Back to Journals » Lung Cancer: Targets and Therapy » Volume 13
Deconstructing ADAURA. It is Not Yet Time to Forgo Platinum-based Adjuvant Chemotherapy in Resected Early Stage (IB-IIIA) EGFR-mutant NSCLC
Authors Brazel D, Nagasaka M ![]()
Received 25 December 2021
Accepted for publication 8 May 2022
Published 19 May 2022 Volume 2022:13 Pages 47—52
DOI https://doi.org/10.2147/LCTT.S346922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Fengying Wu
Danielle Brazel,1 Misako Nagasaka1– 3
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA; 3Department of Medicine, St. Marianna University School of Medicine, Kawasaki, Japan
Correspondence: Misako Nagasaka, Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA, Email [email protected]
Abstract: Recently, the ADAURA study demonstrated statistically significant improved disease-free survival (DFS) with adjuvant osimertinib in patients with resected stage IB-IIIA non-small cell lung cancer (NSCLC) harboring an epidermal growth factor receptor (EGFR) mutation. A consistent improvement in disease-free survival (DFS) was shown, regardless of whether or not patients received adjuvant chemotherapy. Given benefit seen with and without adjuvant chemotherapy, some clinicians may be tempted to forgo chemotherapy and only offer osimertinib post surgical resection. Would this approach be appropriate? Here we carefully dissect data from the ADAURA trial and review how this may fit into the existing evidence on the treatment of early stage NSCLC by discussing five themes, the study design of ADAURA, attempts on adjuvant tyrosine kinase inhibitors, prior studies to support adjuvant chemotherapy, how adjuvant chemotherapy was administered in ADAURA and consideration of toxicities.
Keywords: early stage non-small cell lung cancer, epidermal growth factor receptor, adjuvant therapy, osimertinib, disease-free survival, overall survival
Introduction
Approximately 30% of patients with non-small cell lung cancer (NSCLC) present with resectable disease at the time of diagnosis.1–3 Despite curative intent of treatment, disease recurrence after surgery is high across all stages (stage IB 45%; stage II 62%; stage III 76%).4 This suggests that many patients have micrometastatic disease at the time of complete resection. Indeed, the five-year overall survival remains poor between 36 and 49%.5 Standard treatment for stage II–IIIA NSCLCs includes surgical resection followed by adjuvant chemotherapy and patients with a high risk of recurrence are most likely to benefit from chemotherapy.
The overall benefit of adjuvant chemotherapy has been demonstrated by the lung adjuvant cisplatin evaluation (LACE) meta-analysis,4 which combined individual patient data from five large trials. Based on the LACE meta-analysis, adjuvant cisplatin-based chemotherapy was associated with a 5.4% decreased risk of death with a hazard ratio (HR) of 0.89 (95%CI: 0.82–0.96) (Table 1). As recommended through National Comprehensive Cancer Network (NCCN) guidelines, adjuvant cisplatin-based chemotherapy for resected stage II and IIIA disease is considered standard of care.6
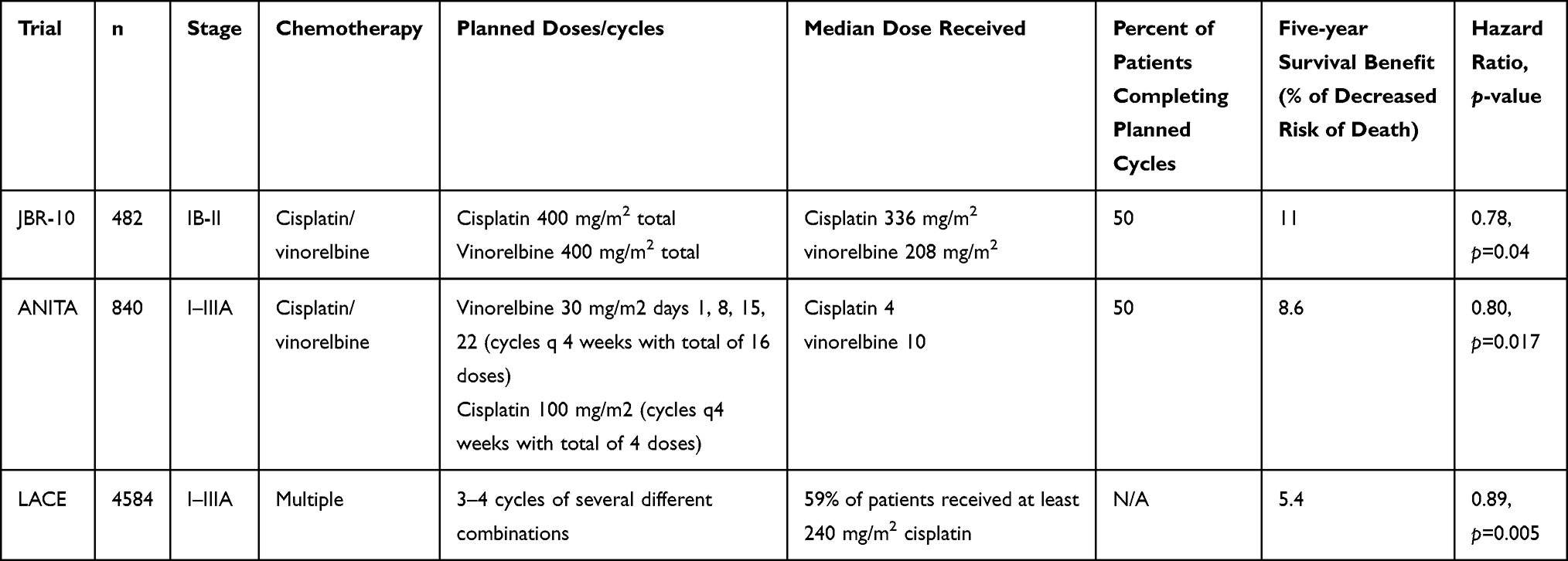 |
Table 1 Adjuvant Trials with Platinum-Based Combinations |
Recently, the ADAURA study demonstrated that adjuvant osimertinib provides statistically significant and clinically meaningful improved disease-free survival (DFS) in stage IB-IIIA epidermal growth factor receptor (EGFR)-positive NSCLC (HR: 0.20; 99%CI: 0.14–0.30; p=0.001).7 The authors also showed a consistent improvement in DFS regardless of whether or not patients received adjuvant chemotherapy (HR: 0.16; 95%CI: 0.10–0.26 with chemotherapy vs HR: 0.23; 95%CI: 0.13–0.40 without chemotherapy).8 Given benefit with and without chemotherapy, some clinicians may be tempted to forgo chemotherapy and only offer osimertinib. Would this approach be appropriate? Here we carefully dissect data from the ADAURA trial and review how this may fit into the existing evidence on the treatment of early stage NSCLC.
Study Design of ADAURA
The ADAURA phase III trial enrolled 682 patients with resected EGFR-positive NSCLC in a 1:1 ratio of osimertinib 80 mg daily vs placebo. Osimertinib is a selective third-generation oral EGFR-tyrosine kinase inhibitor (TKI) with efficacy in central nervous system (CNS) activity. The primary end point was DFS among patients with stage II to IIIA disease based on investigator assessment. Secondary end points included DFS in the overall population of stage IB to IIIA disease, overall survival (OS), and safety. At 24-month follow-up 90% of stage II–IIIA disease on osimertinib vs 44% on placebo were alive and disease free (HR: 0.17). In addition, 89% on osimertinib and 52% on placebo were without CNS disease (HR: 0.18).7
The ADAURA trial was not designed to define the role of adjuvant chemotherapy in resected NSCLC harboring EGFR mutations. Patients were randomized to adjuvant osimertinib vs placebo. If we wanted to ask the question of chemotherapy OR osimertinib post surgery, that should have been the randomization. However, in the ADAURA study, chemotherapy was allowed but not mandatory. In addition, patients were not stratified for adjuvant chemotherapy use, rather, adjuvant chemotherapy was merely part of a prespecified exploratory analysis. Updated data demonstrated that 410/682 patients (60%) received adjuvant chemotherapy (osimertinib, n=203; placebo n=207) for a median of four cycles. Adjuvant chemotherapy was more likely to be given to patients under 70 years old, stage II–IIIA disease, and those enrolled in Asia.8
Prior Evidence on Adjuvant EGFR TKIs
In contrast to ADAURA, studies designed to compare adjuvant chemotherapy to EGFR TKIs have not shown an overall survival benefit. The ADJUVANT-CTONG1104 phase III randomized control trial compared adjuvant gefitinib to vinorelbine plus cisplatin in EGFR-positive, resected stage II–IIIA NSCLC.9 A total of 222 patients received gefitinib for 24 months or vinorelbine plus cisplatin every three weeks for four cycles with a median follow-up time of 80 months. Although interim results found improved DFS in the gefitinib arm (30.8 vs 19.8 months; HR: 0.56; 95%CI: 0.40–0.79), this DFS advantage did not translate to a difference in OS. The median OS was 75.5 and 62.8 months with gefitinib and vinorelbine plus cisplatin, respectively (HR: 0.92; 95%CI: 0.62–1.36, p=0.674).10
The IMPACT Japanese study compared gefitinib vs cisplatin vinorelbine in a phase III randomized control trial.11 Adjuvant gefitinib appeared to prevent early relapse, but did not significantly prolong DFS or OS in patients with completely resected stage II–III, EGFR-mutated NSCLC. The apparent non-inferiority of DFS/OS may justify the use of adjuvant gefitinib in selected subset of patients, especially those deemed unsuitable for cisplatin-based adjuvant therapy.
Lastly, the EVAN trial examined erlotinib vs vinorelbine plus cisplatin in a phase II randomized control trial of stage IIIA EGFR-positive NSCLC.12 Adjuvant erlotinib improved two-year DFS (81.4% vs 44.6%; relative risk 1.823, p=0.0054). Although the OS was in favor of adjuvant erlotinib, the study was powered for its primary endpoint of two-year DFS. Erlotinib was also better tolerated with adverse events across all grades in 58% of patients vs 65% of patients in the chemotherapy arm. While clinical practice should not be altered by a single phase II study, this trial signals that in the future, at least a subset of patients may benefit from targeted therapies without chemotherapy.
Table 2 summarizes the major adjuvant trials with first generation EGFR tyrosine kinase inhibitors.
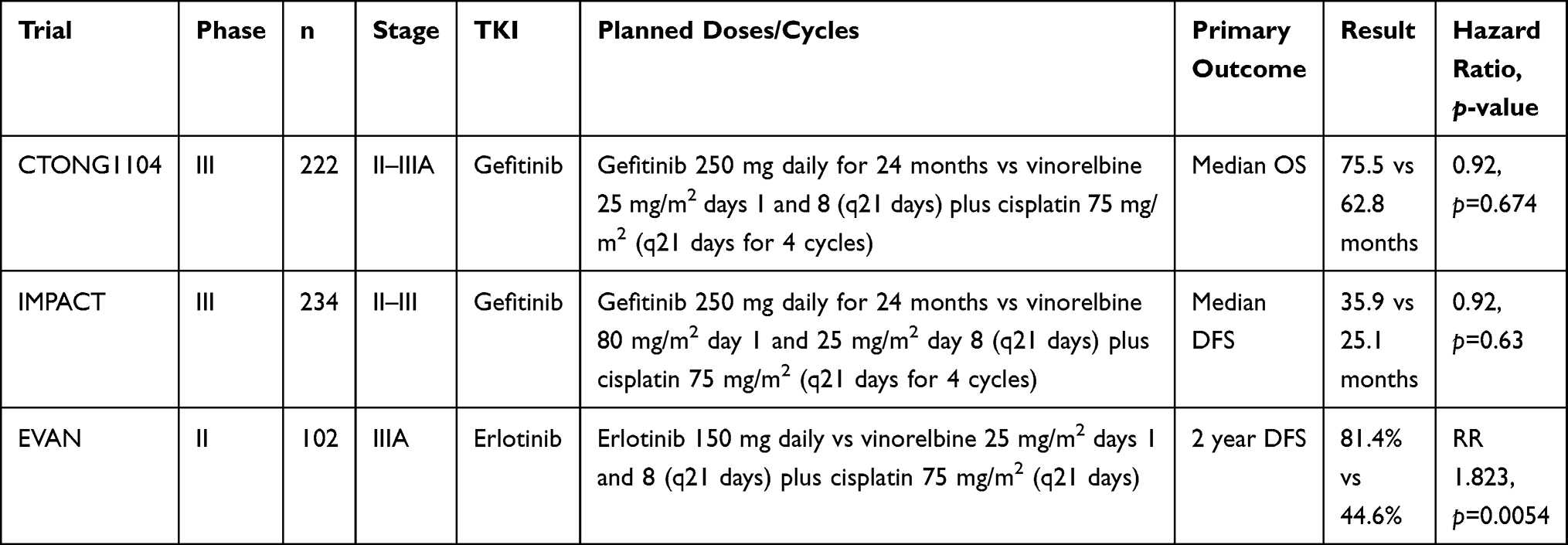 |
Table 2 Adjuvant Trials with First Generation EGFR Tyrosine Kinase Inhibitors |
Prior Studies to Support the Use of Adjuvant Chemotherapy
To date, adjuvant chemotherapy is one of the only treatments with proven OS benefit although the benefit is modest. Conversely, the ADAURA trial shows only DFS benefit at this time and data on OS is immature. It is possible that adjuvant TKIs are providing delayed progression rather than cure.
Multiple randomized control studies powered to study adjuvant chemotherapy have been conducted and the overall benefit has been demonstrated by the LACE meta-analysis4 which combined individual patient data from five large trials. In an analysis of 4584 patients with completely resected NSCLC after a median follow-up of 5.2 years, adjuvant cisplatin-based chemotherapy was associated with 5.4% absolute benefit at five years (HR: 0.89; 95%CI: 0.82–0.96). The effect on survival was statistically significant for stage II disease (HR of death 0.83; 95%CI: 0.73–0.95) and stage IIIA disease (HR of death 0.83; 95%CI: 0.72–0.94). The effect of chemotherapy did not vary significantly by the regimen used. Furthermore, a meta-analysis of patients treated with cisplatin and vinorelbine (n=1888) demonstrated a survival improvement of 8.9% at five years (HR=0.8).13 The survival increments at five years was 14.7% in stage II and 11.6% in stage III patients.
The International Adjuvant Lung Trial (IALT) examined 1867 patients after complete resection of NSCLC with median follow-up of 56 months. This study found significant 4% benefit in five-year OS with chemotherapy (HR: 0.86; 95%CI: 0.76–0.98). In addition, patients assigned to chemotherapy had longer DFS (HR: 0.83; 95%CI: 0.74–0.94). Long-term follow-up of IALT at 7.5 years found prolonged benefit of adjuvant chemotherapy on OS (HR: 0.91; 95%CI: 0.81–1.02) and DFS (HR: 0.88; 95%CI: 0.78–0.98).14 This long-term benefit indicates that adjuvant chemotherapy prevents recurrence rather than merely delaying it.
In ANITA, investigators studied 840 patients with stage IB-IIIA NSCLC on vinorelbine plus cisplatin or observation.15 At a median of 76-month follow-up, median OS was 65.7 months with chemotherapy and 43.7 months on observation (HR: 0.80). The five-year OS was 8.6% higher in patients who received chemotherapy. The findings were statistically significant with this benefit mainly seen in patients with stage II and stage IIIA NSCLC.
The JBR.10 trial compared four cycles of vinorelbine plus cisplatin to observation in stage IB/II NSCLC.16 At long-term follow-up (median of 9.3 years) there remained an 11% improvement in five-year survival.16 Patients with stage II disease had a significant survival benefit with HR: 0.68 (95%CI: 0.5–0.92). Patients with tumor size ≥4 cm also benefitted from chemotherapy with HR: 0.66 (95%CI: 0.39–1.14). The five-year survival for tumors ≥4 cm was 79% with chemotherapy vs 59% with observation. Major adverse effects included fatigue, anorexia, nausea, febrile neutropenia.
In addition, a Cochrane meta-analysis from the Non-Small Cell Lung Cancer Collaborative Group examining 8447 patients demonstrated a 4% OS benefit of adjuvant chemotherapy.17
Although the median age of lung cancer patients in the United States is 71 years, the majority of clinical trials enroll patients with a median age of early 60s. Considering this, the LACE meta-analysis reported a subgroup analysis of patients over 70 years old and a trend toward survival advantage with adjuvant chemotherapy was seen even in this age group with a HR of 0.90 (95%CI: 0.7–1.16).4 The JBR.10 trial also showed survival benefit with chemotherapy in patients at least 65 years (HR: 0.61; 95%CI: 0.38–0.98).18
Adjuvant Chemotherapy Use in ADAURA
As previously stated, the majority of patients (60%) in the ADAURA trial received prior adjuvant chemotherapy. Delivery of adjuvant chemo was allowed per physician and patient preference but not mandatory. Broken down by disease stage, 26% with stage IB, 71% with stage II, and 80% with stage IIIA received adjuvant chemotherapy.8 Due to the discrepancy in administering adjuvant chemotherapy to patients with higher disease stage or other high-risk features, selection bias cannot be excluded. The reason for not administering chemotherapy to the other 40% of patients were not documented, but might include patient preference, age, disease stage, geographical variation, timing/(lack of) recovery following surgery, patients being deemed clinically unfit.
More recent studies (such as IMpower 010) randomized patients post adjuvant chemotherapy to immunotherapy vs observation.19 In this trial of 1005 patients with stage IB to IIIA NSCLC, patients received a median of four cycles adjuvant platinum-based chemotherapy plus adjuvant atezolizumab for one year. At median of 32.2 month follow-up, atezolizumab improved DFS in stage II–IIIA tumors (HR: 0.66 PD-L1 positive; HR: 0.81 all patients). IMpower 010 showed a significant DFS benefit with atezolizumab vs observation in resected stage II–IIIA patients post- adjuvant chemotherapy and this regimen has gained FDA approval. The side effects were tolerable with grade 3 or higher adverse events in 12% of patients. The most common included hepatic laboratory abnormalities, rash, and hypothyroidism. The trend in more recent studies is not trying to replace chemotherapy with additional therapy but rather to add on to the benefits that chemotherapy already provides.
Although the studies included in the LACE meta-analysis utilize older chemotherapy agents (ie vinorelbine with cisplatin), the use of more modern regimens (ie platinum with pemetrexed) along with better antiemetics should only make adjuvant chemotherapy more effective and better tolerated.
Toxicity Consideration and Future Directions
Despite the fact that targeted therapies are generally better tolerated than chemotherapy, they are not without side effects. Adverse effects of osimertinib include diarrhea (39%), paronychia (23%), dry skin (20%), and pruritis (17%). Serious adverse events (grade 3 or above) include diarrhea (2%), stomatitis (2%), pneumonia (1%), electrocardiogram QT prolongation (1%), and interstitial lung disease (<1%). Serious adverse effects occurred in 16% of patients on osimertinib.7 In contrast, adverse events from the typical three months of adjuvant chemotherapy are often transient and may not be as toxic as one may imagine. A sub-analysis of 359 patients from JBR.10 found transient decline in quality of life that returned to baseline nine months later.20 Another survey of 482 patients found adjuvant chemotherapy actually improved quality-adjusted survival despite the toxicity of chemotherapy.21 Nonetheless, in the adjuvant treatment setting, it is important to continuously weigh risks and benefits of therapy as at least a portion of patients are cured with surgical resection alone. It is possible that patients had benefit from osimertinib regardless of chemotherapy because higher stage (and typically higher risk) patients had chemotherapy which may have erradicated the more aggressive clones22 and perhaps this was not necessary in those who did not get chemotherapy who likely had lower risks.
Based on the results of the LACE trial, adjuvant chemotherapy remains one of the only treatment modalities with proven survival benefit. The LACE trial also suggests the toxicities of adjuvant chemotherapy are tolerable for the majority of patients. Although toxicity rates were highly variable across the four trials, in those 1190 patients treated with chemotherapy, 66% experienced grade 3 to 4 toxicity with the most frequent toxicity being neutropenia (grade 3 at 9%, grade 4 at 28%).4
Perhaps one day oncologists may be able to identify patients at high risk of recurrence after surgical resection by utilizing genomic technology such as liquid biopsies or radionomics. These patients could then be selected to receive chemotherapy, avoiding toxic exposure to those with little benefit. Future studies “correctly” randomizing patients to adjuvant targeted therapy vs adjuvant chemotherapy may ultimately reveal targeted therapeutics to have OS benefit over chemotherapy, but until then, it is not yet time to forgo adjuvant chemotherapy.
Conclusion
Adjuvant chemotherapy was allowed but not mandatory in the ADAURA study. The ADAURA study was clearly not designed to compare osimertinib to chemotherapy and thus osimertinib should not replace adjuvant chemotherapy as standard of care. When adjuvant chemotherapy was allowed but not mandatory, the issue of selection bias arise. Those with higher risk disease and who were fit were likely to be offered chemotherapy. Although adjuvant osimertinib was found to be beneficial regardless of adjuvant chemotherapy use, one cannot extrapolate from a single publication on a subgroup analysis which was not designed or powered to evaluate the role of adjuvant chemotherapy vs adjuvant osimertinib. Benefits of adjuvant chemotherapy in early stage disease remain modest but are one of the few proven regimens to improve overall survival in early stage lung cancer. It is not yet time to forgo platinum-based adjuvant chemotherapy in resected early stage (IB-IIIA) EGFR-mutant NSCLC.
Abbreviations
CNS, central nervous system; CT, computed tomography; DFS, disease-free survival; EGFR, epidermal growth factor receptor; IALT, International Adjuvant Lung Cancer Trial; LACE, Lung adjuvant cisplatin evaluation; HR, hazard ratio; MRI, magnetic resonance imaging; NCCN, National Comprehensive Cancer Network; NSCLC, non-small cell lung cancer; OS, overall survival; PET, positron emission tomography; SUV, standardized update value; TKI, tyrosine kinase inhibitor.
Ethics and Consent Statements
This is a review paper. No ethics and patient consents are required.
Funding
No funding was secured for this report.
Disclosure
Dr Misako Nagasaka reports personal fees from AstraZeneca, Caris Life Sciences, Daiichi Sankyo, Takeda, Novartis, EMD Serono, Blueprint Medicines, Janssen, Pfizer, Lilly, Genentech, and Mirati; non-financial support from AnHeart Therapeutics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Datta D, Lahiri B. Preoperative evaluation of patients undergoing lung resection surgery. Chest. 2003;123:2096–2103. doi:10.1378/chest.123.6.2096
2. Chevalier L. Adjuvant chemotherapy for resectable non-small-cell lung cancer: where is it going? Ann Oncol. 2010;21(suppl7):vii196–vii198. doi:10.1093/annonc/mdq376
3. Cagle P, Allen T, Olsen R, et al. Lung cancer biomarkers: present status and future developments. Arch Pathol Lab Med. 2013;137:1191–1198. doi:10.5858/arpa.2013-0319-CR
4. Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552. doi:10.1200/JCO.2007.13.9030
5. Goldstraw P, Chansky K, Crowley J, et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11:39–51. doi:10.1016/j.jtho.2015.09.009
6. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology. Non-small cell lung cancer. Available from: https://www.nccn.org/store/login/login.aspx?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf.
7. Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383:1711. doi:10.1056/NEJMoa2027071
8. Wu YL, John T, Crohe C, et al. Postoperative chemotherapy use and outcomes from ADAURA: osimertinib as adjuvant therapy for resected EGFR-mutated NSCLC. J Thorac Oncol. 2021;17:423–433.
9. Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): a randomised, open-label, phase 3 study. Lancet Oncol. 2018;19:139. doi:10.1016/S1470-2045(17)30729-5
10. Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-mutant NSCLC: final overall survival analysis of CTONG1104 phase III trial. J Clin Oncol. 2021;39:713. doi:10.1200/JCO.20.01820
11. Tada H, Mitsudomi T, Yamanaka T, et al. Adjuvant gefitinib versus cisplatin/vinorelbine in Japanese patients with completely resected, EGFR-mutated, stage II-III non-small cell lung cancer (IMPACT, WJOG6410L): a randomized phase 3 trial. ASCO. 2021;38(15):8501.
12. Yue D, Wu S, Wang Q, et al. Erlotinib versus vinorelbine plus cisplatin as adjuvant therapy in Chinese patients with stage IIIA EGFR mutation-positive non-small cell lung cancer (EVAN): a randomized, open-label, phase 2 trial. Lancet Respir Med. 2018;6:863–873. doi:10.1016/S2213-2600(18)30277-7
13. Douillard JY, Tribodet H, Aubert D, et al. Adjuvant cisplatin and vinorelbine for completely resected non-small cell lung cancer: subgroup analysis of the lung adjuvant cisplatin evaluation. J Thorac Oncol. 2010;5:220–228. doi:10.1097/JTO.0b013e3181c814e7
14. Arriagada R, Dumant A, Pignon JP, et al. Long-term results of the international adjuvant lung cancer trial evaluating adjuvant cisplatin-based chemotherapy in resected lung cancer. J Clin Oncol. 2010;28(1):35–42. doi:10.1200/JCO.2009.23.2272
15. Douillard JY, Rosell R, De Lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]: a randomised controlled trial. Lancet Oncol. 2006;7:719. doi:10.1016/S1470-2045(06)70804-X
16. Butts CA, Ding K, Seymour L, et al. Randomized phase III trial of vinorelbine plus cisplatin compared with observation in completely resected stage IB and III non-small-cell lung cancer: updated survival analysis of JBR-10. J Clin Oncol. 2010;28(1):29–34. doi:10.1200/JCO.2009.24.0333
17. Burdett S, Pignon JP, Tierney J, et al. Adjuvant chemotherapy for resected early-stage non-small cell lung cancer. Cochrane Database Syst Rev. 2015;3:CD011430.
18. Pepe C, Hasan B, Winton TL, et al. Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10. J Clin Oncol. 2007;25:1553. doi:10.1200/JCO.2006.09.5570
19. Felip E, Atorki N, Zou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label phase 3 trial. Lancet. 2021;398(10308):1344–1357. doi:10.1016/S0140-6736(21)02098-5
20. Bezjak A, Lee CW, Ding K, et al. Quality-of-life outcomes for adjuvant chemotherapy in early-stage non-small-cell lung cancer: results from a randomized trial, JBR.10. J Clin Oncol. 2008;26:5052. doi:10.1200/JCO.2007.12.6094
21. Jang RW, Le Maître A, Ding K, et al. Quality-adjusted time without symptoms or toxicity analysis of adjuvant chemotherapy in non-small-cell lung cancer: an analysis of the National Cancer Institute of Canada Clinical Trials Group JBR.10 trial. J Clin Oncol. 2009;27:4268. doi:10.1200/JCO.2008.20.5815
22. La Monica S, Minari R, Cretella D, et al. Third generation EGFR inhibitor osimertinib combined with pemetrexed or cisplatin exerts long-lasting anti-tumor effect in EGFR-mutated pre-clinical models of NSCLC. Exp Clin Cancer Res. 2019;38(1):222. doi:10.1186/s13046-019-1240-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.