Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Decline in FEV1 and hospitalized exacerbations in individuals with severe alpha-1 antitrypsin deficiency
Authors Hiller AM ![]() , Piitulainen E, Jehpsson L, Tanash H
, Piitulainen E, Jehpsson L, Tanash H
Received 2 December 2018
Accepted for publication 1 April 2019
Published 23 May 2019 Volume 2019:14 Pages 1075—1083
DOI https://doi.org/10.2147/COPD.S195847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Adriana-Maria Hiller,1 Eeva Piitulainen,1 Lars Jehpsson,2 Hanan Tanash1
1Department of Respiratory Medicine and Allergology, Skåne University Hospital, Lund University, Lund, Sweden; 2Department of Clinical Sciences, Skåne University Hospital, Lund University, Lund, Sweden
Background and aim: The value of the forced expiratory volume in one second (FEV1) is useful in the diagnosis and prognosis of chronic obstructive pulmonary disease (COPD). Previous studies on lung function in individuals with severe alpha-1 antitrypsin deficiency (AATD) have shown a variable annual decline in FEV1 (∆FEV1). The aim of this study was to analyze ∆FEV1 and to identify risk factors for ∆FEV1 in individuals with severe AATD.
Material and methods: Data on smoking habits, symptoms, results of lung function tests and exacerbations were obtained from the Swedish AATD Register and the Swedish National Patient Register (SNPR). The ∆FEV1 was analyzed by random-effects modeling and adjusted for age and FEV1 at baseline.
Results: One hundred and four (9%) current smokers, 539 (48%) ex-smokers and 489 (43%) never-smokers were included in the study and followed-up from 1991 to 2016. A total of 584 (52%) individuals with severe AATD had COPD at inclusion. The median (IQR) annual severe exacerbation rate was 0.66 (1.4). The adjusted mean ∆FEV1 was significantly higher in the current smokers compared with the ex-smokers and never-smokers (70 [95% CI 56–83] vs 42 [95% CI 36–48] and 32 [95% CI 25–38) mL·yr−1,], in the middle–aged individuals compared with the young individuals (48 [95% CI 41–55] vs 32 [95% CI 18–45] mL·yr−1,), in the individuals with respiratory symptoms at inclusion compared with the asymptomatic individuals (46 [95% CI 40–52] vs 30 [95% CI 22–38]mL·yr−1,), and in the individuals with frequent exacerbations compared with those with infrequent exacerbations (57 [95% CI 47–68] vs 27 [95% CI 17–37] mL·yr−1,).
Conclusion: Active smoking, age, respiratory symptoms at baseline and repeated severe exacerbations of COPD are factors associated with an accelerated decline of lung function in individuals with severe AATD.
Keywords: alpha-1 antitrypsin, decline, exacerbation, lung function, smoking
Introduction
The hereditary disorder, severe alpha-1 antitrypsin (AAT) deficiency, is characterized by reduced serum levels of AAT.1 The genetic defect results in polymerization and misfolding of the AAT molecule in the hepatocytes and to its accumulation in the liver, leading to a decreased quantity of AAT in the circulation.2 Individuals with normal AAT alleles (PiMM) are protected by the circulating AAT in the lungs against the proteolytic activity of neutrophil elastase, which destroys elastin, a supporting protein of the lung parenchyma.2 The main clinical manifestation and the most frequent cause of disability and death associated with severe deficiency of AAT are panacinar emphysema.2 Smoking is the primary environmental risk factor for developing emphysema, and AAT-deficient smokers are at risk of developing early-onset emphysema.2 Smokers with severe alpha-1 antitrypsin deficiency (AATD) have an increased mortality risk compared to nonsmokers.3 Never-smoking individuals with severe AATD, who are identified by screening, seem to have a similar survival rate as the general population.4
The forced expiratory volume in one second (FEV1) is useful in the diagnosis and prognosis of chronic obstructive pulmonary disease (COPD).5 Since Fletcher and Peto described the natural history of FEV1, the rate of decline in FEV1 serves as a marker of the degree of airway obstruction and so of chronic respiratory disease progression.6 Also in healthy individuals, FEV1 changes with age, increasing during childhood to a stage through early adulthood and decreasing thereafter in a relatively linear fashion during adulthood, showing an accelerating decline in the elderly.5,6 In COPD, previous publications have addressed age, dyspnea, continuing smoking, poor bronchodilator response and exacerbation frequency as important prognostic factors10 The initial value of FEV1 has been reported as an accurate predictor of respiratory mortality.8,11
Studies on lung function in individuals with severe AATD have been sparse and included only a limited number of patients, mostly identified by respiratory symptoms.20 Variable annual decline in FEV1 has been reported, with mean values between 41 and 88 mL·yr−1, according to smoking status and COPD severity.20 The aim of this study was to estimate the rate of decline in lung function in individuals with severe AATD, by including a large number of subjects who are identified for reasons other than respiratory symptoms and not receiving regular AAT augmentation therapy. The second aim was to identify factors involved in the rapid decline in lung function.
Methods
Study population and data collection
Data on the individuals with severe AATD in this study were collected from the Swedish National AAT Deficiency Register, which is described elsewhere.21 Criteria for inclusion in the register are written informed consent, diagnosis of severe AAT deficiency (phenotypes PiZZ, PiZNull or PiNullNull) performed by isoelectric focusing and age ⩾18 years. Clinical examination and lung function tests were performed at the patients’ local hospital every 2 years and reported by the attending physician to the AATD register via a questionnaire.
Details on smoking habits were also obtained from the questionnaire. Smoking status was based on the subjects’ self-reports and was divided into three groups: never-, ex- and current smokers. A smoker who stopped smoking during the follow-up period was defined as a “quitter”. A subject was defined as having a respiratory symptom if he or she reported cough, phlegm, dyspnea or wheeze. Based on the age at inclusion in the AATD register, we stratified the individuals into three age subgroups: “young” for individuals aged 18–39 years, “middle-aged” for those aged 40–59 years and “old” for those ≥60 years. None of the patients included in the present analysis received regular AAT augmentation therapy.
Lung function tests
Spirometry including FEV1 and forced vital capacity (FVC) was performed at the patients’ local hospital. Lung volume measurements were made in accordance with the European recommendations.22 The spirometric data are expressed in liters (L) and as a percentage of the predicted reference values according to the European standards.22 In patients with COPD at inclusion (FEV1/FVC ratio below 0.70), the airflow limitation severity was divided into four groups according to the Global Initiative of Lung Disease (GOLD) guidelines; GOLD I FEV1≥80% predicted, GOLD II 50%≤FEV1<80% predicted, GOLD III 30%≤ FEV1<50% predicted and GOLD IV FEV1<30% predicted.11
Decline in FEV1 (∆FEV1)
∆FEV1 is expressed as mL·yr−1. Pre-bronchodilator values were analyzed. In order to analyze the rate of decline in FEV1, the criteria for inclusion in the study were the results of at least 3 spirometric tests at 2-year intervals (or longer) during the whole follow-up time.
Exacerbations
Data on severe exacerbations in individuals with severe AATD and COPD at inclusion were obtained from the Swedish National Patient Register (SNPR). The AATD register was cross-linked with the SNPR using the Swedish system of personal identity numbers. The SNPR covers more than 99% of all hospitalizations since 1987 and about 80% of all hospital-based outpatient care since 2001 nationwide.23 The register contains information regarding hospitalizations, diagnoses, date of admission, age and national identification number. Missing information regarding hospital admissions is estimated to be <1% per year. In this study, hospital admission diagnoses after inclusion in the register due to respiratory diseases were included. Diagnoses were coded according to the 9th (before 1996) and the 10th revisions of the WHO International Classification of Disease (ICD).24,25 ICD codes were grouped (ICD-9; ICD-10). Exacerbations were identified using the diagnosis code for inpatient hospitalizations with a COPD diagnosis code (491–492; J43-J44) in the first position, a diagnosis code for acute exacerbation (466; J440, J441), pneumonia (480–488; J189) or respiratory failure (786A, 799B; J96) in the second position, or the COPD diagnosis code in the second position, and acute exacerbation, pneumonia or respiratory failure diagnosis code in the first position. Patients were followed-up prospectively from the date of inclusion in the register until the date of lung transplantation (LT), lung volume reduction surgery (LVRS), death or study end (June 1, 2016).
The annual exacerbation rate of each individual was estimated as the fraction of the total number of exacerbations and the total number of days he/she participated in the study and multiplying the result by 365. Individuals experiencing more than the median annual exacerbation rate were classified as suffering from frequent exacerbations, while those having less than the median exacerbation rate were classified as suffering from infrequent exacerbations. This kind of division has earlier been reported in studies on COPD exacerbations of similar design as the present study.9,10
Ethical considerations
The study was approved by the Lund University Regional Ethical Review Board (2015/186). In accordance with Swedish research regulations for register-based research, individual patient consent on being included in a study was not required.
Statistical analyses
Baseline data were tabulated using frequencies and percentages for categorical variables and means with SD for normally distributed, continuous variables. Comparisons of continuous variables with normal distribution were analyzed using ANOVA and post hoc Tukey. The individual’s first reported FEV1 measurement at inclusion in the registry was treated as baseline data. The follow-up time for the analysis of ∆FEV1 was defined as the time from the date of the spirometry at inclusion to the first of the following occurrences: LT, lung volume reduction surgery (LVRS) and death or study end (June 1, 2016).
∆FEV1 was analyzed by random-effects modeling,26,27 which included ∆FEV1 (mL·yr−1) as the dependent variable, age at baseline, FEV1 at baseline and follow-up time as covariates, gender, smoking habits, presence of respiratory symptoms and COPD as fixed factors, and the individual patients as random-effects factors. In order to visualize the interaction of age and FEV1 at baseline in predicting lung function decline, we analyzed the predicted values for lung function decline (mL·yr−1) from a linear regression model, using age group and FEV1 at baseline as independent variables, with an interaction term between these two. A p-value <0.05 was considered significant. Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS), version 23.0 (IBM Corporation, Armonk, NY, USA).
Results
Up to June 2016, a total of 1,640 individuals with severe AATD were included in the Swedish National AATD Register. Of these, 1,132 had undergone three or more spirometries and were included in the study. The enrollment flow is presented in Figure 1. The demographic baseline data are shown in Table 1. Thirty patients underwent LVR surgery and 86 underwent LT. The initial reasons for AAT analysis were: respiratory diseases or symptoms in 42% (n=472), liver disease in 7% (n=81), other diseases or symptoms in 27% (n=304) and family/population screening in 24% (n=275).
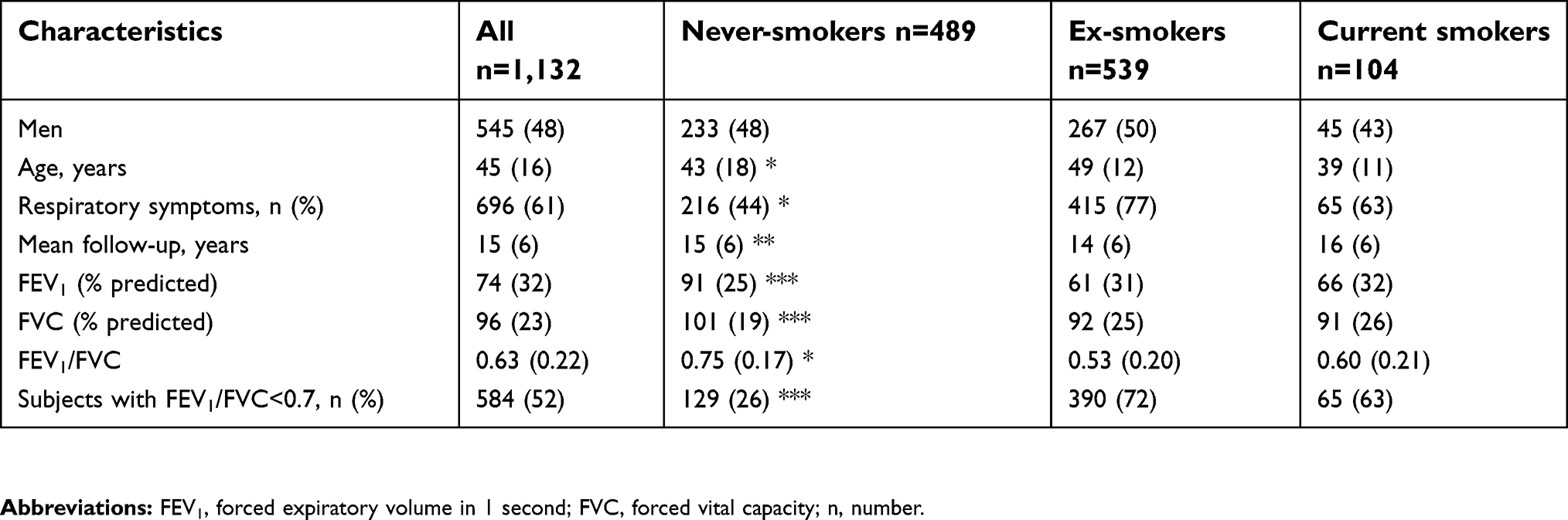 | Table 1 Demographic data of the study population at baseline, stratified by smoking habits |
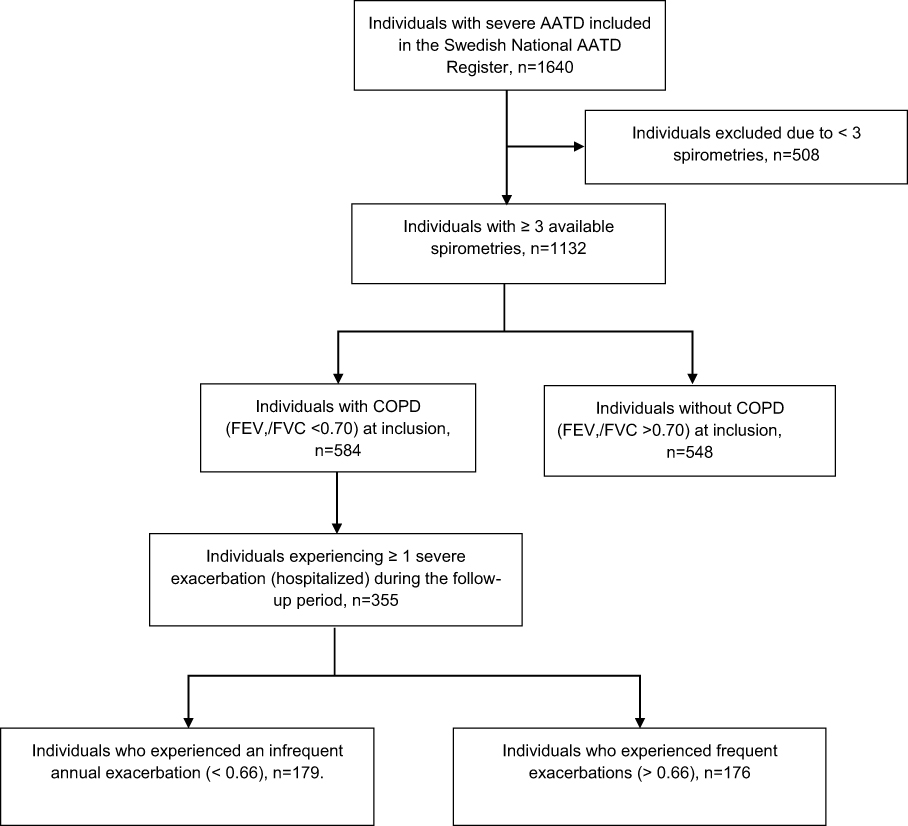 | Figure 1 Consort diagram detailing the enrollment flow in the present study.Abbreviations: AATD, alpha-1 antitrypsin deficiency; COPD, Chronic Obstructive Pulmonary Disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; n, number |
Smoking habits
The FEV1 % of predicted was significantly higher in the never-smokers compared with the current and ex-smokers, Table 1. The current smokers were significantly younger and had a higher tobacco consumption than the ex-smokers, and the mean (range) number of pack-years was 18.2 (0.96–77) and 13.7 (0.1–116), respectively, p<0.001. Of the 104 current smokers at inclusion, 73 (70%) stopped smoking during the follow-up. The median time between inclusion and abstaining from smoking was 2.3 years (range 0.1–17). The mean number of pack-years for the quitters was 21 (range 1.5–98).
COPD exacerbations
Of the 1,132 AATD individuals included in the present study, 584 (52%) were diagnosed as having COPD at the time of inclusion in the AATD Register. Of these, 65 (11%) were current smokers, 390 (67%) were ex-smokers and 129 (22%) were never-smokers.
Of the 584 patients with COPD, 355 (61%) experienced one or more severe exacerbations (admitted to hospital with the diagnosis COPD exacerbation) during the follow-up period. The overall median (interquartile range [IQR]) annual exacerbation rate was 0.66 (1.4). Frequent exacerbations (annual rate >0.66) were found in 176 (30%) of the COPD patients.
Decline in FEV1
The median number of FEV1 measurements was 5 (range 3–15). The overall mean ∆FEV1 for the whole group was 40 (95% CI 36–44) mL·yr−1. The results of annual decline in FEV1 are shown in Table 2. The mean ∆FEV1 adjusted for age and FEV1 at baseline were significantly higher in the current smokers than in the never- and ex-smokers, whereas it did not differ significantly between the never- and ex-smokers. The adjusted mean ∆FEV1 among the quitters was 65 (95% CI 49–82) mL·yr−1. The adjusted mean ∆FEV1 was significantly higher in the middle-aged individuals compared with the young individuals, in the individuals with respiratory symptoms at inclusion compared with the asymptomatic individuals and in the individuals with COPD (FEV1/FVC <0.70) at inclusion compared with those with FEV1/FVC >0.70, Table 2. The number of pack-years of ≥10 was associated with greater ∆FEV1 than the number of pack-years of <10. Individuals with frequent exacerbations (annual rate >0.66) had a significantly greater decline compared with those with infrequent exacerbations. The interaction of age (years) and FEV1 at baseline (mL) in predicting lung function decline (mL·yr−1) is shown in Figure 2.
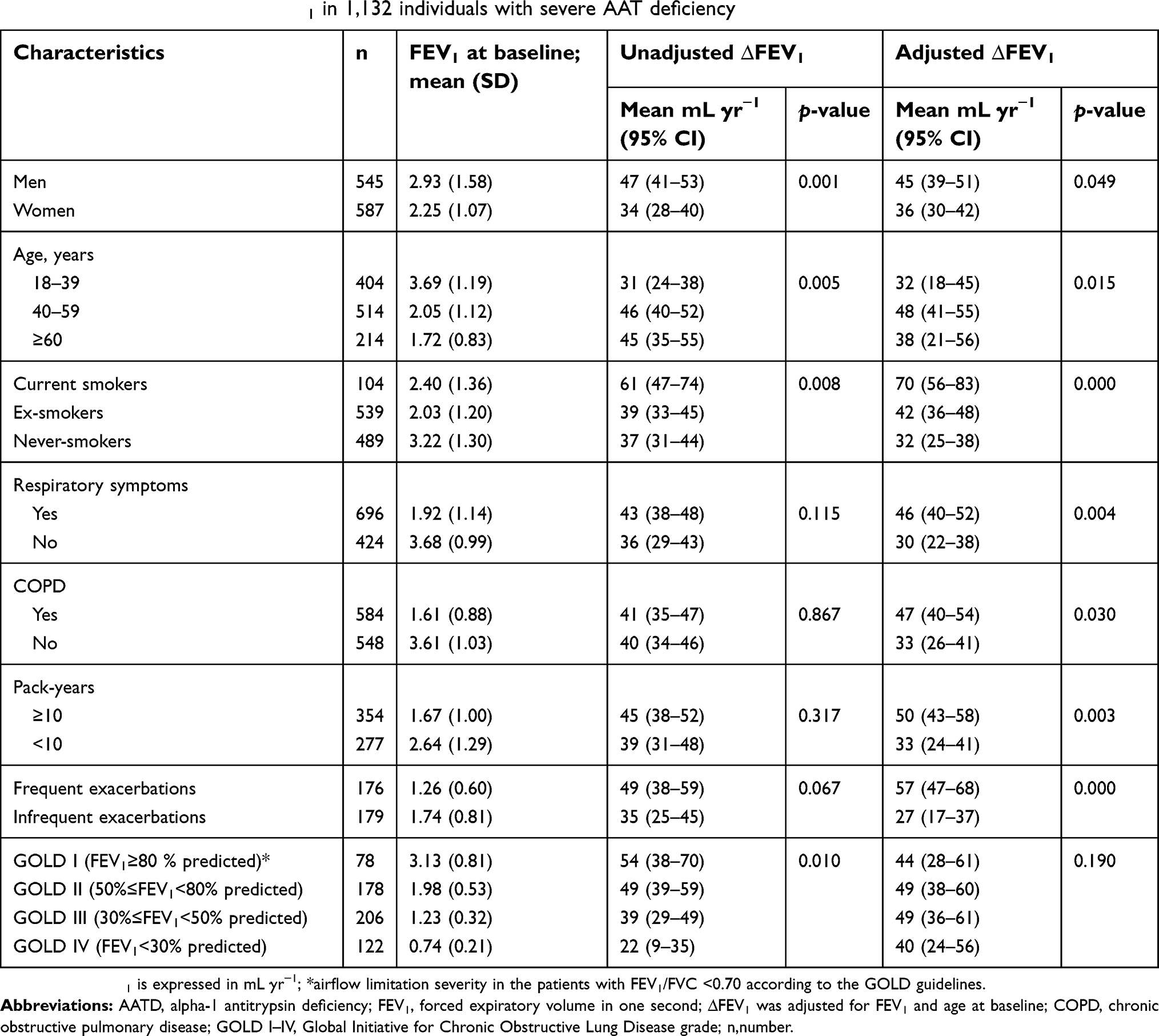 | Table 2 The annual decline in FEV1 in 1,132 individuals with severe AAT deficiency |
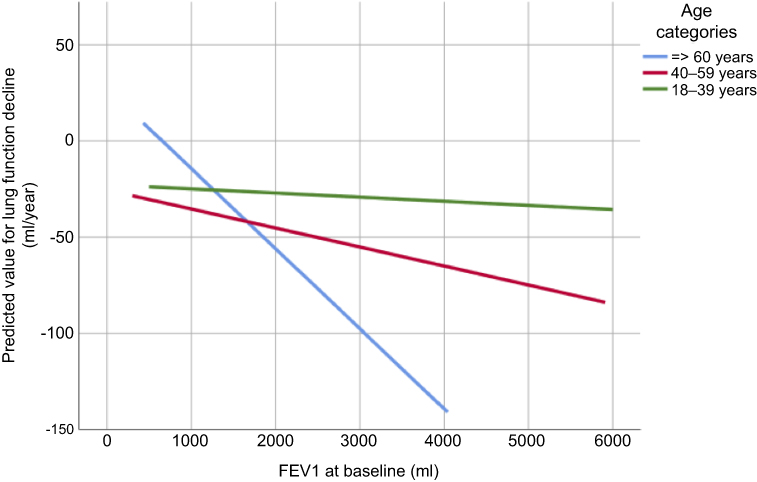 | Figure 2 The predicted values for lung function decline (mL·yr−1) from a linear regression model, using age group and FEV1 at baseline as independent variables, with an interaction term between these two. Abbreviations: mL, milliter; FEV1, forced expiratory volume in 1 second. |
Decline in FEV1 in previously published studies
Table 3 summarizes the results of the present study and of previously published data on the rate of decline in lung function according to smoking habits. The present study includes the largest number of individuals with severe AATD.
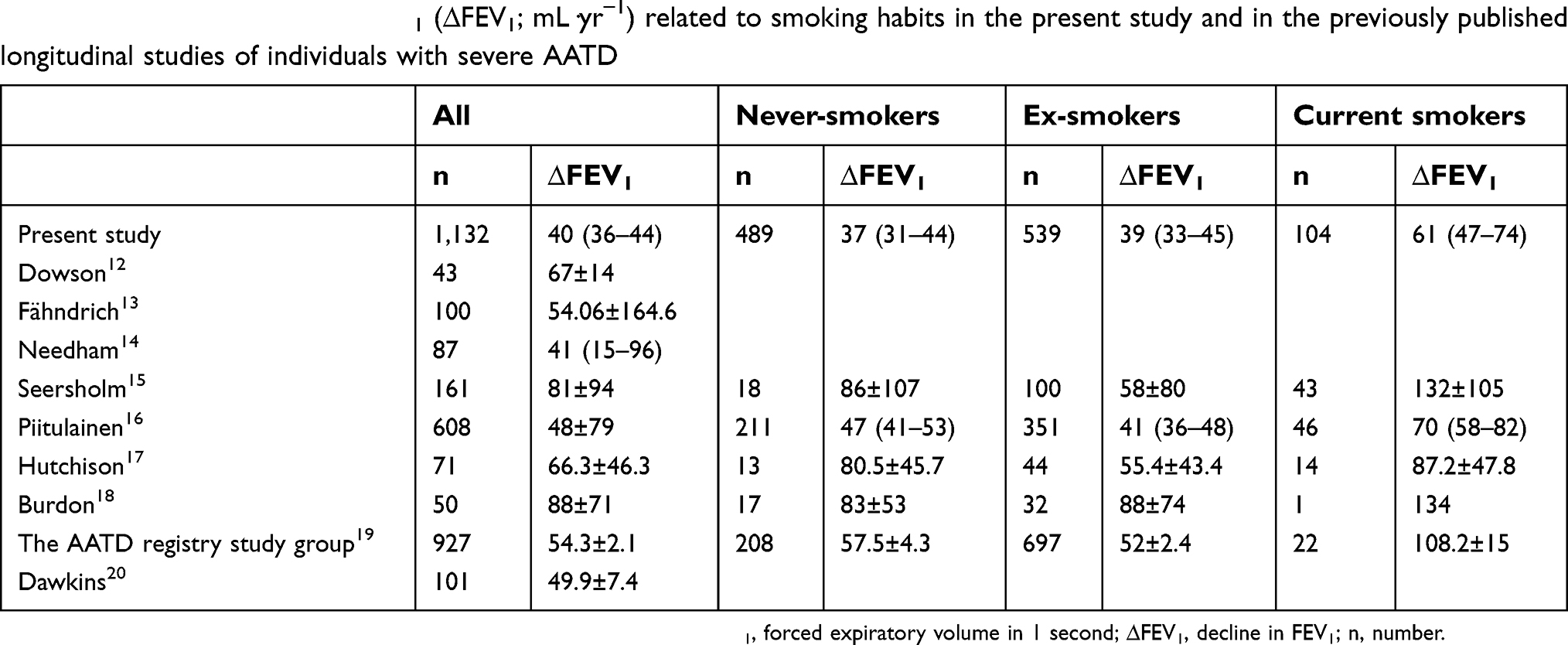 | Table 3 The annual decline in FEV1 (∆FEV1; mL·yr−1) related to smoking habits in the present study and in the previously published longitudinal studies of individuals with severe AATD |
Discussion
Main findings
This prospective, register-based study with a long follow-up time shows that the mean decline in FEV1 is 40 mL·yr−1 in 1,132 individuals with severe AATD, not receiving regular AAT augmentation therapy. The current smokers, men, middle-aged subjects and those with repeated exacerbations of COPD have an accelerated decline in FEV1. Our analysis extends the previously published studies by including a large number of never-smokers and individuals identified for reasons other than respiratory symptoms.
Previous studies of lung function in severe AAT-deficient individuals have reported a high variability in the rate of decline in FEV1, which has varied between 41 and 88 mL per year.20 The decline measured in these studies is greater than in our study. However, similar to our results, some studies have reported a greater decline in current smokers than in ex- and never-smokers.19 Various results on yearly decline have been reported in never-smokers, ranging from 47 mL to 86 mL per year.19 Some studies have even reported a greater decline in never-smokers than in ex-smokers.15,17 However, these studies have included only a limited number of never-smokers. Our results show an annual decline in FEV1 of 37 mL in 489 never-smokers. As in the previous analysis of data from the Swedish AATD Register, we did not find any significant difference in annual decline in FEV1 between the never- and ex-smokers.16 These results indicate that in smoking individuals with severe AATD, the decline in lung function returns to the same level as in the never-smokers, after smoking was stopped.
When lung function at baseline was divided into severity groups according to the GOLD criteria, we found a greater annual decline in FEV1 in the subjects with mild and moderate COPD (GOLD I and II) compared to those with severe COPD. However, the difference became insignificant after adjustment for FEV1 and age at baseline. This finding suggests that the decline in lung function is dependent on the initial FEV1. Thus, the individuals with severe AATD with initial, well-preserved lung function seem to have a sharper decline in FEV1 than those with low initial FEV1. Previous studies have reported that the greatest ∆FEV1 occurs in AAT-deficient patients with moderate COPD (FEV1 50–80% of the predicted value).19,20 The National Heart, Lung and Blood Institute (NHLBI) Register of Patients with Severe AATD has reported a decline of up to 76 mL yearly in AAT-deficient patients with moderate COPD (FEV1 50–80% of the predicted value).19 However, in this study, the follow-up period was only 57 months, and the majority of the 927 individuals had received AAT replacement therapy. In Dawkins’ study, the decline in moderate COPD was 90 mL per year.20 This study included a limited number of 101 individuals with severe AATD and 26 of them had moderate COPD. The follow-up period was 3 years. It is possible that these reasons influenced the results that overestimated the decline.
The FEV1 value is useful in the diagnosis of COPD in general, and a low FEV1 is a predictor for all-cause and respiratory mortality.7,8,11 Exacerbations have also been identified as a risk factor for a poorer prognosis in usual COPD.9,10 Up to 52% of the study population in our study had COPD at inclusion. The majority of the subjects with COPD had at least one severe exacerbation during the follow-up period. The median annual rate of severe exacerbations of 0.66 seems to be lower than has been reported in previous studies on exacerbations with a similar design, in patients with usual COPD and those with AATD. Makris et al have found a significant interaction between the exacerbation frequency and lung function decline in patients with usual COPD.10 They reported a median annual rate of 2.85 exacerbations in 102 patients with usual COPD over 3 years’ follow-up. However, 44% of the patients were smokers, and the exacerbations were self-reported. Needham et al have found that the average number of exacerbations in 265 AATD individuals was similar to that seen in non-AATD COPD.14 The mean number of exacerbations was 1.2±0.1 during the first year of the study, and no association was found between the presence of exacerbations and decline in FEV1 during the study period of 3 years.14 Dawkins et al have reported an annual rate of exacerbations that varied between 1.22 and 1.61 in 101 patients with severe AATD.20 We found that frequent exacerbations were associated with accelerated loss of FEV1. Our findings are in accordance with previous studies of usual COPD and in AATD patients.9,10,12,13,20
Clinical implication
Our findings provide new information on the decline in lung function in individuals with severe AATD. Patients with rapid decline should be offered intense pharmacological and nonpharmacological interventions that may mitigate their risk for further deterioration. The most important intervention is smoking prevention. The use of modern pharmacotherapy in COPD may help slow the rate of lung function decline and reduce further exacerbations. If this is to be of benefit, therapy should start early in the course of the disease.28 We have also identified risk factors for accelerated lung function impairment.
Strengths and limitations
An important strength in our study is that the data are accurate, being assembled from the well-established Swedish National Register of individuals with severe AATD with a correct diagnosis based on isoelectric focusing. The detection rate of severe AAT deficiency is relatively high (30%) in Sweden.21 A large proportion of the individuals with severe AATD in the register are never-smokers (45%) and have been identified for reasons other than respiratory symptoms, which increases the accuracy of the data. The follow-up period was long, from 1991 to 2016, which is another important strength that distinguishes the Swedish National AAT Register from other national registers of AATD.
The data on exacerbations were obtained from the Swedish National Patient Register with a high coverage of all hospitalizations. Diagnoses of exacerbations were accurate because they were made by the physicians at outpatient visits or during periods of hospitalization.
Limitations of the study: The lung function tests were performed at local hospitals throughout Sweden. Another limitation is that only pre-bronchodilator values were analyzed. Furthermore, we have not analyzed other risk factors for decline such as occupational exposure to airway irritants.
Conclusion
In individuals with severe AATD, the mean decline in FEV1 and the annual rate of exacerbations are lower than previously reported. Active smoking, age, respiratory symptoms at baseline and repeated exacerbations of COPD are factors associated with an accelerated decline of lung function.
Acknowledgments
We thank all the Swedish physicians who report data to the Swedish AAT-register. HT was supported by unrestricted grants from the Skåne University Hospital, Swedish Society of Medicine, and the Swedish Heart-Lung Foundation. EP was supported by unrestricted grants from the Swedish Heart-Lung Foundation.
Disclosure
The authors alone are responsible for the content and writing of the paper. The authors report no conflicts of interest in this work.
References
1. Laurell C-B, Eriksson S. The electrophoretic α-1-globulin pattern of serum in a α-1-antitrypsin deficiency. Scand J Clin Lab Invest. 1963;15:132–140. doi:10.1080/00365516309051324
2.
3. Tanash HA, Nilsson PM, Nilsson JA, Piitulainen E. Survival in severe alpha-1-antitrypsin deficiency (PiZZ). Respir Res. 2010;11:44. doi:10.1186/1465-9921-11-62
4. Tanash HA, Nilsson PM, Nilsson JA, Piitulainen E. Clinical course and prognosis of never-smokers with severe alpha-1-antitrypsin deficiency (PiZZ). Thorax. 2008;63:1091–1095. doi:10.1136/thx.2008.095497
5. Wise RA. The value of forced expiratory volume in 1 second decline in the assessment of chronic obstructive pulmonary disease progression. Am J Med. 2006;119(10 Suppl 1):4–11. doi:10.1016/j.amjmed.2006.08.002
6. Fletcher C, Peto R. The natural history of chronic airway obstruction. BMJ. 1977;1:1645–1648.
7. Anthonisen NR, Wright EC, Hodgkin JE;
8. Burrows B. Predictors of loss of lung function and mortality in obstructive lung diseases. Eur Respir Rev. 1991;1:340–345.
9. Donaldson GC, Seemungal TAR, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57:847–852. doi:10.1136/thorax.57.10.847
10. Makris D, Moschandreas J, Damianaki A, et al. Exacerbations and lung function decline in COPD: new insights in current and ex-smokers. Respir Med. 2007;101(6):1305–1312. doi:10.1016/j.rmed.2006.10.012
11.
12. Dowson LJ, Guest PJ, Stockley RA. Longitudinal changes in physiological, radiological, and health status measurements in alpha-1-antitrypsin deficiency and factors associated with decline. Am J Respir Crit Care Med. 2001;164:1805–1809. doi:10.1164/ajrccm.164.10.2106036
13. Fähndrich S, Bernhard N, Lepper PM, et al. Exacerbations and duration of smoking abstinence are associated with the annual loss of FEV1 in individuals with PiZZ alpha-1-antitrypsin deficiency. Respir Med. 2017;129:8–15. doi:10.1016/j.rmed.2017.05.011
14. Needham M, Stockley RA. Exacerbations in α1-antitrypsin deficiency. Eur Respir J. 2005;25:992–1000. doi:10.1183/09031936.05.00074704
15. Seersholm N. Kok-Jensen A, Dirksen A. Decline in FEV1 among patients with severe hereditary α1-antitrypsin deficiency type PiZ. Am J Respir Crit Care Med. 1995;152:1922–1925. doi:10.1164/ajrccm.152.6.8520756
16. Piitulainen E, Eriksson S. Decline in FEV1 related to smoking status in individuals with severe α1-antitrypsin deficiency (PiZZ). Eur Respir J. 1999;13:247–251.
17. Hutchison DCS, Cooper D. Alpha-1-antitrypsin deficiency: smoking, decline in lung function and implications for therapeutic trials. Respir Med. 2002;96:872–880.
18. Burdon JGW, Brenton S, Hocking V, et al. Decline in FEV1 in patients with PiZ alpha-1-antitrypsin deficiency: the Australian experience. Respirology. 2002;7:51–55.
19. The Alpha-1-antitrypsin Deficiency Registry Study Group. Survival and FEV1 decline in individuals with severe deficiency of α1-antitrypsin. Am J Resp Crit Care Med. 1998;158:49–59. doi:10.1164/ajrccm.158.1.9712017
20. Dawkins PA, Dawkins CL, Wood AM, Nightingale PG, Stockley JA, Stockley RA. Rate of progression of lung function impairment in α1-antitrypsin deficiency. Eur Respir J. 2009;33:1338–1344. doi:10.1183/09031936.00061208
21. Piitulainen E, Tanash HA. The clinical profile of subjects included in the Swedish National Register on individuals with severe alpha 1-antitrypsin deficiency (PiZZ). Copd. 2015;12(Suppl):36–41. doi:10.3109/15412555.2015.1021909
22. Quanjer PH. Standardized lung function testing. Report working party. Bull Eur Physiopathol Respir. 1983;19(Suppl 5):1–95.
23. Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450. doi:10.1186/1471-2458-11-450
24.
25.
26. Laird NM, Ware JH. Random-effects models for longitudinal data. Biometrics. 1982;38:964–974. doi:10.2307/2529876
27. Jennrich RI, Schluchter MD. Unbalanced repeated measures models with structured covariance matrices. Biometrics. 1996;42:805–820. doi:10.2307/2530695
28. Gladysheva E, Malhotra A, Owens R. Influencing the decline of lung function in COPD: use of pharmacotherapy. Int J COPD. 2010;5:153–164.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.