Back to Journals » Cancer Management and Research » Volume 18

Cytokeratin-Positive Pleomorphic Chest Wall Sarcoma Mimicking MPNST: A Case Report
Authors Aldakak MA ![]() , Nasra AB
, Nasra AB ![]() , Ahmad R, Alhallaq H, Assoud K, Chaban H
, Ahmad R, Alhallaq H, Assoud K, Chaban H
Received 2 March 2026
Accepted for publication 27 May 2026
Published 3 June 2026 Volume 2026:18 606289
DOI https://doi.org/10.2147/CMAR.S606289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Mohammad Alaa Aldakak,1 Ahmad Bishr Nasra,1 Raneem Ahmad,2 Hamza Alhallaq,2 Kinda Assoud,2 Hussain Chaban2
1Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic; 2National University Hospital, Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic
Correspondence: Mohammad Alaa Aldakak, Email [email protected]
Background: Undifferentiated pleomorphic sarcoma (UPS) is an uncommon high-grade soft-tissue sarcoma and remains a diagnosis of exclusion because it lacks specific differentiation and pathognomonic markers. Primary chest-wall involvement is rare, and epithelial-marker expression may complicate diagnosis by broadening the differential diagnosis.
Case Presentation: A 62-year-old male carpenter and active smoker with diabetes mellitus and ischemic heart disease presented with persistent right-sided chest pain radiating to the back. Examination revealed a firm right anterolateral chest-wall mass fixed to the deep plane. Chest radiography suggested a chest-wall origin, and contrast-enhanced computed tomography demonstrated an extrapleural, lentiform mass displacing the adjacent lung without clear parenchymal invasion. CT-guided core biopsy suggested malignant peripheral nerve sheath tumor.
Case Discussion: The patient underwent en bloc resection of the mass, including anterior portions of ribs 3– 5 and involved serratus anterior muscle, followed by reconstruction using a polypropylene mesh underlay and orthogonally arranged metallic plates. Histopathology showed a malignant spindle-to-epithelioid pleomorphic neoplasm infiltrating skeletal muscle and encasing trabecular rib bone. Immunohistochemistry demonstrated diffuse vimentin and cytokeratin positivity, mild EMA expression, S100 and myogenin negativity, and focal desmin, actin, and CD68 positivity. Correlating morphology with the available immunoprofile, the resection specimen was most consistent with cytokeratin-positive UPS. The anterior margin was involved, while other margins were free.
Conclusion: This case highlights diagnostic pitfalls in cytokeratin-positive pleomorphic chest-wall tumors and the limitations of core biopsy. En bloc resection with rigid reconstruction is feasible, while positive margin status warrants multidisciplinary consideration of adjuvant local therapy and structured surveillance.
Keywords: undifferentiated pleomorphic sarcoma, chest wall neoplasms, malignant peripheral nerve sheath tumor, immunohistochemistry, chest wall reconstruction
Introduction
Soft tissue sarcomas (STS) are uncommon mesenchymal malignancies, representing <1% of all malignant tumors, and most often arise in the extremities, followed by the trunk wall and retroperitoneum.1,2 Within the trunk wall, chest wall sarcomas are rare and clinically challenging because treatment planning depends on accurate assessment of tumor extent, adjacent structure involvement, and the anticipated need for full-thickness resection with reconstruction.3 Recommended initial workup for a suspicious chest wall soft-tissue mass includes cross-sectional imaging, with MRI playing a key role when feasible, followed by core needle biopsy to establish histology and guide staging and management.3,4
Undifferentiated pleomorphic sarcoma (UPS) is classified among undifferentiated sarcomas and remains a diagnosis of exclusion, defined by the absence of an identifiable line of differentiation after careful morphologic assessment and appropriate ancillary studies.5,6 Historically termed malignant fibrous histiocytoma, UPS lacks specific immunohistochemical or molecular markers, making the exclusion of important mimics, particularly poorly differentiated carcinoma, melanoma, and lineage-defined pleomorphic sarcomas, central to diagnosis.2,6 This diagnostic challenge may be amplified when epithelial markers such as cytokeratins are expressed, because keratin reactivity in a pleomorphic spindle-cell tumor can suggest carcinoma, mesothelioma, synovial sarcoma, epithelioid sarcoma, or other cytokeratin-positive sarcomatoid neoplasms rather than conventional UPS.6 Therefore, cytokeratin positivity should be interpreted cautiously and in correlation with tumor morphology, imaging findings, sampling adequacy, and a targeted exclusionary immunohistochemical workup.
Here, we report a large anterior chest wall pleomorphic malignancy initially interpreted as malignant peripheral nerve sheath tumor on core biopsy but ultimately favored as cytokeratin-positive UPS on the resection specimen. This case highlights the diagnostic complexity of pleomorphic chest-wall tumors with epithelial-marker expression, as well as the surgical and surveillance implications of en bloc rib resection and rigid chest-wall reconstruction.
Case Presentation
A 62-year-old male carpenter and active smoker of approximately 30 pack-years, with type 2 diabetes mellitus and ischemic heart disease, presented with several months of persistent right-sided chest pain radiating to the back and unresponsive to analgesics. He denied fever, weight loss, cough, dyspnea, hemoptysis, syncope, palpitations, neurologic symptoms, or gastrointestinal complaints. His medications included aspirin 162 mg daily, clopidogrel 75 mg daily, atorvastatin, and bisoprolol. Approximately one year earlier, he had undergone percutaneous coronary intervention with coronary stent placement.
On examination, his vital signs were stable: blood pressure 130/70 mmHg, heart rate 75 beats per minute, temperature 37 °C, and oxygen saturation 95% on room air. A firm right anterolateral chest-wall mass was palpable, fixed to the deep plane, and extending approximately from the third to the fifth rib levels. The overlying skin was mobile and non-inflamed. The remainder of the physical examination was unremarkable. Baseline electrocardiography was normal. Transthoracic echocardiography showed a left ventricular ejection fraction of approximately 50%, with normal wall motion and no significant valvular disease.
A frontal chest radiograph showed a right lateral hemithoracic extrapleural-type opacity with smooth convex margins and obtuse pleuroparietal angles, suggesting a chest-wall origin (Figure 1). Contrast-enhanced computed tomography confirmed a right anterolateral chest-wall soft-tissue mass with an extrapleural, lentiform configuration forming obtuse pleuroparietal angles. The lesion abutted the parietal pleura and displaced the adjacent lung without clear parenchymal invasion, extending across at least one intercostal space. On imaging, it measured approximately 10×4 × 3 cm (craniocaudal × mediolateral × anteroposterior) (Figure 2A–C). No pleural effusion was identified. CT-guided core biopsy was reported as a malignant spindle-cell sarcoma suggestive of malignant peripheral nerve sheath tumor.
 |
Figure 1 Frontal chest radiograph demonstrating a right lateral hemithoracic extrapleural-type opacity with smooth convex margins and obtuse pleuroparietal angles, suggesting a chest-wall origin. |
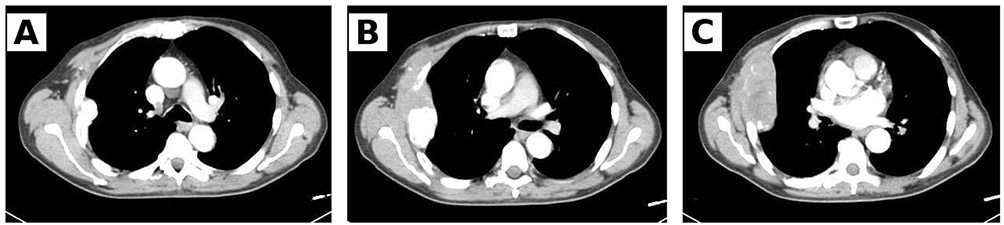 |
Figure 2 (A–C) Contrast-enhanced chest CT showing a right anterolateral extrapleural chest-wall mass with lentiform configuration and obtuse pleuroparietal angles. The lesion abuts the parietal pleura and displaces the adjacent lung without definite pulmonary parenchymal invasion. |
The patient subsequently underwent en bloc resection of the chest-wall mass, including the infiltrated anterior portions of ribs 3 to 5 and the involved segment of the serratus anterior muscle. Chest-wall reconstruction was performed using a polypropylene mesh underlay and two metallic plates arranged orthogonally and anchored to the residual ribs to restore chest-wall rigidity (Figure 3A and B). The gross en bloc resection specimen measured 17×9 × 7.5 cm; the rib-containing component measured 17×7 × 7 cm, and the muscular component measured 10×9 × 3 cm. Sectioning revealed a firm mass measuring 12×6 × 4.7 cm with a homogeneous white solid nodular cut surface. A gross photograph of the en bloc specimen is shown in Figure 3C. Early postoperative chest radiography demonstrated expected postoperative changes, with a right thoracic drain in situ, mild right basilar atelectasis, and no pneumothorax (Figure 4).
 |
Figure 3 (A–C) Intraoperative and gross surgical findings. (A) En bloc chest-wall resection including involved ribs. (B) Chest-wall reconstruction using polypropylene mesh and orthogonally positioned metallic plates. (C) Gross appearance of the resected specimen. |
 |
Figure 4 Early postoperative chest radiograph demonstrating expected postoperative changes with right thoracic drain in situ, mild right basilar atelectatic changes, and no pneumothorax. |
Definitive histopathology demonstrated a malignant spindle-to-epithelioid neoplasm composed of cells with eosinophilic cytoplasm, large vesicular nuclei, prominent nucleoli, rare giant cells, and mitotic activity. The tumor infiltrated skeletal muscle fibers and encased/invaded trabecular rib bone, confirming combined muscular and osseous involvement (Figure 5A–C). Immunohistochemistry showed diffuse cytokeratin and vimentin positivity, negative S100 and myogenin staining, mild focal desmin and actin positivity, focal CD68 positivity, and mild EMA expression. The illustrated immunohistochemical stains demonstrated diffuse cytokeratin positivity, negative S100 and myogenin staining, focal desmin positivity, and mild EMA expression (Figures 6A–Figure 6D and Figure 7A–Figure 7D). Correlating the morphology with the immunohistochemical profile, the core biopsy impression initially favored malignant peripheral nerve sheath tumor; however, evaluation of the larger resection specimen ultimately supported cytokeratin-positive undifferentiated pleomorphic sarcoma as the final diagnosis after exclusion of other lineage-specific pleomorphic neoplasms. The anterior surgical margin was involved by tumor, while all other submitted residual surgical margins were free.
 |
Figure 5 (A–C) Histopathologic examination of the resected tumor. (A) Tumor infiltration involving adjacent trabecular rib bone. (B) Spindle-cell proliferation arranged in intersecting fascicles. (C) High-power view demonstrating marked pleomorphism, enlarged vesicular nuclei, prominent nucleoli, and mitotic activity. |
 |
Figure 6 (A–D) Immunohistochemical profile of the tumor. (A) Diffuse cytokeratin positivity in tumor cells. (B) Negative S100 staining. (C) Negative myogenin staining. (D) Mild focal desmin positivity. |
 |
Figure 7 (A–D) Additional immunohistochemical evaluation of the pleomorphic chest-wall neoplasm. (A, C and D) Cytokeratin staining demonstrating diffuse tumor-cell positivity. (B) Mild epithelial membrane antigen (EMA) positivity. The combined morphologic and immunohistochemical findings supported the diagnosis of cytokeratin-positive undifferentiated pleomorphic sarcoma after exclusion of other lineage-specific pleomorphic neoplasms. |
Standard sarcoma surveillance was planned with clinical review and chest imaging every 3 to 6 months for the first 2 to 3 years, then every 6 months until year 5, and annually thereafter. Imaging of the primary site was planned as clinically indicated, with particular attention to the reconstructed chest wall.
Discussion
Undifferentiated pleomorphic sarcoma (UPS), historically reported under the rubric of malignant fibrous histiocytoma (MFH), is an aggressive soft-tissue sarcoma entity that has been described as accounting for roughly 15% of soft-tissue sarcomas with an overall 5-year survival around 60%, while being far more common in the extremities than in the trunk or chest wall.7,8 Because UPS lacks a defining line of differentiation and specific ancillary markers, several reports emphasize that it is often reached by clinicopathologic exclusion after other pleomorphic malignancies have been ruled out.7,9 Within the chest wall, published cases describe presentations dominated by localized pain, a palpable mass, or respiratory symptoms such as dyspnea when the lesion projects intrathoracically.8,10 Plain radiography can provide an early anatomic clue, as chest-wall tumors may produce an “extrapleural sign” with smooth convexity and obtuse pleuroparietal angles, which was explicitly highlighted in an elderly chest-wall MFH case.10 Cross-sectional imaging in reported chest-wall pleomorphic sarcomas typically demonstrates a soft-tissue mass arising from the thoracic wall with variable enhancement and, in several cases, associated rib involvement or lysis that supports a full-thickness resection strategy.8,10,11 Despite modern imaging, diagnostic uncertainty is common, and multiple papers illustrate that limited tissue sampling may misclassify pleomorphic tumors or even yield non-diagnostic material, including initial interpretations as sarcomatoid pleural mesothelioma, melanoma, benign nodular fasciitis, or inflammatory/necrotic debris.12–15 These pitfalls are clinically relevant because management hinges on histology, yet the literature repeatedly shows that resection specimens can clarify or overturn biopsy impressions once broader morphology and immunohistochemistry are available.12,13
Histologically, chest-wall MFH/UPS cases describe high-grade pleomorphic spindle-cell proliferations, sometimes with storiform-pleomorphic architecture, frequent mitoses, necrosis, and invasion of adjacent skeletal muscle and rib cortex/trabeculae.8,9,11,16 Immunohistochemical profiles across reports are dominated by vimentin positivity with broad negativity for lineage-specific markers, while focal expression of myoid or histiocytic markers (eg, SMA, desmin, CD68) may be seen and should be interpreted in the context of morphology.14,15,17 A key diagnostic nuance for our case is that epithelial-marker reactivity does not exclude UPS, as focal cytokeratin expression was documented in advanced UPS reports, but these authors stress the need to exclude sarcomatoid carcinoma, mesothelioma, and other mimics using targeted panels (eg, calretinin/ERG/SOX10) and, when relevant, molecular tests such as MDM2 FISH.9,17,18 From a molecular standpoint, UPS is generally characterized by complex genomic alterations rather than a single defining recurrent mutation. Reported alterations frequently involve pathways related to cell-cycle regulation, tumor suppression, chromosomal instability, and copy-number changes, which supports its classification as a genetically complex sarcoma rather than a molecularly defined entity. Therefore, in routine practice, molecular testing is most useful for excluding specific mimics, such as dedifferentiated liposarcoma or synovial sarcoma, rather than confirming UPS itself.
Across the chest-wall literature, the cornerstone of potentially curative therapy is wide en bloc surgical excision, frequently including resection of involved ribs and adjacent soft tissues, followed by immediate reconstruction to restore stability and protect intrathoracic organs.7,8,11 Reconstructive strategies reported for large defects include prosthetic mesh (eg, Marlar/Marlex-type materials) sometimes combined with rigid support or soft-tissue coverage using muscle flaps, achieving acceptable early postoperative recovery and, in selected patients, durable local control.8,11,19 Margin status remains a recurrent theme, with the chest-wall systematic review suggesting that a margin distance on the order of 1.5 cm is likely sufficient to prevent recurrence in reported cases, while individual reports describe intentional wider “safety margins” (eg, ~4 cm) when feasible.7,11 When margins are close or microscopically positive, authors report adjuvant radiotherapy as a commonly used strategy and the systematic review notes improved relapse-free survival in patients receiving radiotherapy in some form, including in contexts where further radical resection would be morbid.4,7,11 For unresectable, metastatic, or high-risk disease, systemic therapy experiences in these files include anthracycline-based regimens (doxorubicin ± ifosfamide), and selected cases highlight responses to multimodality approaches incorporating radiotherapy or, in molecularly characterized tumors, targeted therapy such as pazopanib.9,13,17,18 The emerging role of immunotherapy is illustrated by reports in which checkpoint inhibitors preceded dramatic shrinkage or enabled salvage resection in UPS, although these observations are framed as exceptional responses rather than established standards.12,13 Prognosis in UPS appears heterogeneous across sites and clinical contexts, ranging from rapid progression and early mortality in elderly or critically located tumors to long-term disease-free survival after wide chest-wall resection with reconstruction and adjuvant radiotherapy.10–12,16
In the present case, the extrapleural radiographic configuration, chest-wall origin on CT, and need for en bloc resection with rib removal and prosthetic reconstruction align closely with prior chest-wall MFH/UPS experiences, while the initial core-biopsy suggestion of MPNST mirrors the broader literature showing that pleomorphic sarcomas may be misclassified on limited sampling.8,10,12,13 The combination of vimentin positivity, S100 and myogenin negativity, focal myoid/histiocytic staining, diffuse cytokeratin positivity, and mild EMA expression in our resection specimen underscores the importance of a structured exclusionary workup in cytokeratin-positive pleomorphic tumors. We acknowledge that an expanded immunohistochemical and molecular panel, including markers such as SOX10, H3K27me3, INI1, calretinin, ERG, and MDM2 testing, would have further strengthened exclusion of additional mimics; however, these tests were not locally available. Based on the available morphology and immunohistochemical profile, the tumor was considered most consistent with cytokeratin-positive UPS. Given the involved anterior margin, multidisciplinary consideration of adjuvant local therapy and close surveillance was recommended.
Conclusion
Chest wall undifferentiated pleomorphic sarcoma is a rare, aggressive malignancy that may present with nonspecific symptoms, and an extrapleural configuration on initial imaging can suggest a chest-wall origin. Accurate preoperative assessment is essential because definitive management often requires full-thickness en bloc resection with planned reconstruction to restore chest-wall stability. Diagnostically, UPS remains a diagnosis of exclusion, and limited core biopsy may be misleading in pleomorphic tumors, particularly when epithelial-marker reactivity is present. Comprehensive evaluation of the resection specimen with clinicopathologic correlation is therefore critical to exclude mimics such as sarcomatoid carcinoma, mesothelioma, melanoma, and lineage-defined sarcomas. This case highlights the diagnostic complexity of cytokeratin-positive pleomorphic chest-wall tumors and demonstrates that radical resection with rigid reconstruction can be achieved safely in a medically comorbid patient. Given the involved anterior margin, close surveillance is warranted, and adjuvant local therapy should be considered through multidisciplinary discussion.
Data Sharing Statement
Data available on request from the authors.
Ethics Approval Statement
Institutional Review Board (IRB) of Faculty of Medicine, Damascus University approval is not required for de-identified single case reports or case histories, in accordance with institutional policies.
Patient Consent Statement
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Funding
There is no funding to report.
Disclosure
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
References
1. Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO classification of soft tissue tumours: news and perspectives. Pathologica. 2021;113(2):70–8. doi:10.32074/1591-951X-213
2. Mack T, Purgina B. Updates in pathology for retroperitoneal soft tissue sarcoma. Curr Oncol. 2022;29(9):6400–6418. doi:10.3390/curroncol29090504
3. van Roozendaal LM, Bosmans JWAM, Daemen JHT, et al. Management of soft tissue sarcomas of the chest wall: a comprehensive overview. J Thorac Dis. 2024;16(5):3484–3492. doi:10.21037/jtd-23-1149
4. de Juan Ferré A, Álvarez Álvarez R, Casado Herráez A, et al. SEOM clinical guideline of management of soft-tissue sarcoma (2020). Clin Transl Oncol. 2021;23(5):922–930. doi:10.1007/s12094-020-02534-0
5. Schaefer IM, Gronchi A. WHO pathology: highlights of the 2020 sarcoma update. Surg Oncol Clin N Am. 2022;31(3):321–340. doi:10.1016/j.soc.2022.03.001
6. Miettinen M. Immunohistochemistry of soft tissue tumours—review with emphasis on 10 markers. Histopathology. 2014;64(1):101–118. doi:10.1111/his.12298
7. Bennett C, Bharadwaj S, Arndt A, Chawla A. A systematic review of undifferentiated pleomorphic sarcoma of the chest wall. Chin Clin Oncol. 2023;12(6):66. doi:10.21037/cco-23-71
8. An JK, Oh KK. Malignant fibrous histiocytoma of chest wall. Yonsei Med J. 2005;46(1):177–180. doi:10.3349/ymj.2005.46.1.177
9. Till BM, Java A, King C, et al. Undifferentiated pleomorphic sarcoma of the thoracic aorta: a diagnostic and therapeutic challenge. Ann Thorac Surg Short Rep. 2023;1(2):279–281. doi:10.1016/j.atssr.2023.02.002
10. Makar AB, McMartin KE, Palese M, Tephly TR. Formate assay in body fluids: application in methanol poisoning. Biochem Med. 1975;13(2):117–126. doi:10.1016/0006-2944(75)90147-7
11. Shin JW, Chang YJ, Cho DG, Choi SY. Long-term survival after wide resection of malignant fibrous histiocytoma of the chest wall. Korean J Thorac Cardiovasc Surg. 2019;52(1):36–39. doi:10.5090/kjtcs.2019.52.1.36
12. Nakamura A, Kuroda A, Hashimoto M, et al. Salvage resection after immunotherapy for giant undifferentiated pleomorphic sarcoma of the chest wall. J Surg Case Rep. 2025;2025(10):rjaf747. doi:10.1093/jscr/rjaf747
13. Jeon WJ, Moon JH, Pham B, Joung B, Denham L, Brothers J. Case report: an exceptional response to neoadjuvant radiotherapy and chemotherapy in undifferentiated pleomorphic sarcoma following checkpoint inhibitor use. Front Oncol. 2023;13:1198292. doi:10.3389/fonc.2023.1198292
14. Kong J, Shahait AD, Kim S, Choi L. Radiation-induced undifferentiated pleomorphic sarcoma of the breast. BMJ Case Rep. 2020;13(2):e232616. doi:10.1136/bcr-2019-232616
15. Fang Z, Xia T, Pan S, et al. Esophageal carcinosarcoma comprising undifferentiated pleomorphic sarcoma and squamous cell carcinoma: a case report. J Cardiothorac Surg. 2022;17(1):210. doi:10.1186/s13019-022-01957-w
16. Mladenovic Z, Obradovic S, Ristic S, Djenic L, Begic E. A rare case of undifferentiated pleomorphic sarcoma with central necrosis in the right atrium. Turk Kardiyol Dern Ars. 2023;51(2):155–158. doi:10.5543/tkda.2022.97918
17. Matsuoka H, Yoshida KI, Nakai S, et al. Successful pazopanib treatment of undifferentiated pleomorphic sarcoma with coamplification of PDGFRA, VEGFR2 and KIT: a case report. Mol Clin Oncol. 2024;21(4):69. doi:10.3892/mco.2024.2767
18. Li H, Gong Q, Wei W. Undifferentiated pleomorphic sarcoma invading thoracic aorta treated by thoracic endovascular aortic repair: a case report. J Med Case Rep. 2025;19(1):268. doi:10.1186/s13256-025-05329-5
19. Aldakak MA, Al-Bitar A, Ahmad R, Alhallaq H, Assoud K, Chaban H. Primary chest wall Ewing sarcoma with diaphragmatic invasion in an adult: en-bloc resection and polypropylene mesh reconstruction. Clin Case Rep. 2026;14(1):e71824. doi:10.1002/ccr3.71824
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.