Back to Journals » International Journal of General Medicine » Volume 17
CYP2C19 Loss-of-Function is an Associated Risk Factor for Premature Coronary Artery Disease: A Case–Control Study
Authors Chen W, Liu Y, Deng X, Li B, Wang H, Wei G, Chen K, Wang S
Received 15 August 2024
Accepted for publication 26 October 2024
Published 3 November 2024 Volume 2024:17 Pages 5049—5058
DOI https://doi.org/10.2147/IJGM.S486187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Redoy Ranjan
Wenhao Chen,1 Yuanliang Liu,2 Xunwei Deng,3 Bin Li,1 Hao Wang,1 Guoliang Wei,1 Kehui Chen,1 Shen Wang1
1Center for Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou, People’s Republic of China; 2Department of Computer Tomography, Meizhou People’s Hospital, Meizhou, People’s Republic of China; 3Research Experimental Center, Meizhou People’s Hospital, Meizhou, People’s Republic of China
Correspondence: Wenhao Chen, Center for Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou, People’s Republic of China, Email [email protected]
Objective: Cytochrome P450 2C19 (CYP2C19) is a major enzyme involved in the biotransformation and metabolism of various substances. Loss-of-function of the CYP2C19 gene represents downregulation of CYP2C19 enzyme indication limited or no enzymatic function, which may be, in turn, associated with some disease susceptibility. The relationship between CYP2C19 polymorphisms and susceptibility to premature coronary artery disease (PCAD) is not fully understood. This study aimed to assess this relationship.
Methods: This study included 635 PCAD patients, and 548 age-matched non-CAD individuals as controls, from November 2019 to August 2023. The CYP2C19 rs4244285 (681G > A, *2) and rs4986893 (636G > A, *3) were genotyped, and the distribution of CYP2C19 polymorphisms between patients and controls and the relationship between CYP2C19 polymorphisms and PCAD risk were analyzed.
Results: A total of 442 (37.4%), 543 (45.9%), and 198 (16.7%) individuals had CYP2C19 extensive metabolizer (EM) (*1/*1), intermediate metabolizer (IM) (*1/*2 and *1/*3), and poor metabolizer (PM) (*2/*2, *2/*3, and *3/*3) phenotypes, respectively. CYP2C19 *2/*2 genotype frequency was higher, *1/*1 genotype was lower in PCAD patients than controls. Individuals with CYP2C19 PM phenotype had higher triglyceride (TG) levels than those with CYP2C19 EM or IM phenotypes. Logistic regression analysis showed that body mass index (BMI) ≥ 24.0 kg/m2 (≥ 24.0 kg/m2 vs 18.5– 23.9 kg/m2, odds ratio (OR): 1.326, 95% confidence interval (CI): 1.041– 1.688, p = 0.022), smoking (OR: 1.974, 95% CI: 1.283– 3.306, p = 0.002), hypertension (OR: 1.327, 95% CI: 1.044– 1.687, p = 0.021), diabetes mellitus (OR: 1.390, 95% CI: 1.054– 1.834, p = 0.020), CYP2C19 PM phenotype (PM phenotype vs EM phenotype, OR: 1.701, 95% CI: 1.200– 2.411, p = 0.003), and CYP2C19 IM+PM phenotypes (IM+PM vs EM phenotype, OR: 1.369, 95% CI: 1.077– 1.740, p = 0.010) were associated with PCAD.
Conclusion: CYP2C19 PM or IM+PM phenotypes, overweight, smoking, hypertension, and diabetes mellitus were associated with PCAD.
Keywords: premature coronary artery disease, cytochrome P450, CYP2C19, loss-of-function
Introduction
Cardiovascular diseases (CVDs) are a group of diseases of the human cardiovascular system that mainly affects the heart, arteries, veins, capillaries, and other parts of the abnormal.1,2 Survey data show that the prevalence and mortality rates of CVDs in China are on the rise, with the mortality rate being the highest among urban and rural residents.3,4 Coronary artery disease (CAD) caused by myocardial ischemia or necrosis due to stenosis, blockage and spasm of the coronary artery atherosclerosis.5,6 CAD is a major public health problem that seriously threatens the health of residents.7,8 A high incidence of CAD is generally observed in the elderly, but with the acceleration of the pace of life, accompanied by bad living habits, the incidence of CAD in young and middle-aged people has gradually increased.9,10 The onset of CAD in men aged ≤55 years and in women aged ≤65 years is defined as premature coronary artery disease (PCAD).11,12 Compared with mature coronary artery disease (MCAD), most patients with PCAD patients are acute, without precursor symptoms, and most have acute myocardial infarction (AMI) or even sudden death.13 It is necessary to analyze the risk factors for PCAD to provide a basis for the targeted prevention of PCAD risk groups.
Atherosclerosis is the main pathological basis of CAD and other arterial vascular diseases. It is characterized by the accumulation of lipids, the formation of diseased plaques, thickening of intima, and narrowing of arterial spaces, which lead to ischemia or necrosis of tissues and organs supplied by arteries.14,15 Diabetes mellitus, hypertension, hyperlipidemia, obesity, smoking, alcoholism, and other unhealthy lifestyles, in addition to social psychological stress are the risk factors of CAD.16,17 Cytochrome P450 (CYP450) enzymes are involved in the biotransformation and metabolism of some important substances in the body.18,19 The metabolite in arachidonic acid (AA) catalyzed by cytochrome enzymes has the function of relaxation of blood vessels,20 and acting as a vasodilating agent.21 The imbalance of these metabolites is believed to be involved in the occurrence and development of CVDs.22 On the other hand, reactive oxygen species (ROS) produced by coronary endothelial cells during the cytochrome enzyme-catalyzed reaction can inhibit vasodilation.23 Some studies have suggested that CYP450 enzymes are involved in cancer, diabetes mellitus, and cardiovascular and cerebrovascular diseases.24–26 Cytochrome P450 2C19 (CYP2C19) is a major member of the CYP450 family.27 Two major loss-of-function single-nucleotide polymorphisms (SNPs) rs4244285 (681G > A, known as CYP2C19*2) and rs4986893 (636G > A, known as CYP2C19*3) are the most common SNPs in CYP2C19. CYP2C19 can be divided into six genotypes: *1/*1, *1/*2, *1/*3, *2/*2, *2/*3, and *3/*3.28 According to the genotypes of CYP2C19, the enzyme activity types of CYP2C19 can be divided into three phenotypes: extensive metabolizer (EM) (CYP2C19*1/*1), intermediate metabolizer (IM) (CYP2C19*1/*2, and *1/*3), and poor metabolizer (PM) (CYP2C19*2/*2, *2/*3, and *3/*3)).29,30
At present, CYP2C19 gene variants mainly focuses on their impact on antiplatelet efficacy in CAD patients,31,32 and the relationship between CYP2C19 polymorphisms and CAD risk has not been well studied. Some studies found that CYP2C19 polymorphisms were associated with CAD in Japanese women,33 and a Chinese population.34 The probability of PCAD and its influencing factors may be different in different regions and populations with different genetic backgrounds. The distribution of CYP2C19 polymorphisms among PCAD patients in different populations may be different.35 Hakka people are a branch of the Han people in China, and Meizhou is one of the Hakka people’s settlements.36 To date, the relationship in this population is unclear, and this study aimed to investigate it.
Materials and Methods
Study Participants and Data Collection
A total of 635 patients with PCAD who were admitted to Meizhou People’s Hospital from November 2019 to August 2023 were retrospectively analyzed. The control group consisted of age- and sex-matched healthy individuals who underwent physical examination and CYP2C19 gene polymorphisms detection during the same period. A total of 548 age-matched patients without CAD were used as the controls.
The diagnostic criteria for CAD: coronary angiography (CAG) shows that at least one of the main epicardial vessels had a diameter stenosis >50%.37,38 The inclusion criteria for PCAD were as follows: (1) patients were diagnosed with CAD; (2) men aged ≤55 years and women aged ≤65 years; and (3) complete clinical data. The inclusion criteria for the controls were as follows: (1) non-CAD individuals who had been tested for CYP2C19 rs4244285 and rs4986893 polymorphisms; (2) men aged ≤55 years and women aged ≤65 years; and (3) complete demographic information. The exclusion criteria were as follows: (1) congenital heart disease, cardiomyopathy, or congestive heart failure; (2) severe organ dysfunction; (3) malignant tumor; and (4) serious infectious diseases.
Data including age, sex, body mass index (BMI), smoking, drinking, hypertension, diabetes mellitus, serum lipids (total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (Apo-A1), and apolipoprotein B (ApoB)) was collected. According to the Chinese standards, BMI was divided into three grades: <18.5 kg/m2, 18.5–23.9 kg/m2, and ≥24.0 kg/m.239,40 CYP2C19*2 and CYP2C19*3 variant alleles were genotyped using a CYP2C19 genotyping kit (BaiO Technology Co, Ltd, Shanghai, China).28,34
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 (IBM Inc., USA). Continuous variables were compared using Student’s t-test, the Mann–Whitney U-test or analysis of variance (ANOVA). Genotype composition ratios and allele frequencies between groups were analyzed by the χ2 test. Logistic regression analyses were performed to examine the relationship between CYP2C19 metabolic phenotypes and PCAD. Gender, BMI, history of smoking, history of alcoholism, hypertension, and diabetes mellitus were selected as covariates in the multivariate logistic regression analysis for PCAD, based on estimating the odds ratios (OR) and their 95% confidence intervals (CIs). p<0.05 was considered to represent statistical significance.
Results
Baselines of Subjects
There were 447 (37.8%) patients were males and 736 (62.2%) were females. There were 250 males (39.4%) and 385 females (60.6%) in the PCAD group, 197 males (35.9%) and 351 females (64.1%) in the control group; however the sex distribution difference between the PCAD patients and controls was not statistically significant (p = 0.230). In the controls, there were 14 (2.6%), 249 (45.4%), and 285 (52.0%) patients with BMI <18.5 kg/m2, 18.5–23.9 kg/m2, and ≥24.0 kg/m2, respectively. There were 23 (3.6%) PCAD patients with BMI <18.5 kg/m2 and 360 (56.7%) PCAD patients with BMI ≥24.0 kg/m2, with not statistically significant in the two groups (p = 0.100). The proportion of PCAD patients with a history of smoking (16.9% vs 9.5%, p < 0.001) was significantly higher than controls. The PCAD patients had higher TC (5.21±1.35 vs 4.86±1.15 mmol/L, p < 0.001), TG (2.12±1.72 mmol/L vs 1.83±1.49 mmol/L, p = 0.002), LDL-C (2.97±0.91 mmol/L vs 2.81±0.89 mmol/L, p = 0.002), and Apo-B (0.94±0.26 g/L vs 0.88±0.25 g/L, p < 0.001) levels than controls. The differences of history of alcohol consumption, hypertension, and diabetes mellitus were not statistically significant between the patients and controls (Table 1).
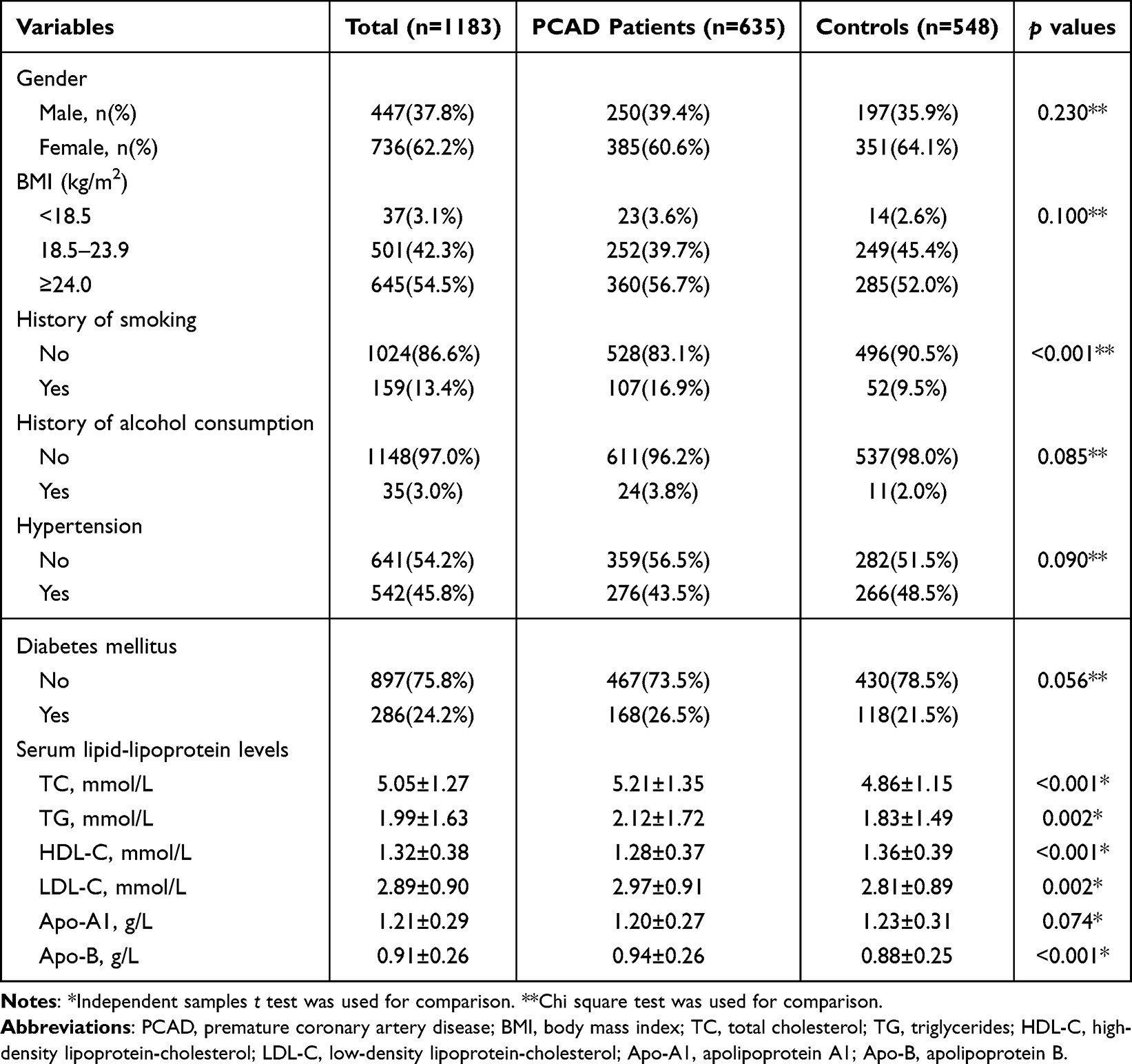 |
Table 1 Clinical Characteristics of the Subjects of This Study |
Distribution Frequencies of the CYP2C19 Genotypes and Alleles in PCAD Patients and Controls
There were 442 (37.4%), 462 (39.1%), 81 (6.8%), 149 (12.6%), 45 (3.8%), and 4 (0.3%) individuals with CYP2C19 *1/*1, *1/*2, *1/*3, *2/*2, *2/*3, and *3/*3 genotype, respectively. There were 442 (37.4%), 543 (45.9%), and 198 (16.7%) individuals with CYP2C19 EM, IM, and PM phenotypes, respectively. CYP2C19 genotypes in the PCAD patients (χ2 = 4.139, p = 0.388), and controls (χ2 = 1.300, p = 0.861) conformed to the Hardy-Weinberg equilibrium, respectively. The frequency of the CYP2C19 *2/*2 genotype was higher (15.0% vs 9.9%, p = 0.008), whereas that of the CYP2C19 *1/*1 genotype was lower in the PCAD patients than controls. The PCAD patients had a higher frequency of the *2 allele (36.3% vs 31.4%, p = 0.013) and a lower frequency of the *1 allele (57.2% vs 63.9%, p = 0.001) than controls (Table 2).
 |
Table 2 Distribution Frequencies of CYP2C19 Genotypes and Alleles in PCAD Patients and Controls |
Clinical Characteristics of Subjects Stratified by CYP2C19 Phenotypes
The proportion of male individuals in CYP2C19 PM group was higher than CYP2C19 EM and IM groups (44.4% vs 34.2% and 38.3%, p = 0.043). The proportion of smoking in CYP2C19 PM group was higher than CYP2C19 EM and IM groups (18.2% vs 10.4% and 14.2%, p = 0.022). The individuals with CYP2C19 PM phenotype had higher TG level than those with CYP2C19 EM and IM phenotypes (2.27±2.04 mmol/L vs 1.85±1.24 mmol/L and 2.00±1.72 mmol/L, p < 0.05) (Table 3).
 |
Table 3 Clinical Characteristics of Subjects Stratified by CYP2C19 Phenotypes |
Logistic Regression Analysis of Risk Factors for PCAD
The results of univariate analysis showed that smoking (odds ratio (OR): 1.933, 95% confidence interval (CI): 1.358–2.752, p < 0.001), diabetes mellitus (OR: 1.311, 95% CI: 1.001–1.716, p = 0.049), CYP2C19 PM phenotype (PM phenotype vs EM phenotype, OR: 1.732, 95% CI: 1.229–2.439, p = 0.002) and CYP2C19 IM+PM phenotypes (IM+PM phenotypes vs EM phenotype, OR: 1.381, 95% CI: 1.091–1.750, p = 0.007) were significantly associated with PCAD. In multivariate logistic regression analysis, BMI ≥24.0 kg/m2 (≥24.0 kg/m2 vs 18.5–23.9 kg/m2, OR: 1.326, 95% CI: 1.041–1.688, p = 0.022), smoking (OR: 1.974, 95% CI: 1.283–3.306, p = 0.002), hypertension (OR: 1.327, 95% CI: 1.044–1.687, p = 0.021), diabetes mellitus (OR: 1.390, 95% CI: 1.054–1.834, p = 0.020), CYP2C19 PM phenotype (PM phenotype vs EM phenotype, OR: 1.701, 95% CI: 1.200–2.411, p = 0.003), and CYP2C19 IM+PM phenotypes (IM+PM phenotypes vs EM phenotype, OR: 1.369, 95% CI: 1.077–1.740, p = 0.010) were associated risk factors for PCAD (Table 4).
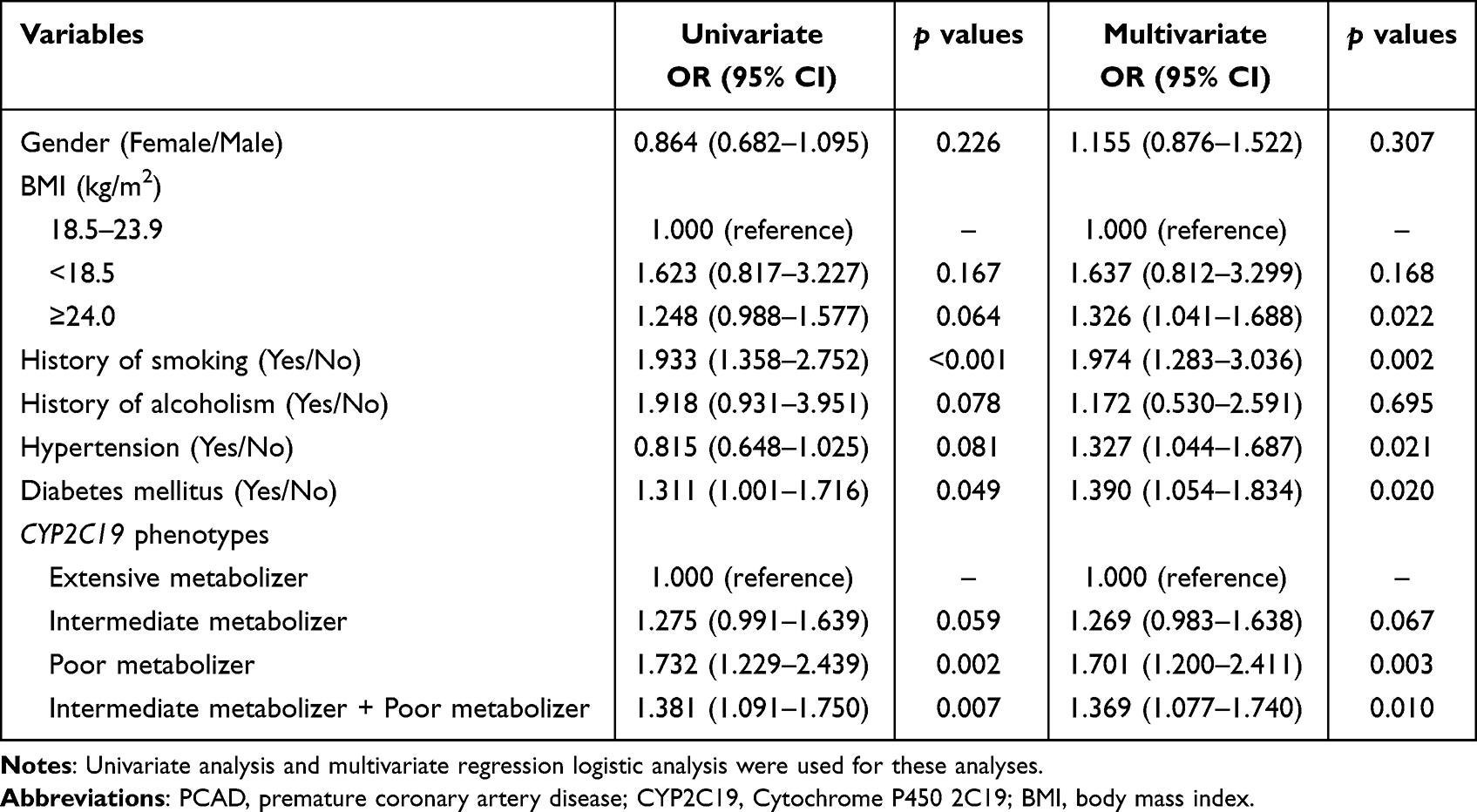 |
Table 4 Logistic Regression Analysis of Risk Factors for PCAD |
Discussion
At present, there are abundant research results on CAD and its risk factors, but it has not been well studied in PCAD. Many studies have ignored the different clinical characteristics and risk factors of patients with different ages, and there is still much space worth exploring. The group covered by PCAD is the main working group of the society, and PCAD is not just the physical damage, but also affect their family life and social production of patients. Therefore, attention should be paid to the identification and screening of people at risk for PCAD, as well as to the determination of risk factors. In terms of mechanism, the metabolite of arachidonic acid (AA) catalysed by CYP450 plays an antihypertensive, anti-inflammatory, and anticoagulant role by activating potassium ion and calcium ion channels, inhibiting platelet aggregation, inhibiting white blood cell adhesion to blood vessel wall, and reducing the expression of vascular cell adhesion molecules.20,21 Nitric oxide produced by 5-hydroxytryptamine (5-HT) catalyzed by CYP450 and catalase can relax blood vessels.41 CYP2C19 is an important member of the CYP450 family, CYP2C19 loss-of-function with only weak enzyme activity, and its metabolites are not enough to maintain the balance of the above processes, so poor metabolizers are more prone to atherosclerosis. CYP2C19 gene polymorphisms have racial differences.35,42 In this study, the relationship of CYP2C19 polymorphisms and susceptibility to PCAD were investigated. BMI ≥24.0 kg/m2, smoking, hypertension, diabetes mellitus, CYP2C19 loss-of-function were associated with PCAD.
There were several reports on the relationship between CYP2C19 polymorphisms and some CVDs susceptibility. CYP2C19*3 was associated with CAD in the Chinese Uyghur population.43 The CYP2C19 PM was a risk factor of CAD in Japanese women.33 CYP2C19 EM was common in CAD patients among a Chinese population.34 Akasaka T et al found that female sex, smoking, and hypertension were associated with coronary microvascular disorder (CMVD), and CYP2C19 PM was predictive factor for CMVD in the female population.44 CAD patients with the CYP2C19 PM phenotype are more likely to experience major adverse cardiovascular and cerebrovascular events (MACCE) after interventional therapy.45 In addition, Cai et al found that CYP2C19 polymorphisms were associated with hypertension susceptibility in the Hakka population.28 Xie et al found that CYP2C19 *2/*2 is a risk factor for multi-site atherosclerosis.46 CYP2C19*2 allele was associated with stent thrombosis after stent implantation in CAD patients.47 Patients with peripheral endothelial dysfunction who carried the CYP2C19*2 or *3 alleles were prone to cardiovascular events.48
CAD may be influenced by environmental factors, living habits, and genetic factors, such as smoking, diabetes, and hypertension are associated with CAD.49,50 Smoking was more common in PCAD patients,51 smoking was associated with multivessel disease PCAD.52 And smoking was a risk for premature multiple CAD in a Chinese population,53 an Iran population.54 Smoking was a major risk for CAD in a rural Indian population.55 Hypertension, diabetes mellitus, and obesity were positively associated with multivessel disease PCAD.52 Diabetes mellitus was an independent risk factor for PCAD.53 Iranian scholars found that diabetes mellitus, smoking, and hypertension were associated with PCAD in Iranian youth.54 A study found that PCAD patients had high levels of BMI, serum TC, TG, and C-reactive protein (CRP) than healthy adults.56 Compared with MCAD patients, the percentages of smoking, abnormal lipid metabolism, and hypertension were higher in PCAD patients.56 PCAD risk was associated with gender differences,57 as well as differences in populations with different traditional lifestyles and genetic backgrounds.58
Moreover, there was a significant difference in the TG levels among different CYP2C19 metabolizers in this study. Specifically, TG level in individuals with CYP2C19 PM phenotype higher than those with CYP2C19 EM phenotype and IM phenotype. Bai et al found that the levels of TC and LDL-C in individuals with CYP2C19 PM phenotype are significantly higher than those in individuals with CYP2C19 EM and IM; however, no differences showed in HDL-C.59 Cai et al found that HDL-C levels vary with CYP2C19 metabolic phenotypes.28 The relationship between CYP2C19 and lipid levels needs more clinical studies and foundation to reveal.
Clinically, when clopidogrel is used for antiplatelet therapy, there are individual differences in treatment effectiveness among patients. Moreover, poor clopidogrel responsiveness is closely associated with the occurrence of major adverse cardiovascular events (MACE) after stenting, a phenomenon called clopidogrel resistance (CR).60,61 The most important internal cause of CR is the difference in metabolic enzyme activity caused by CYP2C19 gene polymorphism.62,63 Many studies have confirmed the association between CYP2C19 loss-of-function and adverse cardiovascular events.64–70 It can be seen that CYP2C19 gene screening can not only be used as a genetic predictor of PCAD but also can effectively help patients select appropriate antiplatelet drugs and dosages.
In this study, CYP2C19 IM + PM phenotypes, overweight, smoking, hypertension, and diabetes mellitus were associated with PCAD. This means that individuals who are overweight, have a history of smoking, hypertension, and diabetes mellitus; and carried the CYP2C19 IM or PM phenotype need to be aware of the risk of developing PCAD. However, this study has some limitations. First, as a retrospective study, the selection of subjects and collection of clinical information in this study may be biased. Second, this study was based on data from a single medical institution, and although data analysis showed that the results were statistically significant, the results of this study require additional data and external case validation. Third, this study did not not analyze the association of CYP2C19 gene polymorphisms with interventional procedures, treatment, and clinical prognosis of PCAD patients.
Conclusion
In summary, CYP2C19 IM+PM phenotypes (CYP2C19 loss-of-function), overweight, smoking, hypertension, and diabetes mellitus are associated risk factors for PCAD. In other words, individuals who are overweight, have a history of smoking, hypertension, diabetes mellitus, and carried the CYP2C19 loss-of-function phenotype are advised to be aware of the risk of PCAD.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
All participants were informed on the study procedures and goals and the informed consent from all the participants. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital.
Acknowledgments
The authors thank their colleagues, who were not listed in the authorship, for their helpful comments on this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program for Social Development of Meizhou (Grant No.: 2023B44).
Disclosure
The authors declare that they have no competing interests.
References
1. Valenzuela PL, Ruilope LM, Santos-Lozano A. Exercise benefits in cardiovascular diseases: from mechanisms to clinical implementation. Eur Heart J. 2023;44(21):1874–1889. doi:10.1093/eurheartj/ehad170
2. Chapman FA, Maguire JJ, Newby DE, Davenport AP, Dhaun N. Targeting the apelin system for the treatment of cardiovascular diseases. Cardiovasc Res. 2023;119(17):2683–2696. doi:10.1093/cvr/cvad171
3. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
4. Writing committee of the report on cardiovascular health and diseases in China. report on cardiovascular health and diseases in China 2021: an updated summary. Biomed Environ Sci. 2022;35(7):573–603. doi:10.3967/bes2022.079
5. Shaya GE, Leucker TM, Jones SR, Martin SS, Toth PP. Coronary heart disease risk: low-density lipoprotein and beyond. Trends Cardiovasc Med. 2022;32(4):181–194. doi:10.1016/j.tcm.2021.04.002
6. Stone PH, Libby P, Boden WE. Fundamental pathobiology of coronary atherosclerosis and clinical implications for chronic ischemic heart disease management-the plaque hypothesis: a narrative review. JAMA Cardiol. 2023;8(2):192–201. doi:10.1001/jamacardio.2022.3926
7. Bauersachs R, Zeymer U, Brière JB, Marre C, Bowrin K, Huelsebeck M. Burden of coronary artery disease and peripheral artery disease: a literature review. Cardiovasc Ther. 2019;2019:8295054. doi:10.1155/2019/8295054
8. Duggan JP, Peters AS, Trachiotis GD, Antevil JL. Epidemiology of coronary artery disease. Surg Clin North Am. 2022;102(3):499–516. doi:10.1016/j.suc.2022.01.007
9. Wang X, Gao M, Zhou S, et al. Trend in young coronary artery disease in China from 2010 to 2014: a retrospective study of young patients ≤ 45. BMC Cardiovasc Disord. 2017;17(1):18. doi:10.1186/s12872-016-0458-1
10. Salomaa V. Worrisome trends in the incidence of coronary artery disease events among young individuals. Eur J Prev Cardiol. 2020;27(11):1175–1177. doi:10.1177/2047487319896051
11. National Cholesterol Education Program (NCEP). Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation. 2002;106(25):3143–3421. PMID: 12485966
12. Medina-Urrutia AX, Martínez-Sánchez FD, Posadas-Romero C, et al. Metabolic control achievement in a population with premature coronary artery disease: results of the genetics of atherosclerotic disease study. Ther Adv Endocrinol Metab. 2020;11:2042018820943374. doi:10.1177/2042018820943374
13. Zeitouni M, Clare RM, Chiswell K, et al. Risk factor burden and long-term prognosis of patients with premature coronary artery disease. J Am Heart Assoc. 2020;9(24):e017712. doi:10.1161/JAHA.120.017712
14. Shao C, Wang J, Tian J, Tang YD. Coronary artery disease: from mechanism to clinical practice. Adv Exp Med Biol. 2020;1177:1–36. doi:10.1007/978-981-15-2517-9_1
15. Dawson LP, Lum M, Nerleker N, Nicholls SJ, Layland J. Coronary atherosclerotic plaque regression: JACC state-of-the-art review. J Am Coll Cardiol. 2022;79(1):66–82. doi:10.1016/j.jacc.2021.10.035
16. Malakar AK, Choudhury D, Halder B, Paul P, Uddin A, Chakraborty S. A review on coronary artery disease, its risk factors, and therapeutics. J Cell Physiol. 2019;234(10):16812–16823. doi:10.1002/jcp.28350
17. Agrawal A, Lamichhane P, Eghbali M. Risk factors, lab parameters, angiographic characteristics and outcomes of coronary artery disease in young South Asian patients: a systematic review. J Int Med Res. 2023;51(8):3000605231187806. doi:10.1177/03000605231187806
18. Li Z, Jiang Y, Guengerich FP, Ma L, Li S, Zhang W. Engineering cytochrome P450 enzyme systems for biomedical and biotechnological applications. J Biol Chem. 2020;295(3):833–849. doi:10.1074/jbc.REV119.008758
19. Stipp MC, Acco A. Involvement of cytochrome P450 enzymes in inflammation and cancer: a review. Cancer Chemother Pharmacol. 2021;87(3):295–309. doi:10.1007/s00280-020-04181-2
20. Fisslthaler B, Fleming I, Busse R. EDHF: a cytochrome P450 metabolite in coronary arteries. Semin Perinatol. 2000;24(1):15–19. doi:10.1016/s0146-0005(00)80048-8
21. Chawengsub Y, Gauthier KM, Campbell WB. Role of arachidonic acid lipoxygenase metabolites in the regulation of vascular tone. Am J Physiol Heart Circ Physiol. 2009;297(2):H495–507. doi:10.1152/ajpheart.00349.2009
22. Froogh G, Garcia V, Laniado Schwartzman M. The CYP/20-HETE/GPR75 axis in hypertension. Adv Pharmacol. 2022;94:1–25. doi:10.1016/bs.apha.2022.02.003
23. Fleming I, Michaelis UR, Bredenkötter D, et al. Endothelium-derived hyperpolarizing factor synthase (cytochrome P450 2C9) is a functionally significant source of reactive oxygen species in coronary arteries. Circ Res. 2001;88(1):44–51. doi:10.1161/01.res.88.1.44
24. Elfaki I, Mir R, Almutairi FM, Duhier FMA. Cytochrome P450: polymorphisms and roles in cancer, diabetes and atherosclerosis. Asian Pac J Cancer Prev. 2018;19(8):2057–2070. doi:10.22034/APJCP.2018.19.8.2057
25. Manna PR, Stetson CL, Slominski AT, Pruitt K. Role of the steroidogenic acute regulatory protein in health and disease. Endocrine. 2016;51(1):7–21. doi:10.1007/s12020-015-0715-6
26. Jamieson KL, Endo T, Darwesh AM, Samokhvalov V, Seubert JM. Cytochrome P450-derived eicosanoids and heart function. Pharmacol Ther. 2017;179:47–83. doi:10.1016/j.pharmthera.2017.05.005
27. Ellithi M, Baye J, Wilke RA. CYP2C19 genotype-guided antiplatelet therapy: promises and pitfalls. Pharmacogenomics. 2020;21(12):889–897. doi:10.2217/pgs-2020-0046
28. Cai N, Li C, Gu X, et al. CYP2C19 loss-of-function is associated with increased risk of hypertension in a Hakka population: a case-control study. BMC Cardiovasc Disord. 2023;23(1):185. doi:10.1186/s12872-023-03207-w
29. Yang E, Kim S, Kim B, et al. Night-time gastric acid suppression by tegoprazan compared to vonoprazan or esomeprazole. Br J Clin Pharmacol. 2022;88(7):3288–3296. doi:10.1111/bcp.15268
30. Amin AM, Sheau Chin L, Azri Mohamed Noor D, SK Abdul Kader MA, Kah Hay Y, Ibrahim B. The personalization of clopidogrel antiplatelet therapy: the role of integrative pharmacogenetics and pharmacometabolomics. Cardiol Res Pract. 2017;2017:8062796. doi:10.1155/2017/8062796
31. Cheng Y, Sun Y, Zhang D, et al. Influence of CYP2C19 genetic variants and smoking on dual antiplatelet efficacy in patients with coronary artery disease. Front Cardiovasc Med. 2023;10:1105001. doi:10.3389/fcvm.2023.1105001
32. Kambhampati NT, Ahamed H, KV K, et al. Cytochrome P450 2C19 polymorphisms and its association with major adverse cardiac events in post-coronary intervention patients on clopidogrel in the tertiary care center. Cureus. 2023;15(2):e34737. doi:10.7759/cureus.34737
33. Hokimoto S, Tabata N, Akasaka T, et al. Gender differences in impact of CYP2C19 polymorphism on development of coronary artery disease. J Cardiovasc Pharmacol. 2015;65(2):148–152. doi:10.1097/FJC.0000000000000171
34. Shi Y, Yang Y, Feng M, et al. Differences in the proportion of CYP2C19 loss-of-function between cerebral infarction and coronary artery disease patients. Int J Gen Med. 2023;16:3473–3481. doi:10.2147/IJGM.S420108
35. Ma L, Yuan Y, Li J, Yu C, Zhao J. Distribution of CYP2C19, ABCB1 and PON1 polymorphisms in Chinese Han, Hui, Uygur and Kazak patients with coronary atherosclerotic heart disease. Int J Immunogenet. 2020;47(6):539–545. doi:10.1111/iji.12511
36. Wang WZ, Wang CY, Cheng YT, et al. Tracing the origins of Hakka and Chaoshanese by mitochondrial DNA analysis. Am J Phys Anthropol. 2010;141(1):124–130. doi:10.1002/ajpa.21124
37. Lee SE, Sung JM, Rizvi A, et al. Quantification of coronary atherosclerosis in the assessment of coronary artery disease. Circ Cardiovasc Imaging. 2018;11(7):e007562. doi:10.1161/CIRCIMAGING.117.007562
38. Liu J, Huang S, Wang X, et al. Effect of the coronary arterial diameter derived from coronary computed tomography angiography on fractional flow reserve. J Comput Assist Tomogr. 2022;46(3):397–405. doi:10.1097/RCT.0000000000001299
39. He W, Li Q, Yang M, et al. Lower BMI cutoffs to define overweight and obesity in China. Obesity. 2015;23(3):684–691. doi:10.1002/oby.20995
40. Tang J, Zhu X, Chen Y, et al. Association of maternal pre-pregnancy low or increased body mass index with adverse pregnancy outcomes. Sci Rep. 2021;11(1):3831. doi:10.1038/s41598-021-82064-z
41. Fradette C, Yamaguchi N, Du Souich P. 5-Hydroxytryptamine is biotransformed by CYP2C9, 2C19 and 2B6 to hydroxylamine, which is converted into nitric oxide. Br J Pharmacol. 2004;141(3):407–414. doi:10.1038/sj.bjp.0705632
42. Wang T, Zhao T, Bao S, et al. CYP2C19, PON1, and ABCB1 gene polymorphisms in Han and Uygur populations with coronary artery disease in Northwestern Xinjiang, China, From 2014 Through 2019. Medicine. 2020;99(29):e20582. doi:10.1097/MD.0000000000020582
43. Yang YN, Wang XL, Ma YT, et al. Association of interaction between smoking and CYP 2C19*3 polymorphism with coronary artery disease in a Uighur population. Clin Appl Thromb Hemost. 2010;16(5):579–583. doi:10.1177/1076029610364522
44. Akasaka T, Hokimoto S, Sueta D, et al. Sex differences in the impact of CYP2C19 polymorphisms and low-grade inflammation on coronary microvascular disorder. Am J Physiol Heart Circ Physiol. 2016;310(11):H1494–1500. doi:10.1152/ajpheart.00911.2015
45. Wang W, Shao C, Xu B, et al. CYP2C19 genotype has prognostic value in specific populations following coronary stenting. Ann Transl Med. 2021;9(13):1066. doi:10.21037/atm-20-7724
46. Xie J, Pan T, Luo W, Zhang S, Fang Y, Xu Z. CYP2C19 *2/*2 genotype is a risk factor for multi-site arteriosclerosis: a hospital-based cohort study. Int J Gen Med. 2023;16:5139–5146. doi:10.2147/IJGM.S437251
47. Luo Y, Zhao YT, Verdo A, Qi WG, Zhang DF, Hu B. Relationship between cytochrome P450 2C19*2 polymorphism and stent thrombosis following percutaneous coronary intervention in Chinese patients receiving clopidogrel. J Int Med Res. 2011;39(5):2012–2019. doi:10.1177/147323001103900548
48. Tabata N, Hokimoto S, Akasaka T, et al. Patients with both CYP2C19 loss-of-function allele and peripheral endothelial dysfunction are significantly correlated with adverse cardiovascular events following coronary stent implantation. J Cardiol. 2016;67(1):104–109. doi:10.1016/j.jjcc.2015.03.010
49. Mehta A, Dhindsa DS, Hooda A, et al. Premature atherosclerotic peripheral artery disease: an underrecognized and undertreated disorder with a rising global prevalence. Trends Cardiovasc Med. 2021;31(6):351–358. doi:10.1016/j.tcm.2020.06.005
50. Jahangiry L, Abbasalizad Farhangi M, Najafi M, Sarbakhsh P. Clusters of the risk markers and the pattern of premature coronary heart disease: an application of the latent class analysis. Front Cardiovasc Med. 2021;8:707070. doi:10.3389/fcvm.2021.707070
51. Fallahzadeh A, Mehraban S, Mahmoodi T. Risk factor profile and outcomes of premature acute coronary syndrome after percutaneous coronary intervention: a 1-year prospective design. Clin Cardiol. 2024;47(1):e24170. doi:10.1002/clc.24170
52. Wei A, Liu J, Wang L, Zheng S, Cong H. Correlation of triglyceride-glucose index and dyslipidaemia with premature coronary heart diseases and multivessel disease: a cross-sectional study in Tianjin, China. BMJ Open. 2022;12(9):e065780. doi:10.1136/bmjopen-2022-065780
53. Du Y, Chen K, Liu E, et al. Gender-specific associations of CD36 polymorphisms with the lipid profile and susceptibility to premature multi-vessel coronary artery heart disease in the Northern Han Chinese. Gene. 2020;753:144806. doi:10.1016/j.gene.2020.144806
54. Poorzand H, Tsarouhas K, Hozhabrossadati SA. Risk factors of premature coronary artery disease in Iran: a systematic review and meta-analysis. Eur J Clin Invest. 2019;49(7):e13124. doi:10.1111/eci.13124
55. Patil RS, Shetty LH, Krishnan S, Trivedi AS, Raghu TR, Manjunath CN. Profile of coronary artery disease in Indian rural youth (< 35 yrs). Indian Heart J. 2020;72(5):394–397. doi:10.1016/j.ihj.2020.08.002
56. Tian R, Zhang LN, Zhang TT, et al. Association between oxidative stress and peripheral leukocyte telomere length in patients with premature coronary artery disease. Med Sci Monit. 2017;23:4382–4390. doi:10.12659/msm.902106
57. Kryczka KE, Kruk M, Demkow M, Lubiszewska B. Fibrinogen and a triad of thrombosis, inflammation, and the renin-angiotensin system in premature coronary artery disease in women: a new insight into sex-related differences in the pathogenesis of the disease. Biomolecules. 2021;11(7):1036. doi:10.3390/biom11071036
58. Babahajiani M, Zarepur E, Khosravi A, et al. Ethnic differences in the lifestyle behaviors and premature coronary artery disease: a multi-center study. BMC Cardiovasc Disord. 2023;23(1):170. doi:10.1186/s12872-023-03192-0
59. Bai Y, Huang R, Wan L, Zhao R. Association between CYP2C19 gene polymorphisms and lipid metabolism in Chinese patients with ischemic stroke. J Int Med Res. 2020;48(7):300060520934657. doi:10.1177/0300060520934657
60. Ali ZO, Bader L, Mohammed S, et al. Effect of CYP2C19 genetic variants on bleeding and major adverse cardiovascular events in a cohort of Arab patients undergoing percutaneous coronary intervention and stent implantation. Pharmacogenet Genomics. 2022;32(5):183–191. doi:10.1097/FPC.0000000000000469
61. Biswas M. Global distribution of CYP2C19 risk phenotypes affecting safety and effectiveness of medications. Pharmacogenomics J. 2021;21(2):190–199. doi:10.1038/s41397-020-00196-3
62. Pradhan A, Bhandari M, Vishwakarma P, Sethi R. Clopidogrel resistance and its relevance: current concepts. J Family Med Prim Care. 2024;13(6):2187–2199. doi:10.4103/jfmpc.jfmpc_1473_23
63. Sun Y, Lu Q, Tao X, Cheng B, Yang G. Cyp2C19*2 polymorphism related to clopidogrel resistance in patients with coronary heart disease, especially in the asian population: a systematic review and meta-analysis. Front Genet. 2020;11:576046. doi:10.3389/fgene.2020.576046
64. Mao L, Jian C, Changzhi L, et al. Cytochrome CYP2C19 polymorphism and risk of adverse clinical events in clopidogrel-treated patients: a meta-analysis based on 23,035 subjects. Arch Cardiovasc Dis. 2013;106(10):517–527. doi:10.1016/j.acvd.2013.06.055
65. Xi Z, Fang F, Wang J, AlHelal J, Zhou Y, Liu W. CYP2C19 genotype and adverse cardiovascular outcomes after stent implantation in clopidogrel-treated Asian populations: a systematic review and meta-analysis. Platelets. 2019;30(2):229–240. doi:10.1080/09537104.2017.1413178
66. Biswas M, Hossain MS, Ahmed Rupok T, Hossain MS, Sukasem C. The association of CYP2C19 LoF alleles with adverse clinical outcomes in stroke patients taking clopidogrel: an updated meta-analysis. Clin Transl Sci. 2024;17(4):e13792. doi:10.1111/cts.13792
67. Biswas M, Sukasem C, Khatun Kali MS, Ibrahim B. Effects of the CYP2C19 LoF allele on major adverse cardiovascular events associated with clopidogrel in acute coronary syndrome patients undergoing percutaneous coronary intervention: a meta-analysis. Pharmacogenomics. 2022;23(3):207–220. doi:10.2217/pgs-2021-0098
68. Biswas M, Kali SK. Association of CYP2C19 loss-of-function alleles with major adverse cardiovascular events of clopidogrel in stable coronary artery disease patients undergoing percutaneous coronary intervention: meta-analysis. Cardiovasc Drugs Ther. 2021;35(6):1147–1159. doi:10.1007/s10557-021-07142-w
69. Biswas M, Kali MSK, Biswas TK, Ibrahim B. Risk of major adverse cardiovascular events of CYP2C19 loss-of-function genotype guided prasugrel/ticagrelor vs clopidogrel therapy for acute coronary syndrome patients undergoing percutaneous coronary intervention: a meta-analysis. Platelets. 2021;32(5):591–600. doi:10.1080/09537104.2020.1792871
70. Biswas M, Rahaman S, Biswas TK, Ibrahim B. Risk of major adverse cardiovascular events for concomitant use of clopidogrel and proton pump inhibitors in patients inheriting CYP2C19 loss-of-function alleles: meta-analysis. Int J Clin Pharm. 2021;43(5):1360–1369. doi:10.1007/s11096-021-01261-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.