Back to Journals » OncoTargets and Therapy » Volume 10
Cytomembranic PD-L1 expression in locoregionally advanced nasopharyngeal carcinoma
Authors Zheng L ![]() , Cao C, Cheng G, Hu Q, Chen X
, Cao C, Cheng G, Hu Q, Chen X
Received 19 September 2017
Accepted for publication 17 October 2017
Published 16 November 2017 Volume 2017:10 Pages 5483—5487
DOI https://doi.org/10.2147/OTT.S152007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yao Dai
Video abstract presented by Xiaozhong Chen.
Views: 356
Linfeng Zheng,1,* Caineng Cao,2,3,* Guoping Cheng,1 Qiaoying Hu,2,3 Xiaozhong Chen2,3
1Department of Pathology, 2Department of Radiation Oncology, Zhejiang Cancer Hospital, Hangzhou, 3Zhejiang Key Laboratory of Radiation Oncology, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Background and objective: The aim of this study was to evaluate the expression of cytomembranic programmed death-ligand 1 (PD-L1) and its clinical significance in locoregionally advanced nasopharyngeal carcinoma (NPC).
Patients and methods: Formalin-fixed, paraffin-embedded tissue biopsies from 85 patients with histological diagnosis of locoregionally advanced NPC treated with radical intensity-modulated radiotherapy and concurrent cisplatin-based chemotherapy were studied. By using immunohistochemistry staining, expressions of cytomembranic PD-L1 on tumor cells were detected.
Results: After a median follow-up duration of 65.8 months, 7 (8.2%), 5 (5.9%), and 5 (5.9%) patients suffered from local failure, regional failure, and distant metastases, respectively. The 5-year local failure-free survival, regional failure-free survival, distant failure-free survival, and overall survival (OS) rates were 90.9%, 94.8%, 94.0%, and 92.2%, respectively. Our results revealed that a high expression of cytomembranic PD-L1 was correlated with shorter OS (5y-OS: 82.5% vs 97.6%, P=0.022). In the multivariate analysis, only the cytomembranic PD-L1 was an independent prognostic factor for OS (hazard ratio: 6.176, 95% confidence interval, 1.166–32.710, P=0.032).
Conclusion: Cytomembranic PD-L1 expression levels correlated with OS in locoregionally advanced NPC. Agreement between different methods is needed for further application of PD-L1 biomarker assays in NPC.
Keywords: nasopharyngeal carcinoma, programmed death-ligand 1, PD-L1, prognosis, overall survival
Introduction
Nasopharyngeal carcinoma (NPC) is an endemic malignancy in southern China, with a peak annual incidence approaching 30 per 100,000 persons.1 More than 70% of patients with newly diagnosed NPC are classified as having locoregionally advanced disease.2 With the advent of concurrent chemoradiotherapy, intensity-modulated radiotherapy (IMRT), and imaging techniques, locoregional control has substantially improved and distant metastasis is now the main source of treatment failure for NPC.1
Programmed death-ligand 1 (PD-L1) is an immune checkpoint which regulates Type 1 T helper immune responses and mediates cancer immune evasion.3 Recently, a Phase Ib trial of metastatic NPC suggested encouraging results after treatment with a programmed death-1 (PD-1) inhibitor.4 However, to date, only a few studies of NPC on PD-L1 are available, and the prognostic role of PD-L1 has not yet been fully evaluated.5–11 Thus, the aim of this study is to evaluate the expression of cytomembranic PD-L1 and its clinical significance in locoregionally advanced NPC.
Patients and methods
Patients and samples
This study was approved by the independent ethics committee, Zhejiang Cancer Hospital. Consent was waived and patient records were deidentified and anonymized prior to analysis.
For this study, 116 NPC patients were consecutively sampled by 1 medical care group from March 2010 to May 2012. Patients were selected based on the following criteria: 1) histologically proven locoregionally advanced NPC with available biopsy specimens; 2) Karnofsky score ≥70; 3) receiving radical IMRT and concurrent cisplatin-based chemotherapy at initial diagnosis;12 4) no previous malignancy or other concomitant malignant disease; and 5) PD-L1 staining was detectable in the tumor cells. Therefore, there were 85 patients who qualified for this study. All patients underwent disease staging using the American Joint Committee on Cancer (AJCC) 2010 staging system. The clinical characteristics are listed in Table 1.
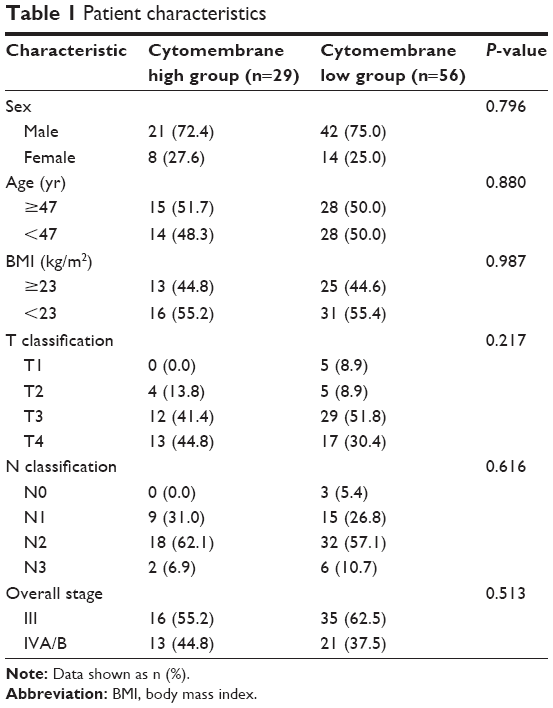 | Table 1 Patient characteristics |
Immunohistochemistry (IHC) staining
Immunohistochemical staining of 5 μm sections from formalin-fixed paraffin-embedded nasopharyngeal biopsies specimens was performed in the Department of Pathology of our hospital with the antibody 1:200 anti-PD-L1 (E1L3N; Cell Signaling Technology, Danvers, MA, USA) using the standard protocol for routine diagnostic specimens. Hematoxylin and eosin sections were also reviewed for the presence of tumors. The immunoreactivity of PD-L1 was scored semi-quantitatively as follows: the percentage of tumor cells with cytomembranic positivity (0, ≤5%; 1, 6 to ≤25%; 2, 26 to ≤50%; 3, 51 to ≤75%; 4, >75%) was added with the intensity of staining (0, negative; 1, weak; 2, moderate; 3, strong), resulting in a score of 0–7. Patients with a score of 1 or 2 were considered low expression.
Statistical analysis
The Statistical Package for Social Sciences, version 17.0 (SPSS, Chicago, IL, USA), software was used for statistical analysis. The local failure-free survival (LFFS), regional failure-free survival (RFFS), distant failure-free survival (DFFS), and overall survival (OS) were estimated by use of the Kaplan–Meier method. LFFS, RFFS, DFFS, and OS were measured from Day 1 of treatment to the date of the event. Log-rank test was used in univariate analysis. χ2 and Fisher’s exact tests were used to compare the differences between the cytomembrane high group and the cytomembrane low group. Multivariate analysis was performed using the Cox proportional hazards model. All statistical tests were two sided, and P<0.05 was considered to be statistically significant.
Results
General information
Among the 85 patients enrolled, including 63 males and 22 females, the median age was 47 years (range from 18 to 67 years). The median body mass index (BMI) was 22.8 kg/m2 (range, 16.7–30.1 kg/m2). All tumors were classified as having nonkeratinizing phenotype. Thirty patients (35.3%) had Stage T4 disease, and 8 patients (9.4%) had Stage N3 disease. After a median follow-up duration of 65.8 months, 7 (8.2%) patients died and 7 (8.2%), 5 (5.9%), and 5 (5.9%) patients suffered from local failure, regional failure, and distant metastasis, respectively. The 5-year LFFS, RFFS, DFFS, and OS rates were 90.9%, 94.8%, 94.0%, and 92.2%, respectively.
Clinicopathologic correlations
PD-L1 staining was detectable in 85 patients (73.3%, 85 of 116 patients) and was mainly located at the membrane or in the cytoplasm region (or both) in the tumor cells. The membrane-mainly tumors accounted for 9.4% of patients (8/85), cytoplasm-mainly tumors accounted for 65.9% of patients (56/85), and similar expression on both the membrane and cytoplasm accounted for 24.7% of patients (21/85). Cytomembranic PD-L1 staining was classified as high expression in 29 patients. Representative cytomembranic staining of PD-L1 in NPC is shown in Figure 1. In this study, high expression of cytomembranic PD-L1 staining was not significantly correlated with the clinicopathological parameters of age, sex, BMI, or clinical stage at diagnosis. Detailed data are summarized in Table 1.
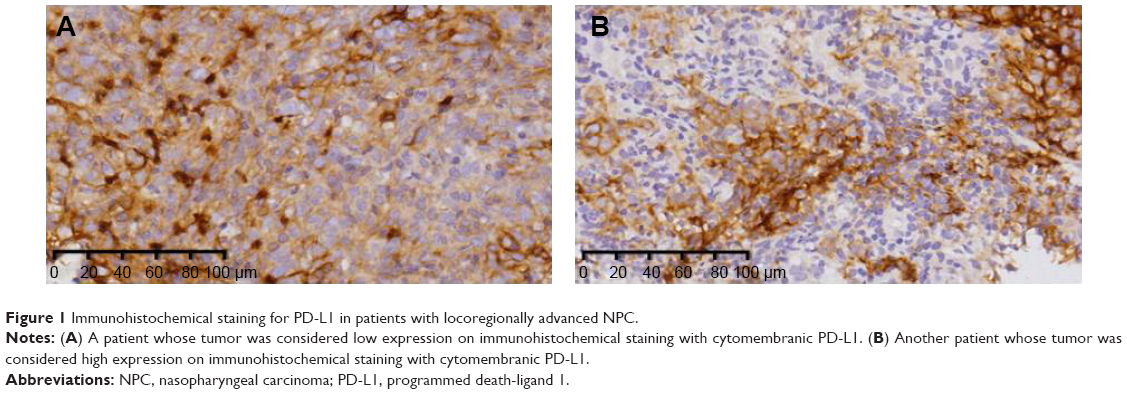 | Figure 1 Immunohistochemical staining for PD-L1 in patients with locoregionally advanced NPC. |
Prognostic values related with PD-L1
The values of various potential prognostic factors including age, sex, BMI, overall stage, and PD-L1 on predicting LFFS, RFFS, DFFS, and OS were evaluated. The outcomes of univariate analysis are shown in Table 2. Our results revealed that a high expression of cytomembranic PD-L1 was correlated with worse OS (5y-OS: 82.5% vs 97.6%, P=0.022, Figure 2). In the multivariate analysis, only PD-L1 was suggested to be an independent prognostic factor for OS (hazard ratio: 6.176, 95% confidence interval, 1.166–32.710, P=0.032).
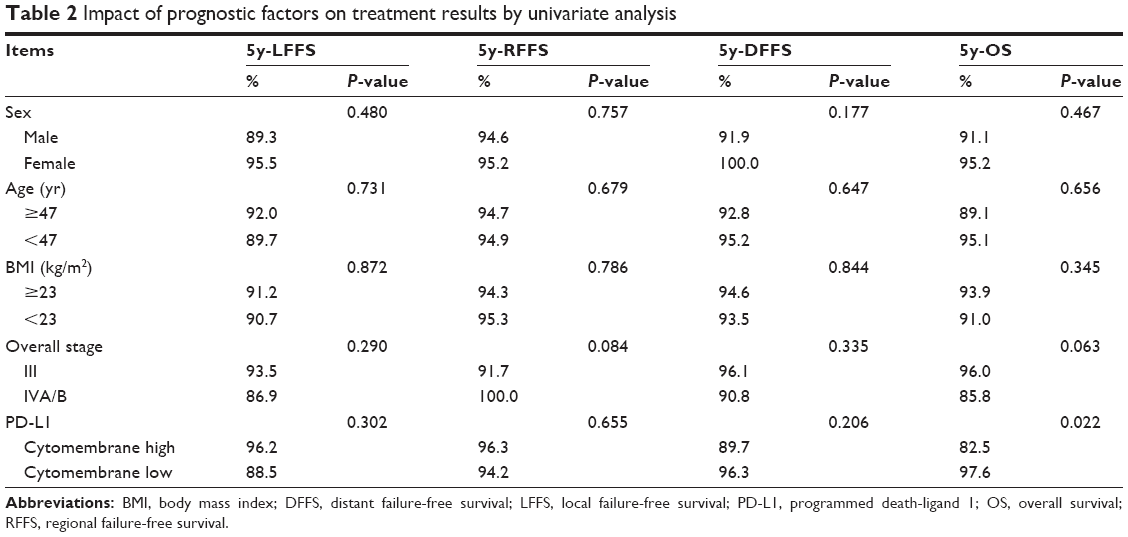 | Table 2 Impact of prognostic factors on treatment results by univariate analysis |
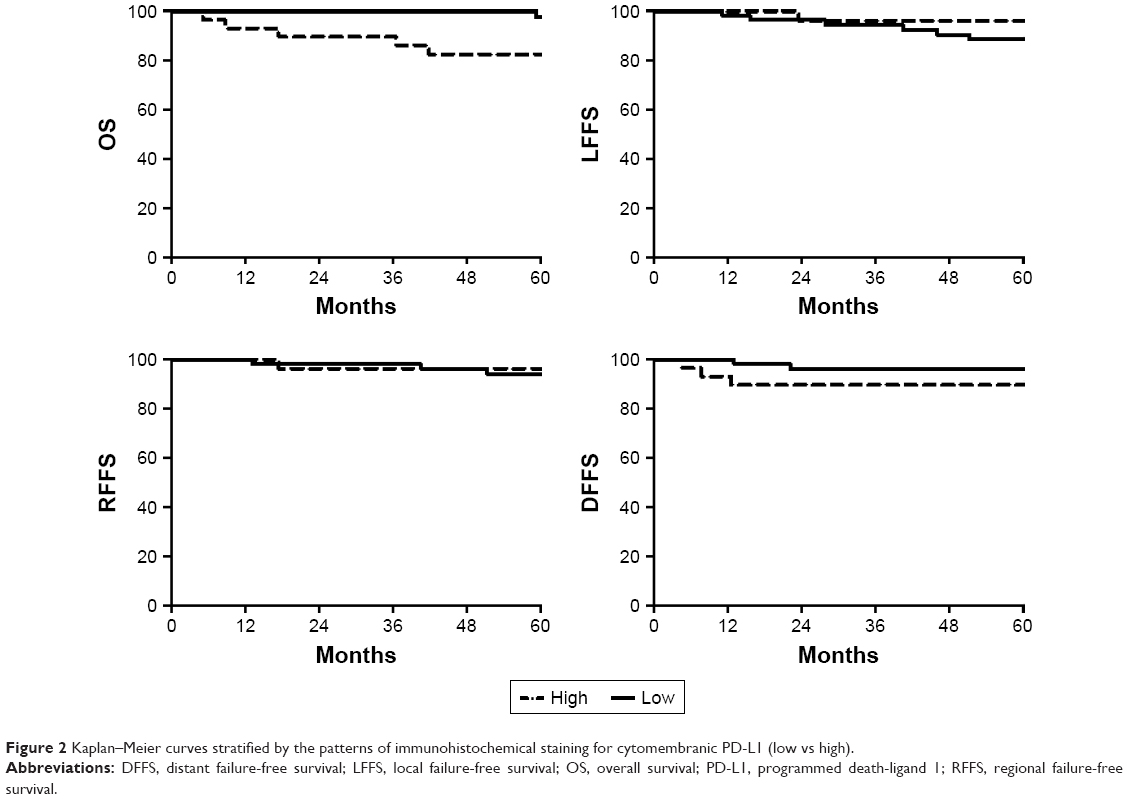 | Figure 2 Kaplan–Meier curves stratified by the patterns of immunohistochemical staining for cytomembranic PD-L1 (low vs high). |
Discussion
In our study, cytomembranic PD-L1 was overexpressed in 73.3% of locoregionally advanced NPC patients, and 25.0% of patients had tumors with high expression of cytomembranic PD-L1. Our results revealed that locoregionally advanced NPC patients with high cytomembranic PD-L1 expression had a significantly reduced survival outcome, which was similar to the results of previous studies.5–7 However, Lee et al8 reported that there was a longer survival rate in nonmetastatic NPC patients treated by IMRT with high PD-L1 expression; Chan et al10 reported that OS and progression-free survival did not correlate with baseline PD-L1 expression in 161 patients with NPC receiving standard-of-care treatment. These differences could have multifactorial causes, such as of the difference in PD-L1 monoclonal antibodies, staining protocols, detection systems, and different scoring algorithms used.
Hsu et al9 demonstrated that the expression rate of PD-1 in intratumoral CD8 cells significantly correlated with a poorer prognosis of OS, disease-free survival, and LFFS of 46 NPC patients. However, in a larger cohort (total n=161), the impact of PD-L1 on tumor-infiltrating immune cells was not obvious.10 Biomarker expression in lymphoid or other immune effector cells is a special challenge for pathologists.13 Inter- and intraobserver bias for tumor cells is higher than for tumor-infiltrating lymphocytes,14 and the pathologist cannot always recognize whether the existing lymphocyte population is inflammation or oncogene driven.14,15 Furthermore, reproducible PD-L1 IHC scoring of tumor cells seems feasible, whereas scoring of immune cells did not yield reproducible results.16 In our study, the impact of PD-L1 on tumor-infiltrating immune cells was not analyzed.
The scoring system of IHC for PD-L1 has yet to be defined.8 However, several groups have evaluated the degree of agreement on PD-L1 among different methods. The extent of concordance among three validated, commercially available PD-L1 IHC assays (Dako 22C3, Ventana SP263, and Dako 28-8) was compared in 493 non-small-cell lung cancer samples. The three assays indicated similar patterns of tumor membrane staining, with high correlation between percentage PD-L1 staining. Between assays at multiple expression cut-offs, including 1%, 10%, 25%, and 50% tumor membrane staining, an overall percentage agreement of >90% was achieved.17 In the present study, the expression of cytomembranic PD-L1 in locoregionally advanced NPC was evaluated. Agreement between different methods is needed for application of PD-L1 biomarker assays in NPC.
There are several limitations in the current study, including the inclusion of patients with cytomembranic PD-L1 staining who completed treatment only, the retrospective nature of the study design, and the limited number of patients with Stage T4 or N3 disease, and these could affect the outcomes. Nevertheless, our report is noteworthy because this is the first study to evaluate cytomembranic PD-L1 expression in locoregionally advanced NPC.
Conclusion
Cytomembranic PD-L1 expression levels correlated with OS in locoregionally advanced NPC. Agreement between different methods is needed for application of PD-L1 biomarker assays in NPC.
Acknowledgments
We thank Dr Feng Jiang, Dr Qifeng Jin, Dr Ting Jin, Dr Shuang Huang, Dr Yuanyuan Chen, Dr Yongfeng Piao, Dr Yonghong Hua, and Dr Xinglai Feng for collecting the data. The present study was supported by Zhejiang Province Medical and Health Science and Technology Project (2017182785).
Disclosure
The authors report no conflicts of interest in this work.
References
Lee AW, Ma BB, Ng WT, et al. Management of nasopharyngeal carcinoma: current practice and future perspective. J Clin Oncol. 2015;33:3356–3364. | ||
Mao YP, Xie FY, Liu LZ, et al. Re-evaluation of 6th edition of AJCC staging system for nasopharyngeal carcinoma and proposed improvement based on magnetic resonance imaging. Int J Radiat Oncol Biol Phys. 2009;73:1326–1334. | ||
Chen DS, Irving BA, Hodi FS. Molecular pathways: next-generation immunotherapy–inhibiting programmed death-ligand 1 and programmed death-1. Clin Cancer Res. 2012;18:6580–6587. | ||
Hsu C, Lee SH, Ejadi S, et al. Antitumor activity and safety of pembrolizumab in patients with PD-L1-positive nasopharyngeal carcinoma: interim results from a phase 1b study. Ann Oncol. 2015;26(Suppl 9):ix94. | ||
Zhang J, Fang W, Qin T, et al. Co-expression of PD-1 and PD-L1 predicts poor outcome in nasopharyngeal carcinoma. Med Oncol. 2015;32(3):86. | ||
Fang W, Zhang J, Hong S, et al. EBV-driven LMP1 and IFN-γ up-regulate PD-L1 in nasopharyngeal carcinoma: implications for oncotargeted therapy. Oncotarget. 2014;5(23):12189–12202. | ||
Zhou Y, Shi D, Miao J, et al. PD-L1 predicts poor prognosis for nasopharyngeal carcinoma irrespective of PD-1 and EBV-DNA load. Sci Rep. 2017;7:43627. | ||
Lee VH, Lo AW, Leung CY, et al. Correlation of PD-L1 expression of tumor cells with survival outcomes after radical intensity-modulated radiation therapy for non-metastatic nasopharyngeal carcinoma. PLoS One. 2016;11(6):e0157969. | ||
Hsu MC, Hsiao JR, Chang KC, et al. Increase of programmed death-1-expressing intratumoral CD8 T cells predicts a poor prognosis for nasopharyngeal carcinoma. Mod Pathol. 2010;23(10):1393–1403. | ||
Chan OS, Kowanetz M, Ng WT, et al. Characterization of PD-L1 expression and immune cell infiltration in nasopharyngeal cancer. Oral Oncol. 2017;67:52–60. | ||
Zhou Y, Miao J, Wu H, et al. PD-1 and PD-L1 expression in 132 recurrent nasopharyngeal carcinoma: the correlation with anemia and outcomes. Oncotarget. 2017;8(31):51210–51223. | ||
Jin T, Qin WF, Jiang F, et al. Interim analysis of a prospective randomized non-inferiority trial of cisplatin and fluorouracil induction chemotherapy with or without docetaxel in nasopharyngeal carcinoma. Oncotarget. Epub 2016 Jul 28. | ||
Hutarew G. PD-L1 testing, fit for routine evaluation? From a pathologist’s point of view. Memo. 2016;9(4):201–206. | ||
Teng MW, Ngiow SF, Ribas A, et al. Classifying cancers based on T-cell infiltration and PD-L1. Cancer Res. 2015;75(11):2139–2145. | ||
Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, openlabel, phase 2 randomised controlled trial. Lancet. 2016;387:1837–1846. | ||
Scheel AH, Dietel M, Heukamp LC, et al. Harmonized PD-L1 immunohistochemistry for pulmonary squamous-cell and adenocarcinomas. Mod Pathol. 2016;29(10):1165–1172. | ||
Ratcliffe MJ, Sharpe A, Midha A, et al. Agreement between programmed cell death ligand-1 diagnostic assays across multiple protein expression cut-offs in non-small cell lung cancer. Clin Cancer Res. 2017;23:CCR-1116–CCR-2375. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.