Back to Journals » OncoTargets and Therapy » Volume 10
Cytokine-induced killer cells/dendritic cells and cytokine-induced killer cells immunotherapy for the treatment of esophageal cancer in China: a meta-analysis
Authors Liu Y, Mu Y, Zhang A ![]() , Ren SD, Wang WH, Xie JP, Zhang YX, Zhou CH
, Ren SD, Wang WH, Xie JP, Zhang YX, Zhou CH
Received 17 January 2017
Accepted for publication 14 March 2017
Published 29 March 2017 Volume 2017:10 Pages 1897—1908
DOI https://doi.org/10.2147/OTT.S132507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Yan Liu,1,* Ying Mu,2,* Anqi Zhang,3 Shaoda Ren,3 Weihua Wang,3 Jiaping Xie,2 Yingxin Zhang,3 Changhui Zhou3
1Department of Gastroenterology, Weifang People’s Hospital, Weifang, 2Department of Gastroenterology, 3Central Laboratory, Liaocheng People’s Hospital, Liaocheng Clinical School of Taishan Medical University, Liaocheng, Shandong Province, People’s Republic of China
*These authors contributed equally to this work
Background: Immunotherapy based on cytokine-induced killer cells or combination of dendritic cells and cytokine-induced killer cells (CIK/DC-CIK) showed promising clinical outcomes for treating esophageal cancer (EC). However, the clinical benefit varies among previous studies. Therefore, it is necessary to systematically evaluate the curative efficacy and safety of CIK/DC-CIK immunotherapy as an adjuvant therapy for conventional therapeutic strategies in the treatment of EC.
Materials and methods: Clinical trials published before October 2016 and reporting CIK/DC-CIK immunotherapy treatment responses or safety for EC were searched in Cochrane Library, EMBASE, PubMed, Wanfang and China National Knowledge Internet databases. Research quality and heterogeneity were evaluated before analysis, and pooled analyses were performed using random- or fixed-effect models.
Results: This research covered 11 trials including 994 EC patients. Results of this meta-analysis indicated that compared with conventional therapy, the combination of conventional therapy with CIK/DC-CIK immunotherapy significantly prolonged the 1-year overall survival (OS) rate, overall response rate (ORR) and disease control rate (DCR) (1-year OS: P=0.0005; ORR and DCR: P<0.00001). Patients with combination therapy also showed significantly improved quality of life (QoL) (P=0.02). After CIK/DC-CIK immunotherapy, lymphocyte percentages of CD3+ and CD3–CD56+ subsets (P<0.01) and cytokines levels of IFN-γ, -2, TNF-α and IL-12 (P<0.00001) were significantly increased, and the percentage of cluster of differentiation (CD)4+CD25+CD127– subset was significantly decreased, whereas analysis of CD4+, CD8+, CD4+/CD8+ and CD3+CD56+ did not show significant difference (P>0.05).
Conclusion: The combination of CIK/DC-CIK immunotherapy and conventional therapy is safe and markedly prolongs survival time, enhances immune function and improves the treatment efficacy for EC.
Keywords: cytokine-induced killer cells, dendritic cells, esophageal cancer, immunotherapy, meta-analysis
Introduction
Esophageal cancer (EC) is a global common cancer, with 450,000 new cases and 400,000 estimated deaths per year.1,2 The incidence of EC has increased exponentially over the past few decades and the 5-year survival rate remains bleak.3 At present, surgery, radiotherapy and chemotherapy are most widely used for EC.4 However, their application is limited by the failure to thoroughly eliminate tumor cells, drug resistance and other adverse effects.5,6 Therefore, a more effective and safer therapeutic method is urgently required.
In recent years, immunotherapy has been rising rapidly and is considered the fourth powerful therapeutic method after surgery, radiotherapy and chemotherapy.6 Cancer immunotherapy is accomplished in multiple ways, including manipulation of the immune system through the use of immune agents, such as vaccines,7 cytokines,8 checkpoint inhibitors (including anti-programmed death 1 [PD-1]/PD-ligand 1 [PD-L1] antibodies and anti-cytotoxic T-lymphocyte-associated antigen (CTLA)-4 antibodies),9,10 kinase inhibitors (such as apatinib and gefitinib)11,12 and immune cells.13–19 However, their applications have the following hurdles. Simply activating the immunity via vaccination is not able to thoroughly eliminate tumor cells because cancer patients are usually in immunosuppression.19 Promotion of molecule-targeted treatment for tumors is also confined only to cancer patients bearing specific antigen-expressing cells.13 Notably, adoptive cellular immunotherapy has been flourishing in cancer treatment. Its effectiveness relies on the application of dendritic cells (DCs),14 tumor-infiltrating lymphocytes (TILs),15 natural killer (NK) cells,16 cytotoxic T lymphocytes (CTLs),17 cytokine-induced killer (CIK) cells18 and other immune cells. CIK cells, which consist primarily of the CD3+CD56+ subset, are induced by interferon (IFN)-γ, interleukin (IL)-1, cluster of differentiation (CD)3 monoclonal antibodies (OKT3) and IL-2 in vitro.5 Compared with other immune cells, CIK cells are easy to obtain from peripheral blood and umbilical cord blood mononuclear cells, and they possess higher in vitro proliferation capacity, stronger antitumor activity and broader antitumor spectrum.6 The tumoricidal ability of CIK cells is implemented by inducing tumor cell apoptosis through direct contact and secretion of cytokines such as IL-2, tumor necrosis factor (TNF)-α and IFN-γ.20 CIK cells have shown promising prospects in immunotherapy for cancers. On the one hand, the cytotoxicity of CIK cells is not affected by immune inhibitors such as cyclosporin A (CsA) and FK506.21 On the other hand, CIK cell-mediated cytotoxicity does not rely on the major histocompatibility complex (MHC). As in most cancers, these cells do not express MHC or human leukocyte antigen (HLA); this property of CIK cells is a great advantage over other immune cells in adoptive cell therapy.22
DCs are the most potent antigen-presenting cells and are essential in CIK activation, proliferation, phenotype expression and cytokine secretion.5,23,24 The cytotoxicity of CIK cells is remarkably enhanced when cocultured with DCs, indicated by the increased proportion of CD3+CD56+ cells and the improved levels of cytokines such as IL-2, IFN-γ, IL-12 and TNF-α.6,23 Meanwhile, cocultured DCs also downregulate the expression of negative regulatory factors, including transforming growth factor (TGF)-β and IL-10, as well as the proportion of CD4+CD25+ regulatory T cells (Tregs) among CIK cells, which suppress the antitumor activity of CIK.5,24 Several research reports have shown that the combination of DCs and CIKs (DC-CIK) is more effective and has indicated more promising clinical prospects than single CIK treatment.6
In EC treatment, there are emerging data indicating CIK or DC-CIK (CIK/DC-CIK) immunotherapy in combination with conventional therapy exhibited better therapeutic efficacy than conventional therapy alone.25–37 However, CIK/DC-CIK immunotherapy clinical application is still in its infancy. In this research, we conducted a meta-analysis to investigate the efficacy and safety of CIK/DC-CIK combined with conventional therapy in comparison with conventional therapy alone for EC, in order to provide scientific evidence for future clinical trials.
Materials and methods
Search strategy and selection criteria
Literature reports were searched across Cochrane Library, EMBASE, PubMed, Wanfang and China National Knowledge Internet databases with the key terms “dendritic cells”, “immunotherapy”, “cytokine-induced killer cells” or “DC-CIK” combined with “esophageal cancer”. No language limits were applied. The initial search was performed in April 2016 and updated in October 2016.
Studies selected in our research were randomized controlled clinical trials for EC. The included studies were all performed with comparison between the combination of CIK/DC-CIK and conventional treatment (defined as combination therapy group) and conventional regimens alone (defined as conventional therapy-alone group).
Data collection and quality assessment
Two authors independently searched and collected literatures from the databases according to our inclusion criteria, and they extracted the data from all the selected articles. Discrepancy was resolved by discussion with a third author. The collected information included the first authors’ names, the years of publication, the numbers of subjects, patient ages, tumor stages, experiment regimens, in vitro cell culture conditions and dosages of the utilized immune cells. The quality of the included articles was evaluated according to the Cochrane Handbook.38
Definition of outcome measurements
Treatment efficacy was assessed in terms of overall survival (OS), overall response rate (ORR; ORR = complete response rate + partial response rate), disease control rate (DCR; DCR = complete response rate + partial response rate + stable disease rate), patients’ quality of life (QoL) and adverse events. OS was defined as the length of time from the initiation of treatment to death from any cause.39 The immune function of EC patients before and after treatment was determined by the status of the lymphocyte subsets (CD3+, CD4+, CD8+, CD3−CD56+, CD3+CD56+ and CD4+CD25+CD127−) and cytokine secretion (IFN-γ, IL-2, TNF-α and IL-12).
Statistical analysis
Data were analyzed using Review Manager version 5.2 provided by Cochrane Collaboration. P<0.05 was considered statistically significant. Heterogeneity among the studies was assessed to determine the most suitable model.40 A random-effects method was applied when heterogeneity existed; otherwise, a fixed-effects method was used. Cochran’s Q-test was performed in order to evaluate homogeneity among studies, and I2<50% or P>0.1 was considered homogeneous. Odds ratios (ORs) were the principal measurements for therapeutic effects and were presented with 95% confidence intervals (CIs).
Results
Search results
A total of 1,405 articles were identified by initial retrieval. After title and abstract review, 1,381 articles were excluded because they did not focus on clinical trials (n=1,261), were in duplication and repetition (n=107) or were unrelated studies (n=13), and 24 studies remained as potentially relevant. After reading the full texts, 8 papers with insufficient data and 5 reviews or meta-analyses were excluded. Finally, 11 trials that included 994 EC patients met the inclusion criteria for our meta-analysis (Figure 1).
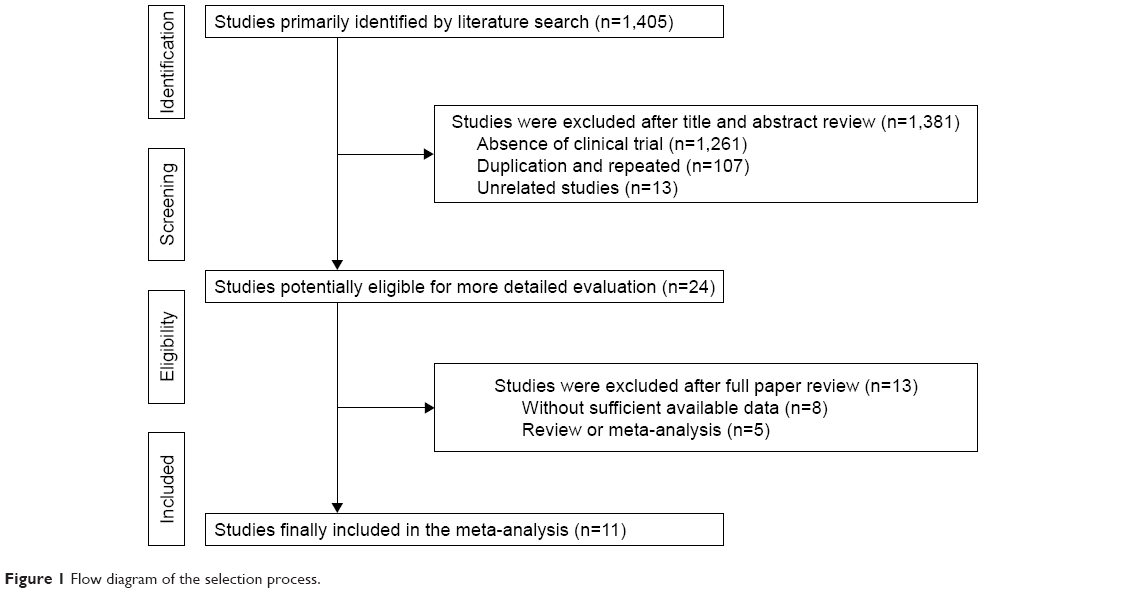 | Figure 1 Flow diagram of the selection process. |
Patient characteristics
In all, 11 eligible trials including 994 EC patients were included in this analysis. All trials were conducted in mainland China. In total, 501 patients were treated by CIK/DC-CIK in combination with conventional therapy (combination therapy), while 493 patients were treated by conventional therapy alone. Detailed clinical information of the trials is presented in Table 1. DC and CIK cells used in the 11 trials were all obtained from autologous peripheral blood. In 4 trials, DC-CIK immunotherapy was applied, whereas in the other 7 trials, only CIK cells were used. In most studies, patients were transfused with >1×109 immune cells, and other studies did not provide accurate cell numbers. Tumor size and injection modes were not analyzed in this article due to the lack of sufficient data in the included studies.
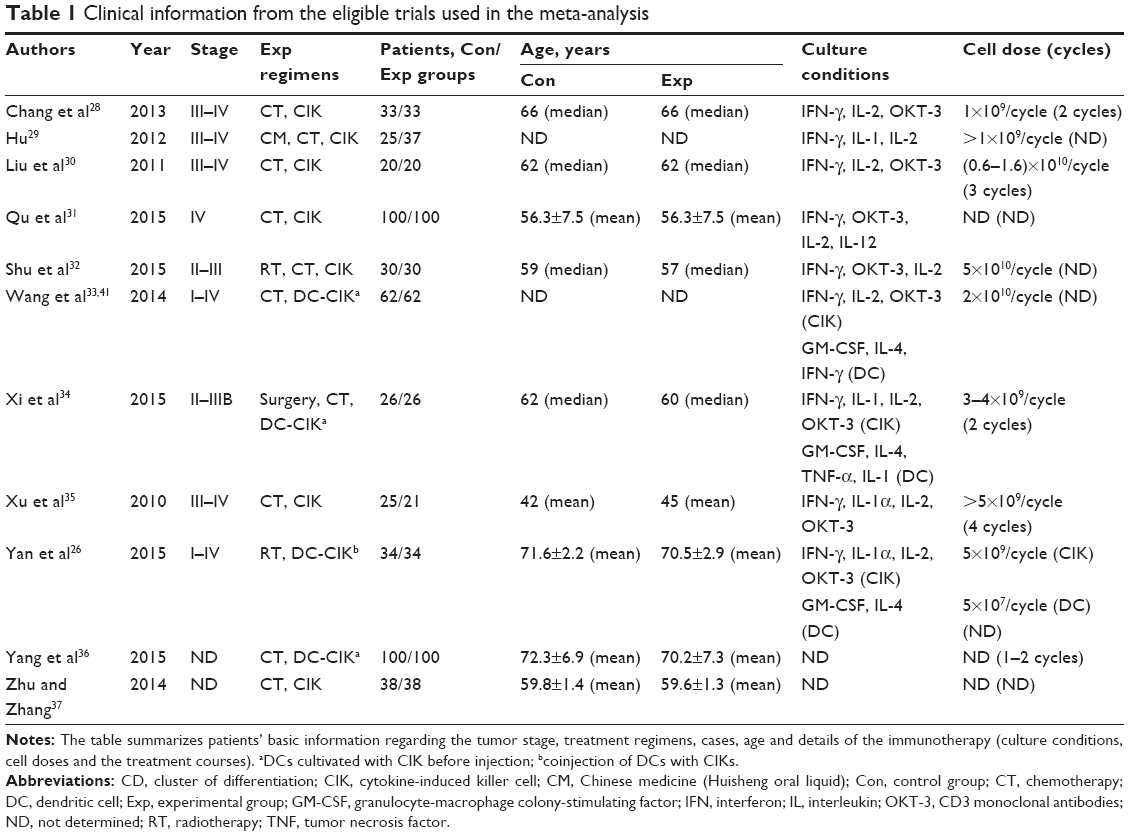 | Table 1 Clinical information from the eligible trials used in the meta-analysis |
Quality assessment
The assessment for risk of bias is shown in Figure 2A and B. The quality of the involved studies ranged from moderate to high: 9 studies were low in risk of bias, while the other 2 studies did not have a clear description of the randomization process. The allocation, performance, detection and attrition risks of the involved studies were low; 3 trials were considered to be of unclear risk owing to their selective reporting, while 3 other studies were considered as high risk as they did not show primary outcome data.
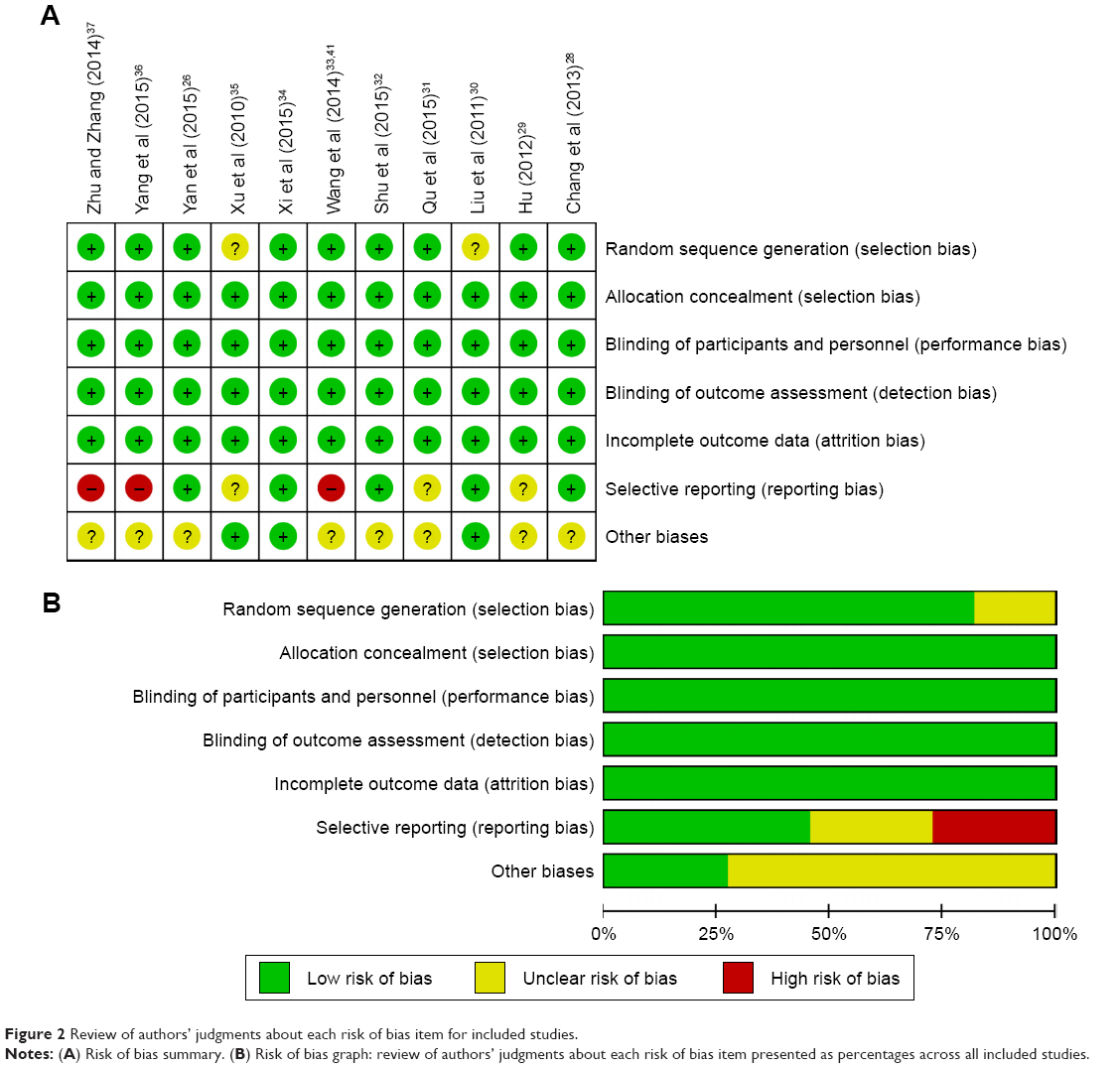 | Figure 2 Review of authors’ judgments about each risk of bias item for included studies. |
Efficacy assessments
This analysis indicated that OS, ORR and DCR were significantly improved in patients who underwent combination therapy compared to those treated by conventional therapy alone (Figure 3, 1-year OS: OR =2.59, 95% CI =1.52–4.40, P=0.0005; ORR: OR =2.18, 95% CI =1.57-3.02, P<0.00001; DCR: OR =3.83, 95% CI =2.47-5.92, P<0.00001). Moreover, the pooled results showed that patients in the combination therapy group had significantly improved QoL (Figure 4, QoL: OR =1.94, 95% CI =1.13-3.33, P=0.02). The fixed-effects model was applied in this analysis considering the slightly significant heterogeneity.
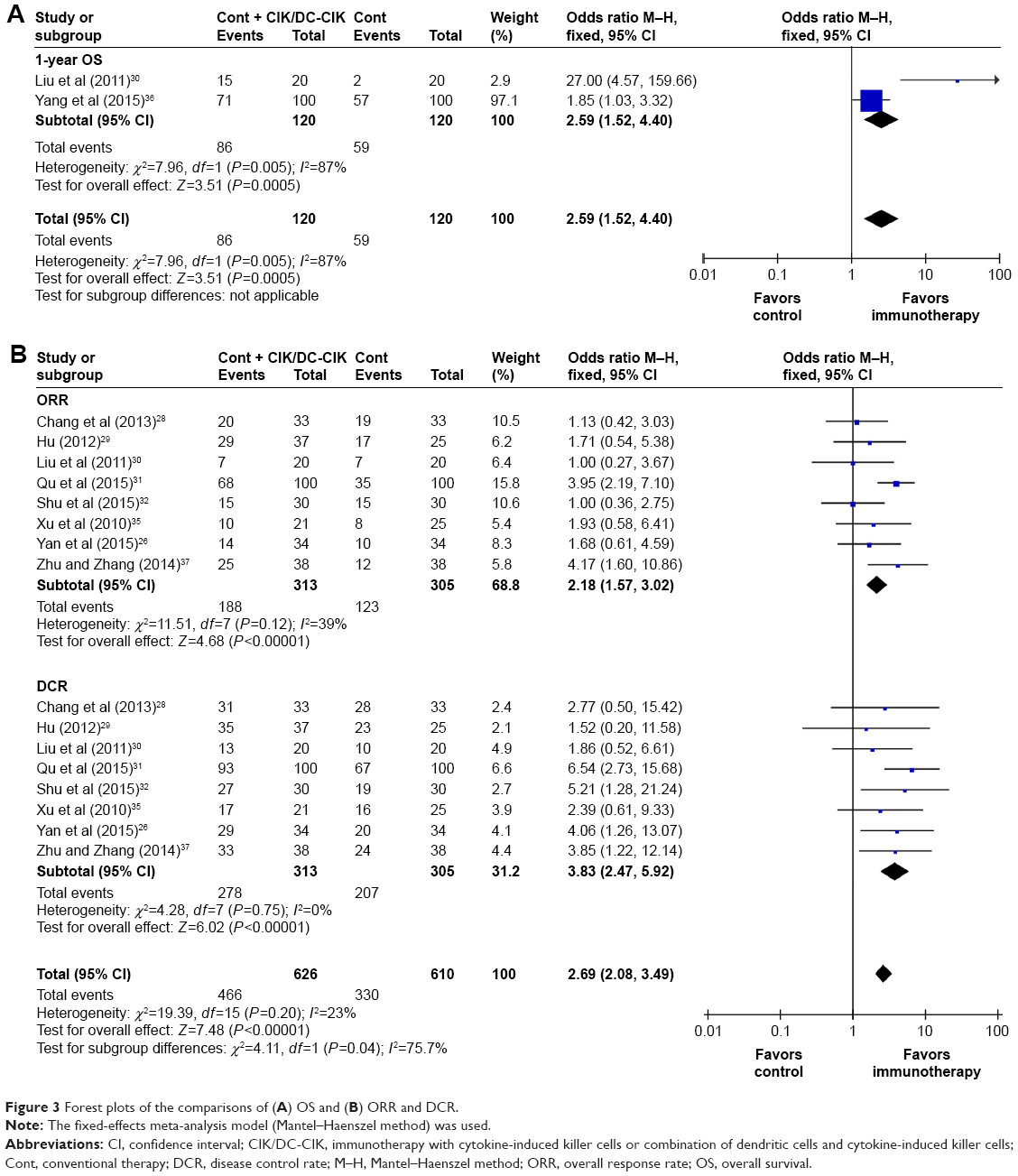 | Figure 3 Forest plots of the comparisons of (A) OS and (B) ORR and DCR. |
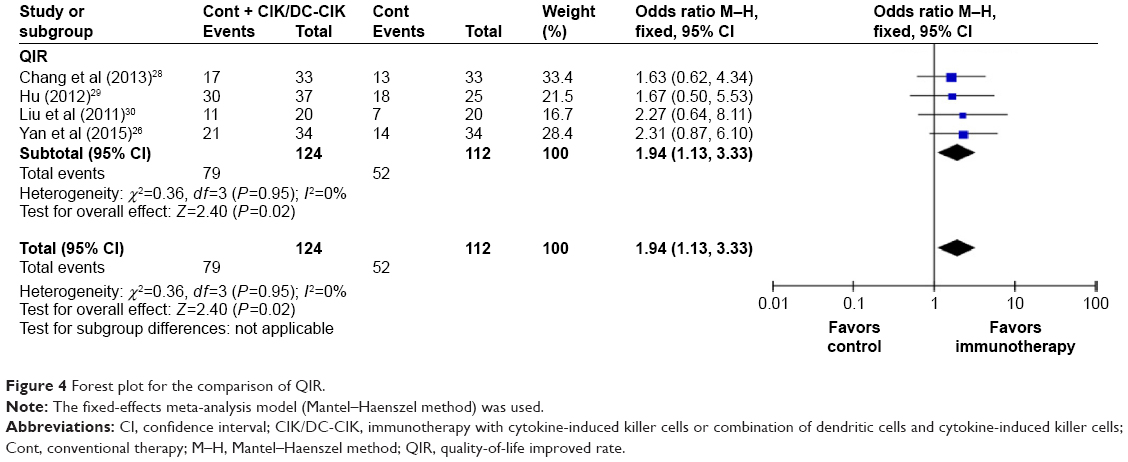 | Figure 4 Forest plot for the comparison of QIR. |
Immune function evaluation
The immune status of patients was examined before and after the treatment. After CIK/DC-CIK treatment, the proportions of CD3+ and CD3−CD56+ in patients were significantly increased (Figure 5, CD3+: OR =9.48, 95% CI =6.19-12.77, P<0.00001; CD3−CD56+: OR =6.57, 95% CI =2.00−11.14, P=0.005), CD4+CD25+CD127− proportion was significantly decreased (CD4+CD25+CD127−: OR =−1.72, 95% CI =−2.15 to −1.28, P<0.00001), whereas the proportions of CD4+, CD8+ and CD3+CD56+ and the CD4+/CD8+ ratio did not show much differences (CD4+: OR =2.93, 95% CI =−2.42 to 8.29, P=0.28; CD8+: OR =2.00, 95% CI =−4.11 to 8.11, P=0.52; CD4+/CD8+: OR =−0.01, 95% CI =−0.53 to 0.51, P=0.97; CD3+CD56+: OR =6.24, 95% CI =−2.48 to 14.97, P=0.16).
 | Figure 5 Forest plot of immunophenotype assessment before and after treatment with CIK/DC-CIK. |
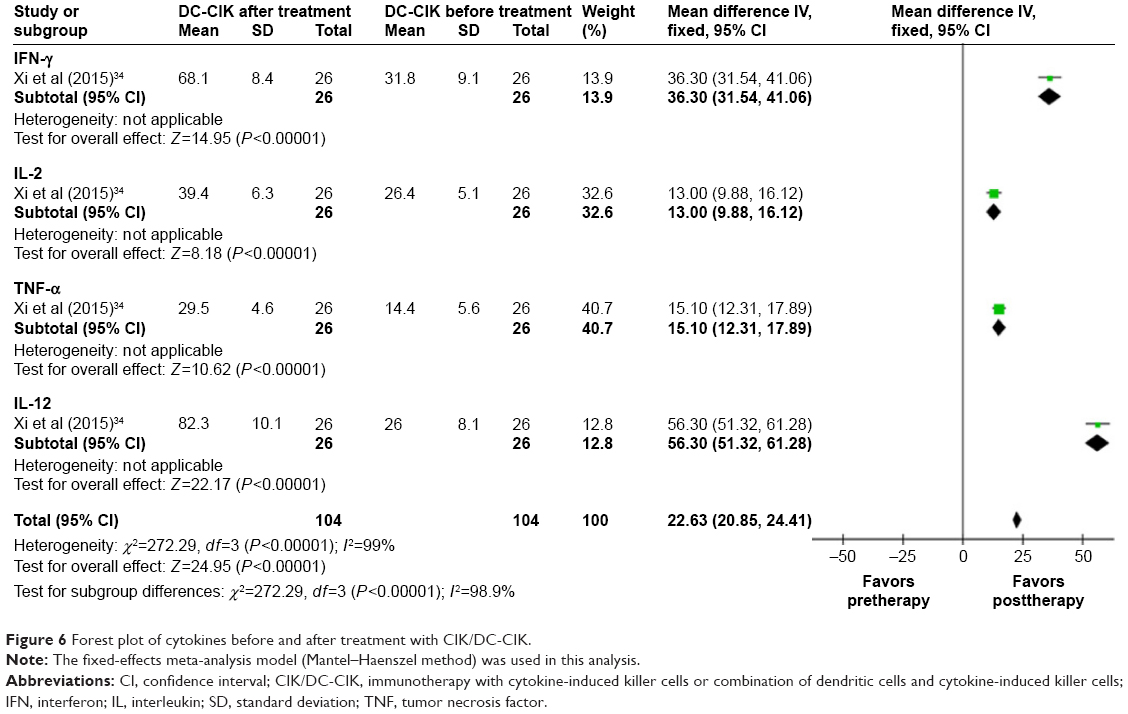
On the other hand, patients’ cytokines levels were also significantly increased after CIK/DC-CIK therapy (Figure 6, IFN-γ: OR =36.30, 95% CI =31.54-41.06, P<0.00001; IL-2: OR =13.00, 95% CI =9.88-16.12, P<0.00001; TNF-α: OR =15.10, 95% CI =12.31-17.89, P<0.00001; IL-12: OR =56.30, 95% CI =51.32-61.28, P<0.00001).
 | Figure 6 Forest plot of cytokines before and after treatment with CIK/DC-CIK. |
Assessment of adverse events
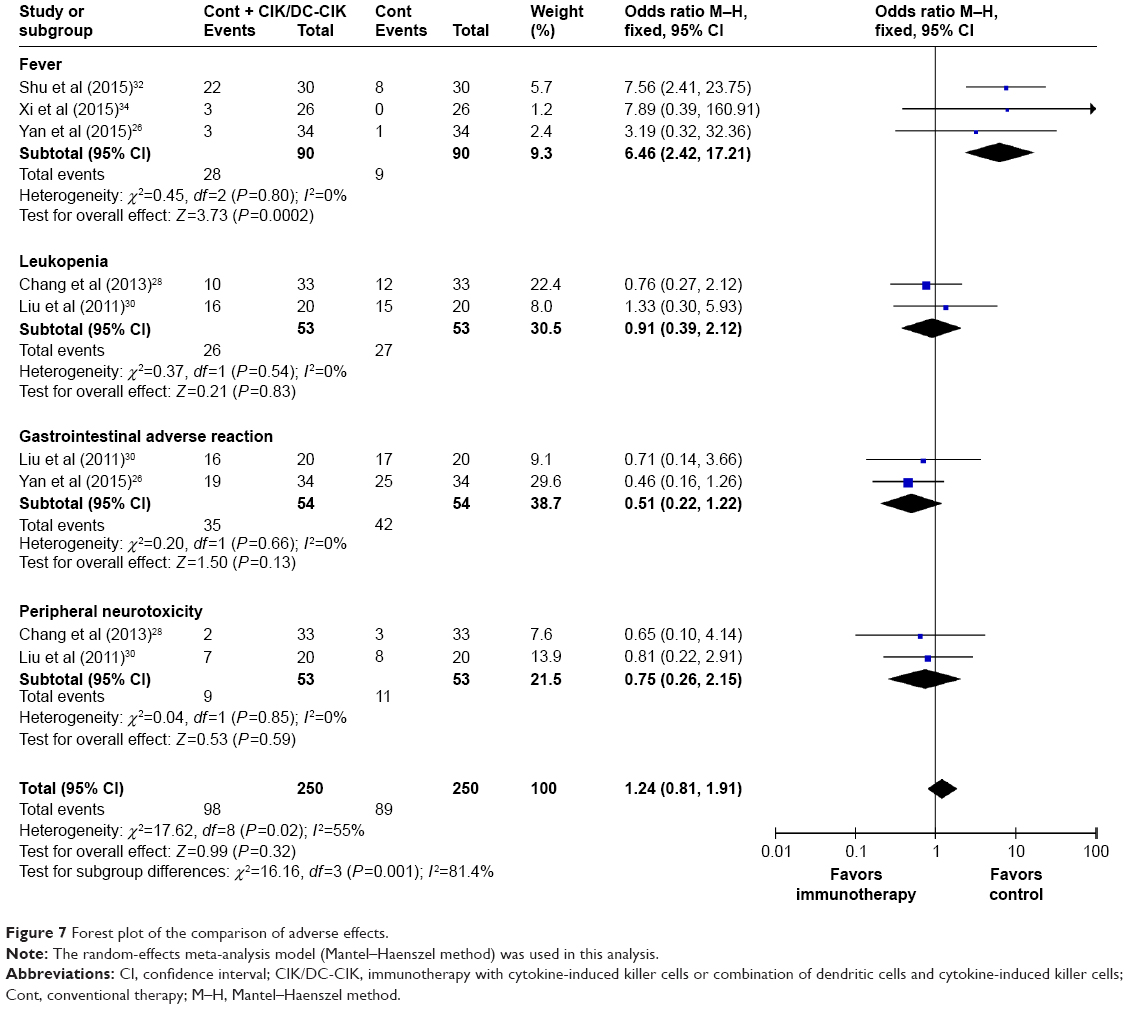
The safety of CIK/DC-CIK therapy in the treatment of EC was evaluated in this meta-analysis. As shown in Figure 7, no serious adverse events or death occurrence was reported in the involved literature. The most common side effect was fever, which subsided naturally within 24 hours. Except the higher incidence of fever in the combination therapy group than in the conventional therapy group (fever: OR =6.46, 95% CI =2.42–17.21, P=0.0002), no significant difference was observed in terms of leukopenia, gastrointestinal adverse reaction and peripheral neurotoxicity (leukopenia: OR =0.91, 95% CI =0.39–2.12, P=0.83; gastrointestinal adverse reaction: OR =0.51, 95% CI =0.22–1.22, P=0.13; peripheral neurotoxicity: OR =0.75, 95% CI =0.26–2.15, P=0.59).
 | Figure 7 Forest plot of the comparison of adverse effects. |
Discussion
Clinical trials have been conducted on CIK/DC-CIK immunotherapy for the treatment of EC.26,31 In this study, we performed an extensive online search, followed by rigorous meta-analysis, in order to evaluate its therapeutic efficacy and safety. Our meta-analysis revealed that the combination of CIK/DC-CIK immunotherapy and conventional therapy was a safe and effective regimen for the treatment of EC. Compared to conventional regimens alone, patients with combination therapy demonstrated higher OS rate, ORR and DCR, as well as improved immune function and QoL.
This study confirmed the safety of CIK/DC-CIK immunotherapy for EC patients, and the adverse events caused were tolerated by all patients. Fever was the most common side effect when patients were treated with combination conventional-plus-CIK/DC-CIK therapy, and its incidence was higher than when treated by conventional therapy alone (P<0.05). No significant difference was observed in terms of other adverse events, such as leukopenia, gastrointestinal adverse reaction and peripheral neurotoxicity between the 2 groups (P>0.05). CIK/DC-CIK immunotherapy enhanced the efficiency of conventional therapy in the treatment of EC. Compared with the conventional therapy-alone group, 1-year OS, ORR and DCR of patients in the combination therapy group were improved remarkably (P<0.01). Moreover, the combination therapy improved patients’ QoL (P<0.05) by relieving pain, reducing fatigue and insomnia as well as improving appetite.
Health status is closely related to human immune function, and a healthy human body has a robust immune system to detect and kill cancer cells.5,6 However, the immune function in cancer patients is compromised, and the percentage of T-lymphocyte subsets in the peripheral blood is usually disordered.5,6 Immune system reconstruction is one of the key factors to effectively treat malignant tumors.6 The antitumor activity of CIK/DC-CIK is mainly attributed to CD3−CD56+ and CD3+CD56+ cells.41 Our analysis indicated that the proportions of CD3+, CD3−CD56+ and CD3+CD56+ T cells were increased after CIK/DC-CIK treatment, although the percentages of CD3+CD56+ T cells did not reach statistical significance. However, no significant differences were found in the percentages of CD4+, CD8+ and CD4+/CD8+ ratios before and after immunotherapy. This may be caused by the different time points when the T-lymphocyte subsets were tested in these trials.6,19,42,43 Our analysis revealed a decreased proportion of CD4+CD25+ CD127− Tregs. This is consistent with a previous study that illustrated a negative role of Tregs in the implementation of CIK’s antitumor activity.44 Besides, the balance between the 2 helper T-cell (Th1 and Th2 cells) classes is also important in immunotherapy.5,41 Th1 cells enhance killer cells’ cytotoxicity and trigger delayed-type hypersensitivity, whereas Th2 cells are associated with tumor immune escape.5,45 Our analysis showed that after CIK/DC-CIK immunotherapy, the levels of Th1 cytokines, including IFN-γ, IL-2, TNF-α and IL-12, were significantly increased (P<0.00001), indicating a strong association between Th1 cytokines and efficacy of CIK/DC-CIK immunotherapy. Although our results indicated that CIK/DC-CIK immunotherapy enhanced the immune function in EC patients, the exact underlying mechanism of action of CIK/DC-CIK immunotherapy on hosts’ immune system remains unclear, which requires further studies on its mechanism.
This meta-analysis has some limitations. First of all, although CIK/DC-CIK immunotherapy has been applied to treat malignancies worldwide for its outstanding curative effects,46–48 all of the clinic trials that met our inclusion criteria were carried out in the Chinese population. We will follow updated publications on CIK/DC-CIK immunotherapy for EC conducted both in China and other countries and subsequently perform further systematic research on it. Moreover, the analysis performed in this study was not subjected to an open external evaluation procedure, which may lead to an overestimation of treatment effects. In addition, insufficient information regarding some patients, small sample sizes and other variables may have introduced bias into our conclusions. Besides, the clinical application of adoptive CIK/DC-CIK immunotherapy was limited due to the low specificity, although it is a promising strategy for the treatment of malignant tumors. Many new methods of immunotherapy, such as chimeric antigen receptor-modified T cells and T-cell receptor-modified T cells, have been developed currently,49–51 limiting the importance of this study.
Conclusion
Taken together, this meta-analysis suggests that the combination of CIK/DC-CIK immunotherapy and conventional regimens is safe and effective in treating patients with EC, with markedly prolonged survival time, enhanced immune function and improved therapeutic efficacy. Considering the limitations of our research, further analysis on studies conducted in countries other than China with larger sample sizes and going through open external evaluation procedure will be valuable to verify the credibility of our conclusions.
Acknowledgment
This research work was supported by grants from the Natural Science Foundation of Shandong (No 2015ZRA15027 to Changhui Zhou), National Natural Science Foundation of China (No 81600087 to Shaoda Ren), Natural Science Foundation of Shandong (No ZR2016HB45 to Shaoda Ren), Medical Science Foundation of Shandong (No 2014WS0300 to Weihua Wang) and Wu Jieping Medical Foundation (No 320.6750.15043 to Weihua Wang).
Author contributions
Changhui Zhou and Yingxin Zhang conceived and designed the experiments. Yan Liu, Ying Mu and Shaoda Ren performed the experiments. Weihua Wang and Jiaping Xie analyzed the data. Yan Liu and Ying Mu drafted the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Lv L, Hu W, Ren Y, Wei X. Minimally invasive esophagectomy versus open esophagectomy for esophageal cancer: a meta-analysis. Onco Targets Ther. 2016;9:6751–6762. | ||
Visser E, Franken IA, Brosens LA, Ruurda JP, van Hillegersberg R. Prognostic gene expression profiling in esophageal cancer: a systematic review. Oncotarget. 2017;8(3):5566–5577. | ||
Mannath J, Ragunath K. Role of endoscopy in early oesophageal cancer. Nat Rev Gastroenterol Hepatol. 2016;13(12):720–730. | ||
Goode EF, Smyth EC. Immunotherapy for gastroesophageal cancer. J Clin Med. 2016;5(10):84. | ||
Mu Y, Zhou CH, Chen SF, et al. Effectiveness and safety of chemotherapy combined with cytokine-induced killer cell/dendritic cell-cytokine-induced killer cell therapy for treatment of gastric cancer in China: a systematic review and meta-analysis. Cytotherapy. 2016;18(9):1162–1177. | ||
Zhou CL, Liu DL, Li J, et al. Chemotherapy plus dendritic cells co-cultured with cytokine-induced killer cells versus chemotherapy alone to treat advanced non-small-cell lung cancer: a meta-analysis. Oncotarget. 2016;7(52):86500–86510. | ||
Si Y, Deng Z, Lan G, et al. The safety and immunological effects of rAd5-EBV-LMP2 vaccine in nasopharyngeal carcinoma patients: a phase I clinical trial and two-year follow-up. Chem Pharm Bull (Tokyo). 2016;64(8):1118–1123. | ||
Passalacqua R, Caminiti C, Buti S, et al. Adjuvant low-dose interleukin-2 (IL-2) plus interferon-alpha (IFN-alpha) in operable renal cell carcinoma (RCC): a phase III, randomized, multicentre trial of the Italian Oncology Group for Clinical Research (GOIRC). J Immunother. 2014;37(9):440–447. | ||
Zhang T, Xie J, Arai S, et al. The efficacy and safety of anti-PD-1/PD-L1 antibodies for treatment of advanced or refractory cancers: a meta-analysis. Oncotarget. 2016;7(45):73068–73079. | ||
Weber JS, D’Angelo SP, Minor D, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16(4):375–384. | ||
Li J, Qin S, Xu J, et al. Randomized, double-blind, placebo-controlled phase III trial of apatinib in patients with chemotherapy-refractory advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction. J Clin Oncol. 2016;34(13):1448–1454. | ||
Boye M, Wang X, Srimuninnimit V, et al. First-line pemetrexed plus cisplatin followed by gefitinib maintenance therapy versus gefitinib monotherapy in East Asian never-smoker patients with locally advanced or metastatic nonsquamous non-small-cell lung cancer: quality of life results from a randomized phase III trial. Clin Lung Cancer. 2016;17(2):150–160. | ||
Stanculeanu DL, Daniela Z, Lazescu A, Bunghez R, Anghel R. Development of new immunotherapy treatments in different cancer types. J Med Life. 2016;9(3):240–248. | ||
Peoples GE, Gurney JM, Hueman MT, et al. Clinical trial results of a HER2/neu (E75) vaccine to prevent recurrence in high-risk breast cancer patients. J Clin Oncol. 2005;23(30):7536–7545. | ||
Dudley ME, Gross CA, Somerville RP, et al. Randomized selection design trial evaluating CD8+-enriched versus unselected tumor-infiltrating lymphocytes for adoptive cell therapy for patients with melanoma. J Clin Oncol. 2013;31(17):2152–2159. | ||
Zhao Z, Liao H, Ju Y. Effect of compound Kushen injection on T-cell subgroups and natural killer cells in patients with locally advanced non-small-cell lung cancer treated with concomitant radiochemotherapy. J Tradit Chin Med. 2016;36(1):14–18. | ||
Chia WK, Teo M, Wang WW, et al. Adoptive T-cell transfer and chemotherapy in the first-line treatment of metastatic and/or locally recurrent nasopharyngeal carcinoma. Mol Ther. 2014;22(1):132–139. | ||
Jäkel CE, Vogt A, Gonzalez-Carmona MA, Schmidt-Wolf IGH. Clinical studies applying cytokine-induced killer cells for the treatment of gastrointestinal tumors. J Immunol Res. 2014;2014:1–12. | ||
Shi LR, Zhou Q, Wu J, et al. Efficacy of adjuvant immunotherapy with cytokine-induced killer cells in patients with locally advanced gastric cancer. Cancer Immunol Immunother. 2012;61(12):2251–2259. | ||
Li GX, Zhao SS, Zhang XG, et al. Comparison of the proliferation, cytotoxic activity and cytokine secretion function of cascade primed immune cells and cytokine-induced killer cells in vitro. Mol Med Rep. 2015;12(2):2629–2635. | ||
Mehta BA, Schmidt-Wolf IG, Weissman IL, Negrin RS. Two pathways of exocytosis of cytoplasmic granule contents and target cell killing by cytokine-induced CD3+ CD56+ killer cells. Blood. 1995;86(9):3493–3499. | ||
Zhu Y, Zhang H, Li Y, et al. Efficacy of postoperative adjuvant transfusion of cytokine-induced killer cells combined with chemotherapy in patients with colorectal cancer. Cancer Immunol Immunother. 2013;62(10):1629–1635. | ||
Wei XC, Yang DD, Han XR, et al. Bioactivity of umbilical cord blood dendritic cells and anti-leukemia effect. Int J Clin Exp Med. 2015;8(10):19725–19730. | ||
Li H, Ren XB, Zhang P, An XM, Liu H, Hao XS. 树突状细胞对CIK细胞中CD4+CD25+ T细胞数量及免疫调节作用的影响 [Dendritic cells reduce the number and function of CD4+CD25+ cells in cytokine-induced killer cells]. Zhonghua Yi Xue Za Zhi. 2005;85(44):3134–3138. | ||
Gao DQ, Li CY, Xie XH, et al. Autologous tumor lysate-pulsed dendritic cell immunotherapy with cytokine-induced killer cells improves survival in gastric and colorectal cancer patients. PLoS One. 2014;9(4):e93886. | ||
Yan L, Wu M, Ba N, et al. Efficacy of dendritic cell-cytokine-induced killer immunotherapy plus intensity-modulated radiation therapy in treating elderly patients with esophageal carcinoma. Genet Mol Res. 2015;14(1):898–905. | ||
Zhang Z, Wang LP, Luo ZZ, et al. Efficacy and safety of cord blood-derived cytokine-induced killer cells in treatment of patients with malignancies. Cytotherapy. 2015;17(8):1130–1138. | ||
Chang ZG, Xu QX, Ma L, He LM. Clinical observation of cytokine induced killer cell intravenous transfusion combined with chemotherapy in treatment of advanced esophageal cancer. Shandong Med J. 2013;53(23):53–54. | ||
Hu YQ. Effect of herb plus adoptive immunotherapy with cytokine induced killer cells on cellular immunity of patients with advanced esophageal carcinoma. J Bengbu Med Coll. 2012;37(9):1062–1066. | ||
Liu GJ, Mei JZ, Xiao P, Li RJ, Li M. Efficacy of chemotherapy combined with cytokine-induced killer cells in the treatment of advanced esophageal carcinoma. J Zhengzhou Univ. 2011;46(2):169–173. | ||
Qu WF, Zhang WM, Ding XY. IL-12 induced CIK cells combined with chemotherapy improve immune function and efficacy in patients with esophageal carcinoma. Shi Jie Hua Ren Xiao Hua Za Zhi. 2015;23(28):4553–4557. | ||
Shu X, Li GX, Zhu XL, Li G, Gan Q, Wang ZY. Autologous cytokine-induced killer cells combined with chemoradiation in the treatment of locally advanced esophageal carcinoma: a randomized control study. Mod Oncol. 2015;23(10):1376–1380. | ||
Wang H, Shu W, Mao GH, Zhang YJ, Shi TL. Effect of dendritic cell-cytokine-induced killer cell adoptive immunotherapy combined with chemotherapy on T cell subsets of patients with esophageal cancer. Contemp Med. 2014;20(28):1–3. | ||
Xi XX, Lv BH, Ye T, Chen R, Xu X. Effect of DC-CIK cells’ biotherapy in comprehensive therapy of esophagus cancer: a randomized controlled trial. Chin J Clin Thorac Cardiovasc Surg. 2015;22(8):765–769. | ||
Xu BL, Gao QL, Fan RH, Liu X, Guo JD, Zhang CJ. Clinical effects on chemotherapy combined with CIK for patients with advanced oesophageal carcinoma. Henan Med Res. 2010;19(3):315–320. | ||
Yang B, Li W, Sun XA, Chen YM. The clinical efficacy of endoscopic implantation with chemotherapeutic slow-release combined with DC-CIK immune cells infusion for patients with obstructive esophageal cancers. China J Endoscopy. 2015;21(5):483–486. | ||
Zhu HP, Zhang QA. Analysis of the effect of injection in treatment of advanced esophageal cancer paclitaxel cisplatin regimen combined with autologous CIK cells. Chin J Clin Oncol Rehabil. 2014;21(7):837–839. | ||
Zeng X, Zhang Y, Kwong JS, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. J Evid Based Med. 2015;8(1):2–10. | ||
Han RX, Liu X, Pan P, Jia YJ, Yu JC. Effectiveness and safety of chemotherapy combined with dendritic cells co-cultured with cytokine-induced killer cells in the treatment of advanced non-small-cell lung cancer: a systematic review and meta-analysis. PLoS One. 2014;9(9):e108958. | ||
Jackson D, White IR, Riley RD. Quantifying the impact of between-study heterogeneity in multivariate meta-analyses. Stat Med. 2012;31(29):3805–3820. | ||
Wang ZX, Cao JX, Wang M, et al. Adoptive cellular immunotherapy for the treatment of patients with breast cancer: a meta-analysis. Cytotherapy. 2014;16(7):934–945. | ||
Milasiene V, Stratilatovas E, Norkiene V. The importance of T-lymphocyte subsets on overall survival of colorectal and gastric cancer patients. Medicina (Kaunas). 2007;43(7):548–554. | ||
Cho MY, Joh YG, Kim NR, et al. T-lymphocyte subsets in patients with AJCC stage III gastric cancer during postoperative adjuvant chemotherapy. American Joint Committee on Cancer. Scand J Surg. 2002;91(2):172–177. | ||
Tao Q, Wang H, Zhai Z. Targeting regulatory T cells in cytokine-induced killer cell cultures (Review). Biomed Rep. 2014;2(3):317–320. | ||
Mu Y, Wang WH, Xie JP, Zhang YX, Yang YP, Zhou CH. Efficacy and safety of cord blood-derived dendritic cells plus cytokine-induced killer cells combined with chemotherapy in the treatment of patients with advanced gastric cancer: a randomized Phase II study. Onco Targets Ther. 2016;9:4617–4627. | ||
Olioso P, Giancola R, Di Riti M, Contento A, Accorsi P, Iacone A. Immunotherapy with cytokine induced killer cells in solid and hematopoietic tumours: a pilot clinical trial. Hematol Oncol. 2009;27(3):130–139. | ||
Lee JH, Lim YS, Lim YS, et al. Adjuvant immunotherapy with autologous cytokine-induced killer cells for hepatocellular carcinoma. Gastroenterology. 2015;148(7):1383.e6–1391.e6. | ||
Introna M, Pievani A, Borleri G, et al. Feasibility and safety of adoptive immunotherapy with CIK cells after cord blood transplantation. Biol Blood Marrow Transplant. 2010;16(11):1603–1607. | ||
Ma Y, Zhang Z, Tang L, et al. Cytokine-induced killer cells in the treatment of patients with solid carcinomas: a systematic review and pooled analysis. Cytotherapy. 2012;14(4):483–493. | ||
Zhang T, Cao L, Xie J, et al. Efficiency of CD19 chimeric antigen receptor-modified T cells for treatment of B cell malignancies in phase I clinical trials: a meta-analysis. Oncotarget. 2015;6(32):33961–33971. | ||
Katz SC, Burga RA, McCormack E, et al. Phase I hepatic immunotherapy for metastases study of intra-arterial chimeric antigen receptor-modified T-cell therapy for CEA+ liver metastases. Clin Cancer Res. 2015;21(14):3149–3159. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.