Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Cutaneous Lymphadenoma: A Case Report and Literature Review
Authors Dong J ![]() , Duan Y, Zhang K, Zhang X
, Duan Y, Zhang K, Zhang X
Received 26 June 2022
Accepted for publication 19 January 2023
Published 23 February 2023 Volume 2023:16 Pages 505—514
DOI https://doi.org/10.2147/CCID.S378468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Jie Dong,1 Yuntao Duan,2 Kunning Zhang,3 Xiuying Zhang1
1Department of Dermatology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Dermatology, Dali Bai Autonomous Prefecture People’s Hospital, Dali Medical College, Yunnan, People’s Republic of China; 3Department of Pathology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Xiuying Zhang, Department of Dermatology, Beijing Chaoyang Hospital, Capital Medical University, 8# South Road, Worker’s Stadium, Chaoyang District, Beijing, 100020, People’s Republic of China, Tel +86 15810698436, Email [email protected]
Abstract: Cutaneous lymphadenoma (CL) is an uncommon epithelioid tumor that is usually present on the head and face. It was first described by Santa Cruz and Barr in 1987, as a lymphoepithelial tumor, and was renamed as CL in 1991. Although CL is considered as a benign tumor, there are cases of recurrence after shave excision and metastasis to regional lymph nodes. Correct diagnosis and complete resection are of great importance. Here, we report a typical case of CL and make a comprehensive review of this rare skin tumor.
Keywords: cutaneous lymphadenoma, skin tumor, carcinoma
Introduction
CL is an uncommon skin neoplasm with a predilection for the head and face, particularly the cheek, eyebrow, and forehead. Less than 100 cases have been reported in the literature since it was named in 1991,1,2 of which, only 5 cases were reported by China. There is still controversy both on its histogenesis and diagnosis. A recent study showed that CL expressing hair follicle bulge stem cell CK15, PHLDA1 and androgen receptor (AR), considering that CL was a distinct benign lymphoepithelial tumor.3 Although it exhibits benign biologic behavior, it could resemble closely to other non-melanoma skin cancers both clinically and histologically, there are also cases of recurrence after shave excision and metastasis to regional lymph nodes, so recognition of CL is of great importance.4,5 Here we report a case of CL in an 80-year-old woman. Written informed consent for publication of the details was obtained from the patient.
Case Presentation
An 80-year-old woman claimed a single small nodule existed on the left side of her nose for 10 years, slowly increasing in size, without any uncomfortable feelings. She was otherwise in good health except for hypertension, with no previous history of any other skin diseases. Physical examination showed a clearly circumscribed semicircular nodule on the left side of the alar of her nose, 9 mm in diameter, skin color, moderate hardness, with smooth surface and telangiectasis, without ulcer and crust (see Figure 1). The clinical impression was a kind of adnexal tumor, and the lesion was completely excised with a 5-mm surgical margin of clinically normal skin and submitted for further histopathology and immunohistochemical study. No recurrence or metastasis had been observed since postoperative follow-ups for 1 year (both by clinical visit and telephone).
 |
Figure 1 A skin color, semicircular nodule on the left side of the alar of the nose, with telangiectasis on the surface. |
Histologic examination showed normal epidermis (See Figure 2), there were several well-circumscribed irregular shaped nodules in the dermis, which were enmeshed in a dense fibrous stroma. At higher magnification, the epithelial nodules were rimmed by a palisading of one or two layers of dark stained basaloid cells, without contraction gap around. In the center of the nodule, there were many large transparent cells with clear cytoplasm, rich in glycogen and vesicular nuclei (named Reed–Sternberg-like cells: RS-L cells), scattered with some lymphocytes. There were prominent lymphoid cells infiltration around the nodules (see Figures 2 and 3). Immunohistochemical study showed cytokeratin and epithelial membrane antigen (EMA) were positive (see Figure 4), and carcinoma embryonic antigen (CEA) was negative. The infiltration was composed of a mixture of T and B lymphocytes, with a predominance of T cells (see Figures 5 and 6). CD30+ cells (RS-L cells) (see Figure 7) are scattered in the center of the lobules, which may be representing activated lymphocytes and histiocytes. S100-positive dendritic cells were stained, and co-expressed CD1a (see Figures 8 and 9), possibly represent Langerhans cells.
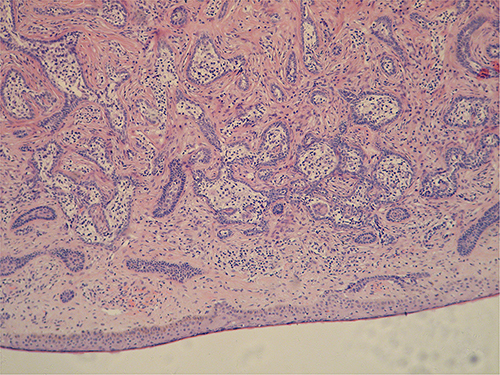 |
Figure 2 The tumor composed of irregularly shaped lobules enmeshed in a dense fibrous stroma. |
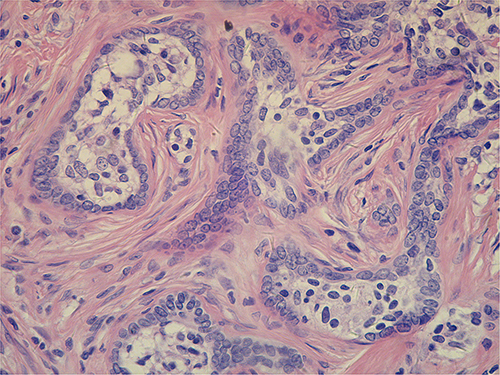 |
Figure 3 The lobules had a peripheral rim of 1 or 2 layers of basaloid cells, central RS-L cells, and lymphocytes infiltration around. (Magnification ×10). |
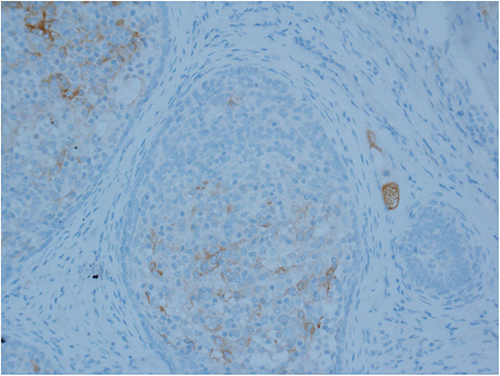 |
Figure 4 EMA-positive staining of the ductal structures. (Magnification ×200). |
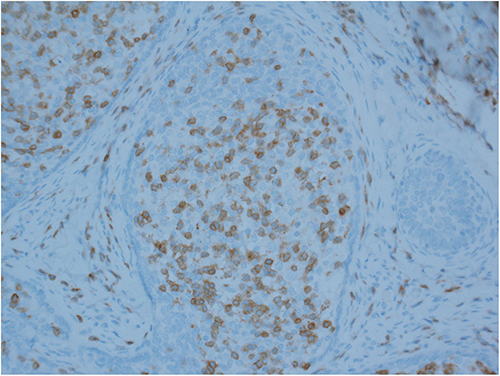 |
Figure 5 T cells were the predominantly infiltrated cells in CL, T cell receptor marker CD3. (Magnification ×200). |
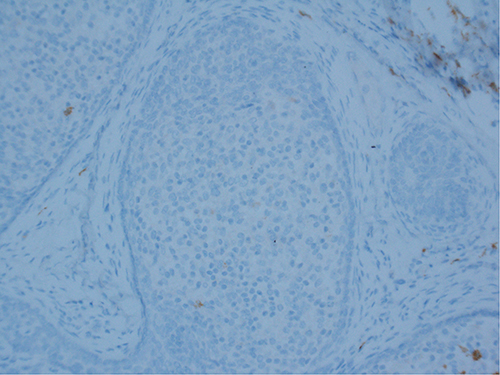 |
Figure 6 B cell marker CD20. (Magnification ×200). |
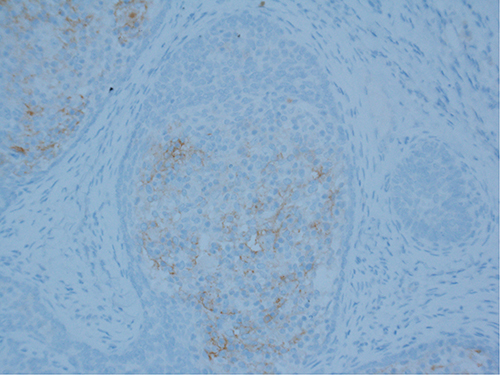 |
Figure 7 RS-L cell marker CD30. (Magnification ×200). |
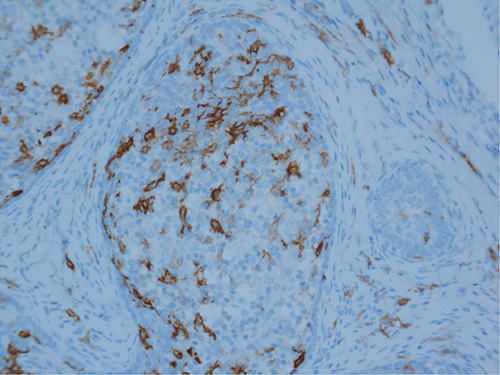 |
Figure 8 CD1a positive staining of many intralobular dendritic cells. (Magnification ×200). |
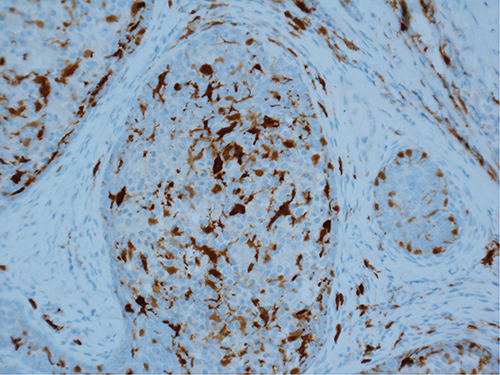 |
Figure 9 S-100-positive staining of many intralobular dendritic cells. (Magnification ×200). |
Discussion and Literature Review of CL
According to the typical histopathological and immunohistochemical characteristics, it is not difficult to make the correct diagnosis of CL in this case. Up to now, less than 100 cases of CL have been reported worldwide, and there was no significant gender difference, with ages varying from newborn to 90 years. Lesions are generally located on head and face, and only a few of them were found on leg, shoulder, or neck, suggesting that sun exposure might be an important trigger factor. Disease duration varied from 3 months to 40 years; most of the patients had only one nodule, and 1 patient had four nodules (congenital CL).6 One patient synchronously had CL on the right cheek and syringoid eccrine carcinoma on the scalp.7 Most of the patients had surgery excision without recurrence, four patients received MMS,8,9 one patient had shave excision and reoccurred,10 one patient metastasized in regional lymph nodes.5 Two patients had congenital CL,6,11 (see Table 1).
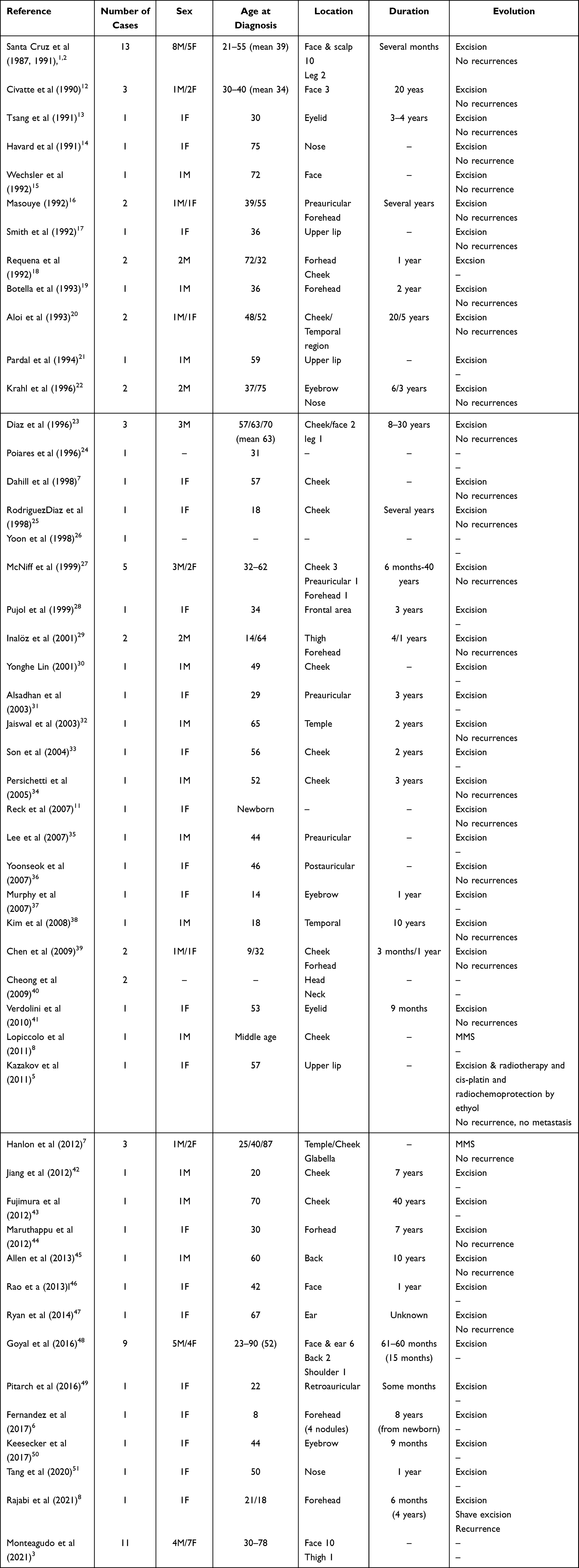 |
Table 1 Clinical Findings in 96 Cases of CL |
Typically, CL featured as slow growing, asymptomatic, skin-color or pink nodules, dome-shaped, usually on the head, particularly the cheek, eyebrow, and forehead, small sized (usually less than 1 cm in diameter). One reported case applied dermoscopic examination. It showed prominent telangiectatic vessels traversing the lesion and branching into finer capillaries. Three peripheral areas were appreciated, divided by the arborizing telangiectasis, with dotted vessels and some glomerular vessels on a white-to-pink background.49 Triphasic tumor with epithelial islands, lymphocytic infiltrates and desmoplastic stroma, unremarkable epidermis were the main histopathologic features of CL. A well-circumscribed tumor located on the dermis, consisting of lobules unconnected or occasionally connected in some areas to the epidermis. The lobules were constituted by a rim of basaloid cells and peripheral palisading, and a central area contained numerous inflammatory cells including lymphocytes (CD3+ T cells) and histiocytes (numerous Langerhans’ cells and the characteristic large RS-L cells with amphophilic cytoplasm, vesicular nuclei, and prominent nucleoli). No peritumoral cleft was visible. No mitoses or nuclear atypia was observed. Rudimentary follicular papillae/hair germs may be present focally. A dense and fibrotic stroma was surrounded the lobules. We also summarized the reported immunohistochemistry staining of CL (see Table 2).
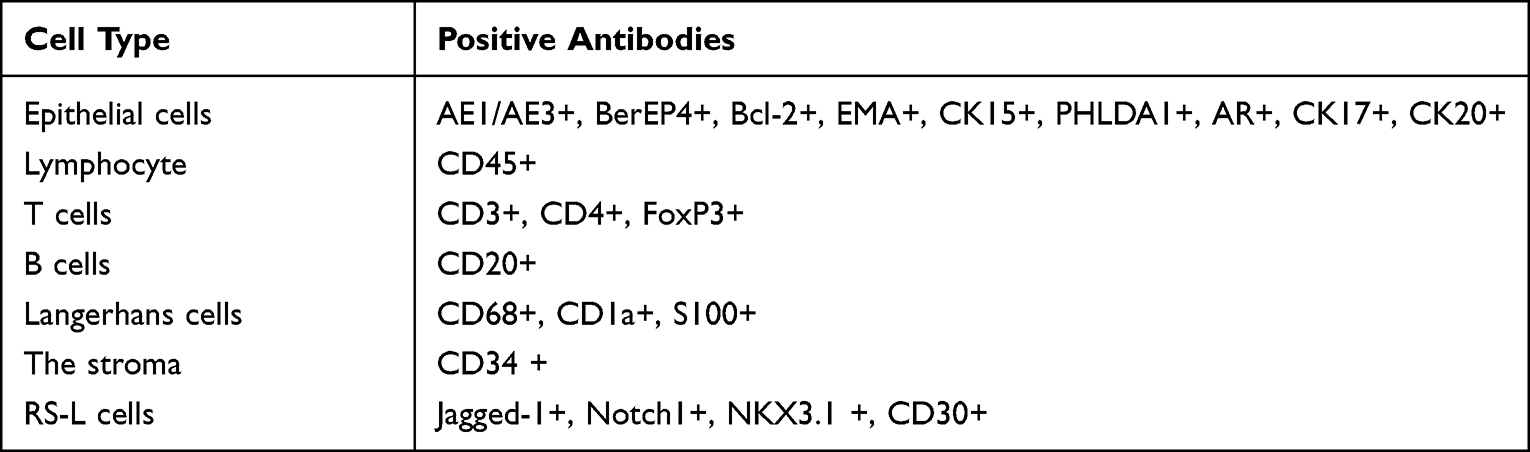 |
Table 2 Cell Types and Positive Immunostaining |
CL should be differentiated with several skin diseases presenting asymptomatic, chronically growth nodules in the head and neck area. Basal cell carcinoma (BCC) shows histological features not seen in CL, such as mitotic and apoptotic bodies, clefting artifact with stroma mucin in the retraction space. Furthermore, immunohistochemical study showed scattered Merkel cells (CK20+) in CL but absent in BCC. CK17, while a patchy and peripheral rim staining in the basaloid islands of CL, diffuse positive staining in BCC.48 Another useful marker, AR, which usually showed focal immunoreactivity in BCC, was diffuses strong immunostaining in CL.3 Trichoblastoma, many reports considered CL similar to trichoblastoma, CL was classified as an adamantoid variant of trichoblastoma in the latest WHO classification.52 However, there are differences in many aspects: firstly, there are intraepithelial lymphocytes and RS-L cells in CL, but not in trichoblastoma; secondly, the latest research found that although both CL and trichoblastoma were positive for CK15, CL was also positive for AR while the latter was AR negative.3 Trichoepithelioma, trichoepithelioma is a benign adnexal tumor of follicular germinative derivation. Although could be single, most are multiple and seen in patients with multiple familial trichoepithelioma or Brooke–Spiegler syndrome. They usually begin during puberty, often appear clinically and histologically similar to BCC.53 Furthermore, trichoepithelioma is AR negative.54 Lymphoepithelioma-like carcinoma of the skin(LELCS), LELCS normally affects elderly patients and most often found in the sun-exposed areas of the head. Histologically, LELCS is an epithelial neoplasm located mainly in the deep dermis and hypodermis, with atypical epithelial cells and mitotic figures, it is now classified as a variant of squamous cell carcinoma, and can be found in many organs besides the skin.55 Other diseases such as clear cell syringoma, dermal thymus, pseudolymphoma, congenital subcutaneous dendritic cell-rich lymphoepithelial hamartoma should also be differentiated.
As for the histogenesis, at the beginning, CL was suggested as adnexal origin since it had immature pilosebaceous differentiation. Later, some authors suggested it represented a form of BCC with pilar or eccrine differentiation and pilosebaceous neoplasm as it closely related to trichoepithelioma. In some cases, there were foci of ductal differentiation, with luminal positivity for CEA and EMA, and postulate that some CL represent a form of immature sweat gland tumor with ductal differentiation.19 Now it is classified as an adamantoid variant of trichoblastoma in the latest WHO classification.14 Recent studies showed that CL being a benign tumor with AR and hair follicle bulge stem cell marker (CK15) expression, RS-L cell-derived Notch 1 ligand, and common EGFR gene mutations.3 It is now considered different with trichoblastoma. Furthermore, EGFR hotspot missense mutations in CL were considered pathogenic, and it was hypothesized that EGFR mutations may provoke a continuous hair follicle stem cell proliferation, and together with the Notch pathway stimulation, responsible for CL tumor growth.3,56
Complete excision is currently the first treatment choice for CL. Recurrence and metastasis were rarely reported. To our knowledge, only one patient reoccurred after shave excision and one patient revealed metastatic involvement of submandibular lymph nodes. The reemergence of the lesion might be attributed to the insufficient margin of shave excision. The case of CL arising in association with a LELCS suggests that CL may rarely progress to a malignant neoplasm capable of metastatic spread. Mohs surgery was applied by four patients, considering the time-consuming and relatively expensiveness, Mohs surgery was particularly used in cases that the tumor margins were not clinically well defined or the tumor located in anatomically sensitive areas where tissue preservation is critical.
Conclusion
CL is a rare skin tumor, presented as slow growing and benign biological behavior. In clinic, it is easily misdiagnosed as BCC, pilomatricoma, skin cyst, etc. Complete surgical excision and histopathological examination are the main treatment and diagnosis methods at present. Histopathologically, it needs to be differentiated from BCC, trichoblastoma, trichoepithelioma, clear cell syringoma, dermal thymus, LELCS, etc. The pathogenesis is still unclear, mainly because the extremely low incidence, so it is difficult to obtain enough specimens for in-depth clinical and laboratory research. Since incomplete resection may cause recurrence, few patients even have the risk of malignancy and metastasis to regional lymph nodes. Physical therapy options such as freezing, laser and simple shaving should be avoided, but there is no need to overtreat either.
Acknowledgments
Publication of the case details was approved by Beijing Chaoyang Hospital, Capital Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Santa Cruz DJ, Barr RJ. Lymphoepithelial tumor of the skin. J Cutan Pathol. 1987;14:35.
2. Santa Cruz DJ, Barr RJ, Headington JT. Cutaneous lymphadenoma. Am J Surg Pathol. 1991;15(2):101–110. doi:10.1097/00000478-199102000-00001
3. Monteagudo C, Funez R, Sanchez-Sendra B, et al. Cutaneous Lymphadenoma Is a Distinct Trichoblastoma-like Lymphoepithelial Tumor with Diffuse Androgen Receptor Immunoreactivity, Notch1 Ligand in Reed-Sternberg-like Cells, and Common EGFR Somatic Mutations. Am J Surg Pathol. 2021;45(10):1382–1390. doi:10.1097/PAS.0000000000001727
4. Cives M, Mannavola F, Lospalluti L, et al. Non-Melanoma Skin Cancers: biological and Clinical Features. Int J Mol Sci. 2020;21(15):5394. doi:10.3390/ijms21155394. PMID: 32751327; PMCID: PMC7432795.
5. Kazakov DV, Banik M, Kacerovska D, Michal M. A cutaneous adnexal neoplasm with features of adamantinoid trichoblastoma (lymphadenoma) in the benign component and lymphoepithelial-like carcinoma in the malignant component: a possible case of malignant transformation of a rare trichoblastoma variant. Am J Dermatopathol. 2011;33(7):729–732. doi:10.1097/DAD.0b013e31820b7b87
6. Fernandez-Flores A, Nicklaus-Wollenteit I, Sathishkumar D, et al. Congenital cutaneous lymphadenoma. J Cutan Pathol. 2017;44(11):954–957. doi:10.1111/cup.13016
7. Dahill SW, Seywright M. Synchronous occurrence of cutaneous lymphadenoma and syringoid eccrine carcinoma in a single patient. Histopathology. 1998;33(1):89–90. doi:10.1046/j.1365-2559.1998
8. LoPiccolo MC, Chaffins ML, Kouba DJ. Mohs micrographic surgery for the treatment of cutaneous lymphadenoma. J Drugs Dermatol. 2011;10(11):1324–1326.
9. Hanlon A, Clayton A, Stasko T. Mohs micrographic surgery for cutaneous lymphadenoma. Dermatol Surg. 2012;38(9):1552–1554. doi:10.1111/j.1524-4725.2012.02445.x
10. Rajabi F, Kamyab K, Firooz A. Cutaneous Lymphadenoma: a Case of Recurrence after Shave Excision. Case Rep Dermatol Med. 2021;2021:5543404. doi:10.1155/2021/5543404
11. Reck SJ, Xia L, Dehner LP, Reising CA. Glandular congenital lymphadenoma. Pediatr Dermatol. 2007;24(5):547–550.
12. Civatte J, Moulonguet-Michau I, Marinho E, et al. Tumeur epithelio-lympho-histiocytaire. A propos de 3 cas. [Epithelio-lymphohistiocytic tumor. Apropos of 3 cases]. Ann Dermatol Venereol. 1990;117(6–7):441–444. French.
13. Tsang WY, Chan JK. So-called cutaneous lymphadenoma: a lymphotropic solid syringoma? Histopathology. 1991;19(4):382–385. doi:10.1111/j.1365-2559.1991.tb00058.x
14. Havard S, Grossin M, Belaich S, Bocquet L. Tumeur lympho-epitheliale cutanee. A propos d’un cas avec revue de la litterature et discussion nosologique. [Lympho-epithelial skin tumor. Case report with review of the literature and nosologic discussion]. Ann Pathol. 1991;11(4):248–252. French.
15. Wechsler J, Fromont G, Andre JM, Zafrani ES. Cutaneous lymphadenoma with focal mucinosis. J Cutan Pathol. 1992;19(2):142–144. doi:10.1111/j.1600-0560
16. Masouye I. Cutaneous lymphadenoma: report of 2 cases. Dermatology. 1992;185(1):62–65. doi:10.1159/000247406
17. Smith N, Whittaker S, Calonje F. Cutaneous lymphadenoma. Br J Dermatol. 1992;127(40):36.
18. Requena L, Sanchez Yus E. Cutaneous lymphadenoma with ductal differentiation. J Cutan Pathol. 1992;19(5):429–433. doi:10.1111/j.1600-0560.1992.tb00616.x
19. Botella R, Mackie RM. Cutaneous lymphadenoma: a case report and review of the literature. Br J Dermatol. 1993;128(3):339–341.
20. Aloi F, Tomasini C, Pippione M. Cutaneous lymphadenoma. A basal cell carcinoma with unusual inflammatory reaction pattern? Am J Dermatopathol. 1993;15(4):353–357.
21. Pardal-de-Oliveira F, Sanches A. Cutaneous lymphadenoma. Histopathology. 1994;25(4):384–387.
22. Krahl D, Kohl PK. Cutaneous lymphadenoma is distinct from basal cell carcinoma. JEADV. 1996;6:40–46.
23. Diaz-Cascajo C, Borghi S, Rey-Lopez A, et al. Cutaneous lymphadenoma. A peculiar variant of nodular trichoblastoma. Am J Dermatopathol. 1996;18(2):186–191. doi:10.1097/00000372-199604000-00012
24. Poiares-Baptista A, Tellechea O, Reis JP. Cutaneous lympho-epithelial tumor (cutaneous lymphadenoma). Nouvelles Dermatologiques. 1996;15(8):582–585.
25. Rodriguez-Diaz E, Roman C, Yuste M, et al. Cutaneous lymphadenoma: an adnexal neoplasm with intralobular activated lymphoid cells. Am J Dermatopathol. 1998;20(1):74–78. doi:10.1097/00000372-199802000-00015
26. Yoon IJ, Kim MK, Song KY. Cutaneous Lymphadenoma: a case report and Review of Literature. Korean J Pathol. 1998;32(4):309–311.
27. McNiff JM, Eisen RN, Glusac EJ. Immunohistochemical comparison of cutaneous lymphadenoma, trichoblastoma, and basal cell carcinoma: support for classification of lymphadenoma as a variant of trichoblastoma. J Cutan Pathol. 1999;26(3):119–124.
28. Pujol RM, Matias-Guiu X, Taberner R, et al. Benign lymphoepithelial tumor of the skin (“cutaneous lymphadenoma”). Dermatol Online J May. 1999;5(1):5.
29. Inaloz HS, Chowdhury MM, Knight AG. Cutaneous lymphadenoma. J Eur Acad Dermatol Venereol. 2001;15(5):481–483. doi:10.1046/j.1468-3083.2001.00302.x
30. Hayashi Y. Cutaneous Lymphadenoma (Adamantinoid Trichoblastoma) -Report of a Case. 2001.
31. Alsadhan A, Taher M, Shokravi M. Cutaneous lymphadenoma. J Am Acad Dermatol. 2003;49(6):1115–1116. doi:10.1016/s0190-9622(03
32. Jaiswal VR, Amirkhan RH, Hoang MP. Pathologic quiz case: a cutaneous nodule on the left temple. Cutaneous lymphadenoma (benign lymphoepithelial tumor of the skin). Arch Pathol Lab Med. 2003;127(12):e432–3. doi:10.5858/2003-127-e432-PQCACN
33. Son SW, Kim YC, Kim IH. Cutaneous lymphadenoma. Clin Exp Dermatol. 2005;30(1):89–90. doi:10.1111/j.1365-2230.2004.01686.x
34. Persichetti P, Langella M, Cogliandro A, et al. Cutaneous lymphoadenoma: a rare clinicopathological entity. J Exp Clin Cancer Res. 2005;24(3):497–499.
35. Lee JH, Lee JD, Cho SH. A Case of Cutaneous Lymphadenoma as a Variant of Trichoblastoma. Korean J Dermatol. 2007;45(11):1217–1220.
36. Yoonseok O, Minjeong K, Jawoong G, et al. A Case of Cutaneous Lymphadenoma. Korean J Dermatol. 2007;45(6):603–607.
37. Murphy M, Brierley T, Pennoyer J, et al. Lymphotropic adamantinoid trichoblastoma. Pediatr Dermatol. 2007;24(2):157–161.
38. Kim DS, Kim DY, Kwon YS, et al. Childhood [corrected] onset lymphadenoma [corrected]. Pediatr Dermatol. 2008;25(3):413–414.
39. Chen LQ, Chen HY, Ling M, et al. Two cases of cutaneous lymphadenoma: a histological and immunohistological study. Chine J Dermatol. 2009;42(7):445–447.
40. Cheong SH, Han YJ, Choi YW, et al. Two cases of cutaneous lymphadenoma. Korean J Dermatol. 2009;47(2):192–195.
41. Verdolini R, Stefanato CM. A pearly nodule on the upper eyelid. Cutaneous lymphadenoma. Clin Exp Dermatol. 2010;35(5):561–562. doi:10.1111/j.1365-2230.2009.03314.x
42. Jiang Y, Chen H, Sun J. Cutaneous lymphadenoma. Indian J Dermatol Venereol Leprol. 2012;78(5):652–654. doi:10.4103/0378-6323.100575
43. Fujimura T, Itoigawa A, Haga T, et al. Cutaneous lymphadenoma: a case report and immunohistochemical study. Case Rep Dermatol. 2012;4(1):50–55. doi:10.1159/000337196
44. Mamthappu T, Freeman A, Bunker C, et al. Adamantinoid trirhohlastoma: a rare clinicopathologic entity mimicking basal cell carcinoma. J Am Acad Dermalol. 2012;66(4):AB77.
45. Allen JE, Lundin K, Erentaite D. Cutaneous lymphadenoma with unusual localization. J Plast Reconstr Aesthet Surg. 2013;66(9):1300–1302. doi:10.1016/j.bjps.2013.04.033
46. Rao L, Monappa V, Musheb M. Cutaneous nodule on the face: adamantinoid trichoblastoma – a rare, unique tumor. Our Dermatology Online. 2013;4(2):218–220.
47. Yu R, Salama S, Alowami S. Cutaneous lymphadenoma: a rare case and brief review of a diagnostic pitfall. Rare Tumors. 2014;6(2):5358. doi:10.4081/rt.2014.5358
48. Goyal A, Solus JF, Chan MP, et al. Cytokeratin 17 is highly sensitive in discriminating cutaneous lymphadenoma (a distinct trichoblastoma variant) from basal cell carcinoma. J Cutan Pathol. 2016;43(5):422–429. doi:10.1111/cup.12700
49. Pitarch G, Botella-Estrada R. Dermoscopy of adamantinoid trichoblastoma. J Eur Acad Dermatol Venereol. 2016;30(2):345–346. doi:10.1111/jdv.12752
50. Keesecker S, Saab J, Magro CM, et al. Cutaneous Lymphadenoma: a Trichoblastoma with Regressive Inflammatory Changes. Facial Plast Surg. 2017;33(1):109–111. doi:10.1055/s-0036-1597951
51. Tang L, Liu BQ, Zhao JY, Wang L. A case report of cutaneous lymphodenoma. J Clin Dermatol. 2020;49(4):221–222.
52. Hurt MA, Kaddu S, Kutzner H, et al. Benign tumours with follicular differentiation. In: Le Boit P, Burg G, Weedon D, Sarasin A, editors. World Health Organization Classification of Tumours. Pathology and Genetics of Skin Tumours. Lyon: IARC Press; 2006:152–159.
53. Johnson H, Robles M, Kamino H, et al. Trichoepithelioma. Dermatol Online J. 2008;14(10):5.
54. Wang Q, Ghimire D, Wang J, et al. Desmoplastic trichoepithelioma: a clinicopathological study of three cases and a review of the literature. Oncol Lett. 2015;10(4):2468–2476. doi:10.3892/ol.2015.3517
55. Lassen CB, Lock-Andersen J. Lymphoepithelioma-like Carcinoma of the Skin: a Case with Perineural Invasion. Plast Reconstr Surg Glob Open. 2014;2(11):e252. doi:10.1097/GOX.0000000000000215
56. Cataloge of somatic Mutations in Cancer (COSMIC v92); 2020. Available from: https://cancer.sanger.ac.uk/cosmic/mutation.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.