Back to Journals » Cancer Management and Research » Volume 17

Decision-Making About Fertility Preservation After Cancer Diagnosis: A Qualitative Study of Patients’ Experiences and Perspectives
Authors Liao S ![]() , Tian X
, Tian X ![]() , Liu Z, Liu X, Chen O
, Liu Z, Liu X, Chen O
Received 13 June 2025
Accepted for publication 29 September 2025
Published 15 October 2025 Volume 2025:17 Pages 2403—2415
DOI https://doi.org/10.2147/CMAR.S543626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Shiyi Liao,1 Xuefei Tian,2 Zhuo Liu,1 Xiumei Liu,1 Ouying Chen1
1College of Nursing, Hunan University of Chinese Medicine, Changsha, 410208, People’s Republic of China; 2College of Integrative Chinese and Western Medicine, Hunan University of Chinese Medicine, Changsha, 410208, People’s Republic of China
Correspondence: Ouying Chen, Email [email protected]
Background: Rising cancer incidence in reproductive-aged individuals, coupled with improved long-term survival, indicates an increasing need for fertility preservation (FP) in this population. However, limited evidence exists on the decision-making of FP from the perspectives of cancer patients in a Chinese context. This qualitative study aimed to examine the patient perceptions of the FP decision and to identify barriers and unmet needs, addressing a significant gap within evolving precision oncology and fertility care contexts.
Methods: Face-to-face, semi-structured interviews were conducted with 12 cancer patients from a tertiary hospital in Hunan Province, China, from March 2024 to June 2024. The interviews were audio-recorded, transcribed verbatim, and analyzed thematically using Colaizzi’s seven-step analysis.
Results: Three themes and nine subthemes were identified: insufficient information support (lack of information sources, inappropriate timing of information disclosure, and poor doctor-patient communication); personal and family concerns (impact on cancer treatment, impact on offspring health, marital and reproductive status, financial constraints); ethical dilemmas (conflicts with survival needs, and emotional challenges).
Conclusion: Young cancer patients predominantly aspire to preserve fertility but face multiple decision-making challenges. To address these challenges, healthcare professionals should fully understand the patients’ needs, provide accurate and timely information tailored to their needs, and enhance communication skills to facilitate informed decision-making regarding FP, with important implications for clinical practice and public health.
Keywords: cancer patients, decision-making, decision aid, fertility preservation, qualitative
Introduction
Cancer is a significant public health concern worldwide, with a rapidly growing disease burden. According to the most recent estimates from the World Health Organization (WHO), the global new cancer cases will exceed 35 million by 2050, marking a 77% increase from 2022.1 Although cancer predominantly affects older adults, the recent few decades have seen an increasing trend of cancer incidence in younger populations of reproductive age. The International Agency for Research on Cancer (IARC) estimated that approximately 3.1 million new global cancer cases occurred in individuals aged 15–39 years in 2020.2
The advancement in cancer diagnosis and treatment has contributed to improved prognosis and increased survival rates.3 Patients with early-stage cancers can achieve a 5-year survival rate of 70% to 80%.4 However, cancer treatment, particularly chemotherapy and radiotherapy, may lead to adverse effects on human reproductive organs and gonads in both males and females, resulting in temporary, long-term, or even permanent infertility.5,6 A large body of research consistently reported that over 70% of young cancer patients express a strong desire to have children after their treatment, indicating the need for fertility preservation (FP).7 Fertility preservation is a process of freezing sperm, eggs, embryos, or reproductive tissues to protect or preserve an individual’s ability to have biological children.8 The American Society of Clinical Oncology (ASCO) also advocates that FP counseling should be provided to young cancer patients prior to treatment.9
To provide effective counseling and informed decision-making, healthcare providers must have a comprehensive understanding of the available fertility preservation options and their underlying biological mechanisms. Fertility preservation includes several established techniques, each with specific biological processes and clinical considerations. For males, sperm cryopreservation is the most direct method. A study conducted by Omes et al evaluated five distinct cryopreservation protocols for human sperm. The findings demonstrated that protocols incorporating a +4°C pre-cooling phase, specifically methods designated as M1 and M3, were most effective in preserving post-thaw sperm motility, viability, DNA integrity, and ultrastructural morphology when TEST-Yolk Buffer was employed as the cryoprotective agent.10 Options for female patients are more varied and technically advanced. Mature oocyte cryopreservation, embryo cryopreservation, and ovarian tissue cryopreservation are the main techniques available. Recent advances in vitrification techniques have significantly improved outcomes, with oocyte survival rates exceeding 75% and live birth rates reaching 35%.11 Embryo cryopreservation, typically performed at the blastocyst stage, shows even better results with survival rates above 95% and live birth rates of approximately 40% for women under 40 years old.11,12
Ovarian tissue cryopreservation offers a valuable option for prepubertal girls or patients who cannot undergo hormonal stimulation due to time constraints or hormone-sensitive cancers. This technique uses either slow-freezing protocols or newer vitrification methods.13 Clinical protocols have also evolved to include random-start ovarian stimulation, which allows treatment to begin at any point in the menstrual cycle, reducing the time needed to just two weeks. Additionally, dual stimulation protocols enable two egg retrievals within a single month, maximizing the number of preserved oocytes.14
The implementation of these techniques, however, involves complex ethical and regulatory considerations that healthcare providers must navigate carefully. Ethical challenges center on informed consent, particularly for adolescents and young adults who may feel overwhelmed by their cancer diagnosis. The concept of reproductive autonomy becomes complex when considering future use of preserved materials, changing life circumstances, and the rights of future partners.15 Religious and cultural beliefs may also conflict with certain preservation methods, especially those involving embryo creation or manipulation.16
Regulatory frameworks differ widely in terms of storage duration (usually 10–15 years with possible extensions), quality standards, and consent requirements. These differences create significant disparities in access to care, insurance coverage, and legal protections.17 Such inequalities particularly affect vulnerable populations and highlight the need for standardized guidelines that balance patient choice with ethical considerations while ensuring fair access to reproductive healthcare services.
The decision-making process for FP in cancer patients is a complex interplay among the patient characteristics, physician characteristics, and the broader socio-cultural environment.18 Patient factors include demographic characteristics (eg, age, gender, education, and socio-economic status), health literacy, past experiences, and personal beliefs.19 Physician factors encompass their personal characteristics (eg, values, beliefs, and biases), clinical experiences, workload and time constraints, and communication skills.20 Environmental factors involve multiple contextual elements, such as social resources and support, the settings, countries, cultures, and legal and ethical considerations.21 All these factors influence the way patients access and understand information to make informed decisions.18 It is thus crucial to fully understand these factors to provide adequate care and support to facilitate the decision-making process.
However, significant differences exist in the FP decision-making in cancer patients across countries, with more resources and legal support available in more developed countries.22–24 For instance, the United States and European countries have issued multiple guidelines underscoring the necessity of informed consent and the respect for reproductive rights.9,25 These guidelines advocate for the inclusion of FP as a standard component of cancer care for patients of reproductive age.9,25 In contrast, in developing countries like China, the policy and practice of FP decision-making remain scarce and underdeveloped. Chinese Confucian culture highly values family continuity and family lineage, with children expected to continue the family name and legacy.26 As a Confucian proverb reads: “There are three ways of being unfilial, and to have no posterity is the greatest of them” (bu xiao you san, wu hou wei da).27 Therefore, maintaining fertility during cancer treatment is essential in the Chinese context. Although some experts in China have highlighted the importance of FP for cancer patients, few studies have explored the decision-making process of FP from the patient’s perspective.
To fill in the research gap, we conducted a qualitative study to examine the experiences and perceptions of FP decision-making in a sample of cancer patients in China. We mainly focused on identifying their unmet needs and the barriers to FP decision-making to gain deeper insights into the challenges they confront in this process. Understanding these challenges and needs would help guide future policy and practice to enhance patient engagement and improve doctor-patient communication to ensure effective, informed decision-making. It will also help optimize resource allocation and utilization, ultimately improving the overall well-being of individuals and communities.
Methods
Study Design
This study utilized a descriptive qualitative approach, employing semi-structured interviews to collect data. This approach is used to depict or extrapolate a phenomenon or event in question, focusing on the lived experiences of participants to obtain a detailed, comprehensive, and direct description of the phenomenon under investigation.28,29 Semi-structured interviews involve a pre-determined set of questions, followed by open questions based on the interviewee’s responses, which allows for a more profound understanding and exploration of personal experiences and perspectives.30 The research team consisted of nine members: a chief nurse, a chief physician of oncology, four specialist nurses, and three master’s students. All researchers received systematic and standard training in qualitative research with a complete understanding of FP decision-making among cancer patients prior to the study. This reporting of this study adhered to the Standards for Reporting Qualitative Research (SRQR) checklist.
Participants
From March to June 2024, 12 cancer patients from a tertiary hospital in Hunan Province were selected for semi-structured interviews using a purposive sampling method. The inclusion criteria were as follows: 1) aged 18–39 years old, 2) with a pathologic diagnosis of cancer, 3) with normal fertility before cancer diagnosis, and 4) proficiency in Mandarin, meeting visual and hearing standards. The exclusion criteria included: 1) in the terminal stage of cancer with an estimated survival duration ≤ 6 weeks; 2) unable to complete the study due to cognitive dysfunction or psychiatric disorders. The sample size was determined based on data saturation when the data were presented repeatedly, and no new themes emerged during data analysis.
Data Collection
Information was gathered through face-to-face, semi-structured interviews with the patients. A preliminary interview guide was developed based on the objectives of the study, integrating insights from the literature review and researcher discussion. The interview guide was pilot-tested in a small group of patients and one nurse. Based on feedback from the interviewees, adjustments were made to enhance the interview structure. Additionally, consultation and discussions with cancer experts were conducted to finalize the interview guide, which is shown in Table 1.
 |
Table 1 Semi-Structured Interview Guide |
The interviews took place in the nurse manager’s office, ensuring a quiet interview environment. The participants were fully informed about the study’s purpose, procedure, benefits, and risks, and signed the informed consent form prior to the interviews. All interviews were audio recorded, and the researcher encouraged participants to share their experiences and thoughts openly during the interview. The interviewers attentively observed and documented the participants’ facial expressions, tones of voice, and body language, repeating and confirming the participants’ perspectives to gain insight into their feelings and thoughts. Field notes were maintained to increase the credibility of the interview data. Finally, a total of 12 participants were interviewed, with the interview duration ranging from 30 to 45 minutes.
Data Analysis
After each interview, the recording was promptly transcribed within 24 hours. This written record is then analyzed to identify areas for improvement in future interviews, such as interviewer performance and questions underexplored, to enhance the overall quality of data collection. The participants were coded anonymously as N1-N12, and the transcribed text was categorized based on field notes, which is shown in Table 2. The interview data analyzed using Colaizzi’s seven-step analysis method,31 which involved the following steps: (i) reading and re-reading the transcripts to obtain a general sense; (ii) extracting significant statements that relate to the study topic; (iii) formulating meanings from the significant statements; (iv) clustering the meanings into themes and subthemes; (v) integrating the findings into an exhaustive elaboration; (vi) describing the fundamental structure of the phenomenon; (vii) validating the findings from the participants. Data were analyzed using NVivo© software (QSR International version 11.0, Australia).
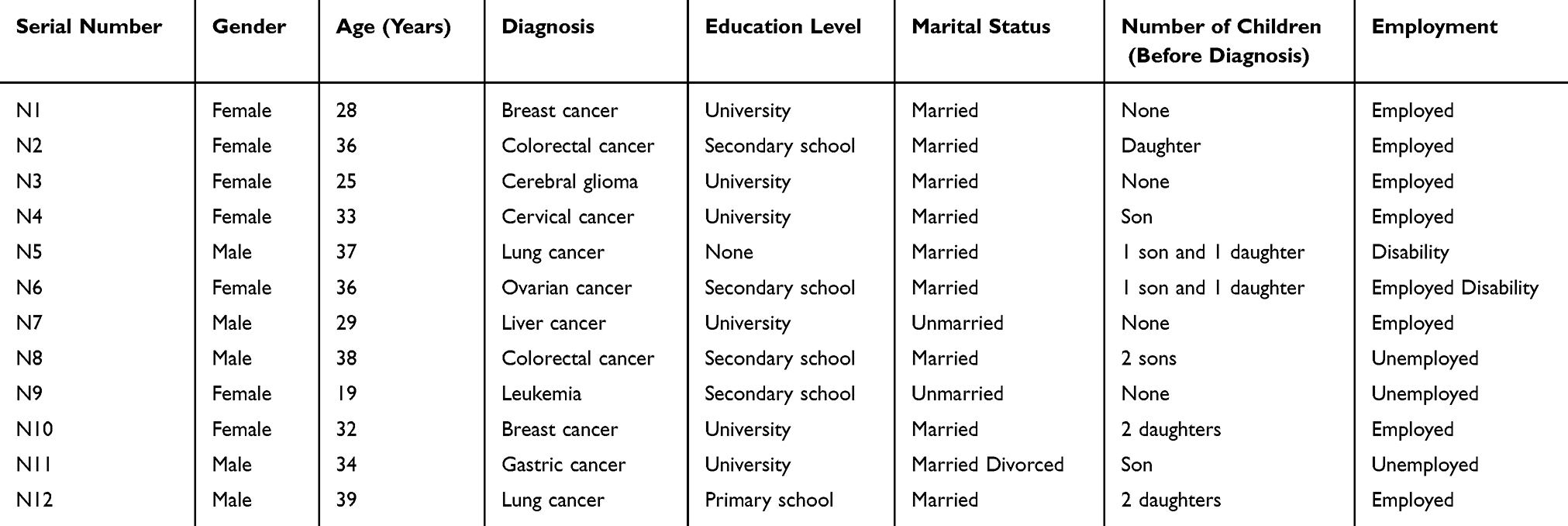 |
Table 2 Characteristics of Participants (N=12) |
Rigor
We employed the criteria of credibility, confirmability, and transferability to ensure the rigor of this study.32 The analysis involved triangulation,33 and researchers with diverse backgrounds engaged in independent research to minimize bias and improve reliability.34 Two researchers independently transcribed the audio recordings, coded the text, analyzed the data, and compared their findings to confirm the themes. When the researchers held different opinions on the topic, a group discussion was held to resolve disagreements. Furthermore, an additional nurse from the hospital, who was not involved in the study, was also invited to provide a critique from an outsider’s perspective. Finally, the data obtained was presented back to the participants for confirmation to increase credibility.
Results
Twelve participants were ultimately included in the analysis, and their characteristics are detailed in Table 2. There were seven females (58.33%) and five males (41.67%), and their average age was 32.2 ± 5.95. Their diagnoses included breast cancer (n=2), colorectal cancer (n=2), lung cancer (n=2), cerebral glioma, cervical cancer, ovarian cancer, leukemia, gastric cancer, and liver cancer. Half of the participants had a university education (50%), and most were married (75%), had kids (66.67%), and were employed (66.67%).
The analysis identified three main themes and nine subthemes: (i) Insufficient information support: lack of information sources, inappropriate timing of information disclosure, and poor doctor-patient communication; (ii) Personal and family concerns: impact on cancer treatment, impact on offspring health, marital and reproductive status, and financial constraints; (iii) Ethical dilemmas: conflicts with survival needs, and emotional challenges.
Insufficient Information Support
This theme focuses on crucial aspects such as the availability of information, the timing of its delivery, and the communication processes between patients and healthcare providers. It highlights the obstacles that patients encounter while trying to access essential information for making informed decisions about FP. Additionally, it emphasizes the importance of timely information and calls for improvements in communication strategies to enhance patient comprehension and autonomy.
Lack of Information Sources
When questioned about how they acquired information regarding FP, most cancer patients expressed encountering challenges in accessing this information. Young cancer patients have a strong desire and take proactive approaches in seeking reproductive health information. However, the online sources of FP often contain misleading or unverifiable information. Consequently, they anticipate that healthcare providers will offer diverse channels to adequately address their informational needs, which can significantly alleviate patients’ anxiety and depression associated with uncertainty. Following their diagnosis, cancer patients primarily engage with healthcare professionals, whom they regard with trust and reliance. However, when healthcare providers fail to meet these informational needs effectively, patients may develop negative emotions, resulting in decision conflict and regret.
I didn’t go to school, I can’t read books or newspapers, and I don’t know how to learn this online. (N5);
Sometimes I am too embarrassed to take the initiative to ask healthcare professionals, but I actually want them to ask me questions and open up a dialog. (N3);
I don’t know how I should find the information I want to know, there will be a lot of false information spreading. (N1);
I have been learning about fertility preservation since I got sick, and I have discussed with my family about going to a professional organization to ask about it, but appointments are often queued up for a long time before they are being postponed. (N6);
No one told me that cancer treatment would affect my fertility, and I still very much desire to have a well-behaved daughter. (N9);
This is a lot of complicated knowledge, and I don’t remember it when I want to talk about it. I wish there were science pamphlets. (N11)
Inappropriate Timing of Information Disclosure
Patients express a strong desire for comprehensive information regarding the effects of cancer treatment on fertility before initiating any procedure. This knowledge enables them to engage in thoughtful consideration and preparation. Moreover, they seek social support and success narratives to boost their confidence and improve their abilities to make informed decisions.
It would be better if the doctor had told me before I had the operation that it would affect my fertility so that I could have been prepared. (N12);
I am going to have chemotherapy soon, and the time left for me to make a decision is too short; if I could have been told earlier, I could have thought it through more thoroughly. (N8);
It would be better if I could have talked to a friend who has had experience with fertility preservation, and I would have been more hopeful knowing that someone else had been successful. (N7);
My doctor told me that I was having breast surgery in a week, during which I could decide whether or not I wanted to freeze my eggs, but I didn’t have any prior information about this and couldn’t make a good decision at short notice, and I don’t know if I would have regretted it. (N1)
Poor Doctor-Patient Communication
There is an expressed urgency among patients to obtain information about FP; however, they frequently encounter communication barriers with healthcare providers. Many patients have a limited understanding of FP, such as the available options and success rates. Additionally, discrepancies between patient priorities and physician recommendations regarding treatment and future fertility plans underscore the importance of more personalized and more transparent communication in healthcare.
Although the doctor did answer my questions, what he said was so deep and specialized that there was still a lot I didn’t understand. (N2);
I already have two children, but when I talked to the doctor, he didn’t understand why I still wanted to do fertility preservation. (N10);
After talking to the doctor, he still didn’t answer my questions, maybe I didn’t ask in the right way. (N1);
I would like to know what the probability of success with fertility preservation is, but the doctor could not tell me clearly either. (N7);
I told the doctor that I wanted to have a child first before having the treatment, but the doctor felt that the treatment was more important, and after discussing it twice, no one was willing to budge. (N3);
If I conceive naturally after successful treatment, what will I do with the frozen eggs? (N4);
I don’t know what fertility preservation is, and I don’t understand what the doctor explained to me. (N10)
Personal and Family Concerns
Patients frequently feel isolated and may struggle to secure the emotional support they need while navigating the decision-making process regarding FP, balancing family expectations, and their health challenges. Family members often encounter difficulties in fully understanding the patient’s viewpoint. Healthcare providers, while dedicated to combating disease, may unintentionally neglect patients’ emotional needs. The decision to preserve fertility involves navigating numerous challenges, including personal, relational, and financial obstacles.
Impact on Cancer Treatment
Patients express uncertainties and concerns that FP might negatively impact their cancer treatment. Patients worry that embryo freezing may affect treatment outcomes and fear that pregnancy may heighten the risk of recurrence and metastasis, particularly in cases of hormone-sensitive cancers.
Freezing the embryos may affect my treatment, and no one will be able to help me if I get worse. (N11);
I want to try, but I’m worried, what if my cancer comes back after I get pregnant? (N6);
My doctor said that my cancer is hormone-sensitive, and pregnancy will raise the hormone level in my body, so what should I do if my condition worsens? (N10);
What should I do if my cancer metastasizes after I get pregnant? I’ve seen news like this, and it scares me. (N2)
Impact on Offspring Health
The desire for their children’s well-being is a deeply ingrained, universal parental instinct, motivating them to consider various aspects of their child’s upbringing and future.
Will my cancer be passed on to my child? (N4);
What if I have chemotherapy that causes problems with my genes? (N5);
If my eggs are damaged by chemotherapy, will I give birth to a deformed child? (N1);
My first child was congenitally disabled, so I still have the desire to have a healthy child. (N11);
Now I can’t even take care of myself, how can I give my child happiness? It may even affect the child’s mental health? (N9);
I have a healthy and active child; I don’t want to have another child with health risks. (N2)
Marital and Reproductive Status
The decision to pursue FP after a cancer diagnosis is significantly influenced by a patient’s family dynamics and emotional support network. Participants emphasize the importance of familial relationships in their fertility-related decisions, highlighting the critical role of family support. Some are content with their existing family structure and their current number of children, thus deciding to have no more children. In contrast, some desire to maintain their reproductive capabilities, often with their partner’s support.
I have a child from my previous marriage, and I want to wait for my child to fully integrate into the new family before considering having another child. Otherwise, my child will feel left out. (N4);
My husband has provided great support and made me realize the beauty of a new life, so I still want to take advantage of assisted reproduction techniques. (N2);
I already have two kids, and my family feels contented with that, except for my illnesses, I am still pleased with my life. (N12);
I have no child, for this reason I have been discussing with my husband for a long time, he still supports me to keep my fertility and inspires me. (N3)
Financial Constraints
Economic constraints constitute a significant barrier for many patients seeking FP. In addition to the high costs of the cancer treatment itself, procedures like cryopreservation and reproductive organ transplantation can add substantial financial burdens to individuals and families, often making them unaffordable for many.
The most fundamental reason I didn’t freeze my eggs was that I couldn’t afford it financially, and I didn’t have insurance. (N6);
The technique doesn’t always work, and I still have to save money for treatment. (N5);
I couldn’t afford fertility treatments and was sad that I wouldn’t be able to conceive a new life. (N4);
If I had fertility preservation, then I would have to pay for both the cancer treatment and the fertility treatments, which I couldn’t afford. (N11);
My parents have already spent a lot of money on my cancer treatment, and I don’t want them to worry about my fertility anymore. (N9)
Ethical Dilemmas
Cancer patients frequently encounter ethical dilemmas when making FP decisions. They need to balance between prioritizing survival and preserving future fertility. Patients often feel overwhelmed and lack sufficient emotional support throughout the decision-making process. Family members may struggle to understand the complexities of the patient’s condition, while healthcare professionals may prioritize disease treatment, potentially overlooking the patient’s emotional needs.
Conflicts with Survival Needs
Following a cancer diagnosis, patients typically prioritize treatment and survival, influenced by the immediate threat to life and the focus on immediate medical needs. Therefore, they may delay considering fertility-related issues.
Ever since I got sick, I have little energy to think about anything else, I hope that I can succeed in my fight against cancer. (N9);
I am afraid of losing my life, and I still have so many people and things I am attached to. (N6);
I feel that the most urgent thing right now is to cure the disease. (N2);
My family is very worried about me, so I will focus on treatment and wait until the right time to think about having children. (N1)
Emotional Challenges
Patients often face a challenging and lengthy process when deciding whether to pursue FP. Those opting for FP find themselves struggling between the roles of “cancer patients” and “fertility patients”, leading to potential feelings of shame due to external judgment or lack of comprehension from others. Conversely, excessive attention can also induce insecurity. Some patients who decline FP cite the heavy psychological burden of the disease, expressing confusion and helplessness with inadequate emotional support from their surroundings.
I was very eager to try embryo freezing after learning that it was possible, but since I made this decision, I feel that everyone is looking at me and talking about me, and I feel very insecure, as if I have no privacy at all. (N3);
When I talked to my doctor about fertility preservation treatments, he said that he did not support them and that they might adversely affect the treatment of my illnesses. (N4);
My family still thinks that it is better to conceive naturally and doesn’t want to use these techniques. (N2);
After I got sick, I was often in a bad mood and wanted someone to listen to me and give me advice. (N10)
Discussion
Major Findings
In China, fertility preservation for cancer patients holds unique significance due to the strong societal emphasis on familial continuity and China’s former one-child policy, which, though relaxed, has led to a cultural preference for having children.2 However, cancer patients face numerous challenges in the decision-making process of fertility preservation, which has been clustered into three themes and nine subthemes in our study: insufficient information support (lack of information sources, inappropriate timing of information disclosure, and poor doctor-patient communication); personal and family concerns (impact on cancer treatment, impact on offspring health, marital and reproductive status, financial constraints); ethical dilemmas (conflicts with survival needs, and emotional challenges). Identifying these barriers is crucial for designing effective interventions that are tailored to the specific needs and challenges faced by cancer patients, which can enhance the broader application and sustainability of the interventions, ultimately improving the well-being of patients.
Our study highlights the importance of strengthening education about fertility preservation among cancer patients, which should be integrated into cancer treatment protocols within China’s healthcare framework. The UK-based charity, Fertility Preservation in Cancer (FPIC), supports cancer patients by offering guidance and financial aid related to fertility preservation.35 FPIC collaborates with medical facilities to guarantee that patients receive essential counseling prior to treatment, which sets a good example for other countries to learn.35 To align with China’s regional diversity of languages, it is feasible to craft localized educational materials, such as simplified Mandarin and dialect versions, to cater to learners with varying language proficiency and educational backgrounds.36 The timing of information dissemination is pivotal, and it is recommended that Chinese healthcare providers should integrate fertility discussions into the initial cancer consultation.37 This approach ensures patients receive timely information and referrals, empowering them to make informed decisions about fertility preservation.37 The doctor-patient communication challenges indicate the need for more training on communication skills to instruct healthcare professionals to convey information in a culturally considerate and patient-centric fashion.
Our study suggests that personal and familial considerations, particularly financial constraints, play a significant role in the decision-making process of fertility preservation, as families also shoulder the added burden of cancer treatment.38 The high costs of fertility preservation procedures, coupled with limited insurance coverage, constitute a significant barrier to accessing healthcare services, leading to uncertainty and concerns about future fertility.39 Despite China’s substantial annual medical expenditure of approximately 9 trillion yuan, the public still faces significant challenges in accessing affordable and convenient healthcare.40 To tackle the complex and expensive medical care dilemma, a multi-pronged approach is needed. It is imperative to reform the healthcare system, optimize resource allocation, improve service efficiency, regulate drug prices, break up monopolies, standardize medical fees, expand medical insurance coverage, and raise reimbursement rates. These measures are essential to reduce disparities in healthcare, making it more accessible and affordable for all.
Finally, our study shows that ethical dilemmas frequently arise in patient care, as survival is often prioritized over fertility.41 It is imperative for healthcare providers to recognize that comprehensive support, encompassing psychological and social aspects, is essential beyond just physical treatment. A multidisciplinary approach involving psychologists, social workers, and fertility experts to offer holistic care is crucial for supporting cancer patients emotionally.42 A comprehensive and strong support network can help patients navigate the emotional and practical challenges of cancer treatment, ensuring their overall well-being.43 Family and societal support significantly impact patients’ ability to make informed and effective healthcare decisions. Education and public awareness campaigns can dramatically reduce stigma and social pressures related to cancer treatment and fertility preservation. These measures can foster a more supportive environment for cancer patients to seek fertility preservation help and make informed decisions about their care, both in the short and long term.
Implications for Practice and Research
Shared decision-making is a crucial approach in healthcare that involves patients and doctors working together to make informed choices about treatment and care, which can improve patient outcomes, increase patient satisfaction, and enhance treatment adherence. Our study highlights the crucial role of healthcare professionals in accurately identifying patients’ fertility needs and providing comprehensive information about FP options. Patients should be empowered to make informed decisions about their reproductive future based on their individual needs, desires, and circumstances while maintaining the right to autonomy in this process. Healthcare professionals should prioritize clear, timely communication with patients to ensure they feel informed, supported, and understood.
Next, intelligent assisted decision-making tools should be developed to facilitate FP decision-making in the future. The application of artificial intelligence (AI), machine learning, and other new technologies has significantly improved medical diagnosis and treatment, making the process more convenient and accurate.44 AI tools can be applied in various aspects of healthcare to facilitate shared decision-making between doctors and patients. AI-driven decision-making can integrate multimodal information sources, such as medical records, literature, and patient profiles, to create a more personalized and efficient decision-making process.45 This process leverages technologies like machine learning and key element topping to facilitate a three-way interaction between doctors, patients, and AI tools, ultimately helping patients make choices aligned with their values.
Our findings show that it is very important to include wider public health views in oncofertility counseling and decision-making.9 Specifically, the management of modifiable health factors, such as obesity, must be addressed as part of a comprehensive fertility preservation strategy.46 Obesity is a known risk factor for multiple cancers and is also associated with reduced success rates in assisted reproductive technologies.11,47 Evidence indicates that obesity can make gonadotoxic effects worse and reduce how ovaries respond to stimulation, so it lowers how well fertility preservation works.48 Healthcare providers should therefore emphasize the importance of weight management and metabolic health as part of pretreatment counseling, following a preventative and health promotive approach.
Furthermore, extra attention is needed for patients with inherited cancer syndromes like Lynch syndrome, which raises the risk of endometrial and other cancers.49 These patients bring special counseling difficulties because of genetic aspects and the chance of passing risks to children. The informed consent process must include full genetic counseling, covering the risks of inherited mutations and choices such as preimplantation genetic testing.50 International guidelines advise that genetic counseling should be given before fertility preservation to support fully informed decisions.51 This is both a clinical must and an ethical need to protect patient independence and reproductive justice.
From a legal view, the duty to give detailed and personalized counseling is supported by international ethics standards and legal cases.52 The Italian National Committee for Bioethics, among others, has stated that consent must be informed, specific, and without pressure, and these ideas also apply to talks about genetic risks and lifestyle changes.53 Also, as oncofertility services grow, unfairness in access stays a serious problem.54 Policymakers and institutional leaders should push for fertility preservation to be part of public health coverage, especially for high-risk groups and people with genetic risks, to make sure everyone has fair access to these key services.55
Given these challenges, future research should work on creating tested decision tools that include genetic details, personal risk estimates, and health behavior changes. Interprofessional teamwork, including oncologists, reproductive specialists, genetic counselors, mental health professionals, and nutritionists, is needed for patient-centered care that covers both body and mind aspects.
Finally, health systems must do better in supporting long-term care. Important steps include making clear referral paths, ensuring continuous care from cancer diagnosis through survival, and teaching patients about long-term health and fertility results. Through combined, ethically aware practices, oncofertility care can achieve its two main goals: saving fertility and supporting overall health.
Limitations
Our study has several limitations. First, the small, purposive sample recruited from one single hospital may not represent the broader population, which may limit the generalization of our findings to a larger context. Future multi-center studies using larger samples are needed to validate our findings further. Second, the study was limited to the perspectives of cancer patients, without involving the viewpoints of patients’ families and medical staff. Future studies should incorporate the opinions of multiple stakeholders to gain a more comprehensive understanding of the FP decision-making. Finally, the qualitative study design may introduce biases, such as self-selection bias in participant recruitment. Additionally, interpretation of qualitative data can be subjective and influenced by the researcher’s perspectives, causing potential bias. Future studies should consider a mixed-method study design combining qualitative and quantitative approaches to improve the robustness and reliability of the results.
Conclusions
Our study demonstrated that young cancer patients predominantly aspire to preserve fertility but face multiple decision-making challenges, including insufficient information support, personal and family concerns, and ethical dilemmas. Key measures to overcome these barriers require a multidisciplinary approach that integrates physical, psychological, social, legal, and policy aspects. Some specific measures include incorporating fertility education into cancer treatment protocols, creating localized educational resources tailored to specific patient demographics and preferences, and effectively disseminating information through multiple channels to ensure well-informed decision-making. Additionally, systemic reforms, such as expanding healthcare insurance and implementing financial navigation programs, can alleviate the economic burden of cancer and healthcare costs. Furthermore, psychosocial support should be strengthened to address ethical dilemmas and conflicts between FP and survival needs.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, Ouying Chen. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Ethics Approval and Consent to Publish
The study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Hunan University of Chinese Medicine Ethics Committee (Approval No. HN-LL-GZR-2024-073) on March 1st, 2024. The study was carried out in compliance with the World Medical Association Code of Ethics (Declaration of Helsinki). Written informed consent for publication was obtained from all patients or their legally authorized representatives. This consent specifically authorizes the publication of de-identified case details, clinical findings, treatment data, and all associated images (including those in Table 2), with the understanding that all personally identifiable information has been removed. For deceased patients, consent was provided by their next of kin. The CARE guidelines (https://www.care-statement.org/) were followed in reporting case details.
Consent to Participate
Informed consent was obtained from all individual participants included in the study. The participants informed consent included publication of anonymized responses/direct quotes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (NSFC) [grant number: 82074450].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Loud JT, Murphy J. Cancer screening and early detection in the 21st century. Semin Oncol Nurs. 2017;33(2):121–128. doi:10.1016/j.soncn
2. Miller KD, Nogueira L, Devasia T, et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022;72(5):409–436. doi:10.3322/caac.21731
3. World Health Organization. Global cancer burden growing, amidst mountingneed for services. Available from: https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing--amidst-mounting-need-for-services.
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Bedoschi G, Navarro PA, Oktay K. Chemotherapy-induced damage to ovary: mechanisms and clinical impact. Future Oncol. 2016;12(20):2333–2344. doi:10.2217/fon-2016-0176
6. Delessard M, Saulnier J, Rives A, et al. Exposure to chemotherapy during childhood or adulthood and consequences on spermatogenesis and male fertility. Int J Mol Sci. 2020;21(4):1454. doi:10.3390/ijms21041454
7. Flink DM, Sheeder J, Kondapalli LA. A review of the oncology patient’ s challenges for utilizing fertility preservation services. J Adolesc Young Adult Oncol. 2017;6(1):31–44. doi:10.1089/jayao.2015.0065
8. Doungkamchan C, Orwig KE. Recent advances: fertility preservation and fertility restoration options for males and females. Fac Rev. 2021;10:55. doi:10.12703/r/10-55
9. Rebar RW, Keator CS. Expanding our knowledge of premature ovarian insufficiency. Fertil Steril. 2021;115(2):328–329. doi:10.1016/j.fertnstert.2020.09.145
10. Omes C, Savio M, Mazzini G, et al. Morphological and functional analysis of cryopreserved human sperm: comparison of different freezing protocols. Cryo Letters. 2025;46(4):261–273.
11. Mutlu L, Manavella DD, Gullo G, et al. Endometrial cancer in reproductive age: fertility-sparing approach and reproductive outcomes. Cancers. 2022;14(21):5187. doi:10.3390/cancers14215187
12. Korzekwa AJ, Buzan E, Pokorny B, et al. Effective cryopreservation of post mortem-collected roe deer gametes by evaluation of post-thaw oocyte and sperm characteristics and in vitro fertilization. Animals. 2025;15(16):2335. doi:10.3390/ani15162335
13. Jones ASK, Shikanov A. Ovarian tissue cryopreservation and novel bioengineering approaches for fertility preservation. Curr Breast Cancer Reports. 2020;12(4):351–360. doi:10.1007/s12609-020-00390-z
14. Pirooznia P, Meighani EM, Ghaffari F. Exploring new frontiers in oncofertility preservation: a case of ovarian stimulation during pregnancy. Jovarian Res. 2025;18(1):39. doi:10.1186/s13048-025-01615-4
15. Zaami S, Melcarne R, Patrone R, et al. Oncofertility and reproductive counseling in patients with breast cancer: a retrospective study. J Clin Med. 2022;11(5):1311. doi:10.3390/jcm11051311
16. Ngan OM, Ng EH, Yue Y, et al. Planned oocyte cryopreservation in Hong Kong: a potential prototype for Mainland China. Sexual Reprod Health Matters. 2025;33(1):2485547. doi:10.1080/26410397.2025.2485547
17. Zaami S, Montanari Vergallo G, Moscatelli M, et al. Oncofertility: the importance of counseling for fertility preservation in cancer patients. Eur Rev Med Pharmacol Sci. 2021;25(22):6874–6880. doi:10.26355/eurrev_202111_27235
18. Tariman JD, Berry DL, Cochrane B, et al. Physician, patient, and contextual factors affecting treatment decisions in older adults with cancer and models of decision making: a literature review. Oncol Nurs Forum. 2012;39(1):E70–E83. doi:10.1188/12.ONF.E70-E83
19. Angarita FA, Elmi M, Zhang Y, et al. Patient-reported factors influencing the treatment decision-making process of older women with non-metastatic breast cancer: a systematic review of qualitative evidence. Breast Cancer Res Treat. 2018;171(3):545–564. doi:10.1007/s10549-018-4865-0
20. Hardy V, Yue A, Archer S, et al. Role of primary care physician factors on diagnostic testing and referral decisions for symptoms of possible cancer: a systematic review. BMJ Open. 2022;12(1):e053732. doi:10.1136/bmjopen-2021-053732
21. Yeom JW, Yeom IS, Park HY, et al. Cultural factors affecting the self-care of cancer survivors: an integrative review. Eur J Oncol Nurs. 2022;59:102165. doi:10.1016/j.ejon.2022.102165
22. American Society for Reproductive Medicine (ASRM). Fertility preservation in patients undergoing gonadotoxic therapy or gonadectomy for cancer or other conditions: a committee opinion. Fertility and Sterility. 2015;103(1):e1–e9. doi:10.1016/j.fertnstert.2014.10.024
23. European Society of Human Reproduction and Embryology (ESHRE). ESHRE-ESI guideline on fertility preservation. Human Reproduction Open. 2018;1:hoy001. doi:10.1093/hropen/hoy001
24. Mulder RL, Font-Gonzalez A, Hudson MM, et al. Fertility preservation for female patients with childhood, adolescent, and young adult cancer: recommendations from the PanCareLIFE consortium and the international late effects of childhood cancer guideline harmonization group. Lancet Oncol. 2021;22(2):e45–e56. doi:10.1016/S1470-2045(20)30594-5
25. Schover LR, Rybicki LA, Martin BA, et al. Having children after cancer. A pilot survey of survivors’attitudes and experiences. Cancer-Am Cancer Soc. 1999;86:697–709. doi:10.1002/sici1097-01421999081586:4<697::aid-cncr20>3.0.co;2-J
26. Gu C, Li Z. The Confucian ideal of filial piety and its impact on Chinese family governance. J Sociol Ethnol. 2023;5(2):45–52. doi:10.23977/jsoce.2023.050208
27. Yan W, Huang C, Chen L, et al. Experiences of autonomy in marriage and divorce within the Chinese traditional system. J Family Issues. 2023;44(6):1547–1571. doi:10.1177/0192513X211060049
28. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. doi:10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-g
29. Turale S. A brief introduction to qualitative description: a research design worth using. Pacific Rim Int J Nursing Res. 2020;24(3):289–291.
30. Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Global Qualitative Nursing Res. 2017;2017:4. doi:10.1177/2333393617742282
31. Chesser-Smyth PA. The lived experiences of general student nurses on their first clinical placement: a phenomenological study. Nurse Educ Pract. 2005;5(6):320–327. doi:10.1016/j.nepr.2005.04.001
32. Guba EG, Lincoln YS. Paradigmatic controversies, contradictions, and emerging confluences. In: Denzin NK, Lincoln YS, editors. The SAGE Handbook of Qualitative Research. Sage Publications; 2018:213–263.
33. Carter N, Bryant-Lukosius D, DiCenso A, et al. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545–547. doi:10.1188/14.ONF.545-547
34. Asselin ME. Insider research - issues to consider when doing qualitative research in your own setting. J Nurses Staff Dev. 2003;19(2):99–103. doi:10.1097/00124645200303000-00008
35. Fertility Preservation in Cancer (FPIC). About us. 2020. Available from https://www.fpic.org.uk/about-us/.
36. Chen X, Shi Y. Cultural values and fertility preservation: a Chinese perspective. J Assisted Reproduction Genetics. 2020;37(6):1145–1148. doi:10.1007/s10815-020-01685-1
37. Wang Y, Sun Y. The impact of traditional Chinese culture on fertility preservation decisions among cancer patients. J Psychosoc Oncol. 2017;35(4):413–425. doi:10.1080/07347332.2017.1322306
38. Zheng C, Li H. The role of traditional Chinese culture in fertility-related decision-making: a review. J Ethnic Cultural Diversity Soc Work. 2015;24(3):213–225. doi:10.1080/15313204.2015.1010495
39. Benedict C, Thom B, Diefenbach M, et al. The impact of cancer-related financial toxicity on reproductive concerns and family-building decision-making in post-treatment survivorship. J Adolesc Young Adult Oncol. 2023;12(3):408–415. doi:10.1089/jayao.2022.0088
40. Xiong W, Deng Y, Yang Y, et al. Assessment of medical service pricing in china’s healthcare system: challenges, constraints, and policy recommendations. Front Public Health. 2021;9:787865. doi:10.3389/fpubh.2021.787865
41. China National Knowledge Infrastructure. Expert consensus on fertility protection inChina. Chinese J Obstetrics Gynecol. 2020;55(3):161–165. doi:10.3969/j.issn.0529-567X.2020.03.002
42. Ferrari A, Stark D, Peccatori FA, et al. Adolescents and young adults with cancer: a position paper from the AYA working group of the European society for medical oncologyand the European society for paediatric oncology. ESMO Open. 2021;6(2):100096. doi:10.1016/j.esmoop.2021.100096
43. Anazodo A, Ataman-Millhouse L, Jayasinghe Y, et al. Oncofertility-An emerging discipline rather than a special consideration. Pediatr Blood Cancer. 2018;65(11):e27297. doi:10.1002/pbc.27297
44. Schork NJ. Artificial intelligence and personalized medicine. Cancer Treat Res. 2019;178:265–283. doi:10.1007/978-3-030-16391-4_11
45. Gama F, Tyskbo D, Nygren J, et al. Implementation frameworks for artificial intelligence translation into health care practice: scoping review. J Med Internet Res. 2022;24(1):e32215. doi:10.2196/32215
46. Carlson MJ, Thiel KW, Yang S, et al. Catch it before it kills: progesterone, obesity, and the prevention of endometrial cancer. Discovery Med. 2012;14(76):215–222.
47. Wang S, Liu H, Yang Y, et al. Investigating the shared genetic architecture between adiposity measures and obesity-related cancers. Briefings Bioinformatics. 2025;26(4):bbaf439. doi:10.1093/bib/bbaf439
48. Kokts-Porietis RL, Elmrayed S, Brenner DR, et al. Obesity and mortality among endometrial cancer survivors: a systematic review and meta-analysis. Obesity Rev. 2021;22(12):e13337. doi:10.1111/obr.13337
49. NCCN clinical practice guidelines in oncology (NCCN Guidelines®). uterine neoplasm. Version 1. 2018—October 13, 2017; NCCN: Plymouth Meeting, PA, USA; 2017.
50. Hampel H, Bennett RL, Buchanan A, et al. A practice guideline from the American college of medical genetics and genomics and the national society of genetic counselors: referral indications for cancer predisposition assessment. Genetics Med. 2015;17(1):70–87. doi:10.1038/gim.2014.147
51. Martinez F. Update on fertility preservation from the Barcelona International Society for Fertility Preservation-ESHRE-ASRM 2015 expert meeting: indications, results and future perspectives. Human Reproduction. 2017;32(9):1802–1811. doi:10.1093/humrep/dex218
52. Italian medical code of ethics. 2017. Available from: https://portale.fnomceo.it/wp-content/uploads/2018/03/CODICE-DEONTOLOGIA-MEDICA-2014.pdf.
53. Italian National Committee for Bioethics. Information and consent to medical procedures. 1992. Available from: http://www.dentistimadonnabianca.it/documents/03bis.InformazioneConsenso.CNB1992.pdf.
54. Zaami S, Stark M, Signore F, et al. Fertility preservation in female cancer sufferers: (only) a moral obligation? European J Contraception Reproductive Health Care. 2022;27(4):335–340. doi:10.1080/13625187.2022.2045936
55. Purandare N, Ruiloba F, Nguyen-Hoang L, et al. Cancer and fertility management: FIGO best practice advice. Int J Gynaecol Obstetrics. 2025. doi:10.1002/ijgo.70426
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.