Back to Journals » OncoTargets and Therapy » Volume 9
Cytogenetic abnormality in patients with multiple myeloma analyzed by fluorescent in situ hybridization
Authors Hu Y, Chen W, Chen S, Huang Z
Received 5 September 2015
Accepted for publication 7 December 2015
Published 3 March 2016 Volume 2016:9 Pages 1145—1149
DOI https://doi.org/10.2147/OTT.S95818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Daniele Santini
Ying Hu, Wenming Chen, Shilun Chen, Zhongxia Huang
Department of Hematology, Beijing Chaoyang Hospital Affiliated to Capital Medical University, Beijing, People’s Republic of China
Objective: To analyze the fluorescent in situ hybridization (FISH) data and the association with clinical characteristics, therapy response, and survival time in patients with multiple myeloma.
Method: We performed a retrospective review of patients with multiple myeloma from November 2010 to April 2014.
Results: Cytogenetic abnormalities by FISH were detectable in 66% of patients. One cytogenetic abnormality, two cytogenetic abnormalities, and complex abnormalities were detectable in 21.2%, 51.5%, and 27.3% of cases, respectively. 1q21 amplification, t(4p16.3/14q32), and 17p deletion were observed in 69.7%, 30.3%, and 21.2% of cases, respectively. Total response rates (complete response [CR] + near CR + partial response) were 93.8% and 82.1%, respectively, in cytogenetic normality group and abnormality group. CR rates were 50% and 32.1%, respectively. Median overall survival (OS) time was 51 months and 24 months, respectively, in cytogenetic normality group and abnormality group (P<0.05). Median OS time was not significantly different between 1q21 amplification group and no 1q21 amplification group in patients with FISH abnormalities (P>0.05). Median OS time was not significantly different between t(4;14) group and no t(4;14) group in patients with FISH abnormalities (P>0.05). Seven patients of 17p deletion died in 2 years.
Conclusion: Multiple myeloma is characterized by a high occurrence of chromosomal aberrations. 1q21 amplification and t(4;14) are the most common abnormalities. Multiple cytogenetic abnormalities are frequently observed in the same one patient. The total response rate, CR rate, and OS time are worse in cytogenetic abnormal patients compared with cytogenetic normal patients. Patients with 17p deletion have a very poor prognosis. Future goals of therapy will be to achieve minimal residual disease, biomarkers, and genomic data, which might provide a better estimate of the depth of response to therapy and OS.
Keywords: multiple myeloma, FISH, clinical characteristics, survival time
Introduction
Cytogenetic abnormalities have important prognostic values for multiple myeloma, especially in distinguishing the high-risk patients. Cytogenetic abnormalities were detected by fluorescent in situ hybridization (FISH) in most patients with newly diagnosed multiple myeloma (MM). MM is a heterogeneous disease with different cytogenetic aberrations, clinical characteristics, and therapy responses. Cytogenetic abnormalities are generally associated with prognosis.
Method
Samples for this study were acquired with written informed patient consent, in compliance with Beijing Chaoyang Hospital Institutional Review Board. We identified 50 patients (22 males, 28 females) with newly diagnosed MM based on the FISH data between November 2010 and April 2014. Median age of them was 62 years (range: 38–79 years). Diagnosis criteria were as defined by the World Health Organization (2001) diagnostic criteria. The examinations included immunoglobulin quantity, immunofixation electrophoresis, bone marrow hemocytology, bone marrow immunophenotype, FISH, X-ray/computed tomography/magnetic resonance imaging, complete blood cell count, Scr, β2-microglobulin (MG), lactate dehydrogenase (LDH), and C-reactive protein (CRP). All the patients were treated with bortezomib-based chemotherapy regimens. Eight patients were treated with lenalidomide. Response criteria were as defined by the International Myeloma Working Group uniform response criteria. The two groups of patients (cytogenetically abnormal vs cytogenetically normal) were evaluated for median overall survival (OS).
Results
FISH probes used in the study included FGFR3/IGH, CCND1/IGH, IGH/MAF, 1q21, and TP53. Cytogenetic aberrations were found in 66% (33 of 50) of patients. According to the Durie–Salmon staging system: one was in stage I, 20 were in stage IIIA, and 12 were in stage IIIB, and as per International Staging System (ISS): three were in stage I, seven were in stage II, and 23 were in stage III. Twelve were with lgG type, ten were with lgA type, and eleven were with light-chain type. Also, twenty-three cases were analyzed by flow cytometry. Positive expressions of CD38, CD138, CD56, CD45, CD2, CD20, CD28, CD22, and CD117 were detected in 100%, 100%, 73.9%, 34.8%, 34.8%, 30.4%, 21.7%, 17.4%, and 17.4% of cases, respectively. Multiple bone lesions were seen in 97% of patients. β2-MG exceeding 3.5 mg/dL was seen in 73.3% of patients. Hypoproteinemia was seen in 56.7% of patients. Anemia was seen in 56.7% of patients. Thrombopenia was seen in 26.7% of patients. Elevated serum creatinine was seen in 30% of patients. Elevated CRP was seen in 38.5% of patients. Elevated LDH was seen in 20.8% of patients. Hypercalcemia was seen in 26.7% of patients. Elevated erythrocyte sedimentation rate was seen in 70.8% of patients (Table 1). One cytogenetic aberration was detected in 21.2% of patients. Two cytogenetic aberrations were detected in 51.5% of patients. Multiple cytogenetic aberrations were detected in 27.3% of patients. 1q21 amplification was seen in 69.7% (23 of 33) of patients. t(4p16.3/14q32) was seen in 30.3% (ten of 33) of patients. 14q32 amplification/deletion was detected in 27.3% (nine of 33) of patients. 17p deletion was seen in 21.2% (seven of 33) of patients. 16q23 deletion/amplification was seen in 21.2% (seven of 33) of patients. t(14q32/11q13) was detected in 15.5% (five of 33) of patients. 11q13 amplification was detected in 18.2% (six of 33) of patients. 4p16.3 deletion was detected in 3% (one of 33) of patients. A dual fusion probe for IGH and a dual fusion probe for CCND1 were used in our study. A translocation with an unknown partner will give an extra signal. So an extra signal is not necessarily indicative of amplification.
 | Table 1 Clinical data in patients with MM |
Response and prognosis
Novel agents including thalidomide, lenalidomide, and bortezomib were used for induction or salvage treatment. Patients were also treated with vindesine, adriamycin, dexamethasone (VAD), vindesine, liposome, dexamethasone (DVD), melphalan, prednisone (MP), vindesine, carmustine, cyclophosphamide, melphalan, prednisone (M2), cyclosphosphamide, thalidomide, dexamethasone (CTD), and cisplatin, etoposide, cyclosphosphamide, prednisone (DECP). Patients with cytogenetic abnormality had lower response rate (complete response [CR] + near CR + partial response) compared with those with cytogenetic normality (82.1% vs 93.8%). Patients with cytogenetic abnormality had lower CR rate compared with those with cytogenetic normality (32.1% vs 50%). The median time to CR of two groups was 3 months. The median time of sustained CR of two groups was 10 months and 12 months, respectively. Patients with cytogenetic abnormality had significant shorter survival time compared with that of cytogenetic normality (21 months vs 54 months, P=0.027) (Figure 1). Response rate and CR rate were 89.5% and 26.1%, respectively, in patients with 1q21 gain. The median time of achieving CR and sustained CR was, respectively, 3 months and 7 months in patients with 1q21 gain. Median OS time was not significantly different between 1q21 amplification group and no 1q21 amplification group in patients with FISH abnormal results (P>0.05) (Figure 2). Median OS time was not significantly different between t(4;14) group and no t(4;14) group in patients with FISH abnormal results (P>0.05) (Figure 3). Seven patients of 17p deletion died in 2 years.
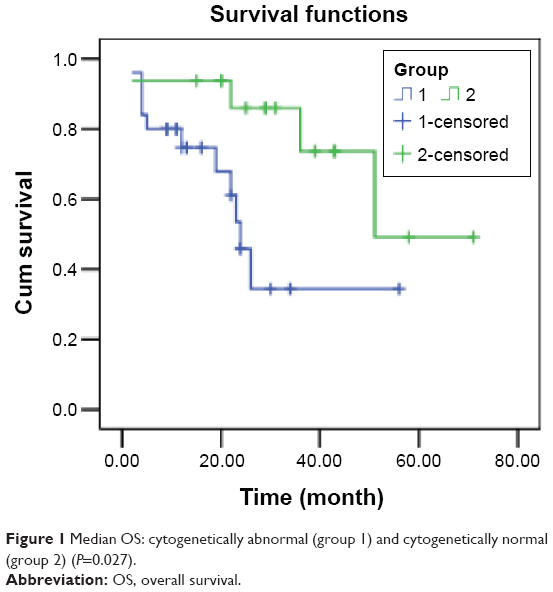 | Figure 1 Median OS: cytogenetically abnormal (group 1) and cytogenetically normal (group 2) (P=0.027). |
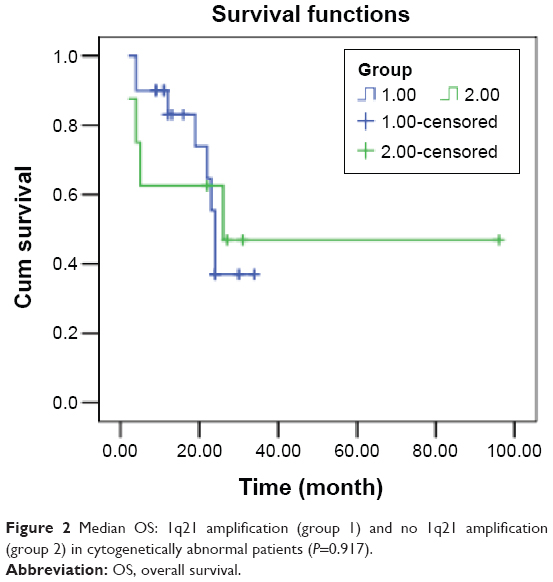 | Figure 2 Median OS: 1q21 amplification (group 1) and no 1q21 amplification (group 2) in cytogenetically abnormal patients (P=0.917). |
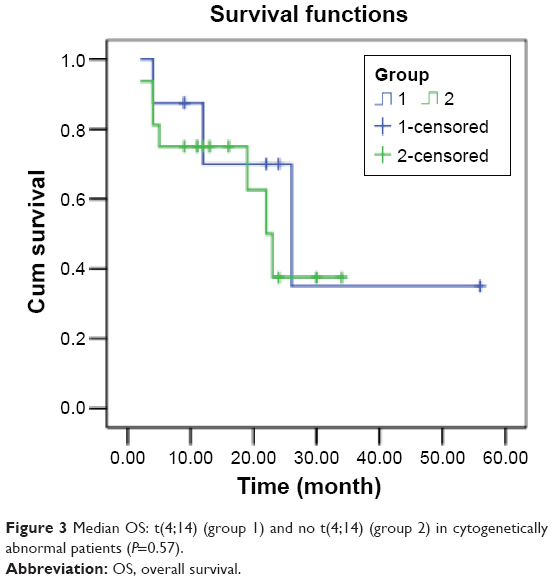 | Figure 3 Median OS: t(4;14) (group 1) and no t(4;14) (group 2) in cytogenetically abnormal patients (P=0.57). |
Discussion
In our study, the patients with abnormal FISH results had higher frequency in stage III of ISS staging, stage III of Durie–Salmon staging, β2-MG, anemia, thrombocytopenia, hypocalcemia, elevated LDH, and elevated CRP compared with those with normal FISH results. These show that patients with cytogenetic abnormality are more serious compared with those with cytogenetic normality. CD138 expression and CD38 expression are seen in all the patients analyzed by immunotyping. The patients with abnormal FISH results have higher frequency of lacking CD45 expression compared with those with normal FISH results. Lacking CD45 expression might have been partially responsible for the worse outcomes. One study reported1 that bone marrow plasma cells strongly express CD38 and usually lack or dimly express CD45. But the mechanism action of CD38 was not clear. Strongly expressed CD138 might be associated with plasma cells homing. In our study, the patients with abnormal FISH results have higher expression of CD20, CD117, CD56, and CD28 compared with those with normal FISH results. King and Nelson2 reported that CD20 expression was infrequent but was responsible for the poor prognosis. CD28 was responsible for the progression. CD56 was not expressed or weak in monoclonal gammopathy of undetermined significance (MGUS), but strong in MM, and was associated with poor outcomes. Shin et al3 showed that CD45-negative cases were associated with deletion 13 or aneuploidy and del(17p). CD45 negativity or CD117 negativity was associated with advanced stage.
In our study, the patients of abnormal FISH results had higher occurrence in 1q21 amplification compared with the reports (69.7% and 50%). Sustained CR was short in patients with 1q21 amplification, which implicated that the patients are inclined to progress. Obtaining superior proliferation in plasma cells of 1q21 was responsible for the progression. In our study, 14q32 amplification/deletion was observed in 72.7% of patients, and t(4;14) was the most common aberration. Lim et al4 reported that IGH rearrangements were the most common abnormality. t(4p16.3/14q32) rearrangements were most frequent. t(4;14) was an early event. The study recorded a low incidence of 17p deletion, which was also observed in our study. 1q21 amplification and del(17p) by FISH conferred a high incidence of progressive disease after initial therapy. Metaphase detection of IgH rearrangements and chromosome 1 aberrations concurrently was associated with a short progression-free survival. Advanced biomarker and genetic testing includes cytogenetics, FISH, and gene expression profiling to estimate the aggressiveness of the disease and personalize the patient’s treatment.
It has been identified that t(4;14), t(14;16), 13q-, and 17p- are associated with poor outcomes. Our study found that the OS time of patients with abnormal FISH results was significantly shorter than those with normal FISH results. Seven patients with 17q deletion died in 2 years. It has been suggested that those with 17p deletion could rank super-high risk. We also find that three of five patients with t(11;14) died in 2 years, while t(11;14) generally is not associated with worse outcomes. Sasaki et al5 studied the impact of t(11;14) on the outcome in patients with MM who received high-dose chemotherapy followed by auto hematopoietic cell transplantation (HCT). t(11;14) and HR abnormalities by conventional cytogenetics (CC) or FISH, β2-MG of >3.5, and relapsed disease at the time of auto-HCT were associated with shorter OS. Patients with t(11;14) had worse outcomes than patients with normal CC or FISH studies. But in our study, it is noteworthy that one patient with t(11;14) harbored a 1q21 amplification, one patient harbored a 17P- in our study. So complex rearrangements portended a poor prognosis. t(14;16) was found only in 7% of patients with MM by FISH. In our study, only 16q23 deletion/amplification was found in seven patients, and no t(14;16) was found. In our study, all the patients were treated by bortezomib-based chemotherapy regimens. Patients with or without t(4;14) did not have a significant difference in median OS time. This actually suggested that bortezomib can abrogate the effects of adverse prognosticator of t(4;14). Inclusion of bortezomib may change the outcome of a single cytogenetic abnormality, but many patients have complex cytogenetic abnormalities. The poor outcome of patients with abnormal FISH results illustrated that bortezomib could not change the outcome of complex cytogenetic abnormalities fundamentally. Paszekova et al6 reported that ~10%–15% of all patients with MM relapse early and have poor prognosis and outcome. Moreover, Moreau et al7 presented that the risk of early MM progression-related death was related to LDH higher than normal, International Staging System 3 (ISS3), and adverse cytogenetics t(4;14) and/or del(17p). Bergsagel et al8 pointed that the introduction of thalidomide, lenalidomide, and bortezomib has dramatically improved the outlook for patients with MM, but their relative benefit (or harm) for different genetic patient subgroups remains unclear. Faiman9 pointed that future goals of therapy will be to achieve minimal residual disease, biomarkers, and genomic data, which might provide a better estimate of the depth of response to therapy and OS.
Disclosure
The authors report no conflicts of interest in this work.
References
Witzig TE, Kimlinger TK, Ahmann GJ. Detection of myeloma cells in the peripheral blood by flow cytometry. Cytometry. 1996;26(2):113–120. | ||
King MA, Nelson DS. Tumor cell heterogeneity in multiple myeloma: antigenic, morphologic, and functional studies of cells from blood and bone marrow. Blood. 1989;73(7):1925–1935. | ||
Shin SY, Lee ST, Kim HJ. Antigen expression patterns of plasma cell myeloma: An Association of Cytogenetic Abnormality and International Staging System (ISS) for myeloma. J Clin Lab Anal. 2014;2(10):1002. | ||
Lim AS, Krishnan S, Lim TH. Amplification of 1q21 and other abnormalities in multiple myeloma patients from a tertiary hospital in Singapore. Indian J Hematol Blood Transfus. 2014;30(4):253–258. | ||
Sasaki K, Lu G, Saliba RM. Impact of t(11;14)(q13;q32) on the outcome of autologous hematopoietic cell transplantation in multiple myeloma. Biol Blood Marrow Transplant. 2013;19(8):1227–1232. | ||
Paszekova H, Kryukov F, Kubiczkova L. High-risk multiple myeloma: different definitions, different outcomes? Clin Lymphoma Myeloma Leuk. 2014;14(1):24–30. | ||
Moreau P, Cavo M, Sonneveld P. Combination of international scoring system 3, high lactate dehydrogenase, and t(4;14) and/or del(17p) identifies patients with multiple myeloma (MM) treated with front-line autologous stem-cell transplantation at high risk of early MM progression-related death. J Clin Oncol. 2014;32(20):2173–2180. | ||
Bergsagel PL, Mateos MV, Gutierrez NC. Improving overall survival and overcoming adverse prognosis in the treatment of cytogenetically high-risk multiple myeloma. Blood. 2013;121(6):884–892. | ||
Faiman B. Myeloma genetics and genomics: practice implications and future directions. Clin Lymphoma Myeloma Leuk. 2014;14(6):436–440. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.