Back to Journals » Infection and Drug Resistance » Volume 19
Daptomycin Dosing Based on Adjusted Body Weight in Obese Patients versus Actual Body Weight: A Multicentre Cohort Study
Authors Almangour TA ![]() , Almosabhi LS, Almojel R, Althubaity R, Almuhisen S, Almohaizeie A, Alowais SA
, Almosabhi LS, Almojel R, Althubaity R, Almuhisen S, Almohaizeie A, Alowais SA ![]() , Bin Saleh K, Damfu N, Alotaibi SN, Aldardeer NF
, Bin Saleh K, Damfu N, Alotaibi SN, Aldardeer NF ![]() , Alotaibi H, Alghamdi AA, Almuzaini M, Alyousef A, Alnehari F, Youssef SA, Alharbi MH, Al Musawa M
, Alotaibi H, Alghamdi AA, Almuzaini M, Alyousef A, Alnehari F, Youssef SA, Alharbi MH, Al Musawa M ![]() , Alsowaida YS
, Alsowaida YS
Received 8 November 2025
Accepted for publication 5 January 2026
Published 14 January 2026 Volume 2026:19 572989
DOI https://doi.org/10.2147/IDR.S572989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Thamer A Almangour,1 Latifa S Almosabhi,2 Rahaf Almojel,1 Rawabi Althubaity,1 Sara Almuhisen,3 Abdullah Almohaizeie,4,5 Shuroug A Alowais,6– 8 Khalid Bin Saleh,6– 8 Nader Damfu,7,9,10 Sultan N Alotaibi,7,10,11 Namareq F Aldardeer,12 Haifa Alotaibi,4 Albandari A Alghamdi,4 Marwah Almuzaini,13 Abdulrahman Alyousef,6 Faisal Alnehari,14 Sara A Youssef,15 Moataz H Alharbi,12 Mohammed Al Musawa,16 Yazed Saleh Alsowaida17
1Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia; 2Clinical Pharmacy Services, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 3Pharmacy services Administration, King Fahad Medical City, Riyadh, Saudi Arabia; 4Pharmaceutical Care Division, King Faisal Specialist Hospital & Research Centre, Riyadh, Saudi Arabia; 5College of Pharmacy, Alfaisal University, Riyadh, Saudi Arabia; 6Department of Pharmacy Practice, College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 7King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 8Pharmaceutical Care Department, King Abdulaziz Medical City, National Guard Health Affairs, Riyadh, Saudi Arabia; 9Infection Prevention and Control Department, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Jeddah, Saudi Arabia; 10King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 11Department of Pharmaceutical Care Services, King Salman Specialized Hospital, Ministry of the National Guard-Health Affairs, Taif, Saudi Arabia; 12Medical and Clinical Affairs Department, King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia; 13Pharmaceutical Care Services, King Salman Medical City, Ministry of Health, Medina, Saudi Arabia; 14Pharmaceutical Science Department, College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 15Department of Pharmaceutical Care, Saudi German Hospital, Hail, 55481, Saudi Arabia; 16Anti-Infective Research Laboratory, Department of Pharmacy Practice, Eugene Applebaum College of Pharmacy and Health Sciences, Wayne State University, Detroit, Michigan, USA; 17Department of Clinical Pharmacy, College of Pharmacy, University of Ha’il, Hail, 81442, Saudi Arabia
Correspondence: Thamer A Almangour, Department of Clinical Pharmacy, College of Pharmacy, King Saud University, P.O. Box 2457, Riyadh, 11451, Saudi Arabia, Email [email protected]
Purpose: Daptomycin-approved dosing is based on actual body weight (ABW). However, the pharmacokinetics and pharmacodynamics of daptomycin are altered in obese patients, leading to increased daptomycin exposure owing to incomplete distribution into excess body tissues. Data regarding the use of alternative weight descriptors for daptomycin dosing are limited. This study aimed to investigate the effectiveness and safety of daptomycin in obese patients by using adjusted body weight (AdjBW).
Methods: This retrospective multicenter cohort study in Saudi Arabia compared the outcomes of obese patients who received daptomycin based on AdjBW with those of obese and non-obese patients who received daptomycin based on ABW. The main outcomes included clinical cure, overall in-hospital mortality, and 30-day mortality. The safety outcomes were evaluated. Multivariate logistic regression was used to control for confounding variables.
Results: A total of 293 patients met the inclusion: 43 patients in AdjBW group, 54 in the ABW group, and 196 in the non-obese group. When comparing the AdjBW and ABW obese groups, no statistically significant difference was observed in clinical cure (83.7% vs 77.8%; p = 0.461; OR, 0.1.47; 95% CI, 0.52– 4.12), overall in-hospital mortality (23.3% vs 35.2%; p = 0.200; OR, 0.56; 95% CI, 0.23– 1.37), or 30-day mortality (16.3% vs 27.8%; p = 0.174; OR, 0.51; 95% CI, 0.19– 1.38). Creatine phosphokinase elevation (8.6% vs 6%; p = 0.651) was similar between the two groups. Similar outcomes were observed when comparing the AdjBW and non-obese groups.
Conclusion: Treatment with daptomycin based on AdjBW in obese patients had similar effectiveness and safety outcomes as treatment with daptomycin based on ABW in obese and non-obese patients. Therefore, future prospective studies are warranted.
Keywords: daptomycin, obese, adjusted body weight, dosing
Background
According to the World Health Organization, 16% of adults aged 18 years and over were living with obesity.1 In Saudi Arabia, 20.2% of adults 18 years and older were classified as obese according to the Ministry of Health.2 The physiology in obese individuals is different from that in non-obese individuals, which creates a considerable alteration in the pharmacokinetics and dosing approach of antimicrobial agents.3 Daptomycin is an antibiotic that is affected by these alterations. Since approval, daptomycin was administered based on the actual body weight (ABW). Increased body weight does not always lead to a proportional increase in the volume of distribution and clearance, particularly for hydrophilic antibiotics. For daptomycin, the absolute volume of distribution and clearance were higher in obese patients than in non-obese patients. However, the increments in these parameters are not proportional to the increment in body weight which increases the exposure to daptomycin.4 In a pharmacokinetic analysis comparing morbidly obese to non-obese subjects, 6 mg/kg was associated with a 2-fold higher area under the curve (AUC), Cmax, and Cmin in morbidly obese patients.5
Daptomycin dosing in individuals with obesity has also been associated with musculoskeletal toxicity. Pharmacokinetic modeling in a post hoc analysis showed that daptomycin Cmin of 24.3 mg/L or more was associated with an increased probability of creatine phosphokinase (CPK) elevation.6 When patients who weighed < 111 kg versus ≥ 111 kg received daptomycin 6 mg/kg daily were examined using Monte Carlo simulation, the probability of exceeding a daptomycin Cmin target of 24.3 mg/L was 6.5% versus 19.4%, respectively.6 In another pharmacokinetic analysis using 6 mg/kg in morbidly obese and non-obese subjects, the probabilities of exceeding a daptomycin Cmin target of 24.3 mg/L were 10.8% and 0.2%, respectively.5 In a retrospective, matched case-control risk factor analysis which reviewed 3042 individuals from 2004 to 2015 found that obesity (odds ratio, 3.28; P = 0.03) is a significant risk factor for daptomycin-associated rhabdomyolysis.7
The standard doses of daptomycin approved by the US Food and Drug Administration are 4 mg/kg for skin and skin structure infections as well as 6 mg/kg for bacteremia and right-sided infective endocarditis. However, daptomycin is concentration-dependent, and data suggest that higher doses may be required, especially for deep-seated and enterococcal infections.8 These data further complicates the dosing for obese patients and justifies the need to explore more appropriate dosing approaches for safety and effectiveness. The adjusted body weight (AdjBW) has been proposed as a weight descriptor for obese patients. In an unpublished pharmacodynamic study using Monte Carlo simulations, dosing based on AdjBW using a correction factor of 0.4 produced similar AUC0-24 of non-obese individuals receiving 6 mg/kg as seen in clinical trials.9
Obese patients were underrepresented in the clinical trials, and pharmacokinetic alteration in obese individuals justifies more investigation.3 Clinical outcome data to support the best dosing approach for the safety and effectiveness of daptomycin in obese patients are very limited. Earlier observational studies showed no difference in clinical and safety outcomes when daptomycin was dosed as 4–6 mg/kg/day using different weight descriptors.10,11 More recently, a retrospective study compared the use of AdjBW to ABW for daptomycin dosing in obese patients.12 This study showed no difference in clinical failure and 90-day mortality. However, this study has several limitations. It was conducted at a single center; most of the dosing regimens were ≤ 8 mg/kg, did not conduct stratification analysis, and did not compare the outcomes to those of non-obese individuals.
This study aimed to investigate the effectiveness and safety of daptomycin in obese patients using AdjBW compared with those in obese and non-obese patients using ABW.
Materials and Methods
Study Design and Setting
This retrospective multicenter cohort study included adult patients treated with daptomycin for infections caused by gram-positive pathogens. The study was conducted at seven hospitals in Saudi Arabia: King Saud University Medical City (KSUMC), a 1500-bed academic teaching hospital in Riyadh; King Faisal Specialist Hospital and Research Center (KFSHRC), a 1600-bed specialist hospital in Riyadh; King Fahad Medical City (KFMC), a 1200-bed hospital in Riyadh; King Abdulaziz Medical City (KAMC)/National Guard Health Affairs, a 1973-bed hospital in Riyadh; King Faisal Specialist Hospital and Research Center (KFSHRC), a 388-bed specialist hospital in Jeddah; King Abdulaziz Medical City (KAMC)/National Guard Health Affairs, a 750-bed hospital in Jeddah; and Saudi German Hospital, a 150-bed hospital in Hail. Adult patients admitted to the hospital between January 2016 and December 2023 and treated with daptomycin for infection due to a gram-positive pathogen for ≥48 hours were eligible for inclusion. Among patients with multiple episodes of infection treated with daptomycin, only the first episode was included. Given the retrospective observational design of the study, no sample size calculation was conducted, as all eligible patients within the predefined study period were included. This study included three groups: 1. AdjBW, the investigation group, included obese patients who received daptomycin based on AdjBW, 2. ABW, the control group, included obese patients who received daptomycin based on ABW, and 3. Non-obese patients, another control group, included non-obese patients who received daptomycin based on the ABW. Patients were excluded if the isolate was confirmed as not susceptible to daptomycin, including E. faecium isolates, not in the susceptible-dose dependent (SDD) interpretive category (MIC > 4 mcg/mL), allergy to daptomycin, creatinine clearance ≤ 30 mL/min, intermittent hemodialysis, continuous renal replacement therapy, or peritoneal dialysis. Clinical cure, overall in-hospital mortality, and 30-day mortality were the main outcomes of this study. Other outcomes included microbiological eradication, days to negative culture, infection-related mortality, length of hospital stay (LOS) from the start of daptomycin treatment, days to death from the index culture, and 60-day recurrence. We evaluated the safety outcomes, including CPK elevation, by assessing the levels at baseline and during treatment when available, as well as myopathy, rhabdomyolysis, and acute kidney injury (AKI). The daptomycin dose (mg/kg) and weight descriptor used were in accordance with each hospital’s protocol. The weight descriptor (ABW vs AdjBW) used for daptomycin dosing was specified in electronic medical records. This study was reviewed and approved by the Institutional Review Boards of the participating centers.
Microbiologic Testing
Identification and antimicrobial susceptibility testing of the bacterial isolates were conducted using automated systems based on each hospital’s protocol: MicroScan WalkAway 96 plus (Beckman Coulter, Inc., Brea, CA, USA), BD Phoenix M50 (Becton Dickinson Diagnostic Systems, Sparks, MD, USA) or VITEK 2 system (bioMérieux, Marcy-l’Étoile, France). Daptomycin E-test strips (BioMérieux SA) were used. Breakpoints used to determine the microbial susceptibility were according to the Clinical and Laboratory Standards Institute (CLSI).13 Microbiology laboratories were consistent with 2019 revisions to daptomycin breakpoints that were published in CLSI document M100 for Enterococcus species.
Definition
Time to active therapy was defined as the number of hours from the time the first index cultures were collected to the administration of any active antibiotic. Time to the study drug was defined as the number of hours from the time the first index cultures were collected to the initiation of daptomycin. Polymicrobial infection was defined as the microbial growth of at least one concomitant pathogenic microorganism during the same episode of index infection.
A number of endpoints used in this study were defined according to the criteria described in our previous studies.14,15 Clinical cure was defined as the resolution of the clinical manifestations associated with the infection, such that no additional therapeutic management for gram-positive infections was needed because of failure or modification due to adverse effects by the end of therapy.14,15 For the evaluation of clinical cure, progress reports documented by the treating clinicians were used in addition to an assessment of vital signs, laboratory data, and radiographic findings, when applicable. Throughout the data collection process, difficult cases or cases with disagreement were resolved by an open discussion between the center’s representatives and the principal investigator to develop a consensus.
In-hospital mortality was defined as death due to any reason during the current admission. The 30-day mortality was defined as death occurring within 30 days of index culture. This mortality was considered infection-related if the patients had ongoing unequivocal clinical and/or biochemical signs of infection at the time of death.14,15 Death notes were also reviewed when possible, and difficult cases or cases with disagreement were resolved through open discussion to develop a consensus.
Microbiological eradication was defined as a subsequent negative culture that showed elimination of the causative organism if repeated cultures were ordered. Persistence was defined as a positive repeat culture result for the same causative pathogen at the same infection site.
60-day infection recurrence was defined as the presence of clinical signs and symptoms of infection with repeated isolation of the same pathogen after evidence of at least one negative culture within 60 days of the primary infection.14,15
As a safety outcome, the RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) criteria were used to evaluate renal function. AKI was considered if any of the aforementioned categories occurred during therapy.16 The incidences of CPK elevation, myopathy, and rhabdomyolysis were retrospectively evaluated from the medical records. The normal reference range for CPK is 0–175 U/L. CPK was considered elevated if one of the following criteria was met up to 3 days after the last dose of daptomycin: ≥ 3 times the upper limit of normal if baseline CPK was within the normal reference range or not checked; ≥ 5 times the upper limit of normal if baseline CPK was greater than the upper limit of normal.6,10 If CPK was considered elevated, the medical records were reviewed for patient-reported symptoms of myopathy. We considered rhabdomyolysis if the patient had a CPK elevation as defined above, plus a positive urine myoglobin or AKI per the RIFLE criterion, or if the diagnosis was reported by the treating clinician in the medical record.
Obesity was defined as a body mass index of ≥ 30. In obese patients, AdjBW was computed as ideal body weight (IBW) + 0.4 x (ABW - IBW). To the best of our knowledge, the ABW closest to the daptomycin dose was used.
Statistical Analysis
Descriptive statistics were used to summarize the data. Categorical variables were expressed as counts and percentages and compared using the χ2 test. Continuous variables were presented as mean ± standard deviation (SD) or median and interquartile range (IQR) and compared using an independent t-test or Wilcoxon rank-sum test, as appropriate. Statistical significance was set at p < 0.05. Multivariate logistic regression analysis was used to minimize the effect of confounding baseline covariates on potential outcomes of interest.
Along with the treatment groups, covariates identified through clinical considerations, relevant demographics, and baseline clinical characteristics associated with a difference (p-value < 0.20) were eligible for inclusion in the model. Odds ratios/adjusted odds ratios from logistic regression and 95% confidence intervals (CI) were used to quantify group comparisons of the outcomes of interest. STATA 18 (StataCorp LP, College Station, Texas, USA) was used for all the analyses.
Results
A total of 1057 patients who received daptomycin were identified from the medical records and screened for eligibility. Of these, 293 patients met the inclusion criteria: 43 patients in the AdjBW group, 54 patients in the ABW group, and 196 patients in the non-obese group (Figure 1). Among the included cohort, 147 (50%) were male and the average age was 56 ± 19 years. Approximately 75% of the patients presented with bacteremia. Polymicrobial infections occurred in 129 (44%) patients. Concurrent antibiotics were administered to 58 (20%) patients. The median (IQR) time to active therapy and the duration of therapy were 24 (5–72) hours and 10.5 (7–15) days, respectively. Half of the etiological pathogens were E. faecium.
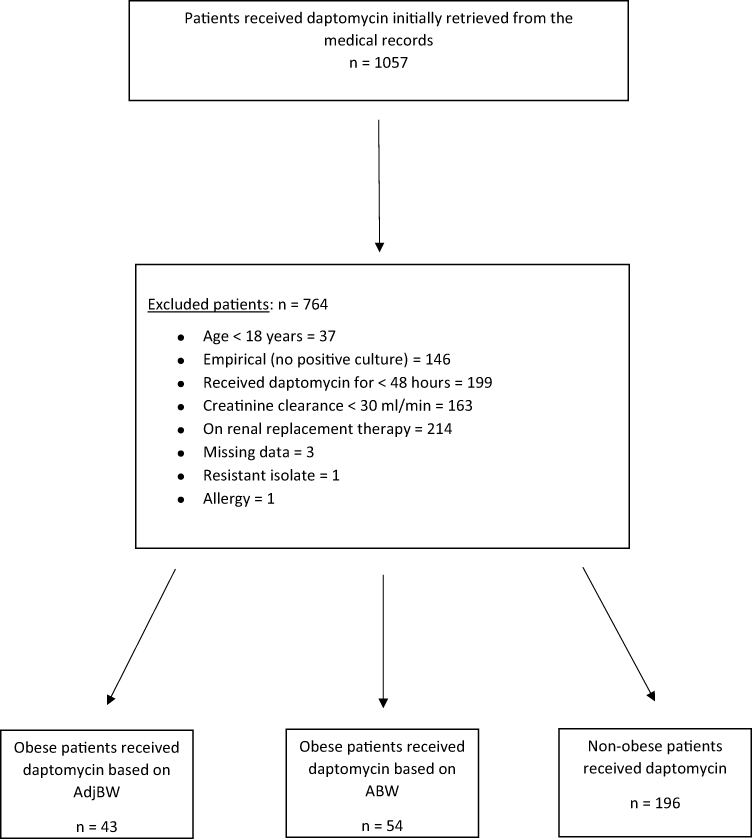 |
Figure 1 Patient enrollment and screening for eligibility. |
Demographics and baseline characteristics were comparable between AdjBW and ABW groups. However, more patients with class III obesity (≥40.0 kg/m2) were in the AdjBW group (30.2% vs 9.3%; p = 0.008). Moreover, the demographic and baseline characteristics were comparable between the AdjBW and non-obese groups. However, significantly more patients with diabetes mellitus (60.5% vs 36.7%; p = 0.004), hypertension (62.8% vs 39.8%; p = 0.006), presented with endocarditis (16.3% vs 5.1%; p = 0.010), received concurrent antibiotics (30.2% vs 16.3%; p = 0.035), and statin therapy (41.9% vs 18.4%; p = 0.001) were in the AdjBW. In contrast, more male patients (56.7% vs 34.9%; p = 0.010) and longer median hospital LOS before index culture (13 (3–34) vs 4 (1–21) days; p = 0.026) were observed in the non-obese group. The additional details are presented in Table 1.
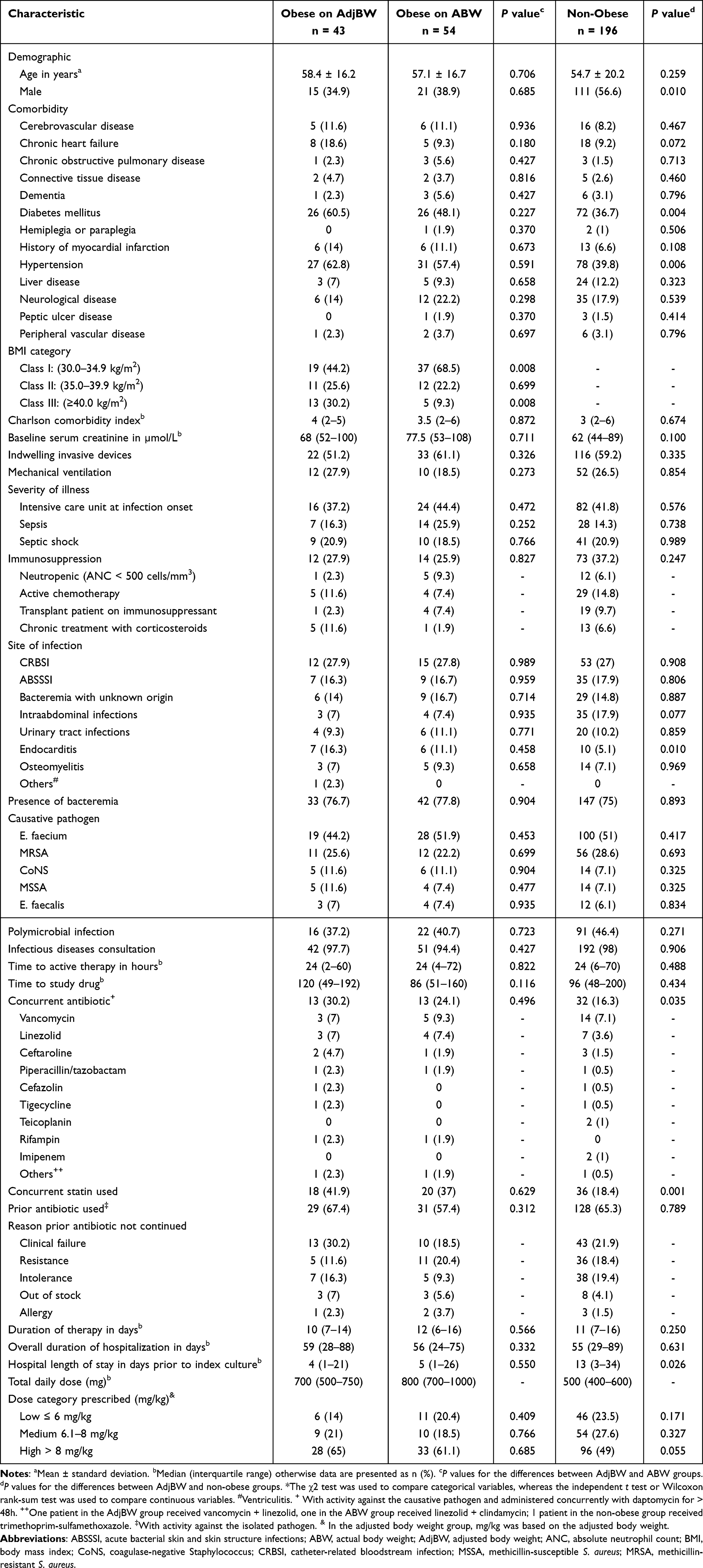 |
Table 1 Demographic and Baseline Characteristics of Included Patients* |
When comparing the AdjBW and ABW groups, no statistically significant difference was observed in clinical cure (83.7% vs 77.8%; OR, 1.47; 95% CI, 0.52–4.12), overall in-hospital mortality (23.3% vs 35.2%; OR, 0.56; 95% CI, 0.23–1.37), 30-day mortality (16.3% vs 27.8%; OR, 0.51; 95% CI, 0.19–1.38), or infection-related mortality (16.3% vs 16.7%; OR, 0.97; 95% CI, 0.33–2.86). After adjusting for differences between the two groups (adjusted for age, intensive care unit admission, presence of bacteremia, polymicrobial infections, time to study drug, concurrent antibiotic therapy, duration of therapy, and chronic heart failure), these outcomes remained statistically insignificant (Table 2). The differences between the two groups in the median days to death and median days to negative culture were not statistically significant (Table 3). The survival probability after the index culture and time to bacterial eradication after the start of therapy in the AdjBW and ABW groups are presented in Figure 2a and b. The safety outcomes, including CPK elevation (8.6% vs 6%; p = 0.651), myopathy (4.7% vs 3.7%; p = 0.816), rhabdomyolysis (2.3% vs 1.9%; p = 0.871), and AKI (16.3% vs 14.8%; p = 0.651), were similar between the AdjBW and ABW groups. The rate of evaluable patients in terms of CPK elevation was lower in AdjBW (81.4 vs 92.6%; p = 0.096); however, the difference was not statistically significant. The differences between the two groups in all other outcomes, including microbiological eradication, 60-day recurrence, and LOS from the start of daptomycin treatment, were not statistically significant (Table 2).
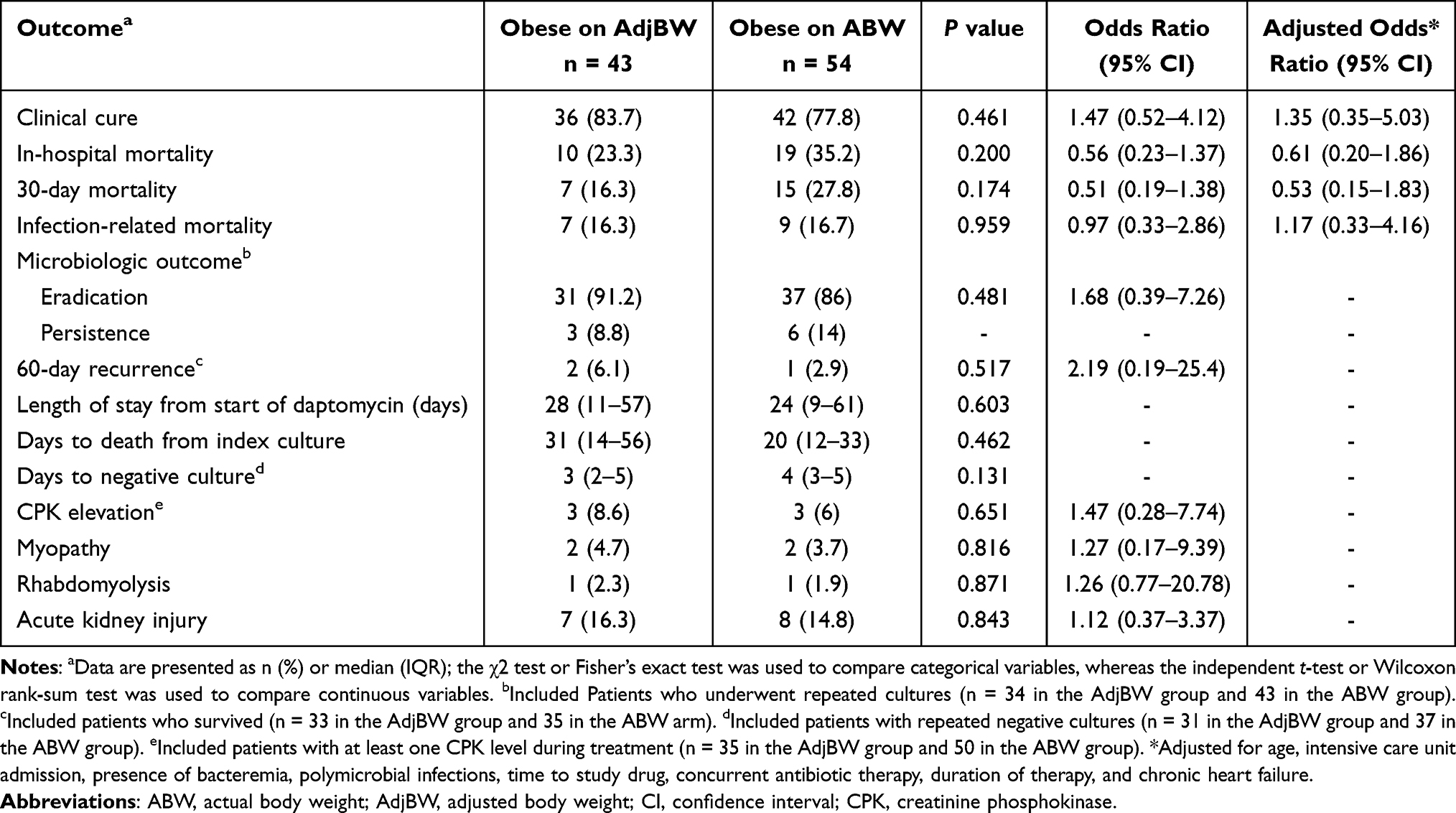 |
Table 2 Outcomes in Obese Patients Receiving Daptomycin Based on AdjBW versus ABW |
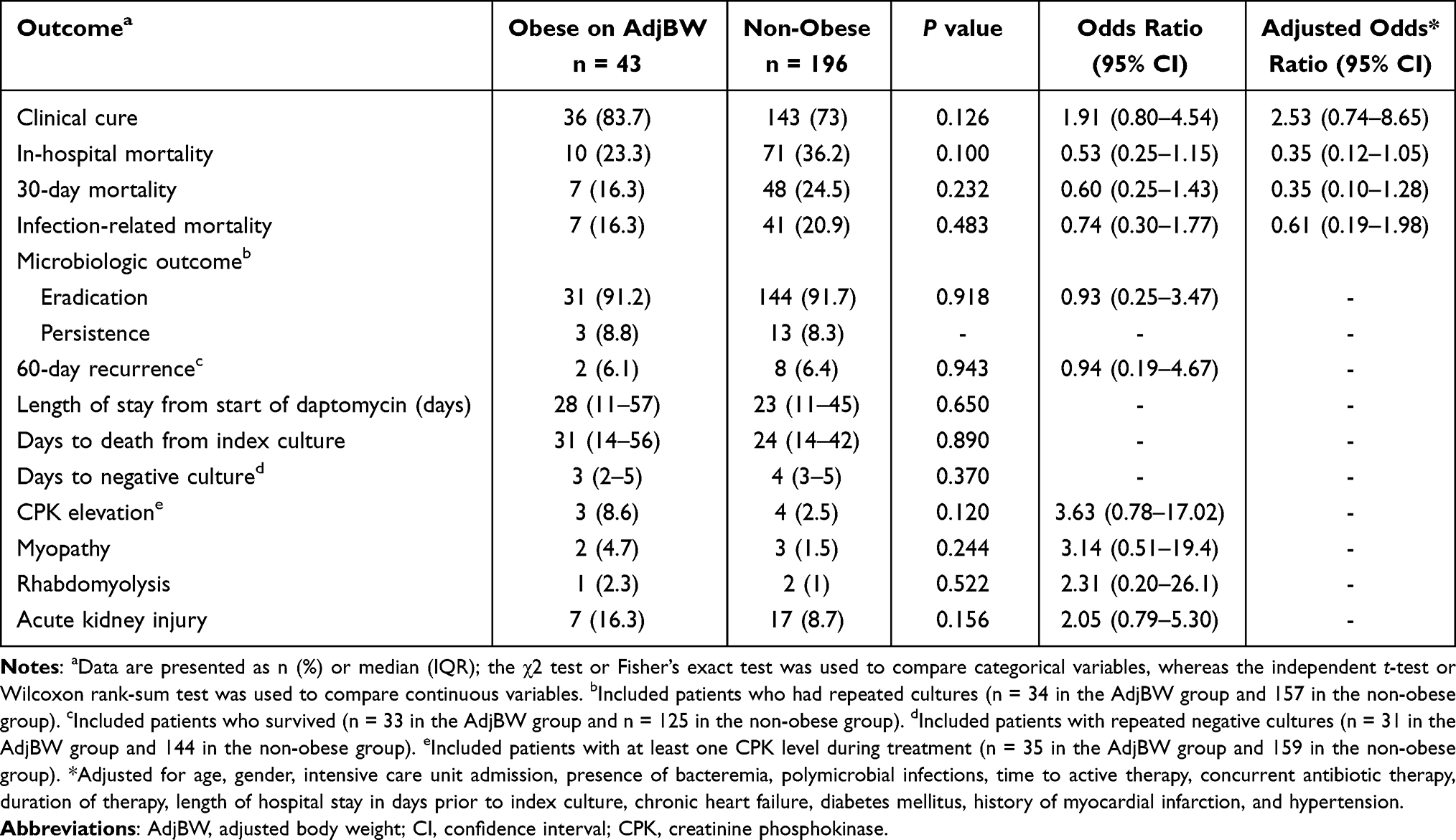 |
Table 3 Outcomes in Obese Patients Receiving Daptomycin Based on AdjBW versus Non-Obese |
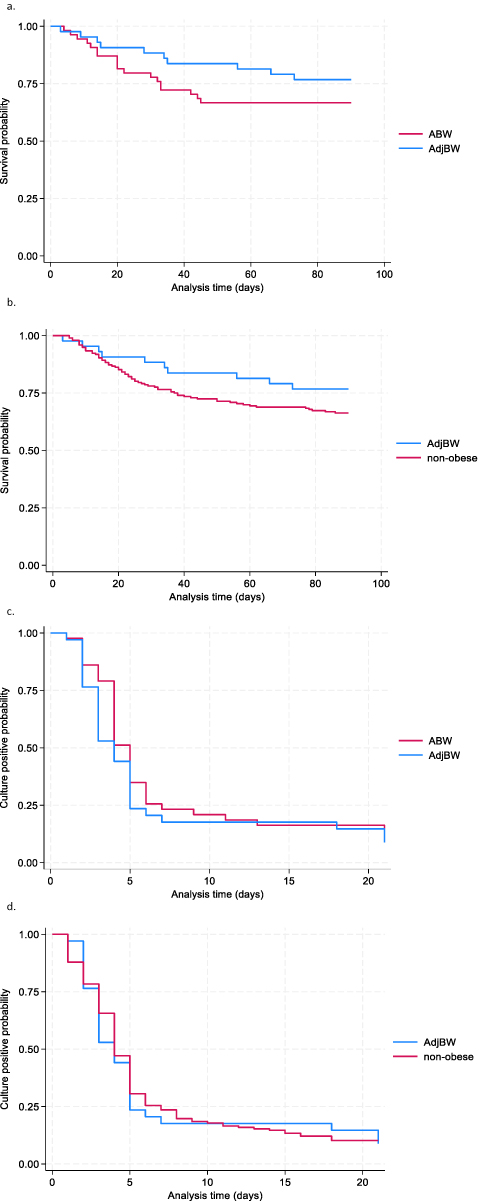 |
Figure 2 (a and b) Kaplan-Meier survival estimates by treatment. No statistically significant difference between the two groups in time to death at 90 days after the index culture. (a) AdjBW vs ABW (p = 0.242), (b) AdjBW vs non-obese (p = 0.183). (c and d) Time to bacterial eradication illustrated by Kaplan-Meier survival plot. No statistically significant difference between the two groups in time to negative culture at 21 days after start of therapy (c). AdjBW vs ABW (p = 0.264), (d) AdjBW vs non-obese (p = 0.728). Patients with repeated cultures were included in these plots (34, 43, and 157 patients in AdjBW, ABW, and non-obese groups, respectively). |
When comparing AdjBW to non-obese groups, no statistically significant difference was observed in clinical cure (83.7% vs 73%; OR, 1.91; 95% CI, 0.80–4.54), overall in-hospital mortality (23.3% vs 36.2%; OR, 0.53; 95% CI, 0.25–1.15), 30-day mortality (16.3% vs 24.5%; OR, 0.60; 95% CI, 0.25–1.43), or infection-related mortality (16.3% vs 20.9%; OR, 0.74; 95% CI, 0.30–1.77). After adjusting for differences between the two groups (adjusted for age, gender, intensive care unit admission, presence of bacteremia, polymicrobial infections, time to active therapy, concurrent antibiotic therapy, duration of therapy, hospital LOS in days prior to index culture, chronic heart failure, diabetes mellitus, history of myocardial infarction, and hypertension), these outcomes remained statistically insignificant (Table 3). The differences between the two groups in the median days to death and median days to negative culture were not statistically significant (Table 3). The survival probability after the index culture and time to bacterial eradication after the start of therapy in the AdjBW and non-obese groups are presented in Figure 2c and d. The safety outcomes, including CPK elevation (8.6% vs 2.5%; p = 0.120), myopathy (4.7% vs 1.5%; p = 0.244), rhabdomyolysis (2.3% vs 1%; p = 0.522), and AKI (16.3% vs 8.7%; p = 0.156), were similar between the two groups. The rate of evaluable patients in terms of CPK elevation was similar between the two groups (81.4 vs 80.6%; p = 0.906). The differences between the two groups in all other outcomes, including microbiological eradication, 60-day recurrence, and LOS from the start of daptomycin treatment, were not statistically significant (Table 3).
MIC data were available for 32, 26, and 103 patients in the ABW, AdjBW, and non-obese groups, respectively. The distributions of the isolates and MIC range are as follow: 53 were S. aureus with MIC ranging between 0.125–1 mcg/mL, 80 were E. faecium with MIC raging between 0.5–4 mcg/mL, 18 were coagulase-negative staphylococcus with MIC ranging between 0.5–1 mcg/mL, and 10 were E. faecalis with MIC ranging between 0.5–2 mcg/mL.
Subgroup analyses of the outcomes in obese patients who received daptomycin based on AdjBW versus obese patients who received daptomycin based on ABW and non-obese patients are shown in Figure 3 and Table 4.
 |
Table 4 Subgroup Analysis of the Outcomes in Obese Patients Who Received Daptomycin Based on AdjBW versus Obese Patients Who Received Daptomycin Based on ABW and Non-Obese Patients |
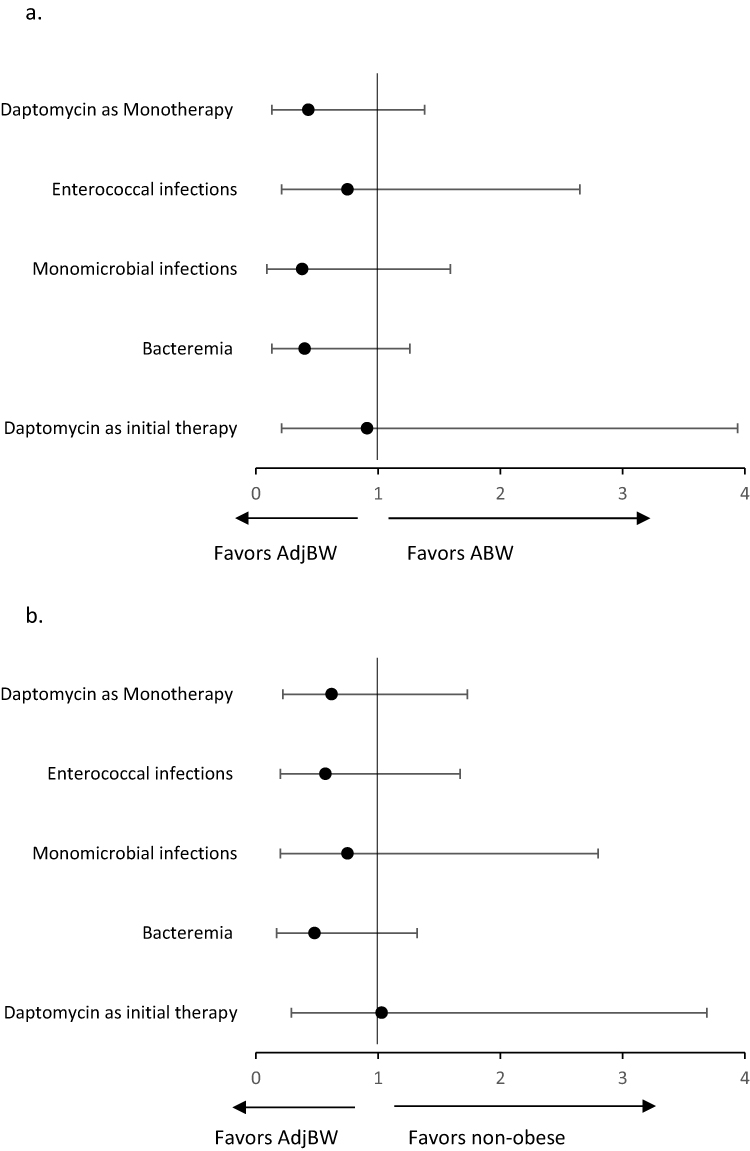 |
Figure 3 Odds ratios of 30-day mortality for (a) AdjBW versus ABW; (b) AdjBW vs non-obese among subpopulation of interest. Forest plot of boxes depicting odds ratio with 95% confidence intervals shown as horizontal lines. |
Discussion
This study showed that daptomycin treatment based on AdjBW in obese patients had similar clinical outcomes to daptomycin treatment based on ABW in obese and non-obese patients with infections caused by gram-positive pathogens. Clinical cure, in-hospital mortality, 30-day mortality, and infection-related mortality remained similar, even after adjusting for differences between the groups. Similar outcomes were observed after subgroup analyses for patients with monomicrobial infections and those who received daptomycin monotherapy. Safety outcomes were comparable between the two groups, including the rates of CPK elevation, myopathy, and AKI. No significant differences between the groups were observed in other outcomes, including bacterial eradication, 60-day recurrence, hospital LOS, days to death from the index culture, and days to negative culture. Although in-hospital mortality was numerically lower in the AdjBW group than in the ABW and non-obese groups, these differences were not statistically significant, possibly because the study was underpowered.
To the best of our knowledge, two studies are currently available that compared the clinical outcomes of daptomycin dose based on AdjBW versus ABW in obese patients are currently available. A single published abstract poster of 92 patients showed no statistically significant differences between daptomycin dosing based on AdjBW and ABW in terms of clinical effectiveness, microbiological success, in-hospital length of stay, mortality, or adverse effects. Although the results of this study were generally congruent with our findings, we could not further compare and contrast the outcomes given the limited available data in the poster abstract.11 The more recent retrospective study of 101 obese patients showed that daptomycin dosed based on AdjBW and ABW were statistically equivalent in clinical failure and 90-day mortality. The CPK elevation, however, was higher in AdjBW group.12 The results of this study were consistent with our findings but the CPK elevation in our study, although numerically higher in AdjBW group (n=3; 8.6%) versus ABW (n=3; 6%) and non-obese (n=4; 2.5%) groups, the differences did not reach the statistical significance. In our study, a justification could be the use of concurrent statins, which occurred in 2/3 of patients who had CPK elevation in the AdjBW group versus only 1/3 and 1/4 in the ABW and non-obese groups, respectively. All obese patients with elevated CPK levels in our study had class I obesity, and none exceeded the 10 mg/kg dose. In our study, we attempted to address and overcome the limitations of the previous study by including a higher daptomycin dosing, a non-obese arm, and stratification analysis.12 Lastly, the rate of evaluable patients in terms of CPK elevation was numerically higher in ABW group compared to AdjBW group. This is not surprising as obese patients on ABW are expected to have closer monitoring. We did not identify any trend toward fewer CPK monitoring in specific hospital in our study.
Daptomycin doses higher than those currently approved to achieve more appropriate target attainment and clinical outcomes have been suggested in several studies. An earlier in vivo pharmacodynamic study suggested that the AUC/MIC of daptomycin to achieve a 1 log-kill is ≥666.17 Pharmacokinetic/pharmacodynamic analyses showed that daptomycin doses ≥ 8 mg/kg are required to achieve this target, especially with MIC = 1 for Staphylococcus aureus infections.18–20 Furthermore, several observation studies,21–24 and current guidelines,25,26 recommended higher daptomycin doses. In a recent meta-analysis,8 the treatment success rate with daptomycin doses ≥ 8 mg/kg was higher in patients with complicated bacteremia and endocarditis. These studies did not address obese patients, and data on the optimal daptomycin dosing strategy in obese patients in light of these recommendations are lacking. Unlike the previous study, in which < 20% of patients received doses ≥ 8 mg/kg,12 approximately two-thirds of the obese patients in our study received this high-dose regimen which increases the generalizability of our study. In addition, the overall mean doses of daptomycin in the present study were 9±2, 9±2, and 8.3±1.8 in the AdjBW, ABW, and non-obese groups, respectively. After adjusting the absolute doses of daptomycin in the AdjBW group based on ABW, the overall mean dose was 7±1.6 mg/kg. Despite the lower overall exposure to daptomycin in the AdjBW group, clinical outcomes were comparable to those in the ABW and non-obese groups. The mean weight-based doses in our study were higher than the FDA-approved dosing of 4–6 mg/kg as well as higher than the mean doses of 5.6 mg/kg and 5.5 mg/kg in the ABW and AdjBW groups, respectively, as described in a previous study.12 It should be considered that more morbidly obese patients received daptomycin based on AdjBW, potentially due to concern for overdosing in those patients when ABW was used. This is consistent with the findings of Fox et al, who showed that more patients received daptomycin based on ABW in class I and II obesity, while more patients received daptomycin based on AdjBW in class III.12 This could affect the validity of the outcome in this obesity category, given that only a few patients were tested using ABW.
The MIC data were available for 161 patients. Although the MIC for the remaining isolates was not available or could not be obtained, the available 2023 antibiogram in our hospitals demonstrated 97–100% susceptibility to daptomycin, including SDD, to E. faecium. In a national antimicrobial surveillance study conducted in the Kingdom of Saudi Arabia and analyzed the data between 2013–2023, susceptibility of S. aureus to daptomycin was > 97%.27 Further, in a retrospective study, conducted in the Kingdom of Saudi Arabia and analyzed the data between 2012–2021, susceptibility of Enterococcus species from clinical samples to daptomycin was > 99%.28 In 2019, revisions to the daptomycin breakpoints were published in CLSI document M100 in which SDD interpretive category was implemented for E. faecium. This breakpoint was based on a dosage regimen of 8–12 mg/kg. The overall mean doses of daptomycin in mg/kg to treat E. faecium infections in our study were 8.5±1.7, 9.3±1.8, and 8.3±1.7 in AdjBW, ABW, and non-obese groups, respectively.
The limitations of this study include the retrospective nature of the design, which may introduce selection bias, inclusion bias, and inability to account for unmeasured residual confounding variables despite our attempts to minimize them using multivariable logistic regression. The sample size was relatively small in the obese versus non-obese groups, which may have affected the outcomes. Data on source control measures were not documented, which may have influenced the results. In addition, data on specific MICs were not documented for all isolates; however, 2023 available antibiograms from our hospitals showed that the susceptibility rate of gram-positive pathogens to daptomycin, including SDD, for E. faecium was 97–100%. Although assessing one microbe and one infection site might be better, we preferred to include multiple microbes and infection sites to increase the sample size and mimic a real-life population. However, we conducted a subgroup analysis to improve the internal validity of the study. For safety assessment, the frequency of CPK monitoring was not standard between different institutions and depended on the institution’s own protocol. However, we included patients with at least one CPK level checked during treatment. Despite these limitations, our study was conducted in seven centers across the kingdom, including a non-obese control. Multiple outcomes were assessed, subgroups were analyzed, and most patients in the obese groups received high-dose daptomycin.
In conclusion, treatment with daptomycin based on AdjBW in obese patients had similar effectiveness and safety outcomes as treatment with daptomycin based on ABW in obese and non-obese patients with infections caused by gram-positive pathogens. Based on the outcomes of our study, which is in line with the previously published pharmacokinetic and pharmacodynamic findings, AdjBW is a reasonable alternative weight descriptor for daptomycin dosing in obese patients, especially those at risk of CPK elevation and needed higher daptomycin doses such as those with complicated bacteremia or endocarditis. These findings may inform clinical decision-making in selecting dosing strategies for morbidly obese patients and in developing institutional protocols. However, our findings should be interpreted carefully in the context of small sample sizes, limited generalizability, and retrospective study design. Moreover, AdjBW as a weight descriptor in obese patients was proposed by a single unpublished pharmacodynamic study. Therefore, more pharmacokinetic/pharmacodynamic data especially with higher daptomycin dosing and clinical studies with larger sample sizes are needed to validate these findings.
Abbreviation
ABW, Actual body weight; AKI, Acute kidney injury; AdjBW, Adjusted body weight; AUC, Area under the curve; CPK, Creatine phosphokinase; IQR, Interquartile range; LOS, Length of hospital stay; SD, Standard deviation (SD).
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the institutional review board of King Saud University Medical City (IRB#E-23-7091) and all participating centers. The data were kept confidential; no one except the research team had access to the files. As the data were collected retrospectively, the institutional review board waived the requirement for consent to participate in accordance with the rules and regulations of the Kingdom regarding the conduct of research, and the IRB and international policies on human subject protection and confidentiality rights. This study was conducted in accordance with the Good Clinical Research Practice (Declaration of Helsinki).
Acknowledgment
The authors wish to thank King Saud University, Riyadh, Saudi Arabia, for supporting this research project: Ongoing Research Funding Program, (ORF-2025-74), King Saud University, Riyadh, Saudi Arabia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Albandari Alghamdi reports grants, personal fees, non-financial support from King Faisal Specialist Hospital, during the conduct of the study. The authors declare that they have no other conflicts of interest in this work.
References
1. World Health Organization. Obesity and overweight. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
2. Ministry of health Saudi Arabia. Obesity. Available from: https://www.moh.gov.sa/en/awarenessplateform/ChronicDisease/Pages/Obesity.aspx.
3. Meng L, Mui E, Ha DR, Stave C, Deresinski SC, Holubar M. Comprehensive guidance for antibiotic dosing in obese adults: 2022 update. Pharmacotherapy. 2023;43(3):226–14. doi:10.1002/phar.2769
4. Dvorchik BH, Damphousse D. The pharmacokinetics of daptomycin in moderately obese, morbidly obese, and matched nonobese subjects. J Clin Pharmacol. 2005;45(1):48–56. doi:10.1177/0091270004269562
5. Butterfield-Cowper JM, Lodise TP Jr, Pai MP. A fixed versus weight-based dosing strategy of daptomycin may improve safety in obese adults. Pharmacotherapy. 2018;38(9):981–985. doi:10.1002/phar.2157
6. Bhavnani SM, Rubino CM, Ambrose PG, Drusano GL. Daptomycin exposure and the probability of elevations in the creatine phosphokinase level: data from a randomized trial of patients with bacteremia and endocarditis. Clin Infectious Dis. 2010;50(12):1568–1574. doi:10.1086/652767
7. Dare RK, Tewell C, Harris B, et al. Effect of statin coadministration on the risk of daptomycin-associated myopathy. Clin Infectious Dis. 2018;67(9):1356–1363. doi:10.1093/cid/ciy287
8. Samura M, Takada K, Hirose N, et al. Comparison of the efficacy and safety of standard- and high-dose daptomycin: a systematic review and meta-analysis. Br J Clin Pharmacol. 2023;89(4):1291–1303. doi:10.1111/bcp.15671
9. Sr FA. Dosing of daptomycin in the morbidly obese: which body weight is it? In:
10. Ng JK, Schulz LT, Rose WE, et al. Daptomycin dosing based on ideal body weight versus actual body weight: comparison of clinical outcomes. Antimicrob Agents Chemother. 2014;58(1):88–93. doi:10.1128/AAC.01018-13
11. Shemanski S, Bennett N, Boyd SE, Woods M, Ploetz J, Kennedy KF. 698: Evaluation of clinical effectiveness utilizing adjusted body weight for daptomycin dosing. Crit Care Med. 2016;44:251. doi:10.1097/01.ccm.0000509375.46415.fe
12. Fox AN, Smith WJ, Kupiec KE, et al. Daptomycin dosing in obese patients: analysis of the use of adjusted body weight versus actual body weight. Ther Adv Infect Dis. 2019;6:2049936118820230. doi:10.1177/2049936118820230
13. CLSI. Clinical and Laboratory Standards Institute. CaLS. Performance Standards for Antimicrobial Susceptibility Testing.
14. Alotaibi S, Damfu N, Alnefaie A, et al. Efficacy of ciprofloxacin in treating gram-negative infections: does obesity matter? Pharmacy. 2024;12(5):147. doi:10.3390/pharmacy12050147
15. Almangour TA, Alkherb Z, Alruwaite S, et al. Trimethoprim-sulfamethoxazole versus levofloxacin for the treatment of Stenotrophomonas maltophilia infections: a multicentre cohort study. J Global Antimicrob Resist. 2024;38:42–48. doi:10.1016/j.jgar.2024.05.016
16. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, the A. Acute renal failure – definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the acute dialysis quality initiative (ADQI) group. Crit care. 2004;8(4):R204. doi:10.1186/cc2872
17. Safdar N, Andes D, Craig WA. In vivo pharmacodynamic activity of daptomycin. Antimicrob Agents Chemother. 2004;48(1):63–68. doi:10.1128/AAC.48.1.63-68.2004
18. Urakami T, Hamada Y, Oka Y, et al. Clinical pharmacokinetic and pharmacodynamic analysis of daptomycin and the necessity of high-dose regimen in Japanese adult patients. J Infect Chemother. 2019;25(6):437–443. doi:10.1016/j.jiac.2019.01.011
19. Yamada T, Ooi Y, Oda K, et al. Observational study to determine the optimal dose of daptomycin based on pharmacokinetic/pharmacodynamic analysis. J Infection Chemother. 2020;26(4):379–384. doi:10.1016/j.jiac.2019.11.002
20. Yamada T, Soda M, Nishida R, et al. Simplified daptomycin dosing regimen for adult patients with methicillin-resistant Staphylococcus aureus infections based on population pharmacokinetic analysis. Drug Metab Pharmacokinet. 2022;44:100444. doi:10.1016/j.dmpk.2022.100444
21. Lai CC, Sheng WH, Wang JT, et al. Safety and efficacy of high-dose daptomycin as salvage therapy for severe gram-positive bacterial sepsis in hospitalized adult patients. BMC Infect Dis. 2013;13:66. doi:10.1186/1471-2334-13-66
22. Kullar R, Casapao AM, Davis SL, et al. A multicentre evaluation of the effectiveness and safety of high-dose daptomycin for the treatment of infective endocarditis. J Antimicrob Chemother. 2013;68(12):2921–2926. doi:10.1093/jac/dkt294
23. Britt NS, Potter EM, Patel N, Steed ME. Comparative effectiveness and safety of standard-, medium-, and high-dose daptomycin strategies for the treatment of vancomycin-resistant enterococcal bacteremia among veterans affairs patients. Clin Infectious Dis. 2017;64(5):605–613. doi:10.1093/cid/ciw815
24. Chuang YC, Lin HY, Chen PY, et al. Effect of daptomycin dose on the outcome of vancomycin-resistant, daptomycin-susceptible enterococcus faecium bacteremia. Clin Infectious Dis. 2017;64(8):1026–1034. doi:10.1093/cid/cix024
25. Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American heart association. Circulation. 2015;132(15):1435–1486. doi:10.1161/CIR.0000000000000296
26. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infectious Dis. 2011;52(3):e18–55. doi:10.1093/cid/ciq146
27. Thabit AK, Alabbasi AY, Alnezary FS, Almasoudi IA. An overview of antimicrobial resistance in Saudi Arabia (2013-2023) and the Need for National Surveillance. Microorganisms. 2023;11(8):2086. doi:10.3390/microorganisms11082086
28. Al Bshabshe A, Algarni A, Shabi Y, et al. Characterization and antimicrobial susceptibility patterns of enterococcus species isolated from nosocomial infections in a saudi tertiary care hospital over a ten-year period (2012-2021). Diagnostics. 2024;14(11):1190. doi:10.3390/diagnostics14111190
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.