidural space based on the region affected by pain in each patient, including leads spanning T8 to T12 vertebral levels in patients with lower back and lower limb pain. Patients first underwent a trial stimulation for up to 7–14 days, and those who had pain relief of 50% or more by the end of the trial period were defined as responders and were eligible to receive a permanently implanted device. Stimulation was delivered at a frequency of 10 kHz, pulse width of 30 μs, and amplitudes adjusted to maximize the patient’s pain relief. Optimized therapy was achieved using standard programming strategies based on patient-reported pain relief, including a pulse dosing program.
Follow-Up
In addition to the standard of care clinical follow-ups, patient management pre- and post-implantation included the support of a local clinical specialist under the guidance of a pain physician.13 Clinical specialist was mainly responsible for the assessment of therapy effectiveness at each clinic visit through a series of structured questions and assisted in carrying out therapy optimization, as necessary. Patients were contacted by telephone if patients were not able to attend regular follow-up visits after permanent implant. Based on patient-reported pain relief, standard programming strategies including an electrode bipole search to determine the optimal stimulation site within the vertebral column were followed. Typically, thoracic vertebral levels 9 and 10 were considered as sweet spots. If needed, additional therapy optimization tools such as more complex electrode combinations, pulse trains and amplitude settings were employed to achieve satisfactory pain relief. Data collected were routinely entered to the global database.
Assessments
Opioid dosage data at baseline and last follow-up visit were obtained from an EMR database associated with the site of treatment. The device manufacturer’s commercial, real-world database (HFXCloudTM) was used to obtain patients’ demographic information and pain relief at the end of the trial stimulation (EoT) and at the last follow-up visit. Pain intensity at the baseline and end of the trial was assessed using the 11-point verbal rating scale (VRS) where 0 = no pain and 10 = worst possible pain. Pain relief was assessed using a patient-reported percentage pain relief (0% = no pain relief, 100% = complete pain relief). Response to therapy was defined as at least 50% pain relief reported by patients on 0–100% scale. Sleep and function improvements were assessed as “yes” or “no”. Program used for therapy was recorded as “pulse dosing”, “MAPS/Bipole interlacing”, “therapy optimization” and “no details”. Data from the last recorded visit were extracted from the respective databases and used for analyses. In addition, therapy-related complaints were collected from the complaints database of the manufacturer, and the respective rate was analyzed.
Analysis
All outcomes were analyzed using descriptive statistics. Continuous variables are reported descriptively, and median ± standard deviation values are reported, where appropriate. Counts and percentages are reported for categorical variables.
Results
Patient Characteristics
A total of 41 patients were identified who were implanted with a 10 kHz SCS device for chronic pain during the time period of interest and whose EMR data included opioid usage at baseline, as shown in Figure 1. Demographic information, pain outcomes, and other relevant data were available in the manufacturer’s database for 40 of the implanted patients. Because this study used data from real-world databases, not all outcomes were available at all timepoints for all patients. All 40 patients had baseline data, while data at the end of the trial stimulation period were available for 37 of the 40 patients, and, the same number (37) had data available for last-visit assessments of pain relief.
 |
Figure 1 Number of patient records available for analysis. Electronic medical records including data on opioid use were available for 41 patients who were implanted with a 10 kHz SCS device for treating pain during the study period. The analysis included records for 40 of these patients with available demographic data in the NevroCloud database. Pain relief at the end of the trial stimulation (EoT) was available for 37 patients, and data for pain relief, opioid use, sleep quality, and functioning at the last visit were available for 37 patients. *Outcomes and demographics were not available for 1 patient in manufacturer database. |
The baseline clinical characteristics of the 40 patients included in this analysis are summarized in Table 1. Over 80% of the patients in this sample reported chronic pain predominantly in the lower back or legs, and 80% had previous spine surgery. The median follow-up interval in these patients was 14.3 ± 14.1 months, and 60% of the patients had follow-up times of 1 year or more. A pulse dosing program was used to optimize pain relief in 7 (17.5%) patients, and none of the patients used other optimization programs, such as MAPS/bipole.
 |
Table 1 Clinical Characteristics of Patients at Baseline |
Opioid Consumption
The distribution of opioid use among the patients in this study is shown in Figure 2A. At baseline, patients reported a relatively wide-spread use of opioid consumption, including 34% who were taking opioids at doses between 1 and 49 MME, 12% who were taking between 50 and 90 MME and 16% who were taking more than 90 MME daily. At the last recorded visit following 10 kHz SCS treatment, the distribution of opioid use shifted, with the proportion of patients taking no opioids increasing to over 60%, while the proportion of patients using opioids at all dose levels decreased, including those taking more than 90 MME daily. The median follow-up interval for opioid dosage data for the 41 patients from the EMR database was 21.4 months and ranged from 0.9 months to 55.7 months. Mean daily opioid intake decreased by 58% from 83.7 ± 23.1 MME at baseline to 35.5 ± 9.4 MME at their last visit (Figure 2B). Out of the 8 patients taking opioids at doses above 90 MME/day at baseline, 5 patients reduced their dose and 3 patients had no change; consequently, mean opioid dose in this subset of patients decreased by 54% from 253.5 ± 61.0 MME at baseline to 117.4 ± 9.8 MME.
 |
Figure 2 Change in opioid use during the study period. (A) The distribution of patients in 4 categories of daily opioid dose in morphine milligram equivalents (MME) at baseline and at the last follow-up visit. (B) The mean daily opioid dose in MME for all patients at baseline and at the last follow-up visit. |
Pain Relief
The percentage pain relief reported by individual patients following the trial stimulation and at the last visit is shown in Figure 3A and B. The baseline responder rate was 100% by definition because only patients who were responders following the trial stimulation period were eligible for inclusion in this study, and pain relief ranged from 50% to 100%. Both the responder rate and mean pain relief were well maintained in these patients until their last recorded follow-up visits after a median treatment interval 14.3 ± 14.1 months. Pain relief with 10 kHz SCS was sustained and durable as seen by the higher mean pain relief (66%; Figure 3C) and responder rate (86%; Figure 3D) in patients with at least 12 months of follow-up.
 |
Figure 3 Pain relief. (A) Tornado plot of patient-reported pain relief at the end of the trial stimulation (EoT; N=37). Data for patients who failed the trial was not available. (B) Tornado plot of patient-reported pain relief at the last follow-up visit (N=37). (C) Mean pain relief values at the last follow-up visit in all patients (N=37) and those with 12 months or more (n=21). (D) Responder rates at the last follow-up visit in all patients (N=37) and those with 12 months or more (n=21). |
Quality-of-Life Outcomes
Sleep and function improvement assessments from the last recorded follow-up visit are summarized in Figure 4. Following 10 kHz SCS treatment, half of the patients indicated that their sleep had improved, while 73% reported improvement in functioning at the last recorded follow-up.
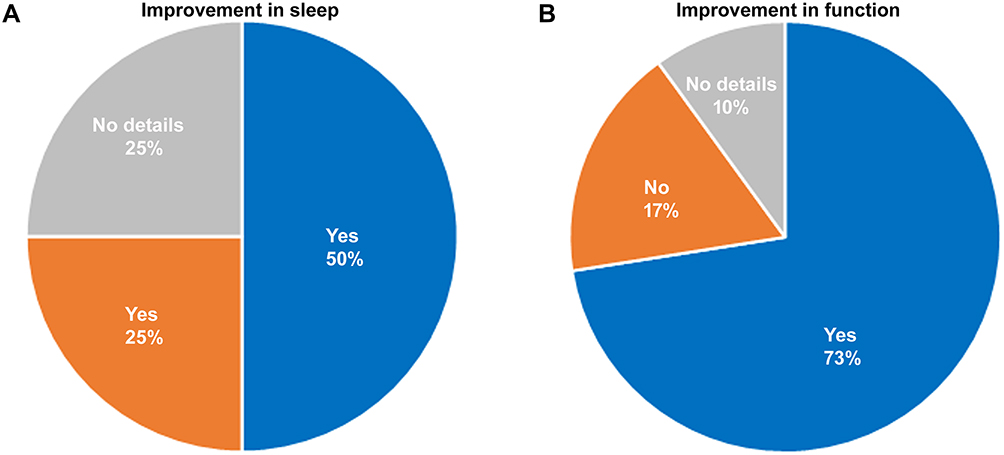 |
Figure 4 Improvement in sleep and patient function (N=40). (A) Proportion of patients reporting improvement in sleep or not at last follow-up. (B) Proportion of patients reporting improvement in functioning or not at last follow-up. |
Therapy-Related Complaints
As listed in Table 2, therapy-related complaints or events were reported in 8 (19.5%) patients at the time of data analysis (February 2021), and all complaints were resolved without sequelae. One patient (2.4%) with infection required explant of the device, whereas other infections were managed with antibiotics. Three patients reported insufficient pain relief or required additional pain relief and were satisfied with programming changes.
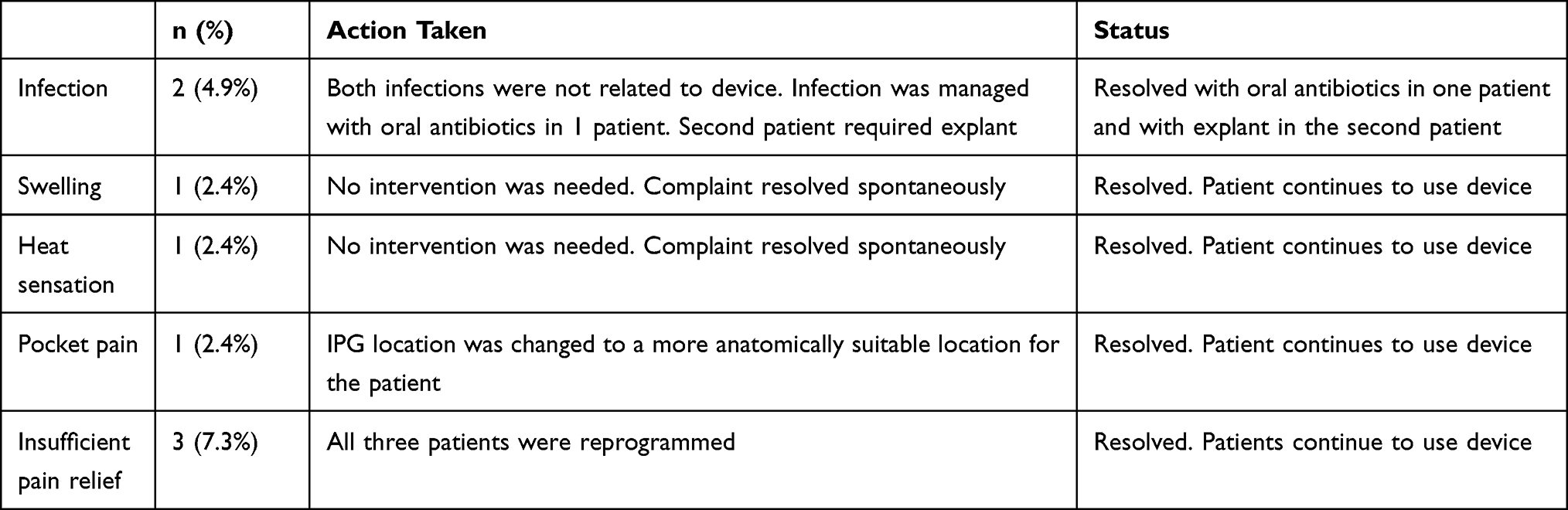 |
Table 2 Therapy Related Events Reported by Patients |
Discussion
The results of this analysis of real-world data from a single treatment center show 10 kHz SCS is associated with reduced consumption of opioid analgesics and pain relief, and these benefits are both substantial and durable. The correlation between 10 kHz SCS and reduced opioid consumption has been reported in many prospective and retrospective studies evaluating this technology14 including the SENZA-RCT study, which reported a 19% decrease in average daily opioid consumption in study subjects treated with 10 kHz SCS for 12 months.6 Results from other recent prospective trials of 10 kHz SCS in patients with back and leg pain also showed reductions from 41% to 64% in average daily opioid dose and increased abstinence among study subjects after 12 months of treatment.7,8,10,15 Retrospective studies of real-world patients likewise showed increased rates of opioid abstinence and declines in opioid daily doses, ranging from 28% to 40%.16–18
The degree to which the association between 10 kHz SCS and decreased opioid use holds true in different patient populations has important implications for chronic pain treatment in the context of the ongoing opioid crisis. Many real-world patients with chronic pain have already been prescribed opioid analgesics with little benefit by the time they are evaluated for treatment with SCS. Therefore, a treatment that both reduces pain in patients taking opioids and the consumption of these drugs would be of particular benefit to treating chronic pain. The proportion of patients in the current study who did not use opioids was nearly 2.5-fold higher after stimulation, and the number of patients using opioids at all dose levels declined, including those taking daily doses of more than 90 MME. Likewise, the mean daily dose of all patients in the study declined by more than half by the final visit. The results found in this sample of real-world patients is comparable to past results in prospective and retrospective studies and further supports the generalizability of the association of 10 kHz stimulation and reduced opioid consumption.6–8,14–18
In addition, reduced opioid consumption was seen in patients at all baseline opioid consumption levels in the present study, which suggests this benefit is applicable to patients taking opioids at a wide range of doses. It is also notable that neither the current study nor any of the previously cited studies of 10 kHz SCS involved direct efforts to reduce opioid consumption.6–8,14–18 Opioid reduction has also been reported with conventional SCS in multiple studies including prospective, retrospective and post hoc settings.19–24 Studies showed a significantly higher percentage of patients with SCS implants reported reduced dependence on opioids for pain management. Interestingly, SCS patients who reduced or stopped their opioid use were shown to achieve better pain relief and functional outcomes compared to patients who continued to use opioids.22
Taken together, data from the current study and previous studies demonstrate the possibility of reduced dependence on opioids for pain management and emphasize encouraging addition of protocols for reducing opioid consumption in chronic pain patients treated with 10 kHz SCS or conventional SCS. A recent pilot study proposed a standardized protocol for elimination of opioids prior to neuromodulation therapy and concluded that the protocol was feasible in clinical practice.25 Data suggest that active encouragement for reducing opioids may result in even greater reductions in opioid use, a valuable outcome in the context of the current opioid crisis in the US.3
Pain relief from 10 kHz SCS was also comparable between our real-world sample and previously published results.6–8,13,15 The SENZA-RCT investigators reported a 79% response rate and 67% reduction in mean back pain after 12 of 10 kHz stimulation.6 Recent prospective trials of 10 kHz SCS have, likewise, reported back pain reductions from 54% to 73% after 12 months of treatment and responder rates of 90%.7,8,15 The retrospective real-world review by Stauss et al13 also reported a decrease in back and lower limb pain intensity of 63% following 12 months of treatment with 10 kHz SCS, further validating the level of pain relief found in the current study. Patients in the current study had a responder rate of 68% at the last recorded visit. It is of particular interest that the responder rate and mean pain relief were higher in patients with more than 12 months of stimulation. This result supports the durability of 10 kHz SCS and may also reflect a better understanding of the program required to achieve optimal pain relief among patients treated for longer periods. However, this study was not designed to examine the effect of programming on pain relief.
Finally, the quality-of-life outcomes of functioning and sleep quality both improved after treatment with 10 kHz SCS, and it is possible these improvements are the result of increased pain relief, reduced opioid use, or both. Our data showed sleep quality improved in 50% of patients and function improved in 73%. Stauss et al reported sleep improvement in 68% and function improvement in 72% of patients in their real-world review.13 Another real-world analysis in patients treated with 10 kHz SCS for chronic upper limb and neck pain, likewise found improved sleep in 53% and improved function in 72% of patients after being treated for a mean of 19 months.26 Likewise, prospective studies have reported improvements in both sleep and function, although these used different assessments.6,7,15 These results further demonstrate that multiple health domains can be improved by the use of 10 kHz SCS for chronic, intractable pain.
Limitations
The interpretation of these results is limited by the retrospective nature of this study, which may have introduced bias into patient selection. However, all eligible patients from the relevant time period have been included to mitigate the effects of selection bias. This study is also limited by unplanned follow-up times, which result in a heterogeneous data set. Study also could not report granular information on programs used to achieve pain relief. Study also could not consider in the analysis the possible spontaneous reductions in opioid prescriptions by pain physicians due to increased focus on opioid use. Finally, this is a study of outcomes in real-world patients and depends on the data available from the source database, which is maintained by the device manufacturer. The database also lacked granular data for patients’ data on sleep and function. These were reported as binary yes/no answers with no assessment of variables, such as sleep latency and quality or degree of improvement in function. Therefore, the findings from this study should be interpreted with full considerations to the limitations as noted.
Conclusions
These results show that in this patient population, 10 kHz SCS reduces opioid consumption, decreases pain, and improves sleep and functioning. These results are similar to those obtained in controlled and prospective trials with 10 kHz SCS and increase the body of evidence supporting these benefits for real-world patients with chronic pain.
Acknowledgments
Funding was provided to Dr. Erik J. MacLaren of Galen Medical Writing, LLC, in his capacity as a medical writer by Nevro Corp., Redwood City, CA, USA, for the preparation of this manuscript.
Disclosure
Dr Anand Rotte is an employee of Nevro Corp. The authors report no other conflicts of interest in this work.
References
1. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67:1001–1006. doi:10.15585/mmwr.mm6736a2
2. Hylands-White N, Duarte RV, Raphael JH. An overview of treatment approaches for chronic pain management. Rheumatol Int. 2017;37:29–42. doi:10.1007/s00296-016-3481-8
3. Gupta M, Abd-Elsayed A, Knezevic NN. Improving care of chronic pain patients with spinal cord stimulator therapy amidst the opioid epidemic. Neurological Sci. 2020;41(10):2703–2710. doi:10.1007/s10072-020-04435-0
4. Dowell D, Haegerich TM, Chou R. CDC Guideline for prescribing opioids for chronic pain–United States, 2016. JAMA. 2016;315:1624–1645. doi:10.1001/jama.2016.1464
5. Verrills P, Sinclair C, Barnard A. A review of spinal cord stimulation systems for chronic pain. J Pain Res. 2016;9:481–492. doi:10.2147/JPR.S108884
6. Kapural L, Yu C, Doust MW, et al. Novel 10-kHz High-frequency Therapy (HF10 Therapy) Is Superior to Traditional Low-frequency Spinal Cord Stimulation for the Treatment of Chronic Back and Leg Pain: the SENZA-RCT Randomized Controlled Trial. Anesthesiology. 2015;123:851–860. doi:10.1097/ALN.0000000000000774
7. Al-Kaisy A, Palmisani S, Smith TE, et al. 10 kHz high-frequency spinal cord stimulation for chronic axial low back pain in patients with no history of spinal surgery: a preliminary, prospective, open label and proof-of-concept study. Neuromodulation. 2017;20:63–70. doi:10.1111/ner.12563
8. Rapcan R, Mlaka J, Venglarcik M, Vinklerova V, Gajdos M, Illes R. High-frequency - Spinal Cord Stimulation. Bratisl Lek Listy. 2015;116:354–356. doi:10.4149/bll_2015_067
9. Van Buyten JP, Al-Kaisy A, Smet I, Palmisani S, Smith T. High-frequency spinal cord stimulation for the treatment of chronic back pain patients: results of a prospective multicenter European clinical study. Neuromodulation. 2013;16:59–65. doi:10.1111/ner.12006
10. Al-Kaisy A, Van Buyten JP, Carganillo R, et al. 10 kHz SCS therapy for chronic pain, effects on opioid usage: post hoc analysis of data from two prospective studies. Sci Rep. 2019;9:11441. doi:10.1038/s41598-019-47792-3
11. HHS. Human subject regulations decision charts: 2018 requirements; 2018. Availabe from: https://www.hhs.gov/ohrp/regulations-and-policy/decision-charts-2018.
12. Gupta M, Scowcroft J, Kloster D, et al. 10-kHz spinal cord stimulation for chronic postsurgical pain: results from a 12-month prospective, multicenter study. Pain Pract. 2020;20(8):908–918. doi:10.1111/papr.12929
13. Stauss T, El Majdoub F, Sayed D, et al. A multicenter real-world review of 10 kHz SCS outcomes for treatment of chronic trunk and/or limb pain. Ann Clin Transl Neurol. 2019;6:496–507. doi:10.1002/acn3.720
14. Al-Kaisy A, Van Buyten JP, Amirdelfan K, et al. Opioid-sparing effects of 10 kHz spinal cord stimulation: a review of clinical evidence. Ann N Y Acad Sci. 2020;1462:53–64. doi:10.1111/nyas.14236
15. Al-Kaisy A, Van Buyten JP, Smet I, Palmisani S, Pang D, Smith T. Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med. 2014;15:347–354. doi:10.1111/pme.12294
16. DiBenedetto DJ, Wawrzyniak KM, Schatman ME, Kulich RJ, Finkelman M. 10 kHz spinal cord stimulation: a retrospective analysis of real-world data from a community-based, interdisciplinary pain facility. J Pain Res. 2018;11:2929–2941. doi:10.2147/JPR.S188795
17. Salmon J. High-frequency spinal cord stimulation at 10 kHz for widespread pain: a retrospective survey of outcomes from combined cervical and thoracic electrode placements. Postgrad Med. 2019;131:230–238. doi:10.1080/00325481.2019.1587564
18. Wilding R, Barnes S, Chincholkar M, Lalkhen A Spinal cord stimulation at 10 kHz is effective in reducing opioid consumption in patients with chronic pain.
19. Simopoulos T, Sharma S, Wootton RJ, Orhurhu V, Aner M, Gill JS. Discontinuation of chronic opiate therapy after successful spinal cord stimulation is highly dependent upon the Daily Opioid Dose. Pain Pract. 2019;19(8):794–799. doi:10.1111/papr.12807
20. Pollard EM, Lamer TJ, Moeschler SM, et al. The effect of spinal cord stimulation on pain medication reduction in intractable spine and limb pain: a systematic review of randomized controlled trials and meta-analysis. J Pain Res. 2019;12:1311–1324. doi:10.2147/JPR.S186662
21. Dougherty MC, Woodroffe RW, Wilson S, Gilles GT, Howard MA, Carnahan RM. Predictors of reduced opioid use with spinal cord stimulation in patients with chronic opioid use. Neuromodulation. 2019. doi:10.1111/ner.13054
22. Gee L, Smith HC, Ghulam-Jelani Z, et al. Spinal cord stimulation for the treatment of chronic pain reduces opioid use and results in superior clinical outcomes when used without opioids. Neurosurgery. 2019;84:217–226. doi:10.1093/neuros/nyy065
23. Sharan AD, Riley J, Falowski S, et al. Association of Opioid Usage with Spinal Cord Stimulation Outcomes. Pain Med. 2018;19:699–707. doi:10.1093/pm/pnx262
24. Lad SP, Petraglia Iii FW, Kent AR, et al. Longer delay from chronic pain to spinal cord stimulation results in higher healthcare resource utilization. Neuromodulation. 2016;19(5):469–476. doi:10.1111/ner.12389
25. Jerjir A, Goudman L, Van Buyten JP, et al. Detoxification of Neuromodulation eligible patients by a standardized protocol: a retrospective pilot study. Neuromodulation. 2021. doi:10.1111/ner.13384
26. Sayed D, Salmon J, Khan TW, et al. Retrospective Analysis of Real-World Outcomes of 10 kHz SCS in Patients with Upper Limb and Neck Pain. J Pain Res. 2020;13:1441–1448. doi:10.2147/JPR.S257071
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.