Back to Journals » Psychology Research and Behavior Management » Volume 19
Culturally Adapted Interpersonal Psychotherapy for Perinatal Depression in Rural China: A Pilot Randomized Controlled Trial
Authors Wang R, Wang SY ![]() , Ouyang YQ, Fu D, Huang X
, Ouyang YQ, Fu D, Huang X
Received 11 September 2025
Accepted for publication 28 January 2026
Published 19 February 2026 Volume 2026:19 566784
DOI https://doi.org/10.2147/PRBM.S566784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Rong Wang,1,* Shi-Yun Wang,2,* Yan-Qiong Ouyang,2 Dou Fu,3 Xing Huang4
1Nursing Department, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 2School of Nursing, Wuhan University, Wuhan, People’s Republic of China; 3General Practice Department, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 4Hospital Administration, Songzi People’s Hospital, Jingzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xing Huang, Hospital Administration, Songzi People’s Hospital, Jingzhou, People’s Republic of China, Email [email protected] Rong Wang, Nursing Department, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China, Email [email protected]
Purpose: This pilot randomized controlled trial examined the feasibility, acceptability, and preliminary effectiveness of a culturally optimized Interpersonal Psychotherapy (IPT) for perinatal depression among rural women in China. It was hypothesized that the adapted IPT would be feasible to deliver, acceptable to participants, and potentially effective in improving depressive symptoms, social support, and family functioning.
Patients and Methods: A pilot randomized controlled trial was conducted with 34 pregnant women recruited from two rural clinics in Hubei, China. Participants were randomized to treatment-as-usual (TAU) or culturally optimized IPT plus TAU. The IPT program comprised three face-to-face sessions and one online follow-up, tailored to rural family and cultural contexts. The Edinburgh Postnatal Depression Scale (EPDS) was used to assess depressive symptoms, with social support and family functioning as secondary outcomes.
Results: Compared with TAU, participants receiving the adapted IPT showed suggested reductions in EPDS scores and improvements in social support and family functioning at postpartum follow-ups. Feasibility was demonstrated by high adherence (94.1%), low attrition, and strong satisfaction. Bayesian mixed-effects modeling confirmed the robustness of these trends.
Conclusion: Findings indicate that the adapted IPT was both feasible and well accepted within rural maternal care systems, suggesting potential psychosocial benefits aligned with the study’s hypotheses. The culturally optimized IPT appears promising as a feasible, acceptable, and potentially effective approach for supporting maternal mental health in rural China. Larger trials with extended follow-up are needed to confirm these preliminary results.
Keywords: social support, family functioning, cultural adaptation, feasibility, bayesian analysis
Introduction
Perinatal depression (PND) is a non-psychotic depressive disorder occurring during pregnancy or within one year postpartum, characterized by low mood and loss of interest.1 It affects maternal well-being and child development, increasing risks of preterm birth, disrupted breastfeeding, impaired mother-infant bonding, and later emotional or behavioral problems in children.2–4 Globally, approximately 26.3% of women are affected by PND, with rates of 28.5% during pregnancy and 27.6% postpartum.5 In China, the prevalence is slightly lower, at 16.3%, but rises to 32.0% in rural areas due to limited healthcare access and cultural barriers.6,7
Psychosocial factors, particularly social support and family function, are critical determinants of PND risk.8,9 Social support, encompassing objective, subjective, and utilization dimensions, buffers stress and protects against depression, yet many women experience reduced interpersonal connections during pregnancy, heightening vulnerability.10–12 However, many women discontinue leisure activities and employment during pregnancy, leading to a loss of interpersonal and group relationships. Coupled with the stress of pregnancy, reduced access to social support can significantly impair psychological health during pregnancy. More importantly, although women may receive a high level of social support during pregnancy, the inability to maintain this support throughout the perinatal period may lead to a heightened sense of loss, thereby increasing the risk of developing mental health disorders.12
Family functioning likewise plays a central role; cohesive, supportive families promote emotional well-being, while dysfunctional dynamics increase depressive symptoms.13–15 In China, particularly in rural areas, the family is a central institution for pregnant women. Marital dissatisfaction, lack of spousal support, and mother-in-law conflicts are key contributors to PND risk.16,17 While this support can be beneficial, it may also lead to stress when conflict arises.17 Common sources of tension include disagreements over pregnancy-related decisions, lifestyle differences, over-involvement by the mother-in-law, and a lack of emotional or practical support from the husband.18,19 Supportive family interactions provide pregnant women with emotional and practical assistance, which can alleviate distress and promote positive emotions.20
Interpersonal Psychotherapy (IPT) is a structured, short-term intervention that alleviates depressive symptoms by improving interpersonal functioning and social support.19 IPT addresses four domains: role transitions, interpersonal conflicts, grief, and social isolation through strategies such as communication analysis, role-playing, and behavioral activation.20 IPT is typically delivered over 8–12 sessions and emphasizes identifying interpersonal problem areas, enhancing communication skills, and mobilizing social support. The therapeutic process involves three phases: initial assessment and interpersonal inventory, intermediate sessions targeting specific problem domains, and a termination phase focusing on consolidation and relapse prevention. Cultural adaptation may include integrating family members, modifying communication exercises, and adjusting session frequency to local contexts.
IPT is one of the most effective non-pharmacological treatments for perinatal depression, with advantages over cognitive-behavioral therapy in some contexts.21 Beyond reducing depressive symptoms, IPT has been shown to enhance family relationships and social support, key protective factors during the perinatal period.22,23 While IPT is widely recommended as a first-line treatment by the WHO and the Chinese Medical Association, its application in rural China remains limited.24 Women in these settings often face unique family-centered challenges, such as marital dissatisfaction and mother-in-law conflicts, which are not fully addressed by standard IPT protocols.24 Adapted forms of IPT, including brief (B-IPT), telephone-delivered (IPT-T), and couple- and family-based models, have demonstrated feasibility and efficacy in improving perinatal outcomes.25–27 Given these findings, developing a culturally optimized IPT that specifically addresses the interpersonal and familial challenges of rural Chinese women is both necessary and promising.
This study aimed to evaluate the feasibility, acceptability, and preliminary effectiveness of a culturally optimized IPT program for perinatal women in rural China. The study was guided by three hypotheses: (1) The optimized IPT would demonstrate high feasibility and acceptability among rural perinatal women. (2) Within the intervention group, depressive symptoms would significantly decrease, while social support and family functioning would significantly improve after the intervention compared with baseline. (3) Compared with the control group, the intervention group would show significantly greater improvements in depressive symptoms, social support, and family functioning at post-intervention and postpartum follow-ups.
Materials and Methods
Program Development
The intervention program was developed based on the Consolidated Framework for Implementation Research (CFIR) and integrated principles from Interpersonal Psychotherapy (IPT).20,28 The design process involved a literature review, expert consultation, and cultural adaptation to the rural maternal population.
An expert panel of 15 professionals (nursing specialists, psychologists, sociologists, psychiatrists, maternal and child health experts, and community nurses with rural experience) was invited based on three criteria: (1) a bachelor’s degree or higher, (2) ≥10 years of clinical or teaching experience, and (3) willingness to participate voluntarily. Two rounds of online consultations were conducted via Email and WeChat. After each round, a designated researcher summarized expert feedback, which the research team discussed and incorporated into the next version of the protocol. To ensure cultural and linguistic appropriateness, a project advisory committee of eight pregnant women from two rural hospitals reviewed the intervention’s wording and procedures. Their feedback was used to refine session content and examples. A small open trial involving five women with elevated depressive symptoms (EPDS ≥ 9.5) was then conducted to assess feasibility, adherence, and participant satisfaction. Feedback from participants and interventionists was used to optimize the final protocol for the main trial.
Study Settings
Pregnant women were recruited by convenience sampling at two obstetrics outpatient clinics in Songzi, a rural area of Jingzhou, Hubei Province, China. The study protocol, in compliance with the Declaration of Helsinki, was approved by the Ethics Committee of Medical Research Committee of Medical College of Wuhan University (WHU-LFMD-IRB2024045) and the Renmin Hospital of Wuhan University (WDRY2024-K196). It has been registered in the Chinese Clinical Trial Registry at www.chictr.org.cn (registration number: ChiCTR2400091952).
Study Sample
Eligibility Criteria
Women who (1) are aged over 20 years, (2) have a gestational age of 28–32 weeks, (3) are pregnant with a singleton, (4) regularly attend obstetric check-ups at this hospital and plan to deliver at the same hospital, and (5) scored ≥ 9.5 on Edinburgh Postnatal Depression Scale (EPDS) were recruited.29 Potential participants were excluded if they (1) were currently receiving mental health services or (2) scored ≥13 on EPDS and met the diagnostic criteria for major depression, dysthymia, depression not otherwise specified (excluding simple phobia), or psychosis, as assessed using the relevant modules of the Structured Clinical Interview for DSM-5 Disorders—Clinician Version (SCID-5-CV).30,31
Sampling Size
The sample size was estimated according to the guidelines provided by Whitehead, Julious, Cooper and Campbell32 The primary trial was designed with 90% power and a two-sided significance level of 5%. Based on a standardized medium effect size (0.5), a sample size of 15 participants per group (30) was recommended for the pilot trial. Considering a 10% attrition rate, the final sample size should be 34 participants.
Randomization and Blinding
A simple randomization procedure was performed using R software (version 4.4.3). A random allocation sequence was generated by randomly permuting 17 “Intervention” and 17 “Control” labels, resulting in a 1:1 allocation ratio. The generated group assignments were then placed into 34 sequentially numbered, opaque, and sealed envelopes. These envelopes were prepared by a study coordinator who was not involved in participant recruitment or outcome assessment. Upon participant enrollment, the next envelope in numerical order was opened by an independent coordinator after baseline data collection, ensuring allocation concealment throughout the randomization process.
Due to the nature of the intervention, blinding of participants and intervention providers was not feasible. However, to minimize bias, several blinding strategies were implemented. The randomization sequence and group assignments were prepared and sealed by an independent coordinator who was not involved in participant recruitment, intervention delivery, or outcome assessment. Recruiters and data collectors remained blinded to group assignments throughout enrollment and baseline assessment. Additionally, the statistician conducting the data analysis was blinded to group allocation until the primary analyses were completed.
Control Group
Participants in the TAU group received standard prenatal and postnatal care provided by the hospital’s antenatal outpatient clinic. The program comprises five structured sessions: (1) preconception and prenatal health management, including conception planning, weight management, and education on conditions such as gestational diabetes and thyroid disorders; (2) common pregnancy discomforts and early signs of labor; (3) childbirth preparation, covering benefits of natural delivery, pain management, and postoperative care; (4) newborn care and breastfeeding; and (5) postpartum recovery and rehabilitation. Apart from initial contact at enrollment, participants will not receive additional guidance or intervention from the research team. The details are shown in Supplementary Figure 1.
Intervention Group
In addition to receiving standard prenatal and postnatal care, participants in the intervention group received culturally optimized IPT sessions scheduled right after the second, third, and fourth standard prenatal programs. This design ensured equal total contact frequency between the intervention and control groups while allowing IPT to be integrated into routine care without disrupting the hospital’s existing schedule. The intervention consisted of three weekly 60-minute sessions and one online follow-up via WeChat. Each session combined psychoeducation, interpersonal formulation, open discussions, and role-playing. Participation of significant family members (eg, spouses or in-laws) was optional and only invited when relevant to the participant’s interpersonal goals, to minimize bias in measuring social support. The first session focused on comprehensive assessment and individualized goal setting using an interpersonal inventory. The second session addressed role transitions, awareness of postpartum depression, and culturally relevant coping strategies. The third session emphasized communication skills, conflict resolution, and building support networks, with attention to culturally specific postpartum practices. The follow-up session reinforced skills, monitored potential relapse, and assessed ongoing support needs. The details are shown in Figure 1.
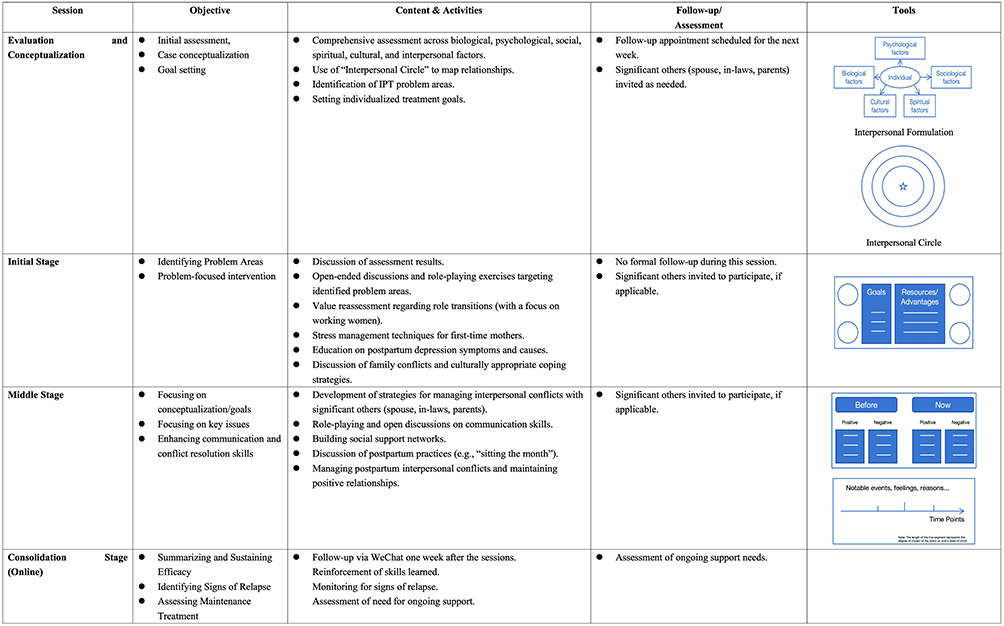 |
Figure 1 Culturally optimized IPT program. |
Data Collection
Basic Information Questionnaire
A researcher-designed questionnaire was used to collect socio-demographic information from participants. This included data on age, education level, monthly household income, conception method, planned pregnancy, gestational age, parity, smoking status, gynaecological conditions, and family medical history.
Mental Health Outcomes
The onset of postpartum depression and depressive symptom severity are the primary outcomes of this study. The EPDS was used to assess perinatal depression at intake, post-intervention, and 7-and 42-day postpartum. According to Lau, Wang, Yin, Chan and Guo,29 and Wang, Guo, Lau, Chan, Yin and Chen,33 the threshold EPDS score for clinical depression in pregnant women in China was 9.5. In postpartum samples, the threshold was >10. If the EPDS score of a woman reached 13 or higher at any measurement time point, referral for further evaluation and treatment by a psychologist would be recommended. Given that referral could potentially serve as a confounding factor in the study, no further follow-up would be conducted once the referral was made.
Sociological Outcomes
(1) Maternal social support level
The Social Support Rating Scale (SSRS) was developed by Xiao10 and is widely used in Chinese populations to assess levels of social support. The SSRS includes 10 items grouped into three dimensions: subjective support, objective support, and support utilization. The total score ranges from 12 to 66. Based on prior studies, scores are categorized as low (12–23), moderate (24–44), and high (45–66) levels of social support. The SSRS has been widely used in China and demonstrates strong validity and reliability.
(2) Maternal family function
Family function was measured using the Family APGAR questionnaire developed by Smilkstein.34 The scale includes five items assessing adaptation, partnership, growth, affection, and resolve. Each item is rated on a 3-point scale, yielding a total score between 0 and 10. Scores of 8–10 indicate good family functioning, 4–7 reflect moderate dysfunction, and 0–3 suggest severe dysfunction. The Chinese version has demonstrated high internal consistency.
Feasibility and Acceptability
The feasibility of the intervention program was evaluated by examining recruitment and refusal rates, participant willingness, follow-up rates, reliability, and questionnaire response quality. The acceptability of the IPT intervention was assessed by monitoring intervention completion and dropout rates. Reasons for discontinuation were analyzed to identify consistent patterns. To assess acceptability and participant satisfaction with the intervention, the self-designed Treatment Satisfaction Questionnaire (see Supplementary Figure 2) and open interviews were conducted at the end of the intervention or upon participant withdrawal. The SPIRIT schedule is presented in Table 1.
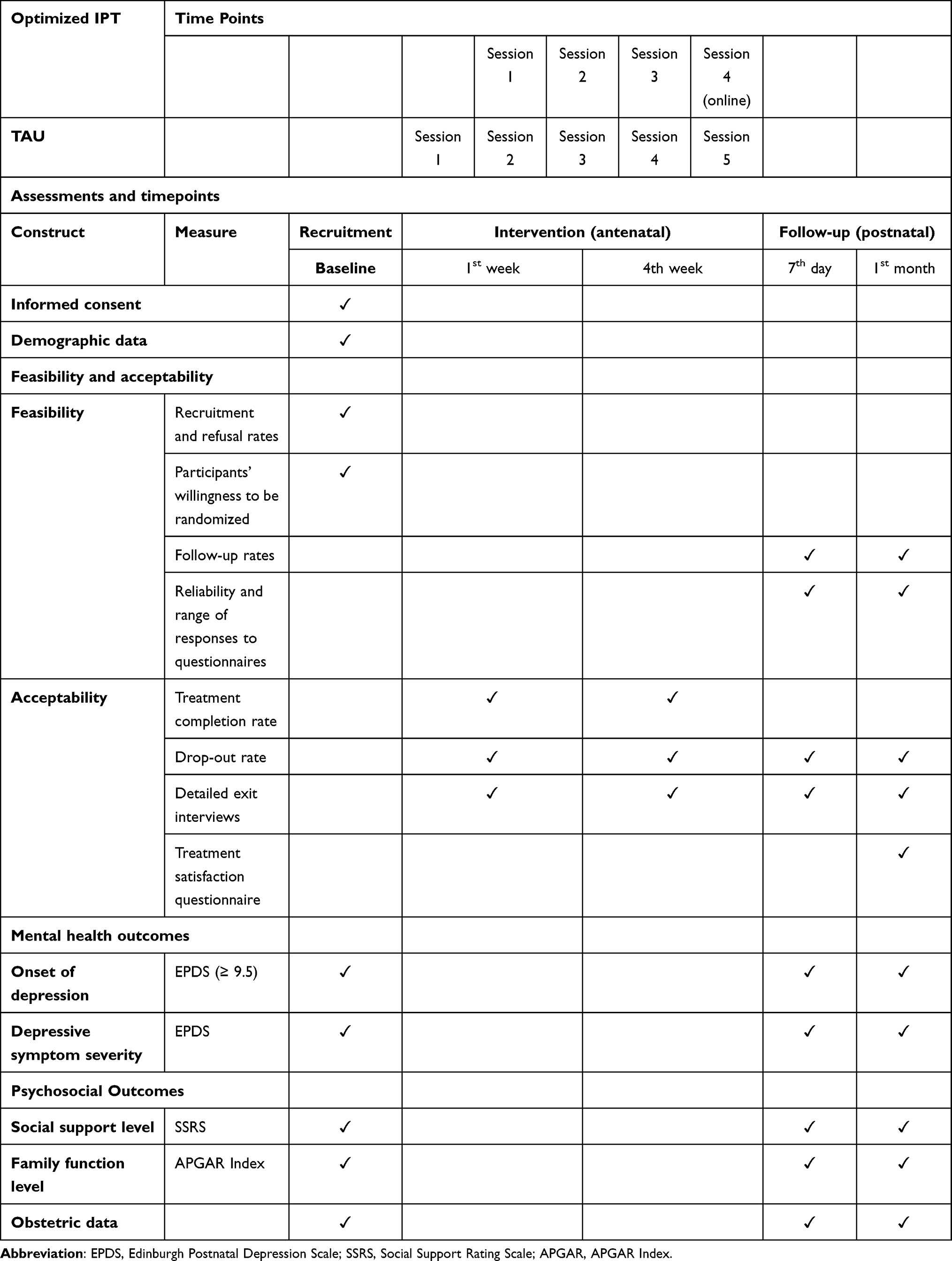 |
Table 1 The SPIRIT Schedule |
Data Collection Process
Interventionists received structured training and competency assessments, followed by ongoing supervision to ensure intervention fidelity. Participant adherence was supported through WeChat reminders, with withdrawal permitted at any time; reasons for withdrawal were documented, and data from these cases were excluded from analyses. Participants with high depressive symptoms were referred to mental health services. Ethical approval was obtained from the institutional review board, and written informed consent was secured from all participants. Standardized self-reported questionnaires were administered at baseline and follow-up via secure electronic platforms, with single-entry restrictions to ensure data integrity. All data were anonymized, encrypted, and stored under strict access control to protect confidentiality.
Statistical Analysis
All statistical analyses were conducted using R (version 4.4.3). Descriptive statistics were used to summarize baseline characteristics and outcome measures. Group comparisons at each time point were conducted using appropriate statistical tests, including chi-square tests for categorical variables and t-tests or non-parametric equivalents for continuous variables.
The primary outcome was the change in depression scores over time between the intervention and control groups. A Bayesian linear mixed model was employed to account for repeated measures and individual variability, adjusting for time, group, and time-by-group interaction effects. The model reported posterior distributions, medians, and 95% credible intervals to interpret group differences.
Missing data were handled using random forest imputation, assuming data were missing at random. Model convergence and stability were confirmed by diagnostic indices, including R-hat values close to 1 and effective sample sizes exceeding 3000.
Result
Data Collection
A total of 40 pregnant women were screened for eligibility; five declined to participate, and one was excluded because they did not meet the inclusion criteria. Ultimately, 34 participants were enrolled and randomly assigned to either the intervention group (n = 17) or the control group (n = 17). After obtaining informed consent, all participants completed the baseline questionnaires. In the intervention group, one participant was lost to follow-up at 42 days postpartum due to unsuccessful contact, resulting in 16 participants completing the final follow-up. In the control group, one participant had an EPDS score of 13 or higher at 7 days postpartum and was not followed further. As a result, all participants completed the post-intervention (T1) and 7-day postpartum (T2) assessments, while 32 completed the 42-day postpartum (T3) follow-up, yielding a follow-up rate of 94.1%. (See Figure 2).
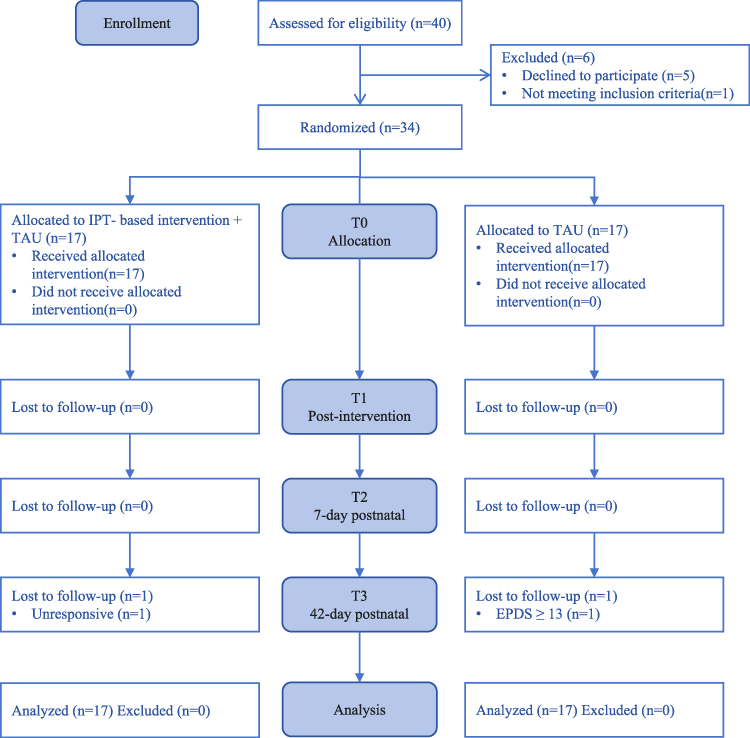 |
Figure 2 CONSORT flowchart. |
Little’s MCAR test indicated that missing data were missing completely at random. Random forest imputation was applied for EPDS, social support, and family function scores, with post-imputation distributions showing no significant bias relative to the original data (Table 2).
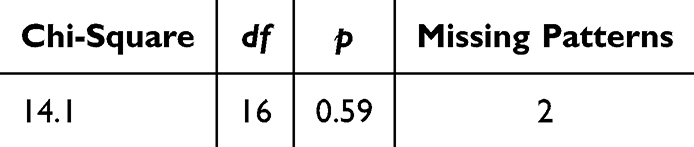 |
Table 2 Results of Little’s MCAR Test for Missing Data |
No significant baseline differences were found between groups in demographic, obstetric, or psychological variables (Table 3 and Figure 3).
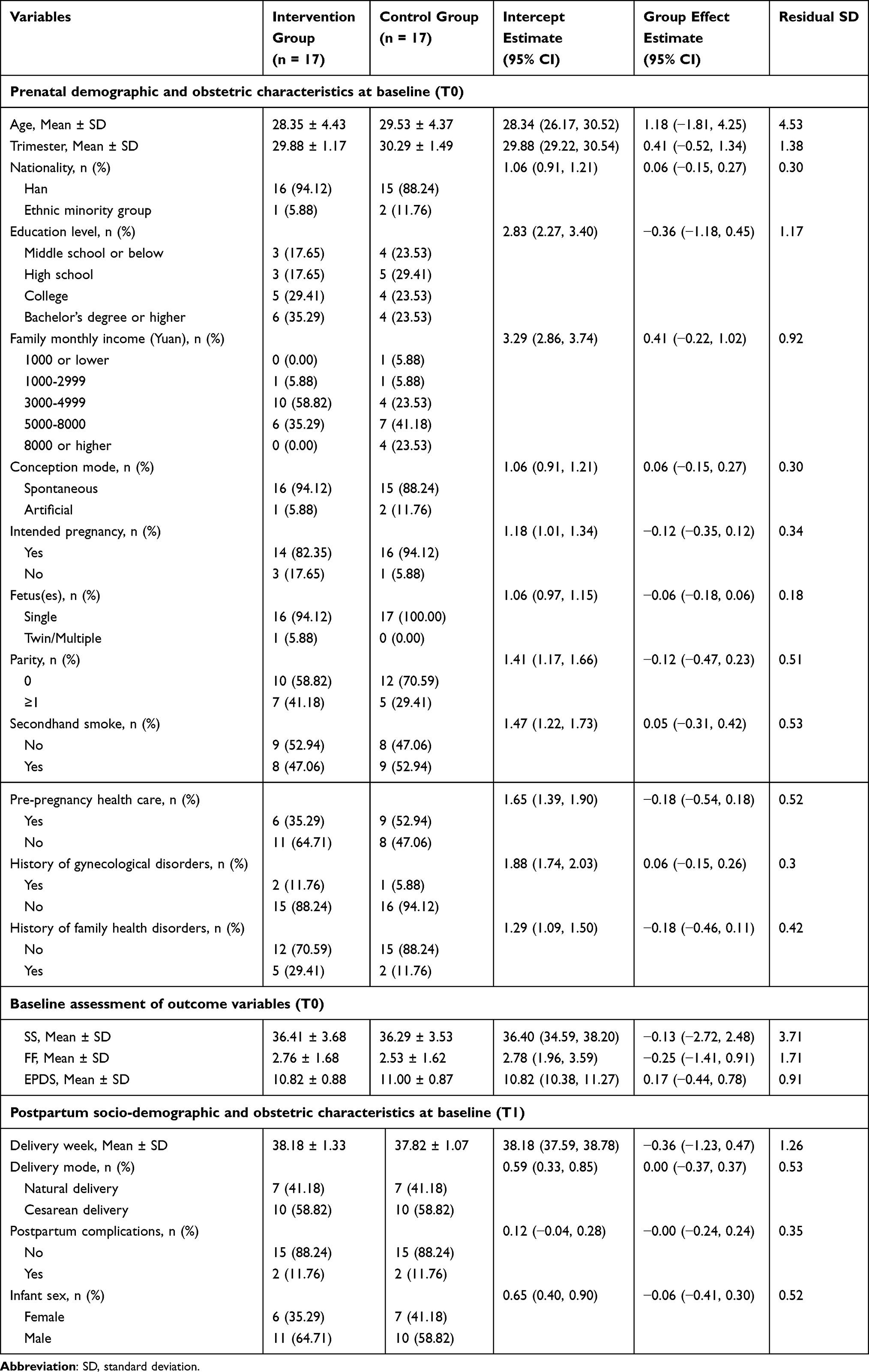 |
Table 3 Baseline Differences Between the IPT and TAU Groups in Demographic, Obstetric, or Outcome Variables |
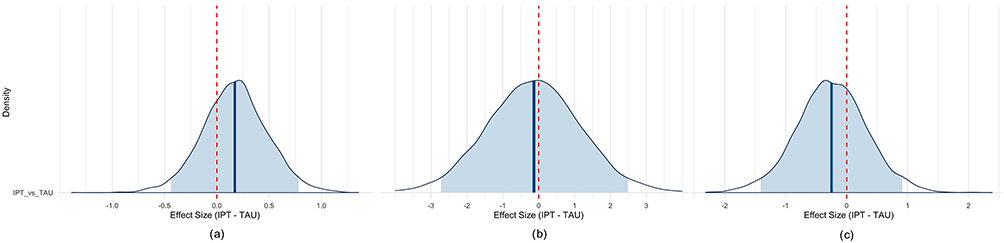 |
Figure 3 Posterior density plots of baseline score differences between IPT and TAU groups. (a) Posterior density plots of baseline score differences in EPDS scores. (b) Posterior density plots of baseline score differences in SSRS scores. (c) Posterior density plots of baseline score differences in Family APGAR scores. Abbreviations: IPT, Interpersonal psychotherapy group; TAU, Treat as Usual group; EPDS, Edinburgh Postnatal Depression Scale; APGAR, APGAR Index; SSRS, Social Support Rating Scale. |
Feasibility and Acceptability
A total of 16 participants in the IPT group completed the Treatment Satisfaction Questionnaire and open-ended responses. The mean score was 23.44 ± 1.03, reflecting a high level of satisfaction. The majority reported that the interpersonal communication content was practical and relevant to their daily lives (93.75%) and that the program was closely aligned with their needs (87.5%). Satisfaction with the delivery format was also high, with 81.25% endorsing the face-to-face sessions, role-playing, and online follow-up, and 93.75% indicating that the frequency and duration were appropriate. No participant rated the intervention as “very unsatisfactory.” Qualitative feedback highlighted preferences for greater flexibility in scheduling, stronger engagement of family members, and the value of digital peer interaction, which was perceived as an important source of emotional support and shared learning.
Within-Group Changes
Growth Curve Analysis
Results of the Bayesian linear mixed-effects model indicated a significant reduction in EPDS scores (b = −1.19, SE = 0.19, 95% HDI [−1.55, −0.83], Cohen’s d = 1.91), reflecting improvements in depressive symptoms. Social support significantly increased (b = 3.12, SE = 0.45, 95% HDI [2.24, 4.03], Cohen’s d = 1.87), while family function also showed marked improvement (b = 1.86, SE = 0.20, 95% HDI [1.47, 2.27], Cohen’s d = 3.19). (Figure 4 and Table 4).
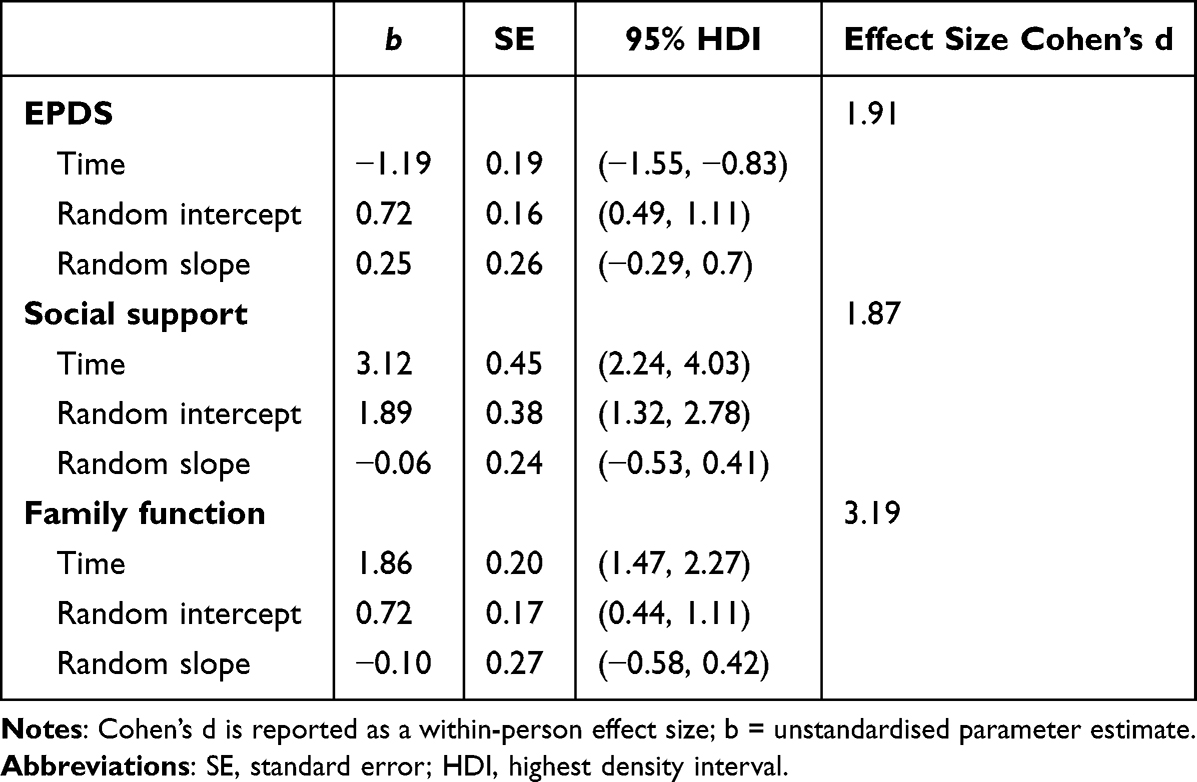 |
Table 4 Growth Curve Model Results for Outcomes |
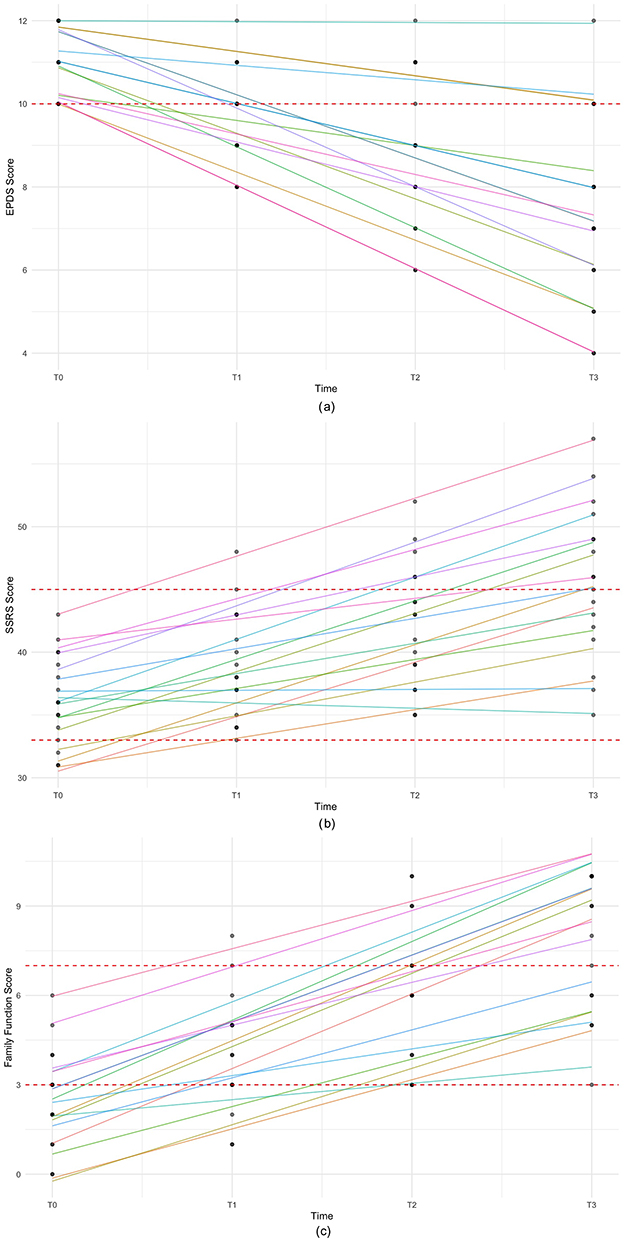 |
Figure 4 The growth curve of the outcome variables from baseline to T3. (a) EPDS score trajectory from baseline to T3. (b) SSRS score trajectory from baseline to T3. (c) Family APGAR score trajectory from baseline to T3. |
Correlation Analysis
Improvements in depressive symptoms were negatively correlated with increases in social support (r = −0.931, p <0.001, BF10 = 16,031.73) and family function (r = −0.680, p <0.01, BF10 = 14.70), while improvements in social support and family function were positively correlated (r = 0.791, p <0.001, BF10 = 97.74). (Figure 5).
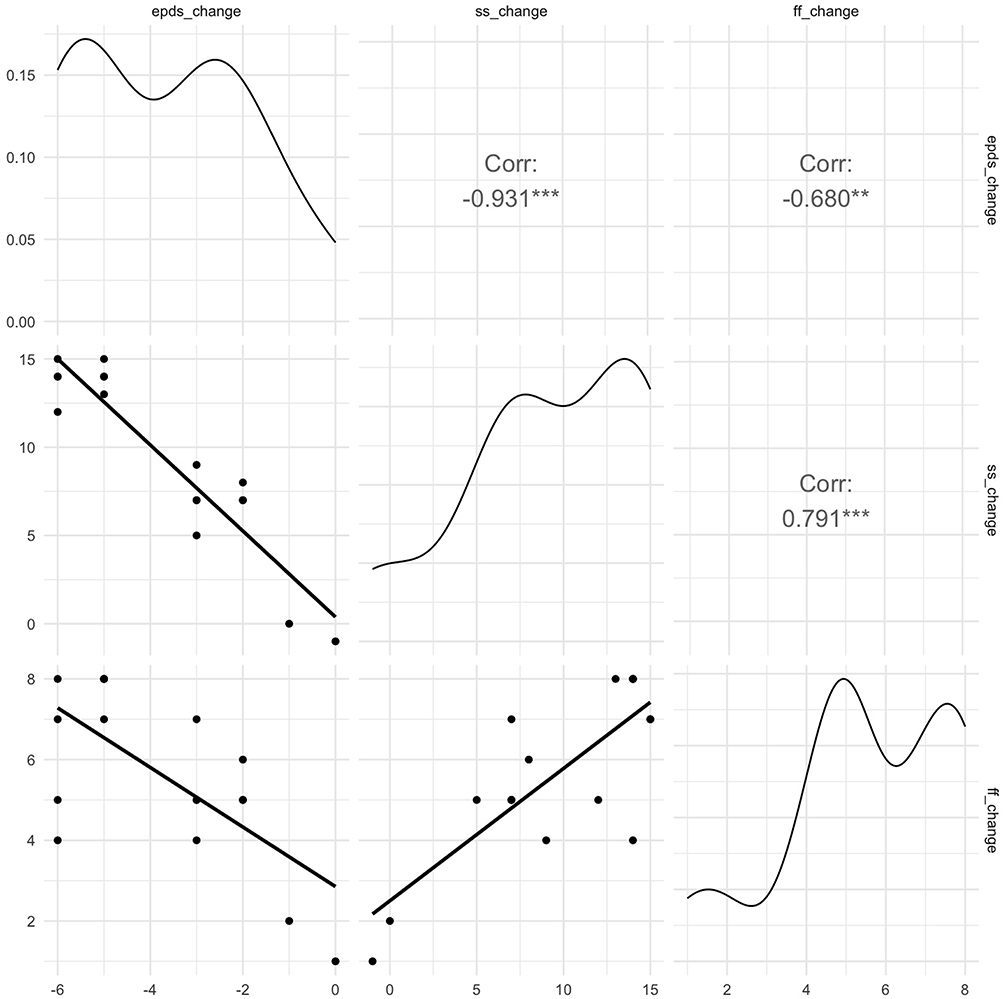 |
Figure 5 Scatterplot matrix of change in outcome variables. Notes: Lower triangle = scatterplots with linear trend line; upper triangle = Pearson correlation coefficients, **p <0.01, ***p <0.001; Along the diagonal = Density plots. |
Between-Group Differences
Estimated Marginal Means Analysis
Compared with the control group (TAU), the intervention group (IPT) demonstrated significant advantages across multiple outcomes (Table 5 and Figure 6). Specifically, EPDS scores were significantly lower at T2 (Δ = −2.12, 95% HDI [−3.29, −0.90]) and T3 (Δ = −3.62, 95% HDI [−4.98, −2.20]); social support was significantly higher at T3 (Δ = 5.81, 95% HDI [1.69, 9.73]); and family function improved significantly at T2 (Δ = 1.91, 95% HDI [0.48, 3.40]) and T3 (Δ = 3.63, 95% HDI [2.36, 4.85]). In addition, the risk of perinatal depression (PND) was significantly reduced at T3 (log-odds Δ = −3.75, 95% HDI [−6.23, −1.37]).
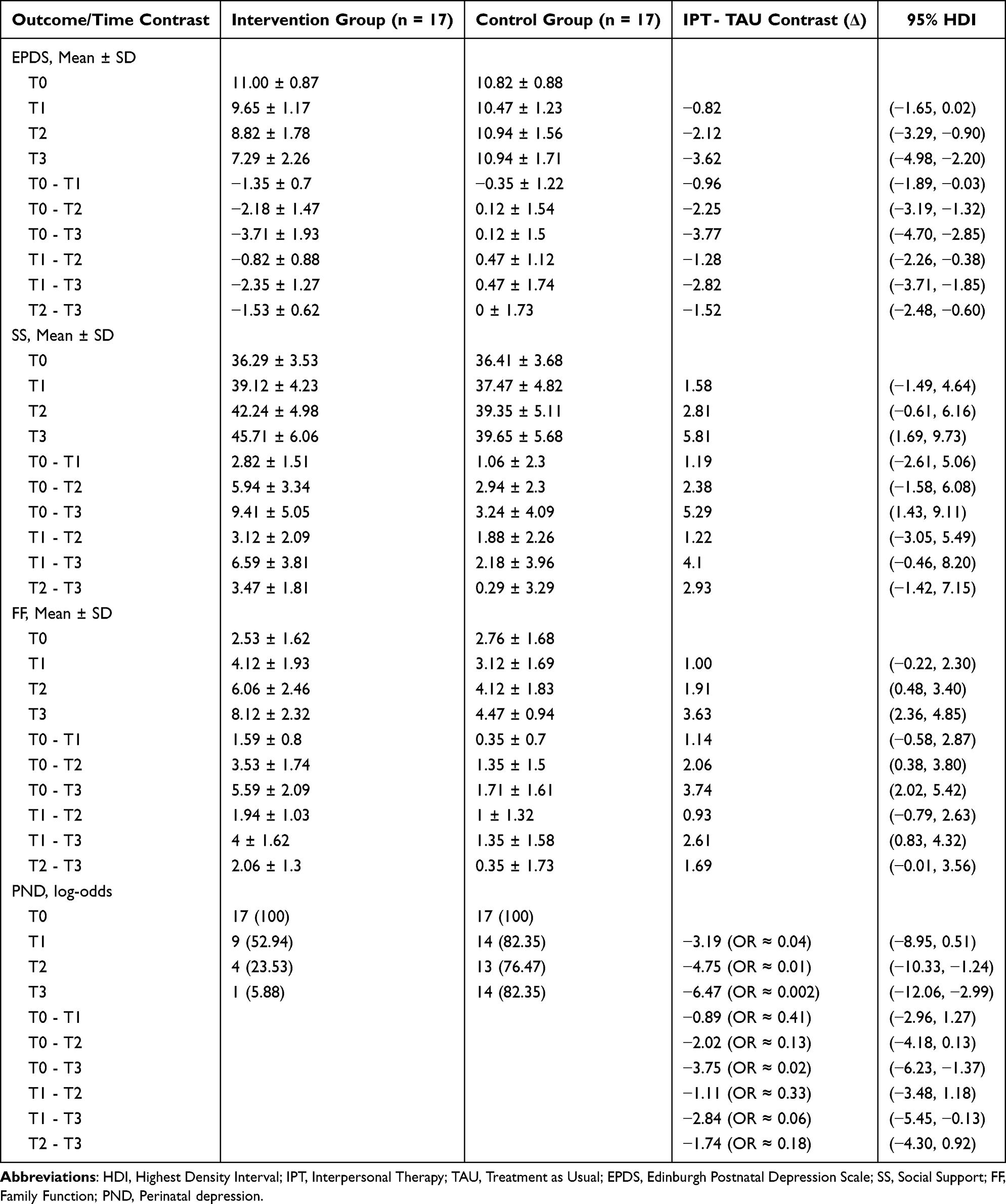 |
Table 5 Bayesian Between-Group Comparisons at Different Time Points |
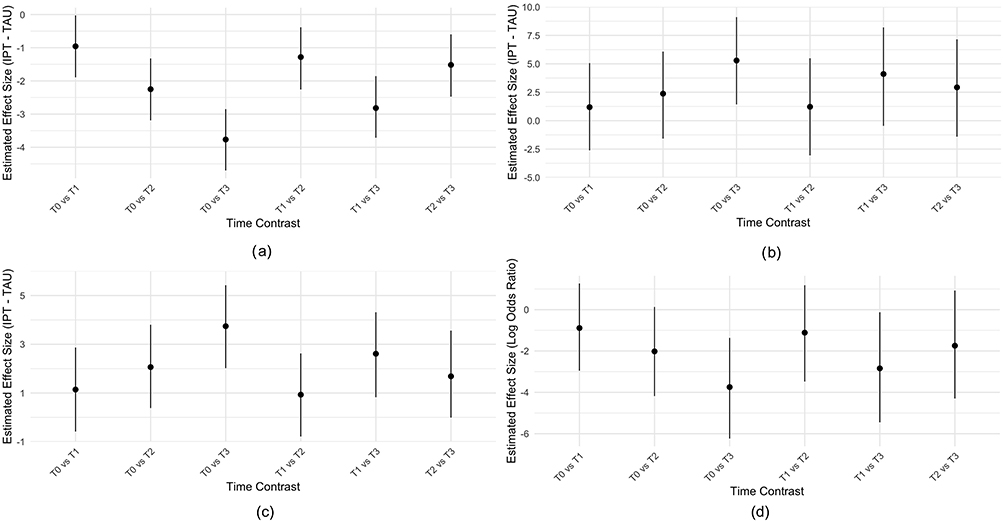 |
Figure 6 Between-group comparisons at different time points. (a) Between-group comparison of EPDS scores. (b) Between-group comparison of SSRS scores. (c) Between-group comparison of Family APGAR scores. (d) Between-group comparison of depression rate. Abbreviations: IPT, Interpersonal psychotherapy group; TAU, Treat as Usual group; EPDS, Edinburgh Postnatal Depression Scale; APGAR, APGAR Index; SSRS, Social Support Rating Scale. |
Bayesian Modeling Validation
Bayesian mixed-effects models further confirmed these findings (Table 6 and Figure 7). Improvements in depressive symptoms emerged immediately post-intervention (Mdn = −0.96, 95% CI [−1.90, −0.03]) and strengthened at T2 (Mdn = −2.25, 95% CI [−3.18, −1.31]) and T3 (Mdn = −3.77, 95% CI [−4.67, −2.81]). Social support showed a significant advantage for IPT at T3 (Mdn = 5.29, 95% CI [1.45, 9.14]), while family function improved significantly at both T2 (Mdn = 2.06, 95% CI [0.37, 3.79]) and T3 (Mdn = −3.77, 95% CI [2.05, 5.46]). The incidence of PND was markedly reduced in the IPT group at T3 (OR = 0.02, 95% CI [0.002, 0.25]). Model diagnostics demonstrated excellent convergence (Ř ≈ 1.000; ESS > 3000), ensuring robust estimation. Collectively, Bayesian results corroborated the EMM analyses and reinforced the statistical and clinical significance of IPT effects.
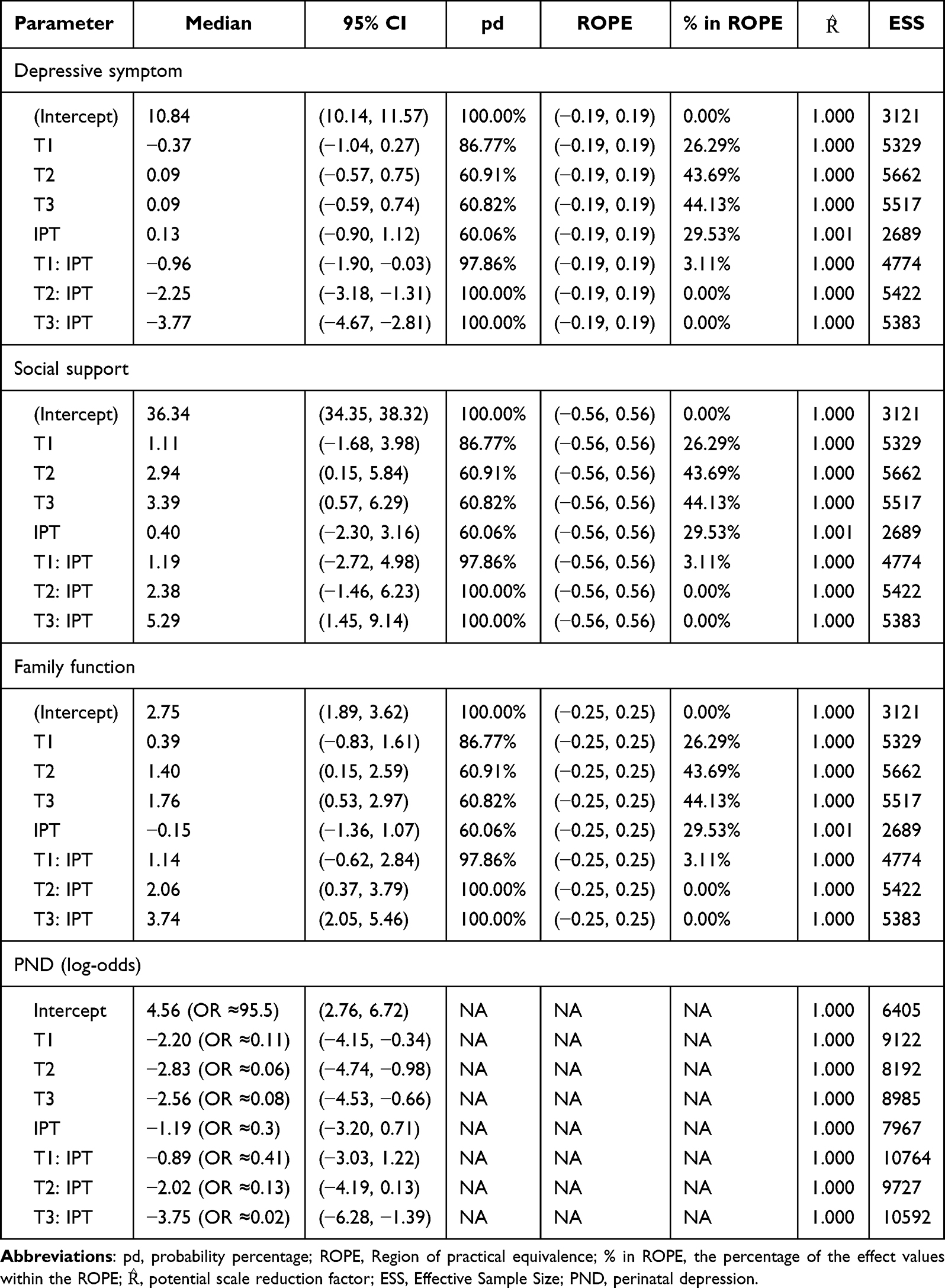 |
Table 6 Bayesian Model Parameter Posterior Distributions |
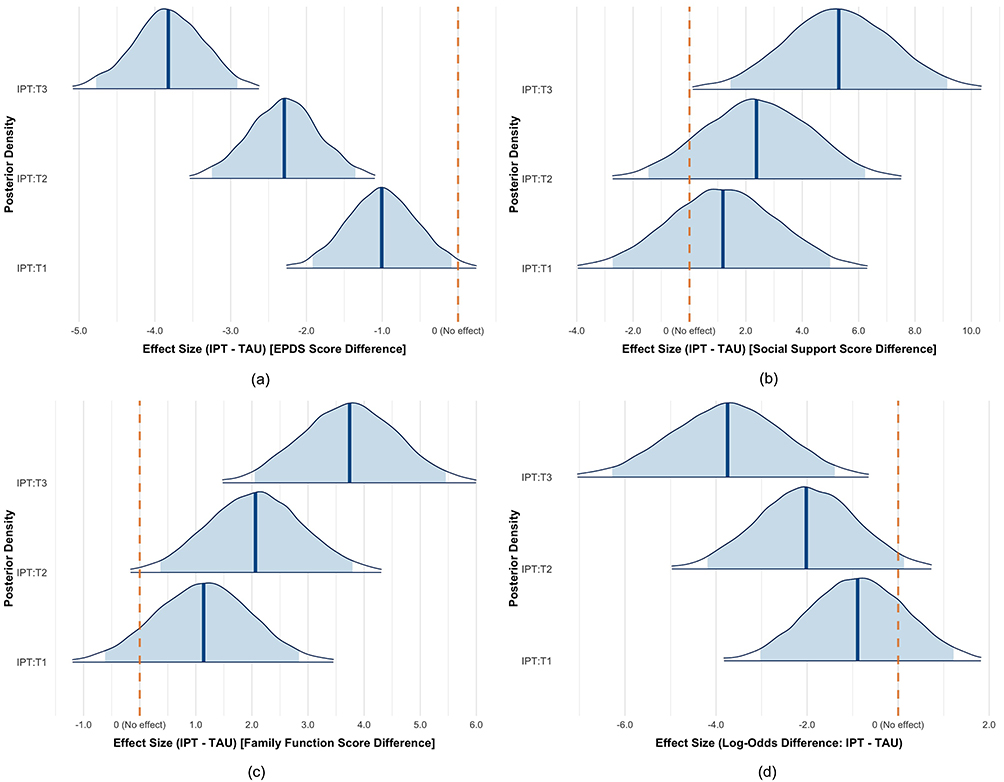 |
Figure 7 Posterior distributions of differences between IPT and TAU groups across time points (T1-T3). (a) Posterior distributions of group differences in EPDS scores. (b) Posterior distributions of group differences in SSRS scores. (c) Posterior distributions of group differences in Family APGAR scores. (d) Posterior distributions of group differences in depression rate. Abbreviations: IPT, Interpersonal psychotherapy group; TAU, Treat as Usual group; EPDS, Edinburgh Postnatal Depression Scale; PND, Perinatal depression; T1, Post-intervention; T2, 7-day postpartum; T3, 42-day postpartum. |
Discussion
Principal Findings and Overall Interpretation
This study provides preliminary evidence that a culturally optimized interpersonal psychotherapy (IPT) is both feasible and effective for rural perinatal women in China. The results confirmed all three hypotheses, showing that optimized IPT was feasible and acceptable, that participants in the intervention group experienced significant within-group improvements in depressive symptoms, social support, and family functioning, and that these improvements were significantly greater than those observed in the control group. These findings are consistent with prior research demonstrating the benefits of IPT for perinatal depression in other setting.23,26,27
Feasibility and Acceptability in the Rural Chinese Context
The high adherence (94.1%) and satisfaction rates observed in this study indicate that optimized IPT was well accepted and feasible to implement within rural maternal healthcare systems. This aligns with previous pilot trials reporting that flexible, community-based IPT delivery improves participation among women in low-resource settings.23 The cultural adaptations in the present study, such as scheduling intervention after prenatal sessions, providing individual rather than group sessions, and maintaining communication via WeChat, enhanced engagement by reducing travel and childcare barriers, similar to findings from telehealth-based IPT interventions in rural areas.35 Moreover, the inclusion of family-related psychoeducation increased perceived relevance, reflecting findings that culturally contextualized interventions yield better engagement.27
Clinical Effects and Mechanisms of Optimized IPT
Within the intervention group, depressive symptoms decreased significantly after treatment, accompanied by improvements in social support and family functioning. These results echo those from previous IPT studies showing that improvements in interpersonal relationships mediate reductions in depressive symptoms.36 The mechanisms underlying these outcomes likely involve strengthened emotional communication, expanded support networks, and improved adaptation to role transitions, all of which reduce interpersonal stress. Similar mechanisms have been observed in studies of perinatal women, where IPT reduced conflict and improved coping during partner and family transitions.23,37 In this study, IPT sessions encouraged participants to articulate needs and seek help from partners, in-laws, and peers, which may have fostered more stable family environments. This aligns with another study, which found that interpersonal communication training significantly improved spousal support and reduced perinatal stress among rural Chinese mothers.38,39
Comparative Insights and Cultural Adaptation
Compared with the control group, the IPT group exhibited greater reductions in depressive symptoms and stronger gains in social support and family functioning. This superiority is consistent with prior comparative studies showing that IPT outperforms usual care in improving psychosocial functioning.26,27,40 Optimized IPT addressed local stressors such as intergenerational household tensions and postpartum confinement practices (“doing the month”). Previous work has shown that the quality of family interactions during “doing the month” determines whether it is protective or stressful.36,41 By improving communication and resolving conflicts with mothers-in-law or spouses, optimized IPT likely transformed these culturally embedded experiences into sources of support rather than distress. This interpretation is consistent with Yang and Yu,42 who reported that family-centered interventions enhance emotional regulation and family harmony among postpartum women in similar rural settings.
Strengths and Limitations
This study has several strengths. It addresses an underserved population, applies culturally optimized IPT, and employs Bayesian modeling to enhance the robustness of findings. The high adherence and satisfaction rates further support feasibility. However, several limitations should be noted. First, the follow-up period was limited to 42 days postpartum, preventing assessment of long-term outcomes. Second, TAU served as the control condition rather than another evidence-based psychotherapy, which limits comparisons across interventions. Third, reliance on self-report measures may introduce bias. Future studies should include longer-term follow-up, objective assessments, and replication in diverse populations.
Despite these limitations, the current findings provide preliminary support for IPT as a feasible, effective, and culturally sensitive intervention for PND in rural China. Future research should investigate the durability of IPT effects beyond the early postpartum period and examine how family or peer-based adaptations may enhance outcomes further. Such work will be crucial to inform scalable strategies that address the substantial burden of perinatal depression in underserved populations.
Conclusion
This study demonstrates that a culturally optimized IPT can be feasibly implemented and well accepted among rural perinatal women in China. The adapted intervention was associated with reductions in depressive symptoms and improvements in social support and family functioning, suggesting meaningful psychosocial benefits within this context. By integrating IPT principles with local cultural practices and healthcare routines, the study highlights the value of culturally responsive approaches to perinatal mental health care. The findings contribute to the growing evidence supporting contextually tailored psychological interventions for underserved populations and provide a foundation for future large-scale trials to strengthen community-based maternal mental health services.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the two corresponding authors on reasonable request.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki and was reviewed and approved by the Ethics Committee of Medical Research Committee of Medical College of Wuhan University (WHU-LFMD-IRB2024045) and the Renmin Hospital of Wuhan University (WDRY2024-K196). Written informed consent was secured from all participants.
Acknowledgments
The authors want to give their sincere thanks to all the participants and the obstetrical professionals involved in the study.
Author Contributions
Rong Wang and Shi-Yun Wang are the co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed that the research has been funded by the Health Bureau of Songzi City (Project NO.HBSSZSHLZX0003).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Kee MZL, Cremaschi A, De Iorio M, et al. Perinatal trajectories of maternal depressive symptoms in prospective, community-based cohorts across 3 continents. JAMA Network Open. 2023;6(10):e2339942. doi:10.1001/jamanetworkopen.2023.39942
2. Pampaka D, Papatheodorou SI, AlSeaidan M, et al. Antenatal depressive symptoms and adverse perinatal outcomes. BMC Pregnancy Childbirth. 2021;21(1):313. doi:10.1186/s12884-021-03783-9
3. Smythe KL, Petersen I, Schartau P. Prevalence of perinatal depression and anxiety in both parents: a systematic review and meta-analysis. JAMA Network Open. 2022;5(6):e2218969. doi:10.1001/jamanetworkopen.2022.18969
4. Rogers A, Obst S, Teague SJ, et al. Association between maternal perinatal depression and anxiety and child and adolescent development: a meta-analysis. JAMA Pediatr. 2020;174(11):1082–19. doi:10.1001/jamapediatrics.2020.2910
5. Al-Abri K, Edge D, Armitage CJ. Prevalence and correlates of perinatal depression. Soc Psychiatry Psychiatr Epidemiol. 2023;58(11):1581–1590. doi:10.1007/s00127-022-02386-9
6. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affect Disord. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
7. Qi W, Liu Y, Lv H, et al. Effects of family relationship and social support on the mental health of Chinese postpartum women. BMC Pregnancy Childbirth. 2022;22(1):65. doi:10.1186/s12884-022-04392-w
8. Masters C, Lewis JB, Hagaman A, et al. Discrimination and perinatal depressive symptoms: the protective role of social support and resilience. J Affect Disord. 2024;354:656–661. doi:10.1016/j.jad.2024.03.039
9. Casu G, de Padua Serafim A, Zaia V, Gremigni P. Editorial: measurement in health psychology. Front Psychol. 2022;13:937700. doi:10.3389/fpsyg.2022.937700
10. Xiao SY. Impact of social support on physical and mental health. Chin J Mental Health. 1987;04:183–187.
11. Tsai SY. Perinatal depressive symptoms among pregnant employees in Taiwan. Int J Environ Res Public Health. 2023;20(4). doi:10.3390/ijerph20043354
12. Seymour-Smith M, Cruwys T, Haslam SA. More to lose? Longitudinal evidence that women whose social support declines following childbirth are at increased risk of depression. Aust N Z J Public Health. 2021;45(4):338–343. doi:10.1111/1753-6405.13099
13. Zhang L, Ren L, Li H, et al. The effects of maternal health literacy, family functioning and self-efficacy on antepartum depression in pregnant women in China: a moderated mediation model. Bmc Psychiatry. 2025;25(1):101. doi:10.1186/s12888-025-06557-1
14. He M, Cabrera N, Renteria J, et al. Family functioning in the time of COVID-19 among economically vulnerable families: risks and protective factors. Front Psychol. 2021;12:730447. doi:10.3389/fpsyg.2021.730447
15. Guerrero-Munoz D, Salazar D, Constain V, Perez A, Pineda-Canar CA, Garcia-Perdomo HA. Association between family functionality and depression: a systematic review and meta-analysis. Korean J Fam Med. 2021;42(2):172–180. doi:10.4082/kjfm.19.0166
16. Desta M, Memiah P, Kassie B, et al. Postpartum depression and its association with intimate partner violence and inadequate social support in Ethiopia: a systematic review and meta-analysis. J Affect Disord. 2021;279:737–748. doi:10.1016/j.jad.2020.11.053
17. Xiao J, Xiong R, Wen Y, et al. Antenatal depression is associated with perceived stress, family relations, educational and professional status among women in South of China: a multicenter cross-sectional survey. Front Psychiatry. 2023;14:1191152. doi:10.3389/fpsyt.2023.1191152
18. Qi W, Zhao F, Liu Y, Li Q, Hu J. Psychosocial risk factors for postpartum depression in Chinese women: a meta-analysis. BMC Pregnancy Childbirth. 2021;21(1):174. doi:10.1186/s12884-021-03657-0
19. Klerman GL, Dimascio A, Weissman M, Prusoff B, Paykel ES. Treatment of depression by drugs and psychotherapy. Am J Psychiatry. 1974;131(2):186–191. doi:10.1176/ajp.131.2.186
20. Markowitz JC, Weissman MM. Interpersonal psychotherapy: principles and applications. World Psychiatry. 2004;3(3):136–139.
21. Jiang X, Li H, Wang D, Shan L, Wang F, Kang Y. Efficacy of nondrug interventions in perinatal depression: a meta-analysis. Psychiatry Res. 2022;317:114916. doi:10.1016/j.psychres.2022.114916
22. Bright KS, Charrois EM, Mughal MK, et al. Interpersonal psychotherapy to reduce psychological distress in perinatal women: a systematic review. Int J Environ Res Public Health. 2020;17(22). doi:10.3390/ijerph17228421
23. Grote NK, Lohr MJ, Curran MC, Cristofalo M. Change mechanisms in brief interpersonal psychotherapy for women with perinatal depression: qualitative study. Am J Psychother. 2021;74(3):112–118. doi:10.1176/appi.psychotherapy.20200039
24. Li MN, Duan XR. Application research of interpersonal psychological intervention focusing on family relationship in postpartum depression patients. Med Theor Pract. 2024;37(01):158–161.
25. Dennis CL, Grigoriadis S, Zupancic J, Kiss A, Ravitz P. Telephone-based nurse-delivered interpersonal psychotherapy for postpartum depression: nationwide randomised controlled trial. Br J Psychiatry. 2020;216(4):189–196. doi:10.1192/bjp.2019.275
26. Miniati M, Marzetti F, Palagini L, et al. Telephone-delivered interpersonal psychotherapy: a systematic review. CNS Spectr. 2023;28(1):16–28. doi:10.1017/S1092852921000948
27. Ngai FW, Gao LL. Effect of couple-based interpersonal psychotherapy on postpartum depressive symptoms: a randomised controlled trial. Asian J Psychiatr. 2022;78:103274. doi:10.1016/j.ajp.2022.103274
28. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/s0033291702006074
29. Lau Y, Wang Y, Yin L, Chan KS, Guo X. Validation of the Mainland Chinese version of the edinburgh postnatal depression scale in chengdu mothers. Int J Nurs Stud. 2010;47(9):1139–1151. doi:10.1016/j.ijnurstu.2010.02.005
30. Jin YZPT, Wang L, Zhang Q. Discussion on screening criteria and incidence factors of postpartum depression. Maternal Child Health Care China. 1995;05:3.
31. First MBW, W JB, Karg RS, Spitzer RL. Structured Clinical Interview for DSM-5® Disorders—Clinician Version (SCID-5-CV). American Psychiatric Association; 2016.
32. Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25(3):1057–1073. doi:10.1177/0962280215588241
33. Wang Y, Guo X, Lau Y, Chan KS, Yin L, Chen J. Psychometric evaluation of the Mainland Chinese version of the edinburgh postnatal depression scale. Int J Nurs Stud. 2009;46(6):813–823. doi:10.1016/j.ijnurstu.2009.01.010
34. Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978;6(6):1231–1239.
35. Xie H, Cong S, Wang R, et al. Effect of eHealth interventions on perinatal depression: a meta-analysis. J Affect Disord. 2024;354:160–172. doi:10.1016/j.jad.2024.03.027
36. Li WY, Ding L, Tang YY. Effect of interpersonal psychotherapy on postpartum mental state and incidence of postpartum depression in primipara. Psychological Monthly. 2024;10(19):134–137. doi:10.19738/j.cnki.psy.2024.10.037
37. He L, Soh KL, Yu J, Chen A, Dong X. Effect of family-centered interventions for perinatal depression: an overview of systematic reviews. Front Psychiatry. 2023;14:1094360. doi:10.3389/fpsyt.2023.1094360
38. Zhou F, Wu J, Wang L, et al. Associations between antenatal depressive symptoms in different trimesters and perinatal outcomes: a prospective multicenter cohort study in China. Asian J Psychiatr. 2024;100:104165. doi:10.1016/j.ajp.2024.104165
39. Dietz LJ. Family-Based interpersonal psychotherapy: an intervention for preadolescent depression. Am J Psychother. 2020;73(1):22–28. doi:10.1176/appi.psychotherapy.20190028
40. Bian C, Zhao WW, Yan SR, Chen SY, Cheng Y, Zhang YH. Effect of interpersonal psychotherapy on social functioning, overall functioning and negative emotions for depression: a meta-analysis. J Affect Disord. 2023;320:230–240. doi:10.1016/j.jad.2022.09.119
41. Ding G, Niu L, Vinturache A, et al. “Doing the month” and postpartum depression among Chinese women: a Shanghai prospective cohort study. Women Birth. 2020;33(2):e151–e158. doi:10.1016/j.wombi.2019.04.004
42. Yang Y, Yu M. Disparities and determinants of maternal health services utilization among women in poverty-stricken rural areas of China: a cross-sectional study. BMC Pregnancy Childbirth. 2023;23(1):115. doi:10.1186/s12884-023-05434-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.