Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Current Practices and Gaps in Management of Dyslipidemia in Type 2 Diabetes Mellitus (T2DM) in Accordance with American Diabetes Association (ADA) Guidelines: A Subset Analysis from a Real-World, Cross-Sectional Observational Study (LEADD Study)
Authors Das AK, Saboo B, Unnikrishnan AG
Received 2 December 2020
Accepted for publication 4 February 2021
Published 15 June 2021 Volume 2021:14 Pages 2693—2700
DOI https://doi.org/10.2147/DMSO.S294842
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Ashok Kumar Das,1 Banshi Saboo,2 Ambika G Unnikrishnan3
1Department of Endocrinology, Pondicherry Institute of Medical Sciences, Pondicherry, India; 2Department of Endocrinology, Dia Care, Ahmedabad, Gujarat, India; 3Department of Endocrinology, Chellaram Diabetes Institute, Pune, Maharashtra, India
Correspondence: Ambika G Unnikrishnan
Department of Endocrinology, Chellaram Diabetes Institute, Pune, 411021, Maharashtra, India
Tel +91 8605011934
Email [email protected]
Background: Diabetic dyslipidemia is a risk factor for coronary artery disease (CAD) in patients with type 2 diabetes mellitus (T2DM). American Diabetes Association (ADA) provides internationally accepted guidelines to manage dyslipidemia in T2DM.
Objective: To assess if ADA guidelines are followed for managing dyslipidemia in patients with T2DM in India.
Methods: This was a subset analysis of a prospective, cross sectional, observational study (LEADD Study) conducted at 199 sites across India to evaluate dyslipidemia management practices in T2DM patients (N=4002), in a real-world setting. The data was stratified based on age and atherosclerotic cardiovascular disease (ASCVD) and ASCVD risk factors to record the percentages of T2DM patients achieving LDL-C target and treated optimally with the Guideline directed intensity of statin. Analysis was conducted using descriptive statistics.
Results: As per ADA 2018 targets: LDL-C levels (< 100mg/dL) were seen in 30.6% of participants. High intensity statins were prescribed to 13.4% of the participants with LDL levels ≥ 100 mg/dL. ASCVD risk assessment details were available for 89.2% of participants. Data was not available for smoking and albuminuria. In participants < 40 years of age, 80% and 64.2% with ASCVD and ASCVD risk factors, respectively, did not achieve target LDL-C levels. In this age group, 15.6% and 83.3% of participants with ASCVD risk factors and ASCVD group, respectively, were not receiving statins in the recommended dose. In participants ≥ 40 years of age, 88.0% and 91.5% with ASCVD and ASCVD risk factors, respectively, did not have LDL-C levels as per ADA 2018 targets. In this age group, 87.2% and 77.9% of participants with ASCVD risk factors and ASCVD, respectively, were not receiving statins in the recommended dose.
Conclusion: The sub-analysis of LEADD study shows sub-optimal adherence to ADA 2018 guidelines for management of diabetic dyslipidemia.
Keywords: diabetic dyslipidemia, hyperlipidemia in diabetes, abnormal lipid profile in diabetes, dyslipidemia in diabetes, hypercholesteremia in diabetes
Introduction
T2DM is commonly associated with comorbid conditions such as dyslipidemia and hypertension, which are important risk factors for atherosclerotic cardiovascular disease (ASCVD). Additionally, diabetes itself is an independent risk factor for ASCVD. Aggressive risk factor modification strategies in the United States in patients with T2DM has significantly improved the 10-year coronary heart disease (CHD) risk along with a decrease in ASCVD morbidity and mortality.1–3
Low-density lipoprotein cholesterol (LDL-C) plays a significant role in the development of atherosclerosis and CHD.4,5 Literature shows multiple benefits of LDL-C reduction in patients with diabetes. Multiple clinical trials have demonstrated that statin therapy provides a significant benefit in primary and secondary prevention of ASCVD events and CHD death in patients with diabetes.6–8 A meta-analysis of 14 randomized trials of statin therapy (N=18, 00; mean follow-up 4.3 years) in patients with diabetes demonstrated that each mmol/L (39 mg/dL) reduction in LDL-C correlated with 9% and 13% reduction in all-cause mortality and vascular mortality, respectively.9
There have been conflicting reports that very low LDL-C levels increase the risk of T2DM.10–12 However, an analysis from the JUPITER trial showed that four to five ASCVD events were prevented for every incident case of diabetes caused by statin therapy.13 The analysis concluded that the cardiovascular and mortality benefits of statins outweighed the diabetes hazard.13 Therefore, the American Diabetes Association (ADA) 2018 guidelines on diabetic dyslipidemia management recommends statins as the drugs of choice for lowering LDL-C and providing cardioprotection.14 The ADA 2018 guidelines recommend that high intensity statin therapy (that lowers LDL-C levels by ≥50%) should be used in T2DM patients with dyslipidemia and ASCVD risk to lower the LDL-C levels to <70 mg/dL.14
Diabetic dyslipidemia is very common in India and most Indian studies report that dyslipidemia is poorly controlled in Indian patients with T2DM.15–17 The ADA 2018 dyslipidemia recommendations can prove to be an important resource for healthcare professionals for managing dyslipidemia in patients with T2DM.
Therefore, this multi-center cross-sectional observational study was conducted in India to evaluate if the real-world practices of managing dyslipidemia in patients with T2DM were in concurrence with ADA 2018 guidelines.
Methods
This is a sub-analysis of the Learnings with Experts to Advance Diabetic Dyslipidemia Management (LEADD) study, a real-world, cross-sectional observational study in patients with T2DM and dyslipidemia conducted over a period of 3 months at 199 centers across India. For patients fulfilling the inclusion criteria, and provided written informed consent, data was collected regarding demographics, co-morbidity, family history, laboratory, risk factors, concomitant medication history, and details of past and ongoing dyslipidemia treatment. The ASCVD risk assessment was done as per the American College of Cardiology’s risk calculator recommended in the ADA 2018 guidelines and the risk level was also documented.18 The 10-year ASCVD risk is stratified into low (<5%), borderline (5–7.5%), intermediate (7.5–20%), and high (≥20%).18,19 Lipid profile normal values and risk levels as per ADA 2018 dyslipidemia guidelines are mentioned in Table 1. Risk stratification as per age, ASCVD risk and recommended statin levels as per ADA 2018 dyslipidemia guidelines are mentioned in Table 2. The data was collected on a self-carbonated prescription writing pad through which data was integrated from across study centers.
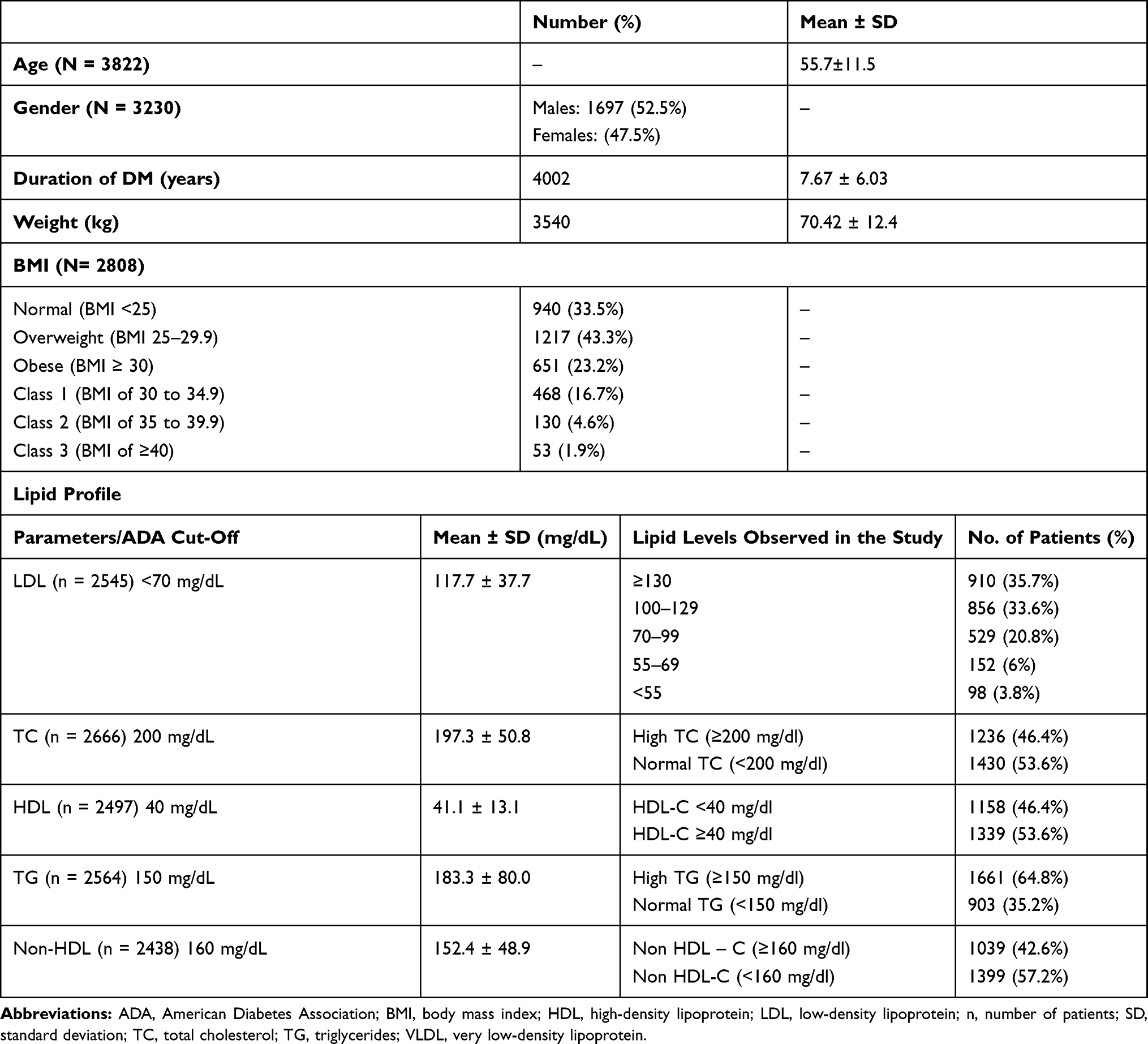 |
Table 1 Demographic and Lipid Profile of Study Population (N=4002) |
Ethical Approval
The study was approved by the Ethics Committee of the Chellaram Diabetes Institute, Pune, India. The study was conducted in compliance with the principles of the Declaration of Helsinki, and Indian regulatory guidelines, Indian Council of Medical Research (ICMR) and Indian Good Clinical Practice (GCP) guidelines). Ethical Committee approval was obtained.
Study Population
Inclusion Criteria
The study included patients of either sex who were ≥18 years of age and had a confirmed diagnosis of T2DM in alignment with ADA 2018 criteria.20
Dyslipidemia was diagnosed in the patients meeting the inclusion criteria in alignment with ADA 2018 targets.20 The body mass index (BMI) of the participants was noted. Patients with BMI of ≥23 kg/m2 were considered as overweight and those with ≥25 kg/m2 as obese as per the ADA, WHO and Indian consensus group BMI cut-off recommendation for Asians.21–24
Exclusion Criteria
Patients with known history of type 1 diabetes, malignancy, uncontrolled hypothyroidism, alcohol or drug abuse were excluded from the study. The following patients were also excluded: with current active liver disease or alanine transaminase (ALT)/aspartate transaminase (AST) levels > 3 times upper limit of normal (ULN); unexplained creatinine levels >3 times ULN; on hormone replacement therapy or oral contraceptives within 3 months of enrollment; undergone any cardiac intervention in last 3 months; pregnant or breast-feeding women and those who had participated in any other interventional study in last 3 months.
Endpoints of the Sub-Analysis
The primary endpoints were:
- Percentage of participants achieving dyslipidemia management goals as per ADA 2018 guidelines
- Percentage of participants on high intensity of statin as per the ADA 2018 guideline.
The secondary endpoints were:
- Percentage of participants evaluated for risk factors as per ADA 2018
- Treatment pattern of participants with diabetes with dyslipidemia in concurrence with ADA 2018 guidelines.
Statistical Analysis
Raw data was collected from all the 199 study centers and integrated on a cloud platform.
Descriptive statistics was used to summarize demographic, baseline characteristics and all other qualitative and discrete variables. Mean, median, range, standard deviation (SD), minimum and maximum data was tabulated for continuous variables and number of patients. Frequencies and percentages were used to compute the data for categorical measurements. Appropriate statistical analysis was conducted to assess the existence of statistically significant association between the variables, if any.
Results
Baseline Demographics
A total of 4002 patients of T2DM were enrolled across 199 centers in India. The mean age of the participants was 55.7 ± 11.5 years. Of these, 52.5% were males and 47.5% were females. Demographic details are provided in Table 1. Dyslipidemia was seen in 52.3% of study population (n =1399/2673).
Results of Sub-Analysis
As per the ADA criteria, the following major risk factors were identified: overweight or obesity 83.3%), LDL cholesterol ≥100 mg/dL (69.4%), family history of DM (50.2%), CKD (Stage 3–5 based on Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI]) (27.3%), hypertension (25.7%) and HDL-C levels <40 mg/dL (24%) (Table 2). Data was not available for smoking and albuminuria.
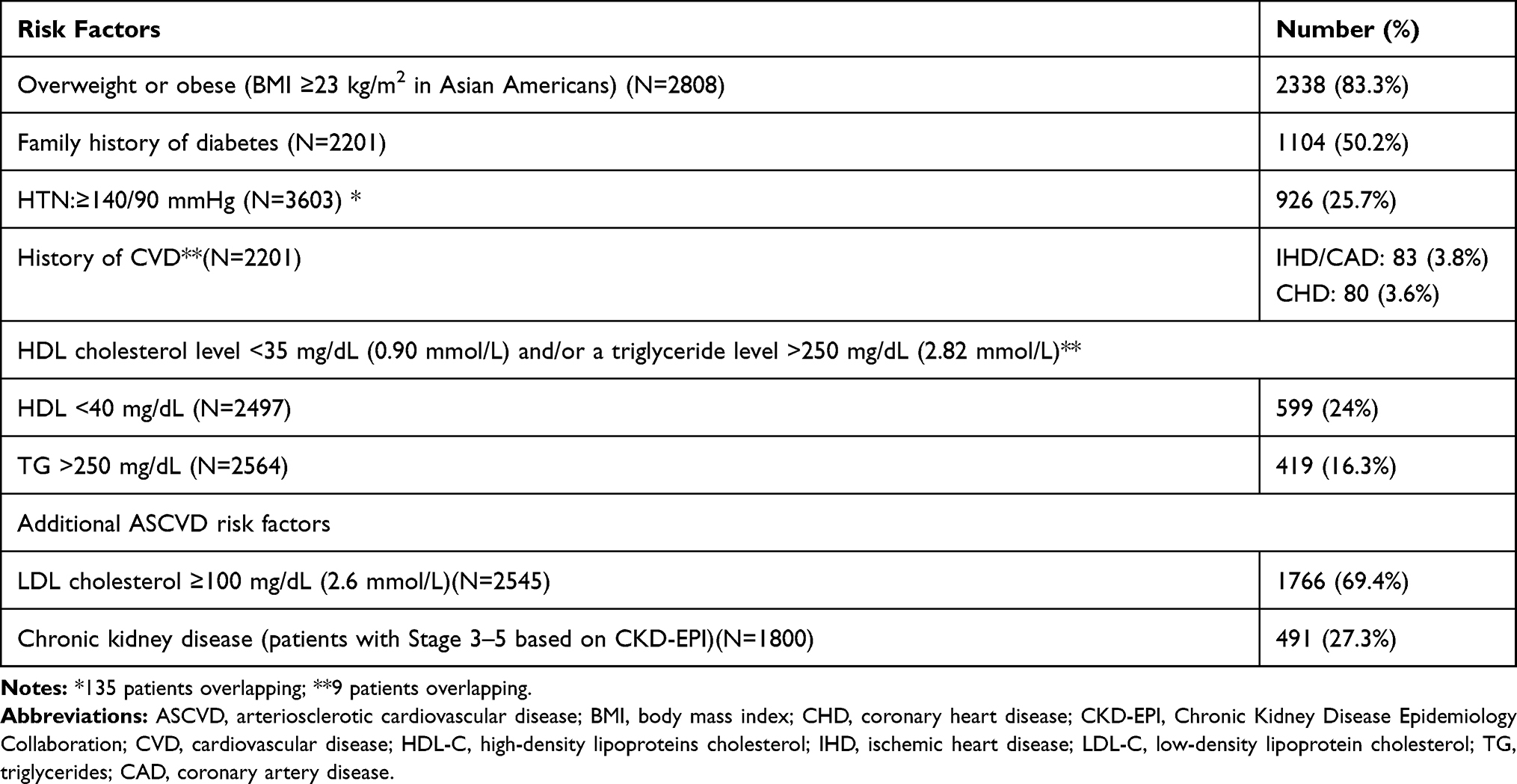 |
Table 2 ASCVD Risk Factors in Study Population (ADA Guidelines) |
Details of ASCVD risk assessment were available for 89.2% of participants. Of these, 99.5% had ASCVD or ASCVD risk factors. For patients of <40 years, ASCVD risk factors and ASCVD were present in 66.4% and 2.2% of participants, respectively. Mean LDL-C levels in patients with ASCVD risk factors was 129.2±38.0 mg/dl and in patients with ASCVD it was 121.3±42.2 mg/dl. For patients of ≥40years, ASCVD risk factors and ASCVD were present in 82.9% and 12.3% of participants, respectively. Mean LDL-C levels in patients with ASCVD risk factors was 121.0±36.7 mg/dl and in patients with ASCVD it was 118.4±41.4 mg/dL. See Table 3.
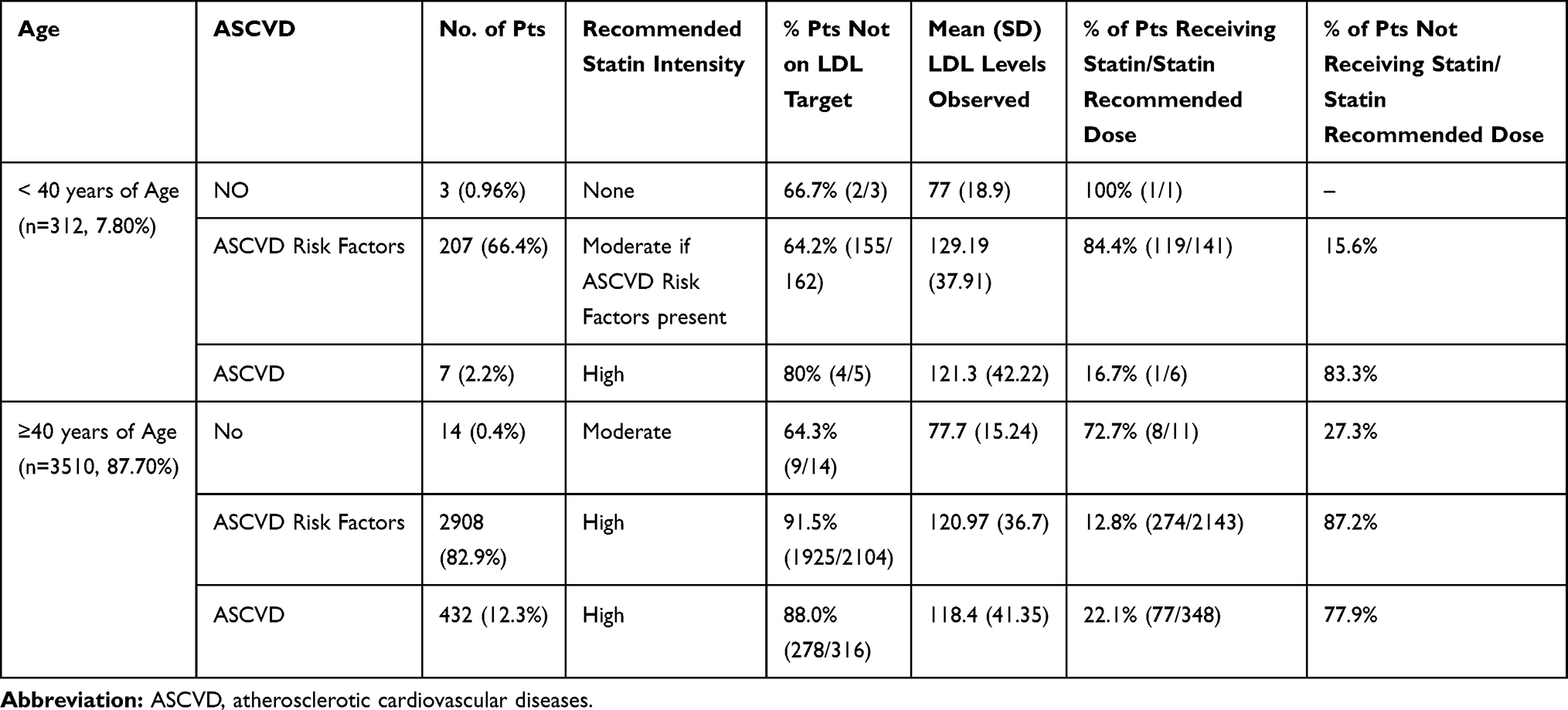 |
Table 3 Risk Stratification and Risk Based LDL Lowering Therapy Assessment in Study Population – Using ADA 2018 Recommendations |
Of the participants evaluated for anti-hyperlipidemic drugs; 77.2% received only statins; fenofibrate and ezetimibe were prescribed to 10.8% and 0.4% of participants, respectively.
Statins were prescribed to 68.1% of the study population. Lipid profile was not always evaluated before starting statins. Table 1 provides the number of participants for which lipid profile values were available. Six hundred and forty-five participants received atorvastatin, 2075 received rosuvastatin. The 10 mg dose was the most prescribed dose in 63.7% of participants on atorvastatin and 64.5% of participants on rosuvastatin.
Most commonly prescribed statins to the participants with raised total cholesterol or LDL cholesterol were rosuvastatin (n=2075/2757, 75.2%) followed by atorvastatin (n=645/2757, 23.4%).
As per ADA 2018 targets, LDL-C levels (<100mg/dL) were seen in 30.6% of participants, serum triglycerides (<150 mg/dl) in 35.2%, HDL-C (≥40mg/dL) in 53.6% and non-HDL-C (<160mg/dL) in 57.2% of participants (Table 1).
In participants <40 years of age (n=312), 80% and 64.2% with ASCVD and ASCVD risk factors, respectively, did not have LDL-C levels as per ADA 2018 targets. In this age group, recommended doses of statins were not received by 15.6% and 83.3% of participants with ASCVD risk factors and ASCVD group, respectively. In participants ≥40 years of age (n=3510), 88.0% and 91.5% with ASCVD and ASCVD risk factors, respectively, did not have LDL-C levels as per ADA 2018 targets. In this age group, recommended doses of statins were not received by 87.2% and 77.9% of participants with ASCVD risk factors and ASCVD, respectively. In participants ≥40 years of age with no ASCVD risk factors, 64.3% did not have LDL-C levels as per ADA 2018 targets and 72.7% were receiving statins in the recommended dose (Table 3).
Of the participants aged ≥40 years with ASCVD risk factors, recommended doses of high intensity statins were received by 12.8% and 22.1% of participants with mean LDL levels of 121.0 (SD 36.8) and 118.4 (SD 41.4), respectively (Table 2).
Discussion
This sub-analysis of LEADD Study, assessed whether ADA 2018 guidelines for management of T2DM with dyslipidemia were followed in current practices in India. An attempt was made to determine the gaps, so that these could be addressed while managing these patients.
The sub-analysis showed that majority of ADA 2018 goals and recommendations for the management of T2DM with dyslipidemia were not met in most of the participants in this real-world study. Majority of participants (87.7%) were ≥40 years old. ASCVD risk assessment was done for 89.2% of participants. However, all the risk factors (lipid levels, hypertension, BMI, kidney status, smoking, albuminuria, family history of premature ASCVD) were not assessed for all the participants due to lack of data. A significant number of participants did not meet the ADA 2018 targets for lipid profile and recommended statin therapy.
The ADA 2018 dyslipidemia management guidelines recommend use of high intensity statins (atorvastatin 40–80/rosuvastatin 20–40) in four patient scenarios: clinical ASCVD; very high-risk ASCVD (high LDL cholesterol and diabetes); severe primary hypercholesterolemia (total cholesterol ≥200 mg/dl); and diabetes-specific risk enhancers.14 High to moderate intensity statins (atorvastatin 10–20/rosuvastatin 5–10) can also be used as primary prevention therapy after assessing 10-year ASCVD risk level.14
In patients at very high-risk ASCVD, the ADA 2018 dyslipidemia guidelines recommend that LDL-C threshold of 70 mg/dL (1.8 mmol/L) should be used to guide addition of nonstatins to statin therapy. If LDL-C level remain ≥70 mg/dL, the guideline suggests adding ezetimibe to maximally tolerated statin therapy and if the LDL-C levels continue to remain ≥70 mg/dL, a PCSK9 inhibitor could be added even though its >three years safety and cost-effectiveness is uncertain. However, majority of participants in this study were on only one anti-hyperlipidemic agent, notably even in case of high the LDL-C levels. Ezetimibe was prescribed to only 0.4% of participants.
The ADA 2018 dyslipidemia guideline recommends that high-intensity statins (atorvastatin 40–80/rosuvastatin 20–40) or maximally tolerated statin dose should be used to reduce LDL-C in patients with clinical ASCVD. This sub-analysis of LEADD Study found that in participants with ASCVD, only 22.1% of participants aged ≥40 years and 16.7% of participants aged <40 years were receiving high intensity statins in the recommended dose. This means that more than two-thirds of participants with ASCVD were not receiving high intensity in the recommended dose. Most participants received 10 mg dose of either rosuvastatin or atorvastatin. Information regarding why the recommended dose was not used was not available.
Suboptimal lowering of high LDL increases the risk of ASCVD and stroke.25 Different doctors use different guidelines to manage statin treatment. However, there is no consensus amongst guidelines about patient population requiring high statin therapy, statin dose that can be considered high intensity and the percent lowering of LDL can be considered as an effective goal.26 This could be one of the reasons for suboptimal statin therapy and suboptimal LDL control seen in this sub-analysis when compared with ADA 2018 guidelines. Other reasons for sub-optimal LDL control could be statin intolerance, poor adherence, and poor LDL control despite optimal therapy.25,27–29
Even after guidelines are formulated and updated, their message does not get disseminated to the practicing physicians. A study found no significant differences in statin prescribing patterns after 2013 and 2014 ACC/AHA guidelines were released.30 In India as well, practicing physicians are often not aware of the information in the guidelines and end up prescribing sub-optimal statin dose.31 Additionally, Indians have different dyslipidemia pattern than Western population with not very high LDL but denser LDL particles, higher TG and lower HDL-C.32 Thus, the response and pharmacokinetics of dyslipidemia lowering drugs may not be as seen in Western population.32
The study also shows that there was sub-optimal adherence to the ADA 2018 dyslipidemia guidelines in majority of the study population. The study brings forward an important gap in management. Majority of patients requiring high intensity statins do not receive it. The reasons behind not prescribing high intensity statins to this patient group needs to be investigated in real-world studies.
Also, though use of statin is governed primarily by LDL-C levels, LDL values were available only for 63.6% of participants. Statins were also prescribed to participants with no documented LDL value. This gap in patient management needs to be addressed.
This real world observational study has several limitations inherent to the design like data missing for various variables and unequal follow-ups. In addition, data on smoking and microalbuminuria were not available. Also, though low-dose statin therapy is generally not recommended in T2DM, it is often the only statin dose that a patient can tolerate. The ADA 2018 guidelines suggest that maximum tolerated statin dose should be used in patients not tolerating the intended intensity of statin. However, though 10 mg dose was found to be most commonly used dose, data on the reason for using this dose was not captured. Though we report that 83.3% of patients aged <40 years with ASCVD did not receive statin, the results must be interpreted with caution because of a low sample size.
Conclusions
The sub-analysis of LEADD study shows sub-optimal adherence to ADA 2018 guidelines for management of diabetic dyslipidemia. Though majority of patients were ≥ 40 years of age and had ASCVD or ASCVD risk factors, they were not treated with high intensity statins, as recommended by ADA 2018 guidelines. This calls for more stringent treatment approach of treating diabetic dyslipidemia using high intensity statins to achieve desired outcomes in patients with ASCVD or ASCVD risk factors.
Ethics Statement
The study was approved by the Ethics Committee of the Chellaram Diabetes Institute, Pune, India.
Acknowledgments
The authors thank Dr. Kokil Mathur and Dr. Punit Srivastava of Mediception Science Pvt Ltd for providing medical writing support in the preparation of this manuscript, funded by Dr. Reddy’s Laboratories. We acknowledge assistance of Dr Shailesh R Deshpande of Chellaram Diabetes Institute for protocol development help. This study was funded by Diabetes Care India, via support from Dr Reddys Laboratories.
Disclosure
Dr Ambika G Unnikrishnan reports grants from Diabetes Care India and Dr Reddys Laboratories. Dr AK Das reports being a speaker for Dr Reddys Laboratories. Dr Banshi Saboo reports grants from Diabetes Care India and Dr Reddys Laboratories. The authors report no other potential conflicts of interest for this work.
References
1. Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. New Eng J Med. 2007;356(23):2388–2398. doi:10.1056/NEJMsa053935
2. Gregg EW, Li Y, Wang J, et al. Changes in diabetes-related complications in the United States, 1990–2010. New Eng J Med. 2014;370(16):1514–1523. doi:10.1056/NEJMoa1310799
3. Rawshani A, Rawshani A, Franzén S, et al. Mortality and cardiovascular disease in Type 1 and Type 2 diabetes. N Engl J Med. 2017;376(15):1407–1418. doi:10.1056/NEJMoa1608664
4. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
5. Wadhera RK, Steen DL, Khan I, Giugliano RP, Foody JM. A review of low-density lipoprotein cholesterol, treatment strategies, and its impact on cardiovascular disease morbidity and mortality. J Clin Lipidol. 2016;10(3):472–489. doi:10.1016/j.jacl.2015.11.010
6. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364(9435):685–696. doi:10.1016/S0140-6736(04)16895-5
7. Knopp RH, d’Emden M, Smilde JG, Pocock SJ. Efficacy and safety of atorvastatin in the prevention of cardiovascular end points in subjects with type 2 diabetes: the Atorvastatin Study for prevention of coronary heart disease endpoints in non-insulin-dependent diabetes mellitus (ASPEN). Diabetes Care. 2006;29(7):1478–1485. doi:10.2337/dc05-2415
8. Sever PS, Poulter NR, Dahlöf B, et al. Reduction in cardiovascular events with atorvastatin in 2532 patients with type 2 diabetes: Anglo-Scandinavian Cardiac Outcomes Trial–lipid-lowering arm (ASCOT-LLA). Diabetes Rev. 2005;28(5):1151–1157.
9. Collaborators CTT (CTT). Efficacy of cholesterol-lowering therapy in 18 686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet. 2008;371(9607):117–125. doi:10.1016/S0140-6736(08)60104-X.
10. Colhoun HM, Ginsberg HN, Robinson JG, et al. No effect of PCSK9 inhibitor alirocumab on the incidence of diabetes in a pooled analysis from 10 ODYSSEY Phase 3 studies. Eur Heart J. 2016;37(39):2981–2989. doi:10.1093/eurheartj/ehw292
11. Ference BA, Robinson JG, Brook RD, et al. Variation in PCSK9 and HMGCR and risk of cardiovascular disease and diabetes. N Eng J Med. 2016;375(22):2144–53. doi:10.1056/NEJMoa1604304
12. Sabatine MS, Wiviott SD, Im K, Murphy SA, Giugliano RP. Efficacy and safety of further lowering of low-density lipoprotein cholesterol in patients starting with very low levels: a meta-analysis. JAMA Cardiol. 2018;3(9):823–828. doi:10.1001/jamacardio.2018.2258
13. Ridker PM, Pradhan A, MacFadyen JG, Libby P, Glynn RJ. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: an analysis from the JUPITER trial. Lancet. 2012;380(9841):565–571. doi:10.1016/S0140-6736(12)61190-8
14. American Diabetes Association. 9. cardiovascular disease and risk management: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl1):S86–S104. doi:10.2337/dc18-S009.
15. Mithal A, Majhi D, Shunmugavelu M, Talwarkar PG, Vasnawala H, Raza AS. Prevalence of dyslipidemia in adult Indian diabetic patients: a cross sectional study (SOLID). Indian J Endocrinol Metab. 2014;18(5):642–647. doi:10.4103/2230-8210.139220
16. Parikh RM, Joshi SR, Menon PS, Shah NS. Prevalence and pattern of diabetic dyslipidemia in Indian type 2 diabetic patients. Diabetes Metab Syndr. 2010;4(1):10–12. doi:10.1016/j.dsx.2009.04.005
17. Kumar SP, Sandhya A. A study on the glycemic, lipid and blood pressure control among the type 2 diabetes patients of north Kerala, India. Indian Heart J. 2018;70(4):482–485. doi:10.1016/j.ihj.2017.10.007
18. American College of Cardiology. ASCVD risk estimator plus; 2020. Available from: http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/.
19. American College of Cardiology. New aspects of the risk assessment guidelines: practical highlights, scientific evidence and future goals. American College of Cardiology; 2018. Available from: http%3a%2f%2fwww.acc.org%2flatest-in-cardiology%2farticles%2f2018%2f11%2f14%2f07%2f10%2fnew-aspects-of-the-risk-assessment-guidelines.
20. American Diabetes Association. Standards of medical care in diabetes—2018 Abridged for primary care providers. Clin Diabetes. 2018;36(1):14–37. doi:10.2337/cd17-0119.
21. Misra A. Ethnic-specific criteria for classification of body mass index: a perspective for Asian Indians and American diabetes association position statement. Diabetes Technol Ther. 2015;17(9):667–671. doi:10.1089/dia.2015.0007
22. Misra A, Chowbey P, Makkar BM, et al. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009;57:163–170.
23. Hsu WC, Araneta MRG, Kanaya AM, Chiang JL, Fujimoto W. BMI cut points to identify at-risk Asian Americans for Type 2 diabetes screening. Diabetes Care. 2015;38(1):150–158. doi:10.2337/dc14-2391
24. Verma M, Rajput M, Kishore K, Kathirvel S. Asian BMI criteria are better than WHO criteria in predicting Hypertension: a cross-sectional study from rural India. J Family Med Prim Care. 2019;8(6):2095. doi:10.4103/jfmpc.jfmpc_257_19
25. Akyea RK, Kai J, Qureshi N, Iyen B, Weng SF. Sub-optimal cholesterol response to initiation of statins and future risk of cardiovascular disease. Heart. 2019;105(13):975–981. doi:10.1136/heartjnl-2018-314253
26. Bittencourt MS, Cesena FHY. Statin dose in primary prevention: aim for the target! Heart. 2019;105(13):969–971. doi:10.1136/heartjnl-2019-314723
27. Toth PP, Granowitz C, Hull M, Anderson A, Philip S. Long-term statin persistence is poor among high-risk patients with dyslipidemia: a real-world administrative claims analysis. Lipids Health Dis. 2019;18(1):175. doi:10.1186/s12944-019-1099-z
28. Toth PP, Patti AM, Giglio RV, et al. Management of statin intolerance in 2018: still more questions than answers. Am J Cardiovasc Drugs. 2018;18(3):157–173. doi:10.1007/s40256-017-0259-7
29. Karlson BW, Wiklund O, Palmer MK, Nicholls SJ, Lundman P, Barter PJ. Variability of low-density lipoprotein cholesterol response with different doses of atorvastatin, rosuvastatin, and simvastatin: results from VOYAGER. Eur Heart J Cardiovasc Pharmacother. 2016;2(4):212–217. doi:10.1093/ehjcvp/pvw006
30. Kelly KE, Jiroutek MR, Lewis K, Zagar B. Assessing changes in statin prescribing patterns surrounding the 2013 American College of Cardiology/American Heart Association Lipid Guidelines. Clin Ther. 2019;41(2):314–321. doi:10.1016/j.clinthera.2018.12.017
31. Enas AE, Dharmarajan TS The lipid association of India expert consensus statement 2016: a sea change for management of dyslipidemia in Indians; 2016. Available from: https://www.jcpconline.org/article.asp?issn=2250-3528;year=2016;volume=5;issue=2;spage=62;epage=66;aulast=Enas.
32. Sarat Chandra K, Bansal M, Nair T, et al. Consensus statement on management of dyslipidemia in Indian subjects. Indian Heart J. 2014;66(Suppl 3):S1–S51. doi:10.1016/j.ihj.2014.12.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.