Back to Journals » Clinical Ophthalmology » Volume 19
Cyclodialysis Surgery for Glaucoma Management: A Systematic Review and Meta-Analysis of 100 Years of Clinical Evidence
Authors Stamper R, Huang A, Toris C, Qiu M ![]() , Gray G, Garg R, Ianchulev T
, Gray G, Garg R, Ianchulev T ![]()
Received 10 June 2025
Accepted for publication 4 August 2025
Published 21 August 2025 Volume 2025:19 Pages 2859—2870
DOI https://doi.org/10.2147/OPTH.S538438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Robert Stamper,1 Alex Huang,2 Carol Toris,3 Mary Qiu,4 Gerry Gray,5 Reena Garg,6 Tsontcho Ianchulev7
1UCSF Department of Ophthalmology, University of California San Francisco, San Francisco, CA, USA; 2Shiley Eye Institute, UCSD, San Diego, CA, USA; 3Department of Ophthalmology, The Ohio State University, Columbus, OH, USA; 4Cleveland Clinic Department of Ophthalmology, Cleveland, OH, USA; 5Data-Fi, LLC Biostatistics, Los Angeles, CA, USA; 6Department of Ophthalmology, Georgetown University, Washington, DC, USA; 7New York Eye and Ear of Mount Sinai, Icahn School of Medicine, New York City, NY, USA
Correspondence: Tsontcho Ianchulev, Email [email protected]
Synopsis: A meta-analysis of over 4000 glaucoma cases over 100 years of surgical experience demonstrates that cyclodialysis surgery is effective in lowering intraocular pressure (IOP) as an uveoscleral outflow enhancing procedure.
Objective: To conduct a systematic review and meta-analysis evaluating the clinical efficacy and safety of surgical cyclodialysis in lowering intraocular pressure in glaucoma patients.
Methods: A comprehensive search of PubMed, Cochrane, Web of Science, and EMBASE identified peer-reviewed interventional studies involving surgical cyclodialysis for IOP reduction. Key outcome measures included long-term IOP control, medication burden, and adverse event incidence. The meta-analysis was registered with PROSPERO (ID: CRD42025632759).
Results: Forty studies spanning more than a century and including 4082 eyes were analyzed. Most studies were observational and non-randomized, with 75% employing ab-externo and 25% ab-key techniques. Given the evolution of surgical techniques and populations over time, analyses accounted for heterogeneity in outcome reporting. Across all studies, the average qualified success rate was 72.3% (range: 33– 97%) over follow-up periods of 6 to 132 months. Ab-interno approaches showed slightly higher efficacy and fewer complications. Durability varied, with reduced outcomes in refractory and advanced glaucoma. Complications such as hyphema, hypotony, and vision loss were infrequent. Notably, newer ab-interno techniques demonstrated improved outcomes in IOP reduction, safety, and procedural longevity.
Conclusion: Cyclodialysis remains a viable and effective surgical option for enhancing uveoscleral outflow in glaucoma management. While outcomes vary by patient severity and surgical technique, particularly with older methods, modern ab-interno approaches offer enhanced efficacy and safety—especially in mild to moderate cases.
Keywords: cyclodialysis, uveoscleral outflow, interventional glaucoma treatment, MIGS, glaucoma
Introduction
Glaucoma is the leading cause of irreversible blindness worldwide, affecting over 80 million people.1 Treatment options are aimed at lowering Intraocular Pressure (IOP) starting with medications or laser trabeculoplasty2,3 as a first-line treatment, followed by surgical intervention if pharmacotherapy fails. The major objective of surgical glaucoma management involves enhancing aqueous humor drainage, either through ab-interno procedures targeting the trabecular or uveoscleral outflow pathways, or externally via transscleral filtration techniques, such as trabeculectomy and glaucoma drainage devices (GDDs).4–6
Cyclodialysis, first introduced by Leopold Heine in 1905 enhances uveoscleral outflow. It was one of the more prevalent surgical treatments in until the 1960’s before the advent of trabeculectomy and glaucoma drainage implants. The more recent innovations of ab-interno suprachoroidal stents and the emergence of MIGS have renewed interest in cyclodialysis as a minimally-invasive approach to the uveoscleral space.7,8 This technique has had over a century of clinical practice with variable acceptance. Mechanistically, cyclodialysis involves the creation of an internal aqueous outflow channel, facilitating egress through the uveoscleral pathway via the suprachoroidal and trans-scleral routes.9 The goal of cyclodialysis is to augment the native uveoscleral outflow pathway through an iatrogenically created cleft that acts as an aqueous conduit and ab-interno filtration reservoir. Cyclodialysis clefts appear to play a role in the natural physiology of uveoscleral outflow. Small endogenous ciliary body clefts have been documented in histological sections and during ocular patient imaging.10–14 These clefts are felt to be important for uveoscleral outflow as their presence or absence correlates with higher or lower uveoscleral outflow in both animals and humans.10–12 The creation of a surgical cyclodialysis is intended to further augment the uveoscleral outflow capacity of the endogenous clefts for the lowering of IOP.
The uveoscleral pathway provides a potentially advantageous surgical target due to its function as a low-resistance sink for aqueous drainage. From studies of the pharmacologic treatment of glaucoma, selective agents for uveoscleral outflow, such as prostaglandin analogues, have been shown to have a higher therapeutic index for aqueous drainage enhancement compared to trabecular outflow drugs. The intrinsic pressure gradient between the anterior chamber and the supraciliary space, coupled with the absorptive properties of the choroid, generates highly favorable conditions for internal aqueous outflow.15 The osmotic gradient across the choriocapillaris is essential in promoting fluid movement in response to the hydrostatic pressure differential between the anterior chamber and the suprachoroidal space.15–17 Notably, while uveoscleral outflow typically functions as a pressure-independent mechanism, the introduction of a cyclodialysis cleft reduces ciliary muscle resistance, rendering the outflow pressure-dependent.18,19 Physiological studies indicate that uveoscleral outflow accounts for approximately 40% to 50% of aqueous drainage in humans and non-human primates, with higher rates observed in pediatric populations, which gradually decrease with age.16,20,21 Moreover, unlike perforating procedures such as trabeculectomy and drainage implants, cyclodialysis provides MIGS-like benefits without the need to manage bleb-related complications, while maintaining the integrity of the conjunctiva and ocular surface.
The surgical technique for the creation of an iatrogenic cyclodialysis has undergone significant refinements over the past century. Heine’s original ab-externo approach, known as the classical cyclodialysis,22 involved a limbus-based concentric ab-externo scleral incision positioned 5 mm posterior to the limbus. A spatulated instrument was then used to disinsert the ciliary body and create the cleft. Over time, advancements in surgical instrumentation facilitated a shift towards a more interventional ab-interno technique in order to minimize tissue trauma and better surgical control and visualization of the cyclodialysis construction. More recent modifications include various strategies to reinforce the filtration channel to increase durability of the internal filtration channel and reduce the risk of closure and restenosis. These reinforcement techniques involve the use of air, viscoelastic substances, scleral allografts, and other scaffolding materials to maintain patency of the cyclodialysis cleft.
Despite the advent of MIGS and conventional filtration surgeries, cyclodialysis remains a valuable, albeit underutilized, option for enhancing uveoscleral outflow. This systematic review synthesizes over a century of peer-reviewed clinical evidence on the efficacy and safety of cyclodialysis surgery, contextualized within the modern era of emerging surgical innovations, including MIGS procedures and advanced uveoscleral outflow interventions.
Methods
Search Strategy and Study Selection
A comprehensive literature search encompassing the PubMed, Cochrane, Web of Science, and EMBASE databases was conducted to identify studies published between 1905 and 2024. The following search terms were applied: “glaucoma” “open angle glaucoma” “closed angle glaucoma” “mixed mechanism glaucoma” “secondary glaucoma” “congenital glaucoma” (population), “cyclodialysis” “ab-interno cyclodialysis” “ab-externo cyclodialysis” (intervention), and “intraocular pressure” (outcome). Synonymous terms were combined using the Boolean operator “OR”, and primary concepts were linked using “AND”. A supplementary search excluded the outcome term to capture earlier studies lacking standardized endpoints. The search encompassed all glaucoma populations. Titles, abstracts, and full texts were meticulously screened to ensure consistency with analytical specifications.
No additional restrictive terms were used for any of the databases and a broad inclusion criteria were maintained to minimize the risk of bias. Extracted outcomes were systematically tabulated from each study. Due to the heterogeneity and variability of outcome measures reported over a century of publications, multiple outcomes were extracted where available. The most consistently reported outcome across historic and contemporary studies was the percentage of patients achieving post-operative success in terms of “qualified” intraocular pressure (IOP) control. Given the heterogeneity in how successful IOP control was defined across studies, and the lack of access to individual patient-level data, we adopted the proportion of subjects achieving qualified postoperative success (with or without adjunctive IOP-lowering medications), as reported by the original authors, as the primary efficacy endpoint. Where available, mean changes in medicated IOP from baseline were also included from a subset of recent studies. Efficacy and safety outcomes were extracted from the longest reported follow-up for each study, and the incidence of procedure-related ocular adverse events was systematically assessed.
Analysis Methods
Meta-analytic methods were used to summarize qualified success outcomes from the 40 included studies. Procedure types were defined and analyzed by group: ab-externo, ab-interno, ab-interno with sub-scleral reinforcement of the cleft, stand-alone procedures and procedures in combination with other surgery (eg cataract surgery). Due to smaller numbers some subgroupings could not be statistically characterized.
The base model was a random-effects meta-analysis, with study as the random effect, assuming that each study has a true qualified success ratepi and that these pi follow a normal distribution. Studies were weighted relative to sample size. An additional fixed effect was added to the base model to investigate the effect of each of: procedure type, approach, stand-alone versus combination procedures, year published, and follow-up time. Each fixed effect was evaluated in a separate analysis using a mixed effects model with study as the random effect. Estimates, standard errors, and confidence intervals are calculated based on the fitted random effects or mixed effects model. Fitting was carried out using R version 4.3.0 and the R package for version 4.6–0. REML methods were used in the fitting. The meta-analysis was registered with PROSPERO ID CRD42025632759.
Results
Study Selection and Data Extraction
In the EMBASE database, 828 research articles met the initial search criteria for cyclodialysis, while 202 references met the criteria in PubMed as of 12/14/2024. The initial search of Web of Science yielded 164 citations. A systematic review applying additional restriction criteria focused on treatment-specific cyclodialysis in glaucoma patients, thereby excluding studies of traumatic or iatrogenic cyclodialysis, suprachoroidal aqueous drainage devices, epidemiologic studies, veterinary reports, and non-surgical investigations. The dataset was further enriched by including pre-1950 publications referenced in the reviewed literature. Ultimately, 40 studies encompassing 4082 surgical cases were included in the final analysis. The steps and the results of the PRISMA procedure are summarized in Figure 1.
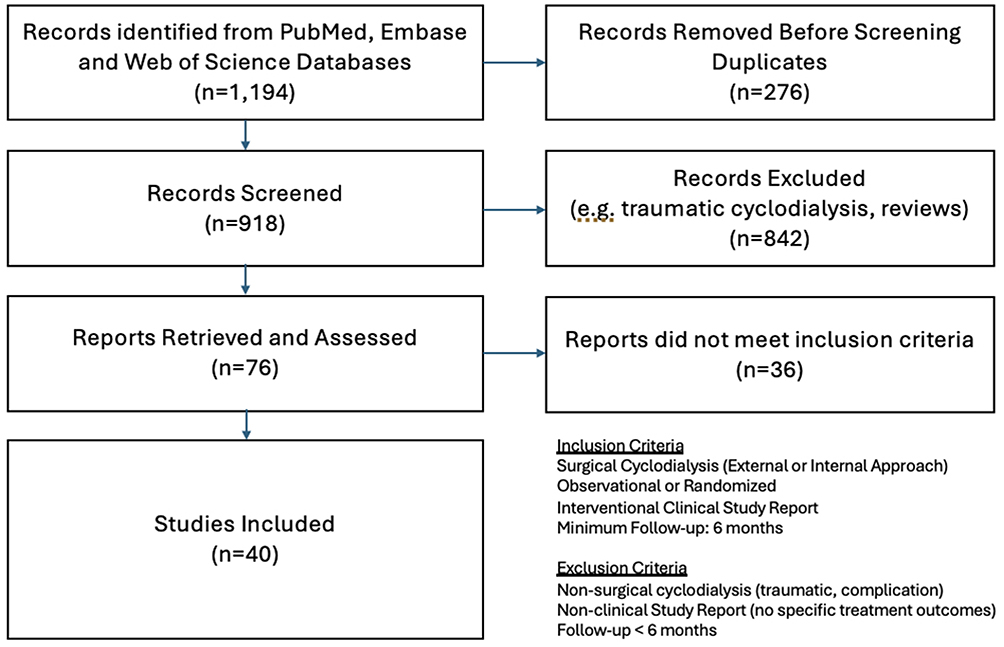 |
Figure 1 PRISMA Flowchart. |
All the studies were further assessed and categorized for the level of bias using the ROBINS-I v2 systematic tool (https://sites.google.com/site/riskofbiastool/welcome/robins-i-v2). Given the non-randomized, uncontrolled, observational nature of the peer-review dataset, there were no studies in the low-risk category. All studies were in the moderate-high risk categories.
Follow-up durations ranged from 6 to 132 months, and the patient cohort spanned a wide patient age group - from a pediatric population (<1 year) to elderly patients (>90 years). The studies included a diverse range of glaucoma subtypes, such as primary and secondary open-angle glaucoma as well as angle-closure glaucoma. Cyclodialysis techniques varied across studies, with earlier publications focusing on standard ab-externo procedures and more recent studies emphasizing ab-interno approaches. Several studies incorporated adjunct cataract procedures and sub-scleral reinforcements to enhance the durability and efficacy of cyclodialysis surgery. Table 1 summarizes the characteristics of the included studies.
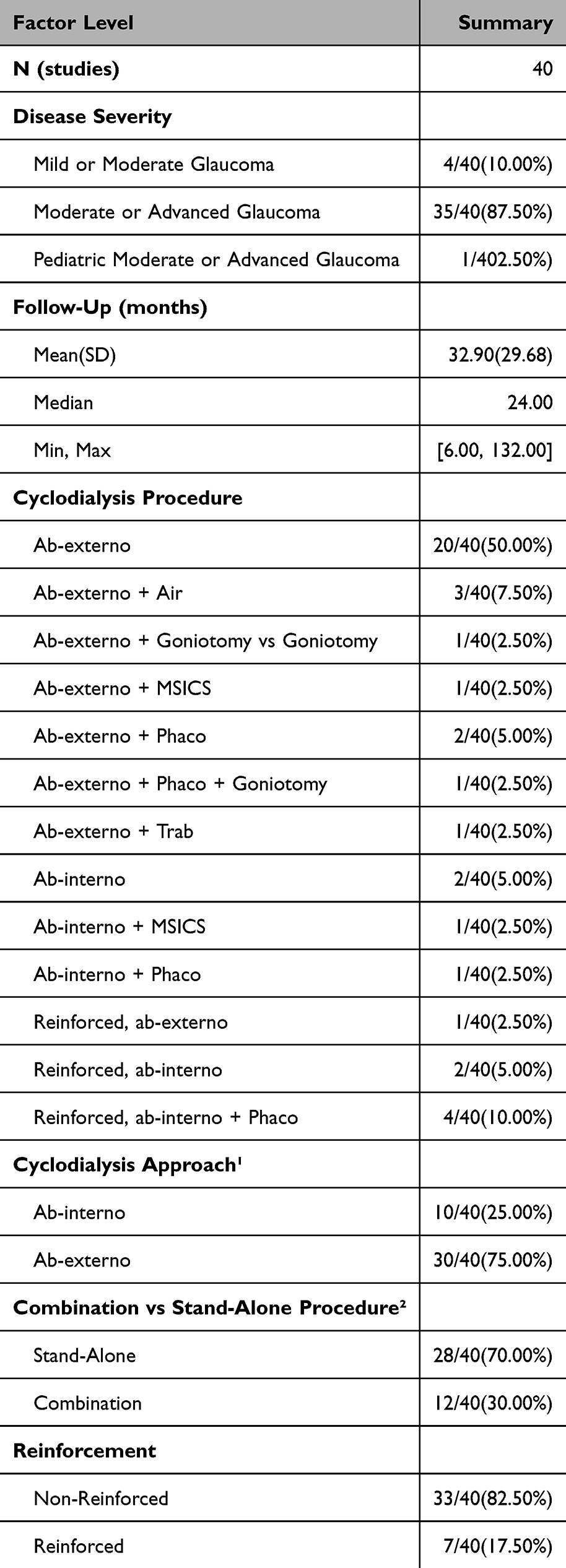 |
Table 1 Summary of Study Characteristics |
Summary of Systematic Analysis
All included studies were observational, comprising both retrospective and prospective designs; no randomized controlled trials (RCTs) were identified in the peer-reviewed literature (Table 1). Among the 40 studies involving 4082 patients, 30 studies (3183 patients) evaluated cyclodialysis performed through an external surgical approach (ab-externo), while 10 studies (899 patients) assessed interventional cyclodialysis using an internal approach (Tables 2 and 3). For analysis purposes the ab-interno and ab-interno + reinforced studies are grouped together as ab-interno and the combination procedures include cyclodialysis performed with another ophthalmic procedure (eg Phaco, Goniotomy, MSICS, or Trabeculectomy). A comprehensive list of the studies with the corresponding citations is included in Table s1.
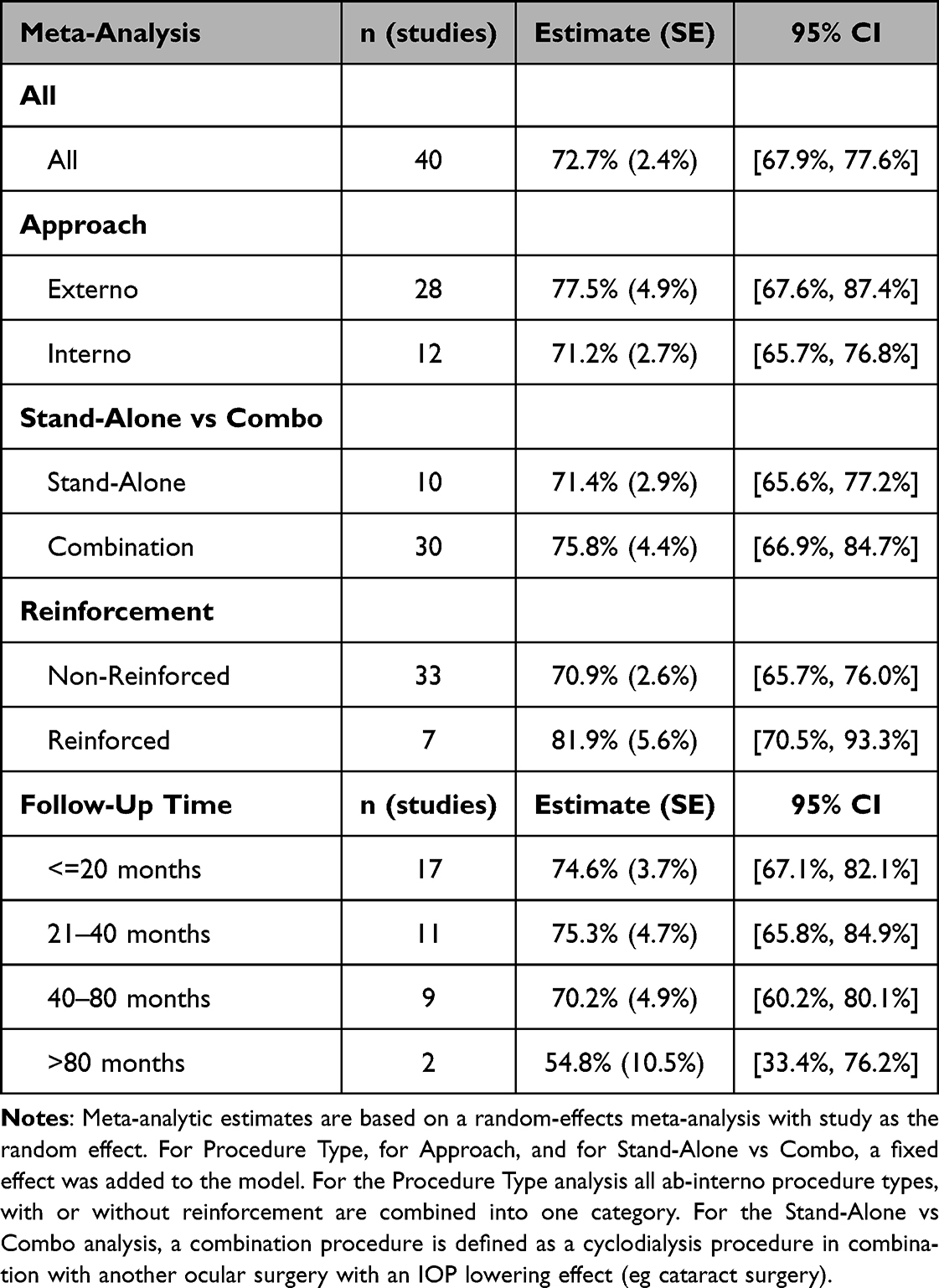 |
Table 2 Meta-Analysis of Qualified Success Rates: Overall, with Fixed Effect for Procedure Type, with Fixed Effect for Approach, and with Fixed Effect for Stand-Alone/Combination |
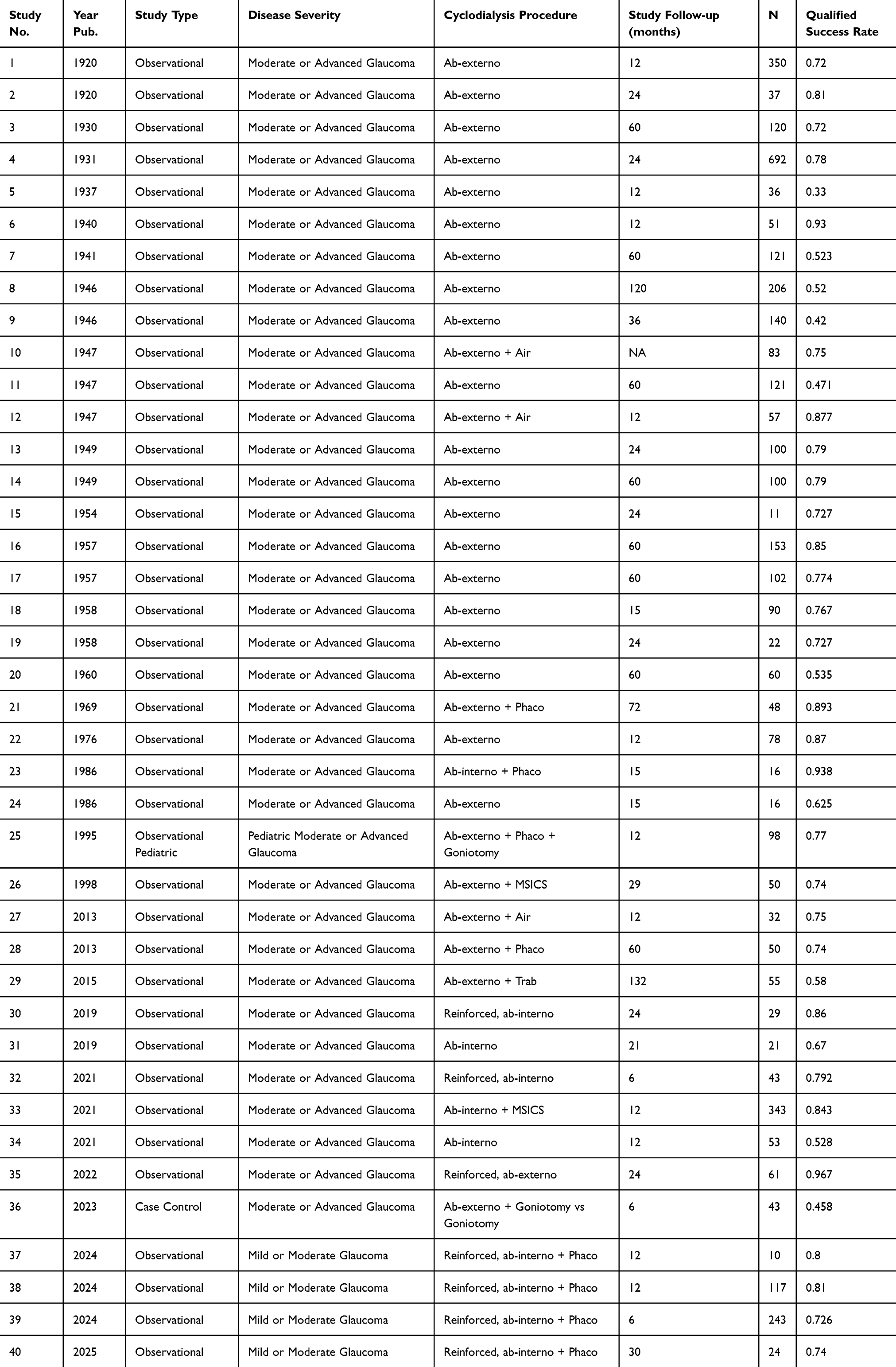 |
Table 3 Final List of Studies Included in the Evidence-Based Review of Cyclodialysis Surgical Treatment |
Meta-Analysis of Outcomes
The estimated overall qualified success rate from the meta-analysis across all studies was 72.7%, with a 95% CI of [67.7%, 77.6%]. Outcomes were similar regardless of Procedure Type, Approach, or Stand-Alone versus Combination procedures. Formal statistical tests of the fixed effects for procedure type, approach, and stand-alone vs combination were not significant (Table 2, Figures 2 and 3).
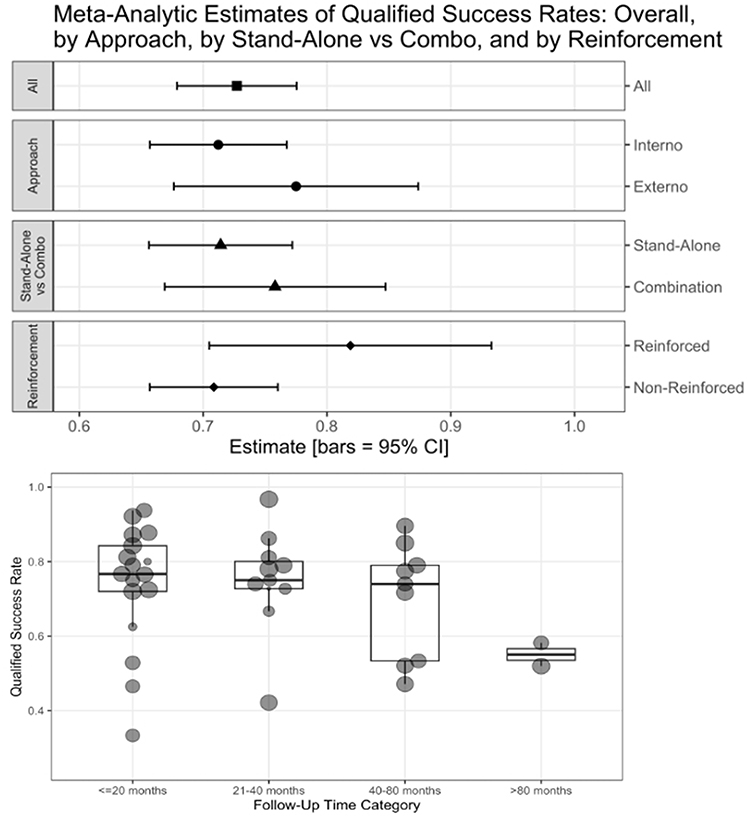 |
Figure 2 (Top) Estimates of qualified success rates from meta-analyses. (Bottom) Qualified success rates over time. Bars indicate 95% confidence intervals. |
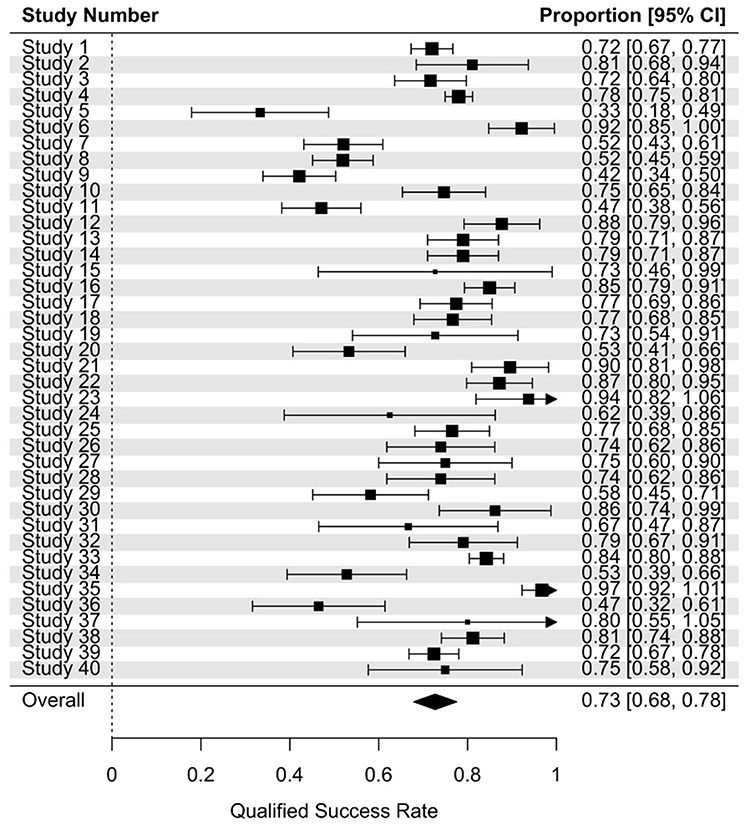 |
Figure 3 Forest plot of overall meta-analysis of qualified success rates. |
A final meta-analysis, with year published as a fixed effect, showed no trends in qualified success through time up to 80 months.
Adverse event reporting was inconsistent, particularly in studies published prior to 1970, making cross-study comparison challenging. Despite this lack of uniformity, the collective body of evidence consistently demonstrates a favorable safety profile for cyclodialysis. Across the studies, few patients experienced significant vision loss, even among extensive ab-externo procedures involving cyclodialysis over 180 degrees of the ciliary body. The recent studies of less invasive, ab-interno techniques report improved safety profile with the internal surgical approach.
Key adverse events reported in from the studies include transient hyphema 3%-79%, clinically significant hypotony 0.5–10.5%, persistent iritis 0–6%.
Discussion
We report the results of a systematic meta-analysis of surgical cyclodialysis treatment for the lowering of intraocular pressure in patients with glaucoma. The review spans more than a century of evolving surgical practice for the treatment of glaucoma across 40 peer-review clinical outcomes publications in over 4000 subjects. It is the most comprehensive systematic review specifically addressing cyclodialysis surgery across a century of clinical practice.
With respect to the main outcome measure of qualified success, the overall efficacy of cyclodialysis exceeded 70%. This demonstrates evidence of clinical benefit in terms of IOP control achieved beyond the efficacy of topical pharmacologic therapy across the entire cohort of peer-review studies. Outcomes were similar regardless of procedure type, approach, or stand-alone versus combination procedures. The additional IOP lowering effect of a combined cataract procedure was demonstrable in our data set with 75.3% of the combined procedures vs 71.0% of the stand-alone cyclodialysis procedures achieving the primary success outcome. While the ab-interno and combined procedures trended toward higher success rates, these differences were not statistically significant, possibly due to sample size limitations. In the early years of cyclodialysis surgery, it was rarely performed in combination with intracapsular cataract extraction and later, with the advent of extracapsular cataract techniques it was combined with manual or phaco-emulsification cataract surgery. The higher level of IOP effect of combined cyclodialysis and cataract intervention is consistent with the experience of more recent glaucoma interventional studies which further substantiate the additive IOP-lowering efficacy of cataract extraction and glaucoma surgery. In addition, the data indicates a trend towards further IOP lowering (78.8% qualified success rate) when cyclodialysis is additionally reinforced with sub-scleral maintainers and spacers to prevent cleft restenosis and increase the durability and patency of the uveoscleral conduit.
To analyze for durability of effect, the dataset was segmented into different periods of post-operative outcomes- < 20 months, 21–40 months, 40–80 months and > 80 months. While a slight attrition of IOP lowering effect can be seen over time from a peak of 74.6% at 20 months post-operative follow-up to 70.2% at 40–80 months, the differences among these post-operative time frames are not statistically significant. The are too few studies beyond 80 months of follow-up to provide an informative dataset for more extended follow-up. Similarly, there is not enough data in the early post-operative period before 6 months to explore if there is any temporal relationship to the post-surgical remodeling and healing of the cyclodialysis. Regardless, the long-term effect across all studies is consistent and sustained. While reinforced cyclodialysis procedures demonstrated improved efficacy at 12- and 24-month follow-ups, data beyond 5 years are lacking, underscoring the need for long-term studies and randomized controlled trials to validate sustained outcomes.
Our analysis also demonstrates comparable efficacy and safety between ab-externo and ab-interno surgical approaches. In fact, a trend towards slightly better IOP lowering effect seems to transpire from the ab-interno studies (77.5% vs 71.2%, respectively). This is clinically important as the size of the cyclodialysis cleft in the ab-externo procedures is generally much larger than the one performed ab-interno, particularly with the more recent interventional techniques, where cleft sizes are discrete and minimally-invasive within 500–1000 microns. This may substantiate the clinical paradigm of the continuity of the uveoscleral outflow where a single discrete entry point can tap into the absorptive outflow capacity of the entire suprachoroidal space. It may also indicate better healing and less fibrosis with minimal intervention and less surgical trauma. The benefits of this more interventional ab-interno approach are also seen in terms of safety where a slightly lower rate of key ocular adverse events are reported in an otherwise homogeneous and favorable safety profile of the cyclodialysis procedure. The overall safety of the procedure is characterized by a relatively low incidence of serious or sight- threatening adverse events and appears more comparable to the newer interventional glaucoma procedures. The characteristic complications of hypotony maculopathy, bleb leaks or loss of visual acuity often reported with trans-scleral glaucoma filtration procedures such as trabeculectomy and external shunt drainage implants are not seen as a major concern with cyclodialysis where aqueous outflow enhancement remains internal to the uveoscleral pathway, there is no violation of the scleral wall and there is no exogenous implantable hardware.22,23
There are several limitations of our analysis. A key limitation is that all 40 available cyclodialysis studies were non-randomized, observational real-world clinical reports. While this is informative of real -world effectiveness, there are confounding factors such as lack of medication wash-out, no protocolized medication re-introduction, no standardized definition of efficacy outcomes, lack of standardized indications for the surgery, and lack of treatment controls. Most studies also had poor definition of mild, moderate or severe glaucoma subtypes and primary open angle versus secondary open angle glaucoma as they did not consistently provide disease category definitions nor baseline visual field data. Another limitation is the insufficient understanding of the precise anatomical location, structural dimensions, and composition of cyclodialysis clefts—possibly critical factors influencing their efficacy and consistency. It is well established that both trabecular and uveoscleral outflows are segmental, making the exact site and scale of intervention potentially useful information.24–29 However, few studies provide detailed accounts of surgical techniques with definition of cleft size nor do they incorporate companion imaging to assess cleft size over time. Furthermore, lack of imaging techniques especially in earlier studies prevented detection of clinically inapparent cystoid macular edema or hypotony maculopathy. Finally, improvements in medical treatment over the last 100+ years would likely favor qualified success rates in more recent studies. Nevertheless, given the span in clinical evidence over 125 years of evolving surgical practice since Leopold Heine first introduced the procedure,30 this integrated evidence-based summary of rather heterogenic reports and data, provides surprisingly consistent evidence of IOP lowering effect and risk-benefit profile of uveoscleral outflow intervention. These observations may be useful in informing and encouraging future surgical innovations in the uveoscleral space. Compared to trabecular bypass MIGS, cyclodialysis targets the uveoscleral pathway, potentially avoiding episcleral venous pressure limitations. This may offer advantages in eyes with compromised trabecular function or secondary glaucoma, where traditional MIGS are less effective.
Conclusion
In conclusion, cyclodialysis represents an established, clinically effective surgical option for glaucoma management, characterized by significant IOP lowering and a favorable safety profile, with a 70% rate of qualified success across the spectrum of published studies. Newer approaches for reinforcement of the cleft could further enhance the durability of the uveoscleral conduit over the long term. As surgical techniques and instrumentation continue to advance, cyclodialysis can fill the gaps across the interventional treatment spectrum from SLT, MIGS to bleb-forming procedures.
Acknowledgments
This paper has been uploaded to medrxiv as a preprint: https://www.medrxiv.org/content/10.1101/2025.04.05.25325239v1.
Disclosure
Dr Alex Huang reports personal fees from AbbVie, Amydis, Celanese, Equinox, Glaukos; Heidelberg Engineering, QLARIS, Santen, Spinogenix, Topcon; research support from Diagnosys, during the conduct of the study. Dr Reena Garg reports speaker honoraria from Iantrek, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. PMID: 24974815. doi:10.1016/j.ophtha.2014.05.013
2. Fahy ET, Montesano G, Garg A, Vickerstaff V, Konstantakopoulou E, Gazzard G; LiGHT Trial Study Group. The impact of baseline intraocular pressure on initial treatment response in the LiGHT trial: selective laser trabeculoplasty versus medication. Ophthalmology. 2024;131(12):1366–1376. PMID: 38964719. doi:10.1016/j.ophtha.2024.06.022
3. ORCA study group; Spital G, Schmitz-Valckenberg S, Müller B, et al. Interpretation of SD-OCT imaging data in real-life conditions versus standardized reading centre analysis in eyes with diabetic macular oedema or macular oedema secondary to retinal vein occlusion: 24-month follow-up of the ORCA study. Graefes Arch Clin Exp Ophthalmol. 2025;263(1):131–139. PMID: 39294392. doi:10.1007/s00417-024-06579-7
4. Bicket AK, Le JT, Azuara-Blanco A, et al. Minimally invasive glaucoma surgical techniques for open-angle glaucoma: an overview of Cochrane systematic reviews and network meta-analysis. JAMA Ophthalmol. 2021;139(9):983–989. PMID: 34264292. doi:10.1001/jamaophthalmol.2021.2351
5. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open-angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
6. Palma A, Covello G, Posarelli C, Maglionico MN, Agnifili L, Figus M. Is the advent of new surgical procedures changing the baseline features of patients undergoing first-time glaucoma surgery? J Clin Med. 2024;13(11):3342. PMID: 38893053; PMCID: PMC11172517. doi:10.3390/jcm13113342
7. Yuan PHS, Dorling M, Shah M, Panarelli JF, Durr GM. Combined microinvasive glaucoma surgery with phacoemulsification in open-angle glaucoma: a systematic review and meta-analysis. Am J Ophthalmol. 2025;270:154–163. PMID: 39089358. doi:10.1016/j.ajo.2024.07.034
8. CyPass Study Group, Vold S, Ahmed IIK, Craven ER, et al. Two-year COMPASS trial results: supraciliary microstenting with phacoemulsification in patients with open-angle glaucoma and cataracts. Ophthalmology. 2016;123(10):2103–2112. PMID: 27506486. doi:10.1016/j.ophtha.2016.06.032
9. Bill A, Phillips CI, MacLellan HM. Uveoscleral drainage of aqueous humor in human eyes. Invest Ophthalmol Vis Sci. 1977;16(11):1008–1017. PMID: 596859.
10. Pederson JE, Gaasterland DE, Tamm E, Tengblad A. Experimental studies of uveoscleral outflow in enucleated human eyes. Exp Eye Res. 1990;51(1):55–63. PMID: 2387261. doi:10.1016/0014-4835(90)90008-9
11. Nilsson SF, Bill A, Kaufman PL. Effect of age on uveoscleral drainage of aqueous humor in man. Exp Eye Res. 1988;47(6):885–889. PMID: 2464531. doi:10.1016/0014-4835(88)90064-3
12. Tamm S, Tamm E, Rohen JW. Age-related changes of the human ciliary muscle: a quantitative morphometric study. Mech Ageing Dev. 1992;62(2):209–221. PMID: 1569790. doi:10.1016/0047-6374(92)90057-k
13. Tamm ER, Kaufman PL. Structure and function of the uveoscleral pathway. In: Ahmed IIK, Alburquerque R, editors. Minimally Invasive Glaucoma Surgery: A Practical Guide. Stuttgart: Thieme; 2017:25–33.
14. D’Amore PA. Encyclopedia of the Eye.
15. Emi K, Pederson JE, Toris CB. Hydrostatic pressure of the suprachoroidal space. Invest Ophthalmol Vis Sci. 1989;30(2):233–238. PMID: 2914753.
16. Toris CB, Yablonski ME, Wang YL, Camras CB. Aqueous humor dynamics in the aging human eye. Am J Ophthalmol. 1999;127(4):407–412. PMID: 10218693. doi:10.1016/s0002-9394(98)00436-x
17. Suguro K, Toris CB, Pederson JE. Uveoscleral outflow following cyclodialysis in the monkey eye using a fluorescent tracer. Invest Ophthalmol Vis Sci. 1985;26(6):810–813. PMID: 2409046.
18. Bill A. Formation and drainage of aqueous humor in cats. Exp Eye Res. 1966;5(1):45–54. PMID: 5929281. doi:10.1016/s0014-4835(66)80006-0
19. Toris CB, Pederson JE. Effect of intraocular pressure on uveoscleral outflow following cyclodialysis in the monkey eye. Invest Ophthalmol Vis Sci. 1985;26(12):1745–1749. PMID: 4066210.
20. Nilsson SF, Lütjen-Drecoll E. Choroidal interstitial fluid pressure and blood flow after cyclodialysis in monkeys. Exp Eye Res. 2009;88(5):768–774. PMID: 19114051. doi:10.1016/j.exer.2008.11.034
21. Nilsson SF. The uveoscleral outflow routes. Eye. 1997;11(Pt 2):149–154. PMID: 9349404. doi:10.1038/eye.1997.43
22. Luo N, Liu M, Hao M, Xu R, Wang F, Zhang W. Comparison of tube shunt implantation and trabeculectomy for glaucoma: a systematic review and meta-analysis. BMJ Open. 2023;13(4):e065921. PMID: 37080625; PMCID: PMC10273552. doi:10.1136/bmjopen-2022-065921
23. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL; Tube Versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789–803.e2. PMID: 22245458; PMCID: PMC4460598. doi:10.1016/j.ajo.2011.10.026
24. Wang Q, Thau A, Levin AV, Lee D. Ocular hypotony: a comprehensive review. Surv Ophthalmol. 2019;64(5):619–638. PMID: 31029581. doi:10.1016/j.survophthal.2019.04.006
25. Goldmann H. Abflussdruck, Minutenvolumen und Widerstand der Kammerwasserströmung des Menschen. Doc Ophthalmol. 1951;5-6(1):278–356. PMID: 14850920. doi:10.1007/BF00143664
26. Sit AJ, Ekdawi NS, Malihi M, McLaren JW. A novel method for computerized measurement of episcleral venous pressure in humans. Exp Eye Res. 2011;92(6):537–544. PMID: 21463627. doi:10.1016/j.exer.2011.03.018
27. Huang AS, Camp A, Xu BY, Penteado RC, Weinreb RN. Aqueous angiography: aqueous humor outflow imaging in live human subjects. Ophthalmology. 2017;124(8):1249–1251. PMID: 28461013; PMCID: PMC5522757. doi:10.1016/j.ophtha.2017.03.058
28. Huang AS, Penteado RC, Papoyan V, Voskanyan L, Weinreb RN. Aqueous angiographic outflow improvement after trabecular microbypass in glaucoma patients. Ophthalmol Glaucoma. 2019;2(1):11–21. PMID: 31595267; PMCID: PMC6781624. doi:10.1016/j.ogla.2018.11.010
29. Lee JY, Akiyama G, Saraswathy S, et al. Aqueous humour outflow imaging: seeing is believing. Eye. 2021;35(1):202–215. PMID: 33060830; PMCID: PMC7852535. doi:10.1038/s41433-020-01215-0
30. Boke H. [History of cyclodialysis. In memory of Leopold Heine (1870–1940)]. Klinische Monatsblätter für Augenheilkunde. 1990;196(4):325–328. doi:10.1055/s-2008-1046254 German
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.