Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 17
Decision-Making Factors Among Dentists for Using Dental Magnifying Loupes: A Cross-Sectional Study
Authors Alghilan MA ![]() , AlShehri A, Almeshrafi A, Alrumi A, Aldibasi O
, AlShehri A, Almeshrafi A, Alrumi A, Aldibasi O
Received 5 November 2024
Accepted for publication 24 January 2025
Published 5 February 2025 Volume 2025:17 Pages 99—110
DOI https://doi.org/10.2147/CCIDE.S501104
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Maryam A Alghilan,1,2 Aram AlShehri,1,2 Azzam Almeshrafi,3 Abdulmajeed Alrumi,4 Omar Aldibasi2
1Restorative and Prosthetic Dental Sciences, College of Dentistry, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia; 2King Abdullah International Medical Research Center, Ministry of National Guard Health Affairs, Riyadh, Kingdom of Saudi Arabia; 3King Saud Medical City, Riyadh, Kingdom of Saudi Arabia; 4King Faisal Specialist Hospital and Research Centre, Riyadh, Kingdom of Saudi Arabia
Correspondence: Maryam A Alghilan, Restorative and Prosthetic Dental Sciences, College of Dentistry, King Saud bin Abdulaziz University for Health Sciences Riyadh, Saudi Arabia, P.O. Box 3660, Riyadh, 11481, Kingdom of Saudi Arabia, Tel +966 11 4299 999 Ext. 95738, Email [email protected]
Purpose: Dental magnifying loupes (DMLs) allow better visualization of the operative field and operator’s seating postures. This study aimed to investigate factors influencing the usage and selection of DMLs among dentists and determine the self-reported musculoskeletal pain and perception regarding DMLs usage.
Methods: A validated self-reported questionnaire of 19 items assessing participant’s characteristics and DMLs usage was distributed to individuals who fit the inclusion criteria: practicing general dentists/dental intern and resident/specialized dentist in various dental specialties. The data were collected and then statistically analyzed using comparisons tests (chi-square/Fisher’s exact test) and logistic regression with significance level (p-value) below 0.05.
Results: The response rate for this study’s questionnaire was 97.33%. There is a significant association between the use of DMLs and training using them in dental school (p < 0.002). Using DMLs in endodontic treatment is significantly associated with the general dentist professional classification. Specialized dentists are 1.94-times more likely to use DMLs than general dentists (p < 0.001). The majority (50%) of DML users believe that DMLs are best used during undergraduate training. Using DMLs for “better vision” was the most selected (63.64%) option by DMLs users, followed by “increased clinical efficacy” (61.36%), “improved patient care” (50%), and “better ergonomics” (47.73%). Of dentists who did not use DMLs, 66.90% reported that DMLs being expensive was a limitation to their usage. Almost 91% dentists who have neck and shoulder discomfort (n = 219) do not use DMLs.
Conclusion: DMLs are under-utilized by dentists. The major factors limiting their use are the high cost and lack of training regarding their use in dental school. Addressing these two factors may contribute to a positive shift in the utilization of DMLs by a larger number of dentists.
Keywords: magnification, loupes, dentists, musculoskeletal disorders
Introduction
Dental procedures are performed in a small and dark operative field; therefore, visibility and illumination are paramount for high precision in dentistry. These physically demanding operating conditions often lead to compromised ergonomics resulting in a high prevalence of musculoskeletal disorders among dental professionals. One meta-analysis found the prevalence of musculoskeletal pain among dental professionals to range between 10.8% and 97.9%.1 Another systematic review has confirmed a high prevalence of 64–93%.2 It is well documented that the use of magnification in dentistry can aid in maintaining better ergonomics and therefore less musculoskeletal symptoms.3–10 Moreover, it has been recommended to incorporate the use of dental magnifying loupes (DMLs) early in the dental career for dental students as part of their pre-clinical training as the benefits are worth the challenges of the cost and the required learning curve.4
There is an abundance of existing evidence supporting the multiple benefits of using DMLs.3–10 The main advantage is the optical magnification that allows for improved visual acuity and better outcomes of diagnostic and procedural operations. Furthermore, DMLs are usually accompanied with illumination systems, which additionally enhance the visual acuity and significantly improve the operator’s ability to distinguish minor details in structures and materials. As a result of improved visualization of the operative field, dental operators who use DMLs were found to possess better seating postures.3,6,9 The use of DMLs can improve ergonomics in dental practice by specific design features like appropriate working distance and lens declination angle,7 which taken together, decrease the need for forward head flexion to improve vision.8
The use of DMLs has been reported to enhance outcomes of procedures in various dental specialties, starting with the diagnosis of lesions of the soft and hard tissues of the oral cavity. Compared to the naked eye, a magnification power of 3.5× was found to significantly improve the detection of oral mucosal diseases.11 The diagnosis of initial caries lesions,12 demineralized tooth structure on preparation margins,13 and cracks can be carried out more reliably under magnification.13 Dental extractions may be performed more conservatively and with less trauma to the extraction site when magnification is used.14 In endodontics, using DMLs with a magnification power as low as 2.5× was found to significantly reduce the time needed to complete root canal treatments.15 Additionally, a higher ability to locate the second mesiobuccal canal was reported when using 3.5× magnification.16 In periodontics, the use of 2.5× magnification increased the effectiveness of supra- and sub-gingival scaling and root planning when compared to performing these procedures with naked eyes.17 Debonding procedures after orthodontic treatment were reportedly more efficient with less damage to the enamel when 2.5× DMLs were used.18
DMLs usually provide magnification ranging from 2.5× to 6×. They are commonly available in two designs: one with the magnifying lenses embedded in the eyeglasses, which is known as “through the lens” (TTL) design, and another with the lenses mounted on the loupes frame through a hinge and hanging in front of the eyeglasses, known as “flip-up” (FU) design. The TTL design is customized according to the specific measurements of each individual operator. The fixed magnifying lenses in this design allow for a slightly wider field of view than the FU design. TTL loupes are usually lighter in weight but more expensive because they require customization.19 The FU design allows for adjustments of interpupillary distance and lens declination angle, therefore allowing the loupes to be shared between different operators; however, the adjustment process can become bothersome and time-consuming.19 The magnifying lenses in this design can be moved out of sight when not in use. Loupes with the FU design are usually less expensive than the TTL loupes, but heavier due to the added hinge mechanism, which can cause strain after prolonged use.19
Dentistry is a quickly evolving field with continuous advancements in dental materials and technologies. This puts an increased demand on dentists to efficiently deliver treatments with high success and predictability. Meeting this demand requires dentists to make the best use of every available resource, including dental magnification. Therefore, this study was conducted to assess the current pattern and factors affecting the use of DMLs among dentists and identify the dentists’ self-reported musculoskeletal pain and perception with regard to DMLs usage. The first hypothesis of the study is that the dentists’ purchasing decisions and use of DML are influenced by factors such as cost, prior training, ergonomic aspects, DML features, and dentist’s characteristics. The second hypothesis is that the use of DML is associated with the reported musculoskeletal pain experience.
Materials and Methods
This is a cross-sectional study design wherein self-reported questionnaire data were analyzed quantitatively. The study was ethically and methodically approved by the Institutional Review Board (IRB) of the King Abdullah International Medical Research Center (KAIMRC).
The structured self-reported questionnaire includes 19 close-ended items assessing the pattern of DMLs usage and participants’ characteristics. The inclusion criteria for participants were as follows: practicing general dentists and dental interns in Riyadh, Saudi Arabia, and practicing dental residents, specialists, and consultants specializing in recognized fields of dentistry (Prosthodontics, Restorative dentistry, Advanced Education in General Dentistry, Endodontics, Periodontics, Pedodontics, and Oral and Maxillofacial Surgery) in Riyadh, Saudi Arabia. Exclusion criteria of participants include any dentist not practicing in Riyadh, Saudi Arabia, and undergraduate dental students. The questionnaire was independently validated using test–retest reliability by piloting the questionnaire items over two phases to 30 subjects who fit the inclusion criteria and were willing to participate. The test–retest reliability analysis of the questionnaire items yielded Cohen’s kappa coefficients ranging from 0.66 to 1. These results suggest a substantial-to-almost perfect agreement in responses, indicating strong reliability of the measures. The questionnaire was prepared as paper-based and electronic-based forms and distributed to eligible individuals. The sample size was calculated based on the estimated population of practitioners and the expected percentage of DMLs usage. Based on a study conducted by AlBaker et al,20 the number of dentists in Riyadh is 12,785. The expected proportion of DMLs usage was noted in 32.4% of participants. Thus, based on the precision of 0.05 and a statistical level of confidence of 95%, the sample size required for the study was 337 participants. The recruitment process of the participants and its outcomes is presented in a flowchart (Figure 1).
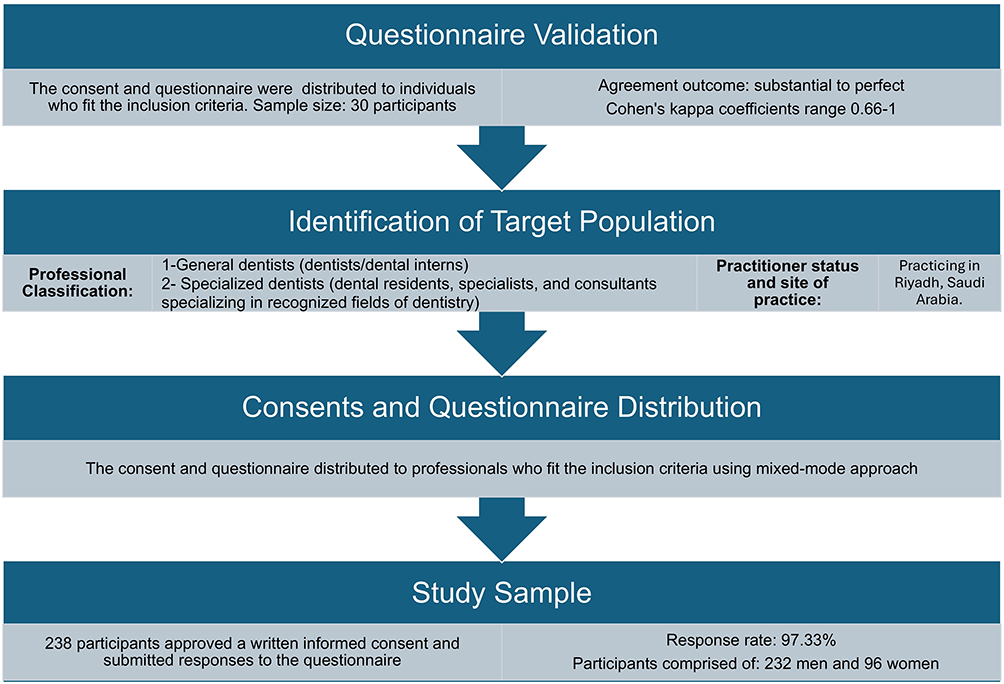 |
Figure 1 Flowchart of the participants recruitment process and its outcomes. |
Participation was voluntary, and all participants provided written informed consent before attempting the questionnaire. All data was collected from general and specialized dentists and residents in dental programs, and a total of 328 participated in the questionnaire. Responses from participants were collected from August 2020 to May 2021.
All statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The sample characteristics were summarized using descriptive statistics to describe all variables. Frequencies and column percentages were calculated for all categorical variables: sex, level of education, type of dental specialty, DML taught in dental school, DMLs training in continuous professional education, perception of proper time for using DMLs, reasons for and barriers against using DMLs, neck and shoulder discomfort, and factors affecting DMLs purchasing decision.
Statistical comparisons between different groups for all categorical variables were carried out using Pearson’s chi-square test. Fisher’s exact test was used when chi-square test was not applicable. The exact p values were calculated and a p-value of <0.05 was used to indicate statistically significant differences.
Binary and multivariate logistic regression models were utilized to examine the factors influencing the use of DMLs among dental professionals. Unadjusted odds ratios (OR) were calculated to assess the crude association between each factor and DML use. Subsequently, multivariate logistic regression models were fitted to estimate the adjusted ORs, controlling for potential confounding variables, to identify the independent predictors of DML use.
Results
The questionnaire items were validated as simple Kappa coefficient scores and ranged from 0.66 to 1, which indicates the validity and reliability of the questionnaire items.
Sample Characteristics and DMLs Use
The response rate for this study’s questionnaire was 97.33% with a total of 328 respondents. Frequencies and column percentages for sex, level of education, and type of dental specialty among both users and non-users of DMLs are presented in Table 1. The socio-demographic characteristics showed that almost 71% respondents were men and approximately 88% respondents were general dentists. Of the 328 dentists who answered the questionnaire, only 13.41% (n = 44) used DMLs. Almost 68% and 43% of DMLs users were men (n = 30) and specialized dentists (n = 19), respectively.
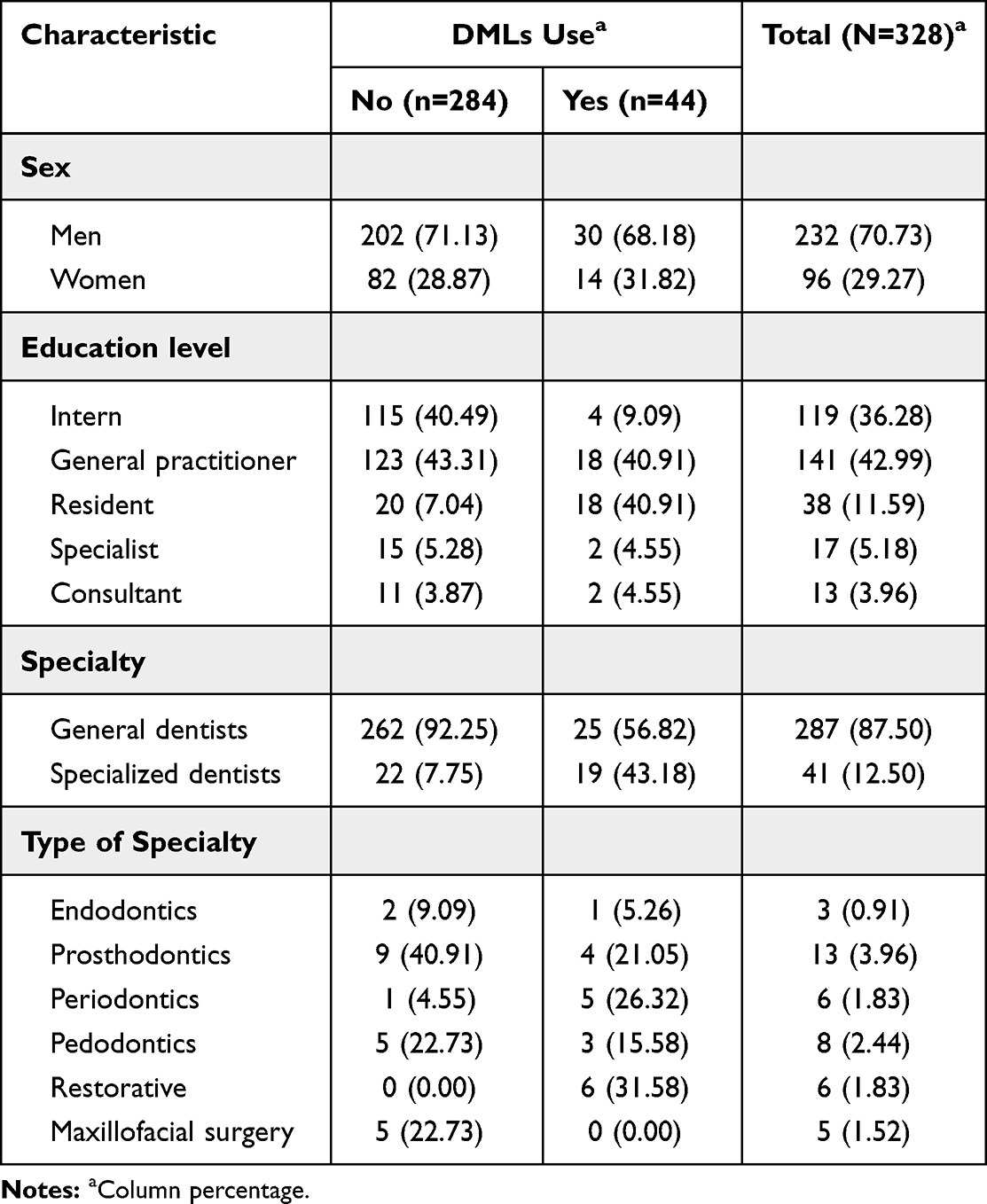 |
Table 1 Socio-Demographic Characteristics of Dentists’ Sample by DMLs Use |
Unadjusted and adjusted ORs for the factors affecting the use of DMLs by logistic regression analyses were calculated. The results revealed that sex did not have a significant impact on the use of DMLs (adjusted OR [95% CI] = 0.10 [–0.07 to 0.89]), p = 0.810]. Specialty had a significant impact on the use of DMLs. The specialized dentists were 1.94-more likely to use DMLs than general dentists (adjusted OR [95% CI] = 1.94 [1.13–2.75], p < 0.001).
Frequencies and column percentages for DMLs’ characteristics and use among dentists and statistical comparisons between general and specialized dentists are presented in Table 2. Most DMLs users reported using FU type (75%, n = 33). Of the 25 general dentists who use DMLs, 80% (n = 20) use them in endodontics treatment. Only 6 of 19 specialized dentists who use DMLs used them with endodontics treatment (31.58%). There is a significant association between being a general dentist and using DMLs with endodontic treatment(c2 = 10.47, p = 0.002).
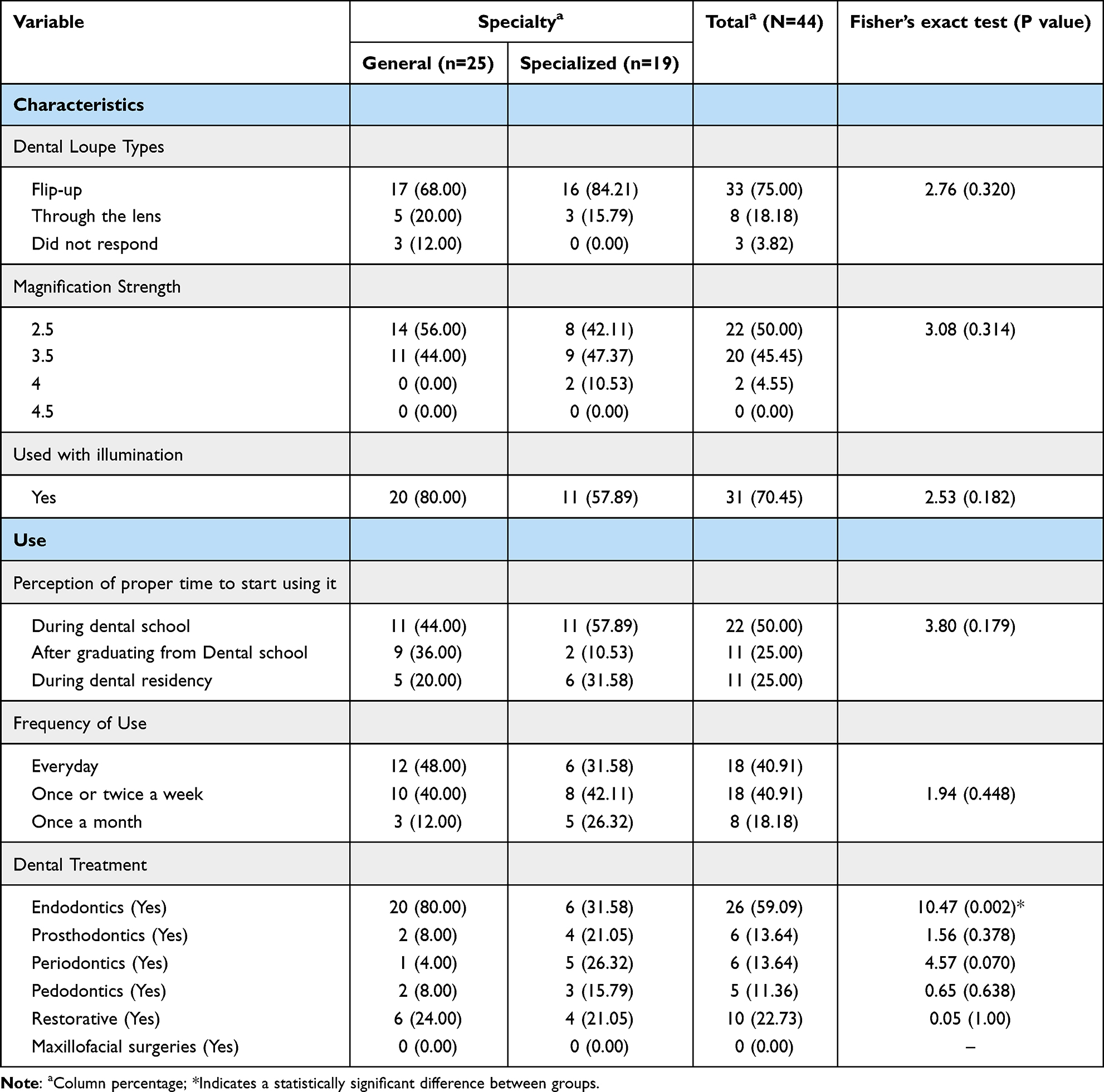 |
Table 2 Statistical Comparisons for the Characteristics and Use of DMLs Among General and Specialized Dentists |
Training, Reasons, Perception, and Barriers for DMLs Use
Statistical comparisons for DMLs training, proper timing perception, reasons for use among users and non-users of DMLs are presented in Table 3. The association of dental loupe use with being taught in dental school was statistically significant (c2 = 36.92, p < 0.002). However, the association of dental loupe use with receiving training in continuous professional education was not statistically significant (c2 = 0.21, p = 0.648). Furthermore, unadjusted and adjusted ORs for the prior training factors impact on the use of DMLs were computed using logistic regression analyses. Results showed that DMLs being taught in school had a significant impact on their use. Dentists who had been taught about DMLs in dental schools were 1.64-times more likely to use them than those who had not been taught (adjusted OR [95% CI] = 1.64 [0.90–2.38], p < 0.001).
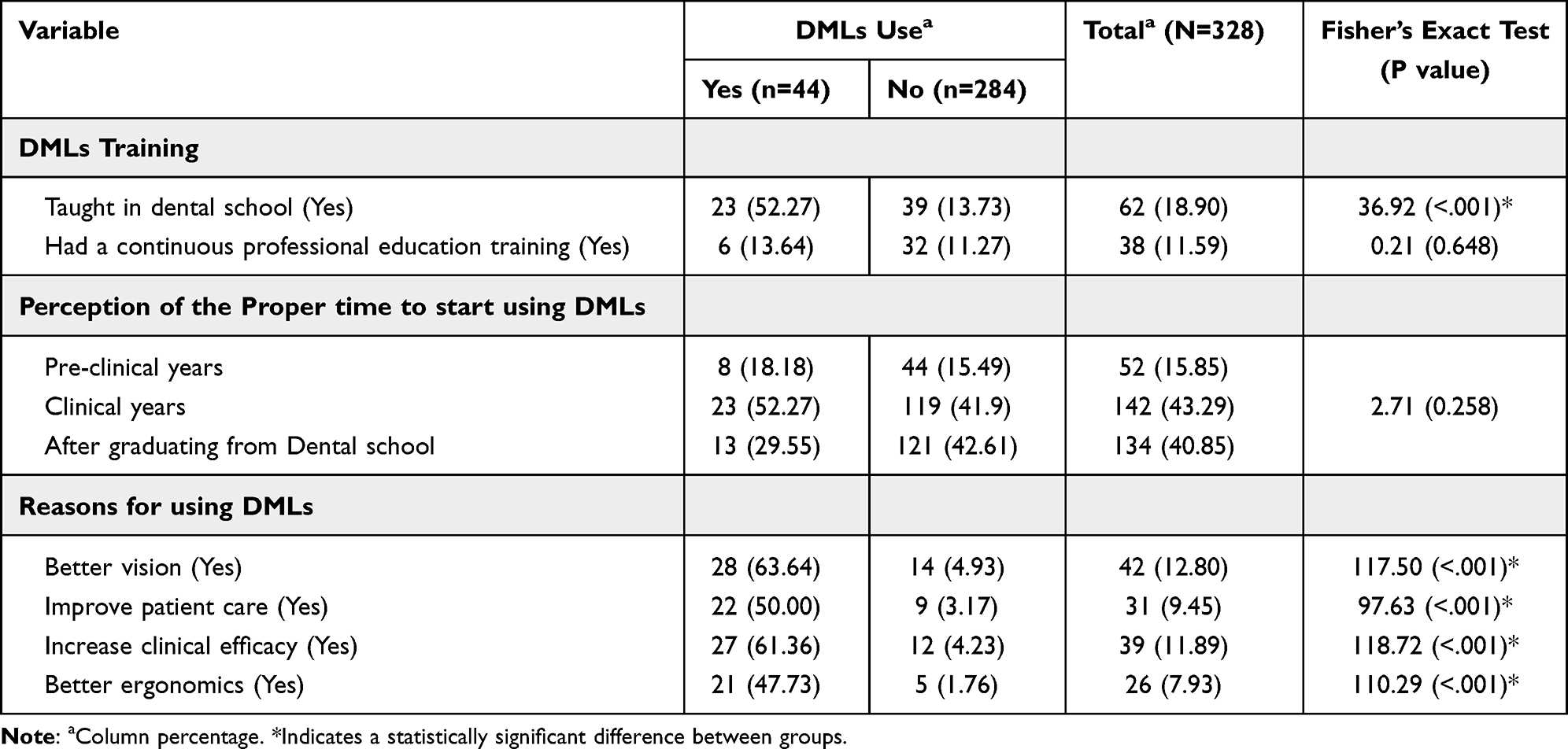 |
Table 3 Statistical Comparisons for DMLs Training, Proper Timing Perception, Reasons for Using DMLs Among Users and Non-Users |
The perception of the proper time to start using DMLs did not statistically differ between dentists who used or did not use them. There was no significant association between DMLs use and the perception of the proper time to start using them (c2 = 2.71, p = 0.258). The majority of participants (84%) indicated that DMLs were most effectively used during clinical years before (43%) and after (41%) graduation from dental school.
The participants indicated that better vision (p < 0.001), increased clinical efficacy (p < 0.001), improved patient care (p < 0.001), and better ergonomics (p < 0.001) were significant reasons for DMLs use. Of the 284 dentists who did not use dental loupes, 190 (66.90%) reported that excessive cost was a barrier for DLM use.
Among the studied potential barriers, being expensive (p < 0.001), no interest (p < 0.001), insufficient training (p < 0.001) and wearing glasses (p = 0.002) were significant barriers against DMLs use indicated by the participants (Figure 2). Of the 284 dentists who did not use DMLs, 190 (66.90%) reported that being expensive was a barrier against DMLs use.
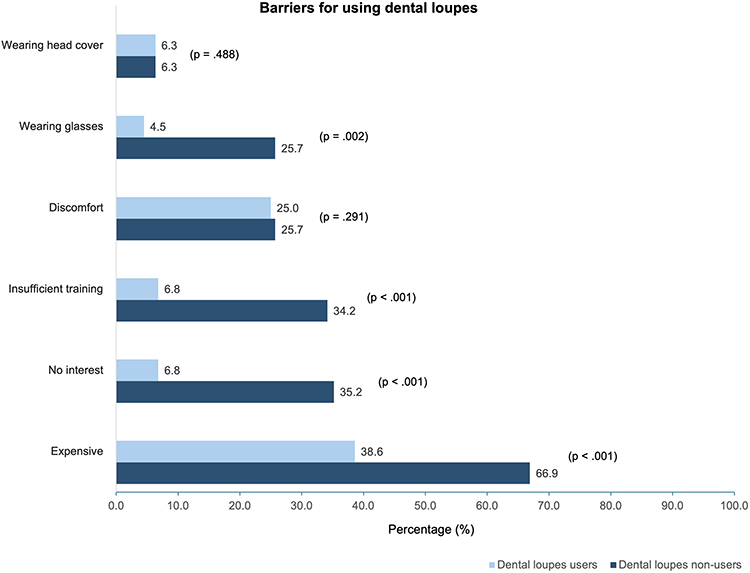 |
Figure 2 Statistical comparisons for using DMLs barriers among users and non-users. |
Neck and Shoulder Discomfort
Results for frequencies, column percentages, and statistical comparisons between having neck and shoulder discomfort among different subgroups are presented in Table 4.
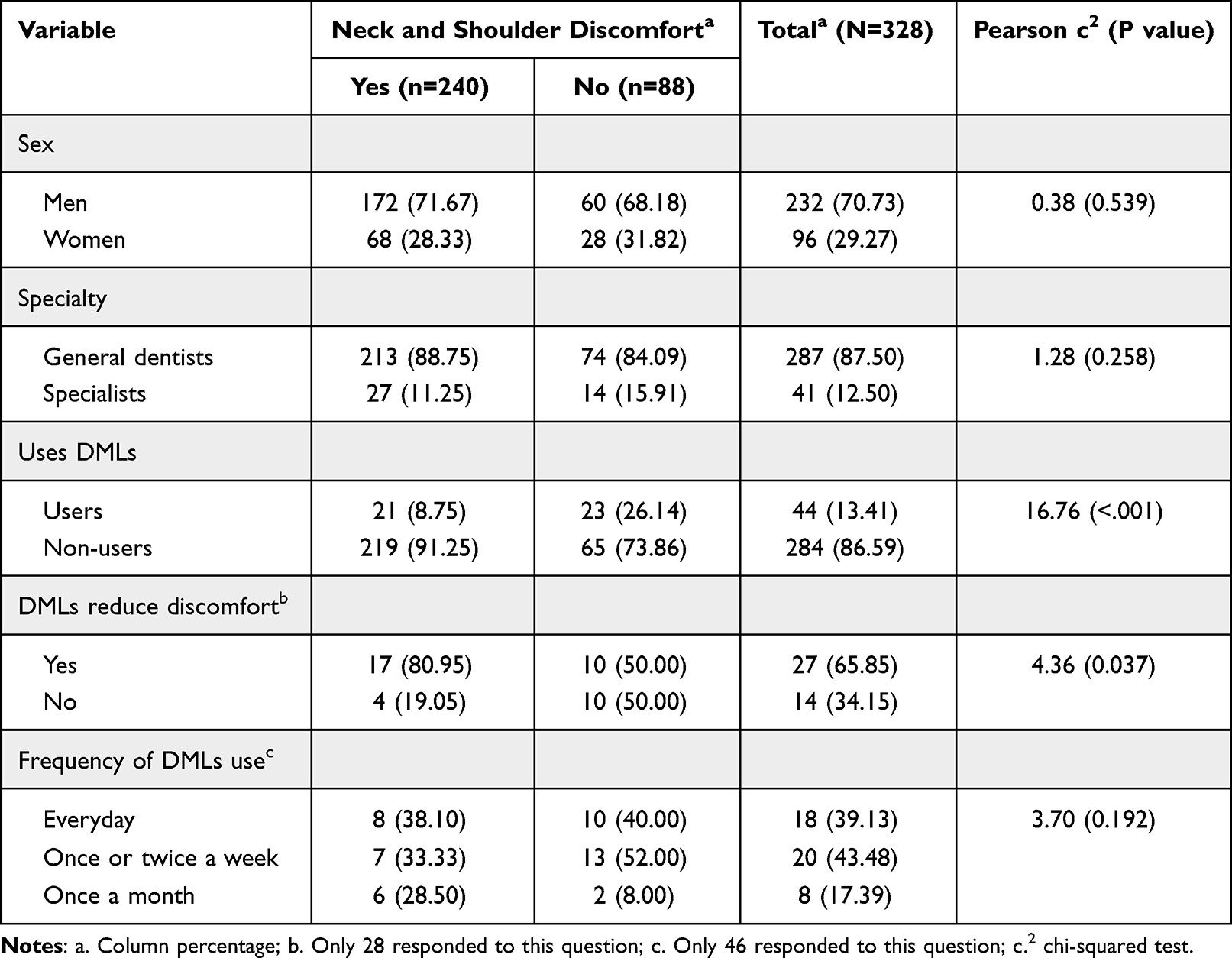 |
Table 4 Statistical Comparisons Between Having Neck and Shoulder Discomfort Among Different Subgroups |
Neck and shoulder discomfort has a significant association with DMLs use (c2 = 16.76, p < 0.001). Almost 91% dentists who had neck and shoulder discomfort (n = 219) did not use DMLs. Almost 81% of 46 dentists with neck and shoulder discomfort reported that DMLs reduced discomfort (p = 0.037).
Results in Table 4 showed that there was no significant association between the frequency of DMLs use and neck and shoulder discomfort (c2 = 3.70, p = 0.192).
Factors Affecting the Purchase Decision
Figure 3 presents percentages for factors affecting the purchase decision among specialized and general dentists. Field depth was the most rated factor affecting purchase decision among general dentists (68%), followed by magnification (63.4%), price (61%), and field width (48.8%). Price, on the other hand, was the most rated factor affecting purchase decision among specialized dentists (72%), followed by field depth (69.9%), magnification (58.7%), and field width (35%). The least chosen purchase decision factors by both dentists’ groups were resolution and patient-dentist distance, ranging from 31.7% to 7.3%.
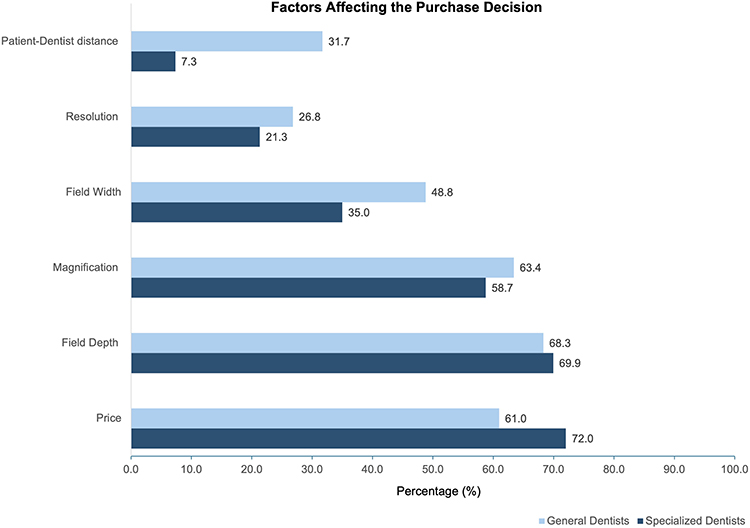 |
Figure 3 Percentages for factors affecting the purchase decision among general and specialized dentists. |
Discussion
This study hypothesized that the dentists’ purchasing decisions and use of DML are influenced by factors such as cost, prior training, ergonomic aspects, DML features, and dentist’s characteristics. Additionally, it is hypothesized that the use of DML is associated with the reported musculoskeletal pain. To test the hypotheses, the study surveyed 328 dentists practicing in Riyadh city and found that the prevalence of using DMLs was only 13.41%, which was lower than anticipated. In 1995, a survey conducted in Scotland revealed that the percentage of general dental practitioners who routinely used DMLs was only 9%.21 Similarly, another study from Scotland and other parts of the United Kingdom surveyed general dental practitioners in 2000 and found that 74% never used magnification in their practice, while only 8% used it routinely in more than half of their operating time.22 A more recent report from the United Kingdom in 2013 showed a prevalence of 31% among general dentists.23 This may indicate the increased usage of DMLs with time. In 2015, a study from Switzerland showed that 64% of the surveyed dentists owned a DML.24 A group of dentists from India were questioned about dental magnification in 2017, and 91.1% of them had the awareness about it, but only 23.8% had actually been exposed to using it.25 In 2018, a study from Saudi Arabia showed that 32.4% of the participating dentists used DMLs.26 Another survey from Saudi Arabia conducted in 2019 found that only 12.25% of all participants currently used DMLs.27 This study shows a very similar prevalence to the one reported in our present study, which is relatively lower than other studies. This could be explained by the inclusion of dental interns in the study sample, which was not done by the other studies reporting higher prevalence of DMLs usage. More than a third of the total participants of the present study (36.28%) were dental interns, typically just at the start of their careers in dentistry with relatively lower incomes. Understandably, the high cost of DMLs was the most identified barrier against their use.
Respondents in this study were questioned about the reasons behind using or not using DMLs, with respect to enhanced vision, patient care, clinical efficacy, and ergonomics. Better vision was the most chosen reason of DMLs usage. The high cost was the topmost reason for the non-use of DMLs, followed by the dentist wearing prescription glasses, insufficient training about DML use, and lastly the dentist having no interest. Another study found very similar reasons limiting the use of DMLs listed as expensive, insufficient training, wearing glasses, and not interested.23 The combined high cost of DMLs with the lack of training can impose a sense of uncertainty and hesitation towards the dentist’s decision to invest in one.
In addition to the expense of DMLs being the most identified barrier against their use, reported by 63% of participants, it was considered by 70% of participants as a major decision-making factor for purchasing DMLs. This finding is confirmed by previous studies.23,25,27 Based on this, it was suggested that dental schools play an active role in facilitating arrangements to offer DMLs for dental students at reduced cost in order to encourage DMLs use at an early stage of their dental career.
A significant correlation was found between the use of DMLs and being taught about them in dental school. Dentists who had been taught about DMLs in dental school were 1.64-times more likely to use them than those who were not. The majority of participants, users and non-users of DMLs believed that the most appropriate time to start using DMLs was during undergraduate clinical training. One study evaluated the attitudes towards magnification among undergraduate and postgraduate students in a dental school in Saudi Arabia and found that the majority of them preferred to have been introduced to dental magnification in the early years of dental school.28 They also reported that <25% of the teaching faculty actually implemented the use of dental magnification.28 Unfortunately, and contrary to what would be expected, Meraner and Nase found that not all faculty members involved in teaching believe that magnification should be taught to dental students early on in their undergraduate curriculum, regardless of the fact that they personally use magnification in their dental practice.29 There seems to be an unaddressed gap between the well-perceived benefits of magnification in dental practice and the implementation of serious steps towards including the use of magnification in dental education. This highlights the role of dental schools in taking the required actions to encourage dental students to adopt the use of DMLs early on in their dental career.
Another significant correlation was found between the use of DMLs and being a specialized dentist. Specialized dentists are 1.94-times more likely to use DMLs than general dentists. This may be partly explained by the increased need for visual enhancement due to age-related visual disturbances as reported by Forgie et al, who found a significant association between the use of DMLs and the dentist’s time of graduation from dental school.21 The visual performance of dentists was reported to be significantly influenced by their age, and many of them were found to be unaware of their visual limitations.24
Regarding the preferred type of DMLs, this study found that the FU type was more commonly used (75%) than the TTL type. Of all the DMLs users, 70.45% used an illumination system with their DMLs. This is in contrast to findings from the study by Farook et al, where the TTL type was more popular (56.7%) over the FU type, and a light source was used by half of the DMLs users (53.3%).23 The same preference for the TTL type was also reported by Basunbul.26 Adnan and Tabassum reported almost the same preference for the two types of DMLs.30 Although the TTL type provides a customized and more comfortable fit to the operator, the reduced cost and shareability among different operators of the FU type perhaps make it the preferred option for some operators.
The present study assessed decision-making factors taken into consideration when purchasing DMLs. The factors listed from most to least chosen are “Price” (70.73%), “Field Depth” (69.51%), “Magnification” (59.15%), “Field Width” (36.59%), “Resolution” (21.95%) and “Patient-Dentist distance” (10.37%). A similar study reported “Magnification” as the most considered factor when purchasing DMLs, followed by price.27 The most used magnification powers in our study were 2.5× (50%), 3.5× (45.45%), and 4× (4.55%), with similar distribution demonstrated by another similar study.27
Neck/shoulder discomfort was reported by 73% of all dentists included in this study. This prevalence falls within previously reported numbers ranging between 64% and 93%.1,2 A significant association exists between neck/shoulder discomfort and DMLs non-users (p < 0.001). The majority of dentists who have neck/shoulder discomfort (91%) did not use DMLs. Almost 81% dentists who have neck/shoulder discomfort reported that DMLs reduce discomfort (p = 0.037). A significant association found between DMLs non-users and musculoskeletal discomfort further confirms the role of DMLs in preventing musculoskeletal disorders, which was previously established by other studies.3–10,27 One study found that musculoskeletal shoulder pain was significantly lower in DMLs users than non-users.27 Farook et al found no difference in the prevalence of back/neck discomfort between users and non-users of DMLs.23 With musculoskeletal disorders being the main cause for early retirement among dentists,31 and the well-established effectiveness of the use of DMLs as a tool to enhance ergonomics in dental practice,3–10 it only seems judicious to recommend the early utilization of DMLs as a preventive measure against the development of work-related musculoskeletal disorders among dentists. A study reported a high prevalence of work-related musculoskeletal disorders among dental students (87%) recommending dental schools to adopt the needed policies for prevention.32 Another study also highlighted the need to include the use of magnification in pre-clinical training to help students maintain better ergonomics.4
Conclusion
Within the limitations of the current cross-sectional study being based on self-reporting and possibly not exploring all related factors, our results suggest that DMLs are under-utilized by dentists. Major factors limiting their use are the high cost and lack of training about their use in dental schools. Addressing these two factors may contribute to a positive shift in utilization of DMLs by a larger number of dentists. Future research may be targeted towards faculty members and administrators in dental schools to investigate the challenges and obstacles that limit integrating magnification in dental training and explore the impact of the years of service in the DML usage patterns employing a longitudinal study design. It cannot be overlooked that neck and shoulder discomfort was reported in this study by almost three-quarters of the participating dentists, the majority of whom did not use DMLs.
Abbreviations
DML, Dental magnifying loupes; FU, Flip-up; IRB, Institutional Review Board; KAIMRC, King Abdullah International Medical Research Center; OR, Odds ratios; TTL, Through the lens.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC) approval RC20/307/R. All participants gave written informed consent before participating in the study in accordance with the ethical approval granted by IRB of KAIMRC. Written consent was obtained from all study participants for voluntary participation in the study and publication of the results.
Acknowledgments
We thank the participants for their contributions to this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lietz J, Kozak A, Nienhaus A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: a systematic literature review and meta-analysis. PLoS One. 2018;13(12):e0208628. doi:10.1371/journal.pone.0208628
2. Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009;7(3):159–165. doi:10.1111/j.1601-5037.2009.00395.x
3. Branson BG, Bray KK, Gadbury-Amyot C, et al. Effect of magnification lenses on student operator posture. J Dent Educ. 2004;68(3):384–389. doi:10.1002/j.0022-0337.2004.68.3.tb03755.x
4. Carpentier M, Aubeux D, Armengol V, Pérez F, T P, Gaudin A. The effect of magnification loupes on spontaneous posture change of dental students during preclinical restorative training. J Dent Educ Apr. 2019;83(4):407–415. doi:10.21815/jde.019.044
5. Hong S, Park J, Jeon MJ, Shin SJ, Park JH, Park JW. Effect of loupe and microscope on dentists’ neck and shoulder muscle workload during crown preparation. Sci Rep. 2024;14(1):17489. doi:10.1038/s41598-024-68538-w
6. Maillet JP, Millar AM, Burke JM, Maillet MA, Maillet WA, Neish NR. Effect of magnification loupes on dental hygiene student posture. J Dent Educ. 2008;72(1):33–44. doi:10.1002/j.0022-0337.2008.72.1.tb04450.x
7. Rucker LM, Beattie C, McGregor C, Sunell S, Ito Y. Declination angle and its role in selecting surgical telescopes. J Am Dent Assoc. 1999;130(7):1096–1100. doi:10.14219/jada.archive.1999.0343
8. Branson BG, Abnos RM, Simmer-Beck ML, King GW, Siddicky SF. Using motion capture technology to measure the effects of magnification loupes on dental operator posture: a pilot study. Work. 2018;59(1):131–139. doi:10.3233/wor-172681
9. Plessas A, Bernardes Delgado M. The role of ergonomic saddle seats and magnification loupes in the prevention of musculoskeletal disorders. A systematic review. Int J Dent Hyg. 2018;16(4):430–440. doi:10.1111/idh.12327
10. Valachi B, Valachi K. Preventing musculoskeletal disorders in clinical dentistry: strategies to address the mechanisms leading to musculoskeletal disorders. J Am Dent Assoc. 2003;134(12):1604–1612. doi:10.14219/jada.archive.2003.0106
11. Zhang Y, Yuan P, Jiang H, et al. Application of medical magnifying loupes in diagnosis of oral mucosal diseases. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2021;50(2):205–211. doi:10.3724/zdxbyxb-2021-0132
12. Forgie AH, Pine CM, Pitts NB. The use of magnification in a preventive approach to caries detection. Quintessence Int. 2002;33(1):13–16.
13. Bud M, Jitaru S, Lucaciu O, et al. The advantages of the dental operative microscope in restorative dentistry. Med Pharm Rep. 2021;94(1):22–27. doi:10.15386/mpr-1662
14. Mamoun J. Use of high-magnification loupes or surgical operating microscope when performing dental extractions. N Y State Dent J Apr. 2013;79(3):28–33.
15. Wong AW, Zhu X, Zhang S, Li SK, Zhang C, Chu CH. Treatment time for non-surgical endodontic therapy with or without a magnifying loupe. BMC Oral Health. 2015;15:40. doi:10.1186/s12903-015-0025-7
16. Vasundhara V, Lashkari KP. An in vitro study to find the incidence of mesiobuccal 2 canal in permanent maxillary first molars using three different methods. J Conserv Dent. 2017;20(3):190–193. doi:10.4103/0972-0707.218308
17. Dadwal A, Kaur R, Jindal V, Jain A, Mahajan A, Goel A. Comparative evaluation of manual scaling and root planing with or without magnification loupes using scanning electron microscope: a pilot study. J Indian Soc Periodontol. 2018;22(4):317–321. doi:10.4103/jisp.jisp_139_18
18. Baumann DF, Brauchli L, van Waes H. The influence of dental loupes on the quality of adhesive removal in orthodontic debonding. J Orofac Orthop. 2011;72(2):125–132. doi:10.1007/s00056-011-0010-y
19. Low JF, Dom TNM, Baharin SA. Magnification in endodontics: a review of its application and acceptance among dental practitioners. Eur J Dent. 2018;12(4):610–616. doi:10.4103/ejd.ejd_248_18
20. AlBaker AA, Al-Ruthia YSH, AlShehri M, Alshuwairikh S. The characteristics and distribution of dentist workforce in Saudi Arabia: a descriptive cross-sectional study. Saudi Pharm J. 2017;25(8):1208–1216. doi:10.1016/j.jsps.2017.09.005
21. Forgie AH, Pine CM, Longbottom C, Pitts NB. The use of magnification in general dental practice in Scotland--a survey report. J Dent. 1999;27(7):497–502. doi:10.1016/s0300-5712(99)00030-5
22. Burke FJ, Wilson NH, Christensen GJ, Cheung SW, Brunton PA. Contemporary dental practice in the UK: demographic data and practising arrangements. Br Dent J. 2005;198(1):39–43. doi:10.1038/sj.bdj.4811956
23. Farook SA, Stokes RJ, Davis AK, Sneddon K, Collyer J. Use of dental loupes among dental trainers and trainees in the UK. J Investig Clin Dent. 2013;4(2):120–123. doi:10.1111/jicd.12002
24. Eichenberger M, Perrin P, Ramseyer ST, Lussi A. Visual acuity and experience with magnification devices in Swiss dental practices. Oper Dent. 2015;40(4):E142–9. doi:10.2341/14-103-c
25. Penmetsa GS, Mani LP, Praveen G, Dwarakanath CD, Awareness SS. Attitude, and prevalence of usage of magnification devices among the dental practitioners in the state of Andhra Pradesh - A questionnaire-based study. J Indian Soc Periodontol. 2017;21(5):398–402. doi:10.4103/jisp.jisp_268_17
26. Basunbul GI. Use of magnifying loupes among dental professionals. J Contemp Dent Pract. 2018;19(12):1531–1537.
27. Aboalshamat K, Daoud O, Mahmoud LA, et al. Practices and attitudes of dental loupes and their relationship to musculoskeletal disorders among dental practitioners. Int J Dent. 2020;2020:8828709. doi:10.1155/2020/8828709
28. Alhazzazi TY, Alzebiani NA, Alotaibi SK, et al. Awareness and attitude toward using dental magnification among dental students and residents at King Abdulaziz University, faculty of dentistry. BMC Oral Health. 2016;17(1):21. doi:10.1186/s12903-016-0254-4
29. Meraner M, Nase JB. Magnification in dental practice and education: experience and attitudes of a dental school faculty. J Dent Educ. 2008;72(6):698–706. doi:10.1002/j.0022-0337.2008.72.6.tb04535.x
30. Adnan S, Tabassum S. Perception and practices of operative and endodontic specialists in Pakistan towards the use of dental magnification. Work. 2021;70(4):1279–1287. doi:10.3233/wor-210045
31. Brown J, Burke FJ, Macdonald EB, et al. Dental practitioners and ill health retirement: causes, outcomes and re-employment. Br Dent J. 2010;209(5):E7. doi:10.1038/sj.bdj.2010.813
32. AlSahiem J, Alghamdi S, AlQahtani R, et al. Musculoskeletal disorders among dental students: a survey from Saudi Arabia. BMC Oral Health. 2023;23(1):795. doi:10.1186/s12903-023-03469-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.