Back to Journals » Nature and Science of Sleep » Volume 18

Cyclic Alternating Pattern and Sleep Microstructure in Parkinson’s Disease: A Systematic Review and Meta-Analysis
Authors Jiang J, Huang Y, Wang M, Zeng Z, Li J
Received 5 March 2026
Accepted for publication 31 May 2026
Published 11 June 2026 Volume 2026:18 606091
DOI https://doi.org/10.2147/NSS.S606091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Jiajun Jiang,1,* Yi Huang,1,* Min Wang,1 Zixuan Zeng,2 Jing Li1– 3
1School of Psychiatry, North Sichuan Medical College, Nanchong, 637000, People’s Republic of China; 2Sichuan Provincial Center for Mental Health, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, 610072, People’s Republic of China; 3Key Laboratory of Psychosomatic Medicine, Chinese Academy of Medical Sciences, Chengdu, 610072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Li, Sichuan Provincial Center for Mental Health, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, 610072, People’s Republic of China, Email [email protected]
Objective: To systematically review polysomnographic sleep differences, with emphasis on cyclic alternating pattern (CAP) microstructure, between patients with Parkinson’s disease (PD) and healthy controls (HC).
Methods: We searched MEDLINE (via OVID), EMBASE (via OVID), CINAHL (via EBSCOhost), APA PsycArticles (via EBSCOhost), and Evidence-Based Medicine databases (via EBSCOhost) for studies published from January 1, 2020, to September 15, 2025. Eligible studies enrolled adults with idiopathic PD, included an internal HC group, used overnight polysomnography, and reported extractable CAP-related outcomes. Study quality was assessed with the Newcastle-Ottawa Scale. Random-effects meta-analyses were performed using Hedges’ g with restricted maximum-likelihood estimation, and certainty of evidence was appraised with GRADE.
Results: Four studies were included. PD patients showed significant reductions in CAP rate, CAP sequence duration, and CAP index (all p< 0.05), with low statistical heterogeneity. Macrostructural parameters showed no statistically significant pooled differences, and several had moderate-to-high heterogeneity. GRADE certainty was very low because the evidence came from a small number of observational studies.
Conclusion: Within a limited evidence base, CAP-related microstructure shows a consistent pattern of reduction in clinically diagnosed PD, whereas macrostructural alterations were not stable across the included studies. CAP measures may provide complementary information in future PD sleep research, but the present evidence is insufficient to support their use as validated biomarkers.
Keywords: Parkinson’s disease, sleep microstructure, polysomnography, cyclic alternating pattern, meta-analysis
Introduction
According to the current international criteria established by the Movement Disorder Society (MDS), the clinical diagnosis of Parkinson’s disease (PD) primarily relies on the identification of core motor signs, such as the presence of bradykinesia in combination with either resting tremor or rigidity.1 However, both prior to the manifestation of motor symptoms and throughout the entire disease course, a substantial range of non-motor symptoms (NMS) exert a profound impact on patients’ quality of life, functional status, and prognosis, even constituting a primary cause of disability.2–4 Among the diverse spectrum of NMS, sleep disturbances represent a frequently encountered non-motor manifestation in PD patients, which intensifies with disease progression.5–7 Common sleep disorders encompass insomnia, excessive daytime sleepiness (EDS), restless legs syndrome (RLS), and, notably, the highly distinctive rapid eye movement sleep behavior disorder (RBD).8,9 Polysomnographic studies suggest that these sleep disturbances correspond to well-defined alterations in sleep architecture, including impairments in macroscopic structure such as reduced sleep efficiency and diminished slow-wave sleep, as well as abnormalities in microscopic architecture such as alterations in sleep spindles.5,10 Importantly, longitudinal follow-up studies indicate that the risk of developing neurodegenerative diseases among individuals with RBD is estimated to exceed 90% in some cohorts, positioning RBD as one of the most specific prodromal biomarkers in relevant populations for Parkinson’s disease.11–13 Consequently, in-depth investigation into sleep disturbances in PD holds critical clinical significance for elucidating early disease pathophysiology, clarifying clinically relevant sleep-related phenotypes and enhancing overall patient management.
Polysomnography (PSG) is a standard objective method for assessing sleep and allows quantification of macroscopic sleep architecture—including total sleep time, sleep efficiency, and sleep-stage distribution—as well as microstructural features, such as sleep spindles, electroencephalographic spectral power, and the cyclic alternating pattern.14 A comprehensive systematic review and meta-analysis conducted by Zhang et al (2020)5 has reported that PD patients may exhibit significant abnormalities in macroscopic sleep structure, manifested as reductions in total sleep time, sleep efficiency, and the proportion of slow-wave sleep, coupled with an increase in wake time after sleep onset. Collectively, these alterations in macroscopic architecture may indicate a notable decline in both the quality and quantity of sleep among individuals with Parkinson’s disease.
With the progressive advancement of research, investigations into PD-associated sleep disturbances have moved beyond conventional macrostructural descriptions toward the evaluation of sleep microarchitecture.15,16 Broadly, NREM sleep microarchitecture can be characterized using complementary domains such as sleep spindles, quantitative electroencephalographic (EEG) spectral power, and the cyclic alternating pattern (CAP).14 These measures may reflect the functional integrity of neural systems vulnerable to PD pathology: spindle abnormalities have been linked to thalamocortical dysfunction,17 whereas spectral measures can capture alterations in cortical synchronization.18 However, the available evidence is uneven across microstructural domains, and sufficiently comparable quantitative data are currently concentrated in CAP-related outcomes.
CAP is a periodic EEG phenomenon of NREM sleep that organizes transient fluctuations in cortical activation. A CAP cycle consists of an activating A phase followed by a background B phase, and at least three consecutive A phases interleaved with B phases constitute a CAP sequence when they occur within the accepted temporal criteria. According to their degree of synchronization and desynchronization, A phases are classified as A1, A2, or A3: A1 is dominated by synchronized slow-wave activity and is generally linked to slow-wave build-up and sleep consolidation; A2 contains mixed slow and fast rhythms; and A3 is characterized predominantly by desynchronized fast activity.19,20 Because CAP reflects the dynamic regulation of NREM sleep stability, it may be relevant to PD-related dysfunction of arousal-modulatory systems, including noradrenergic pathways.21 At the same time, CAP is not disease-specific and may be influenced by dopaminergic or psychotropic medications, comorbid REM sleep behavior disorder (RBD), obstructive sleep apnea (OSA), periodic limb movements, and disease stage.22 Recent work has also linked altered sleep-stage mixing with poorer prognosis in early PD and associated objective sleep features with brain structure and cognition in clinical cohorts,23,24 reinforcing the clinical relevance of systematic PSG phenotyping without implying that CAP is already a validated biomarker.
Although preliminary studies suggest that sleep microarchitecture may be altered in PD, the evidence remains fragmented. Because a prior meta-analysis focused primarily on sleep macrostructure and searched literature published before 2020,5 the present review was designed as a focused update of studies published from 2020 to 2025. The search strategy covered CAP, sleep spindles, and EEG spectral measures as prespecified microstructural domains. This systematic review and meta-analysis aimed to synthesize CAP-related PSG findings in PD, provide a partial update on macrostructural outcomes within CAP-reporting cohorts, and summarize non-CAP microstructural findings reported by eligible studies.
Materials and Methods
Protocol and Registration
This systematic review protocol was registered with PROSPERO (ID: CRD420251144799; https://www.crd.york.ac.uk/PROSPERO/view/CRD420251144799) and was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Eligibility Criteria According to the PICOS Approach
Participants (P)
The study population comprised adults (age ≥18 years) diagnosed with idiopathic Parkinson’s disease according to established clinical criteria, such as the UK Parkinson’s Disease Society Brain Bank Clinical Diagnostic Criteria or Movement Disorder Society (MDS) Clinical Diagnostic Criteria. To maintain population homogeneity, studies involving patients with non-idiopathic parkinsonian syndromes (eg., vascular parkinsonism, drug-induced parkinsonism, multiple system atrophy, progressive supranuclear palsy) were excluded.
Intervention (I)
Eligible studies were required to use at least one full-night polysomnographic recording of at least 6 hours, with standard sleep staging and multichannel signals sufficient to derive the outcomes of interest. Laboratory-based and validated home-based PSG recordings were eligible when scored according to recognized standards. Studies relying only on questionnaires, actigraphy, or non-standard sleep monitoring without extractable PSG outcomes were excluded.
Comparison (C)
The comparator group comprised non-PD adults described by the original studies as healthy controls or low-risk non-manifest participants. We sought age- and sex-comparable groups where available; however, studies were not excluded solely because minor residual imbalance remained after matching, and any material imbalance was considered during interpretation. Comparator participants were required to be free of diagnosed parkinsonian syndromes and to provide an internal reference group for the PD cohort.
Outcomes (O)
The primary outcomes were prespecified CAP metrics reflecting NREM sleep microstructure: CAP rate (%), CAP index (cycles/h), and mean CAP sequence duration (s). Secondary outcomes included conventional PSG macrostructural parameters (eg., total sleep time, wake after sleep onset, sleep efficiency, N1, N2, N3, REM sleep, and apnea-hypopnea index) and non-CAP microstructural findings, including sleep spindle characteristics and EEG spectral-power measures, when reported. Outcomes were pooled when quantitative data were extractable and sufficiently compatible across studies; other relevant CAP and non-CAP microstructural findings were summarized descriptively.
Study Design (S)
This systematic review was restricted to observational study designs, explicitly encompassing case-control studies and cross-sectional investigations. The following categories of publications were excluded: individual case reports and case series, editorial or commentary articles, conference abstracts, publications in languages other than English, and non-human animal studies or other pre-clinical research not involving human subjects.
Information Sources
We conducted a systematic literature search restricted to studies published from January 1, 2020, to September 15, 2025, across MEDLINE via OVID, EMBASE via OVID, CINAHL via EBSCOhost, APA PsycArticles via EBSCOhost, and Evidence-Based Medicine (EBM) databases via EBSCOhost.
Search
The search strategy combined controlled vocabulary and free-text terms relating to Parkinson’s disease, polysomnography, and sleep microstructure. Search terms included CAP, sleep spindles, sigma activity, and EEG spectral-power measures. Reference lists of included studies and relevant reviews were also screened manually. The full search strategies are provided in Supplementary File 1.
Study Selection
Two reviewers (Zixuan Zeng and Jiajun Jiang) independently screened records against the prespecified eligibility criteria. Disagreements were resolved through discussion or, when necessary, arbitration by a third reviewer (Jing Li). Screening was conducted in two stages: title/abstract screening followed by full-text assessment. Before consensus, inter-reviewer agreement was high, with Cohen’s κ values of 0.873 for title/abstract screening and 0.789 for full-text assessment, corresponding to raw agreement rates of 94.7% and 98.0%, respectively.
Data Collection Process
Data from the included studies were independently extracted by two reviewers using a pre-piloted standardized form, with discrepancies resolved by consensus. The extracted variables included: (1) study characteristics; (2) demographic and clinical characteristics of participants; (3) PSG methodology; (4) CAP metrics, sleep spindle characteristics, and EEG spectral-power findings when available; and (5) means, standard deviations, and sample sizes for all relevant outcomes in PD and HC groups. Across 384 prespecified extraction items, the two reviewers agreed on 358 items before consensus, yielding an initial agreement rate of 93.2%. When clarification or data were unavailable in the published reports, missing details were recorded as not reported rather than inferred; no unpublished participant-level data were incorporated.
Quality Assessment
Risk of bias was assessed using the Newcastle-Ottawa Scale (NOS) for the included case-control and cross-sectional studies. Two reviewers (Zixuan Zeng and Jiajun Jiang) independently assessed each study across the domains of selection, comparability, and exposure/outcome ascertainment. Disagreements were resolved by discussion or, when needed, by a third reviewer (Jing Li). Item-level NOS ratings are reported in Supplementary Table S1.
Data Synthesis and Statistical Analysis
All quantitative syntheses were performed in jamovi version 2.7 using the metafor backend. For continuous outcomes, Hedges’ g (bias-corrected standardized mean difference) with 95% confidence intervals was calculated and pooled with a random-effects model using restricted maximum-likelihood estimation. Between-study heterogeneity was assessed using Cochran’s Q and I2 statistics; I2 values of approximately 25%, 50%, and 75% were interpreted as low, moderate, and substantial heterogeneity, respectively, while recognizing that heterogeneity estimates are unstable when k is small. Leave-one-out sensitivity analyses were conducted for each pooled outcome. Because complete sample independence between Doppler et al (2021)21 and Doppler et al (2022)25 could not be established from the published reports, overlap-focused sensitivity analyses excluding one Doppler comparison at a time were additionally examined for outcomes to which both studies contributed.
To investigate potential sources of the observed heterogeneity, pre-specified subgroup analyses and meta-regression were planned. Planned moderators for examination included factors potentially influencing the outcomes, such as the concomitant presence of rapid eye movement sleep behavior disorder, disease severity, medication status (including LEDD when available), and the specific polysomnography scoring criteria employed. However, because each outcome was informed by only 3–4 comparisons, subgroup analyses and meta-regression were not feasible and were therefore not performed.
Assessment of publication bias was considered unreliable because each outcome included fewer than 10 studies. Funnel-plot inspection, Egger’s regression, Begg’s test, and fail-safe N calculations were therefore treated as exploratory only and were not used to support confirmatory inferences regarding the presence or absence of reporting bias.
Given the age imbalance reported in Dagay et al (2025),26 age mismatch was considered a potential confounder in the descriptive synthesis and limitations. We did not compute exclusion-based pooled estimates removing Dagay et al (2025),26 because this would reduce the relevant CAP analyses to only two studies and make pooled inference especially unstable.
Assessment of the Certainty of Evidence
We used the GRADE framework to assess the certainty of evidence for the three primary CAP outcomes. Because all included studies were observational, the starting certainty rating was low. A structured outcome-level evidence profile was constructed across the domains of risk of bias, inconsistency, indirectness, imprecision, and publication bias. Downgrading decisions considered study quality, sample size, residual confounding, and the small number of contributing studies.
Results
Study Selection
Our systematic review, conducted in accordance with PRISMA 2020, identified 536 records from database searches conducted for studies published between 2020 and 2025 (168 from MEDLINE via OVID, 311 from EMBASE via OVID, 21 from CINAHL via EBSCOhost, 30 from EBM databases via EBSCOhost, and 6 from APA PsycArticles via EBSCOhost). After removal of duplicates, 339 unique records were screened, of which 239 were excluded at title/abstract stage. One hundred full-text reports were assessed, and 96 were excluded for the following reasons: no target outcome (n=60), ineligible controls (n=17), ineligible patients (n=9), overlapping data (n=1), review article (n=2), case report (n=1), animal study (n=4), and editorial (n=2). Four studies met all eligibility criteria and were included in the qualitative synthesis and meta-analysis. The study-selection process is shown in Figure 1.
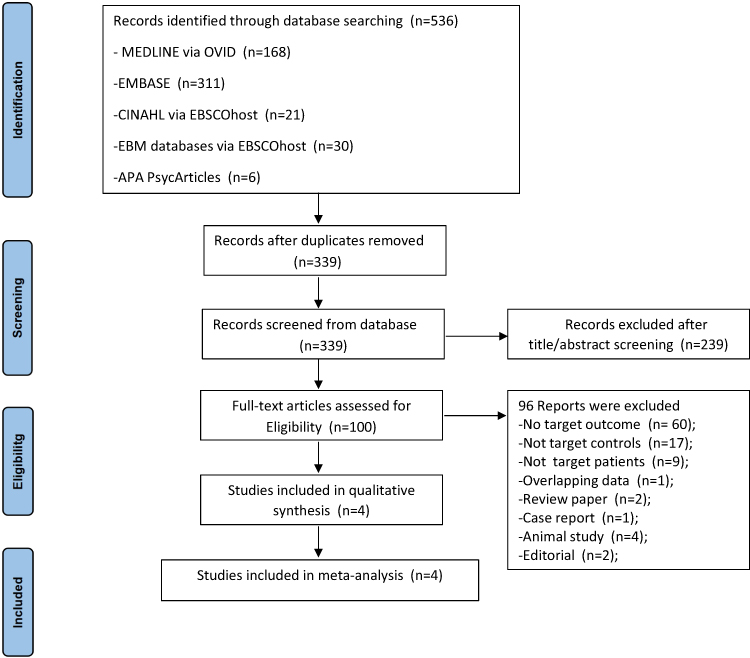 |
Figure 1 PRISMA 2020 flow diagram of study selection. |
Description of the Included Studies
This review included four eligible studies,16,21,25,26 comprising clinically diagnosed PD groups and healthy-control comparators. Sample sizes ranged from 36 participants in Cheng et al (2025)16 to 66 participants in Dagay et al (2025).26 Across the included studies, mean or median ages ranged from 56.83 to 67.4 years, and the proportion of male participants ranged from 44.4% to 69.2%. Disease duration varied from approximately 1.0 year in recent or early PD cohorts to 6.3 years in a more established cohort, indicating clinically meaningful variation in disease stage.
Medication exposure and comorbid sleep-disorder handling also varied across studies. Doppler et al (2021)21 allowed regular evening medication during PSG and included participants with AHI 0–25/h and PLMI 0–80/h. Doppler et al (2022)25 excluded datasets with AHI >30/h or PLMI >100/h and included recent as well as established PD strata. Cheng et al (2025)16 enrolled early-stage medicated PD patients, excluded insomnia, OSA, and arrhythmia, and reported RBD in 3/18 patients. Dagay et al (2025)26 studied early PD, excluded antipsychotic use and extensive PLMS (>50), reported RBD in 37% of PD participants, and evaluated patients while adhering to their usual dopaminergic treatment schedule. These differences were considered clinically relevant potential confounders in the interpretation of pooled findings.
All included studies used AASM-based sleep scoring, although the specific versions differed across reports, and three studies explicitly applied CAP consensus criteria. Because individual studies reported different subsets of CAP parameters, the number of contributing studies varied by outcome. Table 1 summarizes study characteristics, medication status, handling of comorbid sleep disorders, scoring methods, and reported PSG outcomes.
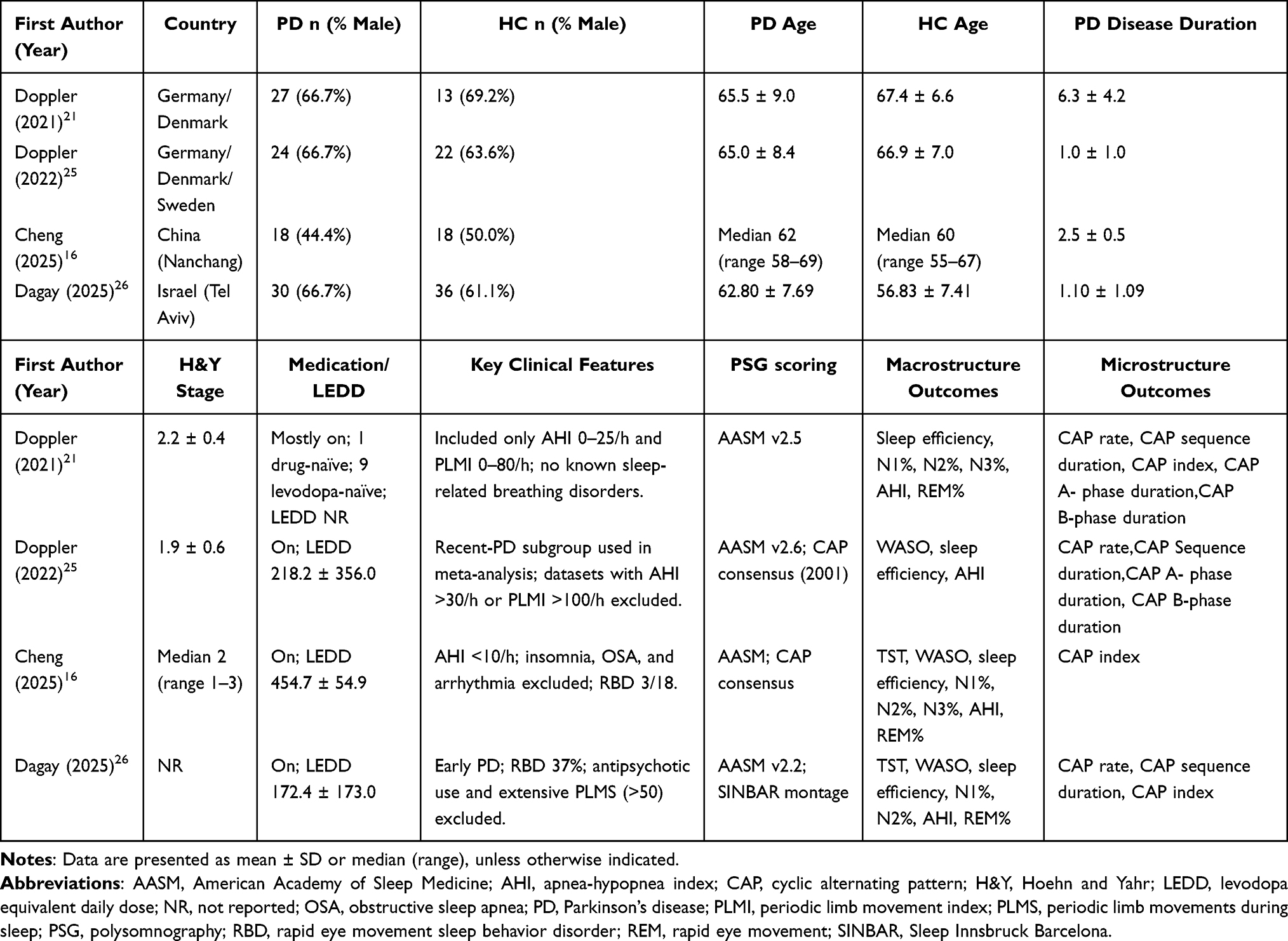 |
Table 1 Baseline Characteristics and Polysomnographic (PSG) Parameters of the Included Studies |
Comparison Between PD Patients and Controls: The Whole Sample
In the overall pooled sample, PD patients showed significant reductions in CAP rate (Hedges’ g = −0.8434, 95% CI: −1.1810 to −0.5059), CAP sequence duration (Hedges’ g = −0.9250, 95% CI: −1.2656 to −0.5843), and CAP index (Hedges’ g = −0.8557, 95% CI: −1.2062 to −0.5051) (Table 2 and Figure 2). CAP rate and CAP sequence duration were analyzed from Doppler et al (2021),21 Doppler et al (2022),25 and Dagay et al (2025),26 whereas CAP index was analyzed from Doppler et al (2021),21 Cheng et al (2025),16 and Dagay et al (2025).26 The direction of effects was concordant across contributing studies, and heterogeneity estimates were near zero for all three CAP outcomes.
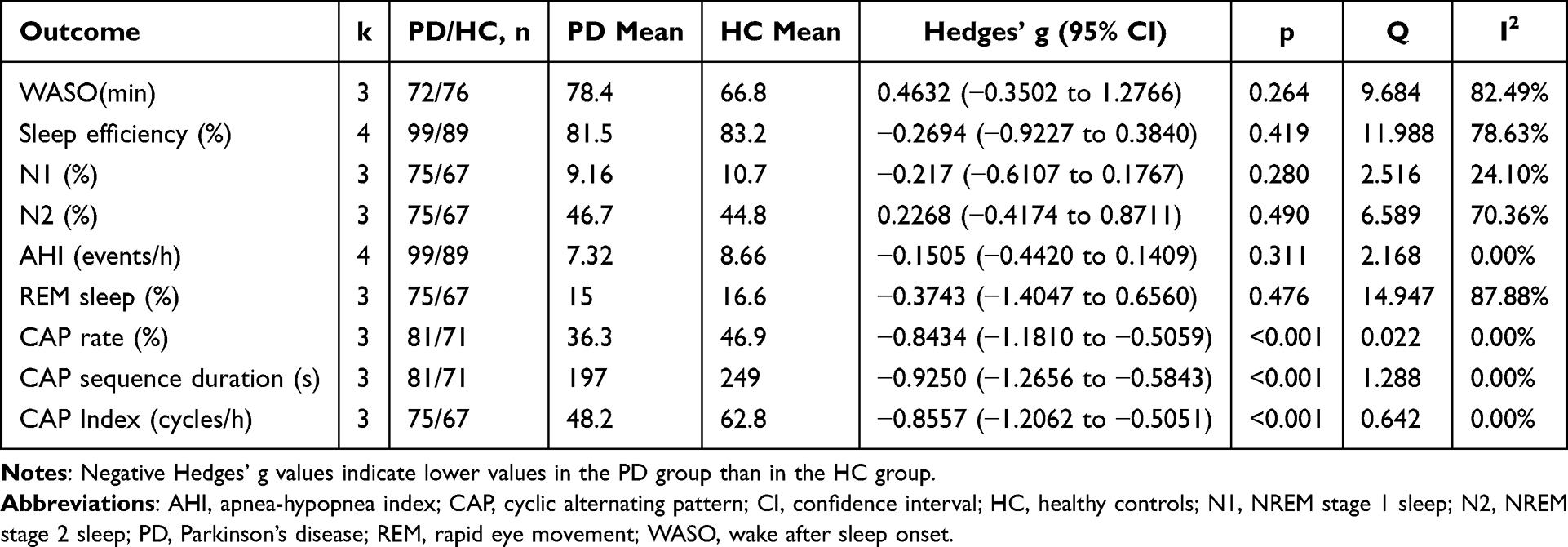 |
Table 2 Meta-Analytic Comparison of Sleep Macro- and Microstructure Between Patients with Parkinson’s Disease and Healthy Controls |
 |
Figure 2 Forest plots of CAP-related microarchitectural outcomes in Parkinson’s disease versus healthy controls (Hedges’ g): (A) CAP rate (%); (B) CAP sequence duration (s); (C) CAP index (cycles/h). |
In the overall sample, no statistically significant differences were generally observed in the macrostructure of sleep, as indicated by the following parameters: WASO (Hedges’g = 0.4632, 95% CI: −0.3502 to 1.2766), SE (Hedges’g = −0.2694, 95% CI: −0.9227 to 0.3840), N1% (Hedges’ g = −0.2170, 95% CI: −0.6107 to 0.1767), N2% (Hedges’g = 0.2268, 95% CI: −0.4174 to 0.8711), AHI (Hedges’g = −0.1505, 95% CI: −0.4420 to 0.1409), and REM% (Hedges’g = −0.3743, 95% CI: −1.4047 to 0.6560). Notably, several of these metrics exhibited moderate to high heterogeneity, exemplified by WASO (I2 ≈ 82.49%), SE (I2 ≈ 78.63%), N2% (I2 ≈ 70.36%), and REM% (I2 ≈ 87.88%) (see Table 2). These findings indicate that, across a small number of studies, conventional macrostructural parameters did not show consistent pooled differences and were characterized by substantial between-study variability. Given the limited evidence base, potential contributors (eg., sample characteristics, medication burden/LEDD, and comorbid RBD) could not be formally tested.
Across CAP outcomes, the pooled effects were negative and moderate-to-large in magnitude, with minimal statistical heterogeneity. Because the evidence base was small, these estimates are reported as group-level differences rather than evidence of superior sensitivity, reliability, or specificity.
Sensitivity Analysis
Leave-one-out analyses showed that the primary CAP findings were directionally stable For CAP rate, omission of any single study produced pooled estimates ranging from −0.821 to −0.857; for CAP sequence duration, estimates ranged from −0.835 to −1.088; and for CAP index, estimates ranged from −0.741 to −0.935. Accordingly, no single study reversed the direction or statistical significance of the pooled CAP effects. Because the independence of Doppler et al (2021)21 and Doppler et al (2022)25 could not be confirmed from published reports, overlap-focused sensitivity analyses were also examined: exclusion of either Doppler comparison from CAP rate and CAP sequence-duration analyses left the pooled effects negative and statistically significant, although the resulting k=2 estimates remain exploratory. Full leave-one-out results are reported in Supplementary Table S2.
Macrostructural findings were less stable Removal of Cheng et al (2025)16 produced the largest change in several analyses, shifting the pooled estimate for WASO from 0.463 to 0.072, sleep efficiency from −0.269 to 0.022, and N2% from 0.227 to −0.102. These changes, together with high heterogeneity for WASO, sleep efficiency, N2%, and REM sleep, indicate that macrostructural results were more sensitive to individual-study characteristics and should be interpreted cautiously.
Publication Bias
Publication-bias analyses were conducted only as exploratory diagnostics because each synthesis included 3–4 studies. Funnel plots, Egger’s regression, Begg’s test, and fail-safe N values are therefore reported descriptively and should not be interpreted as evidence for or against publication bias. For the CAP outcomes, formal tests were non-significant, but the very small k precludes reliable inference.
For macrostructural outcomes, formal tests likewise lacked adequate power. Egger’s test for WASO approached statistical significance (p = 0.063), but given the sparse evidence base, this observation is hypothesis-generating only. Overall, the available data do not permit a dependable assessment of reporting bias for either macrostructural or CAP-related outcomes.
PSG Findings Which Cannot Be Meta-Analyzed
Three studies21,25,26 reported CAP-related temporal parameters that could not be meta-analyzed because of heterogeneous metrics or reporting formats. Their descriptive findings are summarized in Table 3. Non-CAP microstructural findings from the included studies are summarized in Supplementary Table S3. None of the four eligible studies reported extractable sleep-spindle characteristics. Quantitative EEG spectral findings were reported by Cheng et al (2025),16 who observed lower absolute delta power during N3 non-CAP segments together with higher absolute alpha and beta power under selected N3 CAP/non-CAP conditions. Because sleep-spindle and spectral-power measures were sparsely reported and not compatible across studies, these outcomes were summarized descriptively rather than pooled.
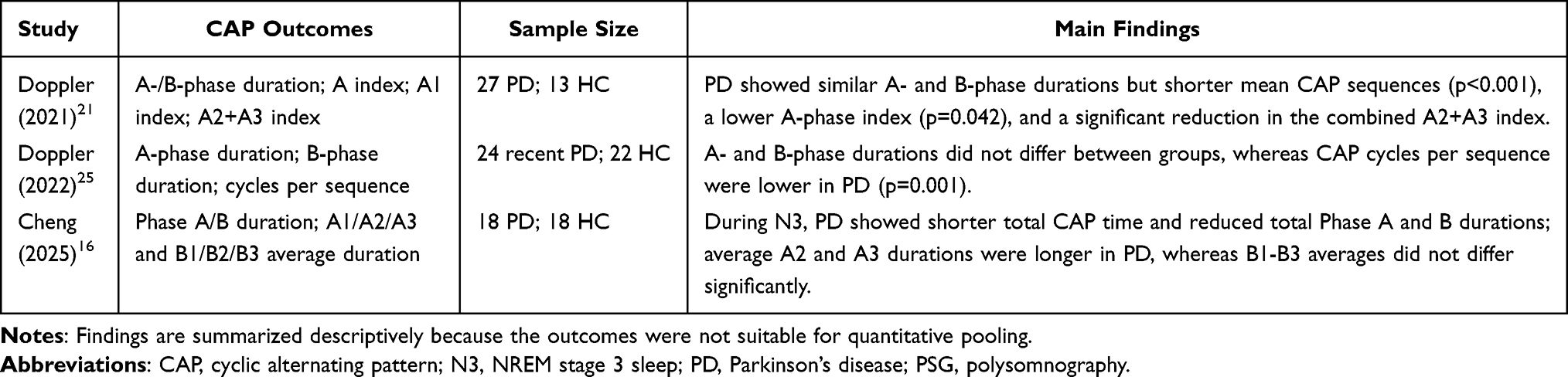 |
Table 3 Summary of CAP-Related Polysomnographic Findings Not Included in the Meta-Analysis |
Certainty of Evidence
Using the GRADE framework, certainty was rated as very low for CAP rate, CAP sequence duration, and CAP index. Although the direction of effect was consistent and statistical heterogeneity was low, confidence in the estimates was downgraded because all evidence came from small observational studies, the number of studies per outcome was very limited, medication and comorbidity confounding could not be excluded, and possible sample overlap between Doppler et al (2021)21 and Doppler et al (2022)25 remained unresolved. The structured evidence profile is presented in Table 4.
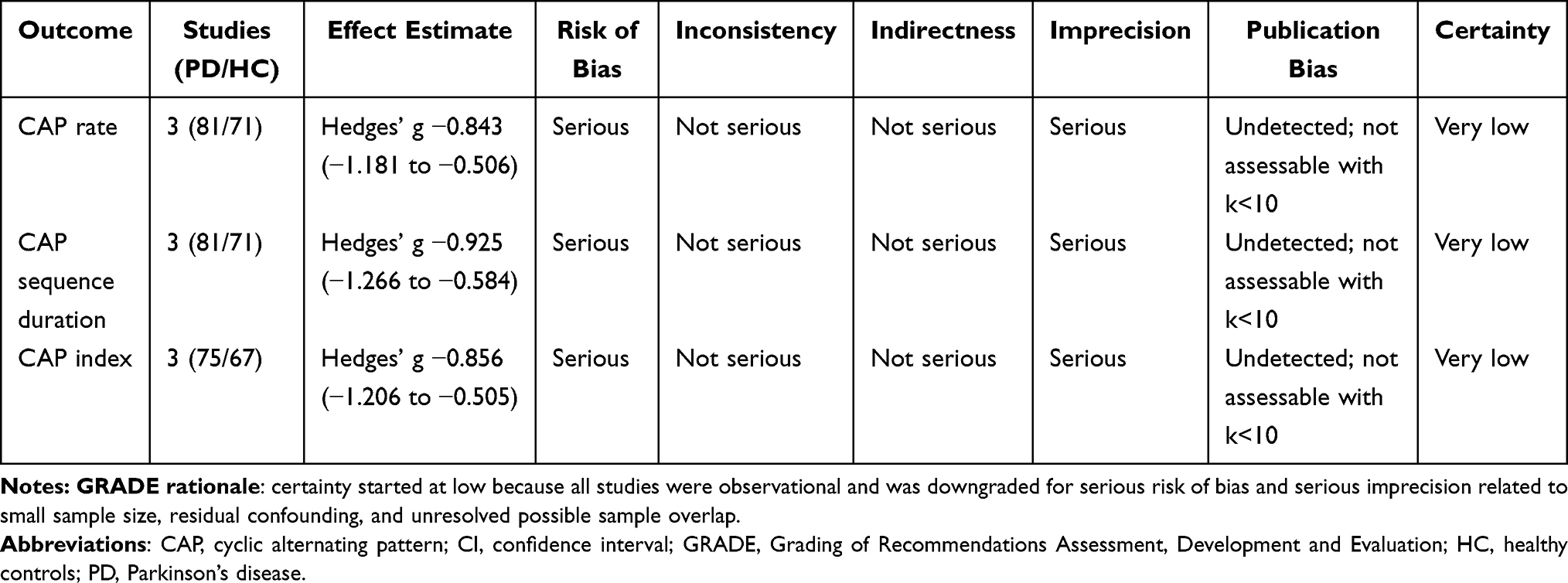 |
Table 4 GRADE Evidence Profile for the Primary CAP Outcomes |
Discussion
Principal Findings
This review focused on CAP-related PSG findings in PD and identified consistent reductions in three pooled CAP measures: CAP rate, CAP sequence duration, and CAP index. These outcomes quantify related but non-identical features of NREM sleep organization. CAP rate reflects the proportion of NREM sleep occupied by CAP activity, CAP index captures the frequency of CAP cycles per hour, and CAP sequence duration reflects the temporal persistence of CAP organization. The concordant direction of these three estimates suggests that the observed group difference is not limited to a single CAP parameter, but more likely reflects a broader attenuation of NREM dynamics mediated by CAP. By contrast, conventional macrostructural outcomes did not show stable pooled differences in the same CAP-reporting cohorts, and several macrostructural estimates were characterized by high heterogeneity. These findings support the relevance of CAP analysis as a complementary PSG approach in PD sleep research, while remaining insufficient for diagnostic or prognostic application.
Neurophysiological Interpretation of CAP Reduction
CAP represents the temporal alternation between transient activating events and background NREM EEG activity. In this framework, a lower CAP rate or CAP index should not be interpreted simply as more stable sleep. In disorders dominated by respiratory events, pain, or insomnia-related hyperarousal, increased CAP activity may reflect repeated reactive arousals. In PD, however, reduced CAP may indicate impaired generation or propagation of physiological NREM phasic activity. This interpretation is biologically plausible because the cyclic organization of CAP depends not only on intrinsic cortical slow oscillations and thalamocortical synchronization, but also on precisely timed excitatory drive from ascending arousal-modulatory systems. Among these, the noradrenergic locus coeruleus plays a privileged role: its phasic firing facilitates the transition from slow oscillatory states to activated network states and gates thalamocortical sensory processing, thereby directly shaping the temporal architecture of CAP sequences. A loss of this phasic noradrenergic facilitation could therefore impair the brain’s ability to initiate and sustain organized CAP dynamics. Among the included studies, Doppler et al (2021)21 provided the most direct mechanistic evidence for this pathway by showing that lower CAP metrics were associated with reduced norepinephrine transporter density in brainstem and thalamocortical regions. This finding links CAP abnormalities to noradrenergic arousal-system dysfunction, but it remains a single-study observation and cannot establish a disease-wide mechanism.
Relationship to Macrostructural PSG Findings
The apparent contrast between reduced CAP measures and non-significant macrostructural differences should be interpreted in relation to the level of sleep analysis. Macrostructural variables summarize the amount and distribution of sleep stages across the night, whereas CAP measures describe dynamic fluctuations within NREM sleep. Therefore, CAP abnormalities may coexist with relatively preserved stage percentages, particularly in small cohorts or in early-to-moderate disease. This distinction helps reconcile the present findings with the larger meta-analysis by Zhang et al,5 which reported reduced total sleep time, sleep efficiency, slow-wave sleep, and REM sleep, together with increased WASO and N1 sleep across a broader PD literature. The present review was restricted to CAP-reporting studies published after 2020 and included far fewer comparisons; therefore, its macrostructural findings should be interpreted as specific to this limited evidence base, not as evidence against macrostructural sleep impairment in PD.
Clinical and Methodological Sources of Uncertainty
Several features of the included studies limit interpretation of a single pooled CAP estimate. First, most PD participants were receiving dopaminergic treatment, and reported LEDD values varied substantially. Medication timing also differed across studies; for example, Doppler et al (2021)21 allowed regular evening medication during PSG, whereas Dagay et al (2025)26 instructed participants to follow their usual dopaminergic schedule. Because dopaminergic therapy and other centrally acting medications can affect sleep continuity, arousal, REM sleep, and movement-related events, the observed CAP reductions may reflect both disease-related and treatment-related influences. Second, comorbid sleep disorders were handled differently. RBD, OSA, insomnia, and periodic limb movements can all modify NREM instability and CAP expression, but exclusion thresholds and reporting were not uniform across studies. Third, disease stage varied from recently diagnosed or early PD to more established PD. This is clinically relevant because PD may follow heterogeneous prodromal and clinical trajectories, including phenotypes with different relative involvement of brainstem, autonomic, limbic, and motor circuits.27–29 Stage-stratified findings in Doppler et al (2022)25 also suggest that CAP sequence duration may change across prodromal, recent, and established PD phases. Finally, complete sample independence between Doppler et al (2021)21 and Doppler et al (2022)25 could not be verified from the published reports. Sensitivity analyses did not change the direction of the CAP findings, but the residual overlap concern contributes to the assignment of a very low certainty rating.
Non-Poolable Microstructural Findings
The broader sleep-microstructure search identified limited non-CAP evidence within the final eligible studies. Sleep-spindle outcomes were not reported in extractable form, and quantitative EEG spectral-power data were available only from Cheng et al (2025).16 That study reported reduced N3 delta power and increased alpha/beta activity under selected CAP and non-CAP conditions, suggesting possible alterations in deep-sleep EEG composition. However, these findings could not be compared quantitatively across studies. Similarly, several CAP-related temporal and subtype outcomes, including A/B-phase durations, total CAP time, and cycles per sequence, were not suitable for meta-analysis because definitions, units, and reporting formats differed. These descriptive results are directionally consistent with reduced CAP organization, but they should be treated as supportive context rather than confirmatory evidence.
Implications for Future Research
The main implication of this review is methodological rather than diagnostic. CAP measures may be useful research endpoints for characterizing NREM microarchitecture in PD, but future studies need more standardized designs before clinical interpretation can be strengthened. Priority should be given to larger longitudinal cohorts, prespecified CAP scoring procedures, explicit reporting of CAP rate, CAP index, sequence duration, A-phase subtype indices, and raw group-level summary statistics. Future studies should also report medication state, LEDD, RBD status, respiratory indices, PLMI, insomnia status, cognitive status, and disease duration in sufficient detail for subgroup analysis. Drug-naive cohorts, medication-state comparisons, or carefully justified washout designs would be particularly informative when ethically feasible. Finally, if CAP is to be evaluated as a candidate biomarker in PD, studies should include longitudinal outcomes and formal diagnostic or prognostic performance analyses rather than relying solely on cross-sectional group differences.
Strengths and Limitations
This review has several strengths, including a registered protocol, duplicate screening and extraction, formal risk-of-bias assessment, GRADE evaluation, and outcome-specific sensitivity analyses. It also updates the PSG literature after the 2020 macrostructure-focused review and separates quantitative CAP findings from descriptive non-CAP microstructural results. The limitations are substantial. Only four studies met the eligibility criteria, each pooled CAP outcome included three comparisons, and all included studies were observational. Residual confounding by medication exposure, comorbid sleep disorders, age imbalance, and disease stage could not be excluded. Publication bias could not be assessed reliably, and possible sample overlap between two Doppler cohorts remained unresolved. These limitations restrict generalizability and preclude causal, temporal, or biomarker-level conclusions.
Conclusion
Within the currently limited CAP-reporting PSG literature, patients with idiopathic PD showed moderate-to-large reductions in CAP rate, CAP sequence duration, and CAP index, while traditional macrostructural outcomes did not show stable pooled differences. These CAP measures may serve as complementary research endpoints worth standardizing in future PD PSG protocols, particularly when interpreted alongside macrostructure and clinically relevant confounders, but they should presently be framed as research measures rather than diagnostic tools.
The primary CAP findings were directionally stable in leave-one-out analyses, but the certainty of evidence was rated very low because the evidence base was small, observational, and vulnerable to residual confounding and unresolved sample-overlap concerns. Publication bias could not be reliably assessed with only 3–4 contributing studies per outcome.
Therefore, it would be premature to regard CAP abnormalities as a stable electrophysiological trait across PD phenotypes or disease stages, or as a validated biomarker for early identification or monitoring. Future studies should use larger longitudinal cohorts, standardized CAP scoring, explicit reporting of RBD/OSA/PLMS status, and rigorous control of medication exposure, ideally including drug-naive or well-defined medication-state designs.
Key limitations of this review include the very small number of eligible studies, heterogeneity in disease stage and comorbid sleep-disorder handling, age imbalance in Dagay et al (2025),26 predominantly medicated PD cohorts, and the unresolved possibility of sample overlap between Doppler et al (2021)21 and Doppler et al (2022).25 The exclusively cross-sectional designs further preclude causal or temporal inference. These factors restrict generalizability, precluded adequately powered subgroup analyses or meta-regression, and reinforce the need for larger longitudinal studies with standardized CAP scoring and clearer cohort reporting.
Data Sharing Statement
All data analyzed in this review were extracted from the published reports of the included studies; no new participant-level data were generated. Data sharing is therefore not applicable beyond the cited source articles.
Author Contributions
Jiajun Jiang (First author): Conceptualization; Writing – original draft; Writing – review and editing.Yi Huang (Co–first author; second author): Visualization (tables and figures); Writing – review and editing.
Min Wang (third author): Methodology; Data curation; Validation of extracted data and statistical outputs; Interpretation of findings; Writing – review and editing.
Zixuan Zeng (fourth author): Visualization (tables and figures); Writing – review and editing.Jing Li (Corresponding author): Conceptualization; Writing – original draft; Writing – review and editing.All authors participated in drafting, revising, or critically reviewing the article; agreed on the journal to which the article was submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Sichuan Science and Technology Program [2025YFHZ0108] and Chengdu Science and Technology Program [2024-KP01-00024-SN] & [2024-YF05-01745-SN].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591–12. doi:10.1002/mds.26424
2. Chaudhuri KR, Healy DG, Schapira AH. National institute for clinical excellence. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006;5(3):235–245. doi:10.1016/S1474-4422(06)70373-8
3. Bang Y, Lim J, Choi HJ. Recent advances in the pathology of prodromal non-motor symptoms olfactory deficit and depression in Parkinson’s disease: clues to early diagnosis and effective treatment. Arch Pharm Res. 2021;44(6):588–604. doi:10.1007/s12272-021-01337-3
4. Taguchi T, Ikuno M, Yamakado H, Takahashi R. Animal model for prodromal Parkinson’s disease. Int J Mol Sci. 2020;21(6):1961. doi:10.3390/ijms21061961
5. Zhang Y, Ren R, Sanford LD, et al. Sleep in Parkinson’s disease: a systematic review and meta-analysis of polysomnographic findings. Sleep Med Rev. 2020;51:101281. doi:10.1016/j.smrv.2020.101281
6. Tam DM, Linh LTT, Trang DT, Thi Ha An, T. Sleep disturbances and associated factors in patients with Parkinson’s disease. Clin Neurol Neurosurg. 2024;244:108436. doi:10.1016/j.clineuro.2024.108436
7. Lebrun C, Gély-Nargeot MC, Bayard S. L’insomnie dans la maladie de Parkinson Partie I: épidémiologie, évaluation et facteurs associés [Insomnia comorbid to Parkinson’s disease Part I: epidemiology, assessment, and related factors]. Geriatr Psychol Neuropsychiatr Vieil. 2020;18(3):321–330. doi:10.1684/pnv.2020.0874
8. Liu Y, Xue L, Zhao J, Dou K, Wang G, Xie A. Clinical characteristics in early Parkinson’s disease with excessive daytime sleepiness: a cross-sectional and longitudinal study. Clin Transl Sci. 2023;16(10):2033–2045. doi:10.1111/cts.13610
9. Breen DP, Vuono R, Nawarathna U, et al. Sleep and circadian rhythm regulation in early Parkinson disease. JAMA Neurol. 2014;71(5):589–595. doi:10.1001/jamaneurol.2014.65
10. Katsuki F, Gerashchenko D, Brown RE. Alterations of sleep oscillations in Alzheimer’s disease: a potential role for GABAergic neurons in the cortex, hippocampus, and thalamus. Brain Res Bull. 2022;187:181–198. doi:10.1016/j.brainresbull.2022.07.002
11. Galbiati A, Verga L, Giora E, Zucconi M, Ferini-Strambi L. The risk of neurodegeneration in REM sleep behavior disorder: a systematic review and meta-analysis of longitudinal studies. Sleep Med Rev. 2019;43:37–46. doi:10.1016/j.smrv.2018.09.008
12. Postuma RB, Berg D. Prodromal Parkinson’s disease: the decade past, the decade to come. Mov Disord. 2019;34(5):665–675. doi:10.1002/mds.27670
13. De Natale ER, Wilson H, Politis M. Predictors of RBD progression and conversion to synucleinopathies. Curr Neurol Neurosci Rep. 2022;22(2):93–104. doi:10.1007/s11910-022-01171-0
14. Rosenberg RS, Van Hout S. The American academy of sleep medicine inter-scorer reliability program: sleep stage scoring. J Clin Sleep Med. 2013;9(1):81–87. doi:10.5664/jcsm.2350
15. Anjum MF, Smyth C, Zuzuárregui R, et al. Multi-night cortico-basal recordings reveal mechanisms of NREM slow-wave suppression and spontaneous awakenings in Parkinson’s disease. Nat Commun. 2024;15(1):1793. doi:10.1038/s41467-024-46002-7
16. Cheng Z, Li Q, Zou X, et al. Cyclic alternating pattern of EEG activities and heart rate variability in parkinson’s disease patients during deep sleep. J Integr Neurosci. 2025;24(3):26397. doi:10.31083/JIN26397
17. Latreille V, Carrier J, Lafortune M, et al. Sleep spindles in Parkinson’s disease may predict the development of dementia. Neurobiol Aging. 2015;36(2):1083–1090. doi:10.1016/j.neurobiolaging.2014.09.009
18. Memon AA, Catiul C, Irwin Z, et al. Quantitative sleep electroencephalogram and cognitive performance in Parkinson’s disease with and without rapid eye movement sleep behavior disorder. Front Neurol. 2023;14:1223974. doi:10.3389/fneur.2023.1223974
19. Zahed H, Zuzuarregui JRP, Gilron R, Denison T, Starr PA, Little S. The neurophysiology of sleep in Parkinson’s disease. Mov Disord. 2021;36(7):1526–1542. doi:10.1002/mds.28562
20. Migueis DP, Lopes MC, Ignacio PSD, et al. A systematic review and meta-analysis of the cyclic alternating pattern across the lifespan. Sleep Med. 2021;85:25–37. doi:10.1016/j.sleep.2021.06.026
21. Doppler CEJ, Smit JAM, Hommelsen M, et al. Microsleep disturbances are associated with noradrenergic dysfunction in Parkinson’s disease. Sleep. 2021;44(8):zsab040. doi:10.1093/sleep/zsab040
22. Parrino L, Balella G, Bottignole D, et al. Phasic events, cyclic alternating pattern (CAP) and sleep disorders. Clin Neurophysiol. 2025;179:
23. Dodet P, During E, Arnulf I, et al. Sleep stage mixing is associated with poor prognosis in early Parkinson’s disease. NPJ Parkinsons Dis. 2025;11(1):275. doi:10.1038/s41531-025-01105-w
24. Wei R, Ganglberger W, Sun H, et al. Linking brain structure, cognition, and sleep: insights from clinical data. Sleep. 2024;47(2):zsad294. doi:10.1093/sleep/zsad294
25. Doppler CEJ, Smit J, Hommelsen M, et al. Disruption of sleep microarchitecture is a sensitive and early marker of Parkinson’s disease. J Parkinsons Dis. 2022;12(8):2555–2560. doi:10.3233/JPD-223442
26. Dagay A, Katzav S, Wasserman D, Gnoni V, Mirelman A, Tauman R. Cyclic alternating pattern dynamics in individuals at risk for developing Parkinson’s disease. Ann Neurol. 2025;98(1):136–146. doi:10.1002/ana.27217
27. Berg D, Borghammer P, Fereshtehnejad SM, et al. Prodromal Parkinson disease subtypes - key to understanding heterogeneity. Nat Rev Neurol. 2021;17(6):349–361. doi:10.1038/s41582-021-00486-9
28. Horsager J, Knudsen K, Sommerauer M. Clinical and imaging evidence of brain-first and body-first Parkinson’s disease. Neurobiol Dis. 2022;164:105626. doi:10.1016/j.nbd.2022.105626
29. Blesa J, Foffani G, Dehay B, Bezard E, Obeso JA. Motor and non-motor circuit disturbances in early Parkinson disease: which happens first? Nat Rev Neurosci. 2022;23(2):115–128. doi:10.1038/s41583-021-00542-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.