Back to Journals » International Medical Case Reports Journal » Volume 18
Cystic Lymphangioma in the Talus Bone: A Case Report
Authors Liang CH, Wong KC ![]() , Lacambra MD, Chu WCW
, Lacambra MD, Chu WCW
Received 14 April 2025
Accepted for publication 23 July 2025
Published 12 August 2025 Volume 2025:18 Pages 1021—1028
DOI https://doi.org/10.2147/IMCRJ.S529233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Video abstract presented by Liang.
Views: 46
Ching Hei Liang,1 K C Wong,2 Maribel D Lacambra,3 Winnie CW Chu4
1Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong; 2Orthopaedic Oncology, Department of Orthopaedics and Traumatology, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong; 3Department of Anatomical and Cellular Pathology, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong; 4Department of Imaging and Interventional Radiology, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong
Correspondence: Ching Hei Liang, Email [email protected]
Background: Lymphangiomas, predominantly observed in pediatric populations, can occasionally be acquired in adulthood. They are rare benign tumors mostly found in the head and neck region, with solitary cystic lymphangioma in bone being very rare.
Case Presentation: We report an uncommon case of a solitary cystic lymphangioma in the talus bone of a 19-year-old Chinese female presented with a history of enduring ankle swelling, rest pain, and frequent sprains. The patient’s T2-weighted Magnetic Resonance Imaging (MRI) revealed a cystic bone lesion with multiple internal fluid levels, which initially suggested a Giant Cell Tumor (GCT) or chondroblastoma with secondary Aneurysmal Bone Cyst (ABC) change. However, histopathological examination of the tissue sample obtained through curettage suggested the diagnosis of intraosseous lymphangioma. The postoperative period was uneventful with no complications. Patients restored near normal ankle range of motion and there have been no signs of recurrence.
Conclusion: This case demonstrates the importance of considering a broad differential diagnosis when evaluating bone lesions, and it underlines the need to correlate pathological findings with radiographic images and clinical examination for an accurate diagnosis.
Keywords: case report, curettage, lymphangioma, solitary cystic lymphangioma, talus
Introduction
Lymphangiomas are rare lymphatic malformations that typically present as fluid-filled, palpable masses. The skin overlying these lesions is often unaltered, but a bluish hue or reddish nodules may occasionally be observed.1 They primarily occur in pediatric populations, with most cases diagnosed before the age of two (80–90%).2 They are predominantly localized in the head and neck region, accounting for nearly 90% of the cases, which is attributed to their embryological origin closely associated with the primordial jugular lymphatic sac.3 Lymphangiomas in the bone of the lower extremities are uncommon, mostly in the form of lymphangiomatosis. Solitary cystic lymphangioma in bone is rarely documented.4
In this report, we present an unusual case of a lymphangioma in the talus bone of a 19-year-old Chinese female. The rarity of this lesion, combined with clinical and radiographic features, led to an initial diagnosis of a Giant Cell Tumor (GCT) or chondroblastoma with secondary aneurysmal bone cyst (ABC) type of change—a more common bone lesion in this age group. As bone cysts in talus often present ambiguous radiological and clinical features that mimic more common lesions, histological examination is essential for confirming a definitive diagnosis of lymphangioma. In this case, the final diagnosis was established after being treated with intralesional curettage and correlating the histopathologic findings with the clinical and radiographic characteristics. This case underscores the importance of considering a wide differential diagnosis for bone lesions and emphasizes the need for a multidisciplinary approach to diagnosis and treatment.
Case Report
A 19-year-old Chinese female with no prior history of trauma presented with visible right ankle swelling, rest pain, and repeated ankle sprains. The pain and swelling persisted for approximately two years, with the pain becoming more intense in recent months. Upon physical examination, the patient complained of pain when palpating on the anterolateral side of the ankle. She also exhibited a limited range of motion and difficulty in balance. There was no skin redness or bruises around the ankle region. The case report followed the CARE Guidelines for case reports.
Plain radiograph of the right ankle showed a mildly expansile osteolytic lesion at the talar neck without aggressive periosteal reaction or matrix mineralization (Figure 1A). MRI revealed a well-defined, cystic lesion of 3.7×2 × 1.9 cm in size, centered in the lateral side of the talar neck, without extension to the subchondral bone of the talar dome or talar neck (Figure 1B). There was extensive marrow edema in the talus without evidence of pathological fractures, and a small volume of effusion indicated mild diffuse synovitis. Cartilage coverage of the ankle joint and subtalar joint appeared intact. The overall imaging features resembled an expansile, bubbly bone lesion with multiple internal fluid levels. The radiological features suggested an ABC, either primary or secondary to other underlying primary lesions like GCT of bone or chondroblastoma.
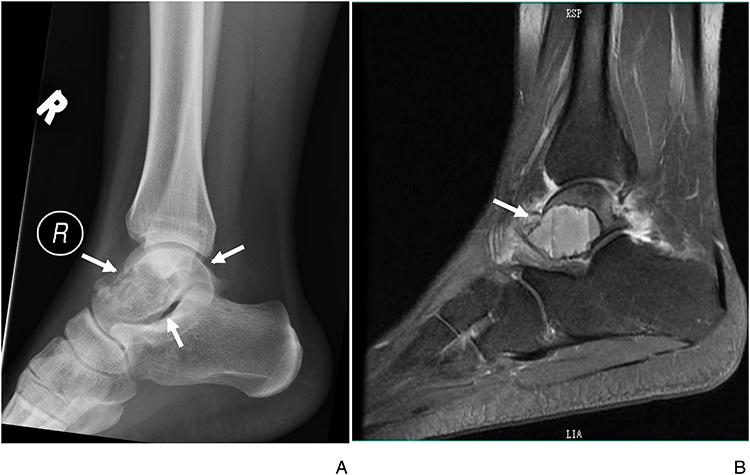 |
Figure 1 (A) Sagittal View of Plain Radiograph of the Right Ankle. The plain radiograph shows a relatively well-defined osteolytic lesion without periosteal reaction or matrix mineralization at the talar neck (white arrows). (B) Sagittal View of MRI Image of the Right Ankle. The view of MRI image shows a well-defined, cystic lesion centered in the lateral side of the talar neck, without extension to the subchondral bone of the talar dome or talar neck. There was extensive marrow edema in the talus without evidence of pathological fractures, and a small volume effusion indicated mild diffuse synovitis. |
A computed tomography (CT) - guided biopsy of the bone lesion was subsequently arranged for tissue diagnosis. The CT imaging found the lesion to be multilobulated and moderately expansile (Figure 2A and B). The anterior part of the internal content was more hyperdense while the posterior part was more hypodense, which corresponded to the fluid layer. Histological examination revealed normal bone tissue with fatty marrow and minimal fibrosis. No malignant-looking cells or osteoclast-like giant cells were seen. However, the amount of tumor tissue obtained during needle biopsy of the cystic bone lesion was insufficient for definitive diagnosis. Surgical resection was decided because of persistent pain symptoms. Via an anterolateral surgical approach, the extensor retinaculum was split, and extensor toe tendons were retracted medially to expose the anterolateral aspect of the talar neck where about 1.5 cm cortical window was made (Figure 2C and D). Intralesional tumor curettage was performed under endoscopic assistance (Figure 3A and B) as the brownish-yellow gross appearance of the tumor tissue looks similar to the GCT of bone (Figure 3C). Bone cement was used to fill up the bone cavity, providing immediate bone stability and possibly reducing local tumor recurrence.
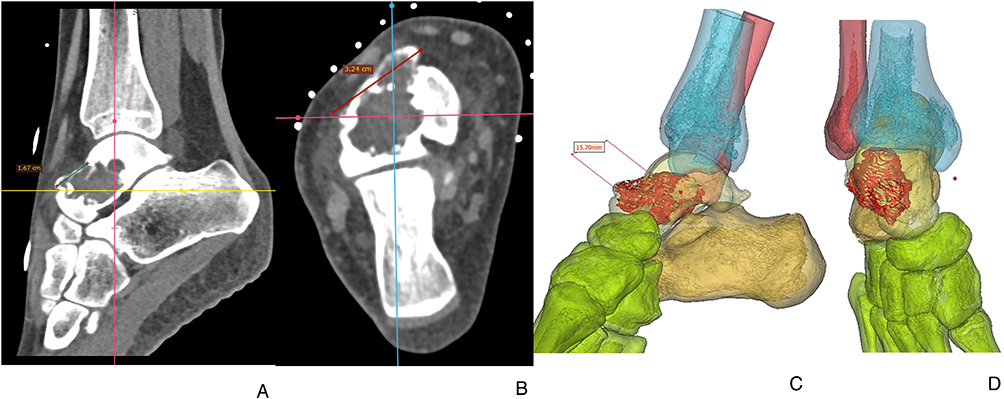 |
Figure 2 Sagittal (A) and Coronal (B) Views of CT Images of Right Ankle. (A and B) show an osteolytic lesion centered at midline to lateral aspect of the talar neck and head is evident. It is measured ~2.5cm x 2.6cm x 2.0cm. It is multilobulated in outline and moderately expansile with lateral, superoanterior and inferior bulging border which are paper thin. No definite fracture can be observed. The mass shows narrow zone of transition, and its outline is sclerotic. Anterior part of the internal content is more hyperdense while the posterior part is more hypodense, which may correspond to the fluid layering. No internal mineralization is seen. Some soft tissue thickening over lateral aspect of the talus is also evident. No periosteal reaction is noted. Lateral (C) and Anterior (D) Views of 3D Bone Reconstruction (C and D) shows the tumor location (red) at the talar bone and the planned cortical window (about 1.5cm) for the intralesional tumor curettage. |
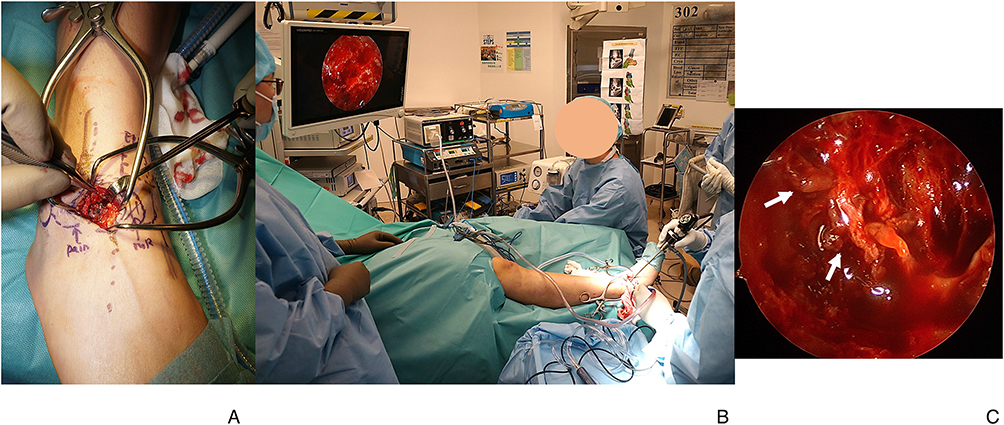 |
Figure 3 (A) Tumor Curettage The anterolateral skin was incised and talar neck was exposed for the intralesional tumor curettage. (B) Endoscopic Assisted Tumor Curettage. The endoscopic visualization provided a magnified view of the tumor cavity, facilitating the better clearance of tumor tissue from the bone cavity. (C) Brownish-yellow Tumor Tissue (white arrow) in the Multicystic Bone Lesion. The gross appearance of the brownish-yellow tumor tissue (white arrow) may suggest GCT of bone. |
Histologically, the lesion showed dilated thin-walled vascular spaces lined by a single layer of endothelial cells with no significant atypia (Figure 4A and B). By immunohistochemistry (IHC) stains, the endothelial cells are highlighted by D2-40, while CD34 was negative (Figure 4C). Polymerase chain reaction (PCR) direct sequencing for H3F3A/H3F3B/GNAS gene mutations in GCT, chondroblastoma and fibrous dysplasia, respectively, were negative; and fluorescence in situ hybridization (FISH) test of USP6 rearrangement in ABC was likewise negative. Hence, the overall features suggested vasoformative lesion favoring the diagnosis of bone lymphangioma.
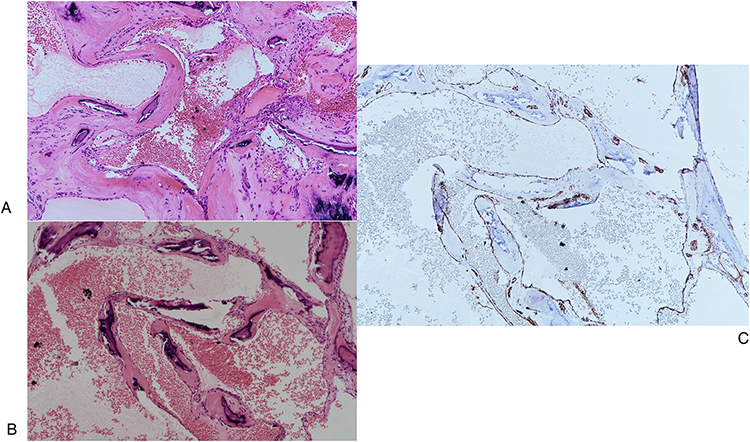 |
Figure 4 (A and B) Tumor Tissue Under Microscope (10× magnification). The lesion showed dilated thin-walled vascular spaces lined by a single layer of endothelial cells with no significant atypia. (C) IHC Stain of the Tumor Tissue (10× magnification). The endothelial cells are highlighted by D2-40 by the IHC stain. |
Clinical and radiographic follow-up were performed two weeks, nine weeks, six months and one year postoperatively to evaluate bone consolidation. The patient restored near normal ankle range of motion. There have been no signs of recurrence.
Discussion
Lymphangiomas are a progressively growing masses estimated to occur in approximately 1 in 2000 to 4000 individuals, with no discernible variations observed among genders or ethnicities but are primarily found in pediatric population. They account for 4% of all vascular tumors in children.2
For congenital lymphangiomas, sequestration of primordial lymphatic cells during fetal development results in persistent accumulation of lymph within the lymphatic channels. When they are unable to join the larger vessels, lymphatic obstruction may occur, giving the lesion its characteristic cystic appearance. While the exact cause remains unknown, lymphangiomas predominantly manifest in the head and neck region — accounting for up to 90% of cases — likely due to their proximity to the primordial jugular lymphatic sac.3 Furthermore, genetic disorders such as Turner syndrome and Down syndrome are believed to link to lymphangiomas.5 Although lymphangiomas in adults are uncommon, they can originate from chronic lymphedema, inflammation or trauma, which disrupts and enlarges previously normal lymphatic pathways. Failure to establish connections between the primary lymphatic sacs and the venous system can result in excessive proliferation of lymphatic vessels.6
From a histological perspective, lymphangiomas can be classified into three subtypes: capillary, cavernous, and cystic. The cystic subtype is the most prevalent and is characterized by the presence of dilated lymphatic channels.1 The enlargement of the lymphatics causing pressure may result in bone erosion, manifesting symptoms such as pain, pathological fracture, and deformity.7
Occurrence in the lower extremities can be rare, in a study conducted by Itakura et al in 2009, out of 114 reported cases of lymphangiomas, only two cases were found to be in the foot. Based on their research, the incidence of lymphangioma in the foot was determined to be 1.75%.1,8 Lymphangiomas in reported cases often originate from adjacent soft tissue, only involving the bone secondarily. Most cases involving only bone are distributed across multiple skeletal sites and/or associated with extensive involvement of organs and tissues in the form of lymphangiomatosis. The presence of a solitary and localized cystic lymphangioma in bone is exceptionally rare.4,9 Solitary intraosseous lymphangiomas have been reported in areas such as the tibia, humerus, mandible, cranium, ileum, skull and spine.7 From the cases reported by Mendez et al, it was found that the spine and mandible were the most documented sites of occurrence.9
An extensive literature search was conducted on Google Scholar and PubMed search engines using the following keywords: lymphangioma, lymphatic malformation, bone, intraosseous, osseous, skeletal, case report. Literature published in the English language up to March 2025 were thoroughly searched. Studies that were duplicates, not in English language, not of interosseous origin, not solitary or unifocal were excluded. Only lesions in the extremities were included due to their shared clinical presentation and treatment outcome with the current case study. The table of cases of solitary cystic lymphangiomas involving bone in the extremities reported in the literature is compiled as follows [see Table 1].9–12
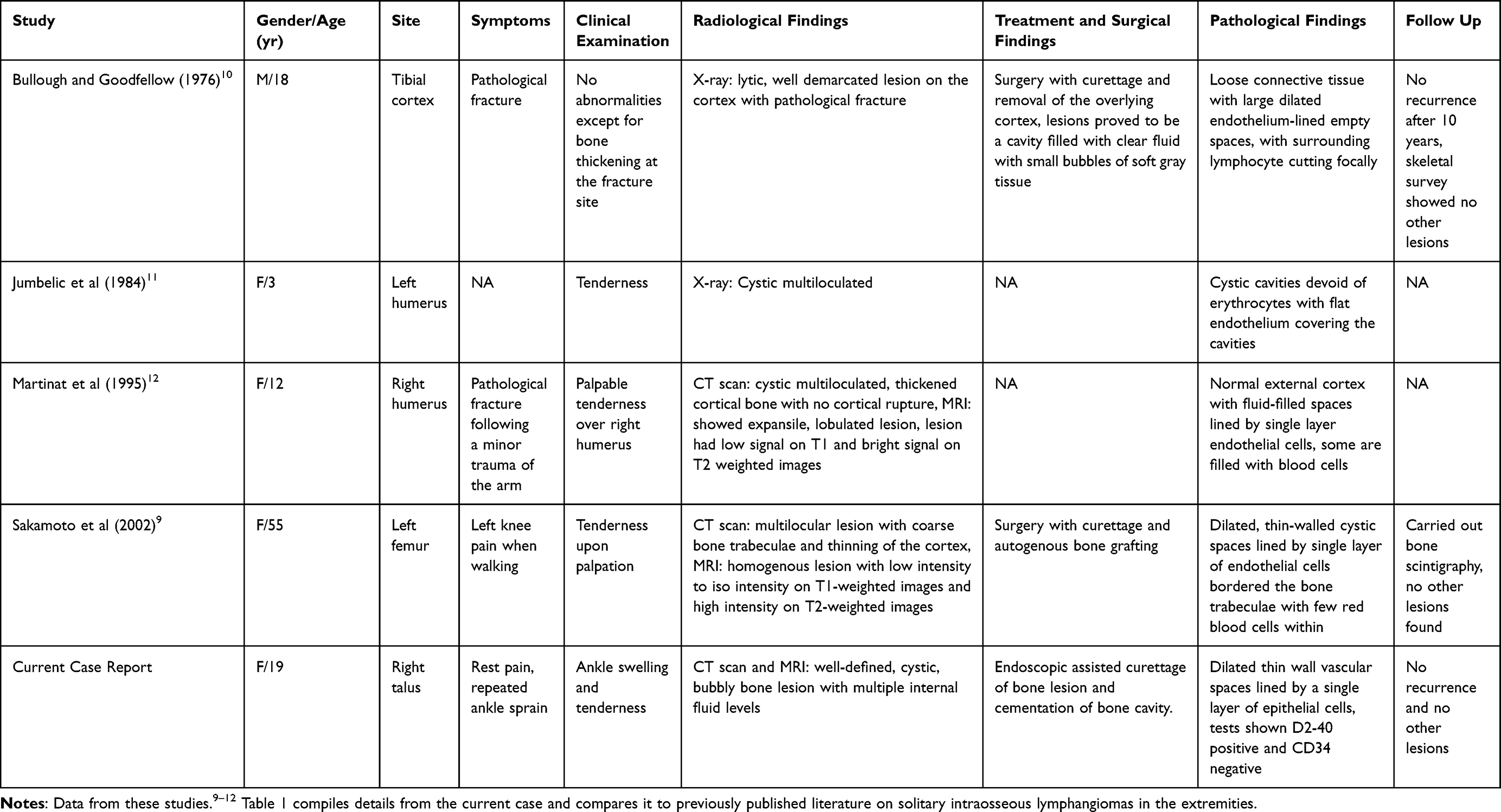 |
Table 1 Cases of Solitary Lymphangiomas Involving Bone in the Extremities Reported in the Literature |
The discussed case is unique from most lymphangiomas due to several factors, including the patient’s age, the location of the lesion, and the ambiguous clinical and radiographic characteristics, contributing to diagnostic challenge. Unlike most cases, the patient did not present with the condition in childhood, and the lesion was located in the talus bone of the foot – an uncommon site for lymphangiomas.
Radiological evaluations effectively ruled out the possibility of malignancy, as more aggressive bone tumors, including chondrosarcoma and osteosarcoma, typically present with more prominent soft tissue components in the older population. The MRI features revealed the cystic lesion with higher signal intensity on T2-weighted images due to fluid levels in talus bone, which resembled that of the GCT with ABC change. Although a GCT of the small bone is also a relatively rare condition, it is usually intraosseous and characteristically affects the mature skeleton, most commonly presenting in individuals in young adults, corresponding to our patient. The clinical features, including pain, swelling, and limited mobility, presented by the patient were consistent with the usual traits of GCT of the bone, leading to an initial misdiagnosis.
Although radiological imaging and clinical assessments are important in initially identifying specific lesions, they may not always provide a conclusive diagnosis when faced with ambiguous characteristics. In such cases, it becomes necessary to pursue further investigative measures through histopathological examination to provide a more definitive diagnosis. In this case, the excised sample was examined for markers related to GCT, primary ABC and fibrous dysplasia, which helped differentiate intraosseous lymphangioma from other tumor types.
The absence of mononuclear cell proliferation and osteoclast-like giant cells precludes the definitive diagnosis of GCT and ABC. FISH analysis showed negative USP6 rearrangement, a characteristic feature present in more than half of ABC cases, further ruling out this diagnosis. PCR direct-sequencing methods were also employed to investigate potential H3F3A and H3F3B gene mutations, which are associated with GCTs and chondroblastoma respectively and both came out negative.
The confirmation of the lymphangioma diagnosis was supported by D2-40 IHC staining, highlighting the lymphatic endothelial cells. Additionally, CD31 and CD34, which are primary markers for vascular endothelium, were negative, suggesting that they predominantly comprise lymphatic vessels.13 Such features are usually absent in GCT, ABC or chondroblastoma. This histopathological finding, coupled with negative USP6 rearrangement and H3F3A/B mutations, provides conclusive evidence for lymphangioma over other bone lesions despite overlapping radiological and clinical presentations.
A wide variety of management strategies has been proposed for lymphangiomas, including surgical excision, electrocautery, cryotherapy, radiotherapy, intralesional steroids, sclerosing agents (OK432), embolization and ligation, laser treatment with Nd: YAG and carbon dioxide, and radiofrequency tissue ablation technique.3 However, surgical intervention remains the fundamental treatment approach for lymphangiomas and is frequently considered the initial choice of therapy. In this case, surgery was performed to provide symptomatic relief and restore weight-bearing functions. Given the tendency of lymphangiomas to expand if left untreated, a complete surgical excision was pursued to prevent recurrence. Reportedly, the recurrence rate is 40% after an incomplete excision and 17% following a macroscopically complete excision.1 During the operation, endoscope assistance was utilized during the surgical procedure for enhanced visualization and minimize damage to surrounding tissues and the tumor’s precise location. Furthermore, based on the initial diagnosis of GCT, the use of bone cement was favored over bone grafting to fill the defect due to lower recurrence rate.6 This rationale may also apply to the management of lymphangioma in bone.
In this case, the lesion was solitary with relatively well-defined boundaries, thus facilitating complete surgical excision with a favorable prognosis. Following surgery, the patient showed near normal ankle movement with no signs of local recurrence one year postoperatively. However, a potential limitation of our study is the short-term follow-up, which may limit the understanding of recurrence. Regular follow-up is thus crucial to monitor the long-term outcome.
Patient’s Perspective
The patient experienced no bone pain after the surgery and regained near normal ankle range of motion after two months of physiotherapy. She could walk unaided and resumed her usual sports activities like running and cycling. There was no clinical nor radiological features to suggest local recurrence at the latest follow-up assessment.
Take-Home Message
Conclusion
In conclusion, the presented case illustrates the complex and varied presentations of lymphangiomas within bone, which contribute to diagnostic challenges due to overlapping clinical and radiographic features with other osseous conditions. This report highlights the necessity of a multidisciplinary diagnostic approach, combining radiological imaging, surgical intervention, and histopathological and molecular analysis, to achieve accurate diagnosis and effective treatment.
Abbreviation
ABC, Aneurysmal bone cyst; CT, Computed tomography; FISH, Fluorescence in situ hybridization; GCT, Giant cell tumor; IHC stain, Immunohistochemistry stain; MRI, Magnetic resonance imaging; PCR, Polymerase chain reaction.
Ethics Approval and Consent to Participate
Not applicable. No institutional approval is required for this case report.
Consent for Publication
Written informed consent to publish any case details and accompanying photographs were obtained from the patient.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bob SF, Panagakos P, Sadri S. Lymphangioma of the foot: a case report. Foot Ankle Online J. 2011;1.
2. Miceli A, Stewart KM. Lymphangioma. Nih.gov. 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470333/.
3. Hasan S, Ahmad SA, Kaur M, Panigrahi R, Panda S. Lymphangioma of the lower lip—a diagnostic dilemma: report of a rare case with a brief literature review. Case Rep Dent. 2022;2022:1–8. doi:10.1155/2022/7890338
4. Falkmer S, Tilling G. Primary Lymphangioma of Bone. Acta Orthop Scand. 1956;26(2):99–110. doi:10.1080/00016470.1956.11978727
5. Liu X, Cheng C, Chen K, Wu Y, Wu Z. Recent progress in Lymphangioma. Front Pediatr. 2021;9. doi:10.3389/fped.2021.735832
6. Vaishya R, Pokhrel A, Agarwal A, Vijay V. Current status of bone cementing and bone grafting for giant cell tumour of bone: a systemic review. Ann Royal Coll Surg Engl. 2019;101(2):79–85. doi:10.1308/rcsann.2019.0004
7. Ac I, K H. Lymphangıomatosıs of the skull base. Theranost Brain Spine Neural Disord. 2023;4(4). doi:10.19080/TBSND.2022.04.555643
8. Itakura E, Yamamoto H, Oda Y, Furue M, Tsuneyoshi M. VEGF-C and VEGFR-3 in a series of lymphangiomas: is superficial lymphangioma a true lymphangioma? Virchows Archiv. 2009;454(3):317–325. doi:10.1007/s00428-008-0720-8
9. Sakamoto A, Matsuda S, Tanaka K, Shukuri T, Harimaya K, Iwamoto Y. Solitary lymphangioma of the femur. A case report. J Orthop Sci. 2002;7(4):501–504. doi:10.1007/s007760200088
10. Bullough PG, Goodfellow JW. Solitary lymphangioma of bone. A case report. JBJS. 1976;58(3):418. doi:10.2106/00004623-197658030-00026
11. Jumbelic M, Feuerstein IM, Dorfman HD. Solitary intraosseous lymphangioma. A case report. JBJS. 1984;66(9):1479. doi:10.2106/00004623-198466090-00029
12. Martinat P, Cotten A, Singer B, Petyt L, Chastanet P. Solitary cystic lymphangioma. Skeletal Radiology. 1995;24(7). doi:10.1007/bf00202161
13. Fukunaga M. Expression of D2-40 in lymphatic endothelium of normal tissues and in vascular tumours. Histopathology. 2005;46(4):396–402. doi:10.1111/j.1365-2559.2005.02098.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Surgical Management of Aneurysmal Bone Cyst of the Pubis: A Case Report and Review of Literature
Dawod MS, Alisi MS, Rabab'a H, Abdulelah AA, Almaaitah HW, Haddad B
International Medical Case Reports Journal 2022, 15:287-292
Published Date: 14 June 2022