Back to Journals » Infection and Drug Resistance » Volume 19
Culture-Confirmed Severe Methicillin-Susceptible Staphylococcus aureus Pneumonia with Lung Abscess, Bacteremia, and Hydropneumothorax Managed without ECMO: A Case Report
Authors Li X, Zhu Y ![]() , Huang F, Jiang Y, Zhou L
, Huang F, Jiang Y, Zhou L
Received 13 May 2026
Accepted for publication 29 June 2026
Published 10 July 2026 Volume 2026:19 624501
DOI https://doi.org/10.2147/IDR.S624501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Xuqin Li,1,* Yue Zhu,2,* Fangfang Huang,1 Yunlong Jiang,1 Li Zhou1
1Department of Nursing, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 2Department of Critical Care Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fangfang Huang, Department of Nursing, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China, Email [email protected]
Background: Methicillin-susceptible Staphylococcus aureus (MSSA) can cause rapidly destructive pneumonia complicated by lung abscess, bacteremia, empyema, and hydropneumothorax. Extracorporeal membrane oxygenation (ECMO) may be considered for refractory hypoxemia but is not always feasible. We report a young adult with severe MSSA pneumonia who recovered with optimized conventional support without ECMO.
Case Presentation: A 36-year-old man presented with fever, melena, hemoptysis, and progressive dyspnea. He developed severe hypoxemic respiratory failure with a PaO2/FiO2 ratio of 75 mmHg, septic shock requiring high-dose vasopressors, and extensive purulent airway secretions. ECMO was considered but declined for financial reasons. Immediate modified prone positioning was initiated through a rapid emergency-to-ICU workflow, and bronchoscopy performed in the prone position removed large volumes of purulent secretions. Computed tomography later showed right hydropneumothorax with approximately 60% lung compression and partial right lung destruction, as well as left pneumothorax with approximately 30% compression. Bilateral chest tubes were inserted with continuous negative-pressure drainage. Repeated early blood and sputum cultures grew Staphylococcus aureus, and oxacillin susceptibility with negative cefoxitin screening confirmed MSSA bacteremia and pneumonia. Antimicrobial therapy was dynamically adjusted according to microbiological results, including later isolation of carbapenem-resistant Acinetobacter baumannii and Klebsiella pneumoniae. Lesion-guided multi-segmental postural drainage was individualized according to imaging findings, air leakage, and drainage characteristics. The patient gradually improved, was weaned from mechanical ventilation, decannulated, and discharged on hospital day 80 with good functional recovery at follow-up.
Conclusion: Fulminant MSSA pneumonia with lung abscess, bacteremia, and bilateral hydropneumothorax may be managed without ECMO in selected patients when rapid, coordinated conventional support and source-control measures are feasible. Early prone positioning, timely pleural drainage, individualized postural drainage, dynamic antimicrobial adjustment, and stepwise rehabilitation may provide a feasible multimodal approach when advanced support is unavailable.
Keywords: Methicillin-susceptible Staphylococcus aureus, severe pneumonia, lung abscess, bacteremia, hydropneumothorax, prone positioning, postural drainage, case report
Background
Staphylococcus aureus is a common and potentially aggressive pathogen responsible for a wide range of infections, including pneumonia, bacteremia, and osteoarticular disease.1,2 Although methicillin-resistant strains (MRSA) often receive greater attention, methicillin-susceptible S. aureus (MSSA) can also cause life-threatening pulmonary infection, particularly when associated with toxin-mediated injury, rapid tissue necrosis, and delayed infectious source control.3
Severe MSSA pneumonia may progress to necrotizing pneumonia, lung abscess, empyema, and hydropneumothorax, creating substantial management challenges. Extensive lung parenchymal destruction and pleural involvement may result in refractory hypoxemia. Abscess rupture or bronchopleural fistula can cause persistent air leakage and unstable respiratory mechanics. In addition, antimicrobial therapy alone may be insufficient when purulent collections, necrotic debris, or pleural space infection are not adequately controlled. Prolonged mechanical ventilation further increases the risk of ICU-acquired complications, including muscle weakness and difficult weaning.4
Initial antimicrobial treatment for severe community-acquired pneumonia is usually empirical and should cover the most likely pathogens according to illness severity, local epidemiology, and risk factors for drug-resistant organisms. Current guideline-based approaches recommend empirical MRSA coverage, most commonly with vancomycin or linezolid, when validated MRSA risk factors are present or when clinical features raise concern for resistant Gram-positive infection while awaiting microbiological confirmation.5 Once MSSA is confirmed and other pathogens have been excluded or appropriately covered, treatment should be narrowed to an antistaphylococcal beta-lactam, such as oxacillin, nafcillin, or cefazolin, whenever clinically appropriate.6 In complicated cases with empyema, hydropneumothorax, lung abscess, or bronchopleural fistula, antimicrobial therapy should be combined with timely drainage and other source-control measures.
For patients with severe acute respiratory distress syndrome (ARDS), prone positioning is a well-established intervention to improve oxygenation when feasible.7 Extracorporeal membrane oxygenation (ECMO) may be considered for refractory hypoxemia, yet it may not be available or may be declined because of resource limitations, cost, or patient/family preferences. In these circumstances, conventional management depends on early recognition, lung-protective ventilation, appropriate antimicrobial therapy, adequate pleural and airway drainage, and stepwise rehabilitation.
We present a 36-year-old man with community-onset MSSA pneumonia, clinically presumed to be community-acquired, that progressed within approximately one week from initial respiratory symptoms to lung abscess, bacteremia, bilateral hydropneumothorax, empyema, and partial lung destruction, resulting in acute hypoxemic respiratory failure. ECMO support was considered but ultimately not pursued. The patient recovered after early prone positioning, bilateral chest drainage, lesion-guided postural drainage, microbiology-guided antimicrobial therapy, and structured rehabilitation. This report is written in accordance with the CARE guidelines for case reports.8
Case Presentation
Patient Information
A 36-year-old man presented to the emergency department in late October 2024 with a several-day history of fever and upper respiratory tract symptoms. Two days before admission, he developed melena following alcohol consumption. One day before presentation, he experienced sudden hemoptysis and progressive dyspnea.
Initial evaluation suggested community-acquired pneumonia with respiratory failure and possible gastrointestinal bleeding. Chest computed tomography (CT) revealed multifocal bilateral pulmonary infiltrates, small bilateral pleural effusions, bronchiectasis in the upper lobes, mucus plugging in several bronchi, and localized emphysematous changes in the right upper lobe. On arrival, he remained conscious but was severely hypoxemic, with oxygen saturation of 81% despite oxygen delivered through a non-rebreather mask. He underwent emergency endotracheal intubation and was transferred to the intensive care unit (ICU) on invasive mechanical ventilation with a fraction of inspired oxygen (FiO2) of 1.0.
Clinical Findings on ICU Admission
On admission to the ICU, the patient was febrile, with a temperature of 39.6 °C, tachycardia with a heart rate of 129 beats/min, and hypotension with a blood pressure of 89/38 mmHg. Respiratory rate was 18 breaths/min under mechanical ventilation. Arterial blood gas analysis revealed pH 7.30, PaCO2 48 mmHg, PaO2 75 mmHg, bicarbonate 23.6 mmol/L, base excess −2.9 mmol/L, and lactate 3.3 mmol/L, corresponding to a PaO2/FiO2 ratio of 75 mmHg and severe acute respiratory distress syndrome (ARDS). High-dose vasoactive support was required, including norepinephrine 0.73–0.80 μg/kg/min, epinephrine 0.18–0.20 μg/kg/min, and dobutamine 12.22–13.33 μg/kg/min, to maintain mean arterial pressure. Key physiological parameters, laboratory findings, imaging findings, microbiological results, and respiratory support at critical time points are provided in Supplementary Table 1.
Given the profound hypoxemia and hemodynamic instability, veno-venous extracorporeal membrane oxygenation (ECMO) was considered. The family declined ECMO because of financial constraints. Management therefore centered on rapid optimization of oxygenation with prone positioning, airway clearance, microbiology-guided antimicrobial therapy, pleural drainage as needed, and early multidisciplinary rehabilitation. The main clinical events and overall management course are summarized in Table 1.
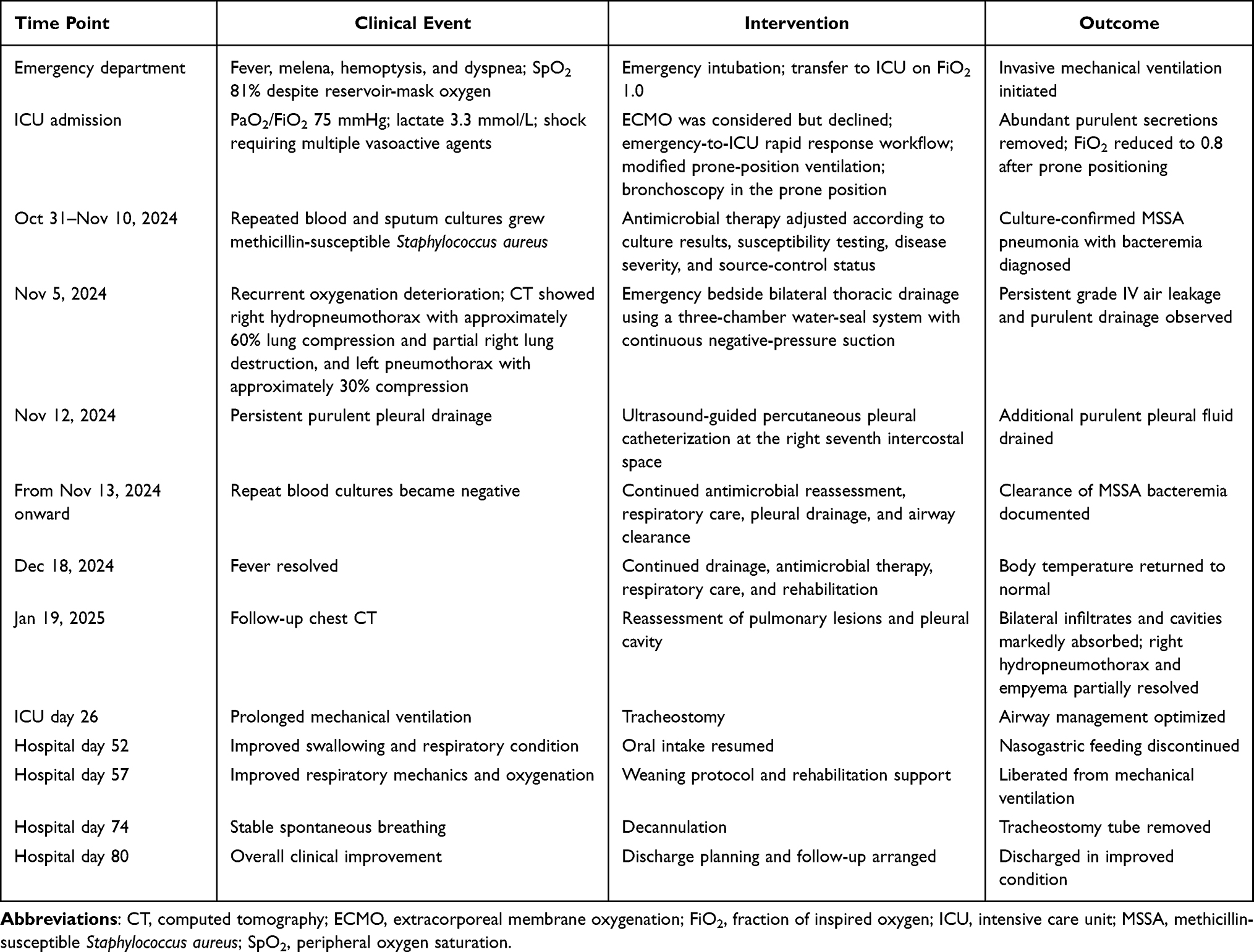 |
Table 1 Main Clinical Events and Management Timeline |
Diagnostic Assessment
Severe methicillin-susceptible Staphylococcus aureus (MSSA) pneumonia complicated by bacteremia, lung abscess, right hydropneumothorax, and left pneumothorax was diagnosed on the basis of clinical features, imaging, and microbiological results. The infection was considered community-onset and clinically presumed to be community-acquired because fever and respiratory symptoms had developed several days before hospital presentation, chest CT at initial evaluation already showed multifocal bilateral pulmonary infiltrates, and early blood and sputum cultures obtained at admission or shortly thereafter grew S. aureus. Methicillin susceptibility was confirmed by automated antimicrobial susceptibility testing, with oxacillin susceptibility and negative cefoxitin screening. The complete antibiogram of the initial S. aureus isolate is provided in Supplementary Table 2. Subsequent blood cultures remained positive during the early hospital course but turned negative from November 13 onward, documenting bacteremia clearance.
Chest CT on November 5 showed right hydropneumothorax with approximately 60% compression of the right lung and partial destruction of the right upper and middle lobes, together with left pneumothorax causing approximately 30% lung compression. Persistent air leakage and purulent pleural drainage suggested rupture of a lung abscess into the pleural space. Follow-up CT on January 19, 2025, demonstrated substantial resolution of bilateral infiltrates and cavities, with partial improvement of the hydropneumothorax and empyema.
To rule out complications of S. aureus bacteremia, repeat blood cultures were monitored until clearance, and transthoracic echocardiography was performed. No. 1 evidence of infective endocarditis was identified. Inflammatory markers, including elevated white blood cell count, C-reactive protein, and procalcitonin, were consistent with severe infection, and no other infectious foci were found. The microbiological findings and antimicrobial treatment course, including antibiotic doses and dosing intervals, are summarized in Table 2.
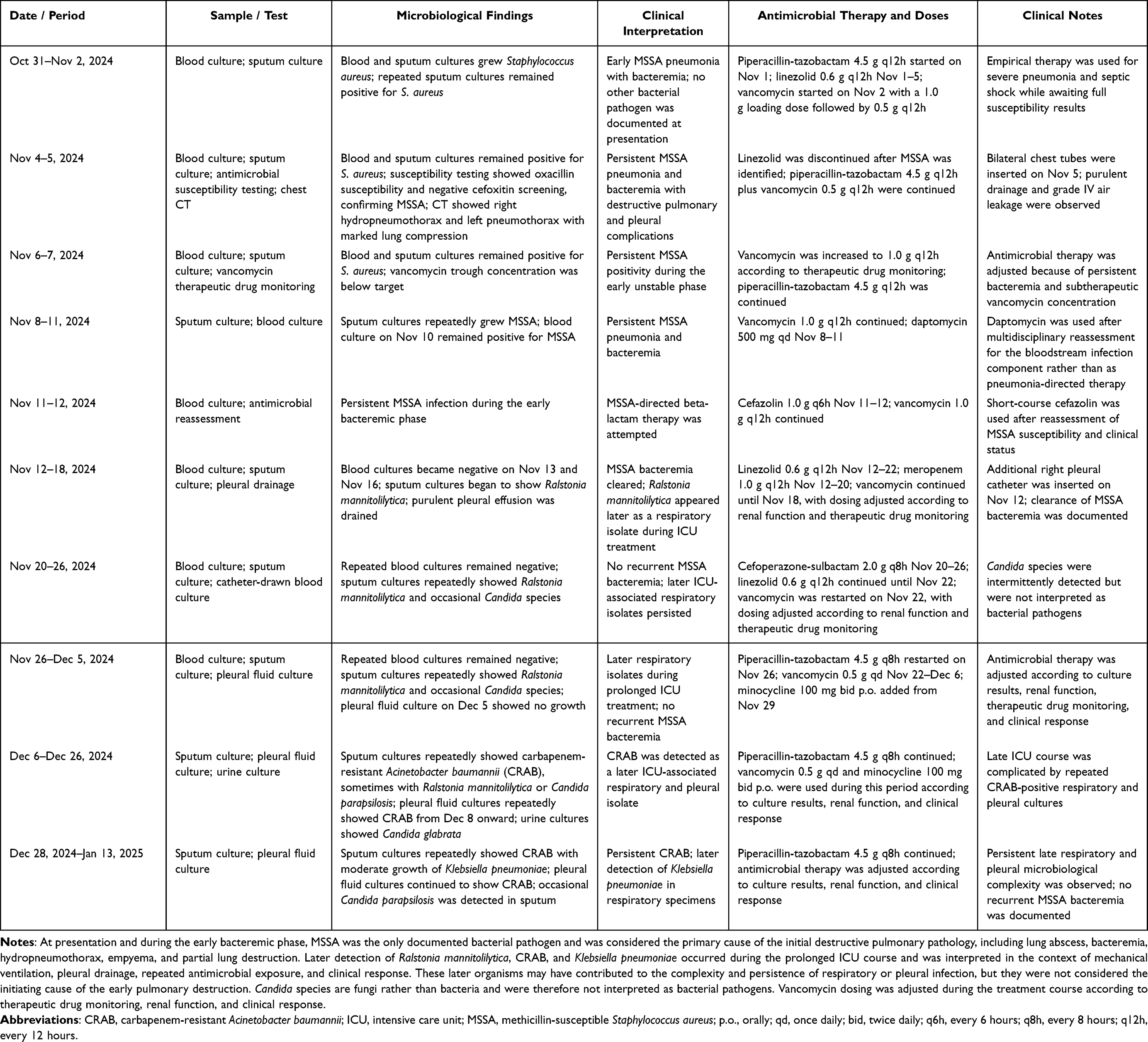 |
Table 2 Microbiological Findings, Isolated Organisms, and Antimicrobial Treatment Timeline |
Therapeutic Interventions
Because ECMO was declined, management emphasized immediate optimization of conventional respiratory support, infectious source control, and stepwise recovery.
Initial Respiratory Support and Prone Positioning
Modified prone positioning was started immediately upon ICU arrival using a pre-prepared rapid-response workflow. The airway was secured, invasive monitoring lines were placed, and all tubes were aligned to minimize traction during turning. A team of four staff members, including nurses, a respiratory therapist, and a physician, performed the turn according to a standardized checklist, completing the procedure within 10 minutes. Sedation was maintained at a Richmond Agitation-Sedation Scale score of −4 to −5. Prone positioning improved oxygenation, allowing FiO2 to be reduced from 1.0 to 0.8. Fiberoptic bronchoscopy performed in the prone position cleared large amounts of yellow purulent secretions from the airways.
Thoracic Drainage and Management of Hydropneumothorax
On November 5, when oxygenation deteriorated further, repeat CT confirmed bilateral pneumothorax/hydropneumothorax with significant lung compression. Emergency bedside insertion of bilateral chest tubes was performed, and the tubes were connected to a three-chamber water-seal system with continuous low negative-pressure suction. Persistent grade IV air leakage and purulent drainage were noted. On November 12, an additional ultrasound-guided pleural catheter was placed in the right seventh intercostal space to enhance drainage of purulent fluid. Drainage volume, air leakage, and fluid characteristics were monitored closely, with gentle tube milking applied when thick pus or necrotic material obstructed flow.
Antimicrobial Treatment
Following identification of MSSA in blood and sputum cultures, antimicrobial therapy was adjusted according to culture results, antimicrobial susceptibility testing, disease severity, organ function, and source-control status. At the time S. aureus was first detected, the patient was receiving piperacillin-tazobactam 4.5 g q12h plus linezolid 0.6 g q12h as empirical therapy for severe pneumonia and septic shock. Vancomycin was added after blood cultures grew S. aureus, with a 1.0 g loading dose followed by 0.5 g q12h, because full susceptibility results were not yet available and the patient had bacteremia with severe respiratory and hemodynamic instability.
After antimicrobial susceptibility testing confirmed MSSA, with oxacillin susceptibility and negative cefoxitin screening, linezolid was discontinued. Piperacillin-tazobactam and vancomycin were continued temporarily during the early unstable phase because of persistent bacteremia, extensive pulmonary destruction, pleural infection, and ongoing source-control procedures. Vancomycin was subsequently increased to 1.0 g q12h according to therapeutic drug monitoring. Because MSSA bacteremia persisted in early follow-up cultures, the regimen was later adjusted after multidisciplinary reassessment to include a short course of daptomycin 500 mg qd for the bloodstream infection component rather than as pneumonia-directed therapy. Cefazolin 1.0 g q6h was then introduced as MSSA-directed beta-lactam therapy after reassessment of susceptibility and clinical status. Blood cultures turned negative from November 13 onward, confirming clearance of bacteremia.
No other bacterial pathogen was documented at presentation or during the early bacteremic phase. Therefore, the early infection was interpreted as culture-confirmed MSSA pneumonia with bacteremia. During the prolonged ICU course, additional organisms were later detected from respiratory or pleural specimens, including Ralstonia mannitolilytica, carbapenem-resistant Acinetobacter baumannii (CRAB), and Klebsiella pneumoniae. These organisms were not isolated at the start and were interpreted as later ICU-associated respiratory or pleural isolates rather than evidence of mixed infection at presentation. Candida species were also intermittently detected, mainly from respiratory or urinary samples; these were described separately because they are fungi rather than bacteria and were not considered the primary bacterial pathogens of the initial pneumonia. Antimicrobial therapy was adjusted dynamically according to the timing of organism isolation, culture results, susceptibility information, renal function, therapeutic drug monitoring, and clinical response. The microbiological findings, including later bacterial isolates, corresponding antimicrobial agents, doses, and dosing intervals, are summarized in Table 2.
Multi-Segmental Postural Drainage
Postural drainage was individualized according to disease stage, air leakage severity, imaging findings, and oxygenation tolerance rather than using fixed positions. In the early phase with prominent air leakage, the patient was kept mainly semi-recumbent or in right lateral decubitus with head-of-bed elevation of approximately 35° to facilitate air evacuation. After air leakage decreased, positions were adjusted to promote drainage of purulent material and necrotic debris.
For upper and middle lobe drainage, a high left lateral position with 45° head elevation and 40° body rotation to the left was performed every 2 hours during routine care. For lower lobe drainage, a 30° head-down tilt with 40° left rotation was limited to 5–10 minutes three times daily to avoid desaturation or reflux. For whole right lung drainage, a 20° head-up slope with left rotation and supportive pillow placement was maintained for about 1 hour twice daily as tolerated.
Before each session, gastric residual volume was checked, subglottic secretions were suctioned, cuff pressure was maintained at 35 cmH2O, and enteral nutrition was temporarily reduced. Vital signs, tidal volume, and SpO2 were monitored continuously; positioning was interrupted if oxygenation or ventilation worsened significantly. Large volumes of purulent and necrotic material were eventually evacuated through this combined approach.
Graded Rehabilitation
Rehabilitation was planned and adjusted daily by a multidisciplinary team, including a rehabilitation therapist, attending physician, and nurse, based on hemodynamic stability, oxygenation, muscle strength, and tube security. In the acute sedated phase, interventions included passive range-of-motion exercises, intermittent pneumatic compression, and airway clearance while maintaining prolonged prone positioning for more than 12 hours/day initially. As consciousness and stability improved, the patient progressed to active-assisted exercises, bedside sitting, cycling, resistance training, and eventual assisted walking, with gradual increases in distance from 50 m to 200 m. Activities were paused if blood pressure, heart rate, or oxygenation deviated beyond predefined safety limits.
Follow-up and Outcomes
The patient’s fever resolved by December 18, 2024. He underwent tracheostomy on ICU day 26, resumed oral intake on hospital day 52, was weaned from mechanical ventilation on hospital day 57, and was decannulated on hospital day 74. He was discharged on hospital day 80 with improved general condition. Follow-up chest CT on January 19, 2025, confirmed marked improvement in pulmonary infiltrates, cavities, and pleural collections. At subsequent outpatient review, he reported no significant residual respiratory symptoms and maintained good functional recovery.
Patient Perspective
Following recovery, the patient described the prolonged mechanical ventilation, repeated drainage procedures, and rehabilitation as both physically exhausting and psychologically challenging. He noted that clear, repeated explanations from the medical team and active family involvement helped him adhere to breathing exercises and progressive mobilization. He expressed satisfaction with the overall outcome and understood the importance of continued follow-up.
Discussion
This case illustrates that methicillin-susceptible Staphylococcus aureus can cause rapidly progressive and destructive pulmonary infection, even when the isolate is confirmed to be methicillin-susceptible.3,9 Recent literature also recognizes S. aureus as an important pathogen in necrotizing pneumonia, which may progress to cavitation, abscess formation, pleural complications, and severe respiratory failure.9 In the present patient, community-onset MSSA pneumonia, clinically presumed to be community-acquired, progressed within approximately one week from initial respiratory symptoms and within 4–5 days after hospital presentation to lung abscess, bacteremia, right hydropneumothorax, left pneumothorax, empyema, partial right lung destruction, severe hypoxemia, and hemodynamic instability. These complications created a complex clinical situation in which oxygenation, antimicrobial treatment, infectious source control, pleural drainage, airway clearance, and prevention of critical illness-related complications had to be addressed simultaneously.
The antimicrobial course needs to be interpreted in the context of the patient’s initial severity and the evolving microbiological findings. At presentation, the patient had severe community-onset pneumonia, septic shock, acute hypoxemic respiratory failure, hemoptysis, gastrointestinal bleeding, and extensive bilateral pulmonary infection. Before culture and susceptibility results were available, severe bacterial pneumonia with possible additional pathogens and drug-resistant Gram-positive infection could not be excluded. Current pneumonia guidelines and recent reviews support empirical antimicrobial selection according to illness severity, local epidemiology, and risk factors for resistant organisms, with MRSA-active agents such as vancomycin or linezolid used when clinically indicated.5,6,9 Piperacillin-tazobactam was therefore started to provide broad empirical coverage for severe pneumonia, while linezolid was used for early Gram-positive coverage in the setting of severe destructive pneumonia. Vancomycin was added after early blood cultures grew S. aureus and before full susceptibility results were available, because the patient had bacteremia with worsening oxygenation and hemodynamic instability. This initial regimen reflected emergency empirical escalation in a critically ill patient and was not intended as a fixed standard combination.
Subsequent susceptibility testing confirmed MSSA, with oxacillin susceptibility and negative cefoxitin screening. Although antistaphylococcal beta-lactams, such as oxacillin, nafcillin, or cefazolin, are generally preferred for proven MSSA infection when clinically appropriate,6,10,11 the actual antimicrobial course required repeated adjustment because of persistent bacteremia, extensive lung destruction, pleural infection, organ dysfunction, and ongoing source-control procedures. After MSSA was identified, linezolid was discontinued, while piperacillin-tazobactam and vancomycin were continued temporarily during the early unstable phase. Vancomycin dosing was subsequently increased to 1.0 g q12h according to therapeutic drug monitoring. Because early follow-up cultures still showed MSSA bacteremia, a short course of daptomycin 500 mg qd was used after multidisciplinary reassessment for the bloodstream infection component rather than as pneumonia-directed therapy. This distinction is important because daptomycin is not considered appropriate for primary alveolar pneumonia owing to inhibition by pulmonary surfactant.12 Cefazolin 1.0 g q6h was then introduced as MSSA-directed beta-lactam therapy after reassessment of susceptibility and clinical status. Blood cultures became negative from November 13 onward, and no recurrent MSSA bacteremia was documented in the available cultures.
The case was defined as MSSA pneumonia with bacteremia because this interpretation was supported by both the published literature and the patient’s microbiological timeline. Previous reports and recent reviews have shown that S. aureus, including methicillin-susceptible strains, can cause necrotizing or destructive pneumonia with cavitation, lung abscess formation, pleural complications, and severe respiratory failure.3,9 In the present case, MSSA was repeatedly isolated from early blood and sputum cultures, and no other bacterial pathogen was documented at presentation or during the early bacteremic phase. Therefore, the initial destructive pulmonary process, including lung abscess formation, bacteremia, hydropneumothorax, empyema, and partial lung destruction, was most consistent with MSSA as the primary pathogen.
During the prolonged ICU course, additional organisms were later detected from respiratory or pleural specimens, including Ralstonia mannitolilytica, carbapenem-resistant Acinetobacter baumannii (CRAB), and Klebsiella pneumoniae. These organisms were not isolated at the start and were interpreted as later ICU-associated respiratory or pleural isolates rather than evidence of mixed infection at presentation. They may have contributed to later clinical complexity by increasing the respiratory or pleural infectious burden, prolonging airway or pleural inflammation, complicating antimicrobial selection, and potentially delaying radiological and ventilatory recovery. However, they were not considered the initiating cause of the early destructive pneumonia. Candida species were also intermittently detected, mainly from respiratory or urinary samples, but these organisms are fungi rather than bacteria and were not considered the primary bacterial pathogens of the initial pneumonia.
Antimicrobial therapy was modified over time according to culture results, susceptibility information, renal function, therapeutic drug monitoring, and clinical response. Later regimens included meropenem 1.0 g q12h, cefoperazone-sulbactam 2.0 g q8h, piperacillin-tazobactam 4.5 g q8h, minocycline 100 mg bid p.o., and vancomycin with dose adjustment when indicated. This course reflects the microbiological complexity of prolonged ICU treatment rather than failure of MSSA-directed therapy alone.
This case also emphasizes that antibiotics alone are unlikely to be sufficient in destructive staphylococcal lung infection with pleural involvement. The patient had extensive purulent airway secretions, lung abscess formation, bilateral hydropneumothorax, empyema, and persistent air leakage. These findings indicated a large burden of infected material and impaired natural drainage. Current literature and pleural disease guidance support timely drainage and source control in pleural infection.13,14 Repeated bronchoscopy, bilateral thoracic drainage, additional pleural catheter placement, continuous negative-pressure drainage, and individualized postural drainage were therefore central to source control. The clearance of bacteremia, absence of echocardiographic evidence of endocarditis, progressive radiological improvement, and eventual clinical recovery suggest that the favorable outcome resulted from the combination of microbiology-guided antimicrobial adjustment and aggressive source-control measures.
Several non-antimicrobial interventions may also have contributed to the favorable outcome despite the absence of extracorporeal membrane oxygenation. First, prone positioning was implemented immediately after ICU admission through a coordinated emergency-to-ICU workflow.7,15,16 At admission, the PaO2/FiO2 ratio was 75 mmHg under FiO2 1.0, and the patient required high-dose vasoactive support. Recent ARDS guidelines support early prone positioning in mechanically ventilated patients with moderate-to-severe ARDS and consideration of VV-ECMO in selected patients with severe ARDS.7,16 ECMO was considered because of the severity of hypoxemia but was not pursued because of financial constraints. Preparation of the airway, vascular lines, sedation, and team roles began before ICU arrival, allowing prone positioning within 10 minutes after admission. This rapid intervention, together with bronchoscopy performed in the prone position, facilitated removal of abundant purulent secretions and provided early support for oxygenation management.
The potential role of ECMO in this case should be interpreted cautiously. Given the initial PaO2/FiO2 ratio of 75 mmHg under FiO2 1.0, ECMO could reasonably have been considered as rescue support for severe hypoxemic respiratory failure.7,16,17 If veno-venous ECMO had been used, it might have provided temporary gas-exchange support, allowed lower ventilator intensity, reduced the risk of ventilator-induced lung injury, and created more time for antimicrobial therapy, bronchoscopy, pleural drainage, and other source-control measures to take effect. In the setting of bilateral pneumothorax/hydropneumothorax and persistent air leakage, ECMO-supported reduction of airway pressures might also have helped facilitate lung rest and limit further barotrauma. However, ECMO would not have directly treated the underlying MSSA pneumonia, lung abscess, empyema, bronchopleural fistula, necrotic lung tissue, or bacterial burden. These conditions would still have required effective antimicrobial therapy, repeated airway clearance, pleural drainage, and careful source control. In addition, ECMO usually requires systemic anticoagulation and specialized resources, which would have required careful risk assessment in this patient because of hemoptysis, gastrointestinal bleeding, pleural drainage, and repeated invasive procedures. Therefore, although ECMO might have improved early oxygenation and provided a bridge to infection control, it cannot be assumed that ECMO would have shortened the disease course or improved the final outcome in this single case. The present outcome should not be interpreted as evidence that ECMO can be routinely avoided in comparable patients; rather, it suggests that selected patients may still recover without ECMO when conventional management is implemented rapidly and comprehensively.
Second, pleural and airway drainage were individualized according to evolving imaging findings and clinical needs.13,14 Initial bilateral chest tube insertion was performed to manage right hydropneumothorax, left pneumothorax, marked lung compression, and persistent air leakage, with priority given to continuous air evacuation to prevent further lung collapse. Once air leakage became more manageable, multi-segmental postural drainage was adjusted according to lesion distribution, drainage characteristics, and oxygenation tolerance. This staged approach, shifting from air evacuation to targeted removal of purulent and necrotic material, supported source control in a situation where fixed postural drainage would have been difficult because pneumothorax and lung destruction coexisted.
Finally, a structured rehabilitation program was started early while the patient was still receiving prolonged mechanical ventilation.4,18,19 Recent guidance on positioning and early mobilization in critically ill adults supports individualized mobilization strategies according to physiological stability, safety criteria, and interdisciplinary assessment.19 Rehabilitation began with passive range-of-motion exercises and airway clearance during deep sedation, then gradually advanced to active-assisted movements, resistance training, bedside sitting, standing, and supported walking as hemodynamic stability and muscle strength recovered. This stepwise approach appeared to limit ICU-acquired weakness and facilitated eventual weaning from ventilation, tracheostomy decannulation, return to oral intake, and functional recovery.
This report has several limitations. As a single case report, the favorable outcome cannot be attributed to any single intervention, and the findings may not apply to all patients with comparable disease severity. Although the timing of symptom onset, initial imaging findings, and early positive blood and sputum cultures supported community-onset infection, molecular typing, whole-genome sequencing, or epidemiological tracing was not performed. Therefore, the case is described as clinically presumed community-acquired MSSA pneumonia based on clinical timing and microbiological evidence, rather than definitive microbiological proof of strain origin. In addition, some detailed quantitative data, including serial PaO2/FiO2 ratios, daily drainage volumes, antimicrobial drug concentrations, inflammatory marker trends, and formal functional scores, were not fully documented. The antimicrobial course was complex and was influenced by evolving culture results, organ function, prolonged ICU treatment, and later ICU-associated pathogens. Long-term pulmonary function tests and extended imaging follow-up would have provided stronger outcome information. Since ECMO was declined for financial reasons, this case offers no direct comparison with ECMO-supported management. Therefore, any discussion of what might have occurred with ECMO remains hypothetical and should be interpreted cautiously. This case should be viewed as an illustration of coordinated multidisciplinary care under resource constraints, rather than evidence that ECMO can be routinely avoided in comparable situations.
Conclusions
In this patient, repeated early isolation of MSSA from blood and sputum cultures, together with the absence of other documented bacterial pathogens at presentation or during the early bacteremic phase, supported MSSA as the primary pathogen of the initial destructive pulmonary process. The later isolation of Ralstonia mannitolilytica, carbapenem-resistant Acinetobacter baumannii, and Klebsiella pneumoniae was interpreted as ICU-associated respiratory or pleural isolates that complicated the subsequent course rather than as evidence of mixed infection at presentation. This case indicates that culture-confirmed community-onset MSSA pneumonia may be associated with rapidly progressive lung abscess, bacteremia, hydropneumothorax, and life-threatening respiratory failure. When ECMO is unavailable or declined, early prone positioning, timely and individualized pleural/airway drainage, microbiologically guided antimicrobial therapy, and early graded rehabilitation may provide a feasible multimodal management pathway in carefully selected patients.
Abbreviations
ARDS, acute respiratory distress syndrome; CRAB, carbapenem-resistant Acinetobacter baumannii; CT, computed tomography; ECMO, extracorporeal membrane oxygenation; FiO2, fraction of inspired oxygen; ICU, intensive care unit; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus; PaCO2, partial pressure of arterial carbon dioxide; PaO2, partial pressure of arterial oxygen; PEEP, positive end-expiratory pressure; RASS, Richmond Agitation-Sedation Scale; SpO2, peripheral oxygen saturation.
Data Sharing Statement
The datasets generated and/or analysed during the current case report are available from the corresponding author on reasonable request, subject to institutional policies and patient privacy protections.
Ethics Approval and Consent to Participate
This case report involved a retrospective analysis of anonymized clinical data. The study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (Approval No. [2025B] IIT Ethics Approval No. 0542, expedited review). The requirement for informed consent to participate was waived by the Ethics Committee because of the retrospective nature of the study and the use of anonymized clinical data.
Consent for Publication
Written informed consent for publication of this case report and any accompanying images was obtained from the patient.
Acknowledgments
The authors sincerely thank Dr. Wenqiao Yu and Dr. Hangyang Li, directors of the ICU at our hospital, for their continuous involvement in the clinical management and treatment of this patient, as well as for their valuable support and guidance during the preparation of this case report. The authors also thank the multidisciplinary team, including ICU physicians, nurses, respiratory therapists, and rehabilitation specialists, for their dedicated care throughout the patient’s hospitalization.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Science and Technology Major Project Young Scientist Program, “Role of Pulmonary Microecology in the Development and Progression of Chronic Respiratory Diseases” (Project No. 2025ZD0549000). The funder had no role in the study design, data collection, data analysis, interpretation of data, writing of the manuscript, or decision to submit the article for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Holland TL, Arnold C, Fowler VG. Clinical management of Staphylococcus aureus bacteremia: a review. JAMA. 2014;312(13):1330–12. doi:10.1001/jama.2014.9743
2. Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–661. doi:10.1128/CMR.00134-14
3. Kreienbuehl L, Charbonney E, Eggimann P. Community-acquired necrotizing pneumonia due to methicillin-sensitive Staphylococcus aureus secreting Panton-Valentine leukocidin: a review of case reports. Ann Intensive Care. 2011;1(1):52. doi:10.1186/2110-5820-1-52
4. Schmidt GA, Girard TD, Kress JP, et al. Liberation from mechanical ventilation in critically ill adults: executive summary of an official American College of Chest Physicians/American Thoracic Society clinical practice guideline. Chest. 2017;151(1):160–165. doi:10.1016/j.chest.2016.10.037
5. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
6. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi:10.1093/cid/ciw353
7. Qadir N, Sahetya S, Munshi L, et al. An update on management of adult patients with acute respiratory distress syndrome: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2024;209(1):24–36. doi:10.1164/rccm.202311-2011ST
8. Gagnier JJ, Kienle G, Altman DG, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. Glob Adv Health Med. 2013;2(5):38–43. doi:10.7453/gahmj.2013.008
9. Kapania EM, Cavallazzi R. Necrotizing pneumonia: a practical guide for the clinician. Pathogens. 2024;13(11):984. doi:10.3390/pathogens13110984
10. Bai AD, Morris AM. Management of Staphylococcus aureus bacteremia in adults. CMAJ. 2019;191(35):E967. doi:10.1503/cmaj.190363
11. McDanel JS, Perencevich EN, Diekema DJ, et al. Comparative effectiveness of beta-lactams versus vancomycin for treatment of methicillin-susceptible Staphylococcus aureus bloodstream infections among 122 hospitals. Clin Infect Dis. 2015;61(3):361–367. doi:10.1093/cid/civ308
12. Silverman JA, Mortin LI, Vanpraagh ADG, Li T, Alder J. Inhibition of daptomycin by pulmonary surfactant: in vitro modeling and clinical impact. J Infect Dis. 2005;191(12):2149–2152. doi:10.1086/430352
13. Elsheikh A, Bhatnagar M, Rahman NM. Diagnosis and management of pleural infection. Breathe. 2023;19(4):230146. doi:10.1183/20734735.0146-2023
14. Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society guideline for pleural disease. Thorax. 2023;78(Suppl 3):s1–s42. doi:10.1136/thorax-2022-219784
15. Guerin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159–2168. doi:10.1056/NEJMoa1214103
16. Grasselli G, Calfee CS, Camporota L, et al. ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med. 2023;49:727–759. doi:10.1007/s00134-023-07050-7
17. Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378(21):1965–1975. doi:10.1056/NEJMoa1800385
18. Girard TD, Alhazzani W, Kress JP, et al. An official American Thoracic Society/American College of Chest Physicians clinical practice guideline: liberation from mechanical ventilation in critically ill adults. Rehabilitation protocols, ventilator liberation protocols, and cuff leak tests. Am J Respir Crit Care Med. 2017;195(1):120–133. doi:10.1164/rccm.201610-2075ST
19. Schaller SJ, Scheffenbichler FT, Bein T. Guideline on positioning and early mobilisation in the critically ill by an expert panel. Intensive Care Med. 2024;50(8):1211–1227. doi:10.1007/s00134-024-07532-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Metagenomic Next-Generation Sequencing Reveals Porphyromonas gingivalis in Geriatric Severe Pneumonia Complicated by Empyema: Case Report
Guo N, Ma G, Liu H, Qiu J, Yu Y, Gao Y, Yi Z, Wan Z, Zhang L, Wu X
Infection and Drug Resistance 2025, 18:4811-4816
Published Date: 9 September 2025