Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Decision-Making in Multidisciplinary Tumor Boards in Breast Cancer Care – An Observational Study
Authors Schellenberger B ![]() , Diekmann A
, Diekmann A ![]() , Heuser C
, Heuser C ![]() , Gambashidze N, Ernstmann N, Ansmann L
, Gambashidze N, Ernstmann N, Ansmann L ![]()
Received 1 January 2021
Accepted for publication 16 March 2021
Published 1 June 2021 Volume 2021:14 Pages 1275—1284
DOI https://doi.org/10.2147/JMDH.S300061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Barbara Schellenberger,1,2 Annika Diekmann,1,2 Christian Heuser,1,2 Nikoloz Gambashidze,3 Nicole Ernstmann,1– 3 Lena Ansmann4
1Center for Health Communication and Health Services Research (CHSR), Department for Psychosomatic Medicine and Psychotherapy, University Hospital Bonn, Bonn, Germany; 2Center for Integrated Oncology (CIO Bonn), University Hospital Bonn, Bonn, Germany; 3Institute for Patient Safety, University Hospital Bonn, Bonn, Germany; 4Division for Organizational Health Services Research, Department of Health Services Research, School of Medicine and Health Sciences, Carl von Ossietzky University Oldenburg, Oldenburg, Germany
Correspondence: Barbara Schellenberger Venusberg Campus 1, Bonn, 53127, Germany
Tel +49 228 287 13797
Email [email protected]
Purpose: Healthcare providers decide on recommendations for further treatment of patients with cancer in multidisciplinary tumor boards (MTBs). As such, communicative processes during MTBs are assumed to influence decision-making and, thereby, treatment planning. The aim of this exploratory study is to gain insights into decision-making during MTBs.
Methods: Case discussions from MTBs in breast cancer centers in North Rhine-Westphalia, Germany, were observed and audiotaped. The transcripts of the audio recordings were analyzed by procedures of conversation analysis.
Results: Based on 38 case discussions from 15 MTBs in four breast cancer centers, an action scheme for decision-making in MTBs in breast cancer care was developed. In addition, the conversational practices used by the participants during interactions were analyzed.
Conclusion: Analysis indicated that conventions in MTBs were observed during individual phases of decision-making but not for the entire process. Although exchanging multidisciplinary knowledge is an essential aspect of MTBs, this exchange does not always seem to occur in practice. The extent to which recommendations are derived from consensus during MTBs remains unclear. Thus, the study suggests developing standards for communication during MTBs to optimize decision-making and, thus, the quality of recommendation.
Keywords: breast cancer, communication, multidisciplinary treatment team, multidisciplinary tumor conferences, oncology
Introduction
Multidisciplinary Tumor Boards (MTBs) are regular meetings of a multidisciplinary treatment team, in which the diagnosis and treatment of patients with cancer are discussed and evidence-based recommendations are decided upon.1,2 Professionals from various disciplines are involved in cancer care due to the increased complexity of diagnosis and treatment.3 Thus, MTBs are established as a standard worldwide.4 Previous studies demonstrate that a multidisciplinary approach to treatment for breast cancer, where different treatment modalities are coordinated in a timely manner,5 leads to better results for patients and healthcare providers.6–12 Positive effects of treatment decision-making can be observed,9,13 indicating that patients are more frequently diagnosed and treated on the basis of relevant evidence-based guidelines.14
Multidisciplinary reasoning is an essential aspect of MTBs. In the medical context, the term refers to joint decision-making among different disciplines.15 Previous studies find that, in 2–52% of cases, team decisions established within MTBs relatively differ from individual decisions made by healthcare providers in terms of diagnosis and therapy.16–19
Communication is an essential factor during MTBs as a prerequisite to decision-making,20 which is a process that precedes the mere statement of a decision and is traceable by means of a transcript.21 The expected outcome of decision-making during MTBs is a treatment recommendation, which exerts a major impact on further therapeutic procedures. The recommendation influences the subsequent steps of the treatment process on the one hand and the quality of life8 of patients and further course of the disease on the other hand.
A previous study in cancer care using conversation analysis revealed that case discussions during MTBs can generally be categorized into the following phases through analysis of the transcript: opening, case presentation, provision of additional information, discussion, articulation of treatment plan, pre-closure, and closure.22 In another study, also using conversation analysis, 4% of case discussions in MTBs in breast cancer care directly started with the discussion, and in MTBs in gynecological cancer care, in 4% of case discussions the decision was not articulated.23
Several factors indicate that poor communication during MTBs leads to an insufficient exchange of multidisciplinary knowledge.24 Research indicates that certain circumstances surrounding and within MTBs can impede open communication and decision-making, such as the setting itself or the manner of presenting treatment options to patients. In a study conducted in Australia, approximately one-third of the interviewed physicians did not rate the MTB setting as conducive for discussion, especially if the prevailing opinion was evident.25 Similarly, a study in Germany observed several case discussions and reported that only one or a few high-ranking physicians contributed to such discussions.26 Further research demonstrates that if healthcare providers fail to agree on a treatment recommendation, then available options are less frequently presented in a neutral manner, thus resulting in the framing effect.27 As such, patients find difficulty in deciding against a physician’s preferred option.28
The majority of existing evidence related to MTBs are derived using quantitative methods29 or qualitative interviews that focus on the perspective of healthcare providers. To gain a deeper insight into the decision-making of MTBs, the study employs procedures of conversation analysis, which is a valuable method for analyzing verbal communicative practices used by individuals in naturally occurring interactions.30 Furthermore, the current study aims to analyze the conversational practices of MTBs during case discussions for decision-making.
The study poses the following research questions: 1) How do MTB members produce decisions for treatment recommendations through communication? 2) What insights can be gained regarding the decision-making of MTBs using procedures of conversation analysis?
Methods
Conversation analysis is based on ethnomethodology and focuses on ordinary interactions.31 Such an approach can reveal existing patterns and conversation analysis can lead to new insights into medical interaction and communication.30
Using conversation analysis, other authors created an action scheme for MTBs.22 Thus, we initially proceeded in a deductive manner and examined the extent to which this action scheme fits our sample, then adapted it inductively. In contrast to the origin of the method, the study focused on practices during the individual phases instead of conversation sequences30,32,33 throughout the process. The reason for this approach is that the study aimed to investigate typical conversational practices used during such individual phases.
Study Design and Sample
Data were collected from a multicenter, non-interventional study entitled ”Patient involvement in multidisciplinary tumor conferences in breast cancer care” (PINTU34), which was conducted on six breast and gynecological cancer centers in North Rhine-Westphalia, Germany’s most populous state. The study mainly aimed to answer the following research questions: 1) How do MTBs with and without patient participation differ in terms of organization, interaction, and patient orientation? 2) How do patients experience participation and what are the immediate effects of participation? 3) How do healthcare providers evaluate patient participation in MTBs in terms of feasibility and quality of decision-making? The study was funded by the German Cancer Aid (grant number 70112286), and the Ethics Committee of the University of Cologne gave a favorable vote (reference number: 17–405). The study observed and audiotaped case discussions during MTBs in certified breast cancer centers in North Rhine-Westphalia. The research team consisted of four researchers, who signed a confidentiality agreement with the personnel administration. The medical staff in the centers recruited patients for the study, except for one center, where the researchers recruited the patients. The inclusion criteria were (a) at least 18 years old, (b) diagnosed with breast cancer according to the International Statistical Classification of Diseases and Related Health Problems,35 and (c) undergoing treatment in one of the participating centers. In addition, German language skills were required to ensure understanding of the written informed consent. All MTB members and patients, whose case discussions were audiotaped, provided written informed consent. The case discussions constitute a PINTU subsample without patient participation.
Data Collection
Two researchers at a time carried out participant observations and audiotaped conversations during MTBs. In addition, field notes were taken, including the duration of case discussions and number of discussed cases. The author transcribed audio data using transcription conventions based on the talk-in-interaction system,36 which integrates the conventions of Jefferson.37 The transcripts were anonymized. Essential aspects related to the research questions were noted in the transcription.
Data Analysis
After developing a description of decision-making based on parts of the first material, it was applied to the entire data set. First, the structure of overall conversations in the transcripts was analyzed. An action scheme was deductively developed using the phases of MTBs proposed by Dew et al.22 On the basis of the material, we inductively adapted this action scheme. Second, micro-analysis was performed by examining conversational practices. Typical patterns of conversational practices observed across cases as well as deviations from such patterns were documented. Two researchers separately conducted the process. For validation, identified activities and conversational practices were discussed until a consensus was reached through regular data sessions among three scientific assistants. Additionally, the entire research team held consultations to embed the results in the context of health services research.
Results
The study presents a five-phase action scheme for decision-making during MTBs conducted in the treatment of patients with breast cancer followed by a description of the conversational practices used by healthcare providers during their interactions in various phases.
The current analysis is based on 33 new case discussions and five re-discussions, among 15 MTBs from four breast cancer centers recorded in January and February 2019. Two of the four breast cancer centers were teaching hospitals. In one center, MTBs were held at a round table, whereas healthcare providers in the three other centers sat in a theater-style seating arrangement. The recorded cases differed in complexity according to clinical stages partly because only non-metastatic cases were discussed within any one MTB in one breast cancer center, whereas non-metastatic and metastatic cases were discussed in the same MTBs in the other centers. Large variations were observed in the numbers of discussed cases for each MTB (range: 9–29; median: 16), healthcare providers (range: 7–23), and speakers involved in discussions (range: 1–8; median: 3). Total audio data lasted for 58 min and 43 s, where individual case discussions varied widely (range: 00:25–05:42 min; median: 1:08 min). The patients in the sample consisted of n=33 women, ages ranging from 29 to 83 years. Table 1 provides a description of the sample.
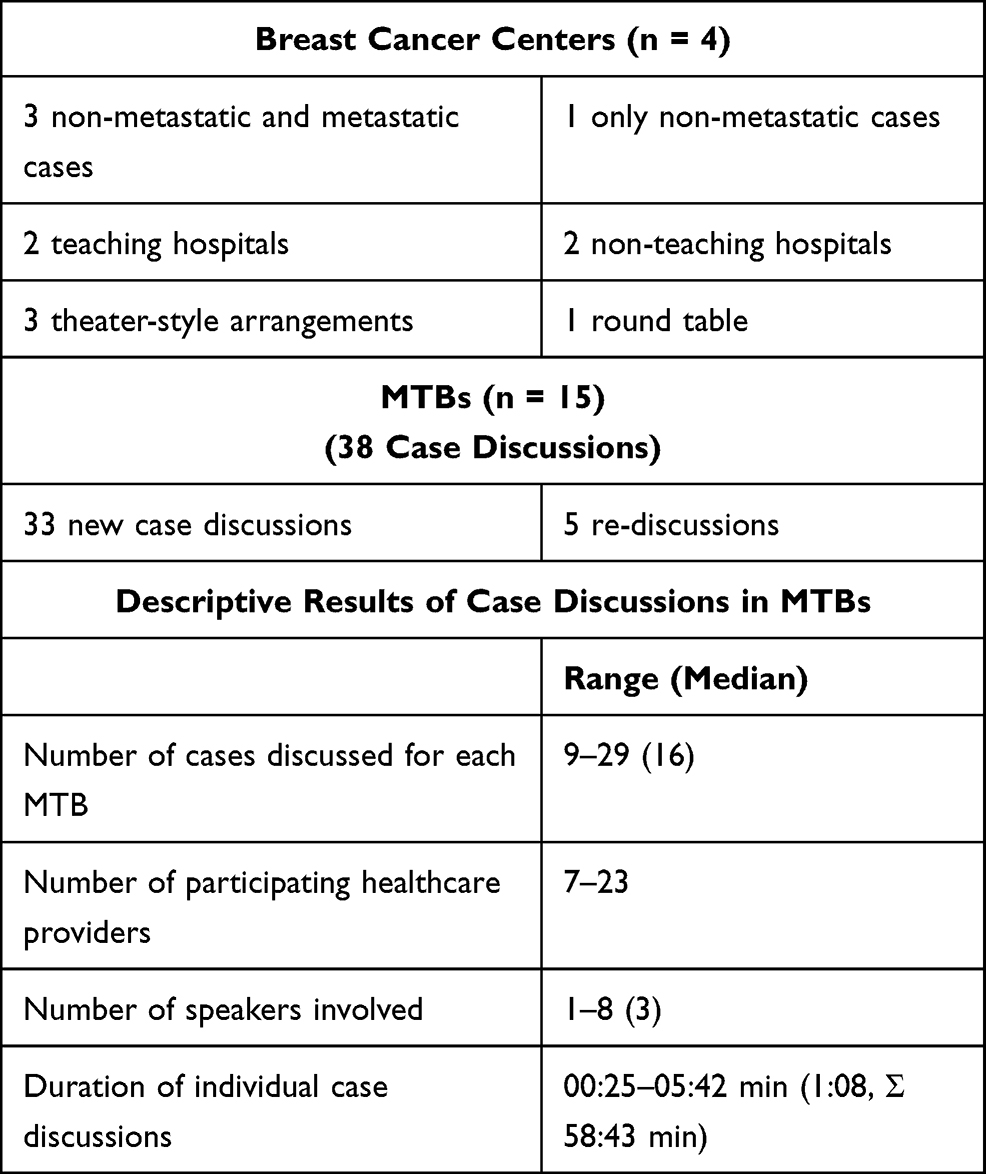 |
Table 1 Description of the Sample |
Action Scheme
Figure 1 illustrates the developed action scheme of the tasks of healthcare providers for decision-making during MTBs.
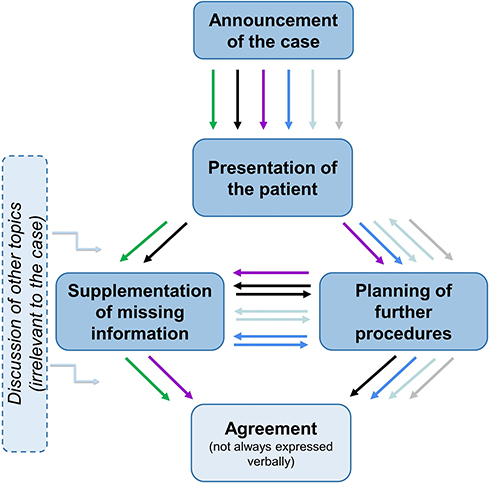 |
Figure 1 Action scheme. Colors symbolize variations in decision-making during case discussions. |
This action scheme varies by case. Colors are used to represent variations observed from available material. Each case discussion began with an announcement of the case followed by the presentation of a patient’s age and a report on current diagnostic and therapeutic statuses. At least one of two optional sequences followed. In the first, missing information was supplied (ie, diagnostic values), which was important for further decisions. In the second, subsequent procedures were planned. Decision-making was deemed completed by reaching agreement. In several case discussions, other topics, such as technical equipment, were discussed. These topics were noted in the margin because they interrupted the decision-making process.
Conversational Practices
A description of the conversational practices used by healthcare providers during interaction in the various phases of decision-making can be found below. The “supplementation of missing information” is an optional phase, which rarely occurred in the observed case discussions, such that no patterns of conversational practices were found. The presentation of the transcripts is explained in the following text and in Figure 2 to facilitate understanding. Lines are numbered (first column), whereas numbers in brackets refer to transcript number. In the excerpts, time is indicated only if relevant. Speakers are numbered (ie, S1, S2 under column 2) to enable matching of statements. In the excerpts, the bold font represents aspects highlighted in the interpretation.
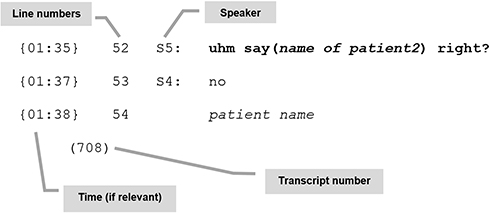 |
Figure 2 Example of presentation of transcripts (assignment). |
The presented analyses of extracts are illustrative of the analyses throughout the dataset. Table 2 shows the transcription conventions employed.36
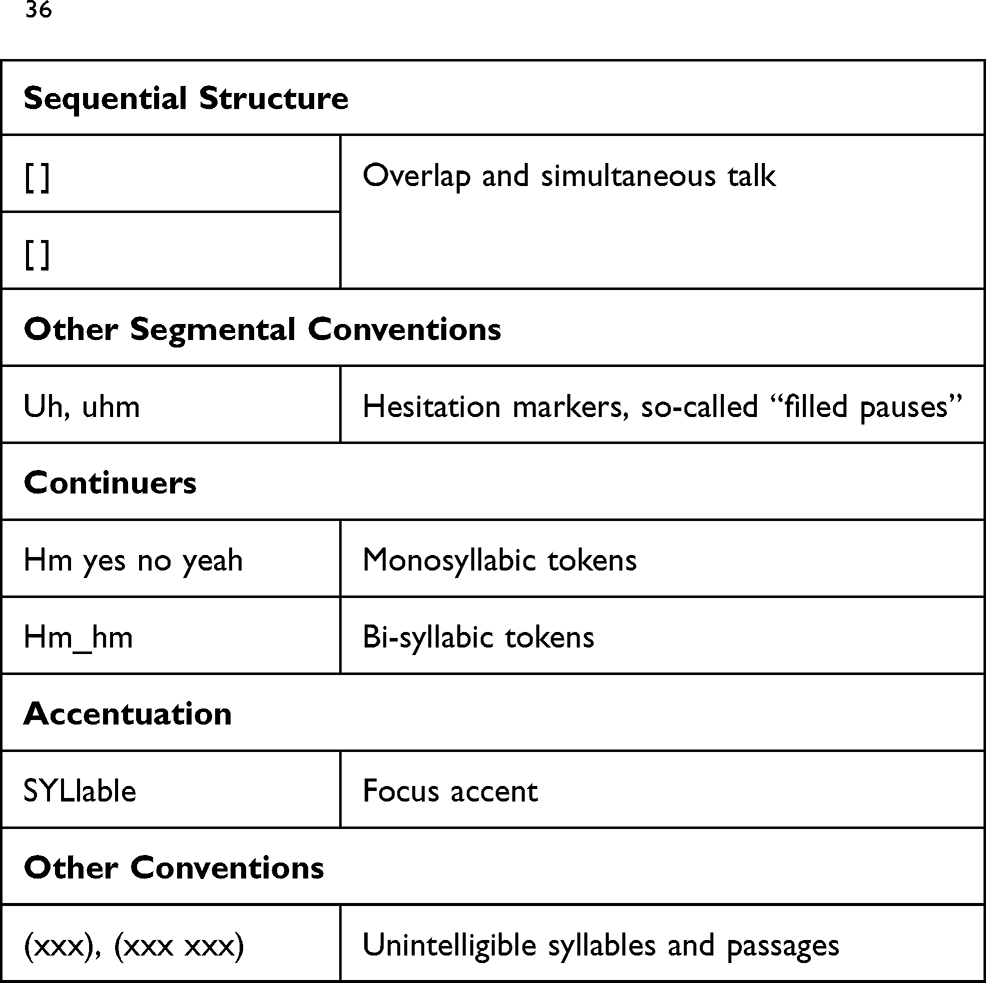 |
Table 2 Selected Transcription Conventions based on Selting et al36 |
Announcement of the Case
In many observed case discussions, the start of the case was first announced. Frequently, the announcement used sequencers, such as “then” (740), “next”, or “first”, in conjunction with the patient’s name:
01 S2: all right then next we will do ms patient name.
(740)
The majority of case discussions presented an agendum, ie, a predetermined sequence from which deviations occurred for various reasons. In the next excerpt, the order of cases was changed, whereas the announcement as the first step is missing. The patient name is announced relatively quietly, followed by the question of whether S2 would like to introduce the case (line 01). The presenting physician then begins with the presentation of the patient. After approximately 90 s of discussion, another physician asks for the name of the discussed patient (line 52):
{00:00}01 S1: <<p>> (xxx) ms patient name, would you like to
present her?
{00:10}02 S2: ms patient name
fifty-one-year-old perimenopausal patient, …
{01:35}52 S5: uhm say (name of patient2) right?
{01:37}53 S4: no
{01:38}54 patient name
(708)
In many cases, the listeners received additional information during, before, or after the announcement. In this excerpt, the first statement directly pointed out that the case is a formal presentation (220):
01 S1: and uhm then we have a formal presentation,
02 ms patient name
(220)
In another announcement of the case, reference is made to the case as problematic (231, line 03):
01 S1: is ms patient name?
02 S2: ms patient name-
03 yes that’s a problem case?
(231)
Presentation of the Patient
In the case discussions, one person was typically responsible for presenting a patient with the name and age, previous diagnosis and, if available, previous course(s) of treatment. In many cases, however, a neutral report presented the patient, whereas speakers in other cases pre-evaluated and commented during this phase (206). In addition to the specific age of the patient, the speaker mentions that the patient is young (line 02). An adjective is used to indicate the defect size in the breast instead of the actual measurement, which is confirmed by repetition and accentuation (line 05: quite). The next utterance contains an additional adverb (line 06: unfortunately):
02 S1: is a young patient postoperative presentation
forty-one years old premenopausal,
03 has a lobular G2 carcinoma hormone-receptor-
positive–
04 received BCS–
05 and has already got a QUITE quite large defect in
the breast,
06 unfortunately she is still R1 in almost all
directions–
(206)
The presentation of the patient ended with a question and an invitation for the healthcare providers in the MTBs to answer (711, lines 10–12) or directly with a proposal for further procedures (409, line 08):
07 S1: uhm and the patient is now presenting for
breast conserving therapy–
08 uhm
10 that is exactly the question for us now,
11 well the lymph node has NOT uhm been diagnostically worked up by punch biopsy,
12 whether one now recommends axillary
dissection to her?
(711)
06 S1: the staging was unremarkable,=
07 she has diabetes mellitus and arterial
hypertension (xxx xxx) and (xxx xxx) thrombosis,
08 uhm yes in her case also radiotherapy (xxx) on the right and an aromatase inhibitor,
(409)
Planning of Further Procedures
Further procedures were planned by submitting proposals, which could be stated in the singular or plural, in the first-person or impersonal. In the following excerpt, S4 proposes tissue removal. Although S4 presents the utterance with an affirmative expression (certainly, line 28), she formulates it vaguely using an impersonal “one” at the same time (101):
27 S4: ok and also scarred osseopulmonary changes-
28 which one should certainly remove at some point.
(101)
In the next excerpt, the proposal is introduced as a personal opinion (line 20). In this case, the leader of the breast cancer center interjects mid-utterance and puts forward a proposal in the collective form “we” (203, line 21):
20 S1: well Iwould just [possibly]
21 S3: [we give (xxx xxx)]
(203)
The following transcripts describe the formulation of proposals and possible reactions.
In general, proposals were made by asking a question. In the excerpt, a case that was previously discussed is presented again. In line 39, a healthcare provider asks whether the classification of the tumor can be changed. Immediately after the question, he justifies it by saying that in such a case, a different procedure may be available to the patient. S6 signals that the identity of the patient under discussion is unclear (line 44). S3 and S6 respond to the question with a statement about the size of the tumor (lines 45 and 46). Although S4 signals understanding (line 47), S3 and S6 reaffirm the correctness of the values before S6 gives a negative answer in line 52 (203):
35 S4: uhm then one more time,
36 that just occurred to me
37 she is after all thirty-three years old –
38 S3: yes
39 S4: could this somehow go through as pt1b,
40 because (I would then with) hormone receptor
negative-
41 she is also eligible for pertuzumab,
42 S3: that
44 S6: this is now ms?
45 S3: that was only a (xxx) millimeter [in size (xxx
xxx)]
46 S6: [that is only]
such a [tiny],
47 S4: [okay all right all right]
48 S6: [exactly]
49 S4: [(unintelligible, appr. 1.3 sec)]
50 S3: that’s correct
51 S4: [yes]
52 S6: [can]not be done with negative results;
(203)
Other proposals were made through statements. In excerpt 708, S1 provides additional arguments for the proposal before (line 32) and after (line 35) the presentation:
32 S1: since that did occur under tamoxifen,
33 we would suggest switching uhm to an aromatase
inhibitor
34 and then adding the (xxx xxx);
35 because we do not know exactly, well–
36 if that will otherwise
37 suffice;
(708)
During treatment planning, the healthcare providers also submitted proposals through objections. Frequently, such objections were preceded by “yes” as a structuring and agreeing element as well as a discourse marker before the introduction of the objection as signified by the word “but” (711):
149 S3: but simply the attempt to do as much as possible.
150 since it’s only that one metastasis;
151 S4: yes but if one goes that way,
152 one does not give cdk4/6 either.
(711)
In certain cases, further actions were dependent on outstanding diagnostic parameters. If this were the case, then the proposal was formulated in a restrictive manner, or possible options were expressed as follows (216):
11 S1: that’s why monday she’s undergoing mri-guided
biopsy,
12 if it’s unilateral mammary carcinoma,
13 she’s included in study name-
14 and um she’s already taking tamoxifen-
15 and if it’s bilateral,
16 she’s excluded–
(216)
Many transcripts clearly revealed that healthcare providers only make recommendations, whereas patients make the final decisions. In the next case, the use of the impersonal word “one” (740, line 30) fails to indicate who will assume the task:
29 S1: we recommend subject to (xxx xxx) if consistent
with dcis adjuvant radiotherapy uhm of the breast,
30 one has to discuss it with the patient–
(740)
Agreement
In the analyzed transcripts, agreement was expressed verbally with less frequency (214). Thus, consent in many cases was expressed by silence because the recommendation in the tumor protocol is regarded as a joint recommendation of all present healthcare providers. Moreover, the absence of further proposals can be regarded as a form of consent:
15 S1: yes then look-
16 we will do restaging under therapy.
S∑: [silence]
(214)
In the following excerpt, a specific question fails to elicit verbal reactions (201_2):
29 S1: then uhm chemotherapy in accordance with the ad
30 of the study name protocol is recomMENDed.
31 any objections?
S∑: [silence]
(201_2)
Discussion
Phases of Case Discussions
The study aimed to gain insights into decision-making during MTBs and examined communication related to decision-making for case discussions and conversational practices of healthcare providers. First, we investigated the extent to which the action scheme for MTBs developed by Dew et al22 fits our sample. By adapting we developed a five-phase action scheme for decision-making in MTBs conducted in the treatment of breast cancer patients. The phases correspond to those described by Dew et al,22 whose delimitation slightly differs from the current study. Thus, the action scheme was developed further, and phases were renamed. For instance, the study found that announcing the beginning of a new case before the presentation of the patient is important. Therefore, the first phase was renamed as “announcement of the case” instead of “opening”. Other phases are “presentation of the patient”, “supplementation of missing information”, “planning of further procedures” and “agreement”, although the order may vary depending on the case.
Presenting Information
After developing the action-scheme, we examined typical conversational practices observed during the phases. At the beginning of each case, the attention of listeners is drawn to the beginning and a clarification of new case. The addition of information at this stage indicates whether the case is relatively simple or difficult to enable the healthcare providers present to follow the discussion with appropriate attention. During the presentation, information about the patient and previous findings and therapies are presented to ensure that all participants are at the same level of knowledge in building a common basis for group decisions. Study results from literature demonstrate that this phase is sometimes omitted, such that in these cases the common basis for the decision is not established.23 In the majority of cases in the present study, information was reported in a neutral manner, whereas other reports included comments or assessments. While Hamilton et al28 observed that treatment options were expressed in a non-neutral manner to patients and that the framing effect thus influenced decisions, the study noted that healthcare providers frequently also use such a non-neutral form of presentation when reporting to other healthcare providers. However, the study was unable to assess the influence of the tone of presentation on decision-making. By adding the presenter’s own standards of judgment and commenting, the report is subjectively colored, which could complicate neutral decision-making.
Exchange of Multidisciplinary Knowledge
Findings from conversation analysis suggest that speakers use personal descriptive expressions (eg, personal and possessive pronouns) to position themselves during interaction. Using the term “one” generalizes statements and avoids expressing a personal opinion. Another type of positioning is collectivization that is, using the first-person plural form to emphasize the joint nature of a decision. However, both types can serve as a demonstration of power38,39 and were observed in MTBs and during proposals. If are worded in a generalized form, the identity that bears responsibility for such proposals remains. In contrast, the collectivized form emphasizes multidisciplinary reasoning,15 ie, decision-making within teams and, consequently, joint responsibility (consensus recommendation). The study further observed, however, the leader of a breast cancer center used a collectivized proposal to interrupt a personal proposal, which indicates a demonstration of power.38,39 In summary, no uniform pattern was found for the submission of proposals and subsequent discussions.
In certain cases, a presented proposal lacked further discussion, whereas silence was used to express consent. In these cases, the MTBs do not aim to discuss treatment and diagnosis in line with the frequent description in the literature,1,2 but to communicate information and proposals. These cases reveal that reasoning processes must have occurred before MTBs and that multidisciplinary reasoning15 is applied even outside MTBs. Such cases may be routine ones that can be decided quickly on the basis of the existing guidelines.18 For this reason, certain studies question whether MTBs should be established as a standard practice in light of the fact that clinical guidelines give a clear recommendation for routine cases, which may thus require no discussion.40 In addition, MTBs represent a high cost factor in healthcare41 and could potentially prolong the decision-making process.14 However, instances where only one person is speaking during a case discussion could be attributed to the fact that the majority of providers do not raise objections during MTBs25 or that the setting does not promote discussion.9 Similar to other studies,42 the exchange of multidisciplinary knowledge may not always be observed.
Consensus-Based Recommendation
The agreement phase reveals that agreement may be expressed through non-verbal means. Despite the consideration of non-verbal aspects, the extent to which they can be observed by healthcare providers present remains unclear given that MTBs are frequently held in rooms with a theater-style seating arrangement. The expected outcome of MTBs is a consensus-based recommendation.43 However, although the absence of further objections may be interpreted as consent, it leaves space for ambiguity regarding whether all healthcare providers actually reached a consensus.
Strengths and Limitations
Data employed in the study were derived from participant observations of case discussions during MTBs, such that the presence of observers and technical equipment for audiotaping may be disruptive factors. To mitigate the effect, the researchers introduced themselves at the centers before data collection, explained the planned method and visited the MTB.44 The regularity of observations over an extended period of time enabled the MTB members to become familiar with the presence of the observers.
Although the recorded cases differed in complexity in terms of clinical staging, the results related to decision-making can be generalized for all case discussions of this study because the analysis is largely focused on case-independent phenomena. Further data are required to promote the transfer of results to MTBs held at different breast cancer centers and other entities related to cancer.
In general, written information is available during MTBs, and information is provided via imaging diagnostics. These aspects, as well as non-verbal ones, are excluded from the analysis. Within the PINTU project, however, video recordings are also examined using video interaction analysis,45 such that further results can be produced in the near future.
We primarily used procedures of conversation analysis to create the action scheme and identify conversational practices typical of individual phases of MTBs. Deviating from the conversation analysis, the study deductively and inductively analyzed the data and did not analyze the entire sequences. A follow-up study on sequence organization32,33 would be useful for examining such dynamic processes.30
However, a major strength of the methodological approach is the use of procedures of conversation analysis. Thereby, identifying the conversational practices of healthcare providers during case discussions within MTBs as a central part of decision-making in breast cancer care was possible. This approach differs from content analysis, which focuses on content and themes and is commonly used as a qualitative method in research on healthcare.46 Furthermore the analysis was conducted in line with the transcript, which is close to the events and very detailed. However, the method is extremely time-consuming due to the small-step procedure, such that only a small sample could be analyzed.
Conclusion
These results can serve as preliminary reference for the design of the decision-making processes regarding treatment recommendations through communication and applied conversational practices among healthcare providers.
Recommendations, which largely influence subsequent therapeutic procedures, are dependent on the results of decisions made during case discussion within MTBs. Theoretically, certification guidelines demand the standardization, among other things, in MTBs.47 Based on the present study, the guidelines for communication are seemingly scarce. An improvement in communication cannot be achieved simply through collaboration among healthcare providers from different disciplines as study results of Rowlands and Cullen48 have already shown. The reason for this notion is that the exchange of multidisciplinary knowledge as an essential aspect of MTBs is not always present.
Ultimately, whether recommendations are in fact consensus-based remains unclear. To optimize decision-making and, thus, the quality of recommendations, standards for communication during MTBs should also be developed. Divergent opinions might be recorded in the protocol, as proposed by Horlait et al,42 and each member of the core team should be required to contribute a statement.
Acknowledgments
The authors would like to thank all hospitals and healthcare providers who participated in this study. We are grateful to the German Cancer Aid for funding this research. An abstract with interim findings of this paper was presented at the conference Quality of Cancer Care (QoCC) 2019 as a poster presentation. The poster’s abstract was published in “Poster Abstracts” in Forum 2019 34:100–101.
Disclosure
Prof. Dr. Nicole Ernstmann report grants from German Cancer Aid, during the conduct of the study; Prof. Dr. Lena Ansmann report grants from German Cancer Aid, during the conduct of the study; The authors report no other conflicts of interest in this work.
References
1. Ansmann L, Kowalski C, Pfaff H, Wuerstlein R, Wirtz MA, Ernstmann N. Patient participation in multidisciplinary tumor conferences. Breast. 2014;23(6):865–869. doi:10.1016/j.breast.2014.09.004
2. Patkar V, Acosta D, Davidson T, Jones A, Fox J, Keshtgar M. Cancer multidisciplinary team meetings: evidence, challenges, and the role of clinical decision support technology. Int J Breast Cancer. 2011;2011:831605. doi:10.4061/2011/831605
3. Borras JM, Albreht T, Audisio R, et al. Policy statement on multidisciplinary cancer care. Eur J Cancer. 2014;50(3):475–480. doi:10.1016/j.ejca.2013.11.012
4. Lamb BW, Sevdalis N, Taylor C, Vincent C, Green JSA. Multidisciplinary team working across different tumour types: analysis of a national survey. Ann Oncol. 2012;23(5):1293–1300. doi:10.1093/annonc/mdr453
5. Brown ERS, Bartlett J, Chalulu K, et al. Development of multi-disciplinary breast cancer care in Southern Malawi. Eur J Cancer Care. 2017;26(1):e12658. doi:10.1111/ecc.12658
6. Fleissig A, Jenkins V, Catt S, Fallowfield L. Multidisciplinary teams in cancer care: are they effective in the UK? Lancet Oncol. 2006;7(11):935–943. doi:10.1016/S1470-2045(06)70940-8
7. Harrison JD, Choy ET, Spillane A, Butow P, Young JM, Evans A. Australian breast cancer specialists’ involvement in multidisciplinary treatment planning meetings. Breast. 2008;17(4):335–340. doi:10.1016/j.breast.2008.03.001
8. Prades J, Remue E, van Hoof E, Borras JMI. It worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy. 2015;119:464–474. doi:10.1016/j.healthpol.2014.09.006
9. Saini KS, Taylor C, Ramirez A-J, Palmieri C, Gunnarsson U, Schmoll HJ. Role of the multidisciplinary team in breast cancer management: results from a large international survey involving 39 countries. Ann Oncol. 2012;23:853–859. doi:10.1093/annonc/mdr352
10. Wright FC, de Vito C, Langer B, Hunter A. Multidisciplinary cancer conferences: a systematic review and development of practice standards. Eur J Cancer. 2007;43(6):1002–1010. doi:10.1016/j.ejca.2007.01.025
11. Kesson EM, Allardice GM, George WD, Burns HJG, Morrison DS. Effects of multidisciplinary team working on breast cancer survival: retrospective, comparative, interventional cohort study of 13 722 women. BMJ. 2012;344:e2718. doi:10.1136/bmj.e2718
12. Soukup T, Lamb BW, Arora S, Darzi A, Sevdalis N, Green JSA. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthc. 2018;11:49–61. doi:10.2147/JMDH.S117945
13. Taylor C, Ramirez AJ. Multidisciplinary team members’ views about MDT working: results from a survey commissioned by the National cancer action team cancer action team. Available from: http://www.ncin.org.uk/view?rid=137.
14. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: a systematic review of the literature. Cancer Treat Rev. 2016;42:56–72. doi:10.1016/j.ctrv.2015.11.007
15. Higgs J, Jones M. Multiple spaces of choice, engagement and influence in clinical decision making. In: Higgs J, Jensen GM, Loftus S, Christensen N, editors. Clinical Reasoning in the Health Professions.
16. Lamb BW, Brown KF, Nagpal K, Vincent C, Green JSA, Sevdalis N. Quality of care management decisions by multidisciplinary cancer teams: a systematic review. Ann Surg Oncol. 2011;18(8):2116–2125. doi:10.1245/s10434-011-1675-6
17. Newman EA, Guest AB, Helvie MA, et al. Changes in surgical management resulting from case review at a breast cancer multidisciplinary tumor board. Cancer. 2006;107(10):2346–2351. doi:10.1002/cncr.22266
18. Ruhstaller T, Roe H, Thürlimann B, Nicoll JJ. The multidisciplinary meeting: an indispensable aid to communication between different specialities. Eur J Cancer. 2006;42(15):2459–2462. doi:10.1016/j.ejca.2006.03.034
19. Ganesan P, Kumar L, Hariprasad R, Gupta A, Dawar R, Vijayaraghavan M. Improving care in ovarian cancer: the role of a clinico-pathological meeting. Natl Med J India. 2008;21(5):225–227.
20. Devitt B, Philip J, McLachlan S-A. Team dynamics, decision making, and attitudes toward multidisciplinary cancer meetings: health professionals’ perspectives. J Oncol Pract. 2010;6(6):e17–e20. doi:10.1200/JOP.2010.000023
21. Domke C. Besprechungen als organisationale Entscheidungskommunikation. Berlin, New York: Walter de Gruyter; 2008.
22. Dew K, Stubbe M, Signal L, et al. Cancer care decision making in multidisciplinary meetings. Qual Health Res. 2015;25(3):397–407. doi:10.1177/1049732314553010
23. Soukup T, Murtagh G, Lamb BW, Green JS, Sevdalis N. Degrees of multidisciplinarity underpinning care planning for patients with cancer in weekly multidisciplinary team meetings: conversation analysis. JMDH. 2021;14:411–424. doi:10.2147/JMDH.S270394
24. Woolley AW, Gerbasi ME, Chabris CF, Kosslyn SM, Hackman JR. Bringing in the experts. Small Group Res. 2008;39(3):352–371. doi:10.1177/1046496408317792
25. Sidhom MA, Poulsen M. Group decisions in oncology: doctors’ perceptions of the legal responsibilities arising from multidisciplinary meetings. J Med Imaging Radiat Oncol. 2008;52(3):287–292. doi:10.1111/j.1440-1673.2007.01916.x
26. Hahlweg P, Hoffmann J, Harter M, Frosch DL, Elwyn G, Scholl I. In Absentia: an exploratory study of how patients are considered in multidisciplinary cancer team meetings. PLoS One. 2015;10:e0139921. doi:10.1371/journal.pone.0139921
27. Kahneman D, Tversky A. Choices, values, and frames. Am Psychol. 1984;39(4):341–350. doi:10.1037/0003-066X.39.4.341
28. Hamilton DW, Heaven B, Thomson RG, Wilson JA, Exley C. Multidisciplinary team decision-making in cancer and the absent patient: a qualitative study. BMJ Open. 2016;6(7):e012559. doi:10.1136/bmjopen-2016-012559
29. Dinh JV, Traylor AM, Kilcullen MP, et al. Cross-disciplinary care: a systematic review on teamwork processes in health care. Small Group Res. 2020;51(1):125–166. doi:10.1177/1046496419872002
30. Drew P, Chatwin J, Collins S. Conversation analysis: a method for research into interactions between patients and health-care professionals. Health Expect. 2001;4(1):58–70. doi:10.1046/j.1369-6513.2001.00125.x
31. Garfinkel H. Studies in Ethnomethodology. Reprinted. Cambridge: Polity Press; 2011.
32. Schegloff EA. Sequence Organization in Interaction. 4. print. Cambridge: Cambridge Univ. Press; 2009.
33. Stivers T. Sequence Organization. In: Sidnell J, Stivers T, editors. The Handbook of Conversation Analysis. Chichester, UK: John Wiley & Sons, Ltd; 2012:191–209.
34. Heuser C, Diekmann A, Ernstmann N, Ansmann L. Patient participation in multidisciplinary tumour conferences in breast cancer care (PINTU): a mixed-methods study protocol. BMJ Open. 2019;9(4):e024621. doi:10.1136/bmjopen-2018-024621
35. World Health Organization. International statistical classification of diseases and related health problems. 10th revision. Available from: https://icd.who.int/browse10/2016/en.
36. Selting M, Auer P, Barth-Weingarten D, et al. A system for transcribing talk-in-interaction: GAT 2. translated and adapted for English by Elizabeth Couper-Kuhlen and Dagmar Barth-Weingarten. Gesprächsforschung - Online-Zeitschrift zur verbalen Interaktion. 2011.
37. Jefferson G. Glossary of transcript symbols with an introduction. In: Lerner GH, editor. Conversation Analysis: Studies from the First Generation. Amsterdam: John Benjamins; 2004:13–31.
38. Brown EL, Raue PJ, Klimstra S, Mlodzianowski AE, Greenberg RL, Bruce ML. An intervention to improve nurse-physician communication in depression care. Am J Geriatr Psychiatry. 2010;18(6):483–490. doi:10.1097/JGP.0b013e3181bf9efa
39. Holly W. Imagearbeit in Gesprächen: Zur Linguistischen Beschreibung Des Beziehungsaspekts. Tübingen: Niemeyer; 1979.
40. Ryan J, Faragher I. Not all patients need to be discussed in a colorectal cancer MDT meeting. Colorectal Dis. 2014;16(7):520–526. doi:10.1111/codi.12581
41. Chinai N, Bintcliffe F, Armstrong EM, Teape J, Jones BM, Hosie KB. Does every patient need to be discussed at a multidisciplinary team meeting? Clin Radiol. 2013;68(8):780–784. doi:10.1016/j.crad.2013.02.011
42. Horlait M, Baes S, Dhaene S, van Belle S, Leys M. How multidisciplinary are multidisciplinary team meetings in cancer care? An observational study in oncology departments in Flanders, Belgium. J Multidiscip Healthc. 2019;12:159–167. doi:10.2147/JMDH.S196660
43. Lamb BW, Taylor C, Lamb JN, et al. Facilitators and barriers to teamworking and patient centeredness in multidisciplinary cancer teams: findings of a national study. Ann Surg Oncol. 2013;20(5):1408–1416. doi:10.1245/s10434-012-2676-9
44. Heath C, Hindmarsh J, Luff P. Video in Qualitative Research: Analysing Social Interaction in Everyday Life. London: Sage; 2011.
45. Tuma R, Schnettler B, Knoblauch H. Videographie: Einführung in die interpretative Videoanalyse sozialer Situationen. Wiesbaden: Springer VS; 2013.
46. Palinkas LA. Qualitative and mixed methods in mental health services and implementation research. J Clin Child Adolesc Psychol. 2014;43(6):851–861. doi:10.1080/15374416.2014.910791
47. Kowalski C, Graeven U, von Kalle C, et al. Shifting cancer care towards Multidisciplinarity: the cancer center certification program of the German cancer society. BMC Cancer. 2017;17(1):850. doi:10.1186/s12885-017-3824-1
48. Rowlands S, Callen J. A qualitative analysis of communication between members of a hospital-based multidisciplinary lung cancer team. Eur J Cancer Care. 2013;22(1):20–31. doi:10.1111/ecc.12004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.