Back to Journals » Clinical Ophthalmology » Volume 17
Cumulative Dissipated Energy (CDE) in Three Phaco-Fragmentation Techniques for Dense Cataract Removal
Authors Fernández-Muñoz E, Chávez-Romero Y, Rivero-Gómez R, Aridjis R, Gonzalez-Salinas R ![]()
Received 7 March 2023
Accepted for publication 27 July 2023
Published 16 August 2023 Volume 2023:17 Pages 2405—2412
DOI https://doi.org/10.2147/OPTH.S407705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Erika Fernández-Muñoz,1,* Yolanda Chávez-Romero,1,* Ricardo Rivero-Gómez,1,* Rebeca Aridjis,2,* Roberto Gonzalez-Salinas1,*
1Anterior Segment Surgery Department. Asociación para Evitar la Ceguera en México I.A.P., Mexico City, Mexico; 2LaSalle School of Medicine, Mexico City, Mexico
*These authors contributed equally to this work
Correspondence: Erika Fernández-Muñoz, Anterior Segment Surgery Department, Asociación para Evitar la Ceguera en México I.A.P, Vicente García Torres 46, Barrio San Lucas, Coyoacán, PO. 04030, Mexico City, Mexico, Tel +52 55 10841400, Ext 1144, Email [email protected]
Purpose: To determine the energy expenditure in phacoemulsification surgery expressed as cumulative dissipated energy (CDE) among the divide and conquer, ultrachopper-assisted divide and conquer, and phaco-chop techniques for dense cataract removal.
Patients and Methods: The clinical data were obtained from the medical charts of dense cataracts patients undergoing routine phacoemulsification employing any of three phaco-fragmentation techniques, including divide and conquer using the Kelman 0.9 mm tip, the ultrachopper tip, and the phaco-chop technique using the Kelman 0.9 mm tip. Cumulated dissipated energy (CDE), longitudinal ultrasound time (UST), and endothelial cell loss were compared among groups at the one-month postoperative.
Results: Surgeries from 90 eyes were analyzed, among whom the conventional divide-and-conquer technique group included 30 patients, 32 in the ultrachopper group, and 28 in the phaco-chop technique group. The average CDE in the conventional divide and conquer group was 44.52 ± 23.00, the ultrachopper technique was 43.27 ± 23.18, and 20.11 ± 11.06 in the phaco-chop group. Phaco-fragmentation chop demonstrated significantly lower CDE than the other techniques (p= < 0.0001). The phaco-chop technique showed statistically significantly lower CDE when compared to the other two groups (p=< 0.0001) with 93.96 ± 39.71 seconds. There were no statistically significant differences in postoperative endothelial cell density between groups (p=0.4916).
Conclusion: The use of the phaco-chop technique in hard cataract phacoemulsification represents a lower energy expenditure than divide and conquer and ultrachopper techniques; nevertheless, no differences regarding endothelial density loss were evidenced.
Keywords: dense cataracts, ultrachopper, phaco-chop, stop-and-chop technique, divide-and-conquer technique, cumulative dissipated energy
Introduction
Phacoemulsification is the most prevalent technique for cataract removal worldwide, demonstrating high standards for efficiency and patient safety.1 Currently, the employment of various phacoemulsification and phaco-fragmentation techniques may contribute to lower energy use and, therefore, less endothelial cell injury due to the amount of ultrasound energy dispensed. Cumulative dissipated energy (CDE) is the total amount of energy expended in the phacoemulsification, expressed in units, calculated using the following equation: CDE = mean phaco power x phaco time.1 Dense cataracts often require more energy for their removal, which has potential implications for corneal endothelial cell loss. The amount of CDE dispensed will depend on various parameters, including lens density, the fragmentation technique, and the surgeon’s experience. Reducing expenditure during phaco-fragmentation and emulsification is one of the main concerns during cataract surgery.2 A higher CDE count has been associated with increased damage to intraocular structures, particularly the corneal endothelium.3,4 Technologic improvement developed to reduce CDE, fluidics, and aspiration time during phacoemulsification.1 Loss of endothelial cells during conventional phacoemulsification has been reported between 4 to 25% for regular nuclei, increasing for hard nuclei up to 42% approximately.5,6
Several techniques have been described to optimize CDE expenditure during the nucleus phacoemulsification, including phaco-chop and divide and conquer.7–12 The Ultrachopper is a modification of the standard phacoemulsification handpiece tip, characterized by a flattened handpiece including a mild downward angulation and two laterally placed aspiration ports. The main purpose of this modification is to assist nucleus phaco-fragmentation the nucleus for dense cataracts.12
The purpose of this study aims to compare the total amount of US energy dispensed employing three phaco-fragmentation techniques: 1. The conventional divide and conquer using the 0.9 mm tip, 2. The ultrasound-knife-assisted (ultrachopper) phaco-fragmentation and the horizontal phaco-chop techniques in terms of energy expenditure and loss of endothelial density.
Materials and Methods
A retrospective study was carried out from 2017 to date at the Anterior Segment Surgery Department, Asociación para Evitar la Ceguera en México I.A.P. in Mexico City, Mexico. The Internal Review Board approved this study, which was conducted following the tenets of the Declaration of Helsinki and Good Clinical Practices Guidelines. We reviewed 90 medical charts of patients who underwent phacoemulsification in our clinic employing the following techniques: divide and conquer with Kelman 0.9 mm phaco tip, divide and conquer with Ultrachopper tip, and phaco chop with Kelman 0.9mm phaco tip. Also, due to the retrospective nature of the review, all retrieved data was anonymized and maintained with confidentiality to enforce the privacy of the participants.
Patients
Key inclusion criteria were patients with dense cataracts (≥ NO4 cataracts according to LOCS III), older than 40 of both genders. We excluded syndromes, poor pupil dilation, angle-closure glaucoma, history of uveitis, ocular trauma, previous intraocular surgery, corneal dystrophies or scarring, and endothelial cell count lower than 1000 cells/mm2 from the analysis.
Surgical Technique
For the phacoemulsification procedure, the Infiniti platform was used for all cases (Infiniti TM Vision System, Alcon Laboratories). The divide and conquer technique was performed using the 0.9 mm 45° Kelman phaco tip, as depicted in Figure 1. The ultrachopper tip was employed in the second group, as shown in Figure 2. In both divide and conquer techniques, longitudinal linear ultrasound at 50% power, 80 mmHg vacuum, 25 cc/min aspiration flow, and 80 cm bottle height were used to accomplish the four-quadrant fracture. For the phaco-chop technique, we used the 0.9 mm 45° Kelman tip, and the parameters employed were: ultrasound of 50% power, at 50 pulses per second with 50% work cycle, 400 mm/Hg vacuum, and aspiration flow of 40cc per minute with a bottle height of 100 cm. The phaco-chop technique is described in Figure 3.
 |
Figure 1 (A) Nucleus disassembly is achieved by sculpting grooves with the phaco probe and cracking the lens into four quadrants. After the nucleus is divided into two, the second instrument spins the lens 90 degrees, suitably placing the lens to create the subsequent groove. (B) Groove carving lateral view. The groove must ideally be at least 1.5 times as wide as the phaco-tip to facilitate adequate nucleus disassembly. |
 |
Figure 2 (A) The ultrachopper phaco-tip was employed to achieve two perpendicular slim grooves in the nucleus allowing four quadrant formation. (B) Lateral view of the nucleus groove sculpting employing the ultrachopper. |
 |
Figure 3 (A) In the phaco chop technique, ultrasound was applied with the 0.9 mm 45° Kelman to penetrate the nucleus. (B) Lateral view of the horizontal mechanical chop performed, obtaining two halves. |
Outcome Measurement
Ultrasound Time (UT) and CDE were registered for all techniques when the four nuclear quadrants were obtained. For nuclear removal, torsional linear continuous ultrasound with 100% power, 350 mmHg vacuum, aspiration flow of 35 cc/min, and bottle height of 100 cm were used in the three groups. Final UT was registered, as well as the CDE. Endothelial cell count was measured and registered previous to the surgical procedure and one month afterward.
Statistical Analysis
Continuous and categorical variables were shown as standard deviation and percentages, respectively. According to data distribution, the differences between the continuous variables were evaluated using a t-test or the Wilcoxon test. Also, we employed Pearson’s correlation coefficient to establish an association between the variables. One-way ANOVA test for repeated measures, Friedman test will be used depending on the data distribution. The distribution of the variables was assessed employing the Shapiro–Wilk test.
Results
We analyzed 90 eyes that underwent cataract phacoemulsification with intraocular lens implants. Thirty eyes in the conventional divide and conquer technique (Kelman 45o tip), 32 in divide and conquer with ultrachopper, and 28 in the phaco chop group. There were 46 right and 44 left eyes; 53% of patients were female. The mean age was 71.31 (range 52–86), as depicted in Table 1. The mean initial best-corrected visual acuity (BCVA) was 1.38 logMAR in the conventional divide and conquer group, 1.31 logMAR in the ultrachopper group, and 1.32 logMAR in the phaco chop group. Mean BCVA after the surgical procedure was 0.17 logMAR, 0.25 logMAR, and 0.18 logMAR for the phaco chop, ultrachopper, and conventional divide and conquer techniques, respectively.
 |
Table 1 Demographic Features |
The mean CDE was 20.11 ± 11.06, 43.27 ± 23.18, and 44.52 ± 23.00 in the phaco chop, ultrachopper, and divide and conquer groups, respectively. There was a statistically significant difference (p = <0.0001) in the amount of CDE in the phaco chop group, as depicted in Figure 4.
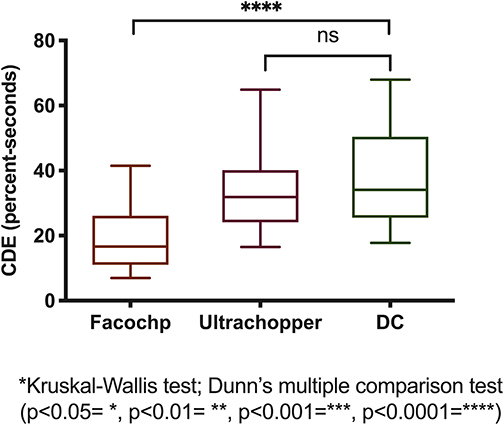 |
Figure 4 CDE comparison among groups. (Kruskal–Wallis test and Dunn’s multiple comparison; p<0.0001=****). Abbreviation: ns, non-significant. |
Regarding ultrasound time, the phaco chop group evidenced a statistically significant less time compared to the other groups (93.96 ± 39.71 seconds; p = 0.0085). The ultrachopper group depicted 132.9 ± 49.52 and 132.59 ± 59.26 for the divide and conquer group, as shown in Figure 5.
 |
Figure 5 Total USG comparison among groups. (Kruskal–Wallis test and Dunn’s multiple comparison; p<0.01= **). Abbreviation: ns, non-significant. |
The preoperative endothelial count was 2290 ± 661.8 cells/mm2, 2119 ± 387.6 cells/mm2, and 2369 ± 375.5 cells/mm2 for the phaco chop, ultrachopper, and divide and conquer, respectively (Table 2). The postoperative endothelial count was 1396 ± 455.8 cells/mm2, 1334 ± 504.5 cells/mm2, and 1512 ± 498.9 cells/mm2 for the divide and conquer, ultrachopper, and phaco chop groups, respectively, Table 2. As for endothelial cell loss, there was no statistically significant difference among groups (p = 0.4916). The phaco chop group had an endothelial cell loss of 729.3 ± 499.3 cells/mm2, the ultrachopper group had 714.9 ± 461.9 cells/mm2, and the divide and conquer group had a cell loss of 877.5 ± 351.5 cells/mm2 (Table 2). The main endothelial cell loss count in this study was 35%.
 |
Table 2 CDE, Endothelial Cell Loss, and US Time |
Discussion
Fragmentation of dense nucleus in four quadrants is the most challenging step in hard cataract surgery through a micro-incision.7,8 The phaco chop technique is considered one of the best for dealing with hard cataracts; also, a lower CDE expenditure has been described compared to other surgical techniques.8–12 In our study, we aimed to compare the total energy expenditure delivered to intraocular tissues, employing three different phaco-fracture techniques for dense nucleus.
The main finding in our study was a statistically significant difference in the CDE expenditure among the included techniques, showing downright lesser values compared to the ultrachopper and the conventional divide and conquer technique. This finding is in concordance with previously reported data by Park et al.13 They compared CDE expenditure, total ultrasound time, and endothelial cell loss employing three fracture techniques: phaco chop, stop-and-chop, and divide-and-conquer in NO2, NO3, and NO4 cataracts according to LOCS III. They reported statistically significantly lesser CDE values and ultrasound time when employing the phaco-chop technique; nonetheless, this applied only to NO4 cataracts. It is worth mentioning that the main CDE and total US time measured in our study differed from that reported by Park.8 This can be partially explained due to the inclusion of denser cataracts in our study, a common occurrence in our elderly population. Moreover, in a recent study in our hospital by Gonzalez-Salinas et al, they compared two phacoemulsification platforms (Infinity vs Centurion), reporting lesser CDE values for NO2 and NO3 cataracts according to the LOCS II classification system.1 Nonetheless, similar CDE values were reported for NO4 and NO5 cataracts compared to our study. Also, the endothelial cell count after surgery was comparable as well. This suggests that, in our population, denser cataracts often undergo phacoemulsification surgery, and therefore, increased CDE values and ultrasound time can be observed. In addition, the ultrasound time was also significantly lesser within the phaco-chop group compared to the divide and conquer and ultrachopper groups. Several reports have described similar ultrasound time measurements.12–14 In a recent study, Parkash8 reported lesser ultrasound time, even though the main part of the included patients had mild to moderate nucleus density.14 Also, other reports have also suggested that the ultrachopper tip helps chop the nucleus while maintaining wound temperature in lower estimates.12 Nonetheless, no reports compare energy expenditure between ultrachopper and other techniques, including dense cataracts.
On the other hand, we found no statistically significant difference in endothelial cell loss among these groups. This finding contrasts with previously reported data by Park.13, Which conversely suggests that increased levels of CDE and ultrasound time are not the only factors associated with endothelial cell injury. Other factors can decisively contribute to decreasing postoperative endothelial cell loss, such as fluidics and instrument manipulation within the anterior chamber.15,16 Also, other variables have been described to contribute to reducing the endothelial cell count postoperatively, including the anterior chamber depth, axial length, and intraocular lens design and location. In this regard, Khalid17–21 measured the impact of such factors on endothelial injury after a phacoemulsification procedure and suggested that the phaco-chop technique is superior in energy efficiency. In addition, Fernández compared endothelial cell loss between diabetic and nondiabetic patients undergoing cataract surgery, employing the phaco-chop technique, describing a similar mean postoperative endothelial cell count in the nondiabetic group.18 Moreover, Ganesan compared the endothelial cell damage in diabetic and nondiabetic patients during phacoemulsification, suggesting that in addition to the risk mentioned above factors, postoperative inflammation also constitutes a significant risk factor for endothelial cell injury in diabetics.19
Our study failed to find a statistically significant difference among groups regarding postoperative endothelial cell loss. Nonetheless, the ultrachopper group demonstrated a slightly non-significant lower endothelial cell loss than the other two groups. Furthermore, we consider it a safe and downright useful tool since it allows comfortable manipulation and requires a fairly low learning curve to manage a hard nucleus adequately, which is in accordance with a previously reported study conducted by Barlow et al, assessing the security and efficacy using the ultrachopper tip.12
Several limitations of this study should be considered. First, studies of retrospective nature made it challenging to gather complete information from medical records, leaving some variables of interest lacking from proper assessment. Secondly, all procedures were not performed by the same surgeon; nonetheless, all surgeries were performed by attending surgeons with experience managing dense cataract cases. Finally, we assessed the endothelial cell loss for at least six months after surgery; nevertheless, other key related variables, including the variability coefficient, further evaluating the impact of the cell injury in the corneal endothelium with each technique were not considered.
Conclusion
In our study, the CDE and the ultrasound time were significantly lower, employing the phaco chop technique compared to divide and conquer and ultrachopper techniques. However, this difference did not translate into a significant postoperative endothelial cell loss favoring any single approach. These findings suggest that the included techniques constitute a valid approach to dense cataracts. Nonetheless, the phaco chop technique produced fewer CDE counts and ultrasound time.
Ethics Approval
All procedures performed in studies involving data from human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent for Publication
As this work is a retrospective study, informed consent was not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgement
We acknowledge the valuable contribution of Fatima Rubio-Tijerina MD, in providing assistance for the figure and diagram elaboration.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this work.
Disclosure
Dr. Gonzalez-Salinas reports fees for Research from LayerBio Inc. The other authors declare no conflicts of interest in this work.
References
1. Gonzalez-Salinas R, Garza-Leon M, Saenz-de-Viteri M, Solis-S JC, Gulias-Cañizo R, Quiroz-Mercado H. Comparison of cumulative dissipated energy delivered by active-fluidic pressure control phacoemulsification system versus gravity-fluidics. Int Ophthalmol. 2017. doi:10.1007/s10792-017-0674-4
2. Shajari M, Rusev V, Mayer W, Diakonis V, Petermann K, Kohnen T. Impact of lens density and lens thickness on cumulative dissipated energy in femtosecond laser-assisted cataract surgery. Lasers Med Sci. 2019;34:1229–1234. doi:10.1007/s10103-019-02715-6
3. Pérez JM, Ibanez BB, Valero SO. Association of cumulative dissipated energy and postoperative foveal thickness among patients with age-related cataract who underwent uncomplicated phacoemulsification. Philipp J Ophthalmol. 2016;41:50–55.
4. Mahdy MA, Eid MZ, Mohammed MA, Hafez A, Bhatia J. Relationship between endothelial cell loss and microcoaxial phacoemulsification parameters in noncomplicated cataract surgery. Clin Ophthalmol. 2012. doi:10.2147/opth.s29865
5. Mencucci R, Ponchietti C, Virgili G, Giansanti F, Menchini U. Corneal endothelial damage after cataract surgery: microincision versus standard technique. J Cataract Refract Surg. 2006;32:1351–1354. doi:10.1016/j.jcrs.2006.02.070
6. Kim EC, Byun YS, Kim MS. Microincision versus small-incision coaxial cataract surgery using different power modes for hard nuclear cataract. J Cataract Refract Surg. 2011;37:1799–1805. doi:10.1016/j.jcrs.2011.04.024
7. Chen D, Tang Q, Yu F, Cai X, Lu F. Consecutive drilling combined with phaco chop for full thickness segmentation of very hard nucleus in coaxial microincisional cataract surgery. BMC Ophthalmol. 2019;19(1):20. doi:10.1186/s12886-019-1033-1
8. Zhao YE, Li Z, Chang P, Wang D, Hu M. Progressive cracking technique for phacoemulsification of superhard cataracts: a case report. Eye Vis. 2019;6:35. doi:10.1186/s40662-019-0163-0
9. Rao A, Sahay P, Das G, Sarangi S, Padhy D. Scoop and chop - A modified phaco-chop technique for pseudoexfoliation and cataract. Oman J Ophthalmol. 2020;13(2):57–62. doi:10.1186/s40662-019-0163-0
10. Coppola M, Marchese A, Rabiolo A, Cicinelli MV, Knutsson KA. Comparison of two popular nuclear disassembly techniques for cataract surgeons in training: divide and conquer versus stop and chop. Int Ophthalmol. 2019;39(9):2097–2102. doi:10.1007/s10792-018-1046-4
11. Escaf LJ, Londoño J, Melo LM. RE: ultrachopper tip. Can J Ophthalmol. 2014;49(3):307. doi:10.1016/j.jcjo.2014.03.017
12. Barlow WR, Pettey J, Olson RJ. The Ultrachopper tip: a wound temperature study. Can J Ophthalmol. 2013;6:512–515. doi:10.1016/j.jcjo.2013.05.007
13. Park J, Yum HR, Kim MS, Harrison AR, Kim EC. Comparison of phaco-chop, divide-and-conquer, and stop-and-chop phaco techniques in microincision coaxial cataract surgery. J Cataract Refract Surg. 2013;39(10):1463–1469. doi:10.1016/j.jcrs.2013.04.033
14. Om Parkash R, Mahajan S, Om Parkash T, Vajpayee RB, Om Parkash T. A rapid technique for en masse soft cataract phacoemulsification. Clin Ophthalmol. 2019;13:755–762. doi:10.2147/OPTH.S197359
15. Mayali H, Baser EF, Kurt E, Ilker SS. Corneal endothelial damage in phacoemulsification using an anterior chamber maintainer compared with using an ophthalmic viscosurgical device. J Cataract Refract Surg. 2021;47(5):612–617. doi:10.1097/j.jcrs.0000000000000493
16. Kunishige T, Takahashi H. Effects of combinations of ophthalmic viscosurgical devices and suction flow rates on the corneal endothelial cell damage incurred during phacoemulsification. J Ophthalmol. 2020;2020:2159363. doi:10.1155/2020/2159363
17. Khalid M, Ameen SS, Ayub N, Mehboob MA. Effects of anterior chamber depth and axial length on corneal endothelial cell density after phacoemulsification. Pak J Med Sci. 2019;35(1):200–204. doi:10.12669/pjms.35.1.92
18. Fernández-Muñoz E, Zamora-Ortiz R, Gonzalez-Salinas R. Endothelial cell density changes in diabetic and nondiabetic eyes undergoing phacoemulsification employing phaco-chop technique. Int Ophthalmol. 2019;39(8):1735–1741. doi:10.1007/s10792-018-0995-y
19. Ganesan N, Srinivasan R, Babu KR, Vallinayagam M. Risk factors for endothelial cell damage in diabetics after phacoemulsification. Oman J Ophthalmol. 2019;12(2):94–98. doi:10.4103/ojo.OJO_200_2017
20. Chen M, Anderson E, Hill G, Chen JJ, Patrianakos T. Comparison of cumulative dissipated energy between the Infiniti and Centurion phacoemulsification systems. Clin Ophthalmol. 2015;9:1367–1372. doi:10.2147/OPTH.S88225
21. Solomon KD, Lorente R, Fanney D, Cionni RJ. Clinical study using a new phacoemulsification system with surgical intraocular pressure control. J Cataract Refract Surg. 2016;42:542–549. doi:10.1016/j.jcrs.2016.01.03723456789
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.