Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Decoding Treatment Response in Hepatocellular Carcinoma: The Era of Radiomics and Radiogenomics
Authors Wang Z, Gan W, Gong J, Li X
Received 13 January 2026
Accepted for publication 9 May 2026
Published 27 May 2026 Volume 2026:13 595928
DOI https://doi.org/10.2147/JHC.S595928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Zongding Wang,1,2,* Wenjie Gan,3,* Jianping Gong,3 Xiuyun Li1
1Department of Hepatobiliary Surgery, Chongqing Dianjiang People’s Hospital, Chongqing, 408300, People’s Republic of China; 2Department of Hepatobiliary Surgery, Chongqing Municipal Hospital of Traditional Chinese Medicine, Chongqing, 400021, People’s Republic of China; 3Department of Hepatobiliary Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiuyun Li, Department of Hepatobiliary Surgery, Chongqing Dianjiang People’s Hospital, Chongqing, 408300, People’s Republic of China, Tel +86-13996286589, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) immunotherapy is significantly constrained by a low objective response rate (~30%) and the lack of universally applicable predictive biomarkers. Radiomics, a non-invasive technique that extracts high-throughput hidden features from medical images, offers innovative solutions for patient selection, treatment response assessment, and prognosis prediction. This review systematically summarizes the application scenarios, feature extraction, and model construction of multimodal imaging data in HCC immunotherapy. It highlights advances in radiomics for predicting treatment response and evaluating the tumor immune microenvironment (TIME) and underlying molecular signatures. It also analyzes key challenges, including limited sample sizes and poor model generalization, and outlines future directions such as multicenter standardized studies and multi-omics integration. The goal is to inform the clinical translation of radiomics for precision management of HCC immunotherapy.
Keywords: hepatocellular carcinoma, immunotherapy, radiomics, prognosis prediction, TIME, deep learning
Current Status and Clinical Needs of Immunotherapy for Hepatocellular Carcinoma
Clinical Challenges in the Diagnosis and Treatment of Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC) is one of the leading causes of cancer-related deaths worldwide, typically presenting with insidious onset and rapid progression. More than 70% of patients are diagnosed at advanced stages, missing the optimal opportunity for surgical resection, which results in a dismal prognosis.1 Even among patients who undergo surgery, the recurrence rate is as high as 50–70%, significantly affecting long-term survival. Traditional treatments such as radiotherapy and chemotherapy offer limited efficacy for advanced HCC and are often accompanied by severe side effects, failing to meet the clinical needs of these patients.
Breakthroughs and Limitations in Immunotherapy
In recent years, immunotherapy—particularly immune checkpoint inhibitors (ICIs) combined with targeted therapies such as anti-angiogenic agents and tyrosine kinase inhibitors (TKIs)—has become a major breakthrough in treating advanced HCC.A clinical study involving 151 patients with advanced HCC showed that this combination therapy achieved an objective response rate (ORR) of 47.7% and a disease control rate (DCR) of 78.1%.Additionally, 23.2% of patients experienced a conversion from unresectable to resectable disease, significantly improving survival outcomes.1,2
However, the clinical application of immunotherapy still faces significant challenges. First, treatment response rates remain limited, with only about 30% of patients experiencing sustained clinical benefit. Most patients risk treatment failure, disease progression, or even immune-related adverse reactions. Second, effective tools for predicting treatment efficacy are lacking, and no universally accepted biomarkers currently exist to accurately identify suitable candidates for immunotherapy.Third, efficacy assessment lags behind, as traditional solid tumor response criteria (mRECIST) struggle to detect early immunotherapy-induced morphological changes in tumors, often delaying timely treatment adjustments.3,4 These challenges highlight the urgent need for non-invasive, highly specific predictive and evaluative technologies to optimize treatment decisions.
Clinical Value of Radiomics
Because HCC typically develops on a background of liver cirrhosis and exhibits profound intra-tumoral heterogeneity and complex neoangiogenesis, traditional needle biopsies are highly prone to sampling errors and fail to capture the entire tumor landscape. Radiomics specifically addresses these HCC-related clinical bottlenecks. Through high-throughput feature extraction and quantitative analysis of medical images, it non-invasively captures whole-tumor morphology, density/signal heterogeneity, blood flow perfusion patterns, and microenvironment status—aligning closely with the clinical needs of precision HCC immunotherapy (Figure 1). Meanwhile, interpretable models derived from susceptibility-weighted imaging (SWI) effectively identify intra-tumoral tertiary lymphatic structures (iTLSs),5 offering valuable evidence for predicting immunotherapy response. The Longitudinal Whole-Liver CT Radiomics Model (LWCTR) achieved AUC values of 0.883, 0.876, and 0.875 in training, internal, and external cohorts, respectively.6 Ultrasound-based models also predict objective response by capturing tumor heterogeneity and microenvironmental changes.7 All these studies confirm that radiomics-based prediction models can reliably predict treatment response and prognosis.
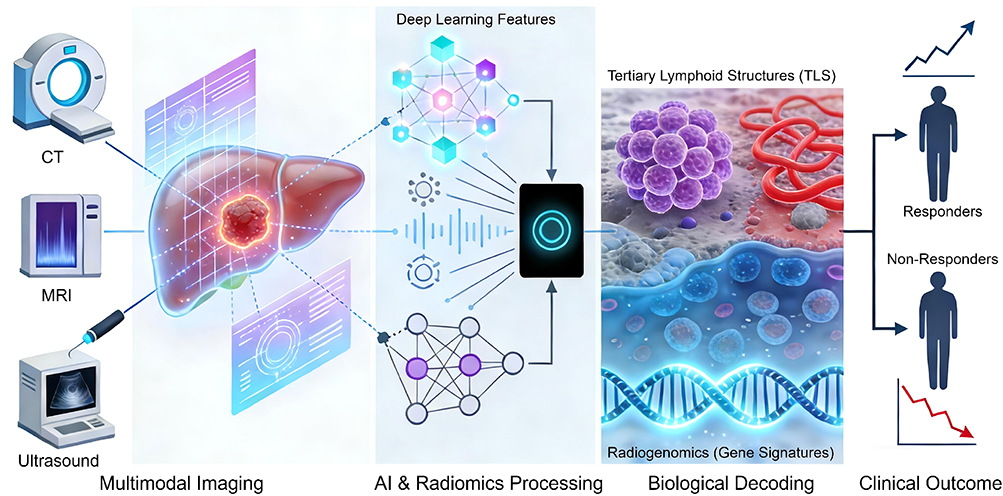 |
Figure 1 Schematic workflow of radiomics and radiogenomics in predicting immunotherapy response and decoding the biological microenvironment in hepatocellular carcinoma. The process involves three key stages: (Left) Multimodal imaging data acquisition including CT, MRI, and Ultrasound; (Middle) Deep learning and radiomics feature extraction to capture high-throughput quantitative data; (Right) Biological decoding (eg, Tertiary Lymphoid Structures, Gene Signatures) to stratify patients into responders and non-responders for precision immunotherapy. Abbreviations: HCC, hepatocellular carcinoma; TLS, tertiary lymphoid structures. |
Furthermore, imaging-based biomarkers, such as radiomics signature of neutrophil extracellular traps (RNETS), effectively differentiate between different prognostic risk groups. Patients in the low RNETS group showed a significantly higher objective response rate (27.8%) compared to those in the high RNETS group (10.8%).8 A comprehensive model integrating radiomics and clinical variables outperformed traditional BCLC staging and ALBI grading in predicting ORR, progression-free survival (PFS), and overall survival (OS),9,10 providing robust support for clinicians in developing personalized treatment strategies.
Fundamentals and Methodological Advances in Radiomics Technology
Medical Imaging Data Types and Clinical Application Scenarios
In HCC radiomics research, multimodal imaging data is widely utilized due to its unique clinical advantages. The technical characteristics and clinical application scenarios of different imaging modalities each have distinct focuses:
MRI Imaging
Multiparametric contrast-enhanced MRI simultaneously captures structural and functional information within and around the tumor,10 making it the imaging modality with the richest feature extraction capabilities to date. Specifically, T2-weighted imaging (T2WI) clearly delineates tumor edema and necrosis, while arterial and portal venous phase contrast-enhanced images reveal tumor blood supply characteristics, providing a basis for assessing tumor invasiveness. In clinical practice, physicians can manually delineate regions of interest (ROIs) using 3D-Slicer software to precisely extract radiomic features of tumors and surrounding tissues. This approach is suitable for baseline assessment before treatment and post-treatment efficacy monitoring.11
CT Imaging
With its advantages of rapid scanning speed, high spatial resolution, and widespread availability, CT has become a routine tool in the clinical diagnosis and treatment of HCC.Longitudinal CT images (arterial and portal venous phases) can extract numerous radiomic features, including texture and morphological characteristics (up to 1316 features per patient).6 Preoperative CT scans can even identify approximately 100 key features associated with immunotherapy response from both whole liver and tumor tissue.12 CT-based radiomics models can achieve standardized feature extraction through pyradiomics tools, making them suitable for multicenter studies and implementation in primary care hospitals.
Ultrasound Imaging
Ultrasound offers non-invasive, real-time, and radiation-free advantages, making it particularly suitable for long-term dynamic follow-up of HCC patients.Machine learning models built upon ultrasound radiomics can analyze tumor characteristics such as echo intensity and boundary morphology to capture internal tumor heterogeneity and microenvironmental changes, providing a convenient tool for dynamic monitoring of immunotherapy efficacy.
Feature Extraction and Modeling Technology Framework
Feature Extraction Process and Core Technologies
Feature extraction in radiomics is a critical step connecting imaging data with clinical applications. Its core workflow encompasses image preprocessing, region of interest (ROI) delineation, feature computation, and feature selection. The preprocessing stage employs techniques such as denoising and normalization to reduce the impact of image artifacts on feature stability. ROI delineation can be performed manually, semi-automatically, or fully automatically. Fully automated methods (eg, deep learning-based segmentation algorithms) improve efficiency and consistency. Feature computation mainly includes first-order features (eg, mean, standard deviation), texture features (eg, grayscale co-occurrence matrix, grayscale-level small-region matrix), and higher-order features (eg, wavelet transform features), comprehensively quantifying tumor heterogeneity.
Feature selection aims to eliminate redundant information and retain key predictors. Common methods include independent samples t-tests and Spearman correlation analysis for preliminary screening of features correlated with the target variable, and LASSO regression combined with 10-fold cross-validation for feature dimensionality reduction and selection. For instance, one study employed this approach to screen 14 core features from a massive dataset for model construction, significantly enhancing the model’s generalization capability.
Modeling Algorithms and Technological Evolution
Imageomics modeling algorithms have progressively evolved from traditional machine learning to deep learning, forming a diversified technical framework:
Traditional Machine Learning
Support Vector Machines (SVM), Extreme Gradient Boosting (XGBoost), Random Forests, and other algorithms have been widely applied in early radiomics research.For instance, the XGBoost algorithm effectively handles high-dimensional imaging features by constructing ensemble decision trees, successfully predicting immune therapy response in HCC patients within ultrasound radiomics models;while SVM classifiers, combined with radiomic features and clinical information, achieved precise prediction of objective response rates to immunotherapy.7
Deep Learning
Leveraging its powerful automatic feature extraction capabilities, deep learning technology has significantly enhanced model performance.For instance, Ensemble-DL models integrating three complementary 3D neural networks effectively enhance prediction accuracy and robustness;1 Deep learning models based on CT can be created using different scanning protocols and integrated with radiomics scores and clinical variables to build ensemble models, further optimizing predictive performance.4 Furthermore, the Transformer architecture overcomes the limitations of traditional methods by efficiently capturing cross-sequence and cross-spatial image feature correlations (ie, “long-range dependencies”) in multi-sequence MRI data. This provides a comprehensive and precise new technical paradigm for integrated analysis of multi-sequence MRI.
Model Performance Evaluation and Clinical Utility Validation
The performance evaluation of radiomics models must balance statistical validity and clinical utility, forming a multidimensional assessment system:
Statistical Metrics
The ROC curve and AUC value are core indicators for evaluating a model’s discrimination capability. High-performing models typically achieve AUC above 0.8, with some exceeding 0.92 or even 1.013 in both training and validation datasets. Additionally, metrics such as sensitivity, specificity, accuracy, positive predictive value, negative predictive value, and F1 score comprehensively reflect a model’s classification performance;Net Reclassification Improvement (NRI) can quantify the model’s improvement over traditional methods.14
Clinical Utility Assessment
Decision curve analysis (DCA) serves as a critical tool for evaluating a model’s clinical value. By comparing the net benefit of the model at different thresholds, it determines its practical application value in clinical practice.Kaplan-Meier survival analysis can validate a model’s ability to stratify patients based on prognostic indicators such as PFS and OS. If significant differences (p < 0.05) exist between survival curves of high- and low-risk groups, the model demonstrates clinical utility.13 For example, the ultrasound radiomics-derived Rad-score effectively stratifies HCC patients’ disease progression risk, identifying those more likely to experience shortened PFS (high-risk) versus those with superior PFS (low-risk), thereby informing treatment optimization strategies.
Research Advances in Imaging-Based Prognostics for Immunotherapy Outcomes in Hepatocellular Carcinoma
Core Predictive Models Based on MRI and CT
Building upon the robust feature extraction techniques and multi-dimensional evaluation frameworks discussed in the previous sections, researchers have successfully translated these methodological foundations into specific clinical tools. Currently, predictive models based on standard MRI and CT imaging represent the most extensively validated core strategies in this domain. MRI and CT, as commonly used clinical imaging modalities, have facilitated the development of radiomics models that play a central role in predicting the efficacy of immunotherapy for HCC. Related research has yielded a series of findings with significant clinical application potential:
MRI Radiomics Model
The AUC of the clinical-radiomics model was 0.887 in the internal validation set and 0.837 in the external validation set, significantly outperforming standalone clinical or radiomics models;The combined radiomics model achieved AUC values of 0.868 and 0.822 in the internal and external validation sets, respectively,10 demonstrating strong generalization capability. Based on multi-sequence contrast-enhanced MRI data, a deep learning framework combining ResNet50 and Transformer was employed. By processing tumor lesion cross-sectional images via multi-instance learning, the model achieved AUC values of 1.000 in both training and validation sets for predicting objective response rates to targeted-immunotherapy combinations in patients with unresectable HCC. The prediction process was visualized through Grad-CAM and SHAP (SHapley Additive exPlanations) algorithms, enhancing clinical interpretability.13
CT Radiomics Model
The longitudinal whole-liver CT radiomics model (LWCTR) demonstrated outstanding performance in predicting treatment response and prognosis for ICI combination therapy, achieving AUC values of 0.883, 0.876, and 0.875 in the training, internal validation, and external test cohorts, respectively. The Rad-Nomo model, constructed based on this framework by integrating Rad-score with mRECIST criteria, achieved time-dependent AUC values of 0.902, 0.823, and 0.850 in the internal validation cohort, and 0.893, 0.848, and 0.762,6 providing a precise tool for patient prognosis stratification. Furthermore, the CT-based clinical radiomics model demonstrated high predictive accuracy for sustained clinical benefit (DCB) in patients with potentially translatable HCC undergoing ICI-based conversion therapy, achieving AUC values of 0.96 (95% CI: 0.94–0.99) and 0.88 (95% CI: 0.77–0.99) on the training and test sets, respectively,4 offering crucial guidance for selecting patients eligible for surgical conversion therapy.
It is noteworthy that combining hepatobiliary and tumor-specific radiomic features further enhances predictive performance. For instance, Model 2 (integrating hepatobiliary and tumor features) achieved an accuracy of 86%, sensitivity of 70%, and specificity of 94%;12 the AUC value of the model constructed using liver and surviving tumor features reached 0.81,outperforming models using liver features alone (AUC=0.77). Among these, the Naive Bayes (NB) classifier demonstrated the highest average performance and excellent specificity due to its simplicity and adaptability to limited training data.12 Comparatively, while CT offers standardized acquisition protocols ideal for multicenter generalizability,6 MRI possesses inherent advantages in soft tissue contrast and functional imaging (eg, SWI, DWI). This makes MRI superior for capturing subtle microenvironmental features, such as TLS5 and specific immune phenotypes,15 which are often invisible on standard CT scans.
Exploratory Applications and Advantages of Ultrasound Imageomics
Despite its relatively low resolution, ultrasound imaging offers unique advantages for dynamic monitoring of HCC immunotherapy due to its non-invasive, real-time, and reproducible nature. Several studies have explored the application value of ultrasound radiomics in predicting treatment efficacy:
Hu et al selected 20 ultrasound radiomic features to construct a model predicting immune therapy response in patients with unresectable HCC. The model achieved an AUC of 0.999 (95% CI: 0.997–1.000) in the training cohort, with an AUC of 0.828 (95% CI: 0.690–0.966) in the validation cohort, significantly outperforming traditional clinical models.7 More importantly, the Rad-score derived from this model showed significant correlation with patient PFS. Patients with Rad-score > 0.057 exhibited significantly longer PFS compared to those with Rad-score < 0.057,7 providing clinicians with a convenient tool for early identification of patients likely to benefit from treatment.
Another major advantage of ultrasound radiomics lies in its dynamic monitoring capabilities. By continuously tracking changes in tumor radiomic features throughout treatment, it enables early warning of treatment failure or disease progression, allowing timely adjustments to therapeutic regimens. This prevents unnecessary waste of medical resources and minimizes adverse patient reactions. In the future, as ultrasound imaging technologies advance—such as elastography and contrast-enhanced ultrasound—the richness of radiomic features will further increase, expanding their application scenarios.
Innovative Practices in Integrating Multimodal and Deep Learning
The integration of multimodal fusion with deep learning represents a crucial approach to addressing the complexity of predicting the efficacy of HCC immunotherapy. By combining complementary information from different imaging modalities with deep learning’s feature extraction capabilities, this approach significantly enhances model performance and generalization ability:
Multimodal Fusion Model
The multimodal fusion (MMF) system integrates CT-derived deep learning features and clinical data to predict overall survival (OS) and progression-free survival (PFS) in HCC patients. It achieved C-index scores of 0.74 (OS) and 0.69 (PFS) in an external validation cohort, outperforming standalone radiomics models, mRECIST criteria, clinical baseline models, and Ensemble-DL models.1 By employing an ensemble learning strategy, the system effectively overcomes the limitations of single-modality data, comprehensively capturing tumor biological characteristics and clinical information to provide robust support for precision prognostic assessment.
Deep Learning Innovation Application
A Transfer Learning Radiomics (TLR) model utilizes pre-trained deep learning networks to extract features from baseline multi-phase MRI scans, predicting iTLS status in HCC. It demonstrated outstanding performance on both the training set (AUC=0.91) and the external validation set (AUC=0.85).16 Patients predicted as iTLS-positive by this model demonstrated significantly higher response rates to combination therapy compared to the negative group (36% vs 13.73%, p=0.009), providing a crucial biomarker for patient selection in immunotherapy.Furthermore, a study developed a “clinical-radiomics integrated model” combining clinical information (such as patient age, liver function classification, tumor marker levels, etc.) with radiomics features. This model employed an MLP classifier (multi-layer perceptron) for prediction, achieving AUC values of 0.900 and 0.893 in the validation cohort, respectively.This model provides a reliable tool for predicting treatment efficacy following LPI (local perfusion immunotherapy) in patients with unresectable HCC.2
Non-Invasive Decoding of Tumor Immune Microenvironment (TIME)
While predicting macroscopic clinical outcomes (such as objective response or survival, as detailed in Research Advances in Imaging-Based Prognostics for Immunotherapy Outcomes in Hepatocellular Carcinoma) is crucial for clinical decision-making, understanding the underlying biological drivers of these responses requires a deeper perspective. Radiomics functions not merely as an algorithmic prognostic tool, but as a non-invasive “virtual biopsy.” The efficacy of immunotherapy in HCC is fundamentally dictated by the spatial heterogeneity of the tumor immune microenvironment (TIME), and recent advances have shifted focus towards decoding these specific biological phenotypes and molecular signatures via radiomics.
Tertiary Lymphoid Structures (TLS) and Immune Cell Infiltration
Tertiary lymphoid structures (TLS) have emerged as critical determinants of effective anti-tumor immunity. Radiomics offers a novel approach to visualizing these structures non-invasively. Long et al first demonstrated that spatial patterns of peritumoral TLS (pTLS) could be accurately predicted using multi-sequence MRI radiomics (AUC=0.91), reflecting the immune infiltration potential at the tumor margin.17 Building on this, their subsequent multicenter study utilized a transfer learning radiomics (TLR) framework to predict intratumoral TLS (iTLS) status. This study was particularly significant as it linked MRI-predicted iTLS density to specific molecular pathways, such as the downregulation of IL6-JAK-STAT3 and mTORC1 signaling, providing a biological rationale for the model’s predictive power regarding combination therapy response.16 Similarly, Liu et al validated the utility of Susceptibility-Weighted Imaging (SWI) in predicting TLS, highlighting the potential of functional MRI sequences in capturing subtle microenvironmental features.5 Besides lymphoid structures, myeloid cells are also crucial. Peng et al18 utilized CT radiomics to evaluate the “myeloid response”, finding that specific radiomic signatures could surrogate the infiltration of immunosuppressive myeloid cells, thereby predicting poor post-surgical survival.
Immune-Hypoxia Crosstalk and Molecular Stratification
Simple dichotomies of “hot” vs. “cold” tumors are often insufficient for predicting ICI response due to the complex interplay between immunity and hypoxia. Song et al proposed a novel “Immune-Hypoxia” stratification system, identifying a “High Immune-Normoxic” (HIN) subtype that benefits most from immunotherapy. They developed an MRI-based radiomics model to non-invasively identify this specific subtype, effectively excluding patients with “High Immune-Hypoxic” tumors who might otherwise be misclassified as responders based solely on immune infiltration.15 Furthermore, Zhang et al constructed an MRI radiomics model to distinguish between immune-activated and non-immune-activated TIME phenotypes, correlating radiomic features with CD8+ T cell density and PD-L1 expression, thereby serving as a surrogate for immunohistochemical markers.10
Radiogenomics: Linking Imaging to Gene Signatures
Radiogenomics bridges the gap between macroscopic imaging phenotypes and microscopic molecular alterations. Wang et al identified a transcriptomic “TACE Failure Signature” (TFS) and demonstrated that preoperative CT radiomics could surrogate this gene signature to predict resistance to TACE and immunotherapy, revealing the underlying immune-suppressive microenvironment (eg, M0 macrophage enrichment) associated with specific imaging features.19 Specifically, the high-risk radiomics group was associated with the upregulation of immune checkpoint genes, including TNFRSF4, CD276, LAG3, CTLA-4, and PDCD1, whereas the low-risk group showed enrichment of NRP1 and IDO1.19 Additionally, Xin et al extended radiomics to the detection of Neutrophil Extracellular Traps (NETs), a distinct immune feature associated with poor prognosis, further expanding the biological interpretability of radiomic models beyond traditional lymphocyte assessment.8
Challenges and Future Perspectives
While radiomics has shown immense potential in optimizing immunotherapy for HCC, reported model performance varies significantly across studies (AUC range: 0.70–1.00) due to heterogeneity in study endpoints and validation cohorts. Several challenges must be addressed to facilitate its translation into clinical practice.
Expanding Imaging Modalities: The Rise of Ultrasomics
Currently, most radiomics studies rely on CT and MRI due to their standardized acquisition protocols. However, these modalities are limited by cost, radiation exposure (CT), and long scanning times. Recent research has highlighted the untapped potential of ultrasomics (ultrasound-based radiomics). Hu et al successfully developed a machine learning-based ultrasomics model to predict the response to TKI combined with anti-PD-1 therapy. Given its cost-effectiveness, real-time capability, and lack of ionizing radiation, ultrasomics represents a promising frontier for frequent, large-scale screening and monitoring of immunotherapy response in HCC patients.7
From Static to Dynamic: Longitudinal Radiomics
In addition to modality limitations,traditional radiomics models typically extract features from a single pretreatment time point (baseline), potentially missing the dynamic evolution of the tumor microenvironment under immune pressure. Longitudinal radiomics, which analyzes changes in imaging features over time (Delta-radiomics), offers a more comprehensive view of treatment resistance. Xu et al pioneered a Longitudinal Whole-liver CT-based Radiomics (LWCTR) model, demonstrating that incorporating temporal feature changes significantly outperformed single-timepoint models in predicting both treatment response and long-term prognosis.6 Future studies should prioritize serial imaging data to capture the “temporal heterogeneity” of HCC.
Advanced Algorithms and Interpretability
As data complexity increases, traditional machine learning algorithms may reach a performance plateau. Deep learning, particularly Transformer architectures, is emerging as a powerful alternative. Chen et al applied a Transformer-based model to multi-sequence MRI, achieving superior predictive accuracy (AUC > 0.90) by effectively capturing long-range dependencies in 3D medical images.13 To address the interpretability challenge of such complex models, techniques such as SHAP (SHapley Additive exPlanations) and Grad-CAM are essential for visualization. For instance, Chen et al13 used Grad-CAM to show that the model focused on the peritumoral boundary—a region biologically known to be rich in immune infiltration—thereby validating the model’s clinical relevance. Despite these visual aids, the abstract nature of deep learning features still poses a barrier. To further enhance trust, future models must integrate biological interpretability—linking abstract deep learning features to concrete biological concepts like tertiary lymphoid structures (TLS) or specific gene expression signatures, thereby establishing a “transparent” AI workflow.
Standardization via Transfer Learning
Scanner variability across centers is a major hurdle for model generalizability. While rigorous preprocessing is standard, advanced techniques like transfer learning are proving more robust. Long et al demonstrated that a transfer learning radiomics (TLR) framework could maintain high diagnostic performance for iTLS prediction across four different centers with varying MRI scanners.16 Adopting such strategies will be crucial for multicenter validation and the eventual regulatory approval of radiomic biomarkers.Furthermore, rigorous adherence to protocols from the Image Biomarker Standardization Initiative (IBSI) is essential to ensure feature reproducibility. To facilitate integration into clinical workflows, future research must also focus on developing fully automated segmentation tools, thereby reducing the time burden of manual ROI delineation.
Summary
The clinical application of HCC immunotherapy has fundamentally transformed the treatment landscape for advanced HCC. However, conventional clinical evaluations, such as mRECIST criteria, often fail to capture the subtle and early microenvironmental changes induced by immune checkpoint inhibitors, leading to delayed or inaccurate efficacy assessments. This inadequacy severely constrains the development of precision medicine and highlights the urgent need for novel predictive tools.
As a non-invasive quantitative analysis technique, radiomics demonstrates immense potential in addressing this clinical gap. It enables the construction of predictive models for efficacy forecasting and the biological decoding of the tumor immune microenvironment (summarized in Table 1). Despite these promising results, the clinical translation of radiomics is currently hindered by specific technical challenges. Chief among these are the lack of standardized imaging acquisition protocols across different centers, the variability in ROI delineation methods, and the “black-box” nature of deep learning algorithms that lack biological interpretability, all of which compromise model generalizability.
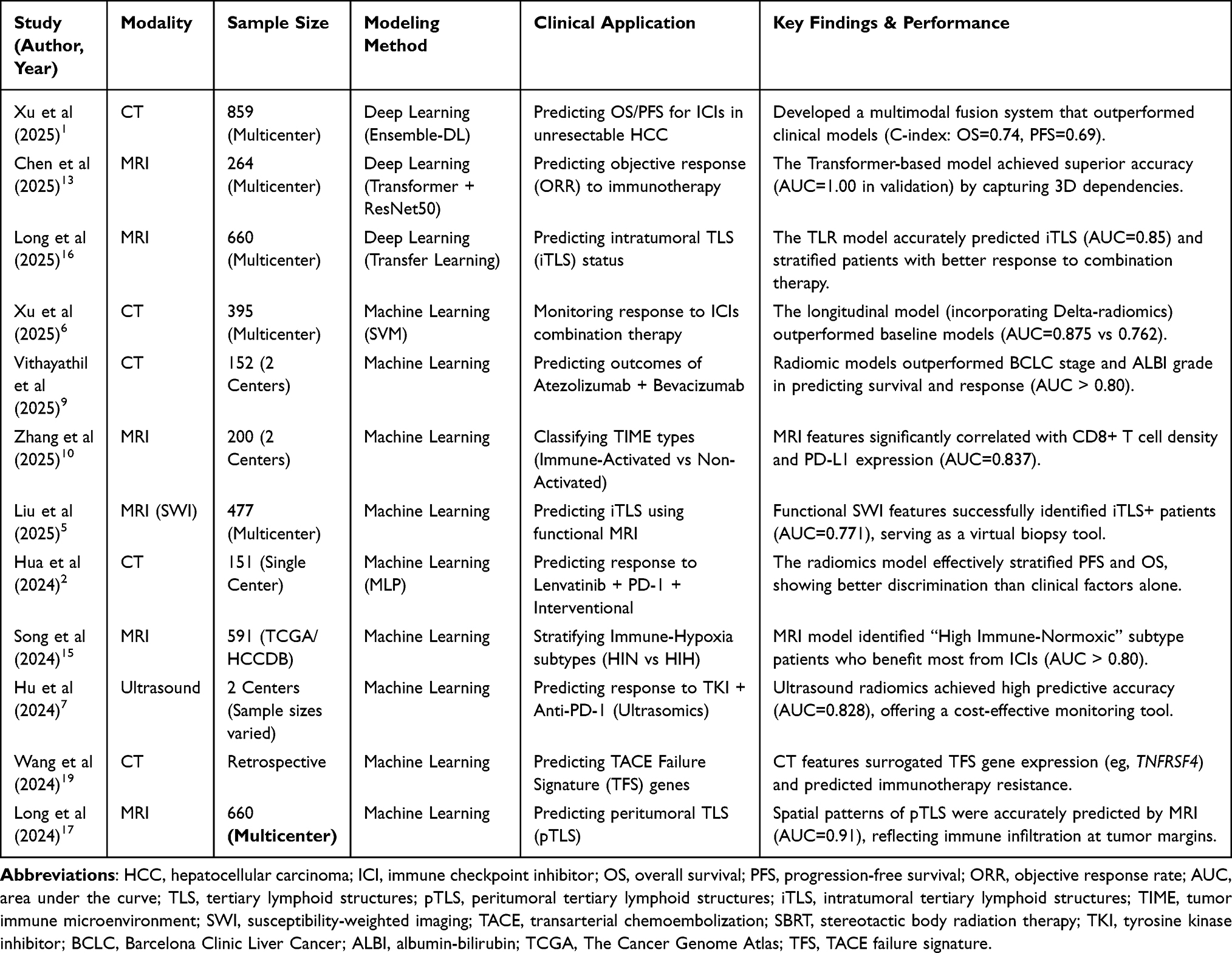 |
Table 1 Summary of Key Studies on Radiomics in HCC Immunotherapy |
Future efforts must prioritize resolving these specific hurdles through rigorous multi-center standardization (eg, adherence to IBSI guidelines), the integration of interpretable AI frameworks, and prospective clinical trials. By utilizing technologies such as ultrasomics and longitudinal monitoring, radiomics can be reliably integrated into routine clinical workflows, ultimately driving HCC immunotherapy toward true precision and individualization.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu J, Wang T, Li J, et al. A multimodal fusion system predicting survival benefits of immune checkpoint inhibitors in unresectable hepatocellular carcinoma. NPJ Precis Oncol. 2025;9(1):185. doi:10.1038/s41698-025-00979-6
2. Hua Y, Sun Z, Xiao Y, et al. Pretreatment CT-based machine learning radiomics model predicts response in unresectable hepatocellular carcinoma treated with lenvatinib plus PD-1 inhibitors and interventional therapy. J Immunother Cancer. 2024;12(7):e008953. doi:10.1136/jitc-2024-008953
3. Qi L, Zhu Y, Li J, et al. CT radiomics-based biomarkers can predict response to immunotherapy in hepatocellular carcinoma. Sci Rep. 2024;14(1):20027. doi:10.1038/s41598-024-70208-w
4. Lin Z, Wang W, Yan Y, et al. A deep learning-based clinical-radiomics model predicting the treatment response of immune checkpoint inhibitors (ICIs)-based conversion therapy in potentially convertible hepatocellular carcinoma patients: a tumor marker prognostic study. Int J Surg. 2025;111(5):3342–10. doi:10.1097/JS9.0000000000002322
5. Liu L, Gao F, Li Y, et al. An interpretable radiomics-based model using susceptibility-weighted imaging for non-invasive prediction of tertiary lymphoid structures in hepatocellular carcinoma. J Hepatocell Carcinoma. 2025;12:2197–2211. doi:10.2147/JHC.S551462
6. Xu J, Li J, Wang T, et al. Predicting treatment response and prognosis of immune checkpoint inhibitors-based combination therapy in advanced hepatocellular carcinoma using a longitudinal CT-based radiomics model: a multicenter study. BMC Cancer. 2025;25(1):602. doi:10.1186/s12885-025-13978-4
7. Hu Y, Zhang L, Qi Q, et al. Machine learning-based ultrasomics for predicting response to tyrosine kinase inhibitor in combination with anti-PD-1 antibody immunotherapy in hepatocellular carcinoma: a two-center study. Front Oncol. 2024;14:1464735. doi:10.3389/fonc.2024.1464735
8. Xin H, Lai Q, Zhou Y, et al. Noninvasive evaluation of neutrophil extracellular traps signature predicts clinical outcomes and immunotherapy response in hepatocellular carcinoma. Front Immunol. 2023;14:1134521. doi:10.3389/fimmu.2023.1134521
9. Vithayathil M, Koku D, Campani C, et al. Machine learning based radiomic models outperform clinical biomarkers in predicting outcomes after immunotherapy for hepatocellular carcinoma. J Hepatol. 2025;83(4):959–970. doi:10.1016/j.jhep.2025.04.017
10. Zhang R, Peng W, Wang Y, et al. MRI radiomics model for predicting tumor immune microenvironment types and efficacy of anti-PD-1/PD-L1 therapy in hepatocellular carcinoma. BMC Med Imaging. 2025;25(1):211. doi:10.1186/s12880-025-01751-9
11. Liu J, Zhao N, Hang Y, et al. Predicting the outcome of transarterial chemoembolization combined with targeted immunotherapy for unresectable hepatocellular carcinoma based on MRI radiomics. Sci Rep. 2025;15(1):34782. doi:10.1038/s41598-025-18586-7
12. Min JH, Chen PJ, Qureshi TA, et al. Prediction of immunotherapy response in hepatocellular carcinoma patients using pretreatment CT images. Diagnostics. 2025;15(16):2090. doi:10.3390/diagnostics15162090
13. Chen J, Chen J, Ye Y, et al. Pretreatment multi-sequence contrast-enhanced MRI to predict response to immunotherapy in unresectable hepatocellular carcinoma using transformer: a multicenter study. J Cancer. 2025;16(8):2663–2672. doi:10.7150/jca.111026
14. Fan R, Shi YR, Chen L, et al. Hepatocellular carcinoma risk stratification for cirrhosis patients: integrating radiomics and deep learning computed tomography signatures of the liver and spleen into a clinical model. J Clin Transl Hepatol. 2025;13(9):743–753. doi:10.14218/JCTH.2025.00091
15. Song LN, Wang B, Cai JL, et al. Stratifying ICIs-responsive tumor microenvironment in HCC: from parsing out immune-hypoxic crosstalk to clinically applicable MRI-radiomics models. Br J Cancer. 2024;130(8):1356–1364. doi:10.1038/s41416-023-02463-z
16. Long S, Li M, Chen J, et al. Transfer learning radiomic model predicts intratumoral tertiary lymphoid structures in hepatocellular carcinoma: a multicenter study. J Immunother Cancer. 2025;13(3):e011126. doi:10.1136/jitc-2024-011126
17. Long S, Li M, Chen J, et al. Spatial patterns and MRI-based radiomic prediction of high peritumoral tertiary lymphoid structure density in hepatocellular carcinoma: a multicenter study. J Immunother Cancer. 2024;12(12):e009879. doi:10.1136/jitc-2024-009879
18. Peng K, Zhang X, Li Z, et al. Myeloid response evaluated by noninvasive CT imaging predicts post-surgical survival and immune checkpoint therapy benefits in patients with hepatocellular carcinoma. Front Immunol. 2024;15:1493735. doi:10.3389/fimmu.2024.1493735
19. Wang C, Leng B, You R, et al. A transcriptomic biomarker for predicting the response to TACE correlates with the tumor microenvironment and radiomics features in hepatocellular carcinoma. J Hepatocell Carcinoma. 2024;11:2321–2337. doi:10.2147/JHC.S480540
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
CT-Based Radiomics for the Recurrence Prediction of Hepatocellular Carcinoma After Surgical Resection
Wang F, Chen Q, Zhang Y, Chen Y, Zhu Y, Zhou W, Liang X, Yang Y, Hu H
Journal of Hepatocellular Carcinoma 2022, 9:453-465
Published Date: 23 May 2022
Trial Designs for Integrating Novel Therapeutics into the Management of Intermediate-Stage Hepatocellular Carcinoma
Su YY, Liu YS, Hsiao CF, Hsu C, Chen LT
Journal of Hepatocellular Carcinoma 2022, 9:517-536
Published Date: 2 June 2022
Bridging the Gap Between Imaging and Molecular Characterization: Current Understanding of Radiomics and Radiogenomics in Hepatocellular Carcinoma
Ren L, Chen DB, Yan X, She S, Yang Y, Zhang X, Liao W, Chen H
Journal of Hepatocellular Carcinoma 2024, 11:2359-2372
Published Date: 27 November 2024
Radiomics and Deep Learning as Important Techniques of Artificial Intelligence — Diagnosing Perspectives in Cytokeratin 19 Positive Hepatocellular Carcinoma
Wang F, Yan C, Huang X, He J, Yang M, Xian D
Journal of Hepatocellular Carcinoma 2025, 12:1129-1140
Published Date: 5 June 2025
A CT-Based Deep Learning Radiomics Scoring System for Predicting the Prognosis to Repeat TACE in Patients with Hepatocellular Carcinoma: A Multicenter Cohort Study
Dai Y, Zhao S, Wu Q, Zhang J, Zeng X, Jiang H
Journal of Hepatocellular Carcinoma 2025, 12:1647-1659
Published Date: 29 July 2025