Back to Journals » Clinical Ophthalmology » Volume 17
Decrease in Ocular Blood Flow Thirty Minutes After Intravitreal Injections of Brolucizumab and Aflibercept for Neovascular Age-Related Macular Degeneration
Authors Kato N ![]() , Haruta M
, Haruta M ![]() , Furushima K, Arai R, Matsuo Y, Yoshida S
, Furushima K, Arai R, Matsuo Y, Yoshida S ![]()
Received 4 February 2023
Accepted for publication 21 March 2023
Published 18 April 2023 Volume 2023:17 Pages 1187—1192
DOI https://doi.org/10.2147/OPTH.S407249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nobuhiro Kato, Masatoshi Haruta, Kei Furushima, Rikki Arai, Yu Matsuo, Shigeo Yoshida
Department of Ophthalmology, Kurume University School of Medicine, Kurume, Japan
Correspondence: Masatoshi Haruta, Department of Ophthalmology, Kurume University School of Medicine, 67 Asahi-machi, Kurume, Fukuoka, 830-0011, Japan, Tel +81 942 31 7574, Fax +81 942 37 0324, Email [email protected]
Purpose: Intravitreal injections of anti-vascular endothelial growth factor (VEGF) agents such as brolucizumab and aflibercept are used widely to treat neovascular age-related macular degeneration (nAMD); however; they may theoretically affect the ocular blood flow. We investigated the short-term changes in the ocular blood flow between eyes with nAMD treated with intravitreal brolucizumab injections (IVBr) and intravitreal aflibercept injections (IVA).
Methods: This study included 21 eyes of 21 Japanese patients with nAMD treated with either IVBr or IVA at Kurume University Hospital from April 2021 through June 2022. The rates of ocular blood flow at the optic nerve head (ONH mean blur rate [MBR]-vessel) and at the choroid (CHOR MBR) were analyzed before and 30 minutes after injections using laser speckle flowgraphy.
Results: In the IVBr-treated group, the ONH MBR-vessel and CHOR MBR rates decreased significantly by 10.6% and 16.9% from baseline to 30 minutes after IVBr, respectively. In the IVA-treated group, ONH MBR-vessel and CHOR MBR rates decreased significantly by 9.4% and 6.1% from baseline to 30 minutes after IVA, respectively. There was no significant difference in the rates of decrease in the ONH MBR-vessel or CHOR MBR between the IVBr-treated and IVA-treated groups.
Conclusion: Intravitreal injections of brolucizumab and aflibercept in eyes with nAMD cause significant decreases in ocular blood flow at the ONH and the choroid 30 minutes after injection. The rate of decrease in ocular blood flow was not significant between the eyes treated with brolucizumab and aflibercept. However, 3 of 10 eyes treated with brolucizumab but none of 11 eyes treated with aflibercept had more than a 30% decrease in the ocular blood flow at the choroid 30 minutes after injection.
Keywords: anti-vascular endothelial growth factor agents, choroid, laser speckle flowgraphy, mean blur rate, optic nerve head
Introduction
Age-related macular degeneration is a major cause of irreversible blindness worldwide. Vascular endothelial growth factor (VEGF) is a key molecule in the development of choroidal neovascularization, and anti-VEGF agents, including brolucizumab (Beovu, Novartis, Basel, Switzerland) and aflibercept (Eylea, Regeneron Pharmaceuticals, Tarrytown, NY, USA), are used widely to treat neovascular age-related macular degeneration (nAMD).1
Laser speckle flowgraphy (LSFG) enables two-dimensional, non-invasive measurements of ocular blood flow at the optic nerve head (ONH) and choroid (CHOR) using the laser speckle phenomenon.2 Recent studies using LSFG have shown that intravitreal aflibercept injection (IVA) administered to treat nAMD led to a significant decrease in the ocular blood flow at the ONH as early as 30 minutes after injection;3,4 however, there is limited information on the changes in ocular blood flow after intravitreal brolucizumab injection (IVBr). Because brolucizumab and aflibercept differ in structure, dose, growth factor specificity, and VEGF binding affinity, we investigated the differences in short-term changes in the ocular blood flow in eyes with nAMD between IVBr and IVA treatments.
Patients and Methods
This study included 10 eyes of 10 Japanese patients with nAMD treated with IVBr and 11 eyes of 11 Japanese patients with nAMD treated with IVA at Kurume University Hospital from April 2021 through June 2022. This study adhered to the tenets of the Declaration of Helsinki. The Ethical Committee of Kurume University Hospital reviewed and approved this study (No. 21120). All patients provided written informed consent before inclusion in this study. The exclusion criteria included a history of ocular surgery during the 3 months preceding the study, vitrectomized eyes, axial length exceeding 26.5 mm, and any relevant ophthalmic diseases or conditions that could interfere with LSFG measurements. Pretreatment with intravitreal anti-VEGF agents was not an exclusion criterion, but the last treatment must have been received at least 6 weeks before study inclusion.
All patients underwent a comprehensive ocular examination before injection, including a slit-lamp examination with indirect funduscopy and measurement of the intraocular pressure (IOP) using the iCare IC200 (iCare, Vantaa, Finland). The systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in the upper arm with a manometer with the patients seated after a resting period of 5 minutes. The mean arterial pressure (MAP) was calculated as MAP = DBP + 1/3 (SBP-DBP), and the ocular perfusion pressure (OPP) as OPP = 2/3 MAP - IOP.
LSFG measurements were performed using the LSFG-NAVI (Softcare Co., Ltd., Fukutsu, Japan) as previously reported.3–5 Briefly, this instrument is comprised of a fundus camera equipped with an 830-nm diode laser as the light source and a standard charge-coupled device sensor as the detector. The mean blur rate (MBR), a measure of the relative blood flow velocity, is determined by examining the pattern of the speckle contrast produced by the movements of the erythrocytes in the ocular blood vessels. To analyze the blood flow at the ONH (ONH MBR-vessel), an ellipsoidal rubber band was put around the ONH. The vessel extraction function of the built-in software then was used to calculate the ONH MBR-vessel. To analyze the blood flow at the choroid (CHOR MBR), a rubber band of 100×100 µm2 was placed at the foveal avascular zone. Representative color map images of the LSFG measurements of a study patient before and after IVBr are shown in Figure 1. All patients were instructed to abstain from alcohol, coffee, and tea for 12 hours before the injection, because they can potentially affect the LSFG results.6 Measurements were performed three times in a quiet, dark room with the patient seated. Follow-up was performed 30 minutes after the injection and included measurements of LSFG, blood pressure, and IOP.
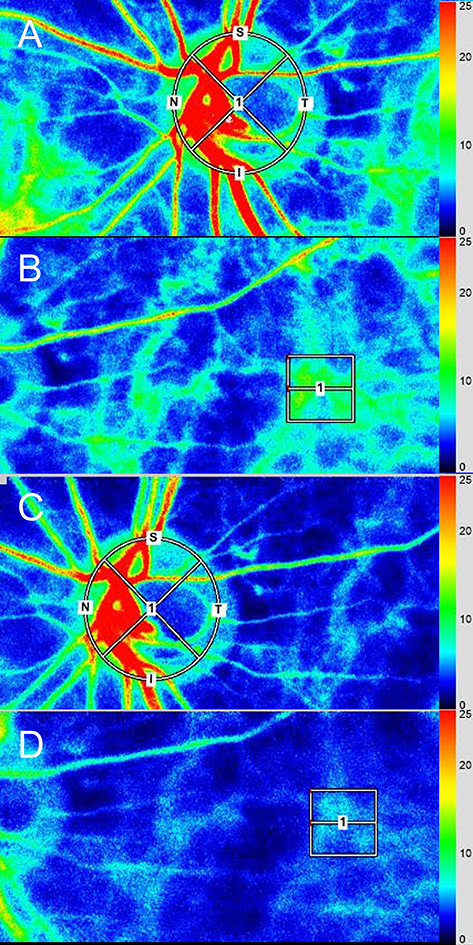 |
Figure 1 Representative color map images of laser speckle flowgraphy. (A) ONH MBR-vessel before intravitreal injection of brolucizumab. (B) The CHOR MBR before intravitreal injection of brolucizumab. (C) The ONH MBR-vessel 30 minutes after intravitreal injection of brolucizumab. (D) The CHOR MBR 30 minutes after intravitreal injection of brolucizumab. Abbreviations: S, superior; N, nasal; T, temporal; I, inferior. |
The data are expressed as the mean ± standard deviation. Statistical analyses were performed using a commercial software package (JMP version 16, SAS Institute, Cary, NC, USA). Pearson’s correlation was used to determine the relationship between the changes in LSFG parameters and the changes in IOP. The Wilcoxon rank-sum test was used to compare the LSFG parameters between before and 30 minutes after the injections. The Mann–Whitney U-test was used to assess the differences in the rates of change in the LSFG parameters between the IVBr-treated and IVA-treated groups.
Results
The baseline clinical characteristics of the 21 patients are shown in Table 1. All eyes had a history of intravitreal injections of anti-VEGF agents. The mean numbers of previous intravitreal injections of anti-VEGF agents were 38.6 ± 23.1 for the IVBr group and 20.7 ± 11.1 for the IVA group (p = 0.045). The intravitreal injections were successfully completed in all treated eyes, and no adverse events including intraocular inflammation, retinal vasculitis, and retinal vascular occlusion were observed during the injection or the follow-up period.
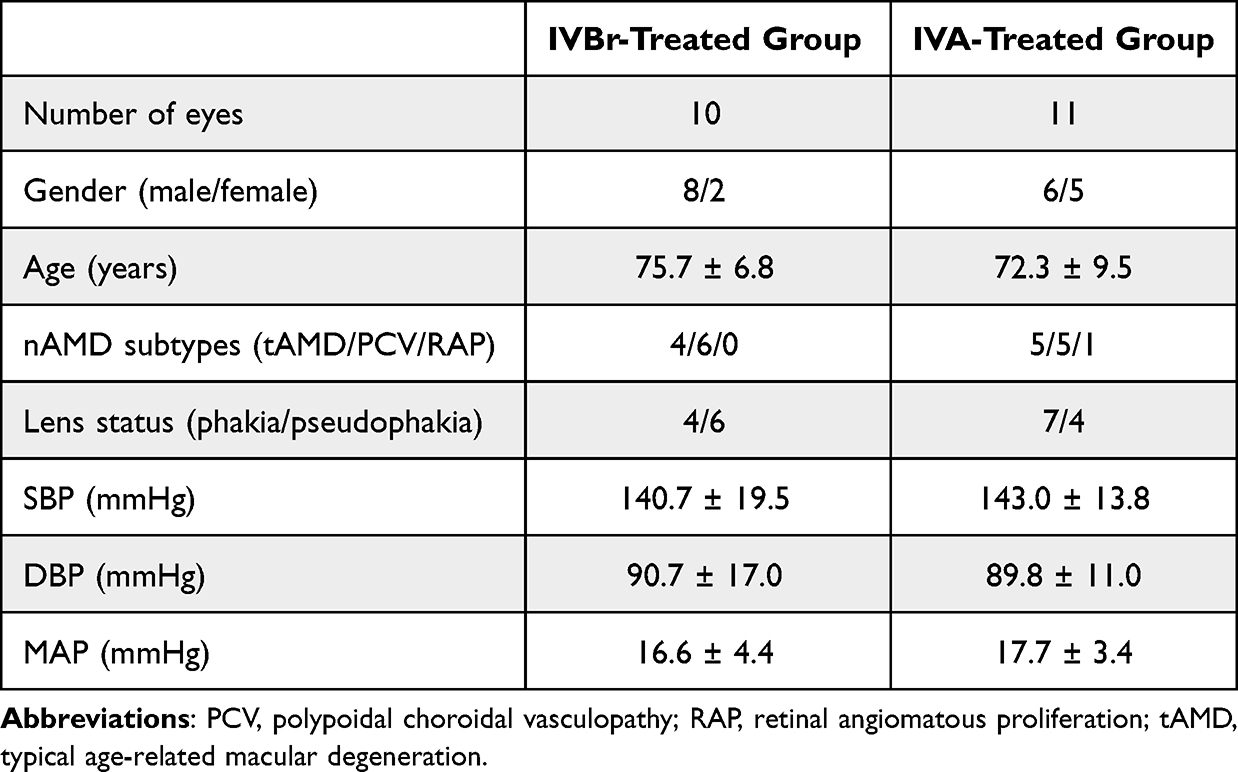 |
Table 1 Clinical Characteristics of Patients |
Table 2 shows the measured values at baseline and 30 minutes after the injections in the two treatment groups.
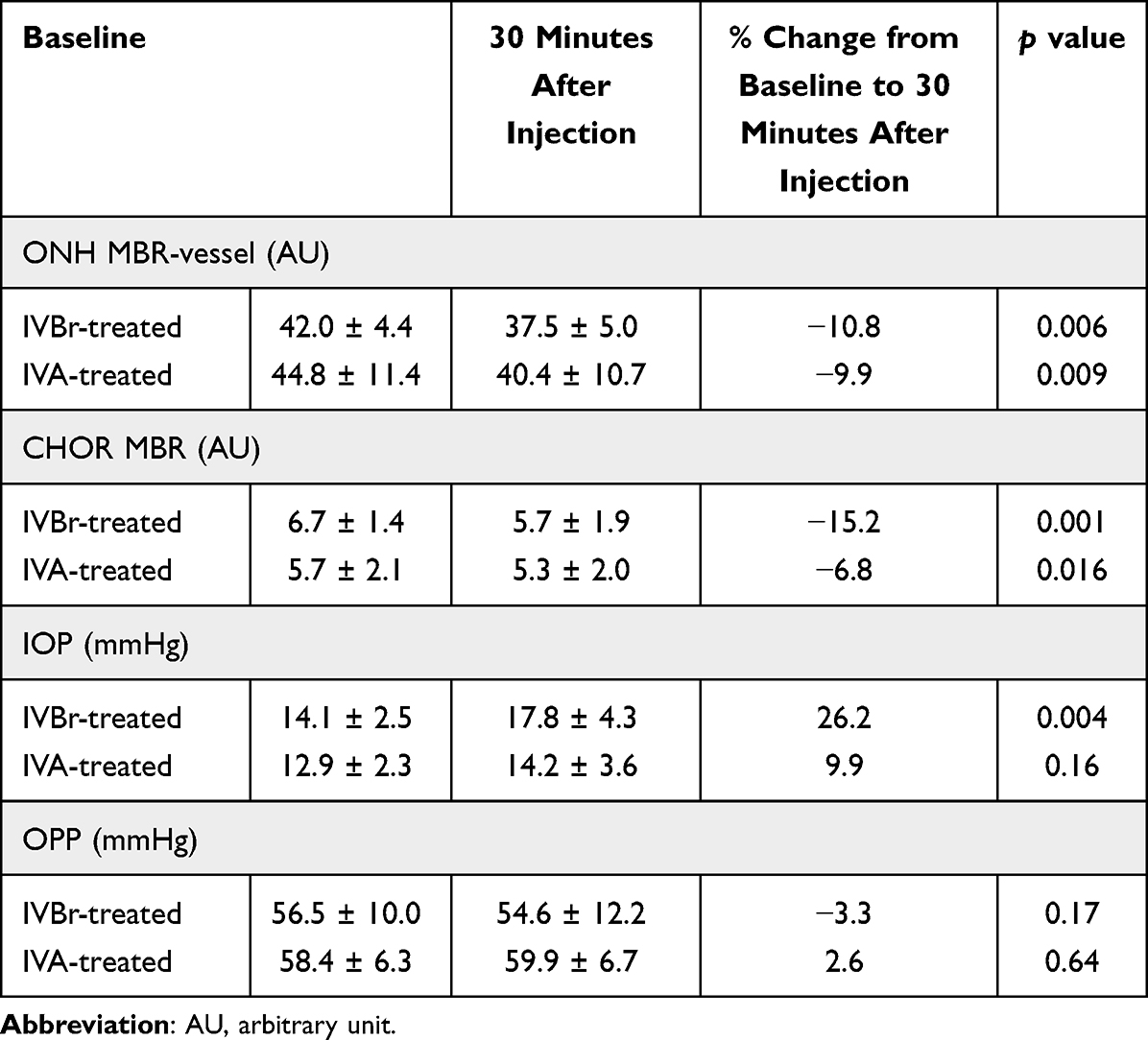 |
Table 2 Changes in Ocular Blood Flow in ONH MBR-Vessel and CHOR MBR from Baseline to 30 Minutes After Injection |
In the IVBr-treated group, the ONH MBR-vessel and CHOR MBR showed 10.8% and 15.2% decreases from baseline to 30 minutes after IVBr, respectively. These decreases reached significance for the ONH MBR-vessel and CHOR MBR (p = 0.006 and p = 0.001, respectively). The mean IOP increased by 3.7 mmHg (p = 0.004) and the mean OPP decreased by 1.9 mmHg (p = 0.17). No negative correlation was found between the changes in the IOP and either those in the ONH MBR-vessel or CHOR MBR (p = 0.308 and p = 0.702, respectively).
In the IVA-treated group, the ONH MBR-vessel and CHOR MBR, respectively, decreased by 9.9% and 6.8% from baseline to 30 minutes after injection, both of which reached significance (p = 0.009 and p = 0.016, respectively). The mean IOP increased by 1.3 mmHg (p = 0.16) and mean OPP increased by 1.5 mmHg (p = 0.64). No negative correlation was found between the changes in IOP and either those in ONH MBR-vessel or CHOR MBR (p = 0.984 and p = 0.268, respectively).
Figure 2 shows the percent changes in the ONH MBR-vessel and CHOR MBR from baseline to 30 minutes after injection. There was no significant difference in either the rate of decrease in the ONH MBR-vessel or CHOR MBR between the IVBr-treated and IVA-treated groups (p = 0.915 and p = 0.098, respectively).
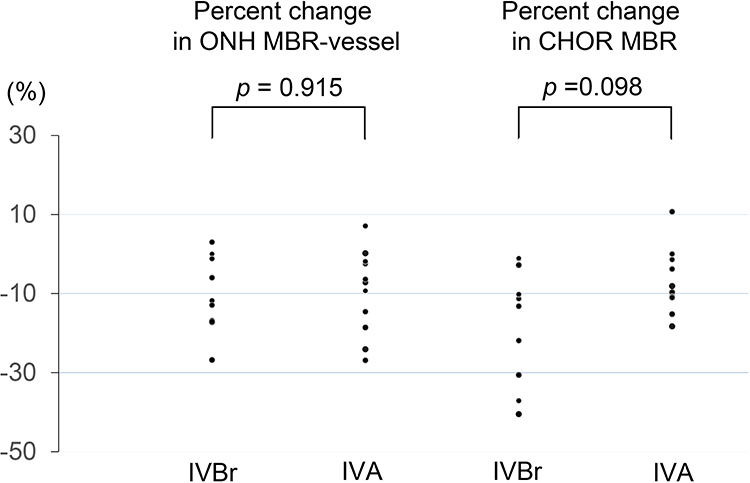 |
Figure 2 % change in the blood flow in the ONH MBR-vessel and CHOR MBR from baseline to 30 minutes after injection. No significant difference is seen in either the rate of decrease in the ONH MBR-vessel or CHOR MBR between the IVBr-treated and IVA-treated groups (p = 0.915 and p = 0.098, respectively). However, it is noteworthy that 3 of 10 eyes treated with IVBr but none of 11 eyes treated with IVA had more than a 30% decrease in the ocular blood flow at the choroid 30 minutes after injection. |
Discussion
Intravitreal injections of anti-VEGF agents such as brolucizumab and aflibercept are used widely to treat nAMD; however; they can theoretically affect the ocular blood flow because VEGF activates endothelial nitric oxide synthase, which produces the potent vasodilator nitric oxide.7 Previous studies using optical coherent tomography have documented the decrease in subfoveal choroidal thickness after anti-VEGF therapy in nAMD and polypoidal choroidal vasculopathy patients, which suggests that anti-VEGF therapy may induce vascular changes not only on the neovascular lesion but also on the underlying choroid.8,9 Brolucizumab is a humanized, single-chain antibody fragment that inhibits all isoforms of VEGF-A, while aflibercept is a soluble decoy receptor that inhibits all isoforms of VEGF-A, VEGF-B, and placental growth factor.10 Brolucizumab is a small anti-VEGF agent with a molecular weight of 26 kDa compared with 115 kDa for aflibercept, and regarding molarity, 6 mg of brolucizumab in one 50-µL injection equals about 12 times 2 mg of aflibercept in one 50-µL injection. Because the greater anti-VEGF capability of brolucizumab may potentially affect the ocular blood flow after IVBr, we investigated the drugs effect on the ocular blood flow in eyes with nAMD 30 minutes after an IVBr. We found that IVBr causes a significant decrease in the ocular blood flow at the ONH and the choroid, as evaluated by ONH MBR-vessel and CHOR MBR, respectively. To the best of our knowledge, this study is the first to evaluate the short-term effect of brolucizumab on the ocular blood flow in eyes with nAMD.
We also investigated the effects of IVA on ocular blood flow in eyes with nAMD 30 minutes after injection. As with IVBr, we found that IVA leads to a significant decrease in the ocular blood flow at the ONH and choroid, as evaluated by the ONH MBR-vessel and CHOR MBR, respectively. Mursch-Edlmayr et al reported that the ONH MVR-vessel but not CHOR MBR significantly decreased 30 minutes after IVA in eyes with nAMD. The discrepancy between the current CHOR MBR results 30 minutes after IVA and those in the previous study might be partly because we placed a rubber band of 100×100 µm2 at the foveal avascular zone to measure the CHOR MBR while the previous study placed a 150×150 pixel square at a temporal location 1 disc diameter from the ONH. However, when the nAMD was treated with three consecutive monthly IVA, Mursch-Edlmayr et al reported that CHOR MBR significantly decreased at 1 week after the first IVA, at the time of second and third IVA, and 1 month after the third IVA.
In the current study, there was no significant difference in either the rate of decrease in the ONH MBR-vessel or CHOR MBR between the IVBr-treated and IVA-treated groups. However, it is noteworthy that 3 of 10 eyes in the IVBr-treated group but none of 11 eyes in the IVA-treated group showed more than a 30% decrease in the CHOR MBR from baseline to 30 minutes after injection (Figure 2). The HAWK and HARRIER trials concluded that brolucizumab exhibited an overall well-tolerated safety profile;1,11 however, retinal vascular occlusion has been described recently as part of the intraocular inflammation and retinal vasculitis spectrum after IVBr.12 The precise mechanisms of retinal vascular occlusion after IVBr are unknown, and further studies are necessary to confirm whether the degree of decease in the ocular blood flow is related to the development of retinal vascular occlusion after IVBr.
Previous studies have reported that the IOP increased significantly after intravitreal injection of bevacizumab (Avastin, Genentech Inc., South San Francisco, CA, USA) or aflibercept but decreased to the baseline values after 30 minutes.3,13 We observed 3.7 mmHg and 1.3 mmHg increases in the mean IOP 30 minutes after IVBr and IVA, respectively, which may affect the OPP. However, no significant decrease was observed in the mean OPP in the IVBr-treated and IVA-treated groups, and no correlation was found between the changes in IOP and those in the ONH MBR-vessel or CHOR MBR. In addition, considering that the ONH can autoregulate its blood flow in response to experimental changes in OPP induced by IOP elevations,5 the current decrease in the ONH MBR-vessel and CHOR MBR may reflect the direct pharmacologic effects of brolucizumab and aflibercept on the ocular blood flow.
The limitations of our study include the small number of cases, the necessary sample size not calculated before the study, the one-time evaluation of 30 minutes after intravitreal injections, and the short duration of follow-up. In addition, although the last treatment was performed at least 6 weeks before study inclusion, all 21 eyes had been treated previously with intravitreal injections of anti-VEGF agents. The population in this study was entirely Japanese, the results of which may not be applicable to a larger nAMD population.
Conclusions
Intravitreal injections of brolucizumab and aflibercept in eyes with nAMD led to a significant decrease in the ocular blood flow at the ONH and choroid 30 minutes after injection. The rate of decrease in the ocular blood flow was not significant between the eyes treated with brolucizumab and aflibercept. However, it is noteworthy that 3 of 10 eyes treated with brolucizumab but none of 11 eyes treated with aflibercept showed more than a 30% decrease in the ocular blood flow at the choroid from baseline to 30 minutes after injection.
Acknowledgments
The authors thank Lynda Charters for English editing.
Disclosure
The authors report no conflicts of interest associated with this work.
References
1. Dugel PU, Singh RP, Koh A, et al. HAWK and HARRIER: ninety-six-week outcomes from the phase 3 trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2021;128:89–99. doi:10.1016/j.ophtha.2020.06.028
2. Sugiyama T, Araie M, Riva CE, et al. Use of laser speckle flowgraphy in ocular blood flow research. Acta Ophthalmol. 2010;88:723–729. doi:10.1111/j.1755-3768.2009.01586.x
3. Mursch-Edlmayr AS, Luft N, Podkowinski D, et al. Short-term effect on the ocular circulation induced by unilateral intravitreal injection of aflibercept in age-related maculopathy. Acta Ophthalmol. 2019;97:e927–e932. doi:10.1111/aos.14098
4. Mursch-Edlmayr AS, Luft N, Podkowinski D, et al. Effects of three intravitreal injections of aflibercept on the ocular circulation in eyes with age-related maculopathy. Br J Ophthalmol. 2020;104:53–57. doi:10.1136/bjophthalmol-2019-313919
5. Iwase T, Akahori T, Yamamoto K, et al. Evaluation of optic nerve head blood flow in response to increase of intraocular pressure. Sci Rep. 2018;8:17235. doi:10.1038/s41598-018-35683-y
6. Okuno T, Sugiyama T, Tominaga M, et al. Effects of caffeine on microcirculation of the human ocular fundus. Jpn J Ophthalmol. 2002;46:170–176. doi:10.1016/S0021-5155(01)00498-1
7. Fontaine O, Olivier S, Descovich D, et al. The effect of intravitreal injection of bevacizumab on retinal circulation in patients with neovascular macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:7400–7405. doi:10.1167/iovs.10-6646
8. Pellegrini M, Bernabei F, Mercanti A, et al. Short-term choroidal vascular changes after aflibercept therapy for neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2021;259:911–918. doi:10.1007/s00417-020-04957-5
9. Shen M, Zhou H, Kim K, et al. Choroidal changes in eyes with polypoidal choroidal vasculopathy after anti-VEGF therapy imaged with swept-source OCT angiography. Invest Ophthalmol Vis Sci. 2021;62:5. doi:10.1167/iovs.62.15.5
10. Dugel PU, Jaffe GJ, Sallstig P, et al. Brolucizumab versus aflibercept in participants with neovascular age-related macular degeneration: a randomized trial. Ophthalmology. 2017;124:1296–1304. doi:10.1016/j.ophtha.2017.03.057
11. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127:72–84. doi:10.1016/j.ophtha.2019.04.017
12. Baumal CR, Bodaghi B, Singer M, et al. Expert opinion on management of intraocular inflammation, retinal vasculitis, and vascular occlusion after brolucizumab treatment. Ophthalmol Retina. 2021;5:519–527. doi:10.1016/j.oret.2020.09.020
13. Hollands H, Wong J, Bruen R, et al. Short-term intraocular pressure changes after intravitreal injection of bevacizumab. Can J Ophthalmol. 2007;42:807–811. doi:10.3129/i07-172
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.