Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Decoding Healthcare Workers’ Knowledge, Practice, and Attitude Toward Cough Etiquette: Is the Elbow Bump a Safe Greeting?
Authors Shalby AYM ![]() , Elbqry MG
, Elbqry MG ![]() , Elmansy FM
, Elmansy FM ![]() , Khorshid SM, Alawad AE
, Khorshid SM, Alawad AE
Received 28 October 2025
Accepted for publication 17 January 2026
Published 23 January 2026 Volume 2026:19 575561
DOI https://doi.org/10.2147/JMDH.S575561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Abeer Yahia Mahdy Shalby,1,2 Mohamed Goda Elbqry,3 Fatma Mohamed Elmansy,3 Sherif Mohamed Khorshid,4 Amal Elhaj Alawad5
1Department of Medical-Surgical Nursing, College of Nursing, Najran University, Najran, Saudi Arabia; 2Department of Medical-Surgical Nursing, Faculty of Nursing, Banha University, Banha, Egypt; 3Department of Medical-Surgical Nursing, College of Nursing, Qassim University, Buraydah, 51452, Saudi Arabia; 4Department of Infection Prevention and Control and Public Health, King Khalid Hospital, Najran, Saudi Arabia; 5Department of Microbiology, Collage of Medicine, Najran University, Najran, Saudi Arabia
Correspondence: Mohamed Goda Elbqry, Department of Medical-Surgical Nursing, College of Nursing, Qassim University, Buraydah, 51452, Saudi Arabia, Tel +966560403003, Email [email protected]
Background: Post-COVID-19, cough etiquette and safe greeting practices, such as the elbow bump, have gained prominence in healthcare settings to reduce respiratory infection transmission. However, evidence on healthcare workers’ knowledge, practice, and attitudes toward these measures remains limited.
Aim: This study aimed to assess the knowledge, practice, and attitudes of healthcare workers regarding cough etiquette techniques and the safety of elbow bump greetings and to examine the influence of demographic factors on these parameters.
Methods: A cross-sectional study was conducted among 216 healthcare workers using a structured, validated, self-administered online questionnaire over five months (May–October 2025). The questionnaire assessed demographics, knowledge (8 items), practice (7 items), and attitude (16 items) toward cough etiquette. Data were analyzed using descriptive statistics, Pearson correlation, and inferential tests to explore associations between variables.
Results: Slightly more than half of the participants demonstrated high knowledge (50.9%), while only 24.1% exhibited good practice, and 40.7% showed a positive attitude. Knowledge showed a weak positive correlation with practice (r = 0.129, p = 0.05), and practice was moderately correlated with attitude (r = 0.402, p < 0.001). Age, occupation, department, education, experience, and training were significantly associated with KAP scores, with Infection Control Unit staff and experienced nurses achieving higher scores.
Conclusion: Although healthcare workers possessed moderate to high knowledge, practical adherence and positive attitudes toward cough etiquette and elbow bump greetings were suboptimal. Practical, hands-on, and department-specific interventions are necessary to bridge the knowledge-practice gap and enhance adherence to infection control measures.
Keywords: healthcare workers, knowledge, attitude, practice, cough etiquette, elbow bump, safe greeting
Introduction
Cough etiquette is a fundamental component of respiratory hygiene and infection prevention, particularly among healthcare workers who are routinely exposed to patients with respiratory illnesses.1 Proper cough etiquette, including covering the mouth and nose during coughing or sneezing is widely promoted to reduce the transmission of infectious respiratory diseases (IRDs) and to protect both healthcare providers and patients.2 In clinical settings, consistent adherence to these practices is critical, as healthcare workers operate in close proximity to vulnerable populations and high-risk environments such as emergency departments, intensive care units, and triage areas.3
Post–COVID-19, research has increasingly focused on what has been described as “the coughing body”” emphasizing coughing not only as a biological event but also as a socially regulated behavior with implications for infection control.4 Public health authorities, including the World Health Organization (WHO), recommend coughing or sneezing into a tissue or the flexed elbow as a standard preventive measure.5 However, emerging evidence suggests that even when cough etiquette is practiced correctly, it may not fully prevent the release of infectious droplets and aerosols capable of penetrating deeply into the respiratory system.6
Laboratory and simulation-based studies have demonstrated that coughing into the elbow or sleeve does not entirely eliminate droplet dispersion and may still permit viral transmission, particularly if contact precautions are not followed.4 Additionally, respiratory viruses such as SARS-CoV-2 and influenza A (H1N1) have been shown to survive on textiles and surfaces for prolonged periods, raising concerns about indirect transmission through contaminated clothing.7 These findings highlight the potential limitations of cough etiquette when practiced in isolation without complementary infection prevention measures.
During the COVID-19 pandemic, alternative greeting behaviors most notably the elbow bump were widely adopted to replace handshakes and reduce direct hand-to-hand contact.8 While perceived as a safer social practice, elbow bumps typically occur at close interpersonal distances and may involve contact with areas of clothing previously exposed to respiratory droplets.6 Consequently, if an individual coughs or sneezes into their elbow and subsequently engages in an elbow bump, this behavior may inadvertently contribute to viral spread.3 Current evidence does not conclusively support the elbow bump as a fully safe greeting in healthcare or community settings without appropriate follow-up precautions.9
Despite growing international interest in cough etiquette and alternative greeting practices, limited research has examined healthcare workers’ knowledge, attitudes, and actual practices regarding these behaviors in Saudi Arabia. Moreover, gaps remain in understanding the alignment between knowledge and real-world adherence to cough etiquette, as well as perceptions of the safety of elbow bump greetings in clinical environments. Addressing these gaps is essential for informing infection prevention policies, refining training programs, and promoting safer behavioral practices among healthcare professionals.
Accordingly, this study aims to assess healthcare workers’ knowledge, practices, and attitudes toward cough etiquette, with particular attention to the perceived safety of elbow bump greetings and to examine the influence of demographic factors on these parameters, in a major Saudi healthcare setting.
Objectives
- To assess healthcare team knowledge and practice toward the use of cough etiquette technique.
- To determine healthcare team attitudes toward the use of cough etiquette technique.
- To examine the relationship between healthcare team knowledge, practice, and attitudes toward the use of cough etiquette technique and their demographic characteristics.
Methods
To Achieve the Study Objectives, a Cross-Sectional Descriptive Study Was Conducted
This design allows for an in-depth analysis of the target population and enables the exploration of relationships among knowledge, attitudes, and practices regarding cough etiquette techniques at a single point in time. The cross-sectional approach is appropriate for assessing current perceptions and behaviors within the healthcare team efficiently.
Setting
Data for the current study collected from the King Kalid Hospital (KKH) health care clusters, Najran City, Saudi Arabia. King Khalid Hospital is the sole reference and specialized hospital in the Najran region, serving as a central hub within the Najran Health Cluster of Saudi Arabia. Today, being a referral hospital only region multiplicity of services and specialties available by, and the largest in terms of the capacity of the clinical and operational capacity, which actually reached about 300 beds and adopted the health of Najran on King Khaled Hospital including owns the possibilities in the development of techniques of health care services new in the region.
Sampling and Population
A convenience sampling technique was employed in this study to recruit healthcare workers who were available and willing to participate during the data collection period. Participants were drawn from various departments and work shifts, including nurses, physicians, and allied health professionals who were directly involved in patient care within the selected healthcare settings. A total of 216 healthcare workers successfully completed the study survey.
The required sample size was determined using Cochran’s formula for sample size estimation for proportions, expressed as n = Z2 × p × (1 − p)/d2, where Z is the standard normal value corresponding to a 95% confidence level (1.96), p is the estimated proportion of the population possessing the characteristic of interest (assumed to be 0.5 to maximize the sample size), and d is the accepted margin of error (0.05). However, since the total number of healthcare workers in the study setting was approximately 450, a finite population correction was applied using the formula nf = n/[1 + (n − 1)/N], where N represents the total accessible population. After applying this correction, the adjusted sample size was approximately 214 participants, which was rounded to 216 to ensure adequate representation across all work shifts and departments. This final number was considered sufficient to achieve the study objectives with acceptable statistical precision and reliability.
Study Procedure
To implement the current study, the researchers followed a structured and ethical research process, detailed as follows:
Ethical Approval and Administrative Coordination
Ethical approval was obtained from the Ethics Committee of the KKH Cluster (IRB Log: April 2025–44A) prior to data collection. The study was conducted in accordance with the principles of the Declaration of Helsinki. All study-related documents, including the protocol, data collection instruments, and informed consent forms, were reviewed and approved. Official administrative permissions were obtained from KKH Specialist Hospital, ensuring institutional support and facilitating participant access across all selected departments and work shifts. Data confidentiality was strictly maintained by collecting data anonymously, restricting access to the research team only, and securely storing all study data in password-protected files.
Implementation Phase
Following the ethical and administrative approvals, the researchers coordinated with the participating hospitals to schedule suitable times for informing staff about the study. Eligible participants were briefed on the study objectives, confidentiality assurances, and the voluntary nature of participation. Informed consent was obtained prior to inclusion in the study. A secure link to the electronic questionnaire, developed using Microsoft Forms, was disseminated through institutional communication channels. This approach provided participants with the flexibility to complete the survey at their convenience and in a setting of their choice. All research activities were conducted in accordance with the policies, standards, and ethical guidelines of the KKH Cluster, ensuring regulatory compliance and fostering active participation.
A pilot study was conducted by distributing an electronic questionnaire link via Microsoft Forms to 10% of the intended participants (n = 22 nurses), who were later included in the final sample. The pilot phase aimed to evaluate the clarity, reliability, and feasibility of the data collection tool within the study context, and to estimate the average completion time, which was approximately five minutes. The instrument was developed based on a comprehensive review of relevant literature and subsequently finalized and formatted electronically. During the pilot phase, participants received detailed instructions regarding the study purpose, completion guidance, and clarification of any queries. The pilot study was administered in English during January 2025. As no major modifications were required following the pilot phase, the collected data were included in the final analysis. Major modifications were made to the instrument following the pilot study and therefore included in the final analysis.
Data Collection
Data were collected over a five-month period, from May to October 2025, using a structured, standardized, self-administered online questionnaire adapted from previous related studies.10–13 The questionnaire was administered electronically via Google Forms to ensure confidentiality, ease of access, and data security, allowing participants to complete it at their convenience while ensuring data security. It comprised the following validated and reliable sections.
Section (1): It was used to collect participants’ demographic and professional characteristics. It included age, gender, educational attainment, current work position, years of professional experience, and prior training related to infection control and respiratory hygiene.
Section (2): It was used to assess participants’ knowledge of cough etiquette techniques and the use of elbow bumps as a safe greeting. This section consisted of eight multiple-choice items, with correct answers scored as “1” and incorrect answers scored as “0.” yielding a total score ranging from 0 to 8. Sample items included statements such as respiratory etiquette alone is not a completely reliable method for preventing the spread of respiratory infections; the correct method of cough etiquette is to sneeze, blow the nose, or cough into a disposable tissue; used tissues should be discarded immediately, followed by hand hygiene using soap and water or an alcohol-based hand rub; and, when tissues are unavailable, coughing or sneezing into the upper arm or sleeve (elbow) while avoiding hand use is recommended.
The full questionnaire is provided via the above-mentioned electronic form as an online Supplementary Figure S1; Full Study Questionnaire to enhance transparency and enable full replication of the study.
Section (3): It was utilized to evaluate participants’ practice regarding cough etiquette through seven items, each scored from 1 to 2, with higher scores indicating better adherence to recommended practices. The total possible score ranged from 7 (lowest adherence) to 14 (highest adherence). Practice levels were categorized as good for scores ≥75% of the total (11–14 points), moderate for scores between 50% and 74% (7–10 points), and poor for scores below 50% (1–6 points). Sample practice items included behaviors such as covering the mouth and nose with a tissue when coughing or sneezing, disposing of used tissues immediately in a waste basket, avoiding coughing or sneezing into the hands, performing effective hand hygiene after coughing, sneezing, or touching used tissues, coughing or sneezing into the upper sleeve or elbow when tissues are unavailable, and wearing a face mask when advised to protect others.
Section (4): It was used to determine participants’ attitudes toward hand hygiene and cough etiquette using a 16-item Likert scale, with responses ranging from 1 (strongly disagree) to 5 (strongly agree). The total possible score ranged from 16 to 80, with higher scores indicating more positive attitudes. Scores above 60 were classified as a positive attitude, scores between 41 and 60 as neutral, and scores between 16 and 40 as negative. Sample items included statements such as: handwashing is very important at all times; wearing gloves does not replace handwashing; hand hygiene remains necessary after practicing cough etiquette; cough etiquette should always be adhered to for infection control; cough etiquette is important in hospital settings; cough etiquette is essential for preventing respiratory infections; coughing into the elbow alone is not sufficient to prevent infection; and coughing or sneezing into the elbow is widely recommended to reduce respiratory virus transmission.
2.5 The content validity of the questionnaire was established through review by a jury of five experts in medical-surgical nursing, who assessed the relevance, clarity, and comprehensiveness of all items. The experts confirmed that the questionnaire effectively captured the constructs of knowledge, practice, and attitudes regarding cough etiquette and safe greeting practices. The reliability of the knowledge section was assessed using Cronbach’s alpha, which demonstrated good internal consistency (r = 0.79). The practice section, measured with seven items on a 2-point scale, showed high reliability (r = 0.89), while the attitude section, assessed with a 16-item Likert scale, also demonstrated high internal consistency (r = 0.90). These results indicate that the questionnaire is both valid and reliable for assessing healthcare professionals’ knowledge, practices, and attitudes toward cough etiquette and elbow bump greetings in the study setting.
Statistical Design
Data were analyzed using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA). Categorical variables are presented as frequencies and percentages. Continuous variables were assessed for normality using the Kolmogorov–Smirnov test and are presented as mean ± standard deviation (SD) and range (minimum–maximum), as appropriate. Comparisons between two independent groups were performed using the Student’s t-test, while comparisons among more than two groups were conducted using one-way analysis of variance (ANOVA). Associations between knowledge, practice, and attitude scores were examined using Pearson’s correlation coefficient (r), with corresponding 95% confidence intervals (95% CI) calculated to assess the magnitude and precision of the observed associations. All tests were two-sided, and a p-value ≤ 0.05 was considered statistically significant.
Results
Table 1 presents that nurses constituted the largest professional group (59.3%), followed by physicians (25.9%). Most participants possessed a bachelor’s degree (71.3%) and had more than five years of professional experience (38.9%). The mean age of the respondents was 31.03 ± 6.39 years, with the predominant age group ranging from 18 to 25 years (40.7%). Additionally, more than half of the participants (56.5%) reported having received a related training course on cough etiquette.
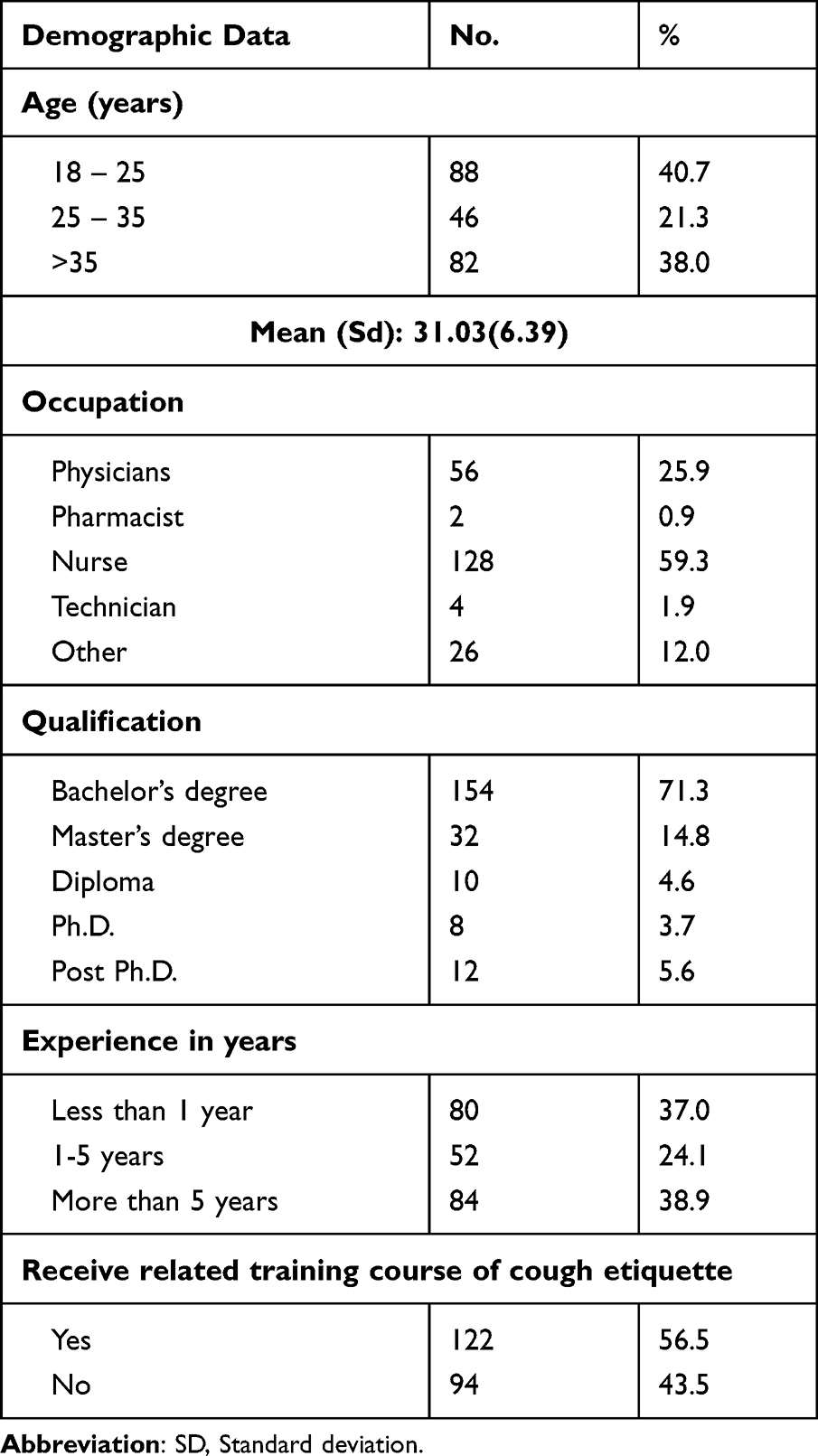 |
Table 1 Distribution of the Healthcare Team Studied According to Their Demographic Data. (n = 216) |
Table 2 illustrates that more than half of the participants demonstrated a high level of knowledge (50.9%), while only 24.1% exhibited good practice, and 40.7% showed a positive attitude. The mean percentage scores were 67.82 ± 21.91 for knowledge, 66.93 ± 35.05 for practice, and 60.33 ± 22.69 for attitude respectively.
 |
Table 2 Level of the Studied Healthcare Team According to Knowledge, Practice, and Attitude Score. (n = 216) |
Figure 1 demonstrates that the highest proportion of participants were from the “Other” departments (39.8%), followed by the Infection Control Unit (28.7%), Critical Care Unit (10.2%), and Clinical Outpatient Departments (9.3%). Smaller proportions were assigned to Inpatient Wards (8.3%), Emergency Units (1.9%), and Operation Rooms (1.9%).
 |
Figure 1 Distribution of the healthcare team studied according to working place. (n = 216). |
Figure 2. shows that most participants considered reliance on the elbow bump alone to be sufficient as a preventive measure, with 40.8% strongly agreeing and 18.5% agreeing. In contrast, 17.7% of participants reported neutral attitudes, while smaller proportions disagreed (9.2%) or strongly disagreed (13.8%).
 |
Figure 2 Distribution of the healthcare team studied according to attitude level of elbow-bump safety technique (n = 216). |
Table 3 shows a weak but statistically significant positive correlation between knowledge and practice levels (r = 0.129; 95% CI: −0.005 to 0.258p = 0.05), while no significant correlation was observed between knowledge and attitude (r = −0.009, CI: −0.142 to 0.125, p = 0.893). In contrast, a moderate positive correlation was identified between practice and attitude levels (r = 0.402, CI: 0.284 to 0.508, p < 0.001), indicating a more precise and meaningful association.
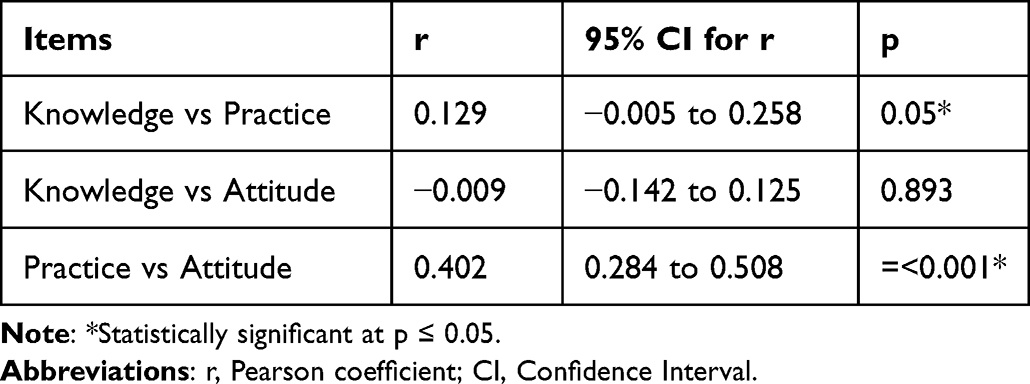 |
Table 3 Correlation Between the Studied Healthcare Team According to Knowledge, Practice, and Attitude Score. (n = 216) |
Table 4 shows that age had a statistically significant effect on practice and attitude scores (p = 0.021), with participants aged >35 years demonstrating higher mean scores. Occupation was significantly associated with practice (p = 0.003) and attitude (p = 0.042). Department significantly influenced knowledge (p < 0.001) and practice scores (p < 0.001), with participants from the Infection Control Unit exhibiting higher knowledge and practice scores compared with other units. Educational qualification had a significant effect on knowledge scores (p = 0.040). Years of experience were strongly associated with knowledge scores (p < 0.001), with participants having less than one year or more than five years of experience achieving higher scores. Attendance at a cough etiquette training course was significantly associated with attitude scores (p = 0.006); notably, higher attitude scores were observed among participants who had not received formal training.
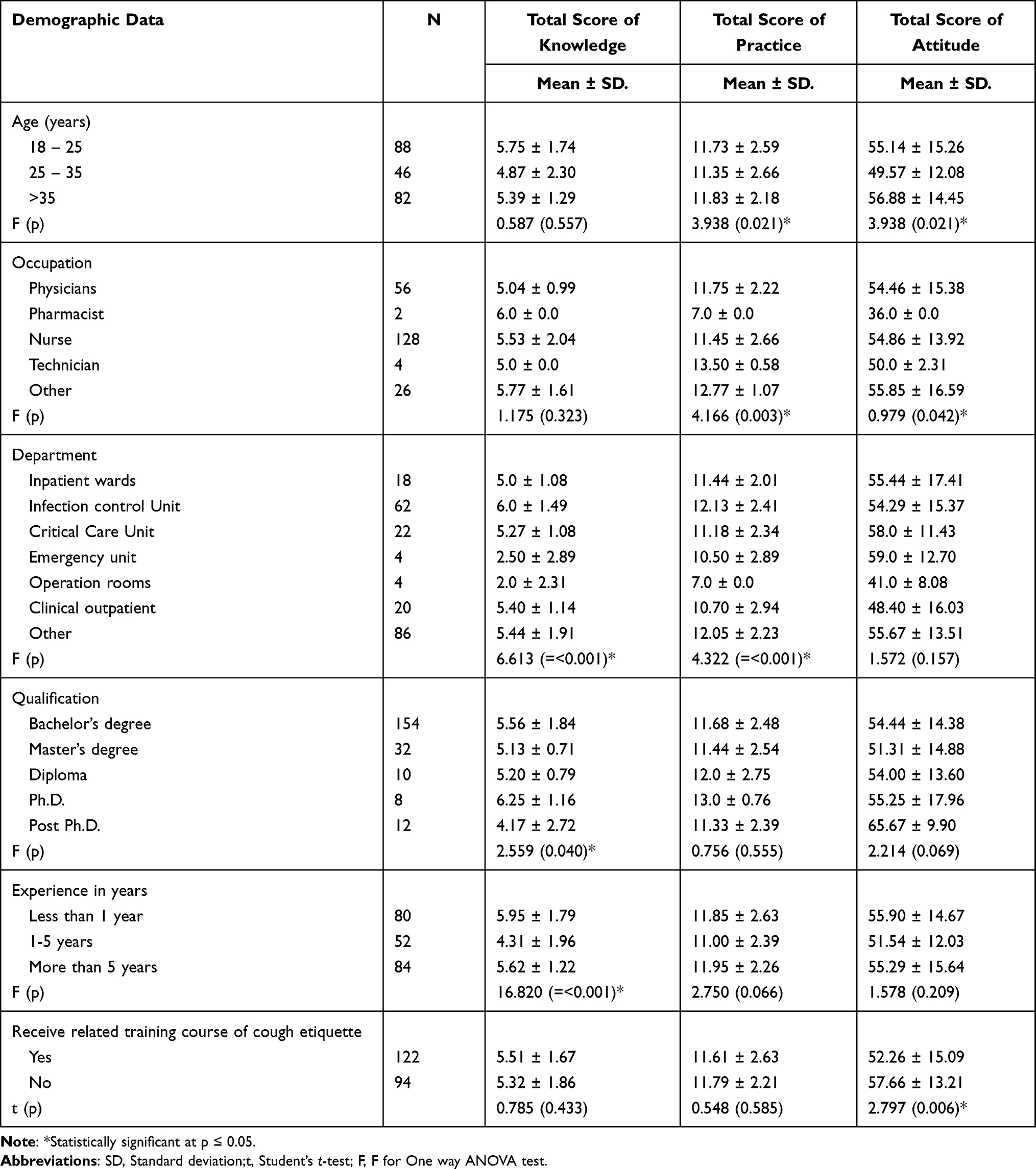 |
Table 4 Relation Between Total Score of the Studied Healthcare Team Knowledge, Practice, and Attitude Score with Demographic Data. (n = 216) |
Discussion
This study aimed to assess healthcare workers’ knowledge, practices, and attitudes toward cough etiquette and the safety of elbow bump greetings.
Demographic Profile & Professional Role
The demographic profile (Table 1), of the healthcare team (n = 216) reflects a predominantly young and well-educated workforce, with nurses forming the largest professional group (59.3%) and the majority holding a bachelor’s degree (71.3%). From the authors’ perspective, this composition likely contributes positively to the adoption of infection control measures, as nurses are typically at the frontline of patient care and play a pivotal role in implementing preventive practices. This aligns with findings by Compliance among Registered Nurses and Doctors in Critical Care Units: Challenges Affecting Their Adherence to Standard Precautions by Elseesy et al, which emphasized that nurses in critical care settings are central to infection-control adherence.14 However, it is important to note a contrasting viewpoint: some studies indicate that even a young, educated nursing workforce does not automatically result in improved infection-control practices. For example, the work by Knowledge, attitude and practice of healthcare workers towards healthcare‑associated infections in Jimma University Medical Center by Shacho et al, found that although knowledge and educational levels were high, practice and attitude remained suboptimal. From the authors’ viewpoint, this underscores that role and education alone are insufficient organizational culture, workload, and reinforcement mechanisms are critical to translating knowledge into practice.15
Age, Training & Institutional Investment
The mean age of participants (31.03 ± 6.39 years) and the predominance of professionals aged 18–25 years indicate a relatively young workforce. The authors suggest that younger professionals may be Showing increased adoption of contemporary hygiene practices, in line with worldwide trends of early-career healthcare workers actively participating in infection-control programs, reflecting global trends of increased engagement from early-career staff in infection-control initiatives. Importantly, 56.5% of participants reported having received training on cough etiquette, indicating moderate institutional investment in infection prevention. While training improves knowledge, the authors note that adherence to recommended practices may still vary, highlighting the importance of ongoing reinforcement and practical supervision that revealed by Abalkhail et al.16 Yet, in contrast, some reports show training alone does not guarantee better practice. For example, in the study by Al-Ahmari et al in Saudi Arabia, although over half of healthcare professionals had training in infection control, 49.5% still demonstrated poor practice levels.17 The authors interpret this discrepancy to mean that training must be interactive, sustained, and embedded within workplace culture, not just sporadic sessions.
Departmental Distribution
The distribution of participants across hospital departments (Figure 1), offers further insight. It shows that the largest proportion were from “Other” departments (39.8%), followed by the Infection Control Unit (28.7%), Critical Care Unit (10.2%), and Clinical Outpatient Departments (9.3%). Smaller proportions were from Inpatient Wards (8.3%), Emergency Units (1.9%), and Operation Rooms (1.9%). The authors interpret this as broad representation across hospital units, with strong inclusion of infection-control personnel who are directly responsible for hygiene protocols. However, lower representation from high-risk areas (Emergency Units, Operation Rooms) may reflect staffing or workload challenges, potentially limiting training and practice opportunities. This observation corresponds with Elbqryet al, and Elseesy et al, who highlighted that department‐specific responsibilities influence infection control adherence.13,14 On the other hand, it has been shown that departmental context sometimes does not significantly affect KAP outcomes. For instance, Yang et al, in Nanjing, China found no significant correlations between age, gender, professional title and knowledge levels across paediatric healthcare workers.18 The authors view this as suggesting that while departmental differences exist, the organizational infection-control infrastructure may exert greater influence than the unit itself.
Knowledge, Practice, Attitude Levels
Regarding knowledge, practice, and attitude levels (Table 2), more than half of participants demonstrated high knowledge (50.9%), whereas only 24.1% exhibited good practice, and 40.7% showed a positive attitude. The mean percentage scores were 67.82 ± 21.91 for knowledge, 66.93 ± 35.05 for practice, and 60.33 ± 22.69 for attitude. The authors point out a discrepancy between knowledge and practice, where solid theoretical knowledge does not consistently result in behavioural or attitudinal change. Similar findings were reported in Awwad et al, and Nassar et al, indicating that knowledge alone is insufficient to ensure consistent practice. Conversely, some studies report higher practice levels.12,19 For example, in the Abu Awwad et al of CT radiographers and nurses, practice scores were relatively high and positively correlated with attitude.12 The authors suggest that contextual factors such as institutional culture, monitoring, and availability of resources may explain variations across settings.
The distribution of attitudes toward elbow-bump safety observed (Figure 2) reflects ongoing debate in the other literature regarding the effectiveness of this practice as a preventive measure. The proportion of participants who agreed or strongly agreed with relying on the elbow bump is consistent with public health messaging and other study during the COVID-19 pandemic, in which elbow bumping was promoted as a safer alternative to handshaking to reduce direct hand contact.2,6 However, the notable proportion of participants who disagreed or expressed neutral attitudes aligns with other growing evidence indicating that coughing or sneezing into the elbow does not fully prevent droplet or aerosol dispersion and that contaminated clothing may act as a potential vehicle for viral transmission.9 From the authors’ perspective, these mixed attitudes are clinically significant and highlight a gap between simplified public health recommendations and the complex realities of infection transmission in healthcare settings. While elbow bumping may reduce direct hand-to-hand contact, it should not be considered a standalone protective strategy and must be complemented by strict hand hygiene, respiratory etiquette, and comprehensive infection prevention and control measures.5
Relationships and Correlations
Correlation analysis (Table 3) showed knowledge had a weak positive correlation with practice (r = 0.129, p = 0.05) but no significant correlation with attitude (r = –0.009, p = 0.893). In contrast, practice and attitude had a moderate positive correlation (r = 0.402, p < 0.001). From the authors’ perspective, these results indicate that behavioural practice is more closely associated with attitude than knowledge, reinforcing the notion that practical engagement and habitual performance drive attitudinal improvements more effectively than theoretical instruction alone that stated by Alshammari et al, and Kumar et al20,21 In disagreement, some literature suggests stronger knowledge-attitude links. For example, Shacho et al found knowledge directly influenced both attitude and practice in their structural equation model.15 The authors believe this divergence may stem from differences in methodology and typology of the behaviours studied including cough etiquette versus broader infection-prevention.
Demographic Associations
The association between demographic characteristics and KAP scores (Table 4) further clarifies influencing factors: Age significantly affected practice and attitude (p = 0.021), with participants over 35 years achieving higher scores. Occupation was associated with both practice (p = 0.003) and attitude (p = 0.042), with nurses and infection-control personnel demonstrating superior adherence. Department influenced knowledge (p < 0.001) and practice (p < 0.001), with Infection Control Unit staff scoring highest. Educational qualification significantly affected knowledge (p = 0.040), and years of experience were strongly related to knowledge (p < 0.001), with both novice (<1 year) and experienced (>5 years) staff achieving higher scores. Interestingly, participants without formal training on cough etiquette had higher attitude scores (p = 0.006), suggesting informal experiential learning, peer modelling, or departmental culture may shape attitudes independently of structured courses. The authors interpret these findings as evidence that age, occupation, department, experience, and informal learning opportunities all influence KAP, and interventions should be tailored accordingly.
In contrast, the Nanjing study by Yang et al, found no significant correlations between age or professional title and KAP outcomes, challenging the assumption that experienced or older staff necessarily perform better.18 The authors view such discrepancies as indicative of institutional variation highlighting that local context, mentorship, and unit culture may modulate demographic influences. Despite the valuable insights, several limitations are acknowledged. First, the use of convenience sampling may limit generalizability. Second, data were collected via self-administered electronic questionnaires, introducing social-desirability and reporting bias. Third, the cross-sectional design prevents causal inferences between knowledge, practice, and attitudes. Fourth, under-representation of high-risk units (Emergency, Operation Rooms) may restrict comprehensive unit-based conclusions. Future research should consider longitudinal designs, direct observation of practices, and larger multi-centre samples to strengthen evidence.
Conclusions
The study revealed that healthcare workers in the studied hospital possess moderate to high knowledge regarding cough etiquette; however, adherence to recommended practices and positive attitudes remain suboptimal. A knowledge-practice gap was evident, and attitudes were more closely associated with practical adherence than with theoretical knowledge. Demographic factors, including age, occupation, department, education, experience, and informal learning, significantly influenced knowledge, practice, and attitudes.
Implications for Practice
The findings carry several important implications for healthcare practice:
- Targeted Training and Reinforcement: Hospitals should implement hands-on, department-specific training programs on cough etiquette, emphasizing practical application rather than solely theoretical knowledge.
- Monitoring and Feedback: Regular monitoring and feedback on adherence to respiratory hygiene practices can help bridge the knowledge-practice gap and promote sustained behavioral change.
- Department-Specific Interventions: Special attention should be given to underrepresented or high-risk departments, such as Emergency and Operation Rooms, to ensure consistent practice across all units.
- Cultivation of Positive Attitudes: Interventions should aim to enhance attitudes toward infection control through modeling, peer reinforcement, and organizational culture initiatives.
- Policy and Guidelines Development: Hospital administrators can use these findings to update and refine infection prevention protocols, particularly in the context of post-COVID-19 practices such as elbow bumps.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Informed Consent Statement
Permission obtained from all participants before data collection.
Acknowledgments
The researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2026). The authors would like to express their sincere gratitude to the administration and staff of KKH Specialist Hospital for their cooperation and support throughout the study. We also extend our appreciation to all healthcare professionals who participated in this research for their time, effort, and valuable contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
A Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2026).
Disclosure
The authors report no conflicts of interest related to this study.
References
1. Steimle MD, Steenblik J, King BD, et al. A pilot study of coughing into the shirt to disrupt respiratory pathogen transmission. Int J Emerg Med. 2025;18(1):94. doi:10.1186/s12245-025-00892-6
2. Bailey C, Johnson P, Moran J, et al. Simulating the environmental spread of SARS-CoV-2 via cough and the effect of personal mitigations. Microorganisms. 2022;10(11):2241. doi:10.3390/microorganisms10112241
3. Brown N, Nettleton S, Buse C, Lewis A, Martin D. The coughing body: etiquettes, techniques, sonographies and spaces. Biosocieties. 2021;16(2):270–12. doi:10.1057/s41292-020-00196-3
4. Wulandari R, Sifai IA. Health education improves knowledge of healthy living and cleanliness behavior for upper respiratory infection prevention. In: International Seminar and Workshop Public Health (ISWHOPHA 2023). Atlantis Press; 2024:187–196.
5. Maude RR, Jongdeepaisal M, Skuntaniyom S, et al. Improving knowledge, attitudes and practice to prevent COVID-19 transmission in healthcare workers and the public in Thailand. BMC Public Health. 2021;21(1):749. doi:10.1186/s12889-021-10768-y
6. World Health Organization “WHO”. Infection prevention and control. Available from: https://www.who.int/teams/integrated-health-services/infection-prevention-control.
7. Madzinga D, Tshitangano TG, Raliphaswa NS, Razwiedani L. Healthcare workers’ perception of measures to reduce the risk of new tuberculosis infections: a qualitative study report. Nursing Reports. 2022;12(4):873–883. doi:10.3390/nursrep12040084
8. Jami A, Qureshi AA, Memon AM, Tunio RA, Khan H, Tariq AB. Impact of cough etiquettes in compliance with preventive measures from airborne disease: a cross-sectional study among symptomatic respiratory patients.
9. Jefferson T, Dooley L, Ferroni E, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Sys Rev. 2023;1(1). doi:10.1002/14651858.CD006207.pub6
10. Olajuyin OA, Olajide TG, Ogunboyo OF, Olajuyin AB, Olajuyin AA, Deji SA. Knowledge and practice of sneeze and cough etiquettes among participants in a randomized study in Ekiti-State, South-Western Nigeria. J Tropical Dis. 2019;7(6):1–5.
11. Elagib MF, Baldo SM, Tawfig A, Alqarni MA, Ghandour IA, Idris AM. Knowledge, attitude, and practice regarding infection control measures among dental students during COVID-19 pandemic. Archiv Envir Occup Health. 2022;77(6):455–467. doi:10.1080/19338244.2021.1931796
12. Abu Awwad D, Hill S, Lewis S, Jimenez Y. Knowledge, attitudes and practice of infection prevention and control in the CT suite. BMC Health Serv Res. 2023;23(1):741. doi:10.1186/s12913-023-09779-9
13. Elbqry MG, Elmansy FM, Elsayed AE, et al. Effect of COVID-19 stressors on healthcare workers’ performance and attitude at Suez Canal university hospitals. Middle East Curr Psych. 2021;28(1):4. doi:10.1186/s43045-021-00084-x
14. Elseesy NA, Al-Zahrani AE, Kandil FS, Mahsoon A, Elhady MM. Compliance among registered nurses and doctors in critical care units: challenges affecting their adherence to standard precautions. Healthcare. 2023;11(22):2975. doi:10.3390/healthcare11222975
15. Shacho E, Ambelu A, Yilma D. Knowledge, attitude, and practice of healthcare workers towards healthcare-associated infections in Jimma University Medical Center, southwestern Ethiopia: using structural equation model. BMC Health Service Res. 2024;24(1):1611. doi:10.1186/s12913-024-12094-6
16. Abalkhail A, Al Imam MH, Elmosaad YM, et al. Knowledge, attitude and practice of standard infection control precautions among health-care workers in a university hospital in Qassim, Saudi Arabia: a cross-sectional survey. Int J Envir Res Public Health. 2021;18(22):11831. doi:10.3390/ijerph182211831
17. Al-Ahmari AM, AlKhaldi YM, Al-Asmari BA. Knowledge, attitude and practice about infection control among primary care professionals in Abha City, Kingdom of Saudi Arabia. J Fam Med Primary Care. 2021;10(2):662–668. doi:10.4103/jfmpc.jfmpc_1278_20
18. Yang R, Yan W, Wang X, et al. Attitudes and practices towards risk of basic nosocomial infection control among pediatric healthcare workers: a cross-sectional study in Nanjing, China. Front Public Health. 2025;13:1599686. doi:10.3389/fpubh.2025.1599686
19. Nassar AA, Al Serouri AA, Al-Shahethi AH, Almoayed KA. Effectiveness of training on health care workers’ knowledge, attitude and practice regarding COVID-19 infection prevention and control, Yemen, 2021. BMC Health Service Res. 2024;24(1):1411. doi:10.1186/s12913-024-11927-8
20. Alshammari SA, Alrasheed SS, Alruhaimi WA, et al. Knowledge, attitude, and practice of standard infection control precautions among medical students at King Khalid University Hospital. Cureus. 2024;16(6).
21. Kumar A, Janmeja AK, Manchanda R, Singh B, Lakra A, Gupta R. A descriptive study to assess the knowledge and practices related to cough and sneeze etiquette among health care providers, respiratory patients and their attendants in a tertiary care centre. Int J Commun Med Public Health. 2023;10(12):4712. doi:10.18203/2394-6040.ijcmph20233768
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.