")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Cutaneous hyphomycosis Caused by Purpureocillium lilacinus Infection Associated with Superficial Venipuncture: A Case Report
Authors Zhou L, Qi X, Guo G, Wang Y, Yang J, Yang D, Huang S
Received 21 May 2023
Accepted for publication 3 September 2023
Published 6 September 2023 Volume 2023:16 Pages 2437—2441
DOI https://doi.org/10.2147/CCID.S422290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Lijun Zhou,* Xinyu Qi,* Guiying Guo, Yanling Wang, Jianjun Yang, Dingbin Yang, Shuqiong Huang
Department of Dermatology, People’s Hospital of Leshan, Leshan, Sichuan, 614000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuqiong Huang, Department of Dermatology, People’s Hospital of Leshan, No. 238, Bai Ta Road, Shi Zhong Qu, Leshan, Sichuan, 614000, People’s Republic of China, Email [email protected]
Abstract: Cutaneous hyphomycosis caused by Purpureocillium lilacinus is a relatively uncommon event in patients, but there has been a gradual increase in reported cases. A 71-year-old female patient was hospitalized in May 2022 due to an acute episode of chronic obstructive pulmonary disease and received glucocorticoid infusion. The skin around the puncture point on the back of her right hand showed erythema, nodules, scabs, and pus discharge, which gradually worsened. Fungal examination revealed the presence of hyphae, while treatment with terbinafine was ineffective. After fungal culture, pathological analysis, and molecular biology identification techniques, this case was diagnosed as cutaneous and subcutaneous infections caused by Purpureocillium lilacinus. After 2 weeks of treatment with itraconazole, the patient recovered. Patients on long-term hormone preparations who undergo superficial venipuncture should be aware of the risk of skin damage and potential infection by Purpureocillium lilacinus. Prompt fungal culture, histopathological analysis, and molecular identification are crucial for accurate diagnosis. Antifungal susceptibility testing should be considered for effective treatment.
Keywords: infection of Purpureocillium lilacinus, superficial venipuncture, a case report, infection
Introduction
Cutaneous hyphomycosis refers to a superficial infection of the skin, hair, and nails caused by various species of hyphomycetes fungi.1 Symptoms include redness, itching, scaling, and sometimes the formation of lesions or ulcers. Common causative agents of cutaneous hyphomycosis include species of Fusarium, Aspergillus, and Scytalidium.2 Paecilomyces lilacinus, a common filamentous fungus, is ubiquitously found in various environments such as soil, decaying vegetation, insects, nematodes, and even as a laboratory air contaminant. It has the potential to cause infections in humans and other vertebrates. Luangsa-Ard J at al. have found that Purpureocillium was a new genus for the medically important Paecilomyces lilacinus.3 Thus, Paecilomyces lilacinus was renamed as Purpureocillium lilacinus since 2011. Pathogenic fungi infection has a high tendency to occur in immunocompromised hosts such as hematologic malignancies, organ transplantation, and systemic use of glucocorticoids. Iatrogenic infections should also be paid attention to.4 Through literature review we found a report about cutaneous infection of Purpureocillium lilacinus associated with peripheral insertion of a central catheter.5 Here we report a case of Purpureocillium lilacinus infection at the venipuncture site on the back of the right hand due to chronic obstructive pulmonary disease (COPD).
Case Presentation
A 71-year-old woman presented to our hospital with complaints of skin erythema, pain, and pus discharge on the back of her right hand for half a month. She developed symptoms of fatigue and asthma due to acute exacerbation of COPD. Hence, she received intravenous infusion of cefoperazone sulbactam for anti-infection, betamethasone for anti-inflammation, and other drugs to relieve cough phlegm, and asthma at a local hospital.
After venipuncture on the back of the right hand, the skin became red, swollen, painful, and started discharging pus. Half a month later, the symptoms gradually worsened and she was admitted to our department. In combination with the characteristics of her skin lesions, fungal culture and pathological features of the affected skin tissues, and molecular biological identification techniques, the case was diagnosed as cutaneous and subcutaneous infections caused by Purpureocillium lilacinus (as shown in Figure 1).
 |
Figure 1 The right hand presented with lesions before treatment. Notes: (A) Erythematous scales on the back of the right hand’s skin, along with local pustules, scaly crusts, and pus discharge under pressure. (B) Erythema nodules observed on the right forearm. |
We performed a skin biopsy of the red nodules on the right forearm. The pathological examination showed focal rupture of the squamous epithelium in the examined tissue, along with a large number of neutrophils. The tissue stained positive for periodic acid-Schiff and hexamine silver staining.
Additionally, we obtained pus and subcutaneous tissue from the dorsal skin of her right hand for bacterial smear and culture, fungal smear and culture, and acid-fast bacillus smear. The result showed negative acid-fast staining, occasional Gram-negative bacilli in the general bacterial smear, yeast-like fungal spores and hyphae in the fungal smear examination (Gram staining), growth of various coagulase-negative staphylococcus in the bacterial culture of pus and tissues, and the presence of Paecilomyces species in the fungal culture of pus and tissue. Mass spectrometry confirmed the identification of Paecilomyces (as shown in Figure 2A–C).
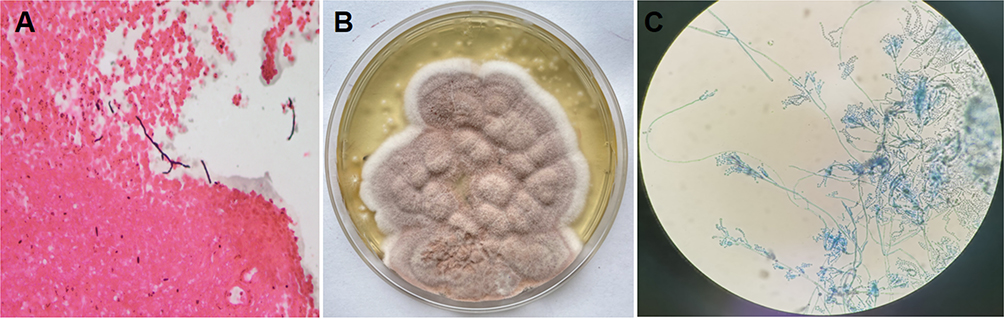 |
Figure 2 Microscopic findings, fungal colony morphology, and slide culture observations. Notes: (A) Under the microscope with a 40x magnification, hexamine silver staining revealed the presence of fungal hyphae. (B) The fungal colony was cultured on Sabouraud dextrose agar (SDA) at 28°C for 5 days. It displayed a woolly surface with a faint lilac color in the center and white color in the peripheral area. (C) Examination of lactophenol cotton blue-stained slides under a 400x magnification revealed the presence of long branching hyphae with septa, tapering phialides, and chain-like conidiophores. |
Diagnosis
Cutaneous and subcutaneous infections caused by Purpureocillium lilacinus.
Treatment
We opted for empirical therapy considering the frequent medication use in elderly patients and the potential for drug interactions. Additionally, we were concerned about the hepatotoxicity associated with itraconazole capsules. Therefore, our initial choice was to prescribe terbinafine hydrochloride tablets instead of itraconazole capsules. The patient initially received oral terbinafine hydrochloride tablets at a dose of 250mg per day. However, after 2 weeks of treatment, the patient returned for a follow-up appointment with aggravated skin lesions (as shown in Figure 3A and B), increased pustules within the skin lesions, and new-onset red nodules on the forearm. Therefore, the medication was changed to oral itraconazole capsules (Xi ‘an Janssen) at a dose of 200mg twice daily. After two weeks of treatment with itraconazole capsules, the patient’s skin lesions improved. There were no new-onset skin lesions, and the original skin lesions showed darkened erythema, reduced pustules, and desquamation. During subsequent phone follow-up, it was reported that the patient’s condition had improved.
 |
Figure 3 (A) Terbinafine hydrochloride tablets were taken orally for 2 weeks. (B) Itraconazole capsules were taken orally for 2 weeks. |
Discussion
Purpureocillium lilacinus, a hyaline hyphomycete widely found in soil and air globally, has the ability to infect individuals with both compromised and unimpaired immune systems.6 It frequently exhibits resistance to conventional antifungal medications and sterilization methods, leading to its recurrent contamination in lotions, as well as its potential colonization of clinical materials like catheters and plastic implants.7 Infections caused by Purpureocillium lilacinus often involve keratitis,8 subcutaneous and subcutaneous tissue infections,9 and onychomycosis10 especially in immunocompromised patients. This report documents the first recorded case of cutaneous hyphomycosis caused by Purpureocillium lilacinus infection associated with superficial venipuncture in our city.
In this case, the patient frequently experienced difficulty breathing and her immune function was impaired due to long-term use of hormone inhalation preparations. Th e local venipuncture caused skin infection, and the disease progression was exacerbated by the systemic use of hormones during hospitalization. Amphotericin B, flucytosine, and fluconazole have been reported to have low antibacterial activity against Purpureocillium lilacinus in vitro, while voriconazole has shown high antibacterial activity.11–13 However, this case was, an in vitro drug sensitivity test could not be conducted due to limited resources. The symptoms worsened after 2 weeks of oral terbinafine hydrochloride treatment, but improved after two weeks of itraconazole treatment. Follow-up over a span of three months revealed improvement in the patient’s condition without recurrence.
Conclusion
Patients who have been using long-term hormone preparations and undergoing superficial venipuncture should be aware of the potential risk of severe skin damage at the puncture site and the possibility of infection by Purpureocillium lilacinus. It is important to promptly conduct fungal culture, histopathological analysis, and molecular biology identification techniques to accurately diagnose the infection. Whenever possible, antifungal susceptibility testing should be performed to ensure appropriate and effective treatment.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
This study was designed in accordance with the Declaration of Helsinki and approved by the ethics committee of People’s Hospital of Leshan.
Consent for Publication
Signed consent was obtained from the patient for the publication of the case details included publication of the images.
Acknowledgments
We would like to acknowledge the reviewers for their helpful comments on this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds, grants, or other support was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Newton GD, Popovich NG. Fungal skin infections. In: Krinsky DL, Berardi RR, Ferreri SP, editors. Handbook of Nonprescription Drugs.
2. Gupta AK, Baran R, Summerbell RC. Fusarium infections of the skin. Curr Opin Infect Dis. 2000;13(2):121–128. doi:10.1097/00001432-200004000-00005
3. Luangsa-Ard J, Houbraken J, van Doorn T, et al. Purpureocillium, a new genus for the medically important Purpureocillium lilacinus. FEMS Microbiol Lett. 2011;321(2):e880–e882. doi:10.1111/j.1574-6968.2011.02322.x
4. Virginia CH, Sanjiva G, Mark DPD, et al. Cutaneous hyalohyphomycosis caused by Purpureocillium lilacinus: report of three cases and review of the literature. Int J Dermatol. 2004;43(9):648–653. doi:10.1111/j.1365-4632.2004.02175.x
5. Lin WL, Lin WC, Chiu CS. Purpureocillium lilacinus cutaneous infection associated with peripherally inserted central catheter insertion (Letter). J Eur Acad Dermatol Venereol. 2008;22(10):1267–1268.
6. Pastor FJ, Guarro J. Clinical manifestations, treatment and outcome of Paecilomyces lilacinus infections. Clin Microbiol Infect. 2006;12:948–960. doi:10.1111/j.1469-0691.2006.01481.x
7. Ezzedine K, Belin E, Guillet S, et al. Cutaneous hyphomycosis due to Paecilomyces lilacinus. Acta Derm Venereol. 2012;92(2):156–157. doi:10.2340/00015555-1179
8. Turner LD, Conrad D. Retrospective case-series of Purpureocillium lilacinus ocular mycoses in Queensland, Australia. BMC Res Notes. 2015;1–10. doi:10.1186/1756-0500-8-1
9. Nayak DR, Balakrishnan R, Nainani S, et al. Paecilomyces fungus infection of the paranasal sinuses. Int J Pediatr Otorhinolaryngol. 2000;52(2):183–187. doi:10.1016/S0165-5876(00)00282-2
10. Patrizia I, Elisabetta P, Dunja V, et al. Persisting Purpureocillium lilacinus nail infection following pregnancy. Mycoses. 2011;54(6):e880–e882. doi:10.1111/j.1439-0507.2011.02021.x
11. Loot ME, Sheehan DJ, Davis LS. Purpureocillium lilacinus infection with a sporotrichoid pattem in a renal transplant patient. J Drugs Dermatol. 2007;6(4):436–439.
12. Rimawi RH, Carter Y, Ware T, et al. Use of voriconazole for the treatment of Purpureocillium lilacinus cutanecous infection: case presentation and review of published literature. Mycopathologia. 2013;175(3–4):345–349. doi:10.1007/s11046-012-9610-3
13. Keshtkar-Jahromi M, McTighe AH, Segalman KA, et al. Unusual case of cutaneous and synovial Purpureocillium lilacinus infecition of hand successfully treated with voriconazole and review of published literature. Mycopathologia. 2012;174(3):255–258. doi:10.1007/s11046-012-9540-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.