Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Current Status and Research Trends in Deprescribing: A Bibliometric Review
Authors Shi C ![]() , Li X, Wu Y, Qin W
, Li X, Wu Y, Qin W ![]() , Liu L
, Liu L
Received 29 July 2025
Accepted for publication 11 November 2025
Published 18 November 2025 Volume 2025:17 Pages 239—252
DOI https://doi.org/10.2147/DHPS.S557043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Siew Siang Chua
Changcheng Shi,1,2 Xinyi Li,1,3 Yan Wu,4 Wangjun Qin,3 Lihong Liu1,3
1China-Japan Friendship Hospital (Institute of Clinical Medical Sciences), Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Key Laboratory of Clinical Cancer Pharmacology and Toxicology Research of Zhejiang Province, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, People’s Republic of China; 3Department of Pharmacy, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 4Department of Pharmacy, Ningbo Yinzhou No.2 Hospital, Ningbo, People’s Republic of China
Correspondence: Lihong Liu, China-Japan Friendship Hospital (Institute of Clinical Medical Sciences), Chinese Academy of Medical Sciences & Peking Union Medical College, No. 2, Yinghuayuan East Street, Chaoyang District, Beijing, People’s Republic of China, Email [email protected]
Background: Polypharmacy has emerged as a major global public health concern. To mitigate its adverse effects, deprescribing has been introduced and integrated into clinical practice. This study aims to analyze the current research landscape and identify emerging trends in deprescribing from a bibliometric perspective.
Methods: Relevant studies on deprescribing published prior to December 2024 were retrieved from the Web of Science Core Collection database. Bibliometric analysis and visualization of co-authorship, citation, co-citation, co-occurrence, and burst detection were performed using VOSviewer, CiteSpace, and Bibliometrix.
Results: A total of 1809 publications were identified, with a marked increase over the past decade. The field is dominated by contributions from developed countries, notably the United States, Australia, and Canada. Studies primarily focus on chronic conditions, such as psychiatric disorders, cardiometabolic diseases, and chronic pain, and the medications used to treat them. Influential publications highlighted barriers and facilitators of deprescribing, deprescribing tools, and deprescribing interventions and their associated outcomes. Burst detection analysis pointed to increasing attention on pharmaceutical care and implementation science.
Conclusion: This study presents the first comprehensive bibliometric overview of deprescribing. The findings demonstrate that the field has grown rapidly but remains dominated by developed countries and a limited set of chronic diseases. The integration of implementation science frameworks emerges as a promising approach to enhance the design and evaluation of deprescribing interventions. Future studies should broaden their scope to include a wider range of diseases and medications, and encourage greater participation from developing countries.
Keywords: deprescribing, polypharmacy, bibliometrics, implementation science
Introduction
Polypharmacy, commonly defined as the concurrent use of five or more medications, has emerged as a major public health concern worldwide.1 A meta-analysis of 54 studies estimated the overall prevalence of polypharmacy at 37%, with the rate increasing to 45% among individuals aged 65 years and older.2 Polypharmacy may contribute to drug-related problems, including adverse drug events, medication nonadherence, and drug interactions, which may significantly compromise patient outcomes and increase healthcare costs.3,4
To mitigate the adverse effects of polypharmacy, various interventions have been explored. Among these, deprescribing has emerged as a particularly promising approach.5 Deprescribing is the process of discontinuing potentially inappropriate medications (PIMs) under the supervision of healthcare professionals with the goal of managing polypharmacy and improving outcomes.6 Numerous studies have examined the impact of deprescribing on health outcomes, and a recently updated meta-analysis that integrated these findings concluded that deprescribing does not increase the risk of falls, fractures, emergency department visits, or unplanned hospitalizations. Furthermore, a survival benefit was observed in a subgroup analysis of patient-specific interventions.7 Deprescribing interventions can also help to reduce the overall medication burden by minimizing the use of PIMs, thereby lowering medication costs and additional expenses associated with inappropriate drug use. Several studies have evaluated the economic impact of deprescribing specific medications, such as sedatives8 and nonsteroidal anti-inflammatory drugs,9 and have consistently demonstrated the cost effectiveness of deprescribing.
Bibliometric analysis is a rigorous methodological approach that leverages bibliometric data to map the intellectual structure and identify emerging trends within a specific field.10 It has been widely applied in medical research.11 Although deprescribing has gained increasing attention in recent years, most existing reviews remain largely narrative.12 A previous bibliometric study examined publications only up to 2018 and focused narrowly on basic authorship patterns, without comprehensively analyzing collaboration networks, keyword co-occurrence, or emerging research themes.13 Therefore, the present study employs bibliometric methods to systematically map the current research landscape and identify emerging trends in deprescribing. These insights are intended to help researchers prioritize future investigations, support evidence-based clinical decision-making, and inform policy development in polypharmacy management.
Methods
This study follows the Guideline for Reporting Bibliometric Reviews of the Biomedical Literature (BIBLIO).14
Data Source and Search Strategy
The Web of Science (WOS) Core Collection database was searched to retrieve literature related to deprescribing. The search strategy employed in this study was TS = “(deprescribing OR deprescription OR deprescriptions OR deprescribe)”, where TS stands for “Topic”, indicating that the search was conducted within the title, abstract, and author keywords. The inclusion criteria were: (1) documents classified as articles or reviews; (2) published in English; (3) published before December 31, 2024; and (4) studies addressing deprescribing in any clinical context. The exclusion criteria were: (1) conference abstracts, book chapter, editorials, letters, notes, or other non-peer-reviewed publications; and (2) duplicate publications. The literature search and data extraction for this study were completed on February 15, 2025. All extracted data were double-checked independently by two authors to ensure accuracy.
Data Analysis and Visualization
Co-authorship analysis of countries, institutions, and authors, citation analysis of journals and publications, co-citation analysis of authors, journals, and references, and co-occurrence analysis of keywords were conducted using VOSviewer (version 1.6.18).15 A co-authorship analysis of countries with a focus on corresponding authors was conducted using Bibliometrix.16 Burst analysis of references and keywords was conducted using CiteSpace (version 6.4.R2 Advanced).17
In the co-authorship analysis of countries, Scotland, England, and Northern Ireland were combined into the United Kingdom, while the People’s Republic of China and Taiwan were unified as China. The visualization of institutional and author collaboration networks as well as keyword co-occurrence was generated by adjusting the “minimum number of documents” parameter, which resulted in the display of 100 entities. In the visualizing of the co-citation author network, the “minimum number of documents” parameter was set to 50. Other parameter settings for VOSviewer were left at their default values.
Author keywords were used for the keyword analysis. To avoid biasing the results toward overly general or self-evident terms, keywords directly related to deprescribing and its synonyms, as well as countries and research types, were excluded from the analysis (Table S1). Keywords that appeared in both singular and plural forms as well as full terms and abbreviations or synonyms were consolidated into a single form prior to analysis. The replaced and replacement keywords are provided in Table S2.
In the analysis conducted using CiteSpace, the time slicing was set from January 2011 to December 2024 with one year per slice. The parameters for the selection criteria, pruning, and burstness were set to their default values.
Results
Annual Publication Trends and Citation Impact
The flow chart illustrating the screening and selection process is shown in Figure S1. Our search strategy identified a total of 1809 publications spanning the period from 2011 to 2024. Of these, 1434 publications (79.3%) were classified as articles, whereas 375 (20.7%) were categorized as reviews. Over the past decade, the annual number of publications and citations on the topic of deprescribing has steadily increased. The number of annual publications rose from 15 in 2015 to 334 in 2024, whereas the number of annual citations surged from 167 in 2015 to 7001 in 2024 (Figure 1A).
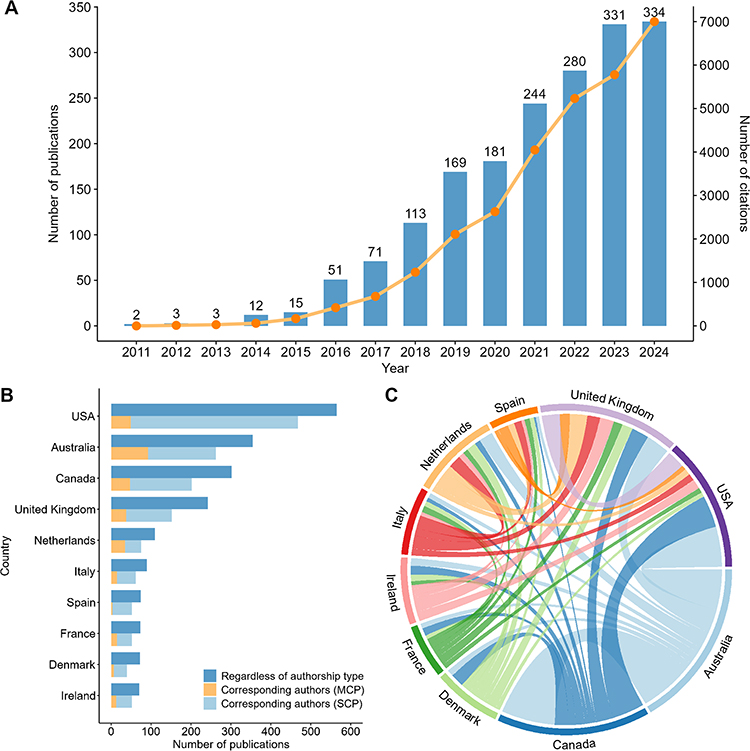 |
Figure 1 Publication trends, global contributions, and collaborations in deprescribing research: (A) Annual trends in publication volume and citation counts; (B) Top 10 countries by publication output; (C) Collaborative networks among the top 10 publishing countries. |
Co-Authorship Analysis of Countries
A total of 84 countries contributed to the field of deprescribing, with the United States (n = 565) leading in publication output, followed by Australia (n = 355) and Canada (n = 302). The countries ranked 4th to 10th in publication output were all European countries (Figure 1B). For publication data from other leading countries, please refer to Table S3. China ranked 20th in publication count, with a total of 23 publications.
Forty-four countries published more than five papers each. The publication collaborations among these countries are shown in Figure S2. Significant cooperation was observed between the United States, Australia, Canada, and European countries. Among the top 10 publishing countries, the median proportion of multiple country publications was 24.6%, with the Netherlands having the highest share at 46.7% (Figure 1B). Figure 1C illustrates the collaboration networks among the top 10 publishing countries in the field of deprescribing. The strongest collaborations were observed between Australia and Canada, followed by those between Australia and the United States. These collaborations highlight key international partnerships and can guide future research and collaboration opportunities.
Co-Authorship Analysis of Institutions
A total of 2785 institutions contributed to the field of deprescribing. The top 5 institutions by publication volume are listed in Table 1, with full details provided in Table S4. Among these, the University of Sydney emerges as the leading contributor, with the highest publication output (n = 151), significantly surpassing all other institutions. Monash University (n = 91) and the University of Toronto (n = 74) also demonstrate substantial publication productivity. In terms of citation impact, the University of Sydney retains its leading position with a total of 6160 citations, followed by the University of Queensland (n = 3824) and Dalhousie University (n = 2809). Figure 2A illustrates the collaboration network among the top 100 institutions by publication volume, which can be grouped into six clusters. The University of Sydney and Royal North Shore Hospital have the highest number of jointly published works, followed by collaboration between the University of Sydney and Dalhousie University. This indicates leading research hubs and potential centers for multicenter studies.
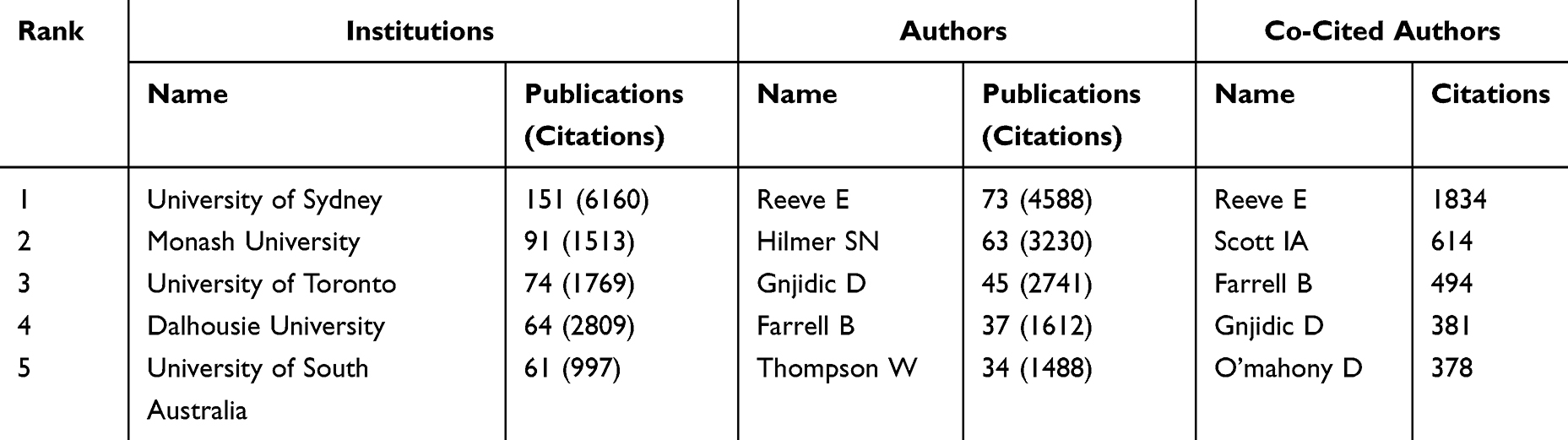 |
Table 1 Leading Institutions and Authors by Publications and Top Co-Cited Authors by Citations |
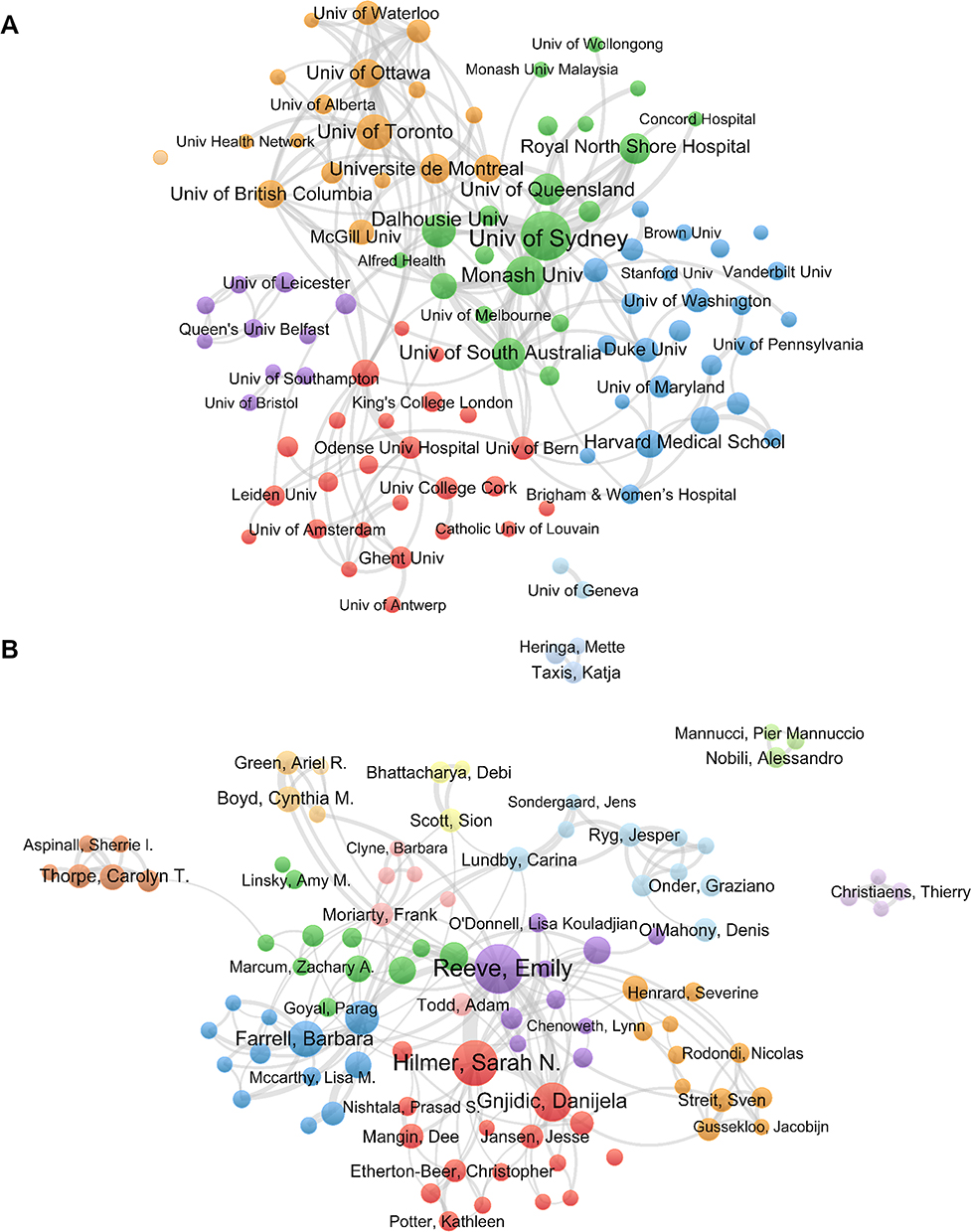 |
Figure 2 Visualization of collaborations among institutions and authors: (A) Top 100 institutions; (B) Top 100 authors. |
Co-Authorship and Co-Citation Analysis of Authors
A total of 7901 authors contributed to the field of deprescribing. The top 5 authors by publication count in the field of deprescribing are listed in Table 1, with full details provided in Table S4. Reeve E ranks first with 73 publications, followed by Hilmer SN (n = 63) and Gnjidic D (n = 45). Figure 2B illustrates the collaboration network among the top 100 authors by publication volume, which can be grouped into 11 clusters. The most frequent collaboration is between Reeve E, Hilmer SN, and Gnjidic D, followed by the collaboration between Farrell B and Thompson W. Identifying these author networks helps understand influential research groups and may guide new collaborations. The top 5 co-cited authors by citation count are presented in Table 1, with Reeve E (n = 1834) in the lead, followed by Scott IA (n = 614) and Farrell B (n = 494). Full details are provided in Table S4. A total of 122 co-cited authors were cited more than 50 times, and their co-citation network is illustrated in Figure S3.
Citation and Co-Citation Analysis of Journals
A total of 518 journals published at least one article on deprescribing. The Journal of the American Geriatrics Society led with the highest number of publications (n=79), followed by Research in Social and Administrative Pharmacy (n=62) and BMC Geriatrics (n=58). In the analysis of co-cited journals, a total of 120 journals were cited more than 100 times. The Journal of the American Geriatrics Society (n = 3644) had the highest number of citations, followed by Drugs & Aging (n = 2217) and the British Journal of Clinical Pharmacology (n = 1732). Leading journals by deprescribing publications and top co-cited journals by citations are presented in Tables 2 and S5. All of these journals are classified within the Journal Citation Reports as either Quartile 1 or Quartile 2.
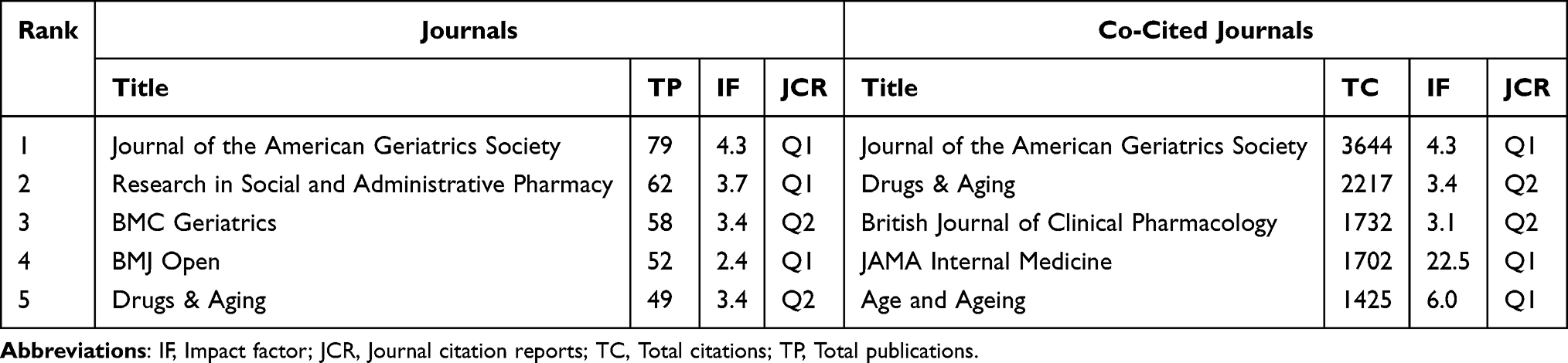 |
Table 2 Leading Journals by Deprescribing Publications and Top Co-Cited Journals by Citations |
Citation Analysis of Publications
Among the 1809 publications on deprescribing included in this study, the 10 most-cited publications are presented in Table S6. The study by Scott et al18 received the highest number of citations (n=993) and primarily proposed a five-step framework for implementing deprescribing. One systematic review investigated the barriers and facilitators that shape prescribers’ decisions to continue or discontinue PIMs,19 while another examined the factors that influence patients’ decision-making regarding deprescribing.20 Reeve et al6 conducted a comparative analysis of definitions of deprescribing in studies published before February 2014 and proposed a revised definition on the basis of their findings. Two studies21,22 focused on deprescribing interventions and their effects. Tannenbaum et al21 conducted a cluster-randomized trial and demonstrated that compared with usual care, a direct-to-consumer educational intervention significantly reduced benzodiazepine use. Page et al22 performed a meta-analysis of nonrandomized data and revealed that deprescribing was associated with a significant reduction in mortality. Farrell et al23 developed guidelines for deprescribing proton pump inhibitors (PPIs) and provided clinical recommendations on when and how to discontinue or taper PPI therapy. Additionally, two guidelines focused on the management of older adults24 and frailty,25 both of which advocated for deprescribing as a strategy to minimize inappropriate medication use. Another study highlighted the risk of adverse drug reactions in older adults and suggested that deprescribing should be considered when medications are no longer effective or when safer alternatives are available.26
Co-Citation and Burst Analysis of References
The top 10 most cited references in research on deprescribing are presented in Figure 3A. Among these, six references6,18–22 also appeared in the previously identified top 10 most cited publications on deprescribing. Among the remaining four highly cited references, three introduced criteria for identifying PIMs, including the STOPP/START criteria27 and the Beers criteria,28,29 whereas the other provided a systematic review of definitions of polypharmacy.1 The top 20 references with the strongest citation bursts are shown in Figure 3B. Nine of these are also among the 10 most-cited references. Two meta-analyses30,31 emerged as highly cited references in the past three years: one reported that a high proportion of patients (84%) and caregivers (80%) were willing to engage in deprescribing,30 whereas the other evaluated the impact of various deprescribing interventions on clinical outcomes.31
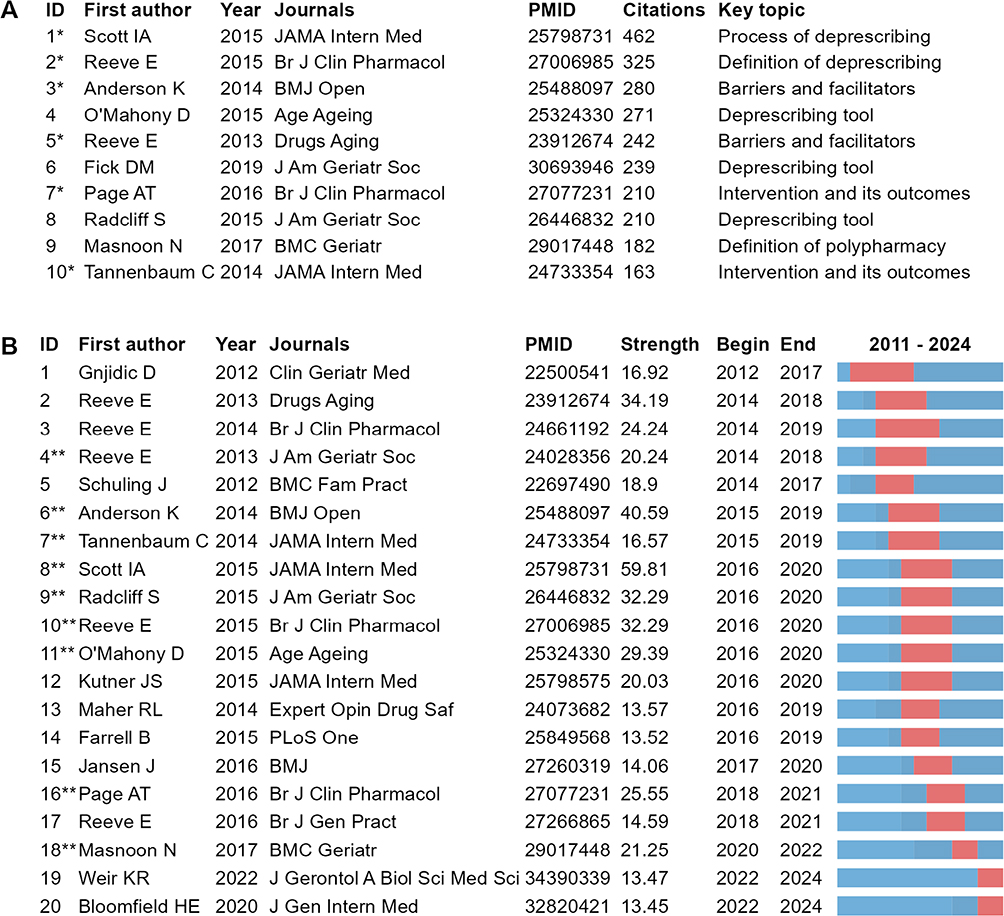 |
Figure 3 Co-citation and citation burst analysis of references: (A) Top 10 most cited references in deprescribing research; (B) Top 20 references with the strongest citation bursts. Notes: *Indicates that this reference is among the ten most cited publications on deprescribing; ** Indicates that this reference is also among the top ten most cited references. |
Co-Occurrence and Burst Analysis of Keywords
A total of 17 keywords appeared more than 50 times, with polypharmacy as the most common (n=525), followed by older adults (n=234) and potentially inappropriate medications (n=114). Additional high-frequency keywords are presented in Table S7.
For disease-related keywords, dementia (n=92) was the most prevalent and significantly exceeded other conditions. Among the medication-related keywords, benzodiazepines (n=74), proton pump inhibitors (n=54), and opioids (n=48) were the top three keywords in terms of frequency. Among the stakeholder-related keywords, pharmacists appeared most frequently (n=61), surpassing caregivers (n=17) and general practitioners (n=15). The frequencies of keywords categorized by disease, medication, and stakeholders are provided in Figure 4.
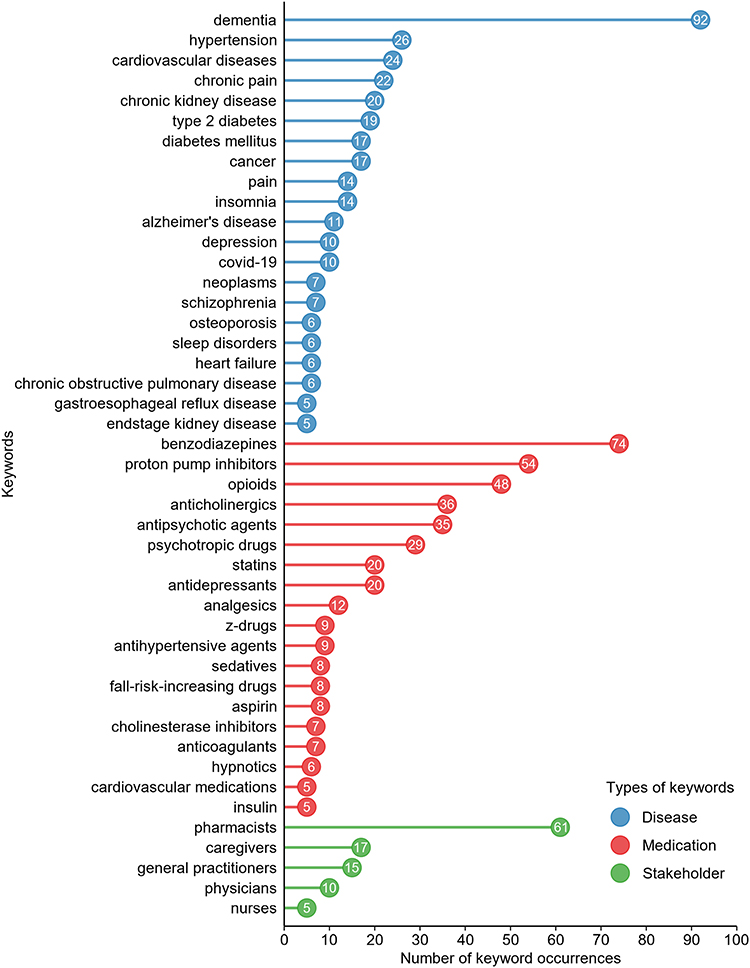 |
Figure 4 Frequency of keywords categorized by disease, medication, and stakeholder. |
The co-occurrence network of the top 100 most frequent keywords is depicted in Figure S4. These keywords are categorized into 7 clusters. Polypharmacy had the greatest co-occurrence with older adults, multimorbidity, medication review, and geriatrics. Figure S5 highlights the top 20 keywords with the strongest citation bursts. Pharmaceutical care and implementation science emerged as the most prominent burst keywords in the past three years.
Discussion
To our knowledge, this study is the first to employ bibliometric methods to explore the research landscape and development trends in the field of deprescribing. Over the past decade, the annual publication volume and citation counts in this domain have steadily increased, reflecting sustained scholarly interest and establishing deprescribing as a research hotspot. However, our findings highlight several challenges, including a geographical research imbalance, a limited range of diseases and medications studied, a high level of heterogeneity in intervention strategies, and a lack of a robust theoretical foundation. This study provides valuable insights into the current state of deprescribing research and offers guidance for future investigations.
Geographical Research Imbalance
Current publications on deprescribing are primarily concentrated in Western developed countries, including the United States, Australia, Canada, and European nations, where institutions and researchers maintain relatively close collaborative relationships. Notably, all of these countries or regions have established their own deprescribing networks. The first deprescribing network was founded in Australia in 2014 and was followed by the establishment of similar networks in Canada, the United States, and Europe.32,33 These networks share a common objective of enhancing medication appropriateness, minimizing unnecessary polypharmacy, and reducing the use of PIMs. Collectively, they have played a pivotal role in advancing deprescribing research and fostering international collaboration in this field.
China’s population is aging at an accelerating pace. Data indicate that the proportion of individuals aged 60 years and older in the total population will increase from 12.4% (168 million) in 2010 to 28% (402 million) by 2040.34 This demographic shift further exacerbates challenges related to multimorbidity, polypharmacy, and the use of PIMs among older adults. In China, the prevalence of multimorbidity among older adults exceeds 32%,35 whereas the rates of polypharmacy and PIM reach 48% and 39%, respectively.36 These figures highlight both the substantial population that could benefit from deprescribing interventions and China’s unique advantage for deprescribing research in terms of sample size. However, this field has received insufficient attention domestically, as evidenced by the notably low volume of related publications. Therefore, we strongly urge relevant authorities and scholars in China to recognize the importance of deprescribing research and actively promote its development.
Importantly, similar demographic transitions are also occurring in other developing countries. According to the World Population Ageing 2023 report by the United Nations, the population aged ≥65 years in the least developed countries is projected to nearly triple between 2023 and 2050, despite starting from a relatively low base.37 Moreover, WHO estimates suggest that by 2050, the majority of the global population aged 60 years and older will reside in low- and middle-income countries.38 These trends indicate that accelerated population aging is a widespread challenge across developing regions, not unique to China, and underscore the urgent need for research and policy innovations, including deprescribing interventions.
Patient Perspectives and Barriers
Deprescribing is a complex process that faces numerous challenges in clinical practice. Our bibliometric analysis shows that among the top 10 most cited references in deprescribing research, two studies specifically focus on the barriers and facilitators of deprescribing. Extensive research has explored the barriers to and facilitators of deprescribing from the perspectives of patients, healthcare providers, and the broader healthcare system. In this study, we identified a reference that has seen a sharp increase in citations over the past three years, reporting that up to 84% of patients were willing to discontinue one or more medications if recommended by their physician.30 However, a multinational survey conducted across 14 countries involving 1340 older adults with polypharmacy reported a lower proportion of 44%.39 Patient-level barriers to deprescribing may include a strong preference for continuing current medications, concerns about potential adverse effects of discontinuation, and discouragement from healthcare professionals.20,40 Furthermore, patients exhibit varied attitudes toward deprescribing: some resist it and prefer the status quo over uncertainty, others defer entirely to their physician’s recommendations, and a third group remains open to deprescribing but favors active involvement in decision-making.41 These findings highlight the need for personalized deprescribing strategies that are tailored to individual patients’ preferences and concerns.
Several systematic reviews have comprehensively summarized the barriers to and facilitators of deprescribing at the level of healthcare providers and the broader healthcare system;42,43 thus, this discussion will not be repeated here. Additionally, recent studies have increasingly focused on the barriers to and facilitators of deprescribing within specific classes of medication, including opioids,44 antidepressants,45 benzodiazepines,46 PPIs,47 and cardiovascular medications.48 A deeper understanding of these barriers and facilitators will enable the effective integration of deprescribing into clinical practice.
Research Scope and Deprescribing Tools
The scope of diseases and medications addressed in current deprescribing research remains limited. Our study revealed that deprescribing research has focused primarily on chronic conditions, including psychiatric disorders, cardiometabolic diseases, and chronic pain. Accordingly, the medications used to treat these conditions are the main subjects of deprescribing studies. The extensive research on these medications may be due to the increased prevalence of inappropriate medication use in clinical practice.49 An early study employed the modified Delphi method to identify 14 classes of medications that should be prioritized for deprescribing from the perspective of practitioners and recommended the development of deprescribing guidelines for these classes.50 Currently, specific deprescribing guidelines are available for medications such as benzodiazepine receptor agonists and other sedatives,51,52 antipsychotics,53 antihyperglycemic agents,54 PPIs,23 cholinesterase inhibitors, memantine,55 and opioid analgesics.56 These guidelines provide actionable recommendations for clinical deprescribing practices.
However, creating specific guidelines for individual drug classes is often time-consuming, and deprescribing recommendations are more commonly integrated into disease treatment guidelines as a smaller component. Recently, Langford et al conducted a comprehensive review of current clinical practice guidelines related to deprescribing recommendations. These authors reported significant variability in both the content and format of these recommendations, with few guidelines offering actionable advice on how to deprescribe.57 Future guideline development may need to place greater emphasis on how to implement deprescribing to make it more actionable in clinical practice.
Among the top 10 most-cited references, three studies focused on criteria for identifying PIMs. Similar to deprescribing guidelines, these criteria are regarded as essential tools that facilitate deprescribing.58 A wide range of tools has been developed to support deprescribing, but their proliferation may complicate clinical decision-making.59,60 The continuous emergence of new evidence may lead to delays in updating these tools because integrating new research findings requires time for systematic review, critical appraisal, and consensus among experts. As a result, updates may lag behind the latest evidence, potentially causing discrepancies in deprescribing recommendations depending on which criteria are applied. Furthermore, most existing tools have been designed for specific populations or drug classes, which limits their applicability across diverse clinical scenarios. To improve the utility and consistency of deprescribing efforts, a systematic review and integration of these tools are warranted. Ideally, these resources should be consolidated into an accessible format, such as a database, to facilitate retrieval and implementation in clinical practice. Although this process may be time consuming, it would provide significant value by advancing the adoption and effectiveness of deprescribing.
Role of Pharmacists and Multidisciplinary Teams
Polypharmacy management typically requires a multidisciplinary team that comprises physicians, pharmacists, nurses, and other healthcare professionals.61,62 Our bibliometric analysis revealed that “pharmacist” appeared significantly more frequently than other team members, and that “pharmaceutical care” has emerged as a keyword with recent citation bursts, highlighting the pivotal role of pharmacists in deprescribing. In recent years, an increasing number of deprescribing studies have been pharmacist-led and have demonstrated promising outcomes.63–67 Moreover, stakeholders, including patients, have shown a positive attitude toward pharmacists’ involvement in deprescribing.68,69 However, it is noteworthy that some physicians remain reluctant to collaborate with pharmacists in the medication use process. While these physicians acknowledge pharmacists’ contributions to dispensing and counseling, they do not regard them as highly beneficial in prescribing or monitoring.70 Therefore, identifying strategies to better integrate pharmacists into multidisciplinary teams and optimize their role in deprescribing is crucial.
Intervention Strategies and Implementation Science
Our study found that deprescribing interventions and their clinical outcomes are widely discussed topics. Various deprescribing strategies have been reported, including medication reviews,71,72 educational programs for patients63,73,74 and prescribers,75 computerized decision support tools,76,77 and family involvement.78 However, many studies have failed to demonstrate significant clinical benefits of deprescribing. Some researchers attribute this to challenges in translating research evidence into clinical practice.79,80
To address this issue, increasing attention has been given to implementation science, which was also identified in our citation burst analysis. Implementation science employs theories, models, and frameworks81 to identify key implementation barriers and facilitators, guide intervention strategies, and evaluate effectiveness. The Consolidated Framework for Implementation Research has been applied successfully to deprescribing interventions and has yielded promising results.82 Integrating implementation science into deprescribing research may be a critical direction for future studies.
Strengths and Limitations
To our knowledge, this study is the first to employ bibliometric methods to explore the research landscape and development trends in the field of deprescribing. Our findings offer valuable insights for practitioners and researchers, provide a comprehensive understanding of the field and serve as a useful reference for future research in this area. However, this study also has several limitations. First, the data used in this research were retrieved exclusively from the WOS database. While this database is globally regarded as one of the most comprehensive citation sources, relying on a single database may result in the exclusion of publications that are indexed only in other databases. However, some scholars argue that searching across multiple databases in bibliometric studies may not always be advantageous because differences in file formats and difficulties in accurate integration may lead to overlap and bias.83 Second, the language was limited to English in this study, which may have led us to overlook non-English publications, thereby introducing potential bias. Third, highly cited publications may be cited for either positive or negative reasons, and our study cannot effectively distinguish between these motivations.
Conclusion
This study provides the first comprehensive bibliometric analysis of deprescribing research, offering a systematic overview of its current state and emerging trends. While deprescribing has become a research hotspot, key challenges remain, including geographical imbalances, a narrow focus on certain diseases and medications, heterogeneity in intervention strategies, and the absence of a strong theoretical foundation. For researchers, these findings highlight the need to broaden the scope of investigation and adopt implementation science frameworks to strengthen study design and evaluation. For healthcare providers, the results underscore the importance of tailoring deprescribing strategies to diverse patient populations and clinical contexts. For policymakers and regulators, the findings suggest that investment in deprescribing research and international collaboration should consider demographic realities, such as the size of the aging population, to ensure recommendations are contextually appropriate. Addressing these gaps will be essential to advance deprescribing as an integral component of polypharmacy management and optimize patient outcomes.
Abbreviations
BIBLIO, Guideline for reporting bibliometric review of the biomedical literature; PIMs, Potentially inappropriate medications; PPIs, Proton pump inhibitors; WOS, Web of Science.
Data Sharing Statement
All data supporting the findings of this study are available within the paper. Raw data can be provided upon reasonable request from the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Research and Development Program of China (grant number: 2024ZD0522305), the Medical and Health Research Project of Zhejiang Province (grant number: 2025KY1093) and the Hangzhou Special Scientific Program for Supporting the Development of the Biomedical and Health Industry (grant number: 2024WJC008).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
2. Delara M, Murray L, Jafari B, et al. Prevalence and factors associated with polypharmacy: a systematic review and meta-analysis. BMC Geriatr. 2022;22(1):601. doi:10.1186/s12877-022-03279-x
3. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57–65. doi:10.1517/14740338.2013.827660
4. Wastesson JW, Morin L, Tan ECK, Johnell K. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf. 2018;17(12):1185–1196. doi:10.1080/14740338.2018.1546841
5. Kurczewska-Michalak M, Lewek P, Jankowska-Polańska B, et al. Polypharmacy management in the older adults: a scoping review of available interventions. Front Pharmacol. 2021;12:734045. doi:10.3389/fphar.2021.734045
6. Reeve E, Gnjidic D, Long J, Hilmer S. A systematic review of the emerging definition of ‘deprescribing’ with network analysis: implications for future research and clinical practice. Br J Clin Pharmacol. 2015;80(6):1254–1268. doi:10.1111/bcp.12732
7. Quek HW, Page A, Lee K, et al. The effect of deprescribing interventions on mortality and health outcomes in older people: an updated systematic review and meta-analysis. Br J Clin Pharmacol. 2024;90(10):2409–2482. doi:10.1111/bcp.16200
8. Turner JP, Sanyal C, Martin P, Tannenbaum C. Economic evaluation of sedative deprescribing in older adults by community pharmacists. J Gerontol a Biol Sci Med Sci. 2021;76(6):1061–1067. doi:10.1093/gerona/glaa180
9. Sanyal C, Turner JP, Martin P, Tannenbaum C. Cost-effectiveness of pharmacist-led deprescribing of NSAIDs in community-dwelling older adults. J Am Geriatr Soc. 2020;68(5):1090–1097. doi:10.1111/jgs.16388
10. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. 2021;133:285–296. doi:10.1016/j.jbusres.2021.04.070
11. Kokol P, Blažun Vošner H, Završnik J. Application of bibliometrics in medicine: a historical bibliometrics analysis. Health Info Libr J. 2021;38(2):125–138. doi:10.1111/hir.12295
12. Zimmerman KM, Linsky AM. A narrative review of updates in deprescribing research. J Am Geriatr Soc. 2021;69(9):2619–2624. doi:10.1111/jgs.17273
13. Pan J, Xu Z, Zhu Y, Fang L. Bibliometric analysis of deprescribing on web of science. Chinese General Pract. 2020;23(6):747–754.
14. Montazeri A, Mohammadi S, M Hesari P, Ghaemi M, Riazi H, Sheikhi-Mobarakeh Z. Preliminary guideline for reporting bibliometric reviews of the biomedical literature (BIBLIO): a minimum requirements. Syst Rev. 2023;12(1):239. doi:10.1186/s13643-023-02410-2
15. van Eck N, Waltman L. Software survey: vosviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
16. Aria M, Cuccurullo C. Bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetrics. 2017;11(4):959–975. doi:10.1016/j.joi.2017.08.007
17. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
18. Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med. 2015;175(5):827–834. doi:10.1001/jamainternmed.2015.0324
19. Anderson K, Stowasser D, Freeman C, Scott I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: a systematic review and thematic synthesis. BMJ Open. 2014;4(12):e006544. doi:10.1136/bmjopen-2014-006544
20. Reeve E, To J, Hendrix I, Shakib S, Roberts MS, Wiese MD. Patient barriers to and enablers of deprescribing: a systematic review. Drugs Aging. 2013;30(10):793–807. doi:10.1007/s40266-013-0106-8
21. Tannenbaum C, Martin P, Tamblyn R, Benedetti A, Ahmed S. Reduction of inappropriate benzodiazepine prescriptions among older adults through direct patient education: the EMPOWER cluster randomized trial. JAMA Intern Med. 2014;174(6):890–898. doi:10.1001/jamainternmed.2014.949
22. Page AT, Clifford RM, Potter K, Schwartz D, Etherton-Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review and meta-analysis. Br J Clin Pharmacol. 2016;82(3):583–623. doi:10.1111/bcp.12975
23. Farrell B, Pottie K, Thompson W, et al. Deprescribing proton pump inhibitors: evidence-based clinical practice guideline. Can Fam Physician. 2017;63(5):354–364.
24. Izquierdo M, Merchant RA, Morley JE, et al. International exercise recommendations in older adults (ICFSR): expert consensus guidelines. J Nutr Health Aging. 2021;25(7):824–853. doi:10.1007/s12603-021-1665-8
25. Dent E, Lien C, Lim WS, et al. The Asia-Pacific clinical practice guidelines for the management of frailty. J Am Med Dir Assoc. 2017;18(7):564–575. doi:10.1016/j.jamda.2017.04.018
26. Lavan AH, Gallagher P. Predicting risk of adverse drug reactions in older adults. Ther Adv Drug Saf. 2016;7(1):11–22. doi:10.1177/2042098615615472
27. O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218. doi:10.1093/ageing/afu145
28. By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American geriatrics society 2019 updated AGS Beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
29. By the American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American geriatrics society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227–2246. doi:10.1111/jgs.13702
30. Weir KR, Ailabouni NJ, Schneider CR, Hilmer SN, Reeve E. Consumer attitudes towards deprescribing: a systematic review and meta-analysis. J Gerontol a Biol Sci Med Sci. 2022;77(5):1020–1034. doi:10.1093/gerona/glab222
31. Bloomfield HE, Greer N, Linsky AM, et al. Deprescribing for community-dwelling older adults: a systematic review and meta-analysis. J Gen Intern Med. 2020;35(11):3323–3332. doi:10.1007/s11606-020-06089-2
32. McDonald EG, Lundby C, Thompson W, et al. Reducing potentially inappropriate polypharmacy at a national and international level: the impact of deprescribing networks. Expert Rev Clin Pharmacol. 2024;17(5–6):433–440. doi:10.1080/17512433.2024.2355270
33. Boyd CM, Steinman MA. The U.S. deprescribing research network: catalyzing research and action to optimize medication use in older adults. J Am Geriatr Soc. 2024;72(5):1611–1613. doi:10.1111/jgs.18856
34. World Health Organization. China country assessment report on ageing and health. Geneva: World Health Organization; 2015. Available from: https://www.who.int/publications/i/item/9789241509312.
35. Hu Y, Wang Z, He H, Pan L, Tu J, Shan G. Prevalence and patterns of multimorbidity in China during 2002-2022: a systematic review and meta-analysis. Ageing Res Rev. 2024;93:102165. doi:10.1016/j.arr.2023.102165
36. Tian F, Chen Z, Wu J. Prevalence of polypharmacy and potentially inappropriate medications use in elderly Chinese patients: a systematic review and meta-analysis. Front Pharmacol. 2022;13:862561. doi:10.3389/fphar.2022.862561
37. United Nations, Department of Economic and Social Affairs, Population Division. World population ageing 2023: challenges and opportunities of population ageing in the least developed countries. New York: United Nations; 2024. Available from: https://desapublications.un.org/publications/world-population-ageing-2023-challenges-and-opportunities-population-ageing-least.
38. World Health Organization. Ageing and Health. Geneva: World Health Organization; 2024. Available from: https://www.who.int/en/news-room/fact-sheets/detail/ageing-and-health.
39. Vidonscky Lüthold R, Jungo KT, Weir KR, et al. Older adults’ attitudes toward deprescribing in 14 countries. JAMA Network Open. 2025;8(2):e2457498. doi:10.1001/jamanetworkopen.2024.57498
40. Bolt J, Abdoulrezzak R, Inglis C. Barriers and enablers to deprescribing of older adults and their caregivers: a systematic review and meta-synthesis. Eur Geriatr Med. 2023;14(6):1211–1222. doi:10.1007/s41999-023-00879-7
41. Weir K, Nickel B, Naganathan V, et al. Decision-making preferences and deprescribing: perspectives of older adults and companions about their medicines. J Gerontol B Psychol Sci Soc Sci. 2018;73(7):e98–e107. doi:10.1093/geronb/gbx138
42. Hung A, Kim YH, Pavon JM. Deprescribing in older adults with polypharmacy. BMJ. 2024;385:e074892.
43. Thompson W, McDonald EG. Polypharmacy and deprescribing in older adults. Annu Rev Med. 2024;75(1):113–127. doi:10.1146/annurev-med-070822-101947
44. Hamilton M, Mathieson S, Gnjidic D, et al. Barriers, facilitators, and resources to opioid deprescribing in primary care: experiences of general practitioners in Australia. Pain. 2022;163(4):e518–e526. doi:10.1097/j.pain.0000000000002340
45. Atkins B, Maden M, Birt L, et al. Primary care healthcare professionals supporting patients to discontinue antidepressants: a scoping review of barriers, enablers and interventions. Res Social Adm Pharm. 2025;21(6):431–443. doi:10.1016/j.sapharm.2025.02.004
46. Shapoval V, de Saint Hubert M, Evrard P, et al. Barriers to deprescribing benzodiazepines in older adults in a survey of European physicians. JAMA Network Open. 2025;8(3):e2459883. doi:10.1001/jamanetworkopen.2024.59883
47. Japelj N, Knez L, Petek D, Horvat N. Improving the feasibility of deprescribing proton pump inhibitors: GPs’ insights on barriers, facilitators, and strategies. Front Pharmacol. 2024;15:1468750. doi:10.3389/fphar.2024.1468750
48. Brunner L, Rodondi N, Aubert CE. Barriers and facilitators to deprescribing of cardiovascular medications: a systematic review. BMJ Open. 2022;12(12):e061686. doi:10.1136/bmjopen-2022-061686
49. Ndai A, Al Bahou J, Morris E, et al. Mapping potentially inappropriate medications in older adults using the anatomical therapeutic chemical (ATC) classification system. J Am Geriatr Soc. 2024;72(1):126–138. doi:10.1111/jgs.18681
50. Farrell B, Tsang C, Raman-Wilms L, Irving H, Conklin J, Pottie K. What are priorities for deprescribing for elderly patients? Capturing the voice of practitioners: a modified delphi process. PLoS One. 2015;10(4):e0122246. doi:10.1371/journal.pone.0122246
51. Pottie K, Thompson W, Davies S, et al. Deprescribing benzodiazepine receptor agonists: evidence-based clinical practice guideline. Can Fam Physician. 2018;64(5):339–351.
52. Palagini L, Brugnoli R, Dell’ Osso BM, et al. Clinical practice guidelines for switching or deprescribing hypnotic medications for chronic insomnia: results of European neuropsychopharmacology and sleep expert’s consensus group. Sleep Med. 2025;128:117–126. doi:10.1016/j.sleep.2025.01.033
53. Bjerre LM, Farrell B, Hogel M, et al. Deprescribing antipsychotics for behavioural and psychological symptoms of dementia and insomnia: evidence-based clinical practice guideline. Can Fam Physician. 2018;64(1):17–27.
54. Farrell B, Black C, Thompson W, et al. Deprescribing antihyperglycemic agents in older persons: evidence-based clinical practice guideline. Can Fam Physician. 2017;63(11):832–843.
55. Reeve E, Farrell B, Thompson W, et al. Deprescribing cholinesterase inhibitors and memantine in dementia: guideline summary. Med J Aust. 2019;210(4):174–179. doi:10.5694/mja2.50015
56. Langford AV, Lin CC, Bero L, et al. Clinical practice guideline for deprescribing opioid analgesics: summary of recommendations. Med J Aust. 2023;219(2):80–89. doi:10.5694/mja2.52002
57. Langford AV, Warriach I, McEvoy AM, et al. What do clinical practice guidelines say about deprescribing? A scoping review. BMJ Qual Saf. 2024;34(1):28–39. doi:10.1136/bmjqs-2024-017101
58. Reeve E. Deprescribing tools: a review of the types of tools available to aid deprescribing in clinical practice. J Pharm Pract Res. 2020;50(1):98–107. doi:10.1002/jppr.1626
59. Mejías-Trueba M, Fernández-Rubio B, Rodríguez-Pérez A, Bernabeu-Wittel M, Sánchez-FIdalgo S. Identification and characterisation of deprescribing tools for older patients: a scoping review. Res Social Adm Pharm. 2022;18(9):3484–3491. doi:10.1016/j.sapharm.2022.03.008
60. Anlay DZ, Paque K, Van Leeuwen E, Cohen J, Dilles T. Tools and guidelines to assess the appropriateness of medication and aid deprescribing: an umbrella review. Br J Clin Pharmacol. 2024;90(1):12–106. doi:10.1111/bcp.15906
61. Baruth JM, Gentry MT, Rummans TA, Miller DM, Burton MC. Polypharmacy in older adults: the role of the multidisciplinary team. Hosp Pract. 2020;48(sup1):56–62. doi:10.1080/21548331.2019.1706995
62. Tarrant C, Lewis R, Armstrong N. Polypharmacy and continuity of care: medicines optimisation in the era of multidisciplinary teams. BMJ Qual Saf. 2023;32(3):121–124. doi:10.1136/bmjqs-2022-015082
63. Martin P, Tamblyn R, Benedetti A, Ahmed S, Tannenbaum C. Effect of a pharmacist-led educational intervention on inappropriate medication prescriptions in older adults: the D- PRESCRIBE randomized clinical trial. JAMA. 2018;320(18):1889–1898. doi:10.1001/jama.2018.16131
64. Green AR, Quiles R, Daddato AE, et al. Pharmacist-led telehealth deprescribing for people living with dementia and polypharmacy in primary care: a pilot study. J Am Geriatr Soc. 2024;72(7):1973–1984. doi:10.1111/jgs.18867
65. Hurley E, Dalton K, Byrne S, Foley T, Walsh E. Pharmacist-led deprescribing using STOPPFrail for frail older adults in nursing homes. J Am Med Dir Assoc. 2024;25(9):105122. doi:10.1016/j.jamda.2024.105122
66. Crutzen S, Baas G, Denig P, Heringa M, Taxis K. Pharmacist-led intervention aimed at deprescribing and appropriate use of cardiometabolic medication among people with type 2 diabetes. Res Social Adm Pharm. 2023;19(5):783–792. doi:10.1016/j.sapharm.2022.11.009
67. Chan M, Plakogiannis R, Stefanidis A, Chen M, Saraon T. Pharmacist-led deprescribing for patients with polypharmacy and chronic disease states: a retrospective cohort study. J Pharm Pract. 2023;36(5):1192–1200. doi:10.1177/08971900221097246
68. Kassis A, Moles R, Carter S. Stakeholders’ perspectives and experiences of the pharmacist’s role in deprescribing in ambulatory care: a qualitative meta-synthesis. Res Social Adm Pharm. 2024;20(8):697–712. doi:10.1016/j.sapharm.2024.04.014
69. Bužančić I, Dragović P, Pejaković TI, Markulin L, Ortner-Hadžiabdić M. Exploring patients’ attitudes toward deprescribing and their perception of pharmacist involvement in a European country: a cross-sectional study. Patient Prefer Adherence. 2021;15:2197–2208. doi:10.2147/PPA.S323846
70. Kim E, Worley MM, Law AV. Pharmacist roles in the medication use process: perceptions of patients, physicians, and pharmacists. J Am Pharm Assoc. 2023;63(4):1120–1130. doi:10.1016/j.japh.2023.05.013
71. Seppala LJ, Kamkar N, van Poelgeest EP, et al. Medication reviews and deprescribing as a single intervention in falls prevention: a systematic review and meta-analysis. Age Ageing. 2022;51(9):afac191. doi:10.1093/ageing/afac191
72. Carollo M, Crisafulli S, Vitturi G, et al. Clinical impact of medication review and deprescribing in older inpatients: a systematic review and meta-analysis. J Am Geriatr Soc. 2024;72(10):3219–3238. doi:10.1111/jgs.19035
73. Jones KF, Stolzmann K, Wormwood J, et al. Patient-directed education to promote deprescribing: a nonrandomized clinical trial. JAMA Intern Med. 2024;184(11):1339–1346. doi:10.1001/jamainternmed.2024.4739
74. Bayliss EA, Shetterly SM, Drace ML, et al. Deprescribing education vs usual care for patients with cognitive impairment and primary care clinicians: the OPTIMIZE pragmatic cluster randomized trial. JAMA Intern Med. 2022;182(5):534–542. doi:10.1001/jamainternmed.2022.0502
75. Pimlott NJ, Hux JE, Wilson LM, Kahan M, Li C, Rosser WW. Educating physicians to reduce benzodiazepine use by elderly patients: a randomized controlled trial. CMAJ. 2003;168(7):835–839.
76. McDonald EG, Wu PE, Rashidi B, et al. The MedSafer study-electronic decision support for deprescribing in hospitalized older adults: a cluster randomized clinical trial. JAMA Intern Med. 2022;182(3):265–273. doi:10.1001/jamainternmed.2021.7429
77. Groos SS, de Wildt KK, van de Loo B, et al. Development of the ADFICE_IT clinical decision support system to assist deprescribing of fall-risk increasing drugs: a user-centered design approach. PLoS One. 2024;19(9):e0297703. doi:10.1371/journal.pone.0297703
78. Mortsiefer A, Löscher S, Pashutina Y, et al. Family conferences to facilitate deprescribing in older outpatients with frailty and with polypharmacy: the COFRAIL cluster randomized trial. JAMA Network Open. 2023;6(3):e234723. doi:10.1001/jamanetworkopen.2023.4723
79. Baumgartner AD, Clark CM, LaValley SA, Monte SV, Wahler RG, Singh R. Interventions to deprescribe potentially inappropriate medications in the elderly: lost in translation? J Clin Pharm Ther. 2020;45(3):453–461. doi:10.1111/jcpt.13103
80. Ailabouni NJ, Reeve E, Helfrich CD, Hilmer SN, Wagenaar BH. Leveraging implementation science to increase the translation of deprescribing evidence into practice. Res Social Adm Pharm. 2022;18(3):2550–2555. doi:10.1016/j.sapharm.2021.05.018
81. Wang Y, Wong EL, Nilsen P, Chung VC, Tian Y, Yeoh EK. A scoping review of implementation science theories, models, and frameworks - an appraisal of purpose, characteristics, usability, applicability, and testability. Implement Sci. 2023;18(1):43. doi:10.1186/s13012-023-01296-x
82. Alaa Eddine N, Schreiber J, El-Yazbi AF, Shmaytilli H, Amin MEK. A pharmacist-led medication review service with a deprescribing focus guided by implementation science. Front Pharmacol. 2023;14:1097238. doi:10.3389/fphar.2023.1097238
83. Öztürk O, Kocaman R, Kanbach DK. How to design bibliometric research: an overview and a framework proposal. Rev Manag Sci. 2024;18:3333–3361.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Are Saudi Arabian Patients Willing to Be Deprescribed Their Medications? An Exploratory Study
Alhurishi SA, AlQahtani MF
Patient Preference and Adherence 2024, 18:779-786
Published Date: 27 March 2024
Establishing Interprofessional Medication Reviews in Home Care Patients – A Feasibility Study
Meyer-Massetti C, Sommer A, Kaiser E, Peschak AM, Preisig M, Aubert CE, Mäder RD, Ramseier L, Riesen IS, Lettieri-Amstutz S, Rölli D, Schönenberger N, Meier CR
Drug, Healthcare and Patient Safety 2025, 17:209-220
Published Date: 8 October 2025
Prevalence of Multiple Chronic Conditions in Older Adults with Undiagnosed Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Primary Care
Summanwar D, Owora AH, Ben Miled Z, Dexter PR, Kulshreshtha A, Strunk S, Jiang B, Coppedge K, Disla S, Galvin JE, Boustani M, Fowler NR
Clinical Interventions in Aging 2025, 20:1799-1809
Published Date: 24 October 2025