Back to Journals » Journal of Asthma and Allergy » Volume 15
Daytime and Nighttime Visual Analog Scales May Be Useful in Assessing Asthma Control Levels Before and After Treatment
Authors Fujiki R, Kawayama T, Furukawa K, Kinoshita T, Matsunaga K, Hoshino T
Received 11 July 2022
Accepted for publication 17 October 2022
Published 26 October 2022 Volume 2022:15 Pages 1549—1559
DOI https://doi.org/10.2147/JAA.S381985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Rei Fujiki,1 Tomotaka Kawayama,2 Kyoji Furukawa,3 Takashi Kinoshita,2 Kazuko Matsunaga,2 Tomoaki Hoshino2
1Fujiki Medical and Surgical Clinic, Miyazaki, 880-2112, Japan; 2Division of Respirology, Neurology, and Rheumatology, Department of Medicine, Kurume University School of Medicine, Kurume, 830-0011, Japan; 3Biostatistics Center, Kurume University School of Medicine, Kurume, 830-0011, Japan
Correspondence: Tomotaka Kawayama, Division of Respirology, Neurology, and Rheumatology, Department of Medicine, Kurume University School of Medicine, 67 Asahi-machi, Kurume, 830-0011, Japan, Tel +81-924-31-7560, Fax +81-942-31-7703, Email [email protected]
Purpose: Few questionnaires evaluate daytime and nighttime symptoms separately, although these assessments could contribute to the improvement of disease control levels and prevention of future risks in asthma. The purpose of this retrospective study was to investigate whether daytime and nighttime visual analog scales (VAS) are useful in measuring the perception of symptoms, assessing disease control levels, and evaluating the treatment effects in asthma.
Patients and Methods: Self-reporting asthma control tests (ACT) before and after treatment are standardized tests used to determine disease control levels. A multiple regression analysis was performed to determine the correlation between daytime and nighttime VAS and the characteristics of patients before treatment, as well as the changes in VAS and lung functions and fractional exhaled nitrogen oxide after treatment in 55 treatment-naïve symptomatic adult patients with asthma.
Results: Both daytime (r = − 0.57, P < 0.0001) and nighttime (r = − 0.46, P < 0.0001) VAS correlated well with ACT scores, and there was a correlation between daytime and nighttime VAS (r = 0.33, P = 0.0148) before treatment. In addition, the changes in daytime (r = − 0.65, P < 0.0001) and nighttime (r = − 0.44, P < 0.0001) VAS were significantly associated with changes in the ACT scores. The multiple regression analysis (β [95% confidence interval]) revealed that improvements in the daytime (− 2.33 [− 4.55 to − 0.11], P = 0.0405) and nighttime (− 3.09 [− 6.25 to 0.07], P = 0.0505) VAS were associated with an increased forced vital capacity after treatment, although there was no correlation between the VAS and characteristics before treatment.
Conclusion: Our study demonstrated that daytime and nighttime VAS were useful in assessing disease control levels and evaluating the treatment effects in asthma.
Keywords: asthma, symptoms, visual analog scale, asthma control test, adult
Plain Language Summary
We demonstrated that the daytime and nighttime visual analog scale (VAS) were associated with the asthma control test (ACT) scores before and after treatment in treatment-naïve and symptomatic patients with asthma. The nighttime VAS was higher than the daytime VAS, and the nighttime VAS also improved faster than the daytime VAS and the ACT score after treatment. We believe that both daytime and nighttime VAS are useful in assessing asthma control levels and evaluating the treatment effects in symptomatic patients with asthma.
Introduction
Uncontrolled and/or severe asthma is a social problem worldwide,1–3 as well as in Japan.4 In 2021, a survey conducted in Middle East and North Africa, which used the Global Initiative for Asthma (GINA) criteria, reported that the percentage of patients with partly controlled and uncontrolled asthma was 29.1% and 41.5%, respectively.1 In 2009, a US survey demonstrated that although 71% of patients self-reported “completely controlled” or “well-controlled” statuses, the percentages of patients with asthma who needed urgent care visits twice and emergency department visits once per year were 67% and 60%, respectively.2 A 2016 global cross-sectional study demonstrated that among 8111 patients, 18.0% and 38.5% of patients had partly controlled and uncontrolled asthma, respectively.3 Japanese internet surveys reported that considering the GINA criteria, 49.8% and 15.1% of patients had partly controlled and uncontrolled asthma, respectively. Daytime and nighttime asthma symptoms were experienced by 51.5% and 44.9% of patients, respectively.4 A global study found that undertreatments are still observed for the management of asthma worldwide.5
The goal of asthma management is to achieve a well-controlled asthma level.6 Understanding the perception of asthma symptoms is necessary for the assessment of asthma control levels. An asthma control test (ACT) has been evaluated for understanding asthma control levels and is used worldwide.7,8 In critical practice, the ACT has 5 items and the total ACT score, but not each item, is expressed as the disease control level.7,8 Similarly, the visual analog scale (VAS) has been evaluated as a useful tool for assessing the perception of respiratory symptoms.9–13
Nocturnal symptoms are accompanied by circadian variations in small airway inflammation, hyperresponsiveness, and dysfunction in asthma.14–16 Nocturnal asthma is associated with emergency visits, increased morbidity, and worsening disease control levels. Moreover, it has an important negative impact on the quality of life of patients with asthma.17,18 Early detection of nocturnal symptoms is important because these symptoms are treatable.19
Therefore, not only the daytime but also the nighttime perception of asthma symptoms should be assessed in each patient. Among the items of the ACT, the questionnaire for daytime and nighttime symptoms includes only one item in each, namely item 1 and item 3, respectively. To assess both daytime and nighttime perception of asthma symptoms, we have modified and used the two types of VAS, daytime and nighttime VAS, in a primary care setting. We conducted a retrospective study for the evaluation of modified daytime and nighttime VAS. Therefore, this study investigated whether the daytime and nighttime VAS were useful in the measurement of perception of asthma symptoms, the assessment of asthma control levels, and the evaluation of treatment effects in symptomatic adult patients with asthma.
Materials and Methods
Study Protocol
A retrospective study was conducted in a single institute and primary care setting to critically evaluate daytime and nighttime VAS for the perceptions of asthma symptoms. Data on self-reported daytime and nighttime VAS, ACT scores, prescriptions, physique (body mass index, BMI), smoking habits, comorbidities, blood eosinophil counts and serum total IgE levels, lung functions by spirometry, and fractional exhaled nitrogen oxide (FENO) were retrospectively collected from the medical records of the patients with asthma who visited Fujiki Medical and Surgical Clinic. Data on daytime and nighttime VAS and ACT scores were collected as patient-reported outcomes (PROs) before treatment as a baseline and 4 weeks and 8 weeks after treatment. Data on FENO and lung functions before treatment as the baseline and 8 weeks after treatment were collected, because the clinic usually required data on each PRO every 4 weeks and spirometry and measurement of FENO every 8 weeks when new or alternative treatment was initiated (Figure 1). However, measurement of airway reversibility was not available using inhaled short-acting bronchodilators in the clinic.
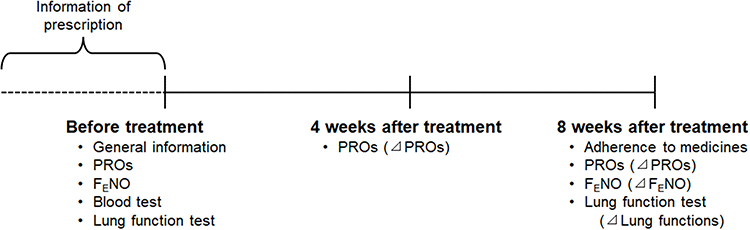 |
Figure 1 Study protocol. Abbreviations: FENO, fractional exhaled nitrogen oxide; PROs, patient-reported outcomes. Notes: The delta was expressed as different values from before treatment to 4 weeks or from before treatment 8 weeks after treatment. |
Patients
Among 302 adult patients with asthma who visited the clinic between December 1, 2020, and May 31, 2021, 188 adults (age ≥20 years old) underwent daytime and nighttime VAS assessments before treatment and 4 weeks and 8 weeks after treatment with inhaled corticosteroids (ICS)/long-acting β2 agonists (LABA) combination therapy. Asthma was defined by a physician’s diagnosis based on the GINA report.6 The non-smoking, prescriptive controller-naïve (no prescriptions for controllers for asthma treatment) and symptomatic (ACT scores <20 points)7,8 patients were selected for this study. The patients who smoked (n = 31) were prescribed with other controllers (n = 45) and had ≥20 points in the ACT scores (n = 54) before treatment were excluded. Three patients who had no data on lung functions before and 8 weeks after treatment were also excluded. Fifty-five patients were finally analyzed (Figure 2).
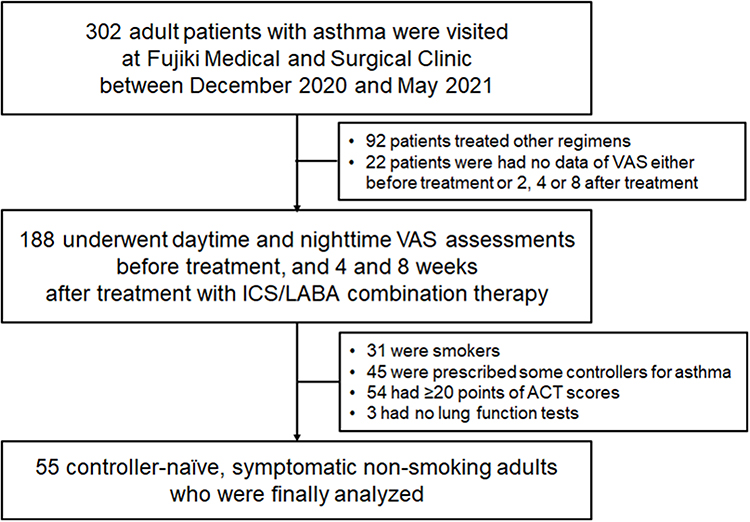 |
Figure 2 Flowchart of patient enrollment. Abbreviations: ACT, asthma control test; ICS, inhaled corticosteroids; LABA, long-actingβ2 agonists; VAS, visual analog scale. Notes: The controller-naïve, symptomatic, non-smoking, adult patients who underwent daytime and nighttime VAS assessments before treatment, and 4 and 8 weeks after treatment with ICS/LABA combination therapy, were enrolled at Fujiki Medical and Surgical Clinic between December 2020 and May 2021. |
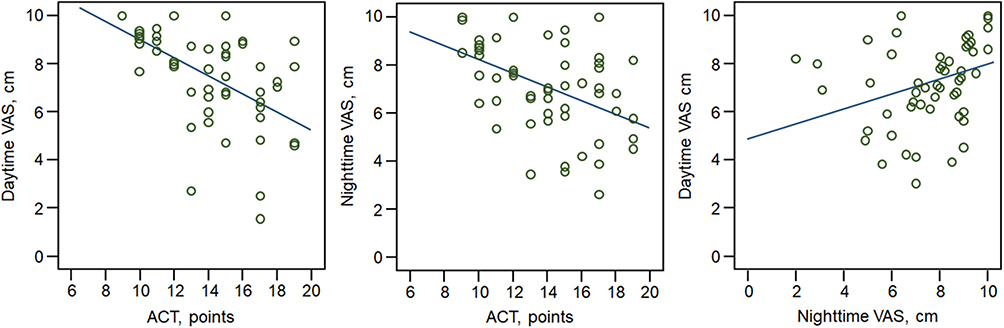 |
Figure 3 The correlation between ACT scores, and daytime and nighttime VAS before treatment. Abbreviations: ACT, asthma control test; VAS, visual analog scale. |
Data Collection
The PROs
The self-reporting ACT7,8 and VAS9–13 assessments were required before the measurement of FENO and lung functions. The modified ACT and VAS assessed the average perception of asthma symptoms in the last one week of the evaluation period. Two types of modified VAS, namely daytime (from 6 am to 6 pm) and nighttime (from 6 pm to 6 am), were used based on the Japanese version of the VAS utilized in a previous study.10 In VAS, the scales ranged from not at all bothersome (0 cm as a good condition) to extremely bothersome (10 cm as a bad condition). After reporting daytime and nighttime VAS, each patient continuously underwent the Japanese version of the ACT for adult asthmatics.20
Measurement of FENO
Morning FENO was measured twice a day at every visit before spirometry by an online electrochemical NO analyzer (NIOX VERO®, Circassia AB, Sweden), and the mean value obtained was used for the analysis.21
Lung Function Tests
Spirometry (Chestgraph Jr HI-101, CHEST, Tokyo, Japan) was repeated twice. We adopted the best values of forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC), in accordance with a Taskforce recommendation.22 The percent predicted values of FEV1 (%FEV1 predicted) and FVC (%FVC predicted) were calculated using a formula for Japanese individuals.23
Ethical Approval
The study was conducted following the Good Clinical Practice guidelines and was approved by the local ethics board of Kurume University, Japan (No. 21–155, September 30, 2021). The study protocol was registered in the University Hospital Medical Information Network (UMIN) Center (UMIN No. 000045636) on October 2, 2021. Patients who visited Fujiki Medical and Surgical Clinic (Miyazaki, Japan) were allowed an opt-out option between September 30, 2021 and March 31, 2022.
Statistical Analysis
All variables were summarized by the number (% of total) of patients by category for qualitative variables and mean ± standard deviation (SD) for quantitative variables. Changes in PROs, lung functions, and FENO before and after treatment were expressed as delta (⊿) (Figure 1). Means were compared from before to after treatment by the Student’s t-test and one-way analysis of variance test. A multiple regression analysis was used to estimate an adjusted coefficient (standardized β [95% confidential interval (CI)]) affected by PROs with adjustment for potential confounders; age,24 gender differences,25,26 BMI,26,27 blood eosinophils and neutrophils,27,28 serum total IgE levels,27,28 FVC and FEV1,27 FENO,27,28 and the presence of other allergic comorbidities.9–13,24,26,27 Supplementary Table 1A and 1B were selected as adjustment variables based on a previous study,29 whereas an unadjusted coefficient of correlation (r) between the characteristics (variances) was analyzed by Spearman tests. The changes in absolute values (L) of lung functions were used after treatment, although both absolute and predicted values (%) were used for analyses as such absolute values are affected by age, gender, and physique. In addition, the blood percentage eosinophils and neutrophils were used because the absolute numbers of these cells are affected by the white blood cell count (Supplementary Table 2). To define the minimum clinically important difference (MCID) for daytime and nighttime VAS, the receiver operating characteristic (ROC) curve analysis was used with the reference MCID > 3 points, which showed improvement of ACT scores from before to after treatment. Statistical significance was set at P < 0.05. JMP version 15 for Windows (SAS Institute, Cary, NC, USA) was used for data analyses.
Results
Profiles of Patients
Table 1 summarizes that in the patients’ demographic data. The mean (SD) age was 49.7 (16.1) years, the number (%) of women was 42 (76.4%), the mean (SD) BMI was 22.9 (3.6) kg/m,2 and the number (%) of patients who were obese was 12 (21.8). In terms of biomarkers, the mean % and absolute number (SD) of blood eosinophils were 3.8% (2.3%) and 239 (157) cells/µL, respectively, and the mean (SD) serum IgE concentration and FENO were 140 (230) U/mL and 49.2 (49.1) ppb, respectively. In terms of PROs, the mean (SD) ACT and daytime and nighttime VAS were 13.9 (3.9) points, 7.3 (1.9) cm, and 7.7 (1.9) cm, respectively. In terms of spirometry measurements, the mean (SD) %FVC and %FEV1 predicted were 96.6% (18.6%) and 91.3% (22.1%), respectively, and the numbers (%) of patients with obstructive and restrictive patterns were 10 (18.2%) and 3 (5.4%), respectively. In terms of the regimens of ICS/LABA therapy, the numbers (%) of patients receiving high-dose ICS and those receiving ICS once a day were 22 (40.0%) and 26 (47.3%), respectively. All patients received new treatment with ICS/LABA combinations for asthma control, although the prescription of leukotriene receptor antagonists and anti-allergic agents was used before new treatment for asthma and the doses were not changed 8 weeks after treatment for asthma for other allergic comorbidities such as allergic rhinitis and dermatitis (Supplementary Table 1A and 1B). The number (%) of patients with high and medium doses of ICS was 22 (40.0) and 33 (60.0), respectively. The doses were continued for at least 8 weeks.
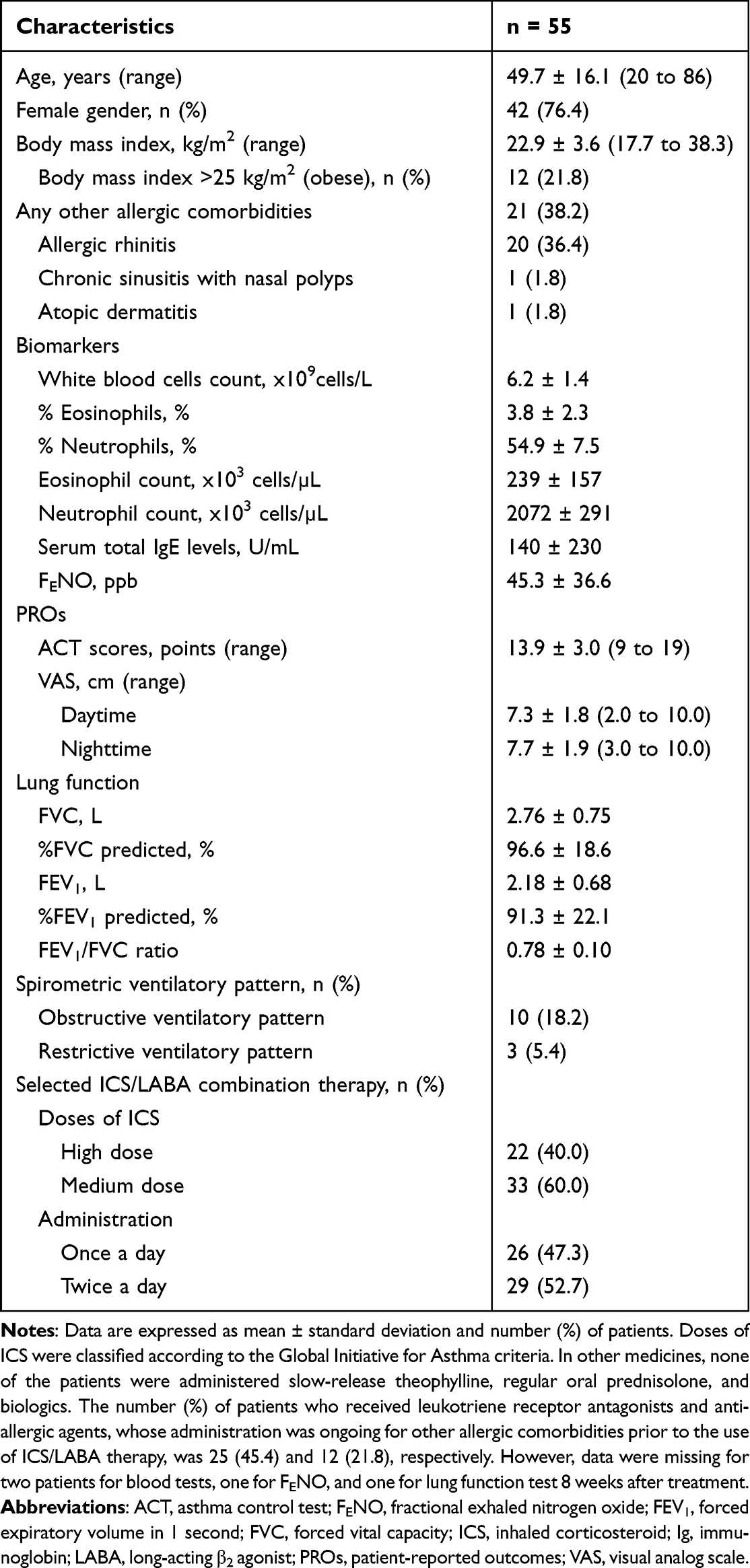 |
Table 1 Profiles of Patients with Asthma Before Treatment |
Correlation Between ACT Scores and Daytime and Nighttime VAS Before Treatment
Figure 3 shows that the ACT scores were significantly associated with daytime (r = −0.57, P < 0.0001) and nighttime VAS (r = −0.46, P < 0.0001), respectively. There was a weak but significant correlation between daytime and nighttime VAS (r = 0.33, P = 0.0148). In the unadjusted analyses, the ACT scores were positively associated with white blood cell count (r = 0.44, P = 0.0024), whereas the daytime VAS was negatively associated with white blood cell count (r = −0.32, P = 0.0222) and FENO (r = −041, P = 0.0019), and the nighttime VAS was negatively associated with white blood cell count (r = −0.50, P = 0.0006) and serum total IgE levels (r = −0.33, P = 0.0152) before treatment (Supplementary Table 3A). However, upon multiple regression analysis, neither the ACT scores nor the daytime and nighttime VAS were significantly associated with the PROs and characteristics before treatment (Supplementary Table 3B). In patients with but not those without other allergic comorbidities (Supplementary Table 3C), the daytime VAS was negatively associated with the percentage neutrophils in the multiple regression analysis (β = −0.35, P = 0.0035) (Supplementary Table 3D).
Effects of ICS/LABA Combination Therapy on PROs, Lung Functions, and FENO
Figure 4 shows that all PROs were improved by treatment with ICS/LABA combinations. In lung functions, the %FEV1, but not FVC, predicted, and the FEV1/FVC ratio was significantly improved, and the FENO levels were significantly decreased 8 weeks after treatment (Supplementary Table 4).
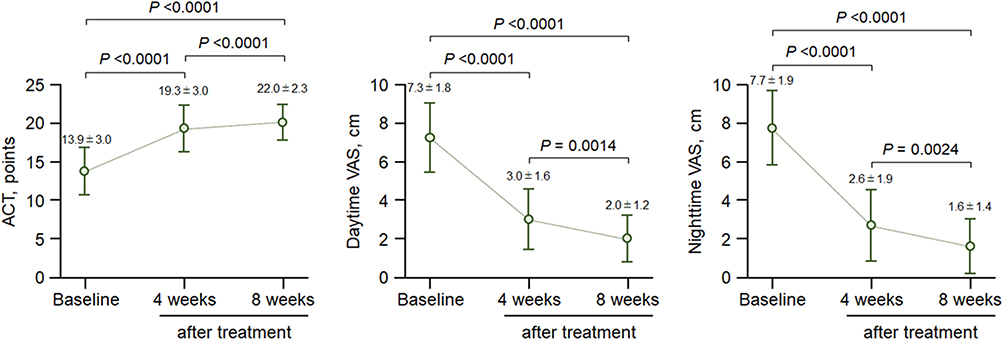 |
Figure 4 Changes in the mean ACT scores, and daytime and nighttime VAS after treatment. Abbreviations: ACT, asthma control test; PROs, patient-reported outcomes; VAS, visual analog scale. Notes: All data were expressed as mean (open circles) ± SD (bars). Data of baseline were the values of PROs before treatment. |
Correlation Between Changes in PROs, Lung Functions, and FENO from Before Treatment to 8 Weeks After Treatment
Figure 5 shows that the changes in the ACT scores were significantly associated with changes in daytime (r = −0.65, P < 0.0001) and nighttime VAS (r = −0.44, P < 0.0001), respectively; however, there was a significant correlation between changes in daytime and nighttime VAS (r = 0.38, P = 0.0038) 8 weeks after treatment. Upon multiple regression analysis, changes in the daytime VAS were significantly associated with changes in FVC (Table 2), whereas the unadjusted analysis revealed that PROs, the white blood cell count, cell differentiation, total serum IgE levels, and FENO before treatment affected changes in PROs (Supplementary Table 5). However, the mean ± SD nighttime VAS (5.0 ± 2.3) improved faster than did the ACT scores (2.2 ± 1.2, P < 0.0001), when assuming that the maximum total score of 25 points was converted to 10 points. The daytime VAS increased from before treatment to 4 weeks after treatment (4.3 ± 2.0, P = 0.0211), although the change in the nighttime VAS (1.1 ± 1.2) was no different from those in the daytime VAS (1.1 ± 1.1, P > 0.05) and ACT score (1.1 ± 0.9, P > 0.05) from 4 to 8 weeks after treatment. In the different administrations of ICS/LABA therapy, there was no difference between administrations of once a day and twice a day in changes in the ACT scores and daytime and nighttime VAS 4 and 8 weeks after treatment (data not shown).
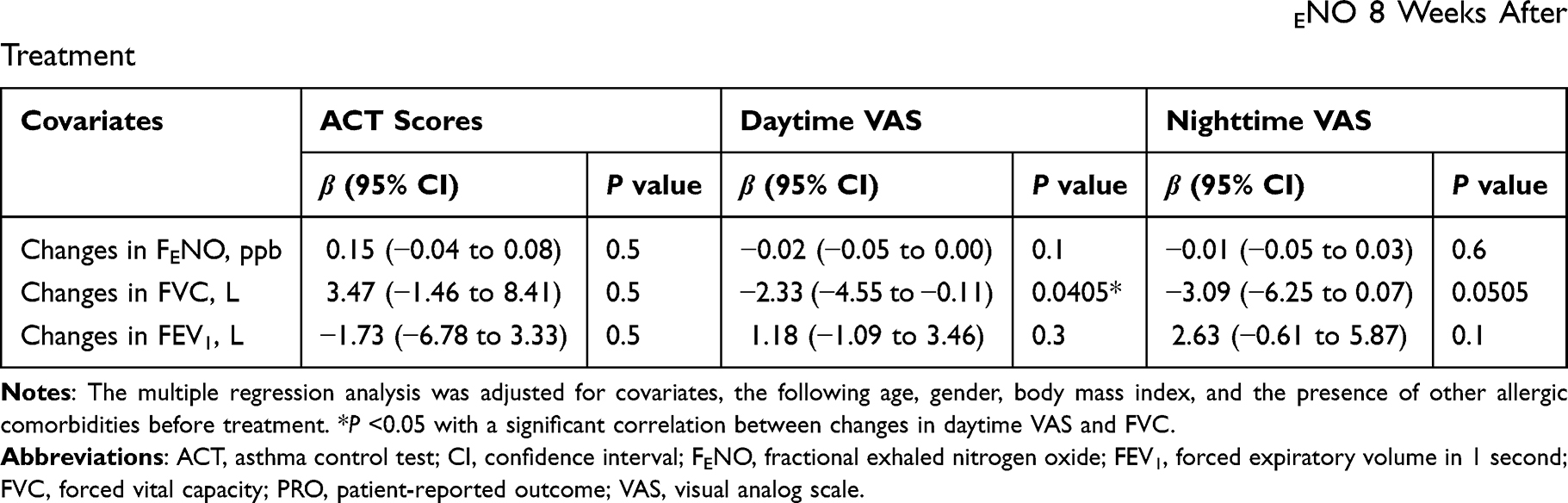 |
Table 2 Multiple Regression Analysis of Changes in PROs and Changes in Lung Functions and FENO 8 Weeks After Treatment |
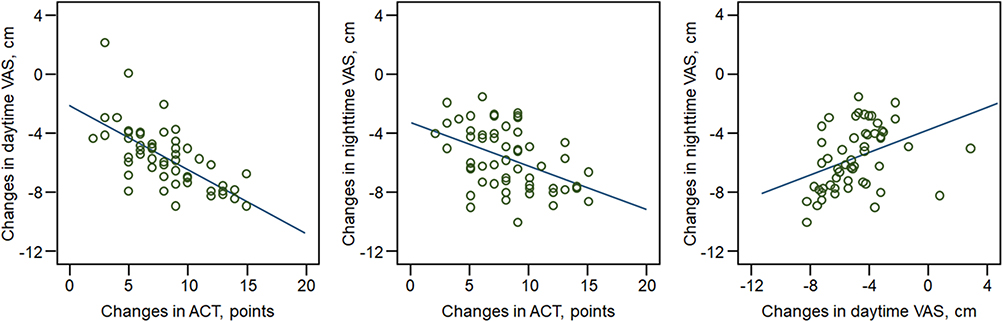 |
Figure 5 The correlation between changes in the ACT scores, and daytime and nighttime VAS from before to 8 weeks after treatment. Abbreviations: ACT, asthma control test; VAS, visual analog scale. |
MCID of Daytime and Nighttime VAS Related to ACT Scores by ROC Curve Analysis
The number (%) of patients with improvements of >3 points (MCID) of ACT scores 4 weeks and 8 weeks after treatment was 47 (85.5%) and 54 (98.2%), respectively. The ROC curves analysis with the MCID of the ACT scores as a reference showed that the area under the curve (sensitivity and 1-specificity) and the estimated MCID were 0.86 (0.85 and 0.13, P = 0.0054) and −3.2 cm for daytime VAS and 0.69 (0.58 and 0.25, P = 0.1179) and −3.3 cm for nighttime VAS 4 weeks after treatment; similarly, the values were 0.77 (0.76 and 0.00, P = 0.5350) and −4.6 cm for daytime VAS and 0.75 (0.74 and 0.00, P = 0.4468) and −4.1 cm for nighttime VAS 8 after treatment (Supplementary Figure 1). However, the number (%) of patients who achieved total asthma control with 25 points in the ACT scores 4 weeks and 8 weeks after treatment was 0 (0) and 3 (5.5), respectively. In addition, no patients who achieved total asthma control with 0 cm in the daytime and nighttime VAS 4 weeks and 8 weeks after treatment showed.
Discussion
Our retrospective study demonstrated that the ICS/LABA combination therapy significantly improved ACT scores as well as daytime and nighttime VAS in treatment-naïve symptomatic adult patients with asthma. The therapy was also significantly positively associated with the %FEV1 predicted and negatively associated with the FENO levels 8 weeks after treatment. Before treatment, both daytime and nighttime VAS were significantly associated with ACT scores. There was a correlation between daytime and nighttime VAS, although nighttime VAS was slightly higher than daytime VAS. After treatment, changes in both the daytime and nighttime VAS were significantly associated with changes in the ACT scores. However, there was a significant correlation between changes in the daytime and nighttime VAS. The MCID of +3 points in the ACT scores was equivalent to a difference of −3.2 cm in the daytime and −3.2 cm in nighttime VAS 4 weeks after treatment, and −4.6 cm in the daytime and −4.1 cm in nighttime VAS 8 weeks after treatment. However, multiple regression revealed that improvements in the daytime and nighttime VAS may be associated with an improvement in FVC after but not before treatment, although we investigated the correlation between the PROs and characteristics (including lung function and biomarker levels) before and after treatment. We also found that the PROs before treatment affect changes in the PROs after treatment (Supplementary Table 5). Poorer PROs may result in a greater improvement in PROs after optimal treatment in patients with asthma.
The GINA report recommends the use of the ACT for assessing asthma symptoms as one of the standard questionnaires in adult patients with asthma.6 The ACT has 5 simple items and can be easily understood by the patients.7,8,10 Subsequently, we adopted the ACT as a standardized questionnaire for the perception of asthma symptoms in this study. The evidence on the correlation between VAS and ACT is still limited for adult patients with asthma,10,30–33 although VAS has been evaluated as a useful tool for assessing the perception of respiratory symptoms.9–13 A large-scale previous Japanese study of adult asthma patients with rhinitis reported that the VAS was well-correlated with asthma control levels using the GINA criteria.10 The VAS was also well-expressed not only in disease control but also in severity levels.11 However, the VAS was standardized as an average perception of symptoms during a full day and the previous 4 weeks of an evaluation period. Hence, the applicability of VAS may remain a problem for assessments of asthma daytime and nighttime conditions. To our knowledge, our study using the modified VAS, which assessed symptoms of averaged daytime and nighttime asthma, and during the previous one week of the evaluation period, was the first to perform such assessments in adult patients with asthma. In our primary care setting, most patients required a shorter-term evaluation period after treatment than the standardized evaluation period in previous studies.7,8,10 Our study successfully demonstrated that the daytime and nighttime VAS before treatment and changes in the VAS after treatment were significantly associated with the ACT scores before treatment and changes in the ACT scores after treatment in adult patients with asthma, respectively. We found that the nighttime VAS improved faster than the ACT score and the daytime VAS with optimal treatment. It may be possible to predict the treatment effect earlier using the nighttime VAS in treatment-naïve and symptomatic patients with asthma, although our study detected the efficacy of ICS/LABA therapy 4 weeks after treatment.
Our multiple regression analyses did not reveal any promising correlations between the PROs and lung function and biomarker levels before and after treatment. Some previous studies reported that the ACT scores negatively correlated with type-2 inflammation in patients with asthma,34–38 whereas other previous studies demonstrated that the ACT scores were not related to any inflammatory biomarkers, such as airway and systemic eosinophilic inflammation and FENO.39–41 Hence, the interaction between ACT scores and type-2 inflammation is still controversial in asthma. The unadjusted analyses revealed that all PROs were negatively associated with white blood cell counts in our study (Supplementary Table 3). Previous studies demonstrated that the white blood cell count may contribute to cigarette smoking and other atopic comorbidities or allergic sensitization, although the correlation between white blood cell count and asthma control levels is controversial.42–44 The presence of not only asthma but also of other allergic comorbidities may affect the white blood cell count and the differentiation of eosinophils and neutrophils (Supplementary Tables 1 and 2). Furthermore, the presence of other allergic comorbidities may also have affected the FENO in our study (Supplementary Tables 1 and 2). Our multiple regression analyses, in which we adjusted for the presence of other allergic comorbidities, did not reveal any correlation between the PROs and type-2 inflammation markers, such as eosinophils, IgE, and FENO before and after treatment. In addition, some previous studies also reported weak-to-moderate correlations between ACT scores and either FEV1 or %FEV1 predicted,37,38,45–48 although some studies demonstrated that there was no correlation between ACT scores and lung function in patients with asthma.39,49 The correlation between ACT scores and lung function thus lacks corroboration in studies on asthma. Our multiple regression analyses revealed no association of daytime and nighttime VAS with lung function before treatment. However, the increase in the FVC may contribute to the improvement of daytime and nighttime VAS after treatment (Table 2). The reason why the FEV1 was not related to the treatment effects as represented by PROs may be that 18.2% of patients have obstructive ventilation patterns50 or poorly controlled asthma with air-trapping in the lungs.51
Our study has several limitations. First, our study was retrospective and conducted in a single primary care setting. Second, the sample size could have been small for the evaluation of PROs when compared with previous studies (mean sample size was 207 [range 68–471]).7,8,20,34–40,48,49 Third, we modified the methods of assessing PROs for a short evaluation period during treatment. The average perception of asthma symptoms in the last one week before treatment may have affected our results. Fourth, our study did not assess airway eosinophilic inflammation, such as sputum eosinophilia, although a previous study demonstrated that nocturnal symptoms were associated with sputum eosinophilia.36 Fifth, patient adherence to medicines was not assessed. However, good adherence to medicines was assumed, because all patients were reconfirmed to receive medicines every 4 weeks based on the refile methods in the study.52 Sixth, our selection of treatment regimens may have had issues. We selected the first-line ICS/LABA combination therapy as a companion medicine for evaluating the changes in PROs. The high-credible MCID for VAS could not be obtained, because the chosen combination therapy might have led to over-treatment, which made most of the patients reach MCID in the ACT scores immediately. However, most patients did not achieve complete asthma control in 8 weeks after treatment, although early improvement may have been achieved by the chosen combination therapy in the primary setting. Nevertheless, the discrepancy between changes in the daytime and nighttime VAS after treatment is still unclear. The mechanism of the discrepancy could be clearer if we selected different regimens such as high-dose ICS alone for anti-type-2 inflammations or low-dose ICS/LABA plus LAMA for maximal bronchodilations. A multi-institution, long-term period, and prospective study will be therefore needed in the future.
Conclusion
In conclusion, our study demonstrated that nighttime VAS was higher than daytime VAS, whereas there was a significant positive correlation between daytime and nighttime VAS before and after treatment in symptomatic patients with asthma, as preliminary findings. The nighttime VAS may be able to detect an improvement of condition faster than the ACT scores and the daytime VAS following optimal treatment. We believe that daytime and nighttime VAS assessments for perceived asthma symptoms, together with the ACT, are useful for the assessment of asthma control levels before and after treatment in symptomatic patients with asthma.
Abbreviations
ACT, asthma control test; ANOVA, analysis of variance; AUC, area under the curve; BMI, body mass index; CI, confidence interval; FENO, fractional exhaled nitrogen oxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroids; LABA, long-acting β2 agonists; MCID, minimum clinically important difference, PROs, patient-reported outcomes; ROC, receiver operating characteristic; SD, standard deviation; UMIN, University Hospital Medical Information Network; US, United States; VAS, visual analog scale.
Acknowledgments
The authors thank for helping all data collections and managements to all members of the Fujiki Medical and Surgical Clinic, Miyazaki, Japan.
Funding
There was no funding for this work.
Disclosure
Prof. Tomotaka Kawayama reports grants from Helios Co. Ltd. and lecture fees from GlaxoSmithKline (GSK), AstraZeneca, Boehringer Ingelheim, Sanofi, Novartis, Kyorin, and Teijin Healthcare. Dr Takashi Kinoshita reports grants from GSK and AstraZeneca and a lecture fee from AstraZeneca. Prof. Tomoaki Hoshino reports a grant from GSK, Novartis, and Chugai Pharmaceutical. The rest of the authors have no potential conflicts of interest in this study.
References
1. Bassam M, Behbehani N, Farouk H, et al. Adherence to medication among adult asthma patients in the Middle East and North Africa: results from the ESMAA study. Respir Med. 2021;176:106244. doi:10.1016/j.rmed.2020.106244
2. Murphy KR, Meltzer EO, Blaiss MS, Nathan RA, Stoloff SW, Doherty DE. Asthma management and control in the United States: results of the 2009 Asthma Insight and Management survey. Allergy Asthma Proc. 2012;33(1):54–64. doi:10.2500/aap.2011.32.3518
3. Braido F, Brusselle G, Guastalla D, et al. Determinants and impact of suboptimal asthma control in Europe: the international cross-sectional and longitudinal assessment on asthma control (LIAISON) study. Respir Res. 2016;17(1):51. doi:10.1186/s12931-016-0374-z
4. Adachi M, Hozawa S, Nishikawa M, Yoshida A, Jinnai T, Tamura G. Asthma control and quality of life in a real-life setting: a cross-sectional study of adult asthma patients in Japan (ACQUIRE-2). J Asthma. 2019;56(9):1016–1025. doi:10.1080/02770903.2018.1514628
5. Reddel HK, Vestbo J, Agustí A, et al. Heterogeneity within and between physician-diagnosed asthma and/or COPD: NOVELTY cohort. Eur Respir J. 2021;58(3):2003927. doi:10.1183/13993003.03927-2020
6. Global Initiative for Asthma. The global strategy for asthma management and prevention; 2021. Available from: https://ginasthma.org/.
7. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
8. Schatz M, Sorkness CA, Li JT, et al. Asthma control test: reliability, validity, and responsiveness in patients not previously followed by asthma specialists. J Allergy Clin Immunol. 2006;117:549–556. doi:10.1016/j.jaci.2006.01.011
9. Ciprandi G, Schiavetti I, Sorbello V, Ricciardolo FLM. Perception of asthma symptoms as assessed on the visual analog scale in subjects with asthma: a real-life study. Respir Care. 2016;61(1):23–29. doi:10.4187/respcare.04171
10. Ohta K, Bousquet PJ, Akiyama K, et al. Visual analog scale as a predictor of GINA-defined asthma control. The SACRA study in Japan. J Asthma. 2013;50(5):514–521. doi:10.3109/02770903.2013.786726
11. Flood EM, De Cock E, Mork AC, Revicki DA. Evaluating preference weights for the Asthma Symptom Utility Index (ASUI) across countries. Health Qual Life Outcomes. 2006;4:51. doi:10.1186/1477-7525-4-51
12. Laforest L, El Hasnaoui A, Pribil C, Ritleng C, Schwalm MS, Van Ganse E. Asthma patients’ perception of their ability to influence disease control and management. Ann Allergy Asthma Immunol. 2009;102:378–384. doi:10.1016/S1081-1206(10)60508-X
13. Laforest L, El Hasnaoui A, Pribil C, et al. Asthma patients’ self-reported behaviours toward inhaled corticosteroids. Respir Med. 2009;103:1366–1375. doi:10.1016/j.rmed.2009.03.010
14. Abdo M, Trinkmann F, Kirsten AM, et al. The relevance of small airway dysfunction in asthma with nocturnal symptoms. J Asthma Allergy. 2021;14:897–905. doi:10.2147/JAA.S313572
15. van der Wiel E, Postma DS, van der Molen T, Schiphof-Godart L, ten Hacken NHT, van den Berge M.Effects of small airway dysfunction on the clinical expression of asthma: a focus on asthma symptoms and bronchial hyper-responsiveness. Allergy. 2014;69(12):1681–1688. doi:10.1111/all.12510
16. van der Wiel E, ten Hacken NH, Postma DS, van den Berge M. Small-airways dysfunction associates with respiratory symptoms and clinical features of asthma: a systematic review. J Allergy Clin Immunol. 2013;131(3):646–657. doi:10.1016/j.jaci.2012.12.1567
17. Calhoun WJ. Nocturnal asthma. Chest. 2003;123(3Suppl):399S–405S. doi:10.1378/chest.123.3_suppl.399s
18. Dales RE, Schweitzer I, Kerr P, Gougeon L, Rivington R, Draper J. Risk factors for recurrent emergency department visits for asthma. Thorax. 1995;50(5):520–524. doi:10.1136/thx.50.5.520
19. Fukuhara A, Saito J, Birring SS. Clinical characteristics of cough frequency patterns in patients with and without asthma. J Allergy Clin Immunol Pract. 2020;8(2):654–661. doi:10.1016/j.jaip.2019.08.053
20. Hasegawa T, Koya T, Sakagami T, et al. The Asthma Control Test, Japanese version (ACT-J) as a predictor of Global Initiative for Asthma (GINA) guideline-defined asthma control: analysis of a questionnaire-based survey. Allergol Int. 2013;62(3):323–330. doi:10.2332/allergolint.13-OA-0535
21. American Thoracic Society and. European Respiratory Society committee. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005;171:912–930. doi:10.1164/rccm.200406-710ST
22. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–338. doi:10.1183/09031936.05.00034805
23. Kubota M, Kobayashi H, Quanjer PH, Omori H, Tatsumi K, Kanazawa M. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig. 2014;52:242–250. doi:10.1016/j.resinv.2014.03.003
24. Skloot GS, Busse PJ, Braman SS, et al. An official American Thoracic Society workshop report: evaluation and management of asthma in the elderly. Ann Am Thorac Soc. 2016;13(11):2064–2077. doi:10.1513/AnnalsATS.201608-658ST
25. Yung JA, Fuseini H, Newcomb DC. Hormones, sex, and asthma. Ann Allergy Asthma Immunol. 2018;120(5):488–494. doi:10.1016/j.anai.2018.01.016
26. Wong M, Forno E, Celedón JC. Asthma interactions between obesity and other risk factors. Ann Allergy Asthma Immunol. 2022;129(3):301–306. doi:10.1016/j.anai.2022.04.029
27. Wenzel SE. Severe adult asthmas: integrating clinical features, biology, and therapeutics to improve outcomes. Am J Respir Crit Care Med. 2021;203(7):809–821. doi:10.1164/rccm.202009-3631CI
28. Lee Y, Quoc QL, Park HS. Biomarkers for severe asthma: lessons from longitudinal cohort studies. Allergy Asthma Immunol Res. 2021;13(3):375–389. doi:10.4168/aair.2021.13.3.375
29. Sullivan PW, Ghushchyan VH, Marvel J, Barrett YC, Fuhlbrigge AL. Association between pulmonary function and asthma symptoms. J Allergy Clin Immunol Pract. 2019;7(7):2319–2325. doi:10.1016/j.jaip.2019.04.019
30. Hojo M, Ohta K, Iikura M, Mizutani T, Hirashima J, Sugiyama H. Clinical usefulness of a guideline-based screening tool for the diagnosis of allergic rhinitis in asthmatics: the self assessment of allergic rhinitis and asthma questionnaire. Respirology. 2013;18(6):1016–1021. doi:10.1111/resp.12116
31. Lammers N, van Hoesel MHT, van der Kamp M, et al. The Visual Analog Scale detects exercise-induced bronchoconstriction in children with asthma. J Asthma. 2020;57(12):1347–1353. doi:10.1080/02770903.2019.1652640
32. Tosca MA, Barba PD, Licari A, Ciprandi G; Asthma And Rhinitis Control Study Group. The measurement of asthma and allergic rhinitis control in children and adolescents. Children. 2020;7(5):43. doi:10.3390/children7050043
33. Rhee H, Belyea M, Mammen J. Visual analogue scale (VAS) as a monitoring tool for daily changes in asthma symptoms in adolescents: a prospective study. Allergy Asthma Clin Immunol. 2017;13:24. doi:10.1186/s13223-017-0196-7
34. Gemicioglu B, Musellim B, Dogan I, Guven K. Fractional exhaled nitric oxide (FeNo) in different asthma phenotypes. Allergy Rhinol. 2014;5(3):157–161. doi:10.2500/ar.2014.5.0099
35. Zhang J, Wang X, Chen Y, Yao W. Correlation between levels of exhaled hydrogen sulfide and airway inflammatory phenotype in patients with chronic persistent asthma. Respirology. 2014;19(8):1165–1169. doi:10.1111/resp.12372
36. Scichilone N, Braido F, Taormina S, et al. Is health-related quality of life associated with upper and lower airway inflammation in asthmatics? Biomed Res Int. 2013;2013:539290. doi:10.1155/2013/539290
37. Papakosta D, Latsios D, Manika K, Porpodis K, Kontakioti E, Gioulekas D. Asthma control test is correlated to FEV1 and nitric oxide in Greek asthmatic patients: influence of treatment. J Asthma. 2011;48:901–906. doi:10.3109/02770903.2011.611958
38. Shirai T, Furuhashi K, Suda T, Chida K. Relationship of the asthma control test with pulmonary function and exhaled nitric oxide. Ann Allergy Asthma Immunol. 2008;101:608–613. doi:10.1016/S1081-1206(10)60223-2
39. Melosini L, Dente FL, Bacci E, et al. Asthma control test (ACT): comparison with clinical, functional, and biological markers of asthma control. J Asthma. 2012;49(3):317–323. doi:10.3109/02770903.2012.661008
40. Shiota N, Yokoyama A, Haruta Y, Hattori N, Kohno N. Association of airway inflammation with asthma control level evaluated by the asthma control test. J Asthma. 2011;48(9):907–913. doi:10.3109/02770903.2011.615430
41. Gill R, Williams EM. Agreement between self-reported asthma symptoms and exhaled nitric oxide levels: impact on inhaled corticosteroid prescribing in general practice. An observational study. Allergy Asthma Clin Immunol. 2019;15:70. doi:10.1186/s13223-019-0390-x
42. Girdhar A, Kumar V, Singh A, Menon B, Vijayan VK. Systemic inflammation and its response to treatment in patients with asthma. Respir Care. 2011;56(6):800–805. doi:10.4187/respcare.00601
43. Nadif R, Siroux V, Oryszczyn M-P, et al. Heterogeneity of asthma according to blood inflammatory patterns. Thorax. 2009;64(5):374–380. doi:10.1136/thx.2008.103069
44. Oryszczyn M-P, Bouzigon E, Maccario J, et al. Interrelationships of quantitative asthma-related phenotypes in the epidemiological study on the genetics and environment of asthma, bronchial hyperresponsiveness, and atopy. J Allergy Clin Immunol. 2007;119(1):57–63. doi:10.1016/j.jaci.2006.09.026
45. Cottee AM, Seccombe LM, Thamrin C, et al. Longitudinal monitoring of asthma in the clinic using respiratory oscillometry. Respirology. 2021;26(6):566–573. doi:10.1111/resp.14053
46. Abdo M, Watz H, Veith V, et al. Small airway dysfunction as predictor and marker for clinical response to biological therapy in severe eosinophilic asthma: a longitudinal observational study. Respir Res. 2020;21(1):278. doi:10.1186/s12931-020-01543-5
47. Huang C-C, Wang C-H, Fu C-H, et al. The link between chronic rhinosinusitis and asthma: a questionnaire-based study. Medicine. 2016;95:e4294. doi:10.1097/MD.0000000000004294
48. Park SY, Yoon SY, Shin B, et al. Clinical factors affecting discrepant correlation between asthma control test score and pulmonary function. Allergy Asthma Immunol Res. 2015;7(1):83–87. doi:10.4168/aair.2015.7.1.83
49. Bora M, Alpaydin AO, Yorgancioglu A, et al. Does asthma control as assessed by the asthma control test reflect airway inflammation? Multidiscip Respir Med. 2011;6:291–298. doi:10.1186/2049-6958-6-5-291
50. An TJ, Rhee CK, Park YB, Yoo KH, Yoon HK. FVC, but not FEV1, is associated with clinical outcomes of asthma-COPD overlap. Sci Rep. 2022;12(1):13820. doi:10.1038/s41598-022-15612-w
51. Chan R, Lipworth B. Forced vital capacity and low frequency reactance area measurements are associated with asthma control and exacerbations. Lung. 2022;200(3):301–303. doi:10.1007/s00408-022-00542-1
52. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. doi:10.1056/NEJMra050100
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.