Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 16
Current Perspectives on Platelet-Rich Plasma Injections for Knee Osteoarthritis: How to Optimize Clinical Outcomes
Authors Dhillon J, Parry D ![]() , Kraeutler MJ
, Kraeutler MJ
Received 15 September 2025
Accepted for publication 21 November 2025
Published 16 December 2025 Volume 2025:16 Pages 179—186
DOI https://doi.org/10.2147/OAJSM.S567695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Andreas Imhoff
Jaydeep Dhillon,1 Dylan Parry,2 Matthew J Kraeutler3
1Department of Orthopedics, Samaritan Health Services, Corvallis, OR, USA; 2Texas Tech University Health Sciences Center School of Medicine, Lubbock, TX, USA; 3Department of Orthopaedic Surgery and Rehabilitation, Texas Tech University Health Sciences Center, Lubbock, TX, USA
Correspondence: Matthew J Kraeutler, Department of Orthopaedic Surgery and Rehabilitation, Texas Tech University Health Sciences Center, School of Medicine, 3601 4th St, Lubbock, TX, 79430, USA, Email [email protected]
Abstract: Knee osteoarthritis (OA) is a common degenerative joint disease affecting approximately 22% of adults over the age of 40 and is a major contributor to pain and disability worldwide. Platelet-rich plasma (PRP) has gained attention as a biologic treatment for this pathology due to its potential in modulating inflammation. This narrative review evaluates the current evidence on PRP for knee OA, comparing its efficacy to hyaluronic acid (HA), corticosteroids, and bone marrow aspirate concentrate (BMAC). High-quality studies consistently demonstrate that PRP provides superior pain relief and functional improvement compared to HA and corticosteroids and offers comparable results to BMAC. PRP is effective across all Kellgren-Lawrence grades, with the greatest benefits seen in early to moderate OA. Three-injection regimens appear more effective than single injections, and while both leukocyte-rich and leukocyte-poor formulations are used, no clear consensus exists on which is superior. Despite promising short- and mid-term outcomes, variability in preparation methods and limited long-term evidence remain important limitations. Current literature suggests that PRP may be a safe and potentially effective nonoperative option for managing knee osteoarthritis, though further high-quality, standardized studies are needed to confirm its long-term efficacy and optimal application.
Keywords: platelet-rich plasma, knee osteoarthritis, intra-articular injections, leukocyte-rich PRP, leukocyte-poor PRP, orthobiologics
Introduction
Osteoarthritis (OA) of the knee is the most common joint disorder in the United States and a major cause of chronic pain and disability worldwide.1 Characterized by progressive cartilage degeneration, synovial inflammation, and subchondral bone remodeling, knee OA impacts mobility and quality of life.2,3 Increasing evidence suggests that knee OA is a whole-joint disease involving not only articular cartilage but also the synovium, subchondral bone, menisci, ligaments, and infrapatellar fat pad.4 These tissues interact through inflammatory and biomechanical pathways and contribute to disease progression and symptom manifestation.5 While definitive treatment for end-stage OA often involves total knee arthroplasty, the focus of early and mid-stage management remains symptom control and preservation of joint function.6 Non-surgical treatment options include lifestyle modifications, physical therapy, oral nonsteroidal anti-inflammatory drugs (NSAIDs), and intra-articular injections. Among the injectable therapies, platelet-rich plasma (PRP) has gained increasing attention as a promising biologic option.7,8
PRP is an autologous blood product obtained by centrifugation, which results in a plasma fraction containing a higher concentration of platelets than baseline. Upon activation, platelets release numerous growth factors from their alpha granules, including transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), insulin-like growth factor-1 (IGF-1), and vascular endothelial growth factor (VEGF).9 These factors are involved in modulating inflammation, stimulating chondrocyte activity, and promoting extracellular matrix production.10,11 In contrast to corticosteroids or hyaluronic acid (HA), which primarily provide symptomatic relief, PRP is believed to exert disease-modifying effects through biologic pathways.12,13 However, it should be noted that HA also has demonstrated biologic activity, including modulation of cartilage matrix turnover and reduction of inflammatory mediators, rather than acting solely as a viscosupplement.13 The proposed advantages of PRP include the suppression of inflammatory cytokines implicated in the OA cascade. Additionally, because PRP is autologous, it minimizes the risk of immunologic reactions or transmission of infectious diseases.14 A recent systematic review of 27 Level I studies, published in 2023,10 demonstrated improved clinical outcomes in patients undergoing treatment for knee OA with PRP when compared to HA. Despite multiple Level I studies demonstrating its efficacy, PRP injections for knee OA are not currently covered by insurance, and patients are often required to pay out-of-pocket, typically ranging from $500 to $2000 per injection.10,15 Furthermore, there are currently no universally accepted guidelines on the optimal number of injections, frequency of treatment, or patient selection criteria for PRP injections in the treatment of knee OA. Recent systematic reviews and meta-analyses have attempted to clarify its role, but significant inconsistency remains among studies due to heterogeneity in PRP preparation methods, leukocyte content, dosing regimens, and outcome reporting, which contributes to ongoing debate regarding true clinical efficacy.16,17 This narrative review aims to evaluate and synthesize the current body of literature regarding PRP for knee osteoarthritis.
Methods
A literature search was conducted using PubMed, Embase, and Cochrane Library databases for studies published from inception to August 31, 2025. Search terms included “platelet-rich plasma,” “PRP,” “knee osteoarthritis,” and “intra-articular injection.” English-language clinical studies, systematic reviews, and meta-analyses evaluating PRP for the treatment of knee OA were included. Exclusion criteria comprised animal studies, non-knee OA applications, case reports, and studies lacking clinical outcome data. Reference lists of relevant reviews were also screened to identify additional articles.
PRP versus Other Injection Options
Given the increasing incidence of knee OA, intra-articular injectables such as PRP, hyaluronic acid (HA), corticosteroids, and bone marrow aspirate concentrate (BMAC) have become common non-surgical treatment options. However, there remains ambiguity regarding the most effective treatment, and clinical guidelines have yet to establish clear recommendations. The 2019 American College of Rheumatology (ACR) and Arthritis Foundation guidelines conditionally recommend against the use of PRP and HA due to heterogeneity in study quality and lack of standardized protocols, while supporting short-term corticosteroid injections for symptom relief.18 Similarly, the 2019 EULAR recommendations acknowledge the potential of PRP and other biologics but advise that evidence remains insufficient for formal recommendation.19 As the evidence base continues to expand, several high-level systematic reviews and meta-analyses have attempted to clarify the comparative efficacy of these modalities.
A systematic review of Level I randomized controlled trials published in 202120 compared outcomes between PRP and HA for the treatment of knee OA (Table 1). The analysis included 18 studies comprising 811 patients treated with PRP and 797 with HA, with an average follow-up of 11.1 months. PRP was associated with significantly superior improvements in several patient-reported outcomes (PROs), including the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analog scale (VAS) for pain, and Subjective International Knee Documentation Committee (IKDC) scores. Notably, 51.7% of outcome comparisons favored PRP over HA, and a higher proportion of PROs demonstrated significant pre- to post-treatment improvement in PRP recipients (81.0%) versus those who received HA (38.1%).
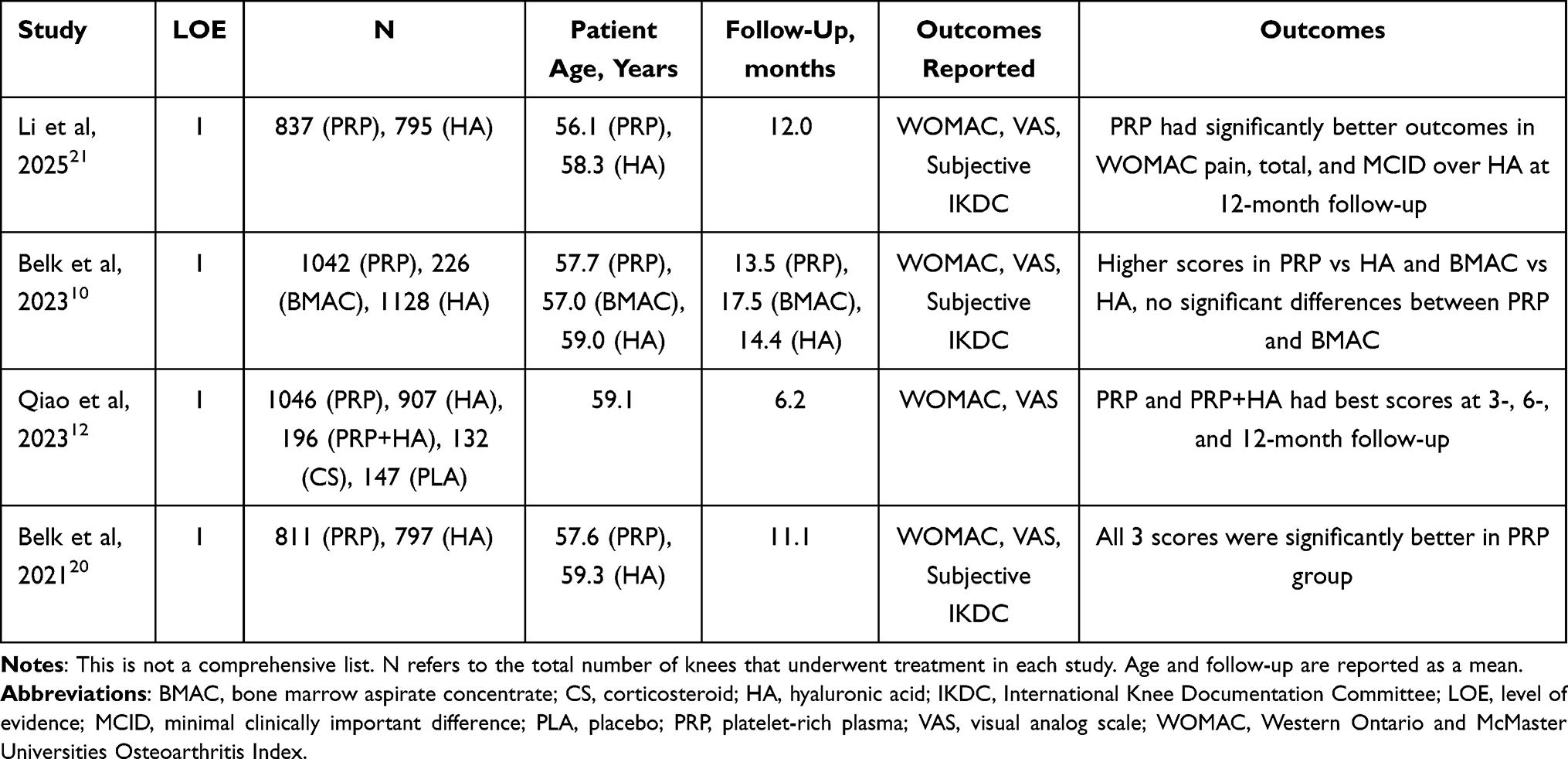 |
Table 1 Systematic Reviews of Randomized Controlled Trials That Compared PRP with Other Treatment Modalities for Knee Osteoarthritis |
An updated systematic review published in 202310 analyzed 27 Level I studies, encompassing 1042 patients treated with PRP, 226 with BMAC, and 1128 with HA. The authors found that both PRP and BMAC were significantly more effective than HA across multiple PROs including WOMAC, VAS, and Subjective IKDC scores. However, no statistically significant difference was observed between PRP and BMAC, suggesting that either biologic may offer comparable benefits in terms of symptomatic relief.
Another meta-analysis published in 2023 by Qiao et al12 evaluated 35 studies involving 3104 patients, comparing corticosteroids, HA, PRP, and PRP+HA combination therapy against placebo. At 3-month follow-up, PRP and PRP+HA yielded the most favorable WOMAC and VAS scores. While PRP+HA maintained superior VAS outcomes across all time points, by 12 months both PRP and PRP+HA demonstrated the most robust improvements in pain and function, reinforcing the potential of PRP as a stand-alone or adjunct treatment.
A 2025 meta-analysis by Li et al21 further validated PRP’s long-term efficacy. This study included 15 double-blind randomized controlled trials comprising 1632 patients with Kellgren-Lawrence grade I–III OA. At 12 months, patients undergoing treatment with PRP demonstrated significantly lower WOMAC pain scores and total scores compared to those receiving HA—both exceeding the minimal clinically important difference (MCID). Additionally, patients treated with PRP had significantly lower VAS pain scores at 12 months and improved Subjective IKDC scores at 1-month post-injection, suggesting a faster and more sustained therapeutic benefit.
Although most of the literature supports PRP as a more effective option for symptomatic relief in knee OA, several limitations persist. Many studies vary in PRP preparation and injection protocols, utilize heterogeneous outcome measures, and lack long-term follow-up data regarding structural progression or time to arthroplasty, which limits definitive conclusions regarding disease modification.
Leukocyte-Rich vs Leukocyte-Poor PRP
Leukocyte-rich PRP (LR-PRP) refers to platelet-rich plasma that contains a higher number of white blood cells, while leukocyte-poor PRP (LP-PRP) has most white blood cells removed, resulting in a preparation that is primarily platelets with minimal immune cells.22 Both LR-PRP and LP-PRP have been utilized for the treatment of knee OA, yet there is limited evidence clearly defining the ideal leukocyte concentration for this indication.23 LR-PRP contains a higher concentration of white blood cells, particularly neutrophils, which can release pro-inflammatory cytokines and growth factors such as IL-1β and TNF-α that may stimulate a more robust early healing response.22 However, LR-PRP may be detrimental because the elevated levels of pro-inflammatory cytokines and reactive oxygen species released by neutrophils can exacerbate inflammation, theoretically leading to increased pain, joint irritation, and potential degradation of cartilage in osteoarthritic joints.24 However, these theories have yet to bear out in clinical trials.18
A 2016 meta-analysis25 incorporating 6 randomized controlled trials and three prospective comparative studies (totaling 1055 patients) evaluated the clinical outcomes and adverse event rates associated with LP-PRP, LR-PRP, hyaluronic acid (HA), and placebo treatments for knee OA (Table 2). The analysis demonstrated that LP-PRP led to significantly better WOMAC scores when compared to HA or placebo, while LR-PRP did not show a significant difference. Across all groups, no significant differences in Subjective IKDC scores were observed. Although PRP treatments were associated with more adverse reactions than HA, leukocyte content did not appear to influence the rate of these effects. Adverse events, which were reported in 1.6% of patients, were generally mild and included swelling and pain; less commonly, symptoms such as syncope, dizziness, headache, gastritis, and tachycardia were reported.
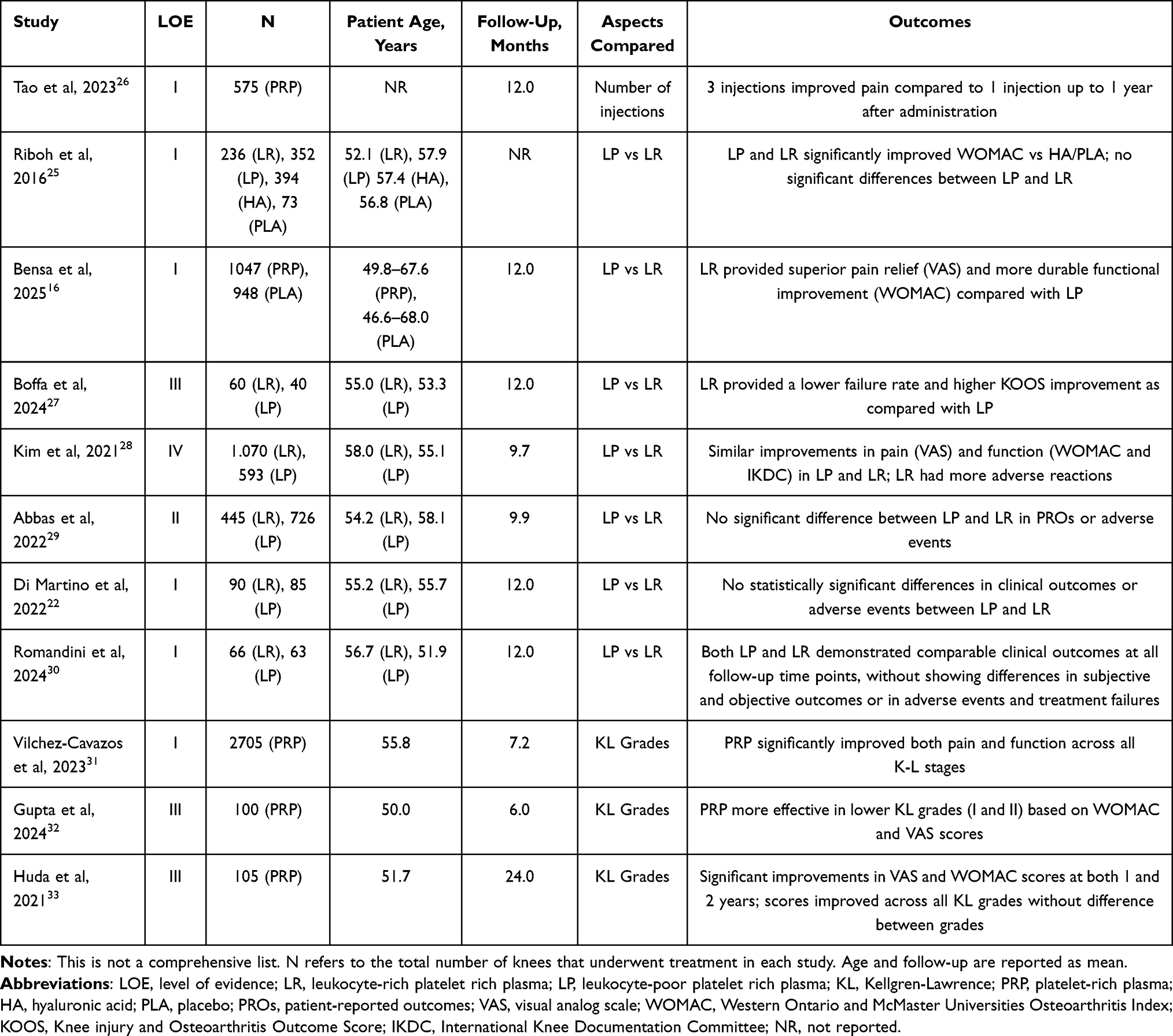 |
Table 2 Studies That Compared Different Aspects of PRP Injections for Knee Osteoarthritis |
A subsequent meta-analysis in 202128 further explored the comparison between LR-PRP and LP-PRP. Among the 32 studies reviewed—most with lower levels of evidence—only one directly compared both PRP types. In total, 1162 knees received LP-PRP and 628 received LR-PRP. Both formulations showed similar improvements in pain and function after 12 months. However, LR-PRP was associated with a higher frequency of adverse reactions.
In 2022, Abbas et al29 conducted a network meta-analysis of 20 RCTs and 3 prospective comparative studies involving 2260 patients with knee OA. Follow-up averaged 9.9 months. The authors found no significant differences between LR-PRP and LP-PRP in terms of PROs or adverse events. That same year, Di Martino et al22 published an RCT comparing 90 patients treated with LR-PRP and 85 with LP-PRP. Again, there were no statistically significant differences between the groups at 12-month follow-up in terms of clinical results or adverse reactions.
In a recent double-blind RCT, Romandini et al30 evaluated 132 patients with Kellgren–Lawrence grade I–III knee osteoarthritis who received either LR-PRP or LP-PRP injections. Over a 12-month follow-up period, both groups demonstrated significant and comparable improvements in pain, function, and overall clinical outcomes, with no differences in treatment failures or adverse events. These findings suggest that the presence of leukocytes in PRP does not significantly influence the efficacy or safety of the injection, supporting the notion that both LR-PRP and LP-PRP can be effectively utilized in the treatment of knee OA.
In summary, current evidence does not favor one PRP formulation over the other for managing knee OA. Further investigation is necessary to better understand how differences in PRP composition and delivery influence joint outcomes. However, despite these comparative analyses, the body of evidence directly evaluating leukocyte concentration as an independent variable remains limited. Variability in PRP preparation methods, leukocyte quantification, and reporting standards makes it challenging to establish definitive conclusions. Consequently, while current data suggest comparable efficacy and safety between LR-PRP and LP-PRP, further high-quality, standardized studies are warranted to clarify the true influence of leukocyte content on clinical outcomes.
Influence of Platelet Concentration on Clinical Outcomes
An important consideration in the clinical application of PRP for knee OA is the variability in platelet concentration achieved with different preparation methods. Since platelets are the primary carriers of growth factors and bioactive molecules, it has been hypothesized that higher concentrations may yield superior therapeutic effects.34 Recent evidence supports this dose–response relationship, suggesting that platelet concentration directly impacts both the magnitude and durability of clinical improvements.35
In a Level III cohort study by Boffa et al,27 the authors analyzed 253 patients with knee OA (Kellgren–Lawrence grade I–III) who received three intra-articular PRP injections and were stratified into high-, medium-, and low-platelet concentration groups. Across all clinical metrics—including Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales (Pain, Symptoms, activities of daily living [ADL], Sport and Recreation) and Subjective IKDC scores—higher platelet concentrations significantly correlated with better outcomes at 2, 6, and 12 months (Table 2). Moreover, the low-platelet group exhibited a notably higher failure rate (15.0%) compared with both the medium- and high-platelet groups (each 3.3%), while adverse event rates were similar across all groups.
A recent meta-analysis16 of 18 RCTs including 1995 patients with knee OA confirmed that PRP provides clinically relevant improvements in pain and function compared with placebo. Subanalysis based on platelet concentration revealed that high-platelet PRP offered superior pain relief and more durable functional improvement at 3, 6, and 12 months, whereas low-platelet PRP failed to provide clinically meaningful pain reduction, particularly in terms of the MCID for VAS scores. These findings underscore the importance of platelet concentration in determining the efficacy of PRP treatment for knee OA.
Collectively, these findings highlight that higher platelet concentrations in PRP are associated with superior clinical outcomes and lower failure rates, reinforcing the importance of preparation methods that maximize platelet yield. Nevertheless, it is important to note that despite these encouraging findings, the current evidence base directly examining the dose–response relationship of platelet concentration remains limited. Most studies employ heterogeneous preparation protocols and inconsistent reporting standards, which restrict definitive conclusions. This highlights the need for further standardized, high-quality studies to clarify the optimal platelet concentration for clinical efficacy.
Single Injection versus Multi-Dose Therapy
The optimal number of PRP injections for treating knee OA remains a topic of clinical debate. While single-dose protocols offer convenience and reduced cost, multiple-dose regimens may provide enhanced and more sustained therapeutic effects by maintaining a higher concentration of growth factors within the joint over time. To better understand the clinical impact of injection frequency, a recent systematic review and meta-analysis26 compared outcomes between single and multiple PRP injections. This review included 7 RCTs (575 patients, aged 20–80 years, balanced sex distribution) and compared the efficacy of one, two, or three intra-articular PRP injections for knee OA (Table 2).26 At 12-month follow-up, the group receiving three PRP injections reported significantly greater pain reduction—measured by a VAS—than the single-dose group (P < 0.0001), whereas the two-dose regimen did not demonstrate a statistically meaningful difference compared to a single injection. Regarding safety, no notable increase in adverse events was associated with either two-dose (p = 0.28) or three-dose (p = 0.24) protocols compared to a single injection. Reported complications were typically mild and transient. Injection spacing in the multi-dose groups was not specified in most studies, but the interval between injections ranged from 1 to 4 weeks in those studies which did report on injection intervals.
PRP Efficacy by Kellgren-Lawrence Grade
A key consideration in the application of PRP therapy is whether its effectiveness varies based on OA severity. The Kellgren-Lawrence (K-L) grading system is the most widely accepted tool to assess the severity of knee OA, with grades ranging from 0 (no radiographic evidence of OA) to IV (severe joint space narrowing and osteophyte formation).36 Clinicians often use this classification to guide treatment selection and prognosis. However, data regarding the relationship between OA grade and PRP outcomes have shown inconsistent results.
A comprehensive meta-analysis of 31 RCTs, including 2705 knees with follow-up periods ranging from 3 months to 2 years, assessed the efficacy of PRP across different stages of OA.31 The studies were grouped by K-L grade into three categories: early OA (grades I–II), mild to moderate OA (grades I–III), and all-stage OA (grades I–IV) (Table 2). The pooled analysis showed that PRP injections significantly improved both pain and function across all K-L stages when compared with control interventions such as HA, corticosteroids, BMAC, prolotherapy, and placebo injections. These findings support the use of PRP as a viable treatment option even in more advanced disease stages, although the greatest benefits were typically observed in those with early to moderate OA. Furthermore, improvements in pain and functional scores were generally sustained throughout the follow-up period, ranging from 3 months up to 2 years, indicating that PRP can provide both short- and long-term benefits for patients across different stages of knee OA.
These findings are further supported by recent prospective studies evaluating outcomes based on radiographic severity. In a study of 100 knees (K-L grades I–IV) undergoing a single injection with LP-PRP, all K-L subgroups demonstrated significant improvements in both VAS and WOMAC scores from baseline to 6-month follow-up, but the greatest improvements were observed in knees with K-L grades I and II.32 Knees with grade IV disease still improved but to a lesser degree. Another prospective cohort study included 105 knees with K-L grades I–III which underwent a series of three LP-PRP injections spaced one month apart.33 Patients were followed for 24 months and showed sustained improvements in both pain and function (as measured by WOMAC and VAS scores), with no statistically significant differences in outcomes between the K-L I, II, or III groups. This suggests that PRP may provide durable and clinically meaningful benefits even in moderate OA, especially when delivered as a series of injections.
Collectively, the evidence suggests that PRP therapy is effective in improving pain and function across all stages of knee OA, with the greatest benefits observed in early and moderate disease. While advanced OA (K-L IV) may demonstrate a lessened response, knees with K-L grades I–III consistently experience meaningful and sustained clinical improvement. These findings reinforce the utility of PRP as a treatment option across a range of OA severities, particularly when initiated before end-stage disease.
Discussion
Based on the current literature, PRP injections are a safe and effective non-surgical option for managing knee OA in patients with all Kellgren-Lawrence grades.31,32 While several studies have demonstrated clinically meaningful improvements in pain and function compared with placebo and hyaluronic acid, others have reported modest or non-significant effects, reflecting ongoing heterogeneity in outcomes. Clinicians may consider offering PRP therapy as an initial non-surgical treatment option for patients who are motivated and able to afford these injections, recognizing that responses may vary. A protocol involving three intra-articular PRP injections spaced 1–4 weeks apart has demonstrated superior pain relief and functional improvement compared to a single injection, without a corresponding increase in adverse events.26 Current evidence shows no consistent differences in safety or efficacy between leukocyte-rich and leukocyte-poor PRP for the treatment of knee OA.29,30
To maximize clinical benefit, PRP treatment should ideally be initiated in the earlier stages of OA.32 However, significant methodological limitations in the existing literature-including variability in PRP preparation and classification, small sample sizes, lack of blinding, and short follow-up durations- continue to limit the strength of current conclusions. Given this variability, standardized protocols regarding dosage, frequency, and composition are needed to improve reproducibility and interpretability of findings. Until such guidelines are established, clinicians are encouraged to use consistent preparation techniques and validated outcome measures to monitor efficacy. In addition, further research should aim to optimize delivery protocols and explore the long-term disease-modifying potential of PRP in knee OA. In particular, more studies are needed on the potential for PRP injections in delaying knee arthroplasty. Collaborative, multicenter randomized controlled trials with uniform methodology will be instrumental in advancing the clinical utility of PRP and integrating it into standardized OA management pathways.
Conclusion
PRP represents a biologically active and increasingly utilized nonoperative treatment option for knee osteoarthritis, particularly in early to moderate stages of disease. Current evidence suggests that PRP provides superior short- to mid-term pain and functional outcomes compared to hyaluronic acid and results comparable to other orthobiologics such as bone marrow aspirate (BMAC). However, significant heterogeneity exists among study protocols, and no single preparation or regimen has demonstrated clear superiority. Overall, PRP appears to be a safe and potentially beneficial adjunct in the management of knee osteoarthritis, though further high-quality randomized trials are needed to establish its long-term efficacy and optimal use parameters.
Disclosure
Dr Matthew Kraeutler reports personal fees from Smith & Nephew, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
2. Ramezanpour S, Kanthawang T, Lynch J, et al. Impact of sustained synovitis on knee joint structural degeneration: 4-year MRI data from the osteoarthritis initiative. J Magn Reson Imaging. 2023;57(1):153–164. doi:10.1002/jmri.28223
3. Obara K, Cardoso JR, Reis BM, Matos MA, Kawano MM. Quality of life in individuals with knee osteoarthritis versus asymptomatic individuals. Musculoskeletal Care. 2023;21(4):1364–1370. doi:10.1002/msc.1814
4. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
5. Berenbaum F, Wallace IJ, Lieberman DE, Felson DT. Modern-day environmental factors in the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2018;14(11):674–681. doi:10.1038/s41584-018-0073-x
6. Grazina R, Andrade R, Bastos R, et al. Clinical Management in Early OA. Adv Exp Med Biol. 2018;1059:111–135. doi:10.1007/978-3-319-76735-2_5
7. Zhou Q, Chen J, Yu W, et al. A critical overview of systematic reviews and meta-analyses of intra-articular injection of platelet rich plasma versus hyaluronic acid for knee osteoarthritis. Clin Rheumatol. 2025;44(2):547–571. doi:10.1007/s10067-024-07264-0
8. Testa G, Giardina SMC, Culmone A, et al. Intra-articular injections in knee osteoarthritis: a review of literature. J Funct Morphol Kinesiol. 2021;6(1):15. doi:10.3390/jfmk6010015
9. Adk L, Enweze L, DeBaun MR, Dragoo JL. Platelet-rich plasma. Clin Sports Med. 2019;38(1):17–44. doi:10.1016/j.csm.2018.08.001
10. Belk JW, Lim JJ, Keeter C, et al. Patients with knee osteoarthritis who receive platelet-rich plasma or bone marrow aspirate concentrate injections have better outcomes than patients who receive hyaluronic acid: systematic review and meta-analysis. Arthroscopy. 2023;39(7):1714–1734. doi:10.1016/j.arthro.2023.03.001
11. Akeda K, An HS, Okuma M, et al. Platelet-rich plasma stimulates porcine articular chondrocyte proliferation and matrix biosynthesis. Osteoarthritis Cartilage. 2006;14(12):1272–1280. doi:10.1016/j.joca.2006.05.008
12. Qiao X, Yan L, Feng Y, et al. Efficacy and safety of corticosteroids, hyaluronic acid, and PRP and combination therapy for knee osteoarthritis: a systematic review and network meta-analysis. BMC Musculoskelet Disord. 2023;24(1):926. doi:10.1186/s12891-023-06925-6
13. Bendinelli P, Matteucci E, Dogliotti G, et al. Molecular basis of anti-inflammatory action of platelet-rich plasma on human chondrocytes: mechanisms of NF-κB inhibition via HGF. J Cell Physiol. 2010;225(3):757–766. doi:10.1002/jcp.22274
14. Alazzeh MS, Naseh HAM, Vasiliadis A, et al. Platelet-rich plasma intra-articular knee injections from open preparation techniques do not pose a higher risk of joint infection: a systematic review of 91 randomized controlled trials and 5914 injections. J Exp Orthop. 2024;11(3):e70002. doi:10.1002/jeo2.70002
15. Piuzzi NS, Ng M, Kantor A, et al. What is the price and claimed efficacy of platelet-rich plasma injections for the treatment of knee osteoarthritis in the United States? J Knee Surg. 2019;32(9):879–885. doi:10.1055/s-0038-1669953
16. Bensa A, Previtali D, Sangiorgio A, et al. PRP injections for the treatment of knee osteoarthritis: the improvement is clinically significant and influenced by platelet concentration: a meta-analysis of randomized controlled trials. Am J Sports Med. 2025;53(3):745–754. doi:10.1177/03635465241246524
17. Costa LAV, Lenza M, Irrgang JJ, Fu FH, Ferretti M. How does platelet-rich plasma compare clinically to other therapies in the treatment of knee osteoarthritis? A systematic review and meta-analysis. Am J Sports Med. 2023;51(4):1074–1086. doi:10.1177/03635465211062243
18. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020;72(2):220–233. doi:10.1002/art.41142
19. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
20. Belk JW, Kraeutler MJ, Houck DA, et al. Platelet-rich plasma versus hyaluronic acid for knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Am J Sports Med. 2021;49(1):249–260. doi:10.1177/0363546520909397
21. Li YF, Xing HH, Wei CK, et al. Platelet-rich plasma is more effective than hyaluronic acid injections for osteoarthritis of the knee: a meta-analysis based on randomized, double-blinded, controlled clinical trials. Arthroscopy. 2025:S0749–8063(25)00484–0. doi:10.1016/j.arthro.2025.06.033
22. Di Martino A, Boffa A, Andriolo L, et al. Leukocyte-rich versus leukocyte-poor platelet-rich plasma for the treatment of knee osteoarthritis: a double-blind randomized trial. Am J Sports Med. 2022;50(3):609–617. doi:10.1177/03635465211064303
23. Khalilizad M, Emadian ST, Marzban Abbas Abadi M. Comparative efficacy of different doses of platelet-rich plasma injection in the treatment of knee osteoarthritis: a systematic review and network meta-analysis. J Orthop Surg Res. 2025;20(1):221. doi:10.1186/s13018-025-05650-1
24. Xue Y, Wang X, Wang X, Huang L, Yao A, Xue Y. A comparative study of the efficacy of intra-articular injection of different drugs in the treatment of mild to moderate knee osteoarthritis: a network meta-analysis. Medicine. 2023;102(12):e33339. doi:10.1097/MD.0000000000033339
25. Riboh JC, Saltzman BM, Yanke AB, Fortier L, Cole BJ. Effect of leukocyte concentration on the efficacy of platelet-rich plasma in the treatment of knee osteoarthritis. Am J Sports Med. 2016;44(3):792–800. doi:10.1177/0363546515580787
26. Tao X, Aw AAL, Leeu JJ, Bin Abd Razak HR. Three doses of platelet-rich plasma therapy are more effective than one dose of platelet-rich plasma in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Arthroscopy. 2023;39(12):2568–2576.e2. doi:10.1016/j.arthro.2023.05.018
27. Boffa A, De Marziani L, Andriolo L, et al. Influence of platelet concentration on the clinical outcome of platelet-rich plasma injections in knee osteoarthritis. Am J Sports Med. 2024;52(13):3223–3231. doi:10.1177/03635465241283463
28. Kim JH, Park YB, Ha CW, Roh YJ, Park JG. Adverse reactions and clinical outcomes for leukocyte-poor versus leukocyte-rich platelet-rich plasma in knee osteoarthritis: a systematic review and meta-analysis. Orthop J Sports Med. 2021;9(6):23259671211011948. doi:10.1177/23259671211011948
29. Abbas A, Du JT, Dhotar HS. The effect of leukocyte concentration on platelet-rich plasma injections for knee osteoarthritis: a network meta-analysis. J Bone Joint Surg Am. 2022;104(6):559–570. doi:10.2106/JBJS.20.02258
30. Romandini I, Boffa A, Di Martino A, et al. Leukocytes do not influence the safety and efficacy of platelet-rich plasma injections for the treatment of knee osteoarthritis: a double-blind randomized controlled trial. Am J Sports Med. 2024;52(13):3212–3222. doi:10.1177/03635465241283500
31. Vilchez-Cavazos F, Blázquez-Saldaña J, Gamboa-Alonso AA, et al. The use of platelet-rich plasma in studies with early knee osteoarthritis versus advanced stages of the disease: a systematic review and meta-analysis of 31 randomized clinical trials. Arch Orthop Trauma Surg. 2023;143(3):1393–1408. doi:10.1007/s00402-021-04304-1
32. Gupta P, Jamra A, Prakash S, Gupta S, Bharti A. Evaluating the efficacy of platelet-rich plasma in treating primary knee osteoarthritis: a prospective interventional study. Cureus. 2024;16(10):e71415. doi:10.7759/cureus.71415
33. Huda N, Islam MSU, Bishnoi S, et al. Role of triple injection platelet-rich plasma for osteoarthritis knees: a 2 years follow-up study. Indian J Orthop. 2021;56(2):249–255. doi:10.1007/s43465-021-00459-6
34. Lubkowska A, Dolegowska B, Banfi G. Growth factor content in PRP and their applicability in medicine. J Biol Regul Homeost Agents. 2012;26(2 Suppl 1):3S–22S.
35. Berrigan WA, Bailowitz Z, Park A, et al. A greater platelet dose may yield better clinical outcomes for platelet-rich plasma in the treatment of knee osteoarthritis: a systematic review. Arthroscopy. 2025;41(3):809–817.e2. doi:10.1016/j.arthro.2024.03.018
36. Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clin Orthop Relat Res. 2016;474(8):1886–1893. doi:10.1007/s11999-016-4732-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.