Back to Journals » Infection and Drug Resistance » Volume 19
Current Evidence on Voriconazole Exposure and Individualized Therapy for Aspergillosis
Received 9 November 2025
Accepted for publication 6 March 2026
Published 27 March 2026 Volume 2026:19 579990
DOI https://doi.org/10.2147/IDR.S579990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Ziyu Wu,1,2 Zhiqiang Lin,1 Li Jiang2
1Department of Pharmacy, Quanzhou First Hospital Affiliated to Fujian Medical University, Quanzhou, Fujian, People’s Republic of China; 2School of Pharmacy, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China
Correspondence: Zhiqiang Lin, Department of Pharmacy, Quanzhou First Hospital Affiliated to Fujian Medical University, No. 248-252, Dongjie Street, Licheng District, Quanzhou, Fujian, People’s Republic of China, Tel +86 13799240306, Email [email protected]
Abstract: With emerging global antifungal resistance, voriconazole is a preferred first-line antifungal agent for the treatment of aspergillosis, and therapeutic drug monitoring (TDM) is frequently utilized during therapy. This review examines evidence from international guidelines, clinical studies, case reports, and population pharmacokinetic analyses to investigate the multifactorial drivers influencing voriconazole therapy. Current guidelines demonstrate variability in recommended target trough concentrations, though a range of 1.0– 5.5 mg/L appears as a frequently cited reference interval; however, these recommendations are often derived from heterogeneous populations rather than being specific to aspergillosis. Plasma voriconazole concentration alone may not fully account for the variability in clinical outcomes. Efficacy and safety are influenced by multiple factors, including CYP2C19 polymorphisms, disease severity, host immune status, and infection site. Consequently, the interpretation of a single concentration threshold may be limited. A multidimensional approach—considering genotype, host factors, inflammatory status, and dynamic clinical context—is a component of individualized therapy for characterizing treatment response and toxicity risk. Within this framework, TDM is an established tool for assessing systemic exposure, and its integration with clinical and biological information is relevant for clinical assessment. Altogether, these observations underscore the value of integrated clinical assessment while identifying remaining evidence gaps for further investigation.
Keywords: voriconazole, Aspergillus, therapeutic drug monitoring, individualized dosing, pharmacokinetics
Introduction
Aspergillosis is a clinically significant fungal infection caused by species of the genus Aspergillus. It predominantly affects immunocompromised individuals, as well as critically ill patients in intensive care units (ICUs), particularly those with severe viral infections.1,2 The incidence of invasive aspergillosis (IA) varies considerably across different patient populations and geographic regions.1–7 In certain areas of Africa, prevalence rates as high as 27% have been reported, with associated mortality exceeding 60%.8 Globally, IA is estimated to affect more than 2 million individuals annually, with crude mortality rates surpassing 85% in high-risk populations, including patients with chronic obstructive pulmonary disease, those admitted to ICUs, individuals with lung cancer, and patients with hematological malignancies.9
Due to environmental selection pressure and the agricultural use of azole fungicides, azole resistance in Aspergillus spp. has shown an upward trend10 with regional variability in resistance rates.11,12 The underlying mechanisms of azole resistance are multifactorial and include mutations in the CYP51A gene, overexpression of efflux transporters, and alterations in non-target genes,13,14 thereby further complicating antifungal therapy.
Current international guidelines recommend triazole antifungals, such as voriconazole, isavuconazole, and posaconazole, as first-line agents for the treatment of aspergillosis.15,16 Voriconazole, a second-generation triazole, has been consistently endorsed as the preferred first-line therapy by multiple clinical practice guidelines.17–21 However, voriconazole is characterized by nonlinear pharmacokinetics, leading to pronounced interindividual and intraindividual variability in systemic exposure.22 Key determinants of voriconazole pharmacokinetics include CYP2C19 genetic polymorphisms, body weight, hepatic function, concomitant medications, and inflammatory status.23 Notably, the prevalence of CYP2C19 poor metabolizer phenotypes is significantly higher in East Asian, Southeast Asian, and Indigenous Oceanian populations compared with Caucasians, whereas rapid metabolizers are more commonly observed in Europe, the Middle East, and Africa.24
Despite its established role as a first-line antifungal agent, voriconazole has a narrow therapeutic window. Most guidelines recommend a target trough concentration range of 1.0–5.5 mg/L, (IDSA;18 ESCMID-ECMM20), whereas Takesue et al25 specify a narrower target of 2.0–4.0 mg/L for Asian patients with aspergillosis. While TDM is frequently utilized to achieve therapeutic levels, consensus remains lacking regarding optimal target concentrations, site-specific therapeutic thresholds, and individualized dosing strategies across diverse patient populations.
This review aims to summarize target concentration ranges, dosing regimens, and individualized TDM practices for site-specific infections in the treatment of aspergillosis from the existing literature.
Methods
Literature Search and Screening
PubMed and Web of Science databases were searched for literature published between January 2002 and July 2025. The objective was to identify studies concerning voriconazole treatment for Aspergillus infections in the context of therapeutic drug monitoring. Search terms included “voriconazole”, “aspergillosis”, “invasive aspergillosis”, “pharmacokinetics”, and “therapeutic drug monitoring”, as well as site-specific terms such as “brain”, “intracranial”, and “CNS”, utilizing Boolean operators (AND/OR). Search terms also included “dose adjustment” and “dose optimization” to capture relevant literature. A manual search of references within the included studies and relevant guidelines was also performed. Following the removal of duplicates, potential literature was screened based on titles and abstracts, followed by a full-text review.
Inclusion Criteria
A literature search was conducted to identify relevant studies on voriconazole for the treatment of aspergillosis. Inclusion criteria comprised randomized controlled trials (RCTs), cohort studies, case-control studies, case series, case reports, retrospective studies, and population pharmacokinetic (PopPK) studies. Specifically, case reports were included for patients meeting the criteria for proven or probable diagnosis as defined by the EORTC/MSG guidelines. Clinical and PopPK studies included patients categorized as proven, probable, or possible cases according to the EORTC/MSG guidelines.26 Eligible studies were required to document voriconazole therapy for aspergillosis in conjunction with TDM and definitive blood concentration measurements.
Guidelines concerning aspergillosis management and voriconazole TDM were included if they provided target concentration ranges, dosing regimens, and dose adjustment strategies.
Data Extraction
Efficacy and safety outcomes of voriconazole at various plasma concentration levels were extracted from the included clinical studies and case reports. Additionally, relevant recommendations for voriconazole therapy in aspergillosis were collected from the identified guidelines.
Results
Associations Between Voriconazole Concentrations and Clinical Outcomes in Patients with Aspergillosis Reported in Clinical Studies
This review integrates the results of six clinical studies27–32 involving voriconazole treatment for aspergillosis. Three of these studies identified associations between voriconazole plasma concentrations and clinical safety or efficacy.29,31,32 Specifically, adverse reactions such as skin rash and elevated liver enzymes, alongside an increased risk of cardiotoxicity, were reported in patients with trough concentrations exceeding established thresholds. Regarding efficacy, subtherapeutic concentrations (< 1.0 mg/L or < 2.0 mg/L) were associated with treatment failure rates ranging from 45% to 83.33%. Conversely, clinical success rates of 32% to 85.7% were observed when trough concentrations remained within the range of 1.0–5.0 mg/L (or 1.0–5.83 mg/L).31,32 Notably, Lee et al31 reported that in patients with chronic pulmonary aspergillosis, the lower trough concentration limit was observed at 0.5 mg/L, which was associated with a 41.7% efficacy rate and mitigated hepatotoxicity. Data extracted from these clinical studies are summarized in Table 1.
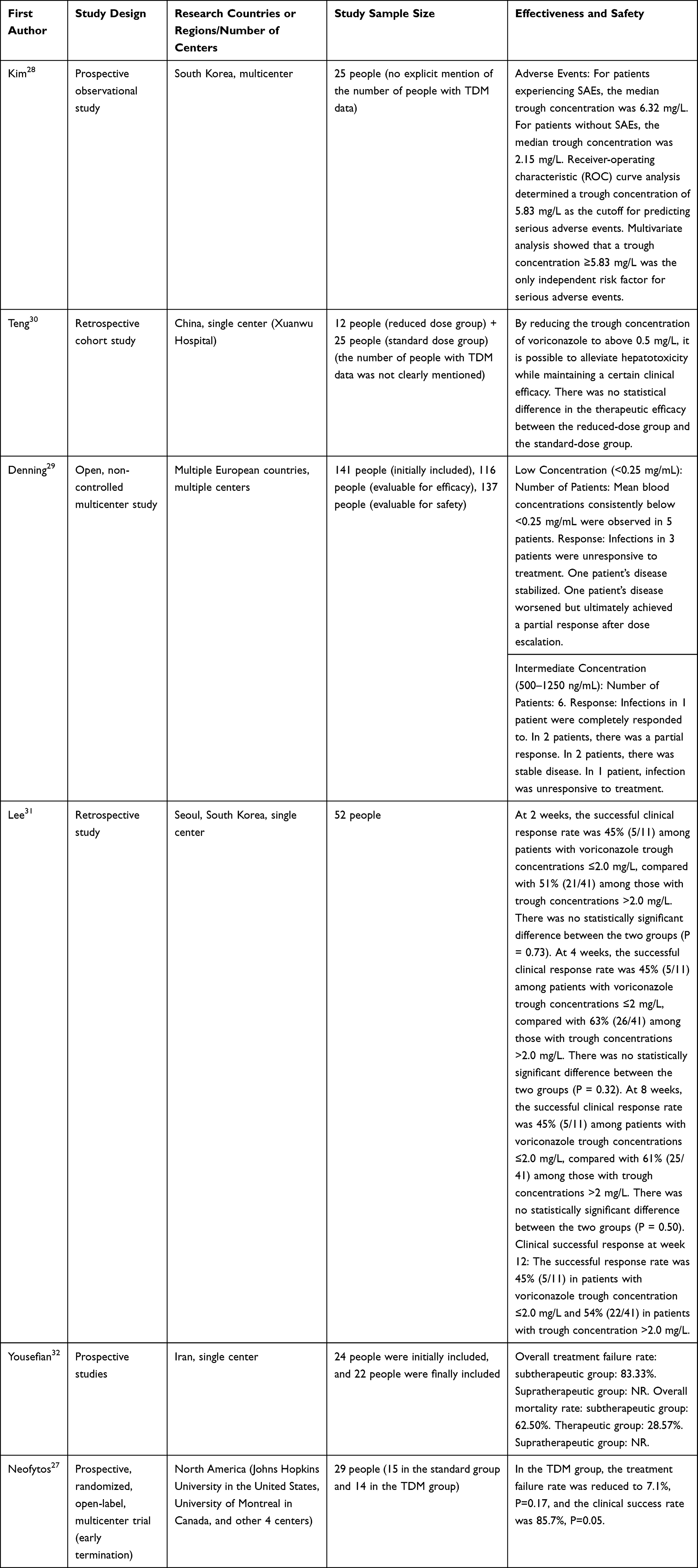 |
Table 1 Data on the Efficacy and Safety of Voriconazole in Clinical Studies Related to Aspergillosis |
Clinical Observations of Voriconazole Concentrations and Outcomes in Aspergillosis Case Reports
Twenty-four clinical cases33–56 provide a supplementary perspective on voriconazole treatment for aspergillosis in real-world settings (detailed in Supplementary Table 1). Analysis of these cases indicates that clinical improvement was observed within a trough concentration range of 1.0–3.0 mg/L, while concentrations below 2.0 mg/L or above 5.0 mg/L were associated with treatment failure and toxicity, respectively. Individual cases showed clinical improvement at relatively low trough concentrations, such as 0.6 mg/L.51 However, some patients did not exhibit favorable clinical responses despite maintaining concentrations within recommended ranges (eg., 2.87 mg/L,49 3.8 mg/L,44 and 4.22 mg/L57). Reflecting the limitations of case-level evidence, these observations remain hypothesis-generating and provide exploratory insights rather than definitive causality or universal therapeutic thresholds.
Voriconazole Dosing and TDM Guidance Within Aspergillosis Treatment Guidelines and Pharmacotherapy TDM Guidelines
Guidelines for both aspergillosis treatment and voriconazole TDM emphasize the importance of conducting TDM.15–21,58–62 While a clinical framework of “loading-maintenance-TDM-readjustment” is widely recognized, specific recommendations regarding dosing and target thresholds vary among different clinical and TDM-specific organizations. For adults, the initial loading dose is typically 6 mg/kg every 12 hours (two doses), followed by a maintenance dose of 4 mg/kg every 12 hours, with TDM initiation recommended during the early phase of treatment (days 4–7).15,18,19,21,58,63 Guidelines state that special populations, such as individuals with hepatic impairment, those undergoing continuous renal replacement therapy (CRRT), or CYP2C19 poor metabolizers, require early monitoring to facilitate individualized dosing and reduce dose-related toxicities. However, the recommended trough concentration ranges are not standardized, with values including 1.0–5.5 mg/L,18–21 1.0–6.0 mg/L,60 and 1.0–5.0 mg/L.17,18 Notably, Takesue et al25 specify a target range of 2.0–4.0 mg/L for Asian patients with aspergillosis. Furthermore, dose adjustment strategies differ, with some guidelines suggesting 50% increments or reductions based on target attainment.58,63 Detailed comparisons of dosing ranges, adjustment schemes, and considerations for special populations are provided in Table 2.
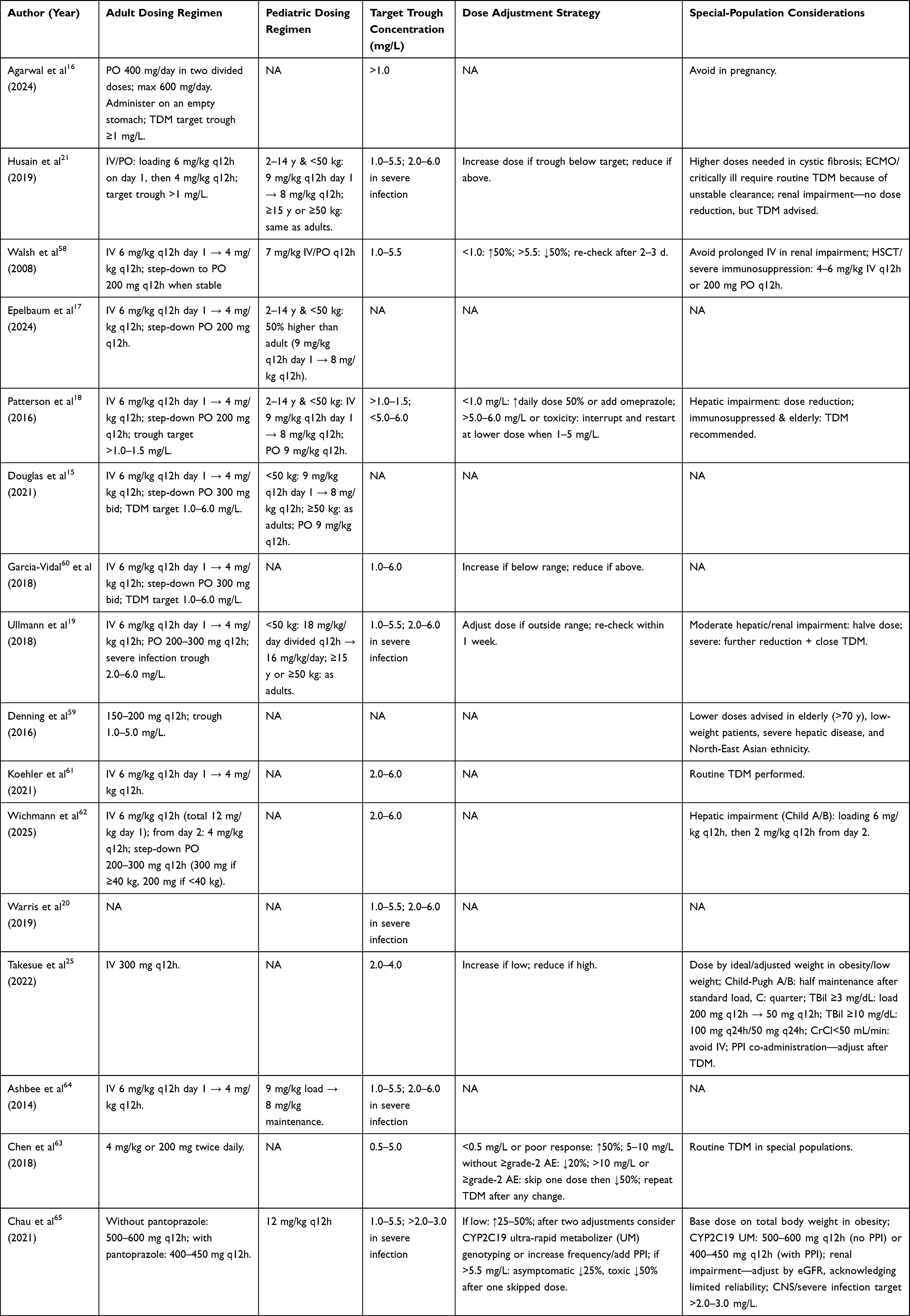 |
Table 2 Comparison of Voriconazole Dosing and TDM Recommendations in Aspergillosis Management and TDM-Specific Guidelines |
Voriconazole Treatment for Aspergillus Infections in Specific Sites
Clinical guideline recommendations for voriconazole therapy are differentiated by the anatomical site of infection (Table 3).15,18,19,21 For extrapulmonary manifestations, the currently available guidelines specify protocols that diverge from standard pulmonary management across three primary variables: therapeutic duration, the timing of surgical adjuncts, and individualized TDM targets. Specifically, the clinical recommendations include prolonged treatment courses for osteoarticular and chronic pulmonary infections, alongside mandatory early surgical debridement for sinonasal and ocular involvements. TDM trough targets for central nervous system (CNS) and disseminated disease are adjusted to higher ranges relative to pulmonary protocols to ensure adequate tissue penetration.
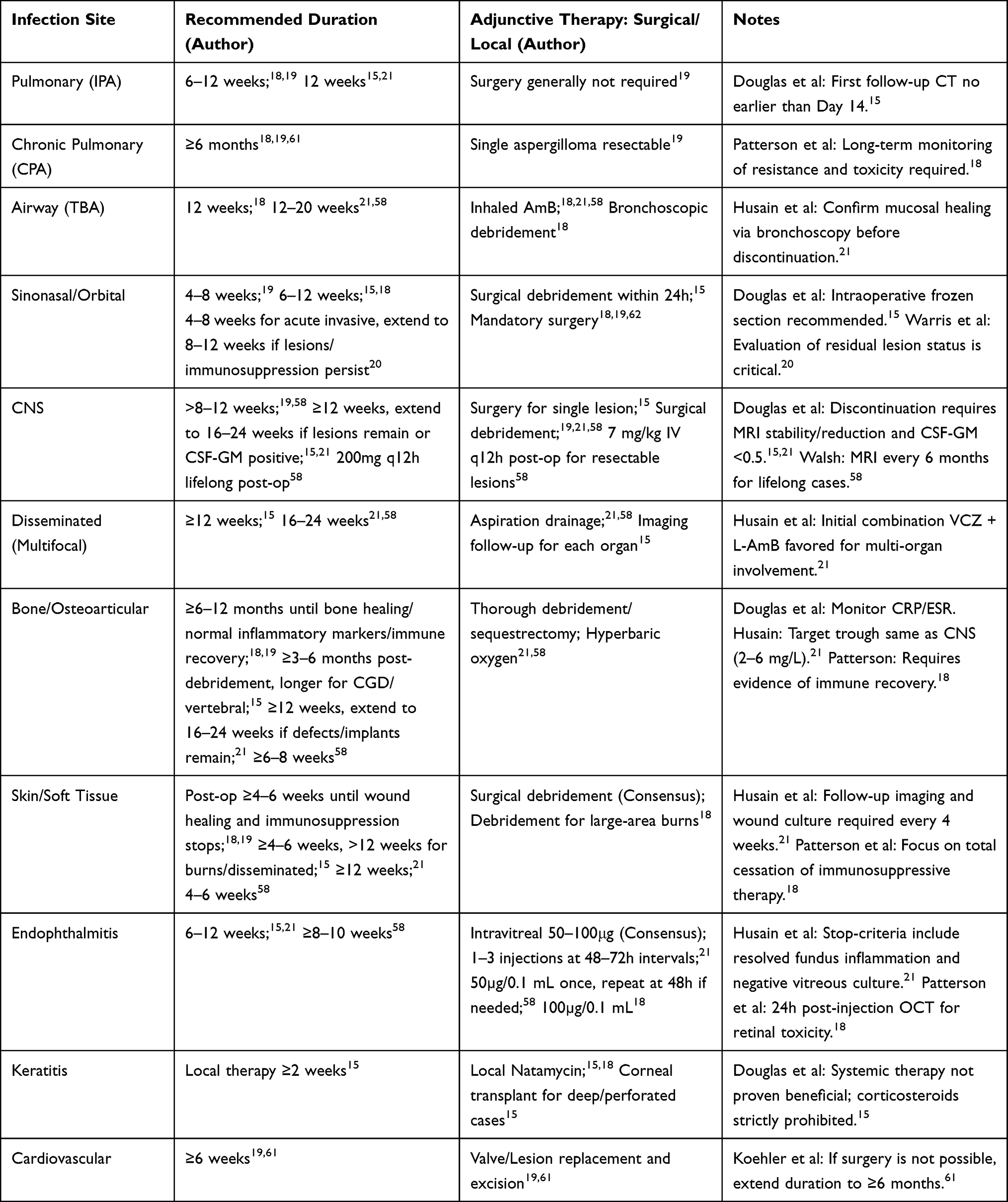 |
Table 3 Summary of Clinical Guideline Recommendations for Voriconazole Therapy Across Different Sites of Aspergillosis Infection |
Summary of PopPK Studies of Voriconazole in Patients with Aspergillosis
This review summarizes 4 PopPK studies involving patients with aspergillosis.66–69 The authors of these investigations made use of a variety of diverse modeling approaches to investigate and explore the factors that are associated with voriconazole exposure variability and the clinical implications that they identified.
Chantharit et al69 reported that for patients with serum albumin (SA) levels ≤ 30.0 g/L, a maintenance dose of 200 mg po q12h enabled 64% of the cohort to reach the target concentration of ≥ 2.0 mg/L. The researchers noted that patients with SA > 30.0 g/L appeared to require higher dosages to achieve the same therapeutic target. They observed no significant influence from the CYP2C19 genotype, suggesting that inflammation-related factors might mask its potential effects, and they identified serum albumin and GGT as parameters for routine clinical monitoring.
In their evaluation, Duangpraphat et al66 found that intravenous administration resulted in higher AUC:EC50 ratios compared to oral dosing. The authors indicated that critically ill patients requiring intubation exhibited significantly elevated AUC:EC50 ratios. They also pointed out that individuals with higher EC50 values might face risks of suboptimal outcomes similar to those observed with elevated minimum inhibitory concentrations (MIC). Consequently, the investigators discussed the possibility of adjusting target concentrations within a range up to 6.0 mg/L, using galactomannan levels as an indirect measure to evaluate therapeutic response and inform dose adjustments.
Wang et al66 stated that patients undergoing CRRT required increased loading doses (≥5 mg/kg q12h) and maintenance doses (4 mg/kg q12h) to reach target levels. For non-CRRT patients, the authors found that 2 mg/kg q12h was sufficient to achieve the target range of 2.0–5.0 mg/L. They also highlighted the influence of CRP, GGT, and AST on drug clearance, suggesting that dosage adjustments be made based on the dynamic changes of these markers.
Liu and Mould67 focused on the concurrent use of voriconazole and anidulafungin, noting a synergistic effect of combined exposure on hepatic adverse events. The authors observed that during monotherapy, dose adjustments might be guided by clinical response and tolerance rather than strict adherence to fixed concentration thresholds. However, in the context of combination therapy, they emphasized that monitoring exposure served as a method to mitigate the risk of cumulative toxicities, such as hepatotoxicity and psychiatric symptoms. The primary findings and characteristics of these four investigations are summarized in Table 4.
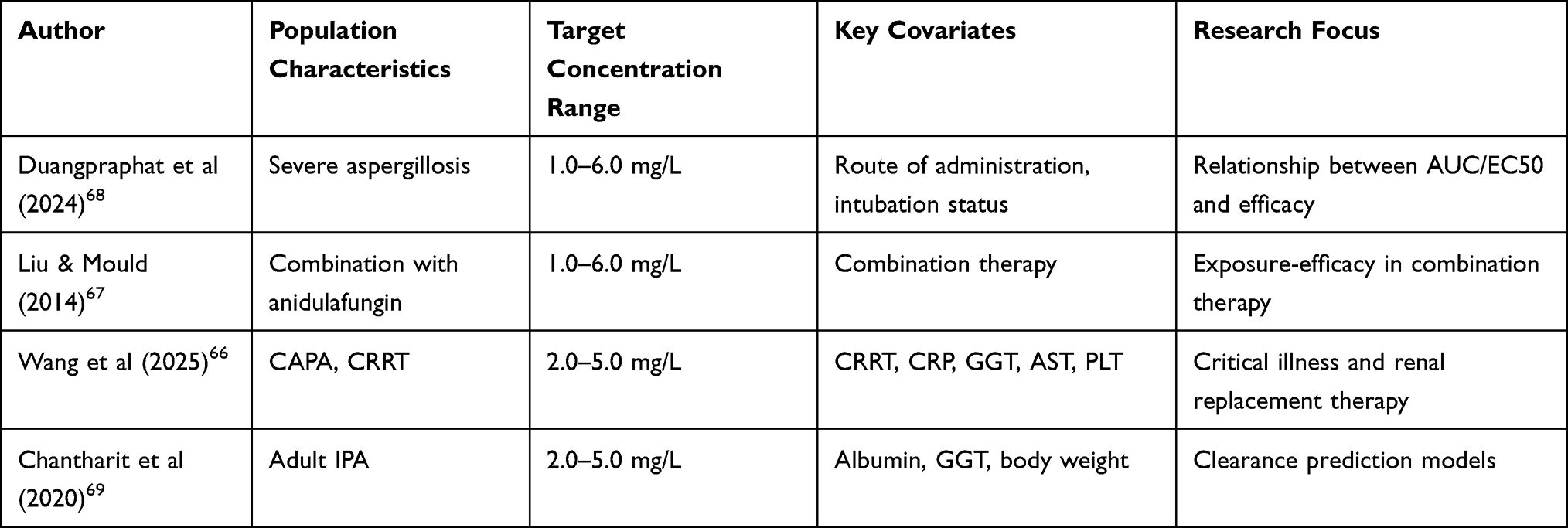 |
Table 4 Summary of Population Pharmacokinetic Studies of Voriconazole in Patients with Aspergillosis |
Discussion
Clinical Utility of Trough Concentration Thresholds in Voriconazole Therapy for Aspergillosis
Currently, it is widely accepted that the clinical efficacy and safety of voriconazole are closely linked to its systemic exposure levels. Accordingly, major clinical guidelines unanimously recognize the pivotal role of voriconazole in aspergillosis treatment and advocate for the implementation of TDM.15,18,20,59 Notably, a seminal 2008 study by Pascual et al70 recommended a target trough concentration range of 1.0–5.5 mg/L, a threshold that has since been extensively cited in the literature. Moreover, multiple meta-analyses have confirmed that maintaining voriconazole plasma concentrations within specific thresholds is significantly associated with improved clinical outcomes.71–74 Corroborating these observations, preclinical mouse models validate that voriconazole efficacy is exposure-dependent, providing a pharmacological foundation for clinical target concentrations.75–77
Although current guidelines offer differing perspectives on the target plasma concentration for voriconazole, most are categorized as strong recommendations based on low-level evidence. An integration of existing guidelines reveals that these recommended concentrations are not entirely consistent. Even regarding the target concentration intervals, descriptions vary among guidelines: most employ closed intervals, whereas others use ranges defined by inequalities; for instance, the guidelines by Patterson et al18 specify a target of >1.0 mg/L and <5.0–6.0 mg/L. Furthermore, multiple aspergillosis treatment guidelines20,21,61,62 cite the 2017 ESCMID guidelines in their plasma concentration recommendations. However, several studies cited by the ESCMID guidelines to establish these targets included patients with various fungal infections,70,78–81 rather than being specifically designed for patients with aspergillosis.
Regarding real-world data, an analysis of select case reports33–56 on voriconazole treatment for aspergillosis found that the range of effective trough concentrations for successful treatment is narrower than the standard reference intervals recommended by major guidelines. Given the limitations of case reports in terms of study design and sample size, these observations should be interpreted with caution; their primary value lies in providing clues to understand the heterogeneity of the voriconazole exposure-response relationship, rather than serving as a basis for establishing a uniform therapeutic threshold. However, a clinical study by Teng et al30 suggested that maintaining voriconazole trough concentrations above 0.5 mg/L can sustain efficacy in chronic pulmonary aspergillosis (CPA). This suggests that CYP2C19 poor metabolizers may also achieve safe, long-term therapy by initially halving the dose and implementing TDM.
Limitations of Fixed Trough Concentration Thresholds and TDM Strategies
Lee et al31 noted that an individual trough concentration may not accurately reflect true systemic exposure, pointing out that host factors such as neutrophil counts and immunosuppression status are more predictive of acute efficacy than drug concentrations alone. This underscores the profound impact of individual patient factors on clinical outcomes. Consequently, several studies have raised dissenting views regarding the sole reliance on voriconazole TDM. For instance, Tan et al82 utilized a probability model to suggest that monitoring liver function is more effective than monitoring voriconazole blood levels. Furthermore, a clinical trial by Veringa et al83 evaluated hematology patients with IA. This study found that a passive TDM strategy maintaining trough concentrations between 1 to 6 mg/L failed to improve the 28-day composite outcome compared to standard dosing. The strategy did not significantly reduce mortality rates or treatment discontinuation caused by toxicity, yielding a P value of 0.93.Troke et al78 further observed that at high concentrations, the efficacy of voriconazole in aspergillosis patients was significantly lower than in those with yeast infections. They contended that efficacy does not monotonically increase with plasma concentration. Instead, it must be integrated with pathogen MIC and host factors, proposing a trough to MIC ratio of 2 to 5 as an individualized TDM target. Similarly, Ueda et al84 found that in non-refractory hematological patients with IA, a trough concentration of 2.0 mg/L or greater was associated with clinical response, while failure rates rose significantly below this threshold. However, in refractory cases, concentrations exceeding 2.0 mg/L yielded no additional benefit. This indicates that simply escalating drug concentrations is insufficient to overcome therapeutic challenges in refractory patients, thereby highlighting the necessity of individualized assessment.
Influence of Aspergillus Resistance on Voriconazole Efficacy
A review indicates that Aspergillus resistance has spread globally, with resistant strains detected in clinical and environmental isolates across numerous countries.85 Mechanisms of voriconazole resistance in Aspergillus include CYP51A mutations,86–91 efflux pump overexpression,92 off-target mutations,93 environmental stress, and genomic instability.94–96 A retrospective study by Lestrade et al97 indicated that voriconazole-resistant Aspergillus infections significantly increased mortality rates. Uluç et al98 suggested that in patients with multidrug-resistant (MDR) and extensively drug-resistant (XDR) bacterial infections in respiratory intensive care units, antimicrobial resistance classification alone is insufficient to predict mortality, with outcomes being more influenced by host factors and disease severity.
Shifting Guidelines from Fixed Plasma Concentration Thresholds to Individualized Approaches
In the 2008 IDSA guidelines by Walsh et al,58 a unified dosing regimen was formally recommended to serve as the initial approach for the clinical management of IA TDM was suggested to be applied within limited scenarios involving treatment failure, signs of toxicity, or special patient populations. In subsequent guidelines, routine TDM has been observed as a standard recommendation. Multiple meta-analyses71,99,100 have reported the influence of individual factors on plasma concentrations.
Recent guidelines, including the 2016 IDSA update18 and the 2021 guidelines by Chau et al,65 maintain reference ranges for voriconazole while emphasizing the integration of multi-dimensional clinical factors such as CYP2C19 genotype, body weight, concomitant medications, and infection site These documents describe dynamic individualized adjustments through TDM to maintain clinical efficacy and limit toxicity. Chau et al65 further noted higher initial dosing regimens for ultra-rapid or rapid metabolizer phenotypes, which may be supplemented with genetic testing or medication switching, and reported the use of pharmacokinetic modeling software for dose prediction. Some guidelines suggest minimum plasma concentrations exceeding 2.0 mg/L for severe invasive pulmonary aspergillosis or CNS involvement,19–21,62 suggesting that severe infections are associated with higher target concentrations.
Japanese guidelines suggest a target plasma concentration of 2.0–4.0 mg/L for Asian patients.25 Meta-analyses by Asian authors further reported an increased neurotoxicity risk when concentrations exceeded 4.0 mg/L.71,73 These observations likely relate to Asian CYP2C19 genetic backgrounds, particularly poor-metabolizer prevalence, potentially limiting their direct application to more diverse global cohorts. Similarly, the CPIC guideline101 noted that treatment failure or toxicity may occur even within conventional concentration ranges due to CYP2C19 genotype variations. This suggests that fixed thresholds may not fully account for individual pharmacodynamic variability. The guideline supports a framework led by CYP2C19 phenotyping and integrated with TDM, age, developmental status, hepatic and renal function, drug interactions, and infection site characteristics. This approach is intended to achieve a balance between efficacy and safety in the treatment of IA.
Clinical Utility and Pre-Emptive Screening of CYP2C19 Polymorphisms
Current mainstream aspergillosis treatment guidelines do not include routine CYP2C19 genotyping as a standard recommendation. The CPIC guideline101 describes CYP2C19 genotyping as an adjunct strategy for voriconazole therapy rather than a routine monitoring measure. In this context, treatment adjustments based on genotype results are noted for specific scenarios, such as therapeutic failure, a high risk of adverse reactions, special populations, or patients identified as ultra-rapid or poor metabolizers.
A meta-analysis102 reported the potential utility of pre-screening CYP2C19 genotypes prior to individualized voriconazole therapy, primarily for patients with invasive fungal infections, particularly within Asian populations. This study also noted the application of screening in high-risk patients requiring voriconazole prophylaxis or treatment, including those with hematologic malignancies, post-hematopoietic stem cell transplantation, or febrile neutropenia. Regarding pediatric patients, the influence of genotype on drug metabolism was reported to be potentially diminished due to more rapid hepatic metabolism, and careful evaluation was suggested for this population.
While one study suggested routine genotyping,103 such observations are often limited to specific populations or based on individual clinical experience. Mangal et al104 emphasized the importance of integrating multiple factors, including the pathogen MIC for voriconazole, the CYP2C19 phenotype, and concomitant proton pump inhibitor use, through the utilization of a PopPK model. Routine CYP2C19 genotyping is generally not described for the general patient population. Instead, it is suggested to serve as an adjunct to guide initial dosing in high-risk populations when feasible, while TDM remains the primary approach for individualized voriconazole clinical management.
Variation in Treatment Recommendations for Specific Sites of Aspergillus Infection
Multiple studies reported that pulmonary and upper respiratory tract infections constitute the largest proportion of aspergillosis sites.105–107 Voriconazole has been observed to exhibit varying tissue penetration rates across different physiological compartments.108,109 Heterogeneity in the evidence for aspergillosis treatment primarily manifests in guideline recommendations regarding treatment duration, administration routes, and surgical intervention strategies. These discrepancies reflect the diversity of clinical evidence and the contextual factors present during the development of each guideline (Table 3). Potential drivers of this heterogeneity include the timing of guideline formulation, specific target populations, advances in diagnostic technology, reliance on distinct epidemiological data, and variations in prognostic assessment metrics. Notably, current PK/PD evidence for various infection sites remains limited and is currently insufficient to support the establishment of clear or extrapolatable site-specific quantitative exposure-response thresholds.
Management Considerations for Specific Patient Populations in Aspergillosis Therapy
In the clinical management of invasive aspergillosis, precision strategies are described for specific patient populations to address varied pharmacokinetic profiles and clinical needs. For pediatric and adolescent patients aged under 12 years or weighing 50 kg or less, higher maintenance dosing regimens are noted due to increased drug clearance, with TDM suggested as early as days 2–3 of treatment.19,21 In critical care settings involving ECMO, severe hypoalbuminemia, or multiple organ dysfunction, an increased TDM frequency of every 3–4 days is described to address fluctuations in distribution volume and potential circuit adsorption. For severe infections or CNS involvement, an elevation of trough concentration targets to 2.0–6.0 mg/L is observed within these recommendations.19,21 Regarding patients with organ impairment, while renal insufficiency is typically described as not requiring direct dose reduction, monitoring for excipient accumulation is suggested. Conversely, hepatic impairment represents a clear indication for dose adjustment, with TDM noted for days 3, 7, and 14, alongside potential dose reduction or transition to alternative antifungal agents based on clinical assessment.15,21 In patients with hematologic malignancies or hematopoietic stem cell transplant recipients, continuous galactomannan monitoring is suggested to track disease progression and therapeutic response. For patients with febrile neutropenia persisting for 4–7 days, the initiation of empirical antifungal therapy is recommended.17,18,61 Additionally, for aspergilloma cases undergoing surgical intervention, the maintenance of antifungal therapy for at least 4 weeks both pre- and post-operatively is reported.18
Perspectives on Clinical Practice for Aspergillosis Management
The routine application of TDM is suggested, particularly in high-variability populations such as those in intensive care, receiving organ support therapy, or with malnutrition, to maintain effective exposure and reduce toxicity risk. While guideline-recommended trough concentration ranges serve as a reference framework, adjustments based on patient-specific factors are described. Inflammatory status, support therapy, and host immune recovery have been suggested to potentially carry more prognostic value than isolated concentration metrics.
Site-specific management involves multidisciplinary collaboration. Evidence for common sites such as the lungs is relatively sufficient, allowing for standard TDM guidance. For rare sites with lower evidence strength, awareness of penetration barriers and consideration of auxiliary interventions, such as surgery or combination regimens, are noted. Precision in dose adjustments is described in special scenarios, as exemplified by the potential benefits of higher initial doses for patients receiving CRRT, while cautious dose reductions for those with low albumin or poor metabolizer status are suggested to balance efficacy and safety.
Voriconazole exhibits non-linear pharmacokinetic characteristics (Michaelis-Menten mechanism), leading to a non-linear dose-exposure relationship and amplified individual variability. PopPK models provide reliable guidance for TDM and individualized dose adjustments by integrating multiple covariates. This approach is reported to be particularly applicable to high-risk groups, such as immunosuppressed patients, children, and those with hepatic dysfunction, helping to maintain efficacy and reduce toxicity risk.110 For populations with a high proportion of CYP2C19 poor metabolizers, a narrower target plasma concentration range is suggested to reduce the risk of adverse reactions. The decision-making process for voriconazole treatment of Aspergillosis is shown in Figure 1.
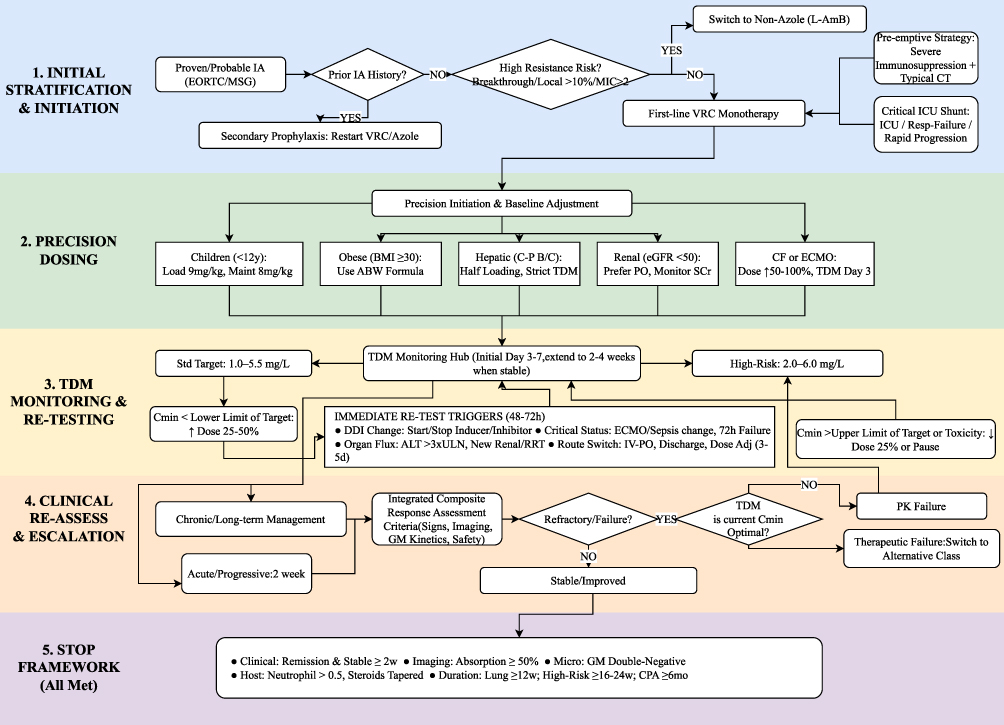 |
Figure 1 A Proposed Flow Diagram for the Management of Aspergillosis Using Voriconazole. Abbreviations: VRC, Voriconazole; TDM, Therapeutic Drug Monitoring; L-AmB, Liposomal Amphotericin B; PK, Pharmacokinetics; GM, Galactomannan. Notes: This flowchart provides a general overview based on a review of major clinical guidelines and literature. It is intended for educational and reference purposes to support the treatment of aspergillosis with Voriconazole. Treatment strategies should be individualized, taking into account patient-specific factors such as underlying conditions, comorbidities, and organ function, as well as local resistance patterns and institutional protocols. The parameters and logic described are meant to supplement, rather than replace, professional clinical judgment or the latest laboratory findings. |
Limitations
Due to the notable heterogeneity among the studies included in this review, a systematic analysis was not feasible, which may limit the precision and broad applicability of the conclusions. Current research on voriconazole for aspergillosis therapy is reported to involve mostly small sample sizes and single-center designs, with observed methodological variations and a lack of large-scale multicenter randomized controlled trials. The inclusion of patients without microbiological confirmation of aspergillosis in some studies is noted, which may influence the disease-specific relevance of the findings. Furthermore, given the marked variation in patient populations across case reports, statistical testing for the safety and efficacy of voriconazole has not been performed, and evaluation results are observed to involve a degree of subjectivity.
Future Research Directions
Refinement of resistance monitoring networks: Future efforts may focus on the expansion of genomic tools to further elucidate resistance mechanisms and transmission patterns, such as CYP51A mutations. These initiatives could provide a scientific foundation for the development of novel antifungal agents.14
Strategic development of pharmacokinetic and pharmacodynamic frameworks: Potential directions involve the establishment of comprehensive TDM protocols, the exploration of concentration thresholds within specific target tissues, and the systematic evaluation of multi-drug combination regimens.
Integration of clinical trials and modelling for diverse patient populations: Prioritizing randomized controlled trials may support the development of robust efficacy and safety models for special populations. For infection sites where sampling remains a challenge, such as the eyes or bone marrow, PopPK modelling could be leveraged to predict local drug exposure and inform the adjustment of therapeutic strategies.
Exploration of adjuvant immunotherapies and host response enhancement: Investigations into adjuvant therapies, such as IFN-gamma and other immunomodulatory agents, could focus on the regulation of cytokine and chemokine networks. These strategies represent a potential pathway to support antifungal outcomes by enhancing the host immune response.111
Conclusion
Current evidence suggests that individualized voriconazole dosing and TDM represent key components in the management of aspergillosis. Since existing target concentration ranges are primarily derived from broader invasive fungal infection populations, further validation within aspergillosis-specific cohorts remains a recognized area for clinical refinement. Individualized therapy is often associated with the integration of genetic background, infection site, and disease severity to address the complexity of host-pathogen interactions. For infections at sites with limited drug penetration, the application of site-specific strategies incorporating host factors and resistance status has been described. These approaches, combined with dose adjustment strategies and emerging immunomodulatory strategies, are suggested to potentially support clinical efficacy while limiting the risk of adverse reactions. Future high-quality research specifically targeting aspergillosis patients may further advance the development and implementation of precision antifungal therapy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by 2024 Fujian Province Science and Technology Innovation Joint Fund Project Plan (2024Y9440); Projects for Quanzhou Science and Technology Plan in 2025 (2025QZNG018); Medical education integration and open Fund projects in 2025 (2025YJRHQH11).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Gangneux J-P, Dannaoui E, Fekkar A. et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: the French multicentre MYCOVID study. Lancet Respir Med. 2022;10(2):180–19. doi:10.1016/S2213-2600(21)00442-2
2. Lu LY, Lee HM, Burke A, et al. Prevalence, Risk Factors, Clinical Features, and Outcome of Influenza-Associated Pulmonary Aspergillosis in Critically Ill Patients: a Systematic Review and Meta-Analysis. CHEST. 2024;165(3):540–558. doi:10.1016/j.chest.2023.09.019
3. Koehler P, Hamprecht A, Bader O, et al. Epidemiology of invasive aspergillosis and azole resistance in patients with acute leukaemia: the SEPIA Study. Int J Antimicrob Agents. 2017;49(2):218–223. doi:10.1016/j.ijantimicag.2016.10.019
4. Shi C, Shan Q, Xia J, et al. Incidence, risk factors and mortality of invasive pulmonary aspergillosis in patients with influenza: a systematic review and meta-analysis. Mycoses. 2022;65(2):152–163. doi:10.1111/myc.13410
5. Neofytos D, Chatzis O, Nasioudis D, et al. Epidemiology, risk factors and outcomes of invasive aspergillosis in solid organ transplant recipients in the Swiss Transplant Cohort Study. Transpl Infect Dis off J Transplant Soc. 2018;20(4):e12898. doi:10.1111/tid.12898
6. Kontoyiannis DP, Marr KA, Park BJ, et al. Prospective Surveillance for Invasive Fungal Infections in Hematopoietic Stem Cell Transplant Recipients, 2001–2006: overview of the Transplant‐Associated Infection Surveillance Network (TRANSNET) Database. Clin Infect Dis. 2010;50(8):1091–1100. doi:10.1086/651263
7. Huang L, He H, Ding Y, Jin J, Zhan Q. Values of radiological examinations for the diagnosis and prognosis of invasive bronchial-pulmonary aspergillosis in critically ill patients with chronic obstructive pulmonary diseases. Clin Respir J. 2018;12(2):499–509. doi:10.1111/crj.12551
8. Yerbanga IW, Nakanabo Diallo S, Rouamba T, et al. A systematic review of epidemiology, risk factors, diagnosis, antifungal resistance, and management of invasive aspergillosis in Africa. J Mycol Medicale. 2023;33(1):101328. doi:10.1016/j.mycmed.2022.101328
9. Denning DW. Global incidence and mortality of severe fungal disease. Lancet Infect Dis. 2024;24(7):e428–e438. doi:10.1016/S1473-3099(23)00692-8
10. Lestrade PPA, Buil JB, Van Der Beek MT, et al. Paradoxal Trends in Azole-Resistant Aspergillus fumigatus in a National Multicenter Surveillance Program, the Netherlands, 2013–2018. Emerg Infect Dis. 2020;26(7):1447–1455. doi:10.3201/eid2607.200088
11. Mayr A, Lass-Flörl C. Epidemiology and antifungal resistance in invasive aspergillosis according to primary disease - review of the literature. Eur J Med Res. 2011;16(4):153. doi:10.1186/2047-783X-16-4-153
12. Burks C, Darby A, Gómez Londoño L, Momany M, Brewer MT. Azole-resistant Aspergillus fumigatus in the environment: identifying key reservoirs and hotspots of antifungal resistance. PLOS Pathog. 2021;17(7):e1009711. doi:10.1371/journal.ppat.1009711
13. Dladla M, Gyzenhout M, Marias G, Ghosh S. Azole resistance in Aspergillus fumigatus- comprehensive review. Arch Microbiol. 2024;206(7):305. doi:10.1007/s00203-024-04026-z
14. Sen P, Vijay M, Kamboj H, Gupta L, Shankar J, Vijayaraghavan P. cyp51A mutations, protein modeling, and efflux pump gene expression reveals multifactorial complexity towards understanding Aspergillus section Nigri azole resistance mechanism. Sci Rep. 2024;14:6156. doi:10.1038/s41598-024-55237-9
15. Douglas AP, Smibert OC, Bajel A, et al. Consensus guidelines for the diagnosis and management of invasive aspergillosis, 2021. Intern Med J. 2021;51(S7):143–176. doi:10.1111/imj.15591
16. Agarwal R, Sehgal IS, Muthu V, et al. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur Respir J. 2024;63(4):2400061. doi:10.1183/13993003.00061-2024
17. Epelbaum O, Marinelli T, Haydour QS, et al. Treatment of Invasive Pulmonary Aspergillosis and Preventive and Empirical Therapy for Invasive Candidiasis in Adult Pulmonary and Critical Care Patients. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2024;211(1):34–53. doi:10.1164/rccm.202410-2045ST
18. Patterson TF, Thompson GR, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63(4):e1–e60. doi:10.1093/cid/ciw326
19. Ullmann AJ, Aguado JM, Arikan-Akdagli S, et al. Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin Microbiol Infect. 2018;24:e1–e38. doi:10.1016/j.cmi.2018.01.002
20. Warris A, Lehrnbecher T, Roilides E, Castagnola E, Brüggemann RJM, Groll AH. ESCMID-ECMM guideline: diagnosis and management of invasive aspergillosis in neonates and children. Clin Microbiol Infect off Publ Eur Soc Clin Microbiol Infect Dis. 2019;25(9):1096–1113. doi:10.1016/j.cmi.2019.05.019
21. Husain S, Camargo JF. Invasive Aspergillosis in solid‐organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33(9):e13544. doi:10.1111/ctr.13544
22. Purkins L, Wood N, Ghahramani P, Greenhalgh K, Allen MJ, Kleinermans D. Pharmacokinetics and safety of voriconazole following intravenous- to oral-dose escalation regimens. Antimicrob Agents Chemother. 2002;46(8):2546–2553. doi:10.1128/AAC.46.8.2546-2553.2002
23. Shi C, Xiao Y, Mao Y, Wu J, Lin N. Voriconazole: a Review of Population Pharmacokinetic Analyses. Clin Pharmacokinet. 2019;58(6):687–703. doi:10.1007/s40262-019-00735-7
24. Fricke-Galindo I, Céspedes-Garro C, Rodrigues-Soares F, et al. Interethnic variation of CYP2C19 alleles, “predicted” phenotypes and “measured” metabolic phenotypes across world populations. Pharmacogenomics J. 2016;16(2):113–123. doi:10.1038/tpj.2015.70
25. Takesue Y, Hanai Y, Oda K, et al. Clinical Practice Guideline for the Therapeutic Drug Monitoring of Voriconazole in Non-Asian and Asian Adult Patients: consensus Review by the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. Clin Ther. 2022;44(12):1604–1623. doi:10.1016/j.clinthera.2022.10.005
26. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
27. Neofytos D, Ostrander D, Shoham S, et al. Voriconazole therapeutic drug monitoring: results of a prematurely discontinued randomized multicenter trial. Transpl Infect Dis. 2015;17(6):831–837. doi:10.1111/tid.12454
28. Kim SH, Yim DS, Choi SM, et al. Voriconazole-related severe adverse events: clinical application of therapeutic drug monitoring in Korean patients. Int J Infect Dis. 2011;15(11):e753–e758. doi:10.1016/j.ijid.2011.06.004
29. Denning DW, Ribaud P, Milpied N, et al. Efficacy and Safety of Voriconazole in the Treatment of Acute Invasive Aspergillosis. Clin Infect Dis. 2002;34(5):563–571. doi:10.1086/324620
30. Teng GJ, Bai XR, Zhang L, Liu HJ, Nie XH. Remission of hepatotoxicity in chronic pulmonary aspergillosis patients after lowering trough concentration of voriconazole. World J Clin Cases. 2020;8(20):4700–4707. doi:10.12998/wjcc.v8.i20.4700
31. Lee YJ, Lee SO, Choi SH, et al. Initial voriconazole trough blood levels and clinical outcomes of invasive aspergillosis in patients with hematologic malignancies. Med Mycol. 2013;51(3):324–330. doi:10.3109/13693786.2012.694082
32. Yousefian S, Dastan F, Marjani M, et al. Determination of Voriconazole Plasma Concentration by HPLC Technique and Evaluating Its Association with Clinical Outcome and Adverse Effects in Patients with Invasive Aspergillosis. Can J Infect Dis Med Microbiol. 2021;2021:1–6. doi:10.1155/2021/5497427
33. Matsuda T, Koreeda Y, Mataki H, Taira T, Noma S, Higashimoto I. A case of Aspergillus empyema successfully treated with combination therapy of voriconazole and micafungin: excellent penetration of voriconazole and micafungin into pleural fluid. Intern Med Tokyo Jpn. 2010;49(12):1163–1169. doi:10.2169/internalmedicine.49.2860
34. Bennis Y, Bodeau S, Bouquié R, et al. High metabolic N-oxidation of voriconazole in a patient with refractory aspergillosis and CYP2C19*17/*17 genotype. Br J Clin Pharmacol. 2015;80(4):782–784. doi:10.1111/bcp.12713
35. Ferguson M, Randles M, De Freitas D. A suspected case of autoinduction of voriconazole metabolism in a patient with cerebral aspergillosis. Drug Healthc Patient Saf. 2017;9:89–91. doi:10.2147/DHPS.S140213
36. Martínez-Casanova J, Carballo N, Luque S, Sorli L, Grau S. Posaconazole achieves prompt recovery of voriconazole-induced liver injury in a case of invasive aspergillosis. Infect Drug Resist. 2018;11:317–321. doi:10.2147/IDR.S154457
37. Boyd NK, Zoellner CL, Swancutt MA, Bhavan KP. Utilization of Omeprazole To Augment Subtherapeutic Voriconazole Concentrations for Treatment of Aspergillus Infections. Antimicrob Agents Chemother. 2012;56(11):6001–6002. doi:10.1128/AAC.00700-12
38. Cojutti PG, Merelli M, Allegri L, Damante G, Bassetti M, Pea F. Successful and safe long‐term treatment of cerebral aspergillosis with high‐dose voriconazole guided by therapeutic drug monitoring. Br J Clin Pharmacol. 2019;85(1):266–269. doi:10.1111/bcp.13789
39. Huang J, Chen Y, Zhong M, Tan R. Case report: dose-dependent interaction between dexamethasone and voriconazole in severely ill patients with non-Hodgkin’s lymphoma being treated for invasive pulmonary aspergillosis. Front Pharmacol. 2024;15:1403966. doi:10.3389/fphar.2024.1403966
40. Mochizuki E, Furuhashi K, Fujisawa T, et al. A case of treatment with voriconazole for chronic progressive pulmonary aspergillosis in a patient receiving tacrolimus for dermatomyositis-associated interstitial lung disease. Respir Med Case Rep. 2015;16:163–165. doi:10.1016/j.rmcr.2015.10.008
41. Danion F, Jullien V, Rouzaud C, et al. Is It Time for Systematic Voriconazole Pharmacogenomic Investigation for Central Nervous System Aspergillosis? Antimicrob Agents Chemother. 2018;62(9):e00705–18. doi:10.1128/AAC.00705-18
42. Poupelin JC, Philit F, Richard JC, et al. Pericardial and pleural diffusion of voriconazole during disseminated invasive aspergillosis: report of a case with successful outcome. Intensive Care Med. 2006;32(6):939–940. doi:10.1007/s00134-006-0113-x
43. Nowak S, Bollmann T, Rosenstengel C, et al. Voriconazole as mono-therapy in orbitofrontal erosive aspergillosis without gross total resection: a case report and review of literature. Clin Neurol Neurosurg. 2018;172:93–95. doi:10.1016/j.clineuro.2018.06.043
44. Meyer M, Waldvogel S, Chalandon Y, Bongiovanni M, Pache JC, Van Delden C. Breakthrough invasive pulmonary aspergillosis despite empirical voriconazole therapy for febrile neutropenia: case report and review of the literature. Scand J Infect Dis. 2007;39(8):731–733. doi:10.1080/00365540701199857
45. Fulco PP, Beaulieu C, Higginson RT, Bearman G. Pharmacogenetic testing for the treatment of aspergillosis with voriconazole in two HIV-positive patients. Pharmacogenet Genomics. 2019;29(6):155–157. doi:10.1097/FPC.0000000000000377
46. Mathieu A, Thiboutot Z, Ferreira V, et al. Voriconazole Sequestration During Extracorporeal Membrane Oxygenation for Invasive Lung Aspergillosis: a Case Report. ASAIO J. 2022;68(3):e56–e58. doi:10.1097/MAT.0000000000001427
47. Réminiac F, Sonneville R, Massias L, Chochillon C, Wolff M. Very-High-Dose Caspofungin Combined with Voriconazole To Treat Central Nervous System Aspergillosis: substantial Penetration of Caspofungin into Cerebrospinal Fluid. Antimicrob Agents Chemother. 2014;58(6):3568–3569. doi:10.1128/AAC.02719-14
48. Gu L, Ai T, Pang L, Xu D, Wang H. Voriconazole-Induced Hepatotoxicity in a Patient with Pulmonary Aspergillosis: a Case Report. Infect Drug Resist. 2023;16:5405–5411. doi:10.2147/IDR.S419382
49. Ohashi R, Kato M, Katsura Y, et al. Breakthrough lung Scedosporium prolificans infection with multiple cavity lesions in a patient receiving voriconazole for probable invasive aspergillosis associated with monoclonal gammopathy of undetermined significance (MGUS). Nippon Ishinkin Gakkai Zasshi. 2011;52(1):33–38. doi:10.3314/jjmm.52.33
50. Schwartz S, Milatovic D, Thiel E. Successful treatment of cerebral aspergillosis with a novel triazole (voriconazole) in a patient with acute leukaemia. Br J Haematol. 1997;97(3):662–665. doi:10.1046/j.1365-2141.1997.972911.x
51. Elter T, Sieniawski M, Gossmann A, et al. Voriconazole brain tissue levels in rhinocerebral aspergillosis in a successfully treated young woman. Int J Antimicrob Agents. 2006;28(3):262–265. doi:10.1016/j.ijantimicag.2006.04.006
52. Gendrot A, De La Blanchardière A, De La Gastine B, Fromager G, Massias L, Verdon R. Neuropathie périphérique sous voriconazole au cours d’une aspergillose pulmonaire cavitaire chronique. Rev Médecine Interne. 2010;31(2):163–166. doi:10.1016/j.revmed.2009.02.021
53. Furudate A, Hirose S, Abe K, et al. Infantile Aspergillus fumigatus ventriculitis successfully treated with monitoring of plasma and cerebrospinal fluid voriconazole concentration level. J Infect Chemother. 2020;26(1):132–135. doi:10.1016/j.jiac.2019.06.011
54. Hu Q, Li Y, Zhang Y, et al. Case Report: first Report of T-Cell Large Granular Lymphocytic Leukemia With NPL-DHX9 Gene Fusion Successfully Treated With Cladribine: clinical Experience and Literature Review. Front Oncol. 2022;12:824393. doi:10.3389/fonc.2022.824393
55. Person AK, Chudgar SM, Norton BL, Tong BC, Stout JE. Aspergillus niger: an unusual cause of invasive pulmonary aspergillosis. J Med Microbiol. 2010;59(Pt 7):834–838. doi:10.1099/jmm.0.018309-0
56. Takatsuka H, Yamazaki S, Watanabe A, et al. Successful treatment of Aspergillus empyema using combined intrathoracic and intravenous administration of voriconazole: a case report. J Infect Chemother off J Jpn Soc Chemother. 2020;26(8):847–850. doi:10.1016/j.jiac.2020.03.013
57. Brüggemann RJM, Antonius T, Heijst AV, Hoogerbrugge PM, Burger DM, Warris A. Therapeutic Drug Monitoring of Voriconazole in a Child With Invasive Aspergillosis Requiring Extracorporeal Membrane Oxygenation. Ther Drug Monit. 2008;30(6):643–646. doi:10.1097/FTD.0b013e3181898b0c
58. Walsh TJ, Anaissie EJ, Denning DW, et al. Treatment of Aspergillosis: clinical Practice Guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(3):327–360. doi:10.1086/525258
59. Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016;47(1):45–68. doi:10.1183/13993003.00583-2015
60. Garcia-Vidal C, Alastruey-Izquierdo A, Aguilar-Guisado M, et al. Executive summary of clinical practice guideline for the management of invasive diseases caused by Aspergillus: 2018 Update by the GEMICOMED-SEIMC/REIPI. Enfermedades Infecc Microbiol Clínica. 2019;37(8):535–541. doi:10.1016/j.eimc.2018.03.018
61. Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021;21(6):e149–e162. doi:10.1016/S1473-3099(20)30847-1
62. Wichmann D, Hoenigl M, Koehler P, et al. Diagnosis and treatment of invasive pulmonary aspergillosis in critically ill intensive care patients: executive summary of the German national guideline (AWMF 113-005). Infection. 2025. doi:10.1007/s15010-025-02572-2
63. Chen K, Zhang X, Ke X, et al. Individualized Medication of Voriconazole: a Practice Guideline of the Division of Therapeutic Drug Monitoring, Chinese Pharmacological Society. Ther Drug Monit. 2018;40(6):663–674. doi:10.1097/FTD.0000000000000561
64. Ashbee HR, Barnes RA, Johnson EM, Richardson MD, Gorton R, Hope WW. Therapeutic drug monitoring (TDM) of antifungal agents: guidelines from the British Society for Medical Mycology. J Antimicrob Chemother. 2014;69(5):1162–1176. doi:10.1093/jac/dkt508
65. Chau MM, Daveson K, Alffenaar JC, et al. Consensus guidelines for optimising antifungal drug delivery and monitoring to avoid toxicity and improve outcomes in patients with haematological malignancy and haemopoietic stem cell transplant recipients, 2021. Intern Med J. 2021;51(S7):37–66. doi:10.1111/imj.15587
66. Wang H, Shen Y, Luo X, Jin L, Zhu H, Wang J. Population pharmacokinetics and dose optimization of voriconazole in patients with COVID-19-associated pulmonary aspergillosis. Front Pharmacol. 2025;16:1554370. doi:10.3389/fphar.2025.1554370
67. Liu P, Mould DR. Population Pharmacokinetic-Pharmacodynamic Analysis of Voriconazole and Anidulafungin in Adult Patients with Invasive Aspergillosis. Antimicrob Agents Chemother. 2014;58(8):4727–4736. doi:10.1128/AAC.02809-13
68. Duangpraphat M, Wilson RC, Rawson TM, et al. Mechanism-Based Pharmacokinetic/Pharmacodynamic Model of Voriconazole for Predicting the Clinical Outcomes of Adult Patients with Invasive Aspergillosis. Ther Drug Monit. 2024. doi:10.1097/FTD.0000000000001268
69. Chantharit P, Tantasawat M, Kasai H, Tanigawara Y. Population Pharmacokinetics of Voriconazole in Patients With Invasive Aspergillosis: serum Albumin Level as a Novel Marker for Clearance and Dosage Optimization. Ther Drug Monit. 2020;42(6):872–879. doi:10.1097/FTD.0000000000000799
70. Pascual A, Calandra T, Bolay S, Buclin T, Bille J, Marchetti O. Voriconazole Therapeutic Drug Monitoring in Patients with Invasive Mycoses Improves Efficacy and Safety Outcomes. Clin Infect Dis. 2008;46(2):201–211. doi:10.1086/524669
71. Jin H, Wang T, Falcione BA, et al. Trough concentration of voriconazole and its relationship with efficacy and safety: a systematic review and meta-analysis. J Antimicrob Chemother. 2016;71(7):1772–1785. doi:10.1093/jac/dkw045
72. Hanai Y, Hamada Y, Kimura T, et al. Favorable Effects of Voriconazole Trough Concentrations Exceeding 1 μg/mL on Treatment Success and All-Cause Mortality: a Systematic Review and Meta-Analysis. J Fungi. 2021;7(4):4. doi:10.3390/jof7040306
73. Hamada Y, Seto Y, Yago K, Kuroyama M. Investigation and threshold of optimum blood concentration of voriconazole: a descriptive statistical meta-analysis. J Infect Chemother. 2012;18(4):501–507. doi:10.1007/s10156-011-0363-6
74. Luong ML, Al-Dabbagh M, Groll AH, et al. Utility of voriconazole therapeutic drug monitoring: a meta-analysis. J Antimicrob Chemother. 2016;71(7):1786–1799. doi:10.1093/jac/dkw099
75. Rudramurthy SM, Seyedmousavi S, Dhaliwal M, Chakrabarti A, Meis JF, Mouton JW. Pharmacodynamics of Voriconazole against Wild-Type and Azole-Resistant Aspergillus flavus Isolates in a Nonneutropenic Murine Model of Disseminated Aspergillosis. Antimicrob Agents Chemother. 2017;61(1):e01491–16. doi:10.1128/AAC.01491-16
76. Mavridou E, Bruggemann RJM, Melchers WJG, Verweij PE, Mouton JW. Impact of cyp51A mutations on the pharmacokinetic and pharmacodynamic properties of voriconazole in a murine model of disseminated aspergillosis. Antimicrob Agents Chemother. 2010;54(11):4758–4764. doi:10.1128/AAC.00606-10
77. Seyedmousavi S, Brüggemann RJM, Melchers WJG, Rijs AJMM, Verweij PE, Mouton JW. Efficacy and pharmacodynamics of voriconazole combined with anidulafungin in azole-resistant invasive aspergillosis. J Antimicrob Chemother. 2013;68(2):385–393. doi:10.1093/jac/dks402
78. Troke PF, Hockey HP, Hope WW. Observational study of the clinical efficacy of voriconazole and its relationship to plasma concentrations in patients. Antimicrob Agents Chemother. 2011;55(10):4782–4788. doi:10.1128/AAC.01083-10
79. Park WB, Kim NH, Kim KH, et al. The effect of therapeutic drug monitoring on safety and efficacy of voriconazole in invasive fungal infections: a randomized controlled trial. Clin Infect Dis off Publ Infect Dis Soc Am. 2012;55(8):1080–1087. doi:10.1093/cid/cis599
80. Pascual A, Csajka C, Buclin T, et al. Challenging Recommended Oral and Intravenous Voriconazole Doses for Improved Efficacy and Safety: population Pharmacokinetics–Based Analysis of Adult Patients With Invasive Fungal Infections. Clin Infect Dis. 2012;55(3):381–390. doi:10.1093/cid/cis437
81. Dolton MJ, Ray JE, Chen SCA, Ng K, Pont LG, McLachlan AJ. Multicenter Study of Voriconazole Pharmacokinetics and Therapeutic Drug Monitoring. Antimicrob Agents Chemother. 2012;56(9):4793–4799. doi:10.1128/AAC.00626-12
82. Tan K, Brayshaw N, Tomaszewski K, Troke P, Wood N. Investigation of the Potential Relationships Between Plasma Voriconazole Concentrations and Visual Adverse Events or Liver Function Test Abnormalities. J Clin Pharmacol. 2006;46(2):235–243. doi:10.1177/0091270005283837
83. Veringa A, Brüggemann RJ, Span LFR, et al. Therapeutic drug monitoring-guided treatment versus standard dosing of voriconazole for invasive aspergillosis in haematological patients: a multicentre, prospective, cluster randomised, crossover clinical trial. Int J Antimicrob Agents. 2023;61(2):106711. doi:10.1016/j.ijantimicag.2023.106711
84. Ueda K, Nannya Y, Kumano K, et al. Monitoring trough concentration of voriconazole is important to ensure successful antifungal therapy and to avoid hepatic damage in patients with hematological disorders. Int J Hematol. 2009;89(5):592–599. doi:10.1007/s12185-009-0296-3
85. Lestrade PPA, Meis JF, Melchers WJG, Verweij PE. Triazole resistance in Aspergillus fumigatus: recent insights and challenges for patient management. Clin Microbiol Infect off Publ Eur Soc Clin Microbiol Infect Dis. 2019;25(7):799–806. doi:10.1016/j.cmi.2018.11.027
86. Slaven JW, Anderson MJ, Sanglard D, et al. Increased expression of a novel Aspergillus fumigatus ABC transporter gene, atrF, in the presence of itraconazole in an itraconazole resistant clinical isolate. Fungal Genet Biol FG B. 2002;36(3):199–206. doi:10.1016/s1087-1845(02)00016-6
87. Mellado E, Garcia-Effron G, Alcázar-Fuoli L, et al. A new Aspergillus fumigatus resistance mechanism conferring in vitro cross-resistance to azole antifungals involves a combination of cyp51A alterations. Antimicrob Agents Chemother. 2007;51(6):1897–1904. doi:10.1128/AAC.01092-06
88. Chowdhary A, Sharma C, Kathuria S, Hagen F, Meis JF. Azole-resistant Aspergillus fumigatus with the environmental TR46/Y121F/T289A mutation in India. J Antimicrob Chemother. 2014;69(2):555–557. doi:10.1093/jac/dkt397
89. Diaz-Guerra TM, Mellado E, Cuenca-Estrella M, Rodriguez-Tudela JL. A point mutation in the 14alpha-sterol demethylase gene cyp51A contributes to itraconazole resistance in Aspergillus fumigatus. Antimicrob Agents Chemother. 2003;47(3):1120–1124. doi:10.1128/AAC.47.3.1120-1124.2003
90. Krishnan Natesan S, Wu W, Cutright JL, Chandrasekar PH. In vitro-in vivo correlation of voriconazole resistance due to G448S mutation (cyp51A gene) in Aspergillus fumigatus. Diagn Microbiol Infect Dis. 2012;74(3):272–277. doi:10.1016/j.diagmicrobio.2012.06.030
91. Fraczek MG, Bromley M, Buied A, et al. The cdr1B efflux transporter is associated with non-cyp51a-mediated itraconazole resistance in Aspergillus fumigatus. J Antimicrob Chemother. 2013;68(7):1486–1496. doi:10.1093/jac/dkt075
92. Camps SMT, Dutilh BE, Arendrup MC, et al. Discovery of a HapE mutation that causes azole resistance in Aspergillus fumigatus through whole genome sequencing and sexual crossing. PLoS One. 2012;7(11):e50034. doi:10.1371/journal.pone.0050034
93. Hagiwara D, Arai T, Takahashi H, Kusuya Y, Watanabe A, Kamei K. Non-cyp51A Azole-Resistant Aspergillus fumigatus Isolates with Mutation in HMG-CoA Reductase. Emerg Infect Dis. 2018;24(10):1889–1897. doi:10.3201/eid2410.180730
94. Dos Reis TF, Silva LP, de Castro PA, et al. The Influence of Genetic Stability on Aspergillus fumigatus Virulence and Azole Resistance. G3 Bethesda Md. 2018;8(1):265–278. doi:10.1534/g3.117.300265
95. Dos Reis TF, Silva LP, de Castro PA, et al. The Aspergillus fumigatus Mismatch Repair MSH2 Homolog Is Important for Virulence and Azole Resistance. mSphere. 2019;4(4):e00416–19. doi:10.1128/mSphere.00416-19
96. Snelders E, Huis Int Veld RAG, Rijs AJMM, Kema GHJ, Melchers WJG, Verweij PE. Possible environmental origin of resistance of Aspergillus fumigatus to medical triazoles. Appl Environ Microbiol. 2009;75(12):4053–4057. doi:10.1128/AEM.00231-09
97. Lestrade PP, Bentvelsen RG, Schauwvlieghe AFAD, et al. Voriconazole Resistance and Mortality in Invasive Aspergillosis: a Multicenter Retrospective Cohort Study. Clin Infect Dis. 2019;68(9):1463–1471. doi:10.1093/cid/ciy859
98. Uluç K, Özçelik HK, Öngel EA, et al. The Prevalence of Multidrug-Resistant and Extensively Drug-Resistant Infections in Respiratory Intensive Care Unit, Causative Microorganisms and Mortality. Infect Drug Resist. 2024;17:4913–4919. doi:10.2147/IDR.S480829
99. Li X, Hu Q, Xu T. Associated factors with voriconazole plasma concentration: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1368274. doi:10.3389/fphar.2024.1368274
100. Hanai Y, Hamada Y, Kimura T, et al. Optimal trough concentration of voriconazole with therapeutic drug monitoring in children: a systematic review and meta-analysis. J Infect Chemother. 2021;27(2):151–160. doi:10.1016/j.jiac.2020.11.014
101. Moriyama B, Owusu Obeng A, Barbarino J, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for CYP2C19 and Voriconazole Therapy. Clin Pharmacol Ther. 2017;102(1):45–51. doi:10.1002/cpt.583
102. Zhang Y, Hou K, Liu F, et al. The influence of CYP2C19 polymorphisms on voriconazole trough concentrations: systematic review and meta-analysis. Mycoses. 2021;64(8):860–873. doi:10.1111/myc.13293
103. Katada Y, Hira D, Umemura K, et al. CYP2C19-Guided Voriconazole Therapy: a Precision Medicine Approach to Mitigate Adverse Effects in Japanese Patients. Clin Transl Sci. 2025;18(8):e70317. doi:10.1111/cts.70317
104. Mangal N, Hamadeh IS, Arwood MJ, et al. Optimization of Voriconazole Therapy for the Treatment of Invasive Fungal Infections in Adults. Clin Pharmacol Ther. 2018;104(5):957–965. doi:10.1002/cpt.1012
105. Khan S, Bilal H, Shafiq M, et al. Distribution of Aspergillus species and risk factors for aspergillosis in mainland China: a systematic review. Therapeutic Advances in Infectious Disease. 2024;11:20499361241252537. doi:10.1177/20499361241252537
106. Bertin-Biasutto L, Paccoud O, Garcia-Hermoso D, et al. Features of Invasive Aspergillosis Caused by Aspergillus flavus, France, 2012–2018. Emerg Infect Dis J. 2025;31(5):241392. doi:10.3201/eid3105.241392
107. Rudramurthy SM, Paul RA, Chakrabarti A, et al. Invasive Aspergillosis by Aspergillus flavus: epidemiology, Diagnosis, Antifungal Resistance, and Management. J Fungi. 2019;5(3):55. doi:10.3390/jof5030055
108. Weiler S, Fiegl D, MacFarland R, et al. Human Tissue Distribution of Voriconazole. Antimicrob Agents Chemother. 2011;55(2):925–928. doi:10.1128/AAC.00949-10
109. Felton T, Troke PF, Hope WW. Tissue penetration of antifungal agents. Clin Microbiol Rev. 2014;27(1):68–88. doi:10.1128/CMR.00046-13
110. Dolton MJ, Mikus G, Weiss J, Ray JE, McLachlan AJ. Understanding variability with voriconazole using a population pharmacokinetic approach: implications for optimal dosing. J Antimicrob Chemother. 2014;69(6):1633–1641. doi:10.1093/jac/dku031
111. Shankar J, Thakur R, Clemons KV, et al. Interplay of Cytokines and Chemokines in Aspergillosis. J Fungi. 2024;10(4). doi:10.3390/jof10040251
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.