Back to Journals » International Journal of Nanomedicine » Volume 21
Current Perspectives on Radiosensitizers in Cancer Radiotherapy
Received 10 February 2026
Accepted for publication 6 May 2026
Published 21 May 2026 Volume 2026:21 602677
DOI https://doi.org/10.2147/IJN.S602677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Dong Wang
Hanguang Ruan,1– 3 Yang Li,4 Songlin Chen5
1Department of Radiation Oncology, Jiangxi Cancer Hospital & Institute, Nanchang City, Jiangxi Province, People’s Republic of China; 2Department of Radiation Oncology, Jiangxi Cancer Center, Nanchang City, Jiangxi Province, People’s Republic of China; 3Department of Radiation Oncology, The Second Affiliated Hospital of Nanchang Medical College, Nanchang City, Jiangxi Province, People’s Republic of China; 4Department of Radiation Oncology, Harbin Medical University Cancer Hospital, Harbin City, Heilongjiang Province, People’s Republic of China; 5Department of Radiation Oncology, Nanchang People’s Hospital, Nanchang City, Jiangxi Province, People’s Republic of China
Correspondence: Songlin Chen, Email [email protected]
Objective: This review analyzes the multifactorial mechanisms of tumor radioresistance and evaluates the current landscape of innovative strategies to overcome this limitation, thereby improving the efficacy of radiotherapy.
Methods: We evaluated the key molecular and cellular drivers contributing to radioresistance. A comprehensive evaluation of contemporary radiosensitization strategies was then undertaken, with particular focus on nanomaterials (the predominant class discussed) while also covering nanomaterials, natural bioactive compounds, targeted molecular inhibitors, immunomodulators, and nucleic acid therapies. Each class of agents was subjected to a critical analysis spanning from mechanistic insights and supportive preclinical data to progress in clinical translation. Findings from foundational in vitro research, in vivo models, and preliminary clinical studies were consolidated to form a cohesive perspective.
Results: Tumor radioresistance is mediated by dynamic interactions between intrinsic cellular properties and the tumor microenvironment. Recent strategies have demonstrated potential through physical dose enhancement, multi‑target modulation, precise interference with DNA damage repair and cell‑cycle regulation, and combinatorial immunoradiotherapy. These approaches collectively enable selective tumor radiosensitization while modulating key resistance pathways.
Conclusion: Despite considerable preclinical promise, clinical adoption faces challenges including biological heterogeneity, suboptimal agent delivery, normal tissue toxicity, and a lack of validated predictive biomarkers. Future advances will rely on the development of intelligent multifunctional platforms, biomarker‑guided patient stratification, and rationally designed combination therapies to achieve durable therapeutic gains.
Keywords: radiotherapy, radioresistance, radiosensitivity, strategy, radiosensitizers
Introduction
Radiotherapy (RT) remains a cornerstone of modern oncology, utilized in over half of all cancer cases across curative, adjuvant, and palliative settings.1 Its efficacy relies on ionizing radiation to induce lethal DNA damage, predominantly DNA double-strand breaks (DSBs), in tumor cells.2 Despite technological advancements that have improved precision, the clinical success of RT is frequently compromised by the development of tumor radioresistance, leading to locoregional recurrence and poor outcomes in numerous solid malignancies. This resistance is not a singular defect but a dynamic, multifactorial phenotype arising from complex interactions between tumor cell–intrinsic adaptations and extrinsic influences from the tumor microenvironment (TME).3 Key intrinsic mechanisms include enhanced DNA damage repair, activation of pro-survival signaling pathways, dysregulated cell-cycle checkpoints, and the properties of cancer stem cells.4–6 Concurrently, the hypoxic, acidic, and immunosuppressive TME further attenuates radiation response.7–9 Overcoming these barriers is therefore critical to improving the therapeutic ratio of RT. This has spurred the development of diverse radiosensitizers designed to exploit these biological vulnerabilities. Moving beyond conventional chemotherapy, contemporary strategies encompass nanomaterials, natural products, molecularly targeted inhibitors, immunomodulators, and nucleic acid–based therapies.10,11 Different classes of radiosensitizers differ considerably in their routes of administration. Nanomaterial-based agents, such as gold nanoparticles, AGuIX, and NBTXR3, are typically delivered via intravenous or intratumoral injection. Notably, NBTXR3 is administered intratumorally to circumvent the poor biodistribution associated with intravenous delivery. Natural products, including curcumin and resveratrol, can be administered orally; however, their low bioavailability often necessitates intravenous or intraperitoneal administration in preclinical studies. DNA damage repair inhibitors are primarily given orally, whereas immune checkpoint inhibitors and growth factor inhibitors are usually infused intravenously. Nucleic acid therapeutics face substantial delivery challenges and predominantly rely on nanocarriers for intravenous or local administration. Although intravenous injection remains the most common systemic route, its efficiency in delivering radiosensitizers to the tumor microenvironment is exceedingly low. It has been well documented that over 80–90% of intravenously administered nanoparticles are sequestered by the reticuloendothelial system in the liver and spleen. As a result, the fraction that reaches the tumor microenvironment is typically less than 10%, and in many cases may fall below 1–5%. Even when tumor accumulation occurs via the enhanced permeability and retention effect, the agents are largely confined to perivascular regions at the tumor periphery, with poor penetration into hypoxic cores. Furthermore, the enhanced permeability and retention effect is highly variable across patients, tumor types, and even within the same tumor over time, rendering the delivered dose unpredictable on an individual basis. This low delivery efficiency not only compromises therapeutic efficacy but also heightens the risk of radiation‑induced injury to normal tissues due to off‑target accumulation in healthy organs. These issues represent major barriers to the clinical translation of radiosensitizers. Accordingly, optimizing administration routes and improving tumor‑targeted delivery efficiency are urgent priorities in the development of next‑generation radiosensitizers.
This review aims to summarize the current understanding of the molecular foundations of radioresistance and provide a comprehensive evaluation of these emerging radiosensitization strategies, discussing their mechanisms, preclinical evidence, translational progress, and future directions for clinical implementation.
The Mechanisms of Tumor Radioresistance
RT is a central component of cancer treatment by delivering ionizing radiation (IR), including X-rays, γ-rays, protons, and carbon ions.12 Despite continuous technological advances, such as intensity-modulated radiotherapy (IMRT), image-guided radiotherapy (IGRT), and stereotactic body radiotherapy (SBRT), which have substantially improved dose conformity and normal-tissue sparing, treatment resistance remains a major obstacle to durable local control.13,14 Radioresistance continues to contribute to locoregional recurrence and poor outcomes in multiple solid malignancies, including glioblastoma (GBM), pancreatic ductal adenocarcinoma (PDAC), non-small cell lung cancer (NSCLC), and head and neck squamous cell carcinoma (HNSCC), and so on.
Radioresistance represents a dynamic and multifactorial process resulting from the interplay between tumor cell–intrinsic mechanisms and the TME.15–17 At the cellular level, intrinsic resistance is driven by several well-characterized pathways. Enhanced DNA damage response (DDR) enables tumor cells to efficiently repair IR-induced DSBs through upregulation of non-homologous end joining (NHEJ) and homologous recombination (HR), mediated by key regulators such as DNA-dependent protein kinase catalytic subunit (DNA-PKcs), ataxia telangiectasia mutated (ATM), ataxia telangiectasia and Rad3-related (ATR), and poly (ADP-ribose) polymerase (PARP). In parallel, activation of pro-survival signaling pathways, including epidermal growth factor receptor (EGFR) and downstream PI3K/AKT/mTOR and NF-κB cascades, promotes proliferation, suppresses apoptosis, and facilitates post-irradiation recovery.18–22 Cell-cycle checkpoint dysregulation further permits cell cycle progression despite unresolved DNA damage. In contrast, cancer stem cells (CSCs) exhibit intrinsic radioresistance through quiescence, enhanced DNA repair capacity, and robust detoxification mechanisms.23–25 Additionally, augmented antioxidant defenses, particularly elevated intracellular glutathione (GSH) levels, limit radiation-induced cytotoxicity by scavenging reactive oxygen species (ROS).26–28
The TME largely governs extrinsic determinants of radioresistance. Tumor hypoxia, arising from aberrant vascular architecture, reduces oxygen availability, thereby diminishing the oxygen fixation effect essential for maximal radiation-induced DNA damage.21,29,30 Hypoxia-induced stabilization of hypoxia-inducible factor-1α (HIF-1α) further promotes angiogenesis, metabolic adaptation, and tumor invasiveness.7,8,31,32 Acidic extracellular pH and elevated interstitial fluid pressure impede drug delivery and compromise therapeutic penetration, while simultaneously fostering an immunosuppressive microenvironment. Moreover, the accumulation of immunosuppressive cell populations, including regulatory T cells (Tregs), tumor-associated macrophages (TAMs), and myeloid-derived suppressor cells (MDSCs), attenuates antitumor immune responses that could otherwise synergize with RT-induced immunogenic cell death.33–35
Radiosensitizers are developed to exploit these biological vulnerabilities and improve the therapeutic ratio of RT. An ideal radiosensitizer should demonstrate preferential tumor selectivity, potent enhancement of radiation response at clinically achievable doses, compatibility with standard fractionation schedules, and an acceptable toxicity profile. While conventional chemoradiosensitizers such as cisplatin and 5-fluorouracil have demonstrated clinical benefit, their lack of specificity often limits therapeutic gain.36–39 Recent advances in molecular targeting, immunomodulation, and nanotechnology have expanded the landscape of radiosensitizers, offering new opportunities for precision radiotherapy.40
Nanomaterial-Based Radiosensitizers
Physical and Chemical Mechanisms of Nanoradiosensitization
The interaction between high-atomic-number (high-Z) nanoparticles (NPs) and IR results in multiple mechanisms that enhance local radiation effects.41,42 Figure 1 shows the details of the relationship between nanomaterial-mediated radiosensitization and irradiation. Related to multiple mechanisms, one is the Physical dose enhancement. High-Z elements such as gold (Au, Z = 79), hafnium (Hf, Z = 72), gadolinium (Gd, Z = 64), and bismuth (Bi, Z = 83) exhibit a substantially higher probability of interacting with kilovoltage X-rays through the photoelectric effect compared with soft tissues, which are primarily composed of low-Z elements (H, C, N, and O). These interactions generate secondary photoelectrons and Auger electrons with very short path lengths (nanometer to micrometer range), leading to highly localized energy deposition and clustered DNA damage in the immediate vicinity of the nanoparticles.43,44 Monte Carlo simulations have played a critical role in quantifying the resulting dose enhancement factor (DEF) and elucidating its dependence on particle composition, size, and radiation energy.45
 |
Figure 1 The Relationship Between Nanomaterial-Mediated Radiosensitization And Irradiation. Abbreviations: GSH, Glutathione; ROS, Reactive Oxygen Species. |
The second one is catalytic generation of ROS (nanozyme activity). Beyond physical interactions, many nanomaterials exhibit intrinsic or surface-engineered enzyme-mimicking properties. For example, MnO2, CeO2, and certain metal sulfides can function as catalase mimics, decomposing hydrogen peroxide (H2O2) into molecular oxygen to alleviate hypoxia, or as peroxidase mimics that catalyze Fenton or Fenton-like reactions, involving Fe or Cu ions, generating highly cytotoxic hydroxyl radicals (•OH).46,47 This chemically mediated radiosensitization directly amplifies the indirect effects of radiation and is particularly relevant in hypoxic or redox-adapted tumors.
The last is the TME modulation. Nanoparticles can also be rationally designed to disrupt protective features of the TME.48 Representative strategies include depleting overexpressed glutathione (GSH) to impair redox homeostasis and in situ oxygen generation or release to reverse tumor hypoxia and restore radiation sensitivity.49–51
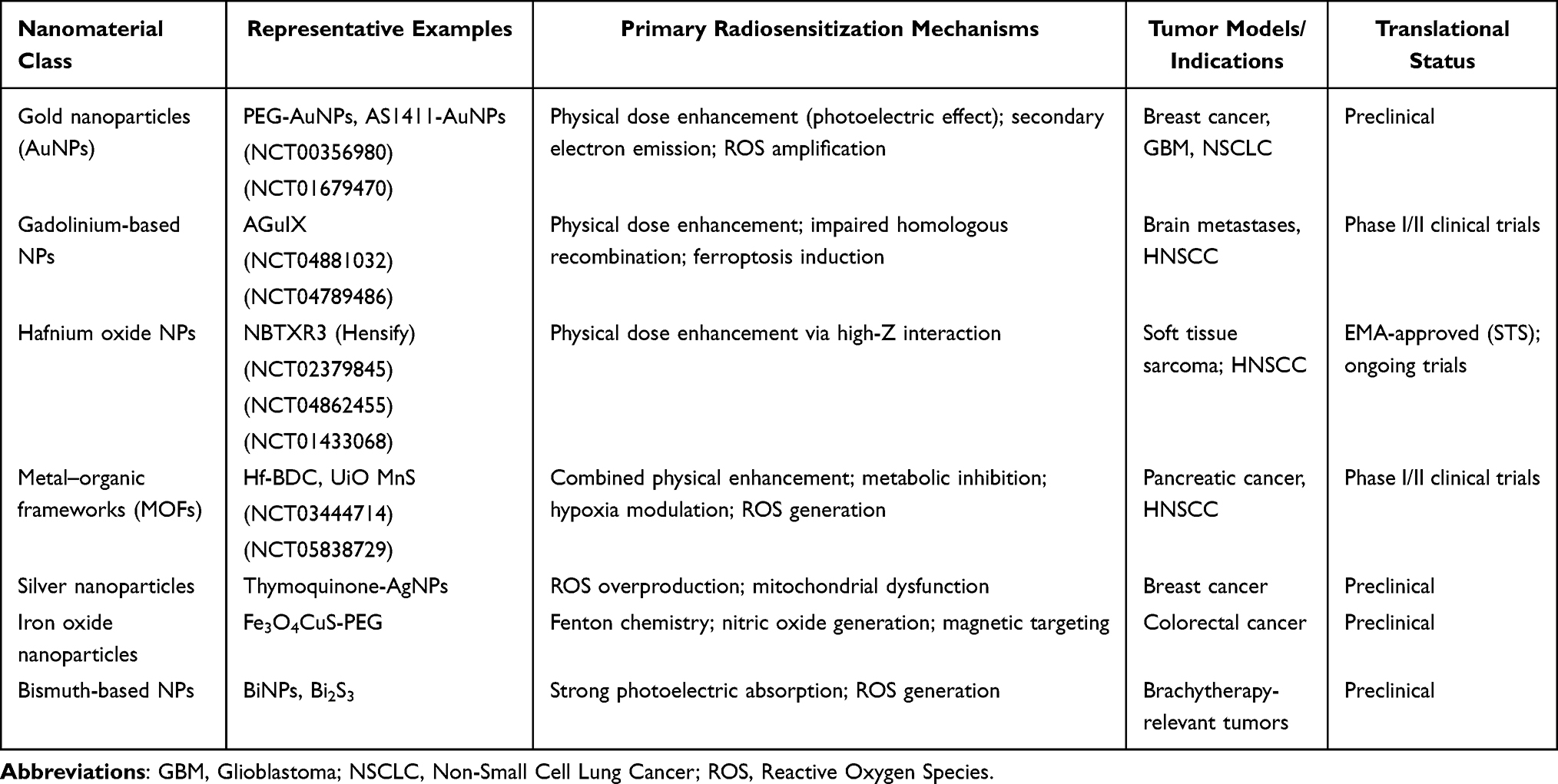 |
Table 1 Representative Nanomaterial-Based Radiosensitizers: Mechanisms and Translational Status |
A comprehensive overview of representative nanomaterial-based radiosensitizers is presented in Table 1, detailing their diverse mechanisms and translational progress. These materials, including gold, gadolinium, hafnium oxide, and metal-organic frameworks, primarily function by physical dose enhancement through their high atomic numbers, which increase radiation absorption. Additional mechanisms include secondary electron emission, amplification of ROS, and disruption of cellular repair processes, such as homologous recombination. The table illustrates a clear translational pathway, with several agents advancing from preclinical studies to clinical trials. Notably, hafnium oxide nanoparticles (NBTXR3) have achieved EMA approval for soft tissue sarcoma, marking a significant milestone in nanomaterial-driven radiation oncology. These innovations are being evaluated across various tumor models, including breast cancer, glioblastoma, and head and neck squamous cell carcinoma, underscoring their broad potential in enhancing radiotherapy efficacy.
Gold Nanoparticles: Prototype and Evolution
Gold nanoparticles (AuNPs) remain the most extensively investigated nanoradiosensitizers owing to their favorable biocompatibility, ease of surface functionalization, and strong photoelectric absorption.
Parameters Influencing Radiosensitization
Radiosensitizing efficacy depends on multiple physicochemical and treatment-related parameters, including particle size (often optimal in the 10–50 nm range for cellular uptake and retention), morphology (with nanorods and nanostars sometimes outperforming spherical particles), surface charge and coating (eg., polyethylene glycol for prolonged circulation), nanoparticle concentration, and radiation energy52,53. Notably, dose enhancement is more pronounced at kilovoltage energies than at megavoltage energies, reflecting the Z3 dependence of the photoelectric effect. Morozov et al demonstrated size- and dose-rate–dependent radiosensitization of DNA, reporting a sensitizer enhancement ratio (SER) of 2.74 for 26-nm AuNPs at 200 kVp.54
Functionalization and Active Targeting
To overcome the variability of the enhanced permeability and retention (EPR) effect in human tumors, active targeting strategies have been developed. Conjugation of AuNPs with the nucleolin-targeting aptamer AS1411 significantly increased cellular uptake and radiosensitization in breast cancer models.55 Similar approaches using RGD peptides targeting αvβ3 integrin or folic acid targeting the folate receptor have also shown promising preclinical results.56
Combination Modalities
AuNPs are well-suited for multimodal therapy. Their strong absorption of near-infrared light enables photothermal therapy, which can act as a radiosensitizer by improving tumor perfusion and oxygenation and by inhibiting DNA repair pathways.57,58 Sears et al demonstrated selective cytotoxicity in triple-negative breast cancer using triangular silver nanoparticles for combined photothermal therapy and radiosensitization, underscoring the potential of metallic nanostructures in combination strategies.59
Gadolinium- and Hafnium-Based Nanoplatforms
AGuIX Nanoparticles
AGuIX nanoparticles are sub-5-nm polysiloxane-based gadolinium chelates and are among the few nanoradiosensitizers to have advanced into clinical trials. These particles demonstrate efficient tumor accumulation, rapid renal clearance, and radiosensitization through multiple mechanisms. Preclinical studies indicate that AGuIX nanoparticles induce autophagy, impair homologous recombination repair, and promote ferroptosis by inhibiting the NRF2–GPX4 axis.60 Simonet et al reported their efficacy in overcoming radioresistance in head and neck squamous cell carcinoma models.61
Hafnium-Based Nanomaterials
A Phase 2–3 trial assessed the safety and efficacy of radiotherapy-activated hafnium oxide (HfO2) nanoparticles, known as NBTXR3, compared with radiotherapy alone when used as a preoperative treatment for patients with locally advanced soft-tissue sarcoma. A total of 176 patients were analysed for the primary endpoint in the intention-to-treat full analysis set (87 in the NBTXR3 group and 89 in the radiotherapy alone group). The results showed that a pathological complete response was noted in 14 (16%) of 87 patients in the NBTXR3 group and seven (8%) of 89 in the radiotherapy alone group (p = 0. 044). Serious adverse events were observed in 35 (39%) of 89 patients in the NBTXR3 group and 27 (30%) of 90 patients in the radiotherapy alone group.62 It has received European approval for intratumoral administration in locally advanced soft tissue sarcoma, primarily exploiting physical dose enhancement. Beyond simple oxide particles, hafnium-based metal–organic frameworks (nMOFs) are emerging as versatile platforms for radiosensitization. Fu et al developed Hf-nMOFs loaded with the glycolysis inhibitor 3-bromopyruvate, achieving simultaneous enhancement of dose deposition and interference with metabolism-dependent DNA repair.63 Huang et al reported a UiO MnS core–shell nanostructure capable of TME-responsive hydrogen sulfide generation, relieving hypoxia and promoting ROS production to enhance immunogenic radiotherapy.47
Other Promising Nanomaterials
Silver nanoparticles, iron oxide nanoparticles, bismuth-based nanomaterials, and multi-component heterostructures have also demonstrated radiosensitizing potential through diverse mechanisms, including mitochondrial dysfunction, Fenton chemistry, and synergistic photothermal effects.64–67 While these platforms offer compelling preclinical efficacy, their clinical translation requires careful evaluation of long-term toxicity, biodistribution, and normal tissue effects.
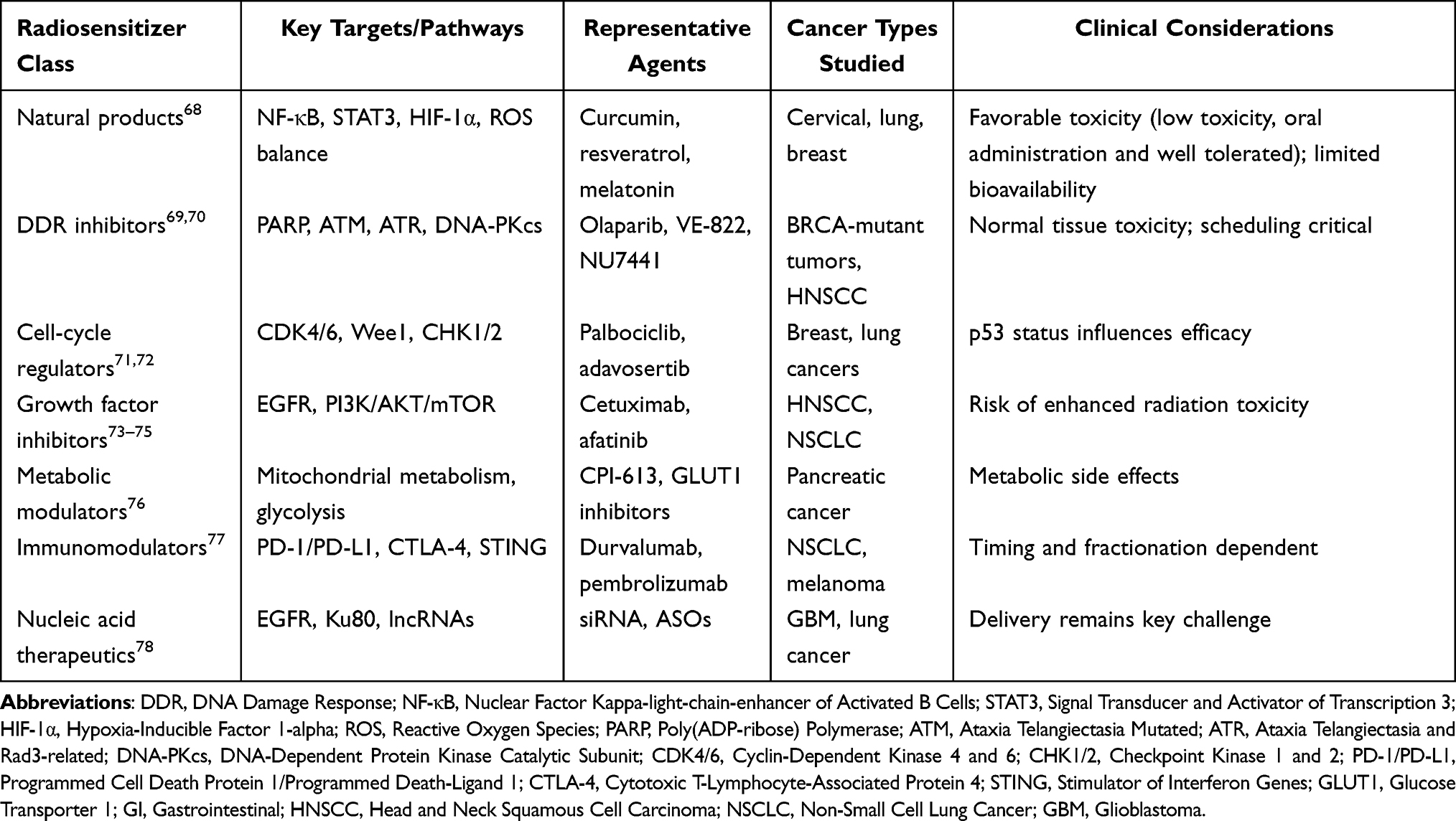 |
Table 2 Non-Nanoparticle Radiosensitizers Targeting Radioresistance Pathways |
Natural Products as Radiosensitizers
It is the non-nanoparticle radiosensitizers targeting specific radioresistance pathways in cancer that are detailed in Table 2. Unlike nanomaterials, these agents—including natural products, DDR inhibitors, cell-cycle regulators, and immunomodulators—act on biological mechanisms such as NF-κB signaling, PARP-mediated repair, and immune checkpoint pathways. While several, like PARP inhibitor olaparib and immune checkpoint blocker durvalumab, have entered clinical use, their translation is accompanied by significant considerations. Challenges include normal tissue toxicity, limited bioavailability (eg., with curcumin), and the critical importance of treatment scheduling and patient selection (eg., p53 status for cell-cycle drugs). The table also notes ongoing hurdles in delivering nucleic acid therapeutics, such as siRNA, effectively to tumors. These pathway-targeted agents represent a precision medicine approach to radiosensitization, aiming to overcome biological resistance while navigating complex clinical trade-offs between efficacy and safety.
Natural compounds derived from plants, fungi, and marine organisms represent a rich source of bioactive molecules with radiosensitizing potential. Their pleiotropic mechanisms, relatively favorable toxicity profiles, and historical use in oncology support continued investigation. However, it is important to explicitly state that for the vast majority of natural products discussed below, the evidence remains confined to in vitro or preclinical animal studies. Only a very limited number, such as curcumin, have been evaluated in small-scale clinical trials, and none have yet reached regulatory approval as radiosensitizers. The following descriptions of mechanistic and efficacy data should be interpreted with this evidence level in mind.
Polyphenols and Flavonoids
Those radiosensitizers amplify radiation-induced oxidative stress by generating a massive burst of ROS, overwhelming the cancer cell’s limited antioxidant defenses. This leads to sustained endoplasmic reticulum (ER) stress and mitochondrial membrane depolarization, triggering the intrinsic apoptotic pathway via caspase-9 and caspase-3. Additionally, they inhibit survival signaling pathways like NF-κB, PI3K/Akt, and STAT3, which normally help cells resist radiation-induced death.79 One randomized controlled trial in cervical cancer demonstrated that curcumin supplementation during RT significantly enhanced survivin suppression, correlating with improved treatment response.80 Nevertheless, this single trial does not provide conclusive evidence for clinical adoption; larger, multi-center studies are required to confirm efficacy and establish optimal dosing regimens. Resveratrol, quercetin, and genistein have similarly been shown to impair DNA repair and promote cell-cycle arrest or senescence, thereby enhancing radiosensitivity across multiple tumor models.81,82 It should be noted that for these latter compounds, all available data derive from in vitro or in vivo animal models, and no clinical trial data on their radiosensitizing effects are currently available.
Terpenoids and Saponins
This large class of compounds, including paclitaxel and ginsenosides, primarily sensitizes cells by disrupting the cell cycle and inhibiting DNA repair. They cause G2/M cell cycle arrest, forcing more cells into the most radiosensitive phase of the cycle. They also inhibit HR and NHEJ, the two major pathways for repairing lethal DNA double-strand breaks (DSBs), by downregulating key proteins like ATM, ATR, DNA-PKcs, and RAD51.79,83,84 This prevents cancer cells from fixing radiation-induced damage, leading to mitotic catastrophe and apoptosis. Ginsenosides, particularly ginsenoside Rg3, sensitize nasopharyngeal carcinoma cells by suppressing radiation-induced epithelial–mesenchymal transition and inhibiting nuclear translocation of EGFR.85 Paclitaxel, although widely used as a chemotherapeutic agent, also functions as a radiosensitizer by inducing G2/M arrest, the most radiosensitive phase of the cell cycle.86,87 Despite these promising mechanistic insights, the radiosensitizing effects of terpenoids and saponins, with the exception of paclitaxel, which is already established as a chemotherapeutic agent, have been demonstrated exclusively in preclinical models. No clinical trials have specifically evaluated their use as radiosensitizers, and caution is warranted when extrapolating the reported findings to human patients.
Alkaloids and Other Compounds
They inhibit checkpoint kinases like Chk1 and Chk2, effectively abrogating the G2/M checkpoint. This forces cells with unrepaired DNA damage to prematurely enter mitosis, resulting in mitotic catastrophe. They also directly inhibit the activity of topoisomerase I and II, creating persistent DNA breaks that compound with radiation damage. Furthermore, some alkaloids generate ROS and downregulate anti-apoptotic proteins like Bcl-2 and survivin, while upregulating pro-apoptotic Bax.25 Berberine, papaverine, and related alkaloids have demonstrated radiosensitizing effects through metabolic inhibition and interference with DNA repair pathways.88 Ononin, an isoflavone from Astragalus, has been identified as a novel radiosensitizer in lung cancer via inhibition of the HIF-1α/VEGF axis.89 All of the aforementioned findings for alkaloids and related compounds are derived from in vitro or limited in vivo studies. The level of evidence for this class remains preliminary, and no clinical data are available to support their use as radiosensitizers at this time.
Melatonin
Melatonin exhibits unique dual properties, enhancing tumor cell radiosensitivity while protecting normal tissues. It downregulates the expression of repair proteins BRCA1, RAD51, and DNA-PKcs, suppressing both HR and NHEJ. Mechanistically, it increases ROS generation in cancer cells, impairs DNA repair, modulates estrogen synthesis, and reduces radiation-induced toxicity in normal tissues, making it an attractive adjunct in radiotherapy.90,91 While melatonin has been investigated in a number of clinical studies as a radioprotective agent, its role as a tumor radiosensitizer remains less well established. Most of the radiosensitizing data come from preclinical models; well-controlled clinical trials specifically designed to assess radiosensitization are lacking. Therefore, the dual role of melatonin should be interpreted cautiously, and further clinical validation is required before it can be recommended as a radiosensitizer.
Discussion
Limitation and Toxicity
Nanomaterial-based radiosensitizers have demonstrated substantial potential to enhance the therapeutic ratio of radiotherapy through physical dose amplification, reactive oxygen species (ROS) overproduction, and disruption of DNA damage repair.92 However, despite promising preclinical results, their clinical translation remains limited. The major hurdles are threefold: (i) toxicity, including chronic organ retention and off-target sensitization; (ii) biodistribution, characterized by reticuloendothelial system (RES) sequestration and poor tumor penetration; and (iii) clinical feasibility, encompassing manufacturing reproducibility, route of administration, and regulatory complexity.
The goal of radiosensitization is to amplify radiation effects exclusively within the tumor. However, when nanoparticles accumulate in healthy organs—particularly the liver, spleen, and kidneys—they sensitize these tissues to ionizing radiation, leading to unintended fibrosis, necrosis, or organ dysfunction. For example, gold nanoparticles (GNPs) with prolonged circulation can induce oxidative stress and chronic inflammation in RES-rich organs.45,52 Many metallic nanoparticles, such as Au, Gd, and Hf, are not readily biodegradable. They can persist in the RES for months to years, causing chronic inflammation, granuloma formation, or late-onset genotoxicity.93 For biodegradable nanoparticles, dissolution and release of metal ions can disrupt cellular homeostasis, inhibit enzymatic activity, or induce ferroptosis in healthy tissues.94,95 Furthermore, nanoparticle surfaces can activate the complement system and trigger cytokine storms, leading to vascular leakage and acute phase reactions.
Intravenously administered nanoparticles are predominantly captured by Kupffer cells and macrophages in the liver and spleen (often > 80–90% of the injected dose).96 Real-time imaging studies have demonstrated that nanoparticles appear in the liver and spleen within 30 seconds of injection and remain there for days, drastically reducing tumor delivery and creating radiosensitive “hotspots” in clearance organs.97,98 Heterogeneous tumor accumulation and poor penetration are other aspects of biodistribution. Even when nanoparticles reach the tumor via the enhanced permeability and retention (EPR) effect, they tend to accumulate at the tumor periphery near blood vessels. They fail to penetrate deeply into avascular, hypoxic regions—the most radioresistant compartments of the tumor. The EPR effect itself is highly variable across patients, tumor types, and even within the same tumor over time, making it impossible to predict the delivered dose of the radiosensitizer in an individual patient.99,100
Nanomaterial radiosensitizers have achieved some outcomes in preclinical experiments, but there are still many clinical challenges from Bench to Bedside. For example, nanoparticle suspensions are prone to aggregation during terminal sterilization. Lyophilization may extend shelf life, but reconstitution often induces aggregation. These stability issues directly impact clinical safety and efficacy. On the other hand, the route of administration dilemmas is also an important factor that makes clinical transformation challenging. Although intratumoral injection bypasses the issue of biological distribution, it is not suitable for deep, metastatic, or sporadic tumors.101 In addition, image guidance is required for each radiotherapy session. Meanwhile, intravenous preparations will lead to poor tumor delivery and higher RES uptake. However, local or inhalation administration of nanomaterials is limited to specific cancers such as bladder cancer and lung cancer. The most advanced clinical candidate, NBTXR3 (Nanobiotix), illustrates these translational challenges. It is administered via intratumoral injection to circumvent issues with intravenous biodistribution.
Nanomaterial Radiosensitization Across Different Radiation Energies and Modalities
The foregoing discussion of nanomaterial‑based radiosensitizers, particularly those utilizing high‑Z) elements, predominantly relies on studies employing kilovoltage (kV) and megavoltage (MV) X‑rays. It is important to clarify that the radiosensitization effects described—such as physical dose enhancement via the photoelectric effect—are highly energy‑dependent. As noted in the present review, dose enhancement is substantially more pronounced at kV energies than at MV energies due to the Z3 dependence of the photoelectric effect. However, the consistency of these effects across other radiation modalities, including γ‑rays, protons, and carbon ions, remains insufficiently characterized. Protons and carbon ions deposit energy primarily through ionizing and excitational interactions along the Bragg peak, and the contribution of high‑Z nanomaterials to additional dose deposition via secondary electron emission is less established and likely differs from that seen with photon irradiation. Furthermore, the radiosensitizing mechanisms mediated by catalytic reactive oxygen species generation or DNA repair interference may be influenced by radiation quality. Therefore, the conclusions drawn in this review regarding the efficacy of nanomaterial radiosensitizers should not be directly extrapolated to all radiation energies or all particle‑beam modalities without further experimental validation. Future investigations are warranted to systematically evaluate nanomaterial radiosensitization under clinically relevant proton, carbon‑ion, and emerging FLASH radiotherapy conditions, and to define the optimal energy windows and material designs for each modality.
Future Direction
The success of nanoparticles such as hafnium oxide (NBTXR3) has validated the potential of nanomaterial-based radiosensitizers, but future designs will likely move beyond passive energy deposition. Smart or stimuli-responsive nanosystems, such as pH-sensitive or enzyme-activated particles that release radiosensitizing payloads only within the tumor microenvironment, are under active development. Theranostic nanoparticles that combine real-time imaging, radiosensitization, and treatment monitoring may eventually enable personalized dose painting and adaptive radiotherapy.
Hypoxia remains a major obstacle to effective radiotherapy. Next-generation radiosensitizers are being designed not only as oxygen mimetics such as nimorazole derivatives, but also as agents that actively remodel the tumor microenvironment.100 Examples include inhibitors of HIF-1α and metal-organic frameworks or gold-based nanoclusters that generate reactive oxygen species independent of oxygen levels.102
The convergence of radiotherapy and immunotherapy has opened new opportunities for radiosensitizers. Agents that enhance DNA damage while triggering immunogenic cell death (ICD) can convert the irradiated tumor into an in-situ vaccine.15 Combining such radiosensitizers with immune checkpoint inhibitors, STING agonists, or TLR agonists may amplify abscopal effects, leading to regression of distant metastases.103
Instead of broadly increasing radiation sensitivity, future radiosensitizers are expected to target DDR pathways specifically. Inhibitors of PARP, ATM, ATR, and DNA-PKcs are already in clinical trials.21 Pairing these molecular radiosensitizers with advanced radiation techniques such as FLASH or proton therapy could achieve synergistic tumor control while minimizing normal tissue toxicity.104 Predictive biomarkers, including DDR gene mutations, will be essential for patient selection, moving radiosensitization into the realm of precision medicine.
The emergence of FLASH radiotherapy creates both opportunities and challenges for radiosensitizers. While FLASH spares normal tissue (the FLASH effect), not all tumors respond equally. Radiosensitizers that preferentially accumulate in tumors and enhance sensitivity under FLASH conditions, without compromising the protective effect on healthy tissue, represent a high-priority research area. High-atomic-number materials with short-lived excitation states, such as gold or bismuth nanoparticles with tailored surface chemistry, are among the candidates.
Future directions of radiosensitizers in cancer radiotherapy are moving away from one-size-fits-all radiosensitization toward intelligent, tumor-selective, and immune-activating systems. Advances in nanotechnology, molecular targeting, and immunomodulation, aligned with emerging radiotherapy modalities such as FLASH, may soon yield radiosensitizers that not only improve local tumor control but also convert localized therapy into systemic antitumor immunity. Moreover, future preclinical studies should explicitly model clinically relevant fractionation schedules rather than relying solely on single high-dose irradiation. Comparative testing of radiosensitizers across multiple fractionation regimens would reveal agent-specific dependencies. Similarly, orthotopic and genetically engineered mouse models that recapitulate the histopathology and microenvironment of human tumors are preferred over subcutaneous xenografts for evaluating tumor-type-specific barriers. For clinical trial design, adaptive or platform trial designs that allow simultaneous evaluation of multiple radiosensitizers or schedules within a single disease context should be considered. Regulatory science for radiosensitizers would also benefit from early engagement with health authorities to qualify surrogate endpoints and imaging biomarkers that can serve as early indicators of radiosensitization activity, thereby reducing the cost and duration of pivotal trials.
Conclusion
The development of radiosensitizers has evolved from cytotoxic agents toward mechanism-driven strategies, including nanomaterials, natural products, targeted inhibitors, and immunomodulators. However, as discussed in this review, each class exhibits inherent limitations and toxicity that hinder clinical translation. Nanomaterials offer physical dose enhancement but suffer from reticuloendothelial system sequestration, chronic organ retention, and off-target sensitization of healthy tissues. Natural products demonstrate pleiotropic effects and favorable safety profiles but are limited by poor bioavailability and inconsistent pharmacokinetics. Molecularly targeted inhibitors provide precision against specific resistance pathways yet carry risks of normal tissue toxicity and require biomarker-guided patient selection. Immunomodulators and nucleic acid therapeutics face delivery barriers, timing-dependent efficacy, and potential immune-related adverse events. Addressing these challenges—poor tumor delivery, unpredictable biodistribution, normal tissue toxicity, and lack of predictive biomarkers—will be critical for successful clinical translation. Future directions should prioritize: (i) smart stimuli-responsive nanosystems for tumor-selective activation; (ii) combination with immunotherapy to harness abscopal effects; (iii) integration with emerging modalities such as FLASH radiotherapy; and (iv) biomarker-driven patient stratification to enable precision radiosensitization. Interdisciplinary collaboration remains essential to translate these advances into improved therapeutic outcomes.
Abbreviation
RT, Radiotherapy; IMRT, Intensity-Modulated Radiotherapy; IGRT, Image-Guided Radiotherapy; SBRT, Stereotactic Body Radiotherapy; NHEJ, Non-Homologous End Joining; HR, Homologous Recombination; ATM, Ataxia Telangiectasia Mutated; ATR, Ataxia Telangiectasia and Rad3-Related; PARP, Poly (Adp-Ribose) Polymerase (Parp); EGFR, Epidermal Growth Factor Receptor; CSCs, Cancer Stem Cells; GSH, Glutathione; ROS, Reactive Oxygen Species; TAMs, Tumor-Associated Macrophages; MDSCs, Myeloid-Derived Suppressor Cells; HIF-1α, Hypoxia-Inducible Factor-1α; GBM, Glioblastoma; PDAC, Pancreatic Ductal Adenocarcinoma; NSCLC, Non-Small Cell Lung Cancer; HNSCC, Head and Neck Squamous Cell Carcinoma.
Data Sharing Statement
This review study has no raw data and has generated analysis data.
Ethics Approval and Consent to Participate
This study does not require ethics approval.
Author Contributions
Hanguang Ruan and Yang Li are co-first authors of the article. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflict of interest.
References
1. Hutchinson M-KND, Mierzwa M, D’Silva NJ. Radiation resistance in head and neck squamous cell carcinoma: dire need for an appropriate sensitizer. Oncogene. 2020;39(18):3638–14. doi:10.1038/s41388-020-1250-3
2. Ruan H, Okamoto M, Ohno T, Li Y, Zhou Y. Particle radiotherapy for breast cancer. Front Oncol. 2023;13:1107703. doi:10.3389/fonc.2023.1107703
3. Wu Y, Song Y, Wang R, Wang T. Molecular mechanisms of tumor resistance to radiotherapy. Mol Cancer. 2023;22(1):96. doi:10.1186/s12943-023-01801-2
4. Lee DY, Bermúdez-Cruz RM, Díaz-Chávez J. Editorial: the Role of DNA Repair Pathways in Resistance to Chemotherapy and Radiotherapy in Cancer. Front Oncol. 2022;12:894357. doi:10.3389/fonc.2022.894357
5. Patil T, Rohiwal SS, Tiwari AP. Stem Cells: therapeutic Implications in Chemotherapy and Radiotherapy Resistance in Cancer Therapy. Curr Stem Cell Res. Ther. 2023;18(6):750–765. doi:10.2174/1574888x17666221003125208
6. Wang C, Yuan M, Gao Y, Hou R, Song D, Feng Y. Changes in Tumor Immune Microenvironment after Radiotherapy Resistance in Colorectal Cancer: a Narrative Review. Oncol Res Treat. 2023;46(5):177–191. doi:10.1159/000530161
7. He D, Zhao Z, Fu B, et al. Exosomes Participate in the Radiotherapy Resistance of Cancers. Radiat Res. 2022;197(5):559–565. doi:10.1667/rade-21-00115.1
8. Hill RM, Rocha S, Parsons JL. Overcoming the Impact of Hypoxia in Driving Radiotherapy Resistance in Head and Neck Squamous Cell Carcinoma. Cancers. 2022;14(17):4130. doi:10.3390/cancers14174130
9. Peng J, Yin X, Yun W, Meng X, Huang Z. Radiotherapy-induced tumor physical microenvironment remodeling to overcome immunotherapy resistance. Cancer Lett. 2023;559:216108. doi:10.1016/j.canlet.2023.216108
10. An L, Li M, Jia Q. Mechanisms of radiotherapy resistance and radiosensitization strategies for esophageal squamous cell carcinoma. Mol Cancer. 2023;22(1):140. doi:10.1186/s12943-023-01839-2
11. Oršolić N, Jazvinšćak Jembrek M. Potential Strategies for Overcoming Drug Resistance Pathways Using Propolis and Its Polyphenolic/Flavonoid Compounds in Combination with Chemotherapy and Radiotherapy. Nutrients. 2024;16(21):3741. doi:10.3390/nu16213741
12. Abdel-Wahab M, Giammarile F, Carrara M, et al. Radiotherapy and theranostics: a Lancet Oncology Commission. Lancet Oncol. 2024;25(11):e545–e580. doi:10.1016/s1470-2045(24)00407-8
13. Chandra RA, Keane FK, Voncken FEM, Thomas Jr CR. Contemporary radiotherapy: present and future. Lancet. 2021;398(10295):171–184. doi:10.1016/s0140-6736(21)00233-6
14. Lei G, Mao C, Yan Y, Zhuang L, Gan B. Ferroptosis, radiotherapy, and combination therapeutic strategies. Protein Cell. 2021;12(11):836–857. doi:10.1007/s13238-021-00841-y
15. You R, Shen Q, Lin C, et al. Single-cell and spatial transcriptomics reveal mechanisms of radioresistance and immune escape in recurrent nasopharyngeal carcinoma. Nat Genet. 2025;57(8):1950–1965. doi:10.1038/s41588-025-02253-8
16. Shen R, Jiang Z, Wang H, Zheng Z, Jiang X. Molecular mechanisms of m6A modifications regulating tumor radioresistance. Mol Med. 2025;31(1):64. doi:10.1186/s10020-025-01121-9
17. Nguyen QK, Koo BS. Radioresistance Mechanisms in Head and Neck Cancer. Clin Exp Otorhinolaryngol. 2025;18(3):210–224. doi:10.21053/ceo.2025-00029
18. Morillo-Huesca M, I GL-C, Conesa-Bakkali R, et al. Radiotherapy resistance driven by Asparagine endopeptidase through ATR pathway modulation in breast cancer. J Exp Clin Cancer Res. 2025;44(1):74. doi:10.1186/s13046-025-03334-6
19. Liu L, Song L, Liu T, et al. Recombinant oncolytic virus NDV-anti-VEGFR2 enhances radiotherapy sensitivity in NSCLC by targeting VEGF signaling and impairing DNA repair. Gene Ther. 2025;32(5):517–528. doi:10.1038/s41434-025-00540-x
20. Li J, Feng L, Zhang L, et al. Saikosaponin D Mitigates Radioresistance in Triple-Negative Breast Cancer by Inducing MRE11 De-Lactylation via HIF1α/HDAC5 Pathway. Theranostics. 2025;15(17):8935–8951. doi:10.7150/thno.113517
21. Hofstad M, Woods A, Parra K, et al. Dual inhibition of ATR and DNA-PKcs radiosensitizes ATM-mutant prostate cancer. Oncogene. 2025;44(22):1746–1760. doi:10.1038/s41388-025-03343-x
22. Manunu B, Serafin AM, Akudugu JM. BAG1, MGMT, FOXO1, and DNAJA1 as potential drug targets for radiosensitizing cancer cell lines. Int J Radiat Biol. 2023;99(2):292–307. doi:10.1080/09553002.2022.2074164
23. Wu Q, Liu X, Wang LM, et al. Oleandrin enhances radiotherapy sensitivity in lung cancer by inhibiting the ATM/ATR-mediated DNA damage response. Phytother Res. 2024;38(8):4151–4167. doi:10.1002/ptr.8237
24. Chow Z, Johnson J, Chauhan A, et al. Inhibition of ribonucleotide reductase subunit M2 enhances the radiosensitivity of metastatic pancreatic neuroendocrine tumor. Cancer Lett. 2024;596:216993. doi:10.1016/j.canlet.2024.216993
25. Nathansen J, Meyer F, Müller L, Schmitz M, Borgmann K, Dubrovska A. Beyond the Double-Strand Breaks: the Role of DNA Repair Proteins in Cancer Stem-Cell Regulation. Cancers. 2021;13(19):4818. doi:10.3390/cancers13194818
26. Liu C, Kuang S, Wu L, et al. Radiotherapy and radio-sensitization in H3(K27M) -mutated diffuse midline gliomas. CNS Neurosci Ther. 2023;29(7):1721–1737. doi:10.1111/cns.14225
27. Qiu Y, Hu X, Zeng X, Wang H. Triple kill: DDR inhibitors, radiotherapy and immunotherapy leave cancer cells with no escape. Acta Biochim Biophys Sin. 2022;54(11):1569–1576. doi:10.3724/abbs.2022153
28. Lu Y, Zhang X. Radiochemotherapy-induced DNA repair promotes the biogenesis of gastric cancer stem cells. Stem Cell Res Ther. 2022;13(1):481. doi:10.1186/s13287-022-03165-8
29. Lip H, Zetrini A, Park E, et al. Mitigating radioresistance mechanisms by polymer-lipid manganese dioxide nanoparticles enhances immunogenic cell death and antitumor immune response to facilitate abscopal effect in breast tumor models. Drug Deliv Transl Res. 2026;16(1):180–194. doi:10.1007/s13346-025-01873-1
30. Qin L, Tang G, Gui R, et al. ATRX loss inhibits DDR to strengthen radio-sensitization in p53-deficent HCT116 cells. Sci Rep. 2025;15(1):793. doi:10.1038/s41598-024-85085-6
31. Grzmil M, Boersema P, Sharma A, et al. Comparative analysis of cancer cell responses to targeted radionuclide therapy (TRT) and external beam radiotherapy (EBRT). J Hematol Oncol. 2022;15(1):123. doi:10.1186/s13045-022-01343-y
32. Wang YH, Guo Z, An L, et al. LINC-PINT impedes DNA repair and enhances radiotherapeutic response by targeting DNA-PKcs in nasopharyngeal cancer. Cell Death Dis. 2021;12(5):454. doi:10.1038/s41419-021-03728-2
33. Hsieh K, Dickstein DR, Runnels J, et al. Radiotherapy and Immunotherapy in Lung Cancer. Biomedicines. 2023;11(6):1642. doi:10.3390/biomedicines11061642
34. Yu S, Wang Y, He P, et al. Effective Combinations of Immunotherapy and Radiotherapy for Cancer Treatment. Front Oncol. 2022;12:809304. doi:10.3389/fonc.2022.809304
35. Tang B, Zhu J, Shi Y, et al. Tumor cell-intrinsic MELK enhanced CCL2-dependent immunosuppression to exacerbate hepatocarcinogenesis and confer resistance of HCC to radiotherapy. Mol Cancer. 2024;23(1):137. doi:10.1186/s12943-024-02049-0
36. Zefrei FJ, Shormij M, Dastranj L, et al. Ferroptosis Inducers as Promising Radiosensitizer Agents in Cancer Radiotherapy. Curr Radiopharm. 2024;17(1):14–29. doi:10.2174/0118744710262369231110065230
37. Seo HK, Jung EH, Song G. Exploring radiotherapy combined with a radiosensitizer for Bacillus Calmette-Guérin-unresponsive non-muscle-invasive bladder cancer with carcinoma in situ. Transl Androl Urol. 2024;13(11):2354–2357. doi:10.21037/tau-24-480
38. Manabe Y, Takahashi Y, Sugie C, et al. Biological effects of prostaglandin E2-EP4 antagonist (AAT-008) in murine colon cancer in vivo: enhancement of immune response to radiotherapy and potential as a radiosensitizer. Transl Cancer Res. 2023;12(2):351–358. doi:10.21037/tcr-22-1857
39. Zhang S, Jiao X, Heger M, et al. A tumor microenvironment-responsive micelle co-delivered radiosensitizer Dbait and doxorubicin for the collaborative chemo-radiotherapy of glioblastoma. Drug Deliv. 2022;29(1):2658–2670. doi:10.1080/10717544.2022.2108937
40. Tudda A, Donzelli E, Nicolini G, et al. Breast radiotherapy with kilovoltage photons and gold nanoparticles as radiosensitizer: an in vitro study. Med Phys. 2022;49(1):568–578. doi:10.1002/mp.15348
41. Yan J, Wang G, Xie L, et al. Engineering Radiosensitizer-Based Metal-Phenolic Networks Potentiate STING Pathway Activation for Advanced Radiotherapy. Adv Mater. 2022;34(10):e2105783. doi:10.1002/adma.202105783
42. Li R, Zhao W, Wu T, et al. Tantalum-carbon-integrated nanozymes as a nano-radiosensitizer for radiotherapy enhancement. Front Bioeng Biotechnol. 2022;10:1042646. doi:10.3389/fbioe.2022.1042646
43. Clement S, Campbell JM, Deng W, et al. Mechanisms for Tuning Engineered Nanomaterials to Enhance Radiation Therapy of Cancer. Adv Sci. 2020;7(24):2003584. doi:10.1002/advs.202003584
44. Huang Q, Zhang S, Zhang H, et al. Boosting the Radiosensitizing and Photothermal Performance of Cu(2- x)Se Nanocrystals for Synergetic Radiophotothermal Therapy of Orthotopic Breast Cancer. ACS Nano. 2019;13(2):1342–1353. doi:10.1021/acsnano.8b06795
45. Kim H, Sung W, Ye SJ. Microdosimetric-Kinetic Model for Radio-enhancement of Gold Nanoparticles: comparison with LEM. Radiat Res. 2021;195(3):293–300. doi:10.1667/rade-20-00223.1
46. Pi F, Deng X, Xue Q, et al. Alleviating the hypoxic tumor microenvironment with MnO(2)-coated CeO(2) nanoplatform for magnetic resonance imaging guided radiotherapy. J Nanobiotechnology. 2023;21(1):90. doi:10.1186/s12951-023-01850-1
47. Huang N, Tang XY, Meng W, et al. Immunogenic Radiation Therapy for Enhanced Antitumor Immunity via a Core-Shell Nanosensitizer-Mediated Immunosuppressive Tumor Microenvironment Modulation. ACS Nano. 2023;17(20):19853–19864. doi:10.1021/acsnano.3c04189
48. Li D, Wang J, Li X, et al. Interactions between radiotherapy resistance mechanisms and the tumor microenvironment. Crit Rev Oncol Hematol. 2025;210:104705. doi:10.1016/j.critrevonc.2025.104705
49. Zhou J, Zhou Q, Mo Y, et al. A Novel Peculiarity of TXNIP Reversing the Radioresistance of NPC and Inducing Ferroptosis by xCT-GSH-GPX4-ROS Axis. Head Neck. 2026;48(1):134–147. doi:10.1002/hed.70004
50. Yang Z, Shao B, Wang D, et al. A TNBC-targeting nano-radiosensitizer reverses radioresistance by synergizing GSH scavenging with dual inhibition of Trop2 and lncRNA MNX1-AS1. Biomaterials. 2026;327:123787. doi:10.1016/j.biomaterials.2025.123787
51. Yuan Z, Liu T, Jiang P, et al. PEX5 deficiency enhances radiosensitivity via MGST1-GSH detoxifying function and promotes ferroptosis in liver cancer. Sci China Life Sci. 2025;68(10):2908–2922. doi:10.1007/s11427-024-2938-3
52. Loscertales E, López-Méndez R, Mateo J, et al. Impact of gold nanoparticle size and coating on radiosensitization and generation of reactive oxygen species in cancer therapy. Nanoscale Adv. 2025;7(4):1204–1214. doi:10.1039/d4na00773e
53. Xu J, Wang C, Zhang L, Zhao C, Zhao X, Wu J. In Situ Aggregated Nanomanganese Enhances Radiation-Induced Antitumor Immunity. ACS Appl Mater Interfaces. 2024;16(27):34450–34466. doi:10.1021/acsami.4c03838
54. Morozov KV, Kolyvanova MA, Kartseva ME, et al. Radiosensitization by Gold Nanoparticles: impact of the Size, Dose Rate, and Photon Energy. Nanomaterials. 2020;10(5):952. doi:10.3390/nano10050952
55. Mehrnia SS, Hashemi B, Mowla SJ, Nikkhah M, Arbabi A. Radiosensitization of breast cancer cells using AS1411 aptamer-conjugated gold nanoparticles. Radiat Oncol. 2021;16(1):33. doi:10.1186/s13014-021-01751-3
56. Wang Y, Han X, Zhang S, et al. Dual-Targeted Pt@Ce-MOF Nanoplatform Enhances Radiotherapy Efficacy via Tumor-Specific Delivery and Mitochondrial Dysfunction in Breast Cancer. Biopolymers. 2025;116(6):e70054. doi:10.1002/bip.70054
57. Li W, Ruan B, Chen X, Zhou F, Sun X, Lv Y. One step synthesis of ultrafine PHF@AuNPs nanocomposite and its application in NIR triggered photodynamic therapy. PLoS One. 2025;20(11):e0336714. doi:10.1371/journal.pone.0336714
58. Fernandez-Palomo C, Potez M, Haberthür D, et al. Synchrotron Microbeam Radiation Therapy in Combination With Gold Nanoparticles Improves Control of Mouse Melanoma. Int J Radiat Oncol Biol Phys. 2025;123(5):1383–1394. doi:10.1016/j.ijrobp.2025.07.1427
59. Sears J, Swanner J, Fahrenholtz CD, et al. Combined Photothermal and Ionizing Radiation Sensitization of Triple-Negative Breast Cancer Using Triangular Silver Nanoparticles. Int J Nanomed. 2021;16:851–865. doi:10.2147/ijn.S296513
60. Sun H, Cai H, Xu C, et al. AGuIX nanoparticles enhance ionizing radiation-induced ferroptosis on tumor cells by targeting the NRF2-GPX4 signaling pathway. J Nanobiotechnology. 2022;20(1):449. doi:10.1186/s12951-022-01654-9
61. Simonet S, Rodriguez-Lafrasse C, Beal D, et al. Gadolinium-Based Nanoparticles Can Overcome the Radioresistance of Head and Neck Squamous Cell Carcinoma Through the Induction of Autophagy. J Biomed Nanotechnol. 2020;16(1):111–124. doi:10.1166/jbn.2020.2871
62. Bonvalot S, Rutkowski PL, Thariat J, et al. NBTXR3, a first-in-class radioenhancer hafnium oxide nanoparticle, plus radiotherapy versus radiotherapy alone in patients with locally advanced soft-tissue sarcoma (Act.In.Sarc): a multicentre, phase 2–3, randomised, controlled trial. Lancet Oncol. 2019;20(8):1148–1159. doi:10.1016/s1470-2045(19)30326-2
63. Fu Z, Liu Z, Wang J, et al. Interfering biosynthesis by nanoscale metal-organic frameworks for enhanced radiation therapy. Biomaterials. 2023;295:122035. doi:10.1016/j.biomaterials.2023.122035
64. Montazersaheb S, Farahzadi R, Mansouri E, Jafari S, Fathi E. Radiosensitizing effects of silver nanoparticles targeting angiogenesis and matrix metalloproteinase signaling in triple negative breast cancer cell lines. Sci Rep. 2026. doi:10.1038/s41598-026-35662-8
65. Mahmoud TM, Abdelfatah MM, Omar MM, et al. Enhancing the Therapeutic Effect and Bioavailability of Irradiated Silver Nanoparticle-Capped Chitosan-Coated Rosuvastatin Calcium Nanovesicles for the Treatment of Liver Cancer. Pharmaceutics. 2025;17(1):72. doi:10.3390/pharmaceutics17010072
66. Yang R, You Z, Xie B, et al. Plasmon-boosted titanium nitride-based nanoplatform for synergistic photothermal-chemodynamic cancer therapy with smart degradability. Biomaterials. 2026;329:123950. doi:10.1016/j.biomaterials.2025.123950
67. Tarighatnia A, Amanzadeh M, Darvish L, Amraee A, Ghojazadeh M, Aghanejad A. Radiosensitivity enhancement of bismuth-based nanoparticles in radiotherapy: a systematic review and meta-analysis. Comput Biol Chem. 2026;120(Pt 1):108767. doi:10.1016/j.compbiolchem.2025.108767
68. Berkovitz S, Collaço N, Dolakova K, Hughes J. A Systematic Review of Turmeric/Curcumin for Prevention and Treatment of Oral Mucositis Due to Radiotherapy and/or Chemotherapy for Head and Neck Cancer. J Integr Complement Med. 2026;27683605261426992. doi:10.1177/27683605261426992
69. Loap P, Loirat D, Berger F, et al. Concurrent Olaparib and Radiotherapy in Patients With Triple-Negative Breast Cancer: the Phase 1 Olaparib and Radiation Therapy for Triple-Negative Breast Cancer Trial. JAMA Oncol. 2022;8(12):1802–1808. doi:10.1001/jamaoncol.2022.5074
70. Navran A, Al-Mamgani A, Elzinga H, et al. Phase I feasibility study of Olaparib in combination with loco-regional radiotherapy in head and neck squamous cell carcinoma. Clin Transl Radiat Oncol. 2024;44:100698. doi:10.1016/j.ctro.2023.100698
71. Jost T, Heinzerling L, Fietkau R, Hecht M, Distel LV. Palbociclib Induces Senescence in Melanoma and Breast Cancer Cells and Leads to Additive Growth Arrest in Combination With Irradiation. Front Oncol. 2021;11:740002. doi:10.3389/fonc.2021.740002
72. Sriramulu S, Thoidingjam S, Brown SL, Siddiqui F, Movsas B, Nyati S. Molecular targets that sensitize cancer to radiation killing: from the bench to the bedside. Biomed Pharmacother. 2023;158:114126. doi:10.1016/j.biopha.2022.114126
73. Su YC, Lee WC, Wang CC, Yeh SA, Chen WH, Chen PJ. Targeting PI3K/AKT/mTOR Signaling Pathway as a Radiosensitization in Head and Neck Squamous Cell Carcinomas. Int J Mol Sci. 2022;23(24):15749. doi:10.3390/ijms232415749
74. Deng H, Chen Y, Wang L, et al. PI3K/mTOR inhibitors promote G6PD autophagic degradation and exacerbate oxidative stress damage to radiosensitize small cell lung cancer. Cell Death Dis. 2023;14(10):652. doi:10.1038/s41419-023-06171-7
75. Kundu M, Dey A, Dasgupta S. Replication stress response and radioresistance in lung cancer: mechanistic insights and advanced therapeutic approaches. Curr Probl Cancer. 2025;56:101206. doi:10.1016/j.currproblcancer.2025.101206
76. Xia W, Need E, Schiavone C, et al. Image-guided targeting of mitochondrial metabolism sensitizes pediatric malignant rhabdoid tumors to low-dose radiotherapy. Sci Adv. 2025;11(21):eadv2930. doi:10.1126/sciadv.adv2930
77. Cabon J, Lerouge D, Thureau S, et al. Impact of KRAS G12C mutation on the efficacy of chemoradiotherapy in patients with unresectable stage II or III non-small cell lung cancer. Front Oncol. 2025;15:1675825. doi:10.3389/fonc.2025.1675825
78. Zhao X, Qiu Y, Chen J, et al. Non-Coding RNAs in Breast Cancer Radioresistance: mechanisms, Functional Roles and Translational Potentials. Cell Prolif. 2026;59(2):e70119. doi:10.1111/cpr.70119
79. Gong EY, Lee HW, Oh H, et al. Nitroxoline Enhances Radiosensitivity in Non-Small Cell Lung Cancer by Suppressing STAT3-AKT-MTOR Survival Signaling. Int J Mol Sci. 2026;27(5):2504. doi:10.3390/ijms27052504
80. Hidayat YM, Wagey F, Suardi D, Susanto H, Laihad BJ, Tobing MDL. Analysis of Curcumin as a Radiosensitizer in Cancer Therapy with Serum Survivin Examination: randomised Control Trial. Asian Pac J Cancer Prev. 2021;22(1):139–143. doi:10.31557/apjcp.2021.22.1.139
81. Gao M, Zhu K, Wang Z, et al. Engineering Hafnium Oxide-Based Nanoplatforms for Precision Radiosensitization. Adv Healthc Mater. 2026;2026:e05200. doi:10.1002/adhm.202505200
82. Cheng Y, Mou Y, Wang H, et al. Platinum-based functional nanomaterials: mechanisms and therapeutic strategies in cancer radiotherapy sensitization. Mol Cancer. 2026;25(1):18. doi:10.1186/s12943-025-02421-8
83. Kudo KI, Feng Q, Chosco MI, et al. Androgen receptor contributes to radioresistance through DNA repair and autophagy in AR-positive prostate cancer cells. bioRxiv. 2025;2025:690226. doi:10.64898/2025.12.03.690226
84. Zhao H, Gao S, Han Y, et al. Conversion of Ku80 K568 crotonylation to SUMOylation facilitates DNA non-homologous end joining and cancer radioresistance. Signal Transduct Target Ther. 2025;10(1):127. doi:10.1038/s41392-025-02210-1
85. Hu G, Luo N, Guo Q, et al. Ginsenoside Rg3 Sensitizes Nasopharyngeal Carcinoma Cells to Radiation by Suppressing Epithelial Mesenchymal Transition. Radiat Res. 2023;199(5):460–467. doi:10.1667/rade-22-00183.1
86. Reni M, Macchini M, Orsi G, et al. Preoperative mFOLFIRINOX versus PAXG for stage I-III resectable and borderline resectable pancreatic ductal adenocarcinoma (PACT-21 CASSANDRA): results of the first randomisation analysis of a randomised, open-label, 2 × 2 factorial Phase 3 trial. Lancet. 2026;406(10522):2945–2956. doi:10.1016/s0140-6736(25)01685-x
87. Langer CJ, Harris J, Horwitz EM, et al. Phase II Study of Low-Dose Paclitaxel and Cisplatin in Combination With Split-Course Concomitant Twice-Daily Reirradiation in Recurrent Squamous Cell Carcinoma of the Head and Neck: long-term Follow-up of NRG Oncology RTOG 9911. Int J Radiat Oncol Biol Phys. 2026;124(1):50–60. doi:10.1016/j.ijrobp.2025.07.1434
88. Komorowska D, Radzik T, Kalenik S, Rodacka A. Natural Radiosensitizers in Radiotherapy: cancer Treatment by Combining Ionizing Radiation with Resveratrol. Int J Mol Sci. 2022;23(18):10627. doi:10.3390/ijms231810627
89. Zhang YM, Miao ZM, Chen YP, et al. Ononin promotes radiosensitivity in lung cancer by inhibiting HIF-1α/VEGF pathway. Phytomedicine. 2024;125:155290. doi:10.1016/j.phymed.2023.155290
90. Simsek Z Ö, Aras S, Cikrikcioglu M, Baydili KN, Cortuk M. Melatonin as a radioprotective agent against flattening filter and flattening filter-free beam in radiotherapy-induced lung tissue damage. Int J Radiat Biol. 2025;101(1):28–34. doi:10.1080/09553002.2024.2381492
91. Basirat U, Bin Tariq U, Moeen N, et al. A Systematic Review of the Chemo/Radioprotective Effects of Melatonin against Ototoxic Adverse Effects Induced by Chemotherapy and Radiotherapy. Curr Pharm Des. 2023;29(15):1218–1229. doi:10.2174/1381612829666230503145707
92. Cihan YB. Nanoparticle-Based Radiosensitizers in Radiotherapy Applications. Cancer Biother Radiopharm. 2021;36(4):305–306. doi:10.1089/cbr.2020.4211
93. Hu B, Xiao X, Chen P, et al. Enhancing anti-tumor effect of ultrasensitive bimetallic RuCu nanoparticles as radiosensitizers with dual enzyme-like activities. Biomaterials. 2022;290:121811. doi:10.1016/j.biomaterials.2022.121811
94. Biagiotti G, Cazzoli R, Andreozzi P, et al. Biocompatible cellulose nanocrystal-based Trojan horse enables targeted delivery of nano-Au radiosensitizers to triple negative breast cancer cells. Nanoscale Horiz. 2024;9(7):1211–1218. doi:10.1039/d4nh00042k
95. Babu B, Stoltz SA, Mittal A, et al. Inorganic Nanoparticles as Radiosensitizers for Cancer Treatment. Nanomaterials. 2023;13(21):2873. doi:10.3390/nano13212873
96. Liu J, Zhao L, Sun Y, Fu Q, Xiao W. Hybrid biomaterials-based radiosensitizers: preparations and their applications in enhancing tumor radiotherapy. Mater Today Bio. 2025;34:102186. doi:10.1016/j.mtbio.2025.102186
97. Diz FM, Monteiro WF, Silveira IS, et al. Zinc-Modified Titanate Nanotubes as Radiosensitizers for Glioblastoma: enhancing Radiotherapy Efficacy and Monte Carlo Simulations. ACS Omega. 2024;9(27):29499–29515. doi:10.1021/acsomega.4c02125
98. Cao Y, Zheng M, Zhou Q, Dong Y, Hou Y, Ge Z. PolyMOF Radiosensitizers as Nanocarriers with X-Ray-Triggered Dual-Gas Release for Enhanced Radiotherapy. ACS Appl Mater Interfaces. 2025;17(31):44263–44274. doi:10.1021/acsami.5c11614
99. Nosrati H, Baghdadchi Y, Abbasi R, et al. Iron oxide and gold bimetallic radiosensitizers for synchronous tumor chemoradiation therapy in 4T1 breast cancer murine model. J Mater Chem B. 2021;9(22):4510–4522. doi:10.1039/d0tb02561e
100. Chen M-H, Yiu H-P, Wang Y-C, Liu T-Y, Li C. Multifunctional Nanoparticles as Radiosensitizers to Overcome Hypoxia-Associated Resistance in Cancer Radiotherapy. Nanomaterials. 2024;15(1):37. doi:10.3390/nano15010037
101. Xiang H, Li X, Wei H, et al. Biomimetic Engineering of Hybrid Radiosensitizers to Boost Radiotherapy against Cancer Metastasis. Adv Mater. 2025;37(34):e2501077. doi:10.1002/adma.202501077
102. Han Z, Wang Y, Zang X, Liu H, Su J, Zhou Y. FePt/MnO 2 @PEG Nanoparticles as Multifunctional Radiosensitizers for Enhancing Ferroptosis and Alleviating Hypoxia in Osteosarcoma Therapy. IEEE Transactions on NanoBioscience. 2025;24(2):180–190. doi:10.1109/tnb.2024.3475051
103. Wu J, Yuan J, Liu Z, et al. KAT2A-driven succinylation of SRSF11 enforces spliceosome-mediated RAD52 splicing to promote homologous recombination and radioresistance in hepatocellular carcinoma. Signal Transduct Target Ther. 2025;10(1):364. doi:10.1038/s41392-025-02458-7
104. Mendes E, Aprà P, Belchior A, et al. Green-synthesized gold-coated nanodiamonds as potential radiosensitizers for proton therapy. Nanoscale Horiz. 2026;11(3):883–898. doi:10.1039/d5nh00424a
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.