Back to Journals » Clinical Ophthalmology » Volume 18
Cyclophotocoagulation versus Ahmed Glaucoma Implant in Neovascular Glaucoma with Poor Vision at Presentation
Authors Alabduljabbar K, Bamefleh DA, Alzaben KA, Al Owaifeer AM, Malik R
Received 12 June 2023
Accepted for publication 19 December 2023
Published 16 January 2024 Volume 2024:18 Pages 163—171
DOI https://doi.org/10.2147/OPTH.S424321
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Khaled Alabduljabbar,1 Dania A Bamefleh,2 Khawlah Adel Alzaben,1 Adi M Al Owaifeer,2,3 Rizwan Malik4
1Fellowship and Residency Training Program, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 2Glaucoma Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 3Ophthalmology Unit, Department of Surgery, College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia; 4Department of Surgery, Sheikh Khalifa Hospital, Abu Dhabi, United Arab Emirates
Correspondence: Khaled Alabduljabbar, Fellowship and Residency Training Program, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia, Email [email protected]
Purpose: To evaluate the outcomes of surgical intervention in eyes with neovascular glaucoma (NVG) and poor vision, comparing the Ahmed glaucoma implant with cyclophotocoagulation (CPC).
Patients and Methods: This study is a double-armed cohort retrospective review of medical records of patients with NVG who had a visual acuity of 20/200 or less and underwent one of the two procedures as a primary intervention: Ahmed glaucoma valve (AGV) or cyclophotocoagulation (CPC). The study was conducted at King Khaled Eye Specialist Hospital in Riyadh, Saudi Arabia, from January 2014 to June 2019, with a total study period of 1 year. The main outcome measures included the surgical success rate, changes in intraocular pressure (IOP), the number of antiglaucoma medications, corrected distance visual acuity, and the reoperation rate for glaucoma.
Results: The preoperative IOP was 40.4 ± 10.6 mmHg (Median 40) in the CPC group and 39.4 ± 10.2 mmHg (Median 40) in the AGV group (P = 0.6). At 1 year, the IOP ranged from 12.5 to 28 mmHg (Median 18) in the CPC group and 14 to 21.5 mmHg (Median 17) in the AGV group (P = 0.016). Survival analysis showed a 51% success rate in the CPC group and an 89% success rate at 1 year in the AGV group (p> 0.0001).
Conclusion: CPC and AGV procedures yielded good outcomes with similar IOP levels 12 months after the surgery. However, AGV demonstrated a higher overall success rate and a lower medication requirement than CPC.
Keywords: neovascular glaucoma, NVG, Ahmed glaucoma valve, Ahmed glaucoma implant, cyclophotocoagulation
Introduction
Neovascular glaucoma (NVG) is a secondary glaucoma that can cause blindness. It is characterized by the development of neovascularization of the iris, elevated intraocular pressure (IOP), and compromised vision.1 NVG can be caused by retinal or ocular ischemia and ocular inflammation.2 It is associated with forming a fibrovascular membrane on the anterior surface of the iris and in the iridocorneal angle of the anterior chamber.3 This fibrovascular membrane invades the anterior chamber, obstructing the aqueous outflow in an open-angle manner. Eventually, it contracts, leading to secondary synechial angle-closure glaucoma with high IOP.4 The development of new vessels in the iris and angle typically occurs prior to the elevation of intraocular pressure (IOP).5 While medical management provides temporary relief, definitive surgical intervention is ultimately necessary.
After successfully managing the neovascular process using anti-vascular endothelial growth factor (VEGF) agents and/or pan laser photocoagulation, surgical intervention becomes the mainstay of glaucoma treatment, with glaucoma drainage devices (GDD) being commonly employed. In poor vision, Cyclophotocoagulation (CPC) is considered an alternative treatment option. However, there is an ongoing debate regarding the comparative risk-benefit ratio of cyclophotocoagulation versus GDD in eyes with poor vision.6–8 While GDDs have traditionally been reserved for eyes with relatively functional vision, there is currently insufficient evidence to favor one intervention over the other in the context of poor vision.
Yildirim et al found no significant difference in the success rate at 24 months between Ahmed valve implantation and diode cyclophotocoagulation in the treatment of NVG.9 However, considering the potential risk of hypotony following transscleral cyclophotocoagulation, as well as the possibility of requiring multiple treatments,10,11 a comparison of outcomes between GDD and cyclophotocoagulation (CPC) in the treatment of NVG is necessary. The objective of this study was to compare the outcomes of the Ahmed Glaucoma Valve (AGV) and CPC in terms of preserving vision in patients with NVG.
Methods
Study Design
The study was conducted at a tertiary eye center in central Saudi Arabia after obtaining approval from the Institution Research Board (2010-R) at King Khaled Eye Specialist Hospital. This retrospective double-arm cohort study included patients with neovascular glaucoma and poor vision who underwent either CPC or AGV as the primary glaucoma procedure between January 2014 and June 2019. The patients were followed up for at least 12 months, and the study adhered to the principles outlined in the Declaration of Helsinki. Due to the retrospective nature of the study, written informed patient consent was waived by the IRB. All data were anonymized for collection and analysis, and this report contains no identifiable information.
Data Collection
Data was collected using a customized data collection sheet. Demographic information, such as age and gender, was recorded for each patient. Preoperative data encompassed visual acuity, IOP, and medication usage. Operative data included the power and timing settings employed for CPC and any surgical complications. Postoperative data were documented at various intervals (Day 1, Week 1, 1 month, 3 months, 6 months, and 12 months) following the procedure. The number of glaucoma medications used during each visit was also recorded.
Surgical Technique
Description of the Ahmed Glaucoma Valve procedure: The AGV implantation followed a standard surgical technique. Initially, a fornix-based conjunctival flap was created in the desired quadrant for implantation. The plate was then fixed approximately 8 mm posterior to the limbus using 9/0 nylon or 9/0 prolene sutures. Next, the tube was trimmed to an appropriate length and inserted into the anterior segment (either anterior or sulcus) through a scleral tunnel created with a 23-gauge needle. To secure the tube, a 9/0 nylon or prolene suture was used 2 mm posterior to its entry point on the sclera. The tube entry site was also covered with donor pericardial tissue (Tutoplast, IOP, Inc, Costa Mesa, CA). Finally, the conjunctiva was sutured to the limbus in a watertight manner using 9/0 vicryl sutures.
Description of the CPC procedure performed with the patient under local or general anesthesia: Adequate access was achieved using a lid speculum. Transillumination of the ciliary body was utilized to confirm its position. The contact G-probe (IRIS Medical Instruments, Inc., Mountain View, CA) was employed for all treatments. Treatment parameters were tailored to each case. Typically, the number of applications ranged from 10 to 40. The starting power was set at 1500 mW for 1500 ms and gradually increased until soft “pops” were heard during treatment. The number of treated quadrants varied, with the superior-temporal quadrant usually spared in the initial treatment session to preserve it for potential future glaucoma surgeries. Areas of scleral thinning and pigmentation were avoided. Subconjunctival dexamethasone was administered after the procedure. Following treatment, topical corticosteroids and atropine were administered. Attempts were made to reduce antiglaucoma medications after the procedure if the IOP response was deemed satisfactory.
Eligibility Criteria
The inclusion criteria were patients with neovascular glaucoma (NVG) clinically diagnosed within the age range of 20 to 80 years. The diagnostic criteria consisted of iris neovascularization, with or without ectropion uveae of the pupillary border, the presence of peripheral anterior synechia, elevated IOP (>21 mmHg), visual acuity of 20/200 or worse, and characteristic visual field defects with glaucomatous optic disc cupping.
Exclusion criteria encompassed blind eyes (with no light perception), pregnant or nursing women, and secondary forms of glaucoma such as endothelial syndrome, epithelial or fibrous down growth, aphakia, vitreous in the anterior chamber, as well as chronic or recurrent uveitis.
Sample Size
A search of the available data revealed that a total of 135 patients (66 who underwent AGV and 69 who received CPC) at King Khaled Eye Specialist Hospital (KKESH) between January 2014 and June 2019 met the visual acuity criteria. All 135 patients were included in the study.
Patients Visits
Baseline demographic and clinical information was collected for the enrolled patients. A total of seven follow-up visits were conducted, including one preoperative visit and six postoperative visits. These visits were numbered as follows: visit 1 (day 1 postoperatively), visit 2 (1 to 2 weeks), visit 3 (1 to 2 months), visit 4 (3 to 5 months), visit 5 (6 to 9 months), and visit 6 (10 to 12 months postoperatively). During each visit, the following examinations were conducted: measurement of Snellen’s visual acuity (VA), IOP, slit lamp biomicroscopy, and ophthalmoscopy.
At each follow-up visit, any postoperative interventions and surgical complications were documented. For patients requiring a reoperation, additional information was collected, including the date of surgery, the type of procedure performed, and the IOP level and number of glaucoma medications before the reoperation.
Outcome Measures
The outcome measures encompass IOP, VA, utilization of medical therapy, the occurrence of surgical complications, and instances of failure. Failure was prospectively determined as an IOP exceeding 21 mm Hg or falling below 5 mm Hg during two consecutive follow-up visits after 3 months, reoperation for glaucoma, or the loss of vision characterized by a perception of light. Reoperation for glaucoma refers to any additional glaucoma surgery necessitating a return to the operating room within the first year following the initial glaucoma surgery.
Eyes that did not meet the failure criteria mentioned above and did not require supplemental medical therapy were considered complete successes. On the other hand, eyes that did not meet the failure criteria but still required medical therapy were categorized as qualified successes.
Snellen VA measurements were converted to logMAR equivalents for the purpose of data analysis, as previously reported. The time to failure was defined as the duration between the surgical treatment and either reoperation for glaucoma, loss of vision characterized by a perception of light, or the occurrence of two consecutive study visits after a three-month period where the patient consistently had high IOP greater than 21 mm Hg or IOP lower than 5 mm Hg.
Statistical Analysis
The data was collected using TakCare (Trakcare Intersystems, Cambridge, MA) and entered into a customized Microsoft Access 2003 spreadsheet (Microsoft, Redmond, WA). After cleaning the data, it was exported to the Statistical Package for Social Sciences (SPSS 25) spreadsheet (IBM, NY, USA). Qualitative variables were presented as numbers and percentages, while quantitative variables were analyzed using distribution curves. For normally distributed variables, mean, and standard deviations were calculated, while for non-normally distributed variables, median and interquartile range were estimated. To compare outcomes between the cases and the comparison group, the Student’s t-test was used for two independent variables, and the chi-square value, degree of freedom, and two-sided p-value were estimated for more than two independent variables. For quantitative variables, the difference in means, its 95% confidence interval, and two-sided p-value was calculated. Nonparametric methods such as the Mann–Whitney U-test and Freedman’s test were used as required to validate comparisons involving non-normally distributed outcome variables. Treatment comparisons for time to failure and time to reoperation for glaucoma were assessed using stratified Kaplan-Meier survival analysis and the Log rank test. Risk factors for failure were evaluated using the Kaplan-Meier survival Log rank test. Multivariate analysis was also performed.
Results
We conducted a review of 69 eyes from 69 patients who underwent CPC and 66 eyes from 66 patients who underwent implantation of the AGV for the management of neovascular glaucoma (NVG). The participant characteristics are outlined in Table 1. Both groups exhibited almost similar profiles in terms of age, sex, lens status, ocular comorbidity, and IOP prior to the proposed surgical management of NVG. However, the CPC group had lower BCVA, a higher number of eyes with a prior previous surgeries and lower number in the previous retinal procedures in compare to the AGV group.
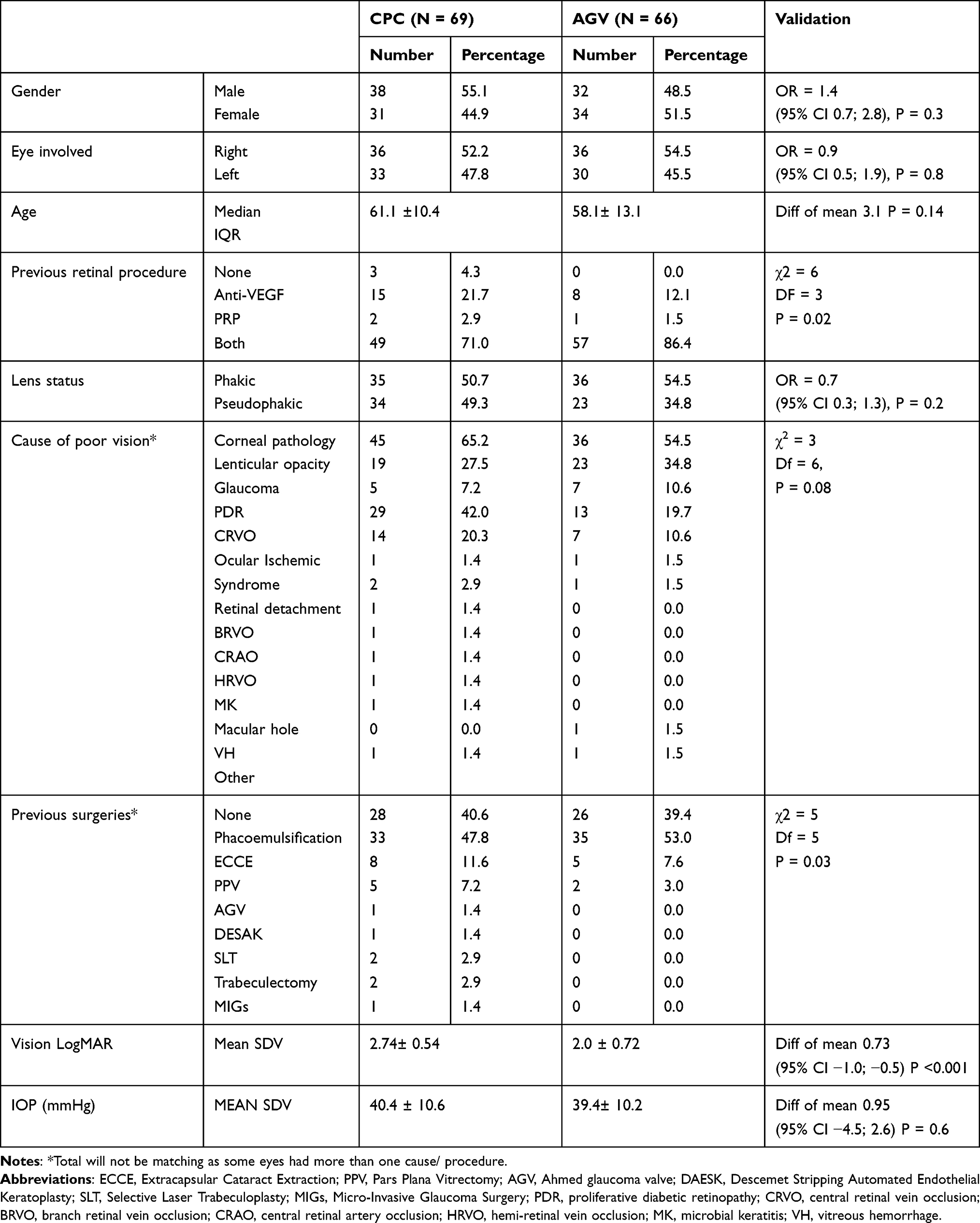 |
Table 1 Profile of Participants |
The AGV group exhibited various intraoperative and postoperative complications, including shallow anterior chamber (4; 6.1%), choroidal effusion (5; 7.6%), hyphema (16; 24.2%), hypotony (3; 4.5%), one case each of encapsulation and tube obstruction (1.5%), aqueous misdirection (2; 3%), and other complications such as loss of vision and phthisis bulbi (3; 4.5%). On the other hand, the complications observed in the CPC group consisted of inflammation (1, 1.4%), hyphema (1, 1.4%), aqueous misdirection (1, 1.4%), and other complications like loss of vision and cataract (1, 1.4%). The incidence of complications in the AGV group was significantly higher compared to that in the CPC group [relative risk (RR) = 10.4 (95% CI: 3.3; 32.1), P < 0.001].
The success and failure rates of the two surgeries for managing NVG were compared based on a definition of success as achieving an IOP within the range of 5 to 21 mmHg. The absolute success rate for IOP control 1 year after CPC was 14.5% (95% CI: 7.3; 21.7), while the absolute success rate for IOP control 1 year after AGV was 15.2% (95% CI: 7.7; 22.7). There was no significant difference in the absolute success rate 1 year after CPC and AGV, with a RR of 1.2 (95% CI: 0.5; 2.7).
The qualified success rate in the CPC group was 49.3% (95% CI: 54.0; 73.6), while the qualified success rate for IOP control 1 year after AGV was 50% (95% CI: 55.3; 75.1). The difference in qualified success rates at 1 year after CPC (49.3%) and AGV (50%) was not statistically significant, with a risk ratio of 1.44 (95% CI: 0.8; 3.7) and a p-value of 0.2.
The difference in failure rates at 1 year after CPC (34.8%) and AGV (21.2%) was not statistically significant, with a risk ratio of 1.44 (95% CI: 0.8; 3.7) and a p-value of 0.2.
The comparison of IOP before and at different follow-ups between the two groups is presented in Table 2. On Day 1, the AGV group exhibited a greater decline in IOP than the CPC group. However, over time, at the 12-month mark with additional management, the difference became similar between the two groups. The preoperative IOP was 40.4 ± 10.6 mmHg in the CPC group and 39.4 ± 10.2 mmHg in the AGV group (P = 0.6). At the 1-year mark, the IOP ranged from 12.5 to 28 mmHg in the CPC group and 14 to 21.5 mmHg in the AGV group (P = 0.016) (Figure 1).
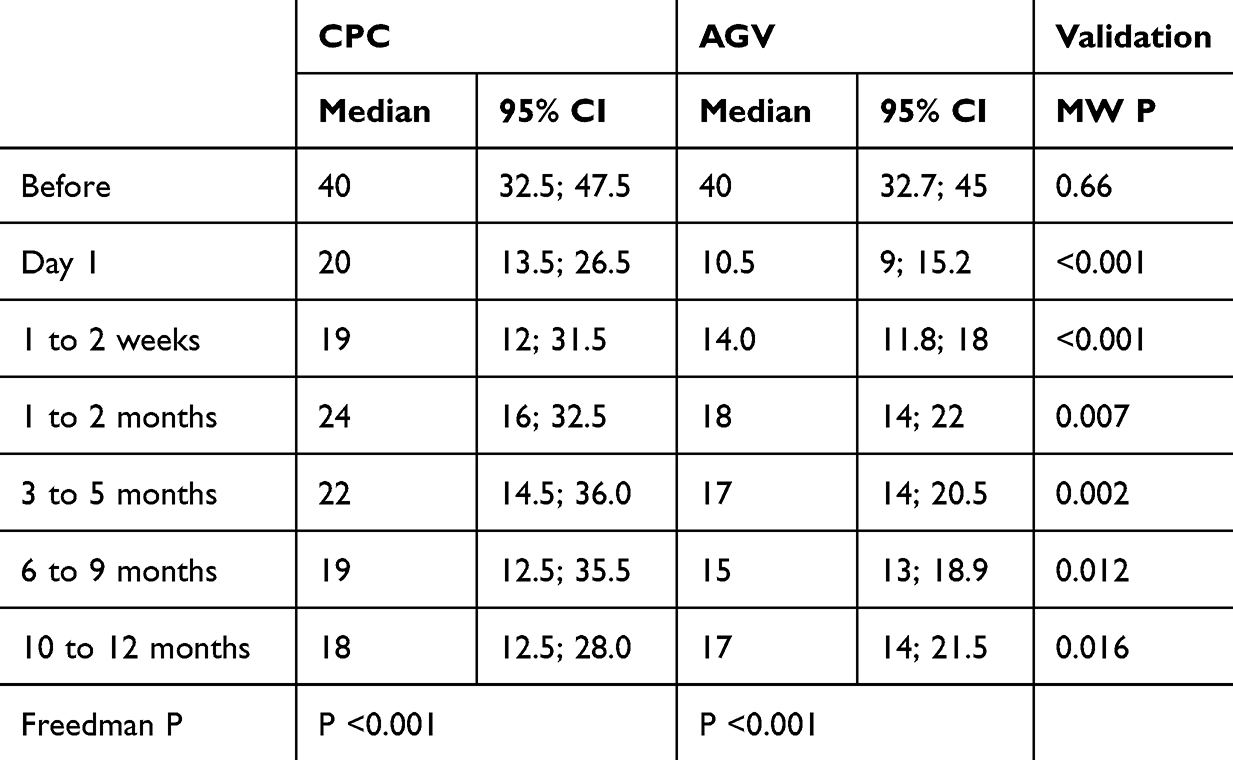 |
Table 2 Changes in IOP at Different Follow-Ups |
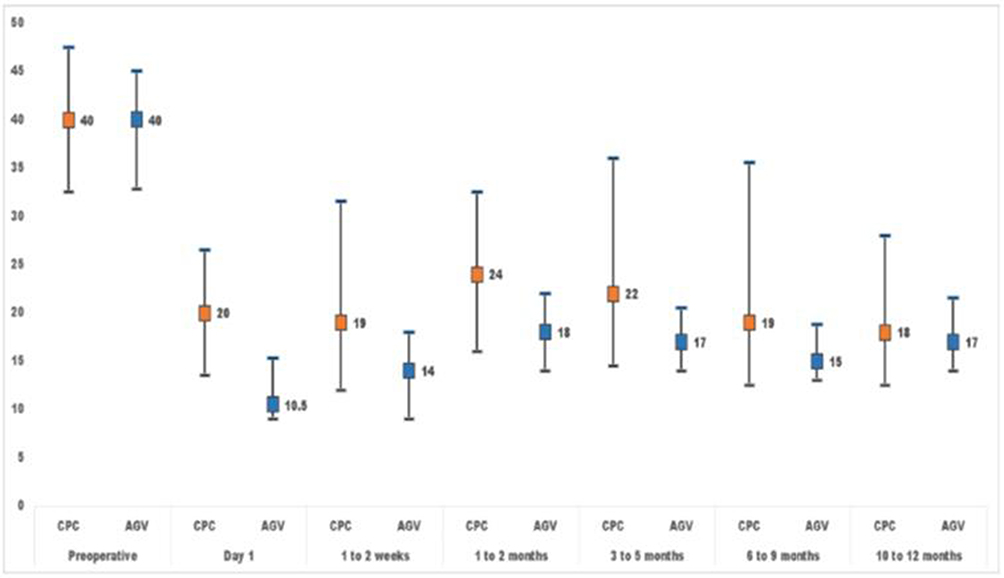 |
Figure 1 Changes of IOP before and at different follow-ups between the two groups. |
The comparison of glaucoma medications before and at different follow-up visits between the CPC and AGV groups is presented in Table 3. In both groups, there was a significant decline in the number of glaucoma medications required at different follow-up visits than before the surgery (Friedman P < 0.001). Additionally, the AGV group required significantly fewer glaucoma medications to control IOP than the CPC group during the follow-up visits (Mann–Whitney U P < 0.001).
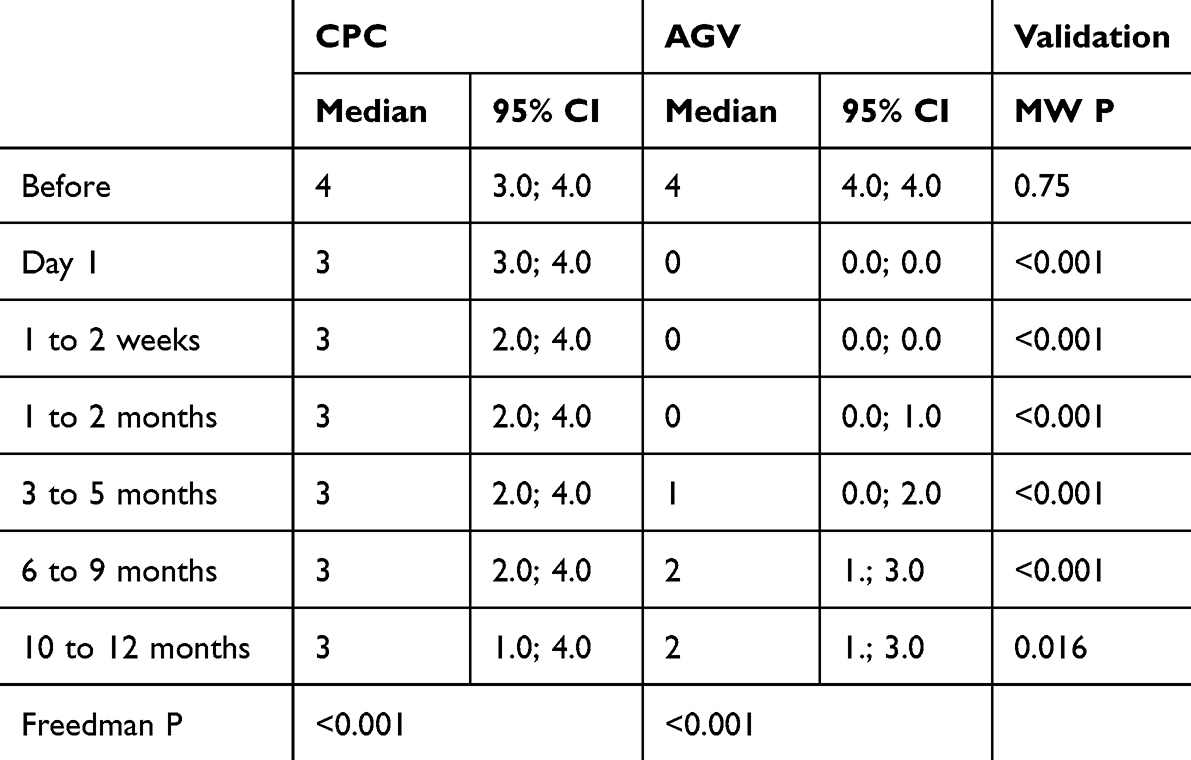 |
Table 3 Glaucoma Medications at Different Follow-Up in Two Groups |
A total of 24 eyes in the CPC group underwent reoperation, while 11 eyes in the AGV group required reoperation. The risk of reoperation in the CPC group (24, 34.8%) was significantly higher compared to the AGV group (11, 16.7%) [Risk Ratio = 2.1 (95% CI: 1.1; 3.9), P = 0.02]. In the CPC group, 14 eyes (20.3%) underwent repeat CPC, seven eyes (10.1%) received AGV, and one eye each underwent ultrasound cyclo-plasty (UCP), another non-valve tube, and trabeculectomy (1.4%). In the AGV group, surgeries performed to control IOP included CPC in seven eyes (10.6%), tube revision in two eyes (3.0%), another non-valve tube in one eye (1.5%), and UCP in one eye (1.5%).
The survival probability of absolute success in maintaining IOP between 5 and 21 mmHg at different follow-up intervals was depicted in Figure 2 to compare the CPC and AGV groups. The survival analysis revealed a 51% success rate in the CPC group and an 89% success rate at 1 year in the AGV group (p > 0.0001).
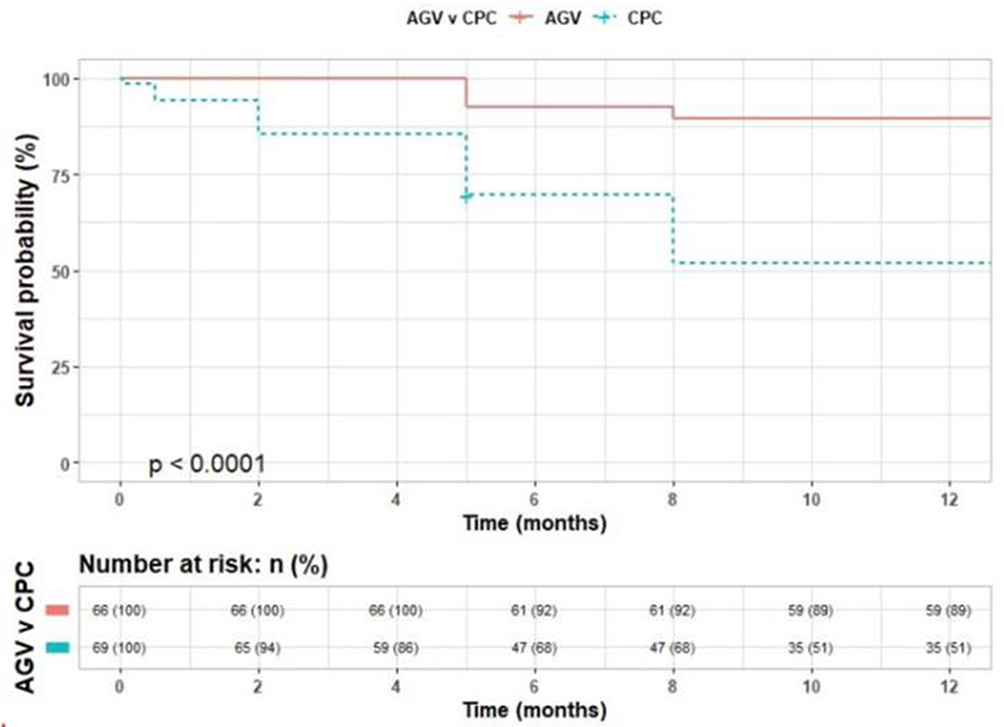 |
Figure 2 The survival probability of absolute success at different follow-ups between the two groups. |
The comparison of presented vision (best-corrected VA (BCVA)) before and at different follow-ups was conducted between the CPC and AGV groups (Table 4). The BCVA in the eyes of the CPC group was initially worse than that in the AGV group before surgery. This difference in BCVA remained consistently and significantly better in the AGV group compared to the CPC group at various follow-ups. Both groups demonstrated a significant improvement in BCVA at different follow-ups compared to the preoperative BCVA (Friedman P < 0.001).
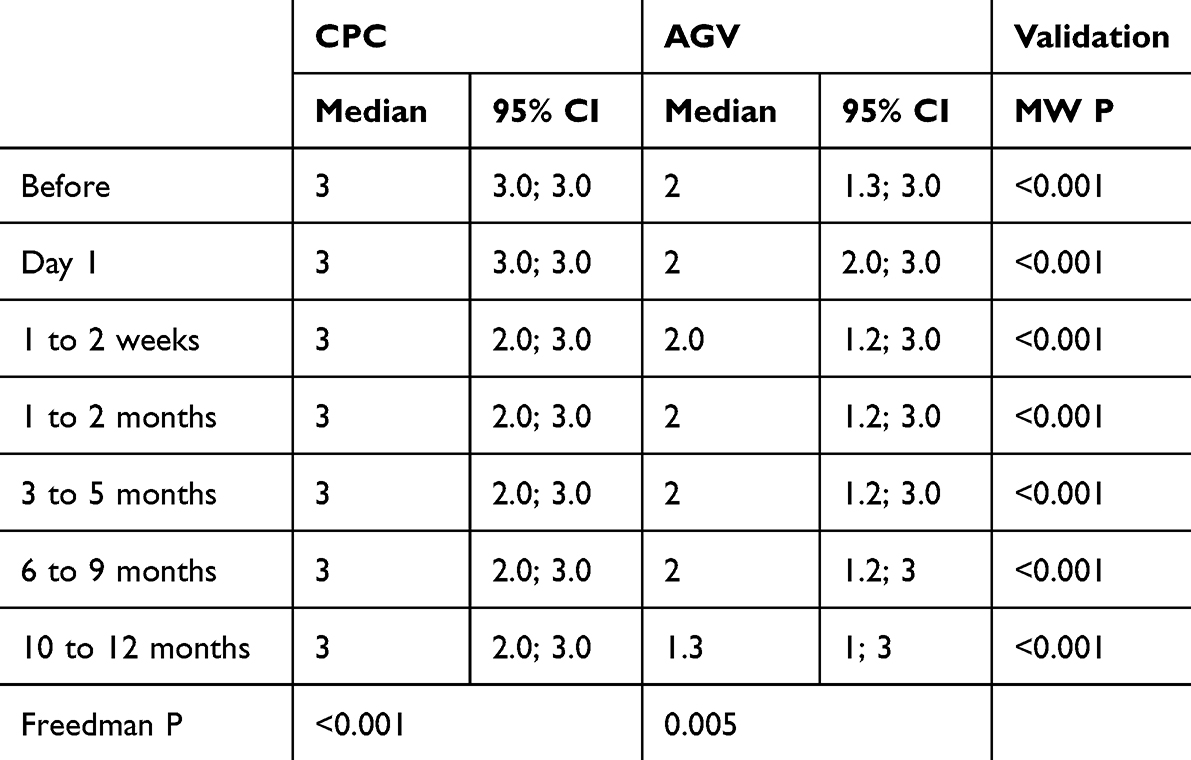 |
Table 4 Changes in Vision at Different Visits in CPC Vs AGV Group |
Discussion
Neovascular glaucoma (NVG) is a challenging secondary form of glaucoma associated with a poor prognosis. The primary objective of treatment is to manage the underlying cause of NVG, which is posterior segment ischemia leading to neovascularization. Treatment options include pan-retinal photocoagulation and anti-VEGF therapy.4 In cases where initial medical management fails, various interventions have been proposed, such as trabeculectomy with mitomycin c (MMC), CPC, and the use of GDD like the AGV.1
Limited data comparing the long-term success rates of cyclophotocoagulation (CPC) and AGV implantation in neovascular glaucoma (NVG) patients can be found in the literature.12 Our study aimed to compare the success rates of CPC and AGV implantation in NVG patients. Our findings revealed that the success rate at the 1-year follow-up was 89% for the AGV group compared to 51% for the CPC group (p<0.0001) (Figure 2). Lima et al12 conducted a study comparing the long-term results of endoscopic cyclophotocoagulation (CPC) and AGV implantation and reported no significant difference in success rates. Additionally, Yildirim et al9 recently compared the success rates of CPC and AGV for NVG at 24 months, which were found to be 63.6% and 59.3%, respectively, with no significant difference (P>0.05). However, Chalam et al13 compared the success rates of pars plana Baerveldt tube surgery with cyclo-YAG laser treatment at the 6-month follow-up and concluded that outcomes for NVG were better with pars plana Baerveldt tube surgery.
In our study, both CPC and AGV demonstrated significant reductions in IOP. In the CPC group, the mean preoperative IOP of 40.4 ± 10.6 mmHg decreased to a range of 12.5–28 mmHg at the 1-year follow-up (Table 2). Similarly, in the AGV group, the preoperative IOP of 39.4 ± 10.2 mmHg decreased to a range of 14–21.5 mmHg at the 1-year follow-up. Comparing the two groups, we observed that the AGV group had lower IOP levels within the first two weeks after surgery (P<0.001). However, at the 1-year mark, the CPC group had slightly higher IOP levels (P = 0.016). In contrast, Yildirim et al9 found that the AGV group had slightly higher IOP levels 1 year after surgery, but the difference between the two groups was not statistically significant.
Both CPC and AGV implantation procedures are associated with potential complications. Our study found that eyes undergoing AGV implantation experienced a higher rate of complications than those treated with CPC. The main complications observed in the CPC group included inflammation, hyphema, and aqueous misdirection. On the other hand, the AGV group experienced complications such as the shallow anterior chamber, choroidal effusion, hyphema, hypotony, encapsulated bleb, tube obstruction, and aqueous misdirection. Schwartz et al14 conducted a study that demonstrated tube shunt implantation had additional complications not observed in CPC procedures, including tube exposure, diplopia, and cystic bleb formation. Similarly, in a recent study by Mistlberger et al,15 anterior chamber inflammation and hyphema were the most frequently observed complications following CPC, which aligns with the findings of our study.
Conclusion
Both CPC and AGV procedures have demonstrated favorable outcomes, with similar IOP levels observed at 10 to 12 months post-procedure. Additionally, the AGV group required a lower number of medications compared to the CPC group. AGV exhibits a higher success rate, primarily attributed to its reduced need for additional surgical interventions compared to CPC. Based on our findings, we recommend that AGV be considered the first-line treatment in the management of neovascular glaucoma (NVG) whenever feasible.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rodrigues GB, Abe RY, Zangalli C, et al. Neovascular glaucoma: a review. Int J Retina Vitreous. 2016;2:26. doi:10.1186/s40942-016-0051x
2. Shazly TA, Latina MA. Neovascular glaucoma: etiology, diagnosis and prognosis. Semin Ophthalmol. 2009;24(2):113–121. doi:10.1080/08820530902800801
3. Hayreh SS. Neovascular glaucoma. Prog Retin Eye Res. 2007;26(5):470–485. doi:10.1016/j.preteyeres.2007.06.001
4. Wang JW, Zhou MW, Zhang X, et al. Short-term effect of intravitreal ranibizumab on intraocular concentrations of vascular endothelial growth factor-A and pigment epithelium-derived factor in neovascular glaucoma. Clin Exp Ophthalmol. 2015;43(5):415–421. doi:10.1111/ceo.12477
5. Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med. 1994;331(22):1480–1487. doi:10.1056/NEJM199412013312203
6. Iliev ME, Domig D, Wolf-Schnurrbursch U, Wolf S, Sarra GM. Intravitreal bevacizumab (Avastin) in the treatment of neovascular glaucoma. Am J Ophthalmol. 2006;142(6):1054–1056. doi:10.1016/j.ajo.2006.06.066
7. Sivak-Callcott JA, O’Day DM, Gass JD, Tsai JC. Evidence-based recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmology. 2001;108(10):1767–1776. doi:10.1016/s0161-6420(01)00775-8
8. Yalvac IS, Eksioglu U, Satana B, Duman S. Long-term results of Ahmed glaucoma valve and Molteno implant in neovascular glaucoma. Eye. 2007;21(1):65–70. doi:10.1038/sj.eye.6702125
9. Yildirim N, Yalvac IS, Sahin A, Ozer A, Bozca T. A comparative study between diode laser cyclophotocoagulation and the Ahmed glaucoma valve implant in neovascular glaucoma: a long‑term follow‑up. J Glaucoma. 2009;18:192–196. doi:10.1097/IJG.0b013e31817d235c
10. Iliev ME, Gerber S. Long-term outcome of trans-scleral diode laser cyclophotocoagulation in refractory glaucoma. Br J Ophthalmol. 2007;91(12):1631–1635. doi:10.1136/bjo.2007.116533
11. Ramli N, Htoon HM, Ho CL, Aung T, Perera S. Risk factors for hypotony after transscleral diode cyclophotocoagulation. J Glaucoma. 2012;21(3):169–173. doi:10.1097/IJG.0b013e318207091a
12. Lima FE, Magacho L, Carvalho DM, et al. A prospective, comparative study between endoscopic cyclophotocoagulation and the Ahmed drainage implant in refractory glaucoma. J Glaucoma. 2004;13:233–237. doi:10.1097/00061198-200406000-00011
13. Chalam KV, Gandham S, Gupta S, Tripathi BJ, Tripathi RC. Pars plana modifid Baerveldt implant versus neodymium: YAG cyclophotocoagulation in the management of neovascular glaucoma. Ophthalm Surg Lasers. 2002;33:383–393. doi:10.3928/1542-8877-20020901-08
14. Schwartz KS, Lee RK, Gedde SJ. Glaucoma drainage implants: a critical comparison of types. Curr Opin Ophthalmol. 2006;17:181–189. doi:10.1097/01.icu.0000193080.55240.7e
15. Mistlberger A, Liebmann JM, Tschiderer H, Ritch R, Ruckhofer J, Grabner G. Diode laser transscleral cyclophotocoagulation for refractoryglaucoma. J Glaucoma. 2001;10:288–293. doi:10.1097/00061198-200108000-00008
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.