Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Decreased Aryl Hydrocarbon Receptor Gene Expression and Polymorphic Variants Association with Increase COPD Risk
Authors Sadr M ![]() , Asgari A
, Asgari A ![]() , Assadiasl S, Mojtahedi H, Abdollahi A, Nicknam MH, Edalatifard M, Soleimanifar N
, Assadiasl S, Mojtahedi H, Abdollahi A, Nicknam MH, Edalatifard M, Soleimanifar N
Received 1 July 2025
Accepted for publication 28 October 2025
Published 30 October 2025 Volume 2025:20 Pages 3545—3557
DOI https://doi.org/10.2147/COPD.S550884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Maryam Sadr,1 Alireza Asgari,2 Sara Assadiasl,1 Hanieh Mojtahedi,1 Alireza Abdollahi,3 Mohammad Hossein Nicknam,1 Maryam Edalatifard,2 Narjes Soleimanifar1
1Molecular Immunology Research Center, Tehran University of Medical Sciences, Tehran, Iran; 2Thoracic Research Center, Tehran University of Medical Sciences, Imam Khomeini Hospital, Tehran, Iran; 3Department of Pathology, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Narjes Soleimanifar, Email [email protected] Maryam Edalatifard, Email [email protected]
Background: The Aryl Hydrocarbon Receptor (AHR) is a ligand-activated transcription factor that regulates gene expression, including those involved in metabolizing xenobiotic chemicals. The association of AHR with the onset and severity of Chronic Obstructive Pulmonary Disease (COPD) has not yet been elucidated. This study aimed to investigate the correlation between two AHR polymorphisms and the expression levels of this gene in COPD patients compared to healthy controls.
Methods: The AHR gene expression level and frequency of two polymorphisms, rs2066853 and rs2074113, were studied in 154 COPD patients and 145 healthy individuals using RT-PCR and AS-PCR methods respectively.
Results: The findings showed a significant difference in the frequencies of G and A, as well as GG and GA genotypes in rs2066853 between patients and healthy controls [G: OR: 0.4, CI: 0.24– 0.67, (p=0.0002); A: OR: 2.44, CI: 1.48– 4.03, (p=0.0002); genotypes GG: OR: 0.37, CI: 0.21– 0.65, (p=0.0002) and GA: OR: 2.42, CI: 1.40– 4.18 (p=0.001)]. Additionally, the GT genotype frequency in the rs2074113 was different between two groups [GT: OR: 0.23, CI: 0.07– 0.72, (p=0.008)]. Moreover, AHR gene expression was significantly lower in COPD patients compared to healthy controls (P=0.03). Noteworthy, individuals with the GA genotype in rs2066853 exhibited lower AHR expression levels than those with the GG genotype.
Conclusion: The presence of allele A and the GA genotype of the rs2066853 polymorphism in the AHR gene is significantly associated with COPD, suggesting a genetic predisposition. Moreover, reduced AHR expression in patients supports its key role in COPD pathogenesis.
Keywords: chronic obstructive pulmonary disease, aryl hydrocarbon receptor, single nucleotide polymorphism, gene expression
Introduction
Chronic obstructive pulmonary disease (COPD), including emphysema and chronic bronchitis, is a chronic inflammatory condition characterized with persistent airflow obstruction, excessive mucus secretion, dilation of distal airways, alveolar destruction, and impaired lung function.1 COPD is currently the third leading cause of death worldwide after ischemic heart disease and stroke, causing 3 million people per year, accounting for approximately 4.72% of all deaths.2 The number of COPD deaths are expected to increase due to the rising prevalence of risk factors such as obesity, air pollution and tobacco smoking.3
Both genetic and environmental factors could be implicated in developing COPD. For example, congenital deficiency of serine protease inhibitors (serpins) like alpha-1-antitrypsin (AAT), as well as smoking and long-term exposure to household and outdoor air pollutants increase the susceptibility for COPD.3 However, none of these risk factors is considered a definite cause of disease; for instance, despite a considerable correlation between smoking and COPD, only 15 to 20% of smokers develop COPD.4 Therefore, it appears that a combination of intrinsic and extrinsic factors predisposes a person to disease.
Aryl hydrocarbon receptor (AHR) is a ligand-dependent transcription factor that regulates responses to exogenous and endogenous risk factors.5 AHR is expressed in the lung tissue and may play a protective role against environmental pollutants, particularly polycyclic aromatic hydrocarbons (PAHs) in engine exhaust fumes and tobacco.6,7 AHR is activated by binding to PAHs, persistent organic pollutants (POPs), and related environmental chemicals to modulate their biological and toxic effects. It has also been found that ambient particulate matter (PM) associated with traffic-related air pollution (TRAP) contains significant amounts of PAHs, which causes AHR activation.8 Evidence suggests that toxic substances are metabolized by enzymes such as cytochrome P450, glutathione s-transferase, epoxide hydrolase, and UDP-glucosyltransferase, all of which are regulated by AHR.9 For instance, it has been shown that AHR and specificity protein 1 (Sp1) are involved in CYP1A1 expression, since AHR binding to the promoter recruits Sp1 to activate CYP1A1 expression.10 Moreover, polycyclic aromatic hydrocarbons and dioxins binding to AHR results in transcriptional activation of CYP1A1, CYP1A2, and CYP1B1; in turn, these enzymes catalyze oxidative detoxification or activation of most ligands.11 An investigation showed that AHR-deleted mice were unable to induce the expression of the cytochrome P450 in response to stimulants.12 Considering the role of AHR in detoxification and chronic inflammation,13 its activating ligands have been studied in pulmonary diseases like asthma.14
The genetic variation of the AHR gene has also been studied in asthma; for instance, AHR-G1661A single nucleotide polymorphism (SNP: rs2066853) causes an arginine to lysine substitution that has been shown to be associated with an increased risk of developing severe disease.15 In addition, experimental studies have shown that AHR inhibits smoking-induced acute lung inflammation in vivo and modulates oxidative stress and cell death pathways in vitro.6 These and other findings suggest an association between AHR expression level and susceptibility to develop COPD in individuals at higher risk of genetic or environmental factors; therefore, we aimed to evaluate two frequent gene polymorphisms of AHR and its expression level in patients with COPD compared to the healthy controls. Establishing any correlation between AHR expression and disease susceptibility or severity might suggest this molecule and its ligands as therapeutic targets in treating COPD patients.
Patients and Methods
Patients
The present study was conducted as a case–control study between April 2023 and January 2024 at Imam Khomeini Hospital in Tehran. COPD patients were diagnosed according to clinical examination, spirometry findings (post-bronchodilator FEV1/FVC < 0.7), and imaging results.1 In accordance with GOLD criteria. Patients with autoimmune disorders, active infections, or chronic lung diseases other than COPD were excluded. All COPD patients enrolled were hospitalized due to acute exacerbation, and peripheral blood samples were obtained on the first or second day of admission, prior to initiation of systemic corticosteroids or antibiotics whenever possible. A total of 154 patients with a mean age of 65.7 ± 11.1 years, including 123 males and 31 females, were recruited. For the control group, 145 healthy individuals with no history of chronic respiratory disease, autoimmune disorders, active infection, or malignancy were included. Demographic and clinical data were collected using a structured questionnaire. All procedures were performed in accordance with the Helsinki Declaration and its amendments, and the study was approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.IKHC.REC.1402.500).
DNA Extraction and Genotyping AHR Allele Frequencies
Genomic DNA was extracted from peripheral blood samples using a commercial DNA extraction kit (SKU: DN983060, ROJE Technologies, Iran) according to the manufacturer’s instructions. Genotyping was performed for two single nucleotide polymorphisms (SNPs) in the Aryl Hydrocarbon Receptor gene: rs2066853 (located in exon 10) and rs2074113 (located in intron 7), based on the GRCh38 reference genome at positions 7:17339486 (G>A) and 7:17334147 (G>T), respectively.
The SNPs AHR rs2066853 and rs2074113 were genotyped using allele-specific PCR (AS-PCR) to determine the alleles and genotypes of each SNP in both patient and healthy control groups. For each SNP, three primers were designed: one common forward primer and two allele-specific reverse primers. The 3′-terminal nucleotide of each reverse primer was designed to match the specific SNP variant, allowing for the discrimination of alleles based on amplification success. Additionally, a primer pair targeting the GAPDH housekeeping gene was included in each PCR reaction as an internal control to confirm the validity of the amplification process. The reaction was performed on a SimpliAmpTM Thermal cycler PCR System (Applied Biosystems by life technology) according to the instructions, in a total volume of 10 μL containing 5 μL of PCR master mix (Red2x Amplicon, USA),10 pmol. L-1 of each primer (pishgam Co., Iran), and 50ng of genomic DNA as a template, overloaded with a drop of mineral oil. The PCR programed as three steps as follows; step1: initial denaturation at 95°C for 1 min, and the step 2 include 3 stages for 40 cycles as denaturation at 95°C for 15 sec, annealing at 57°C for 15 sec, and elongation at 72°C for 15 sec, the last step as program ended with elongation at 72°C for 1 min.
All PCR products were exposed to electrophoresis (Akhtarian horizontal electrophoresis,Iran) on a 2% agarose gel containing DNA safe stain (Sina-Clone®, Iran) and visualized by UV illumination (E-Box, Vx2/20M). Details of the SNPs, including genomic locations and primer sequences used for genotyping, are provided in Tables 1 and 2.
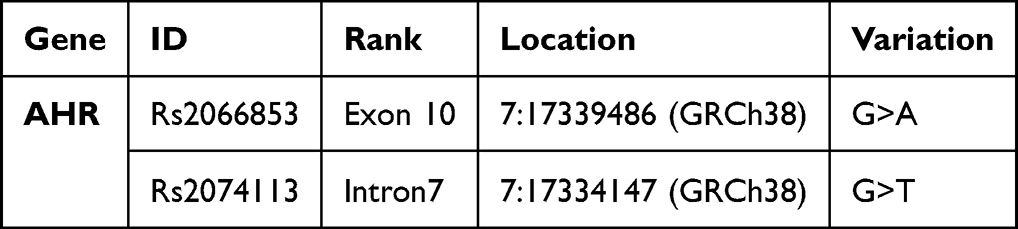 |
Table 1 Information of AHR Gene SNPs |
 |
Table 2 Sequences of Primers and the Product Length |
RNA Extraction and RT-PCR Test
RNA was extracted from whole blood using an extraction kit (SKU: RN983006, ROJE Technologies, Iran). RNAs were reverse translated to cDNA with the kit SKU: EB983021 ROJE Technologies, Iran. RNA concentration and purity were determined using a NanoDrop spectrophotometer. Samples with an A260/A280 ratio between 1.8 and 2.0 and an A260/A230 ratio > 2.0 were used for subsequent analysis. To prevent amplification from genomic DNA, qPCR primers were designed to span exon-exon junctions, which selectively amplifies cDNA. GAPDH gene was used as housekeeping control gene. Forward and reverse primers sequences of RT-PCR test are listed in Table 3.
 |
Table 3 Sequences of 18s rRNA and AHR Primers Used for Gene Expression Analysis |
Each sample was analyzed in duplicate, and non-template controls were included in each run. The amplification efficiency for both the AHR and the housekeeping gene primers was confirmed to be between 99% via a standard curve. The threshold cycle (Ct) values were used for relative quantification using the 2–ΔΔCt method. Samples with a reference gene (GAPDH) Ct value > 30 were excluded from the analysis to ensure data quality.
Statistical Analysis
To examine the frequency of genotypes and alleles and determine their association with COPD, the online software Epi Info 7 was applied. The χ2 and Fisher’s exact tests were used for comparison between groups (SPSS 26.0; SPSS Inc., Chicago, USA). P-values less than 0.05 were considered significant.
Results
Demographic and Clinical Characteristics of Studied Population
One hundred and fifty-four COPD patients were recruited in the study from a single referral center. Healthy controls were selected from a group of healthy volunteers with no clinical history of chronic respiratory diseases. They had no active infection and were not under immunosuppressive or anti-inflammatory treatments. The mean age of the patients and control groups were 65.7 ± 11.1 and 63.9 ± 8.5 years, respectively. Most COPD patients were male (80%) compared to 103 men (71%) and 42 women (29%) in the control group. The mean duration of COPD in the patient group was 5.8 ± 2.8 years. The mean BMI of the patients was 26.7 ± 6.6 and comparable to the control group. Fifty-five patients (35.7%) were smoker, 44 patients (28.6%) had quit smoking, and 52 patients (33.8%) were not active or passive smoker. Forty-eight patients (31.2%) had a history of opioid abuse and twenty-six patients (16.9%) had been working in traditional bread bakeries, constantly exposed to fire smoke. Forty-one patients (26.6%) were under treatment with Inhaled Corticosteroid plus Long-acting beta agonist (ICS-LABA) inhalers and 32 (20.8%) were using Long-acting muscarinic antagonist (LAMA) inhalers (Tables 4 and 5).
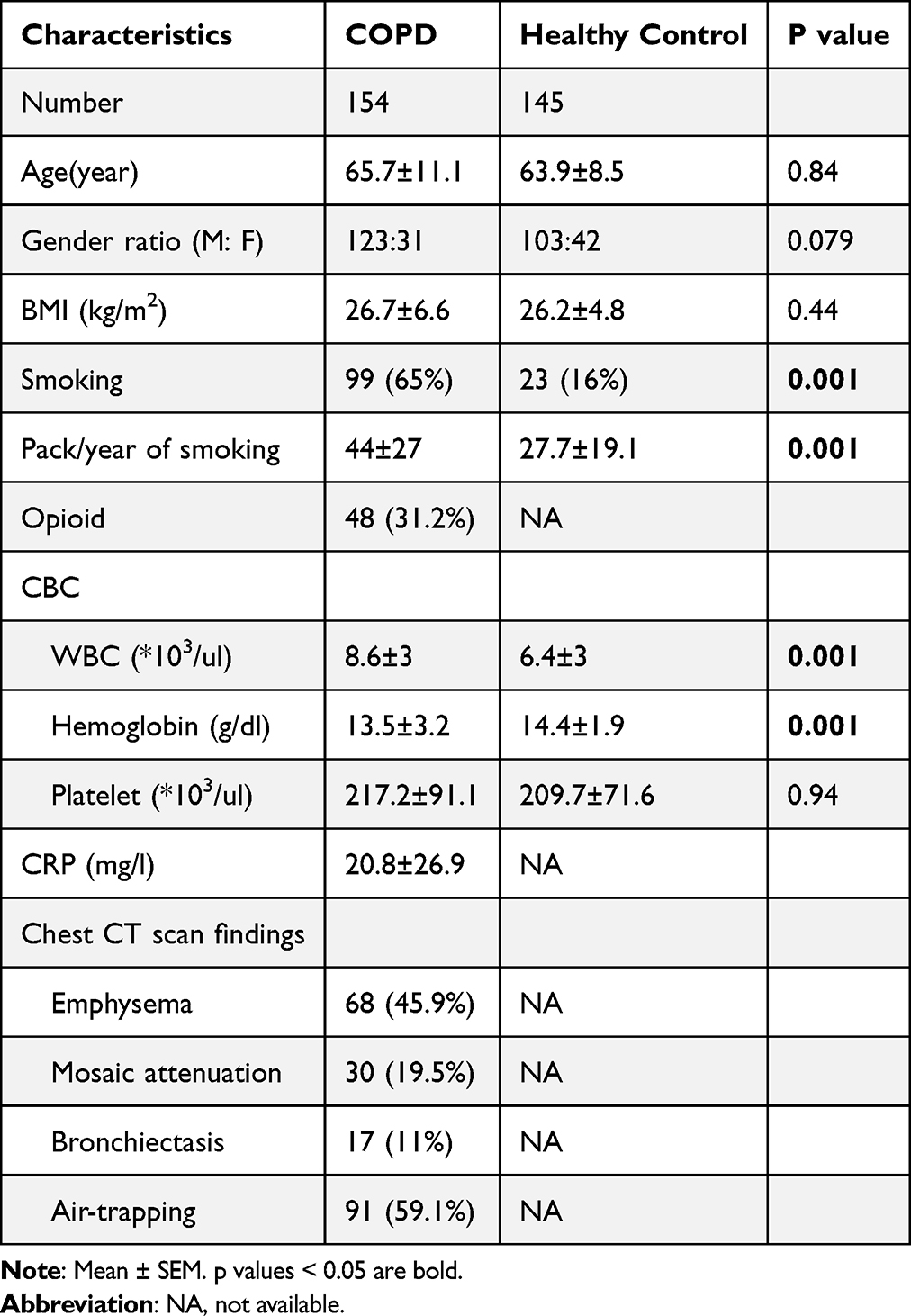 |
Table 4 Clinical and Demographic Characteristics of COPD Patients and Healthy Controls |
 |
Table 5 Baseline Characteristics and Treatment Profile of the COPD Patients |
Comparison of Genetic Polymorphisms Between COPD Patients and Healthy Controls
Polymorphism analysis showed a different frequency of G and A allele as well as GG and GA genotypes in rs2066853 between patient group and healthy controls. The number of individuals with the dominant genotype (GG) in the rs2066853 was significantly lower in the patient group than in the control group [OR: 0.37 (0.21–0.65), P.value: 0.0002]. In contrast, the frequency of GA genotype was significantly higher in the patient group [OR: 2.42 (1.40–4.18), P.value: 0.001] (Table 6 and Figure 1).
 |
Table 6 Genotype and Allele Frequencies of AHR rs2066853 Polymorphism in COPD Patients and Healthy Controls |
 |
Figure 1 Rs2066853 Genotyping Results. Electrophoresis gel showing allele-specific PCR products for rs2066853 in three patients. Patient 1 is homozygous (GG), showing only the G-allele band (334 bp). Patients 2 is heterozygous (GA), displaying bands for G and A allele. GAPDH is included as an internal control (163 bp). A 100 kp ladder is shown for size reference. |
The frequency of heterozygote genotype TG in the rs2074113 was significantly lower frequency in the patient group comparing healthy control group, [OR: 0.23 (0.07–0.72), P.value: 0.008] (Table 7 and Figure 2).
 |
Table 7 Genotype and Allele Frequencies of AHR rs2074113 Polymorphism in COPD Patients and Healthy Controls |
 |
Figure 2 Rs2074113 Genotyping Results. Electrophoresis gel showing allele-specific PCR products for rs2074113 in three patients. Patient 1 is heterozygous (TG), displaying bands for both T and G alleles (258 bp). Patients 2 and 3 are homozygous for the G allele (GG), showing only the G-allele band. GAPDH is included as an internal control (163 bp). A 100 kp ladder is shown for size reference. |
 |
Figure 3 AHR gene expression in COPD and control group. The “*” indicator presented P-value <0.05. |
The A allele of rs2066853 and T allele of rs2074113 are considered recessive or altered alleles in the population; accordingly, the recessive homozygote genotypes AA and TT were present in 1.9% of patients, but in none of healthy individuals.
Gene Expression Differences Between COPD Patients and Healthy Individuals
The gene expression assay was done among 57 patients and 50 healthy controls and the results showed a significant reduced expression of AHR gene in COPD group compared to the control group according to the fold change (2−ΔΔCt) analysis [20.34 ± 5.64 vs 45.46 ± 11.7 (mean ± SEM) (P.value 0.03)] (Figure 3). This suggests a potential role of reduced AHR expression in the pathogenesis or progression of COPD. The reduction may reflect downregulation of detoxification or anti-inflammatory pathways in patients.
Distribution of AHR Gene Expression in COPD Patients Based on rs2066853 Genotypes
A non-significant reduced expression of AHR gene was observed in the GA genotype compared to the GG genotype of rs2066853 [15.8 ± 6.3 vs 43.3 ± 9.5 (mean ± SEM)] in COPD patients. Of note, AHR expression in AA genotype was not detectable, suggesting that the presence of recessive allele A in rs2066853 reduces the expression of AHR gene (Figure 4).
 |
Figure 4 Comparison of AHR gene expression in COPD patients based on rs2066853 genotypes. |
Genotype and Allele Frequencies of AHR rs2066853 in COPD Patients and Healthy Controls
The distribution of genotypes and alleles for the rs2066853 SNP in the AHR gene between COPD patients and healthy individuals. The GG genotype, representing the wild-type allele, was significantly more frequent in the control group than in patients (P < 0.05), suggesting a possible protective role against COPD. Conversely, the GA heterozygote genotype was observed more frequently in the COPD group, indicating a potential association with increased disease susceptibility. Notably, the AA homozygote genotype—representing the recessive allele—was detected only in 1.9% of COPD patients and was completely absent in the control group, implying that the A allele may contribute to disease development, albeit at a low frequency (Figure 5).
 |
Figure 5 Comparison of AHR gene expression in COPD patients and controls based on GG and GA genotypes of rs2066853. |
AHR Gene Expression Trends Across COPD Severity Stages
Regarding disease severity, the patients were categorized into four groups mild, moderate, severe, and very severe subgroups. Of note, the mild subgroup showed the lowest expression level of the AHR gene among four subgroups [6.92 ± 5.57 (mean ± SEM)]; however, in moderate, severe and very severe subgroups, the expression level of AHR gene decreased with increasing disease severity, while a decreasing trend in expression was observed from moderate to very severe subgroups (Figure 6 and Table 8).
 |
Table 8 Statistical Comparison of AHR Gene Expression Levels in Patients Regarding the Severity |
 |
Figure 6 AHR Gene Expression Trends Across COPD Severity Stages. |
Discussion
In this research, we demonstrated that there was significant correlation between AHR polymorphisms and susceptibility to chronic obstructive pulmonary disease. Specifically, the rs2066853 polymorphism revealed that the presence of allele A and GA genotype were associated with an increased risk of COPD and reduced expression of the AHR gene, while the GG genotype had a protective effect. An allele prevalence was markedly higher among patients, conferring a 2.4-fold increased risk increase for COPD, whereas allele G had a protective effect. Consistent with this, GA genotype carriers had more than a twofold increased risk of developing COPD compared to GG carriers, yet the GG genotype was associated with a risk reduction. Although the AA genotype was observed in only a small subset of patients, but not in controls, its low frequency negated statistical significance; but, the trend points to a probable disease-susceptibility association. These findings strongly support the role of rs2066853 as a potential genetic factor for COPD susceptibility, possibly through its impact on the expression and activity of AHR. Furthermore, in the case of the rs2074113 polymorphism, allele frequencies per se were not significantly disparate across groups, but genotype distributions provided informative findings. The GG genotype was more prevalent in the patients with COPD and was associated with an increased risk of the disease, while the GT genotype was significantly less frequent in patients compared to controls, suggest a strong protective effect. In particular, AHR gene expression was lower in COPD patients compared to healthy controls, and individuals carrying the GA genotype for rs2066853 were more poorly expressed than GG carriers.
The observed correlation of AHR polymorphisms with COPD susceptibility may be due to their potential effect on the AHR protein function. The gene such as rs2066853 can alter the ligand-binding domain or the transcriptional activity of AHR, thereby leading to impaired nuclear translocation, reduced heterodimerization with ARNT, and decreased regulation of target genes involved in xenobiotic metabolism, response to oxidative stress, and inflammation. These alterations could undermine the protective role of AHR in sustaining pulmonary homeostasis and thereby contribute to chronic airway inflammation and tissue injury in COPD. Furthermore, dysregulation of AHR-mediated signaling may influence immune reactions to environmental stimuli and pathogens and thereby further enhance disease progression.
Given the increasing prevalence of consequent to the rising trend of smoking and air pollution, and its high burden on the healthcare system, addressing the cause of the disease as well as finding new preventive and therapeutic solutions has become of interest to researchers.16 So far, many environmental factors have been suggested to trigger and progress COPD; numerous studies, for instance, have identified smoking as the most important risk factor for COPD; however, evidence suggest that only 15 to 20% of smokers develop the disease, while about half of COPD patients have never been active or passive smokers.17 These findings highlight the role of genetic background in the susceptibility to the disease. Among genetic factors that link environmental triggers to intrinsic responses is aryl hydrocarbon receptor. AHR is a ligand-activated transcription factor with a 47.146 KB gene located on chromosome 7.p15.18 Its activation is inhibited with chaperones Hsp90 and XAP but upon ligand binding, AHR is released and translocated to the nucleus, where heterodimerizes with Aryl hydrocarbon receptor nuclear translocator (ARNT) and binds to the DNA.19 Evidence suggests that AHR might play a protective role against environmental damages in lung tissue.6 It might also play a role in protection against infectious pulmonary disease.20,21
Although previous studies have examined the effect of AHR on the incidence and pathogenesis of chronic obstructive pulmonary disease,22–24 no human study had been conducted to determine the frequency of AHR gene polymorphisms in association with gene expression levels in COPD patients. Accordingly, the present study aimed at understanding the correlation between gene expression level of AHR and developing COPD. Overall findings showed that the mean expression of AHR genes in the COPD group was significantly lower than in the control group. Moreover, a comparison between four subgroups of disease severity demonstrated a decreasing trend of AHR expression with increasing disease severity. Noteworthy, the AHR expression level in the patients with mild disease was lower than other subgroups, which might be due to the small number of patients in this subgroup.
In addition, two SNPs in the AHR gene—rs2066853 (G>A) and rs2074113 (G>T)—were investigated in COPD patients and healthy individuals. The A and T alleles were considered the recessive alleles in the studied population. Notably, 1.9% of COPD patients had homozygous AA or TT genotypes, which were completely absent in the healthy control group. Furthermore, the dominant GG genotype of rs2066853 was significantly less frequent in patients than in controls, whereas the GA heterozygous genotype was more common among patients.
Interestingly, a previous study on asthmatic patients reported a protective role for the A allele of rs2066853, particularly in those with mild asthma symptoms.9 This finding stands in contrast to our results, where the presence of the A allele (in the form of GA or AA) appeared to be more associated with COPD. Moreover, that same asthma study also indicated that individuals carrying this polymorphism may be at increased risk for severe asthma, suggesting a complex, possibly dual role of this SNP depending on disease context.
This discrepancy may stem from fundamental differences in the pathophysiological mechanisms of asthma and COPD. While asthma is primarily driven by immune hypersensitivity and allergic inflammation, COPD is more strongly influenced by chronic exposure to environmental toxins, especially cigarette smoke, which is known to activate the AHR signaling pathway [Ref]. Therefore, the functional consequences of the same polymorphism may differ in diseases with distinct environmental and immunological etiologies.
In the next step, the correlation between the AHR gene polymorphisms and expression levels was evaluated; the results showed that recessive allele of rs2066853 in the exon region had significantly lower gene expression. This correlation was observed in both the patients and healthy. Therefore, the presence of a recessive allele might make an individual susceptible to COPD by impairing AHR gene expression. However, it should be noted that gene expression level is not exclusively affected by a single polymorphism, and other genetic variations, eg epigenetics, as well as environmental factors, may be involved in gene expression that were not evaluated in the present study. It is also worth noting that gene polymorphisms do not necessarily act by reducing mRNA expression, and they might cause structural modifications that influence the protein product’s function. A previous study has demonstrated that A>G (rs2066853) SNP substitutes arginine with lysine in the AHR-transactivation domain (TAD) that leads to a change in the protein secondary structure, and maybe ligand binding site.15 Besides, epigenetic variations can affect AHR expression and function as one study showed that smoking can increase the risk of COPD by hypomethylation of the Aryl Hydrocarbon Receptor Repressor (AHRR) gene.24 The environmental factors that could affect AHR gene expression include nutrients and dietary supplements,25 physical factors such as temperature, pH, and light,26 microorganisms eg viruses, bacteria, and protozoa,27 hormones, in particular steroids,28 oxidative stress, and chemical toxins,29 which were not considered in the present study.
In addition, the gene expression levels of the AHR across COPD subgroups are categorized as mild, moderate, severe, and very severe. Interestingly, a decreasing trend of gene expression with increasing disease severity was still noticeable across moderate to severe groups, suggesting a potential relationship between disease progression and impaired signaling of the AHR gene.
The lowest average gene expression in the mild group was unexpected. However, our findings should be interpreted cautiously as the low expression in the mild group can be influenced by the small sample size.
Our significant results from this study have some limitations, such as a small sample size and being conducted in a single center. To confirm these findings, larger multi-center studies are required.
Moreover, it could be helpful to follow-up the patients with certain polymorphisms to evaluate disease progression rate and response to treatment. The protein expression of AHR in the lung was not studied due to the human study and lack of indication for tissue biopsies, which is suggested to be performed in experimental models. We did not adjust for important confounders such as smoking intensity, air pollution exposure, and comorbidities, which might have influenced the results. Finally, the lack of external validation in an independent cohort reduces the robustness of our conclusions. Future multicenter studies with larger sample sizes, adjustment for confounders, and validation across diverse populations are warranted.
Conclusion
Our results demonstrate that the frequency of allele A and the GA genotype of the rs2066853 polymorphism in the AHR gene correlate significantly with COPD, suggesting that this allele is most likely a genetic susceptibility allele. Moreover, the significant reduction in AHR gene expression in the case of COPD patients suggests the extreme contribution of this gene towards pathogenesis. Interestingly but not significantly, those with the GA genotype exhibited reduced levels of AHR expression compared to individuals with the GG genotype, suggesting a possible regulatory effect of this variant on gene expression. In addition, decreased expression of AHR gene in the COPD patient underscores the role of this receptor in protecting the lung tissue against chronic obstructive pulmonary disease. Therefore, AHR and its activating ligands may be considered as therapeutic targets in treating COPD patients. These findings suggest that AHR polymorphisms and patterns of expression underlie susceptibility to COPD and validate the importance of including genetic risk factors in subsequent studies of prevention and clinical management of COPD. Although AhR represents a potential therapeutic target, further research is required to overcome challenges related to gene–environment interactions, variability in genetic backgrounds, and translation of these findings into effective COPD therapies.
Ethical Declaration
The study was approved by the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.IKHC.REC.1402.500).
Funding
The present study was supported by Tehran University of Medical Sciences (grant number: 1402-4-154-70462).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kahnert K, Jörres RA, Behr J, et al. The diagnosis and treatment of COPD and its comorbidities. Dtsch Arztebl Int. 2023;120(25):434. doi:10.3238/arztebl.m2023.027
2. Papaioannou AI, Hillas G, Loukides S, et al. Mortality prevention as the centre of COPD management. ERJ Open Res. 2024;10(3):00850–2023. doi:10.1183/23120541.00850-2023
3. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–e8. doi:10.1016/S2213-2600(24)00413-2
4. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. doi:10.1016/S0140-6736(07)61380-4
5. Sondermann NC, Faßbender S, Hartung F, et al. Functions of the aryl hydrocarbon receptor (AHR) beyond the canonical AHR/ARNT signaling pathway. Biochem Pharmacol. 2023;208:115371. doi:10.1016/j.bcp.2022.115371
6. Guerrina N, Traboulsi H, Eidelman DH, et al. The aryl hydrocarbon receptor and the maintenance of lung health. Int J Mol Sci. 2018;19(12):3882. doi:10.3390/ijms19123882
7. Soleimanifar N, Assadiasl S, Kalateh E, et al. Circulating exosomes and ambient air pollution exposure in COPD. chronic obstructive pulmonary diseases. J COPD Foundation. 2023;10(4):412. doi:10.15326/jcopdf.2023.0400
8. Vogel CFA,Van Winkle LS, Esser C, et al. The aryl hydrocarbon receptor as a target of environmental stressors - Implications for pollution mediated stress and inflammatory responses. Redox Biol. 2020;34:101530.
9. Cauchi S, Stücker I, Solas C, et al. Polymorphisms of human aryl hydrocarbon receptor (AhR) gene in a French population: relationship with CYP1A1 inducibility and lung cancer. Carcinogenesis. 2001;22(11):1819–1824. doi:10.1093/carcin/22.11.1819
10. Ye W, Chen R, Chen X, et al. AhR regulates the expression of human cytochrome P450 1A1 (CYP1A1) by recruiting Sp1. Febs J. 2019;286(21):4215–4231. doi:10.1111/febs.14956
11. Nebert DW, Karp CL. Endogenous functions of the aryl hydrocarbon receptor (AHR): intersection of cytochrome P450 1 (CYP1)-metabolized eicosanoids and AHR biology. J Biol Chem. 2008;283(52):36061–36065. doi:10.1074/jbc.R800053200
12. Shimizu Y, et al. Benzo [a] pyrene carcinogenicity is lost in mice lacking the aryl hydrocarbon receptor.
13. Ahmadi M, Soleimanifar N, Rostamian A, et al. Aryl hydrocarbon receptor gene expression in ankylosing spondylitis and its correlation with interleukin-17, RAR-related orphan receptor gamma t expression, and disease activity indices. “Arch. Rheumatol. 2023;39(1):123. doi:10.46497/ArchRheumatol.2023.10203
14. Poulain-Godefroy O, Bouté M, Carrard J, Alvarez-Simon D, Tsicopoulos A, De Nadai P, et al. the aryl hydrocarbon receptor in asthma: friend or foe? Int J Mol Sci. 2020;21(22):8797. doi:10.3390/ijms21228797
15. Aftabi Y, Amiri-Sadeghan A, Gilani N, et al. Investigating possible effects of aryl hydrocarbon receptor G1661A polymorphism on asthma severity in adults. Indian J. Biochem. Biophys. 2022;59(3):311–319.
16. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw Open. 2023;6(12):e2346598–e2346598. doi:10.1001/jamanetworkopen.2023.46598
17. Organization WH. Chronic Obstructive Pulmonary Disease (COPD) Geneva. Switzerland: World Health Organization; 2017.
18. Chen D, Tian T, Wang H, et al. Association of human aryl hydrocarbon receptor gene polymorphisms with risk of lung cancer among cigarette smokers in a Chinese population. Pharmacogenetics Genomics. 2009;19(1):25–34. doi:10.1097/FPC.0b013e328316d8d8
19. Kou Z, Dai W. Aryl hydrocarbon receptor: its roles in physiology. Biochem. Pharmacol. 2021;185:114428. doi:10.1016/j.bcp.2021.114428
20. Major J, Crotta S, Finsterbusch K, et al. Endothelial AHR activity prevents lung barrier disruption in viral infection. Nature. 2023;621(7980):813–820. doi:10.1038/s41586-023-06287-y
21. Wang T, Wyrick KL, Pecka MR, et al. Mechanistic exploration of AhR-mediated host protection against Streptococcus pneumoniae infection. Int Immunopharmacol. 2012;13(4):490–498. doi:10.1016/j.intimp.2012.05.008
22. Guerrina N, Traboulsi H, Rico de Souza A, et al. Aryl hydrocarbon receptor deficiency causes the development of chronic obstructive pulmonary disease through the integration of multiple pathogenic mechanisms. THE FASEB J. 2021;35(3):e21376. doi:10.1096/fj.202002350R
23. Chiba T, Chihara J, Furue M. Role of the Arylhydrocarbon Receptor (AhR) in the Pathology of Asthma and COPD. J Allergy. 2012;2012(1):372384. doi:10.1155/2012/372384
24. Chen Q, Nwozor KO, van den Berge M, et al. From differential DNA methylation in COPD to mitochondria: regulation of AHRR expression affects airway epithelial response to cigarette smoke. Cells. 2022;11(21):3423. doi:10.3390/cells11213423
25. Mierziak J, Kostyn K, Boba A, et al. Influence of the bioactive diet components on the gene expression regulation. Nutrients. 2021;13(11):3673. doi:10.3390/nu13113673
26. Politis SN, Mazurais D, Servili A, et al. Temperature effects on gene expression and morphological development of European eel, Anguilla anguilla larvae. PLoS One. 2017;12(8):e0182726. doi:10.1371/journal.pone.0182726
27. Barreira-Silva P, et al. The role of the AHR in host–pathogen interactions. Nat Rev Immunol. 2024;24:1–17. doi:10.1038/s41577-023-00981-8
28. Ing NH. Steroid hormones regulate gene expression posttranscriptionally by altering the stabilities of messenger RNAs. Biology Reproduction. 2005;72(6):1290–1296. doi:10.1095/biolreprod.105.040014
29. Kou Z, Tran F, Dai W. Heavy metals, oxidative stress, and the role of AhR signaling. Toxicol Appl Pharmacol. 2024;482:116769. doi:10.1016/j.taap.2023.116769
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.