Back to Journals » Clinical Interventions in Aging » Volume 18
Cross-Sectional Study on the Association Between Respiratory Muscle Strength and Dynapenic Abdominal Obesity in Community-Dwelling Older Adults
Authors Pereira LN, Pegorari MS ![]() , Patrizzi LJ, de Walsh IAP, Silva CFR, da Silva JS, Matos AP, Pinto ACPN, Ohara DG
, Patrizzi LJ, de Walsh IAP, Silva CFR, da Silva JS, Matos AP, Pinto ACPN, Ohara DG
Received 5 March 2023
Accepted for publication 7 August 2023
Published 16 August 2023 Volume 2023:18 Pages 1351—1359
DOI https://doi.org/10.2147/CIA.S411170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Larissa do Nascimento Pereira,1 Maycon Sousa Pegorari,2– 4 Lislei Jorge Patrizzi,2,3 Isabel Aparecida Porcatti de Walsh,2,3 Caroline de Fátima Ribeiro Silva,1 Juliana de Souza da Silva,4 Areolino Pena Matos,1,4 Ana Carolina Pereira Nunes Pinto,1,5– 7 Daniela Gonçalves Ohara2
1Department of Biological and Health Sciences, Federal University of Amapá, Macapá, AP, Brazil; 2Department of Applied Physiotherapy, Federal University of Triângulo Mineiro, Uberaba, Minas Gerais, Brazil; 3Postgraduate Program in Physical Therapy, Federal University of Triângulo Mineiro, Uberaba, Minas Gerais, Brazil; 4Postgraduate Program in Health Sciences, Federal University of Amapá, Macapá, AP, Brazil; 5Iberoamerican Cochrane Centre - Biomedical Research Institute Sant Pau (IIB Sant Pau), Barcelona, Spain; 6Cochrane Brazil, Center for Evidence-Based Health Studies and Health Technology Assessment, Sao Paulo, Brazil; 7Department of Medicine, Evidence-Based Health Post-Graduation Program, Federal University of São Paulo, Sao Paulo, Brazil
Correspondence: Maycon Sousa Pegorari, Department of Applied Physiotherapy, Federal University of Triângulo Mineiro, Boulevard Frei Paulino, n° 30, Abadia, Uberaba, Minas Gerais, 38025-180, Brazil, Email [email protected]; [email protected]
Purpose: Impaired respiratory muscle strength has been associated with some geriatric syndromes. However, no studies have previously evaluated the relationship between respiratory muscle strength and dynapenic abdominal obesity. This study aimed to analyze whether there is an association between respiratory muscle strength and abdominal obesity, dynapenia and dynapenic abdominal obesity (DAO) in community-dwelling older adults.
Patients and Methods: Cross-sectional study conducted with community-dwelling older adults (n=382 / 70.03 ± 7.3 years) from Macapá, Amapá, Brazil. Respiratory muscle strength was assessed by measuring maximal inspiratory and expiratory pressures (MIP and MEP, respectively), using an analog manovacuometry. DAO was defined as the combination of dynapenia (grip strength < 26 kgf for men and < 16 kgf for women) and abdominal obesity (abdominal circumference > 102 cm for men and > 88 cm for women). We performed descriptive and inferential statistical analyses using the student’s t-test for independent and related samples and linear regression model.
Results: Older adults with abdominal obesity, dynapenia, and DAO presented lower mean values (obtained and obtained versus predicted; except abdominal obesity versus MIP) for maximal respiratory pressures compared to individuals without these conditions. However, the adjusted analysis only indicated an association between MIP and the following conditions: dynapenia (MIP - β =− 0.171; p< 0.001), abdominal obesity (MIP - β=0.102; p=0.042), and DAO (MIP - β=− 0.101; p=0.028).
Conclusion: Older adults with abdominal obesity, dynapenia, and DAO showed impaired maximal respiratory pressures. The results of the adjusted analysis indicate that inspiratory muscle strength may require greater attention by health professionals aiming at preventing respiratory complications and improving respiratory health care in older people with these conditions.
Keywords: respiratory muscles, muscle strength, respiratory function tests, obesity, abdominal, aged
Introduction
The aging process can lead to changes in body composition, with an increase in the percentage of body fat and a decrease in global muscle mass, with important consequences on strength and physical performance.1 Regarding the distribution of body fat, older people may present abdominal obesity (AO) and intramuscular fat deposition.2 AO has a high prevalence in older adults, ranging from 16.15% to 54.2%, and is associated with increased susceptibility to the development of cardiovascular, metabolic, cancer, and other diseases.3 In addition, AO is associated with increased functional limitations and worse quality of life.4
Another common condition in older adults is dynapenia, which is characterized by the reduction in peripheral muscle strength associated with aging (not as a consequence of muscle or neurological diseases).5 The prevalence of dynapenia varies from 25.1% to 30.9% in developed and developing countries, respectively.3 In isolation, dynapenia and AO are associated with impairments in physical function in older adults and, when these conditions coexist, the impairments can be potentiated, which is defined as dynapenic abdominal obesity (DAO).6
DAO may be associated with negative outcomes, such as functional decline, increased risk of falling, prolonged hospital stays, higher health care costs, and mortality.7,8 In recent years, the repercussions of obesity on respiratory function have been studied, showing that this condition can lead to respiratory muscle weakness4 and lung function decline9,10 in the long term. Thus, it is suggested that AO, when associated with dynapenia, may further impair respiratory muscle strength.4,11 Of note, both dynapenia and AO are closely related to modifiable factors including the reduction of muscle strength and obesity. Therefore, the early identification of subjects with DAO can allow for management in a timely fashion and prevent the development of adverse outcomes.12
Some studies have demonstrated an association between respiratory muscle strength and dynapenia in specific populations. For instance, a previous study showed an association between respiratory muscle strength and dynapenia.13 In that study, dynapenic older adults with chronic obstructive pulmonary disease (COPD) had lower maximal respiratory pressure values when compared to non-dynapenic older adults with COPD.13 However, to our knowledge, no studies have been published that assess possible associations between DAO and respiratory muscle strength, as well as their repercussions on the respiratory system in community-dwelling older adults, mainly without any previous respiratory conditions, thus requiring further investigation. Understanding the association between dynapenia, AO and DAO and respiratory muscle strength represent an important knowledge base that may help provide a better clinical management of these older people in the future. Therefore, the aim of this study was to analyze whether there is an association between respiratory muscle strength, AO, dynapenia, and DAO in community-dwelling older adults.
Materials and Methods
Study Design and Population
This is a cross-sectional study developed in the urban area of Macapá, in 2017, with community-dwelling older adults. Macapá is a municipality in the Amazon region, capital of the state of Amapá, in the north of Brazil. The sample size calculation considered a prevalence of health problems in 50% of the elderly population, accuracy of 5%, and a 95% confidence interval for a finite population of 19,955 elderly, reaching a minimum required sample of 377 subjects. Information on sample size calculation and population characteristics are available in a previous study.14
Eligibility Criteria
We included older adults living in the urban area of Macapa, aged 60 years or older who agreed to participate in the study, and were able to walk. We excluded those that moved to another city, that could not be located after three attempts by the interviewer, presented cognitive decline, who had neurological sequelae and/or were hospitalized, and/or conditions that would make it impossible for them to carry out the assessments. We excluded individuals if they had any medical conditions contraindicated for assessing respiratory muscle strength15 (Figure 1). Thus, 382 older adults (Figure 1), of both sexes participated in this study. This study was approved by the Research Ethics Committee of the Federal University of Amapá, opinion no. 1,738,671, and all individuals signed informed consent before commencing their participation. This research followed the ethical principles present in the Helsinki Declaration.
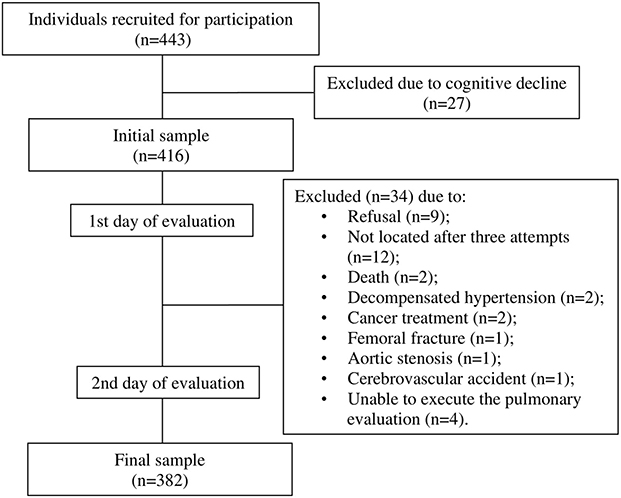 |
Figure 1 Flow diagram representing the loss of the sample and final sample composition. |
Instruments and Measures of Assessment
Respiratory Muscle Strength
We assessed respiratory muscle strength using manovacuometry to obtain maximal respiratory pressure values (MIP and MEP), which reflect the strength of the inspiratory and expiratory muscles, respectively.16 For these measurements, we used a properly calibrated manovacuometer, containing a rigid plastic mouthpiece, a plastic trachea, and a leak hole (2 mm in diameter), which was used to prevent pressure increase in the oral cavity after the contraction of the face and oropharynx muscles.17
Measurements were taken in the sitting position using a nose clip.18 The MIP was obtained from a maximum inspiratory effort preceded by a maximum expiration close to the residual volume (RV), while for MEP, a maximum inspiration was performed close to the total lung capacity (TLC), followed by a maximum expiratory effort.17 A minimum of three and a maximum of five maneuvers were performed. The evaluation was considered valid when three acceptable measurements (pressure sustained for at least one second) and two reproducible measurements (variation equal to or less than 10% of the highest value) were obtained. We considered the highest value obtained for the analyses.18,19
Dynapenia
To measure muscle strength, handgrip strength was assessed using a SAEHAN® Hydraulic Hand Dynamometer model SH5001, following the recommendations of the American Society of Hand Therapists.20 Three measurements were obtained, with a one-minute interval, and the mean value of the measurements was considered for the analyses. We determined the presence of dynapenia by adopting cut-off points for handgrip strength: we considered as reduced muscle strength values < 16 kgf for women and < 26 kilograms/force (kgf) for men.21
Abdominal Obesity
Waist circumference was measured at the end of expiration with the abdomen relaxed using an inelastic tape measure, placed at the midpoint between the iliac crest and the last rib. For the measurement, the subject remained in an upright position, with the arms relaxed along the body and with the region of the measurement free of clothes.22 Abdominal obesity was defined by waist circumference, being characterized as present when > 102 cm for men and > 88 cm for women.23
Dynapenic Abdominal Obesity
DAO was defined by the combination of cut-off points for handgrip muscle strength (< 26 kgf for men and < 16 kgf for women)21 and waist circumference (> 102 cm for men and > 88 cm for women).23
Adjustment Variables
We considered age, sex, smoking status, level of physical activity, and number of medications and diseases24 as adjustment variables. The long version of the International Physical Activity Physical Activity Questionnaire (IPAQ) for Brazilian older adults25,26 as used to measure physical activity intensity, determined based on the amount of moderate (MPA) and vigorous physical activity (VPA) practiced for at least 10 minutes continuously during a typical week day and in different domains. This variable was then dichotomized in: sufficiently active (> 150 min/week of MPA, 75 min/week of VPA or a combination of both); and insufficiently active.27
Statistical Analysis
We performed the statistical analysis using descriptive analysis (absolute numbers, and percentages, and means and standard deviations). We performed bivariate analysis for the continuous variables, using the student’s t-test - independent and related samples were used to compare values obtained, obtained versus predicted between the groups with AO, dynapenia, DAO, and without any of these conditions. We used the chi-square test for the categorical variables; and crude and multivariable through multiple linear regression, to verify the association between the variables of maximum respiratory pressures, AO, dynapenia, and AO. Significance of p < 0.05 and a 95% confidence interval (CI) were considered. The minimum necessary prerequisites were considered, including residual analysis (normality, homoscedasticity, and linearity) and multicollinearity. Data analyses were performed using the Statistical Package for Social Sciences (SPSS), version 21.0.
Results
After considering the inclusion and exclusion criteria, a total of 382 older adults were finally included. The mean age of the participants was 70.03±7.3, being 131 males (34.3%) and 251 females (65.7%). The prevalence of AO was 65.7% (n=251), dynapenia 18.5% (n=71), and DAO 10.7% (n=41). The other sample characterization and adjustment variables are expressed in Table 1.
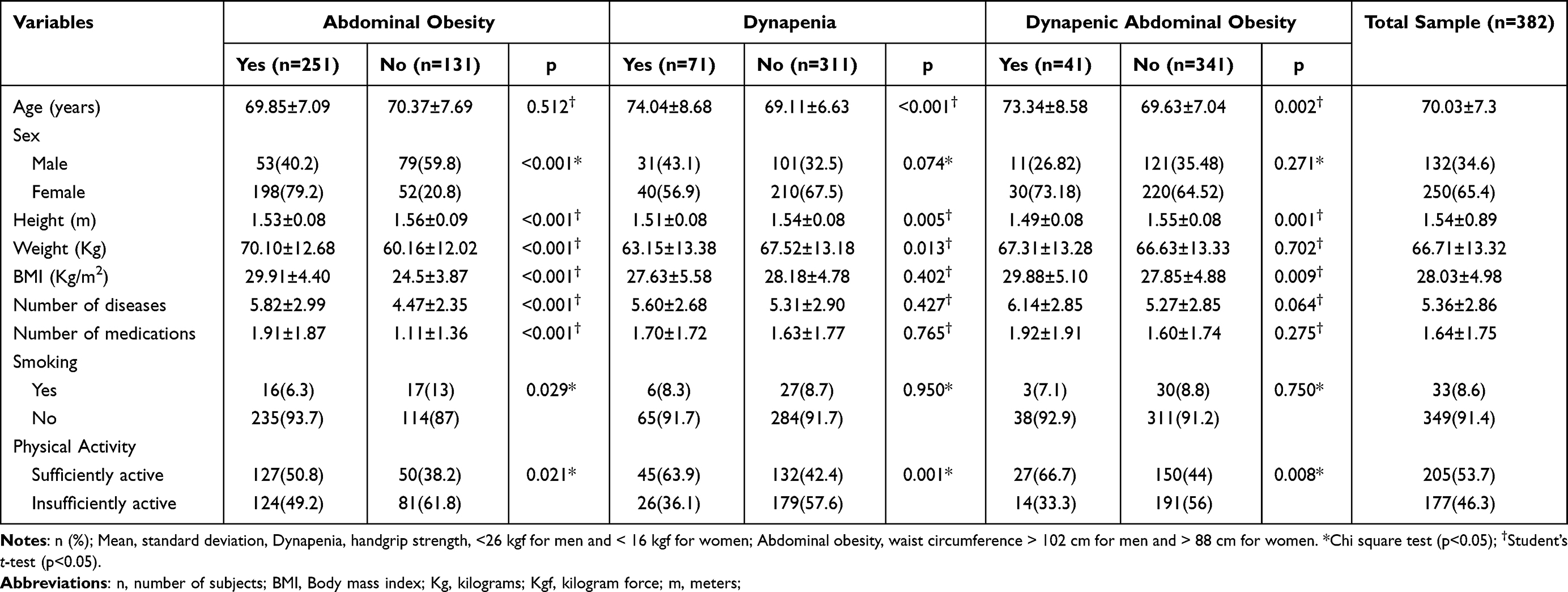 |
Table 1 Characteristics of the Older Adults According to the Conditions of Abdominal Obesity, Dynapenia, and Dynapenic Abdominal Obesity. Macapá, AP, Brazil, 2017 (n=382) |
Individuals with AO, dynapenia, and DAO obtained values of both MIP and MEP that were significantly lower than the predicted values in all groups. When comparing obtained values of MIP and MEP of individuals who had AO, dynapenia, and DAO, these values were also significantly lower than of those individuals without these conditions, except for MIP, in the AO group, in which there was no significant difference in these values (Table 2).
 |
Table 2 Comparison of Obtained, and Obtained versus Predicted Values of Maximal Respiratory Pressures According to the Presence of Abdominal Obesity, Dynapenia, and Dynapenic Abdominal Obesity Conditions. Macapá, AP, Brazil, 2017 (n= 382) |
The adjusted analysis only indicated an association between MIP and the following conditions: AO (MIP - β= 0.102; p=0.042), dynapenia (MIP - β= −0.171; p<0.001), and DAO (MIP - β= −0.101; p=0.028). In the adjusted analysis, no differences were found between groups for MEP (Table 3).
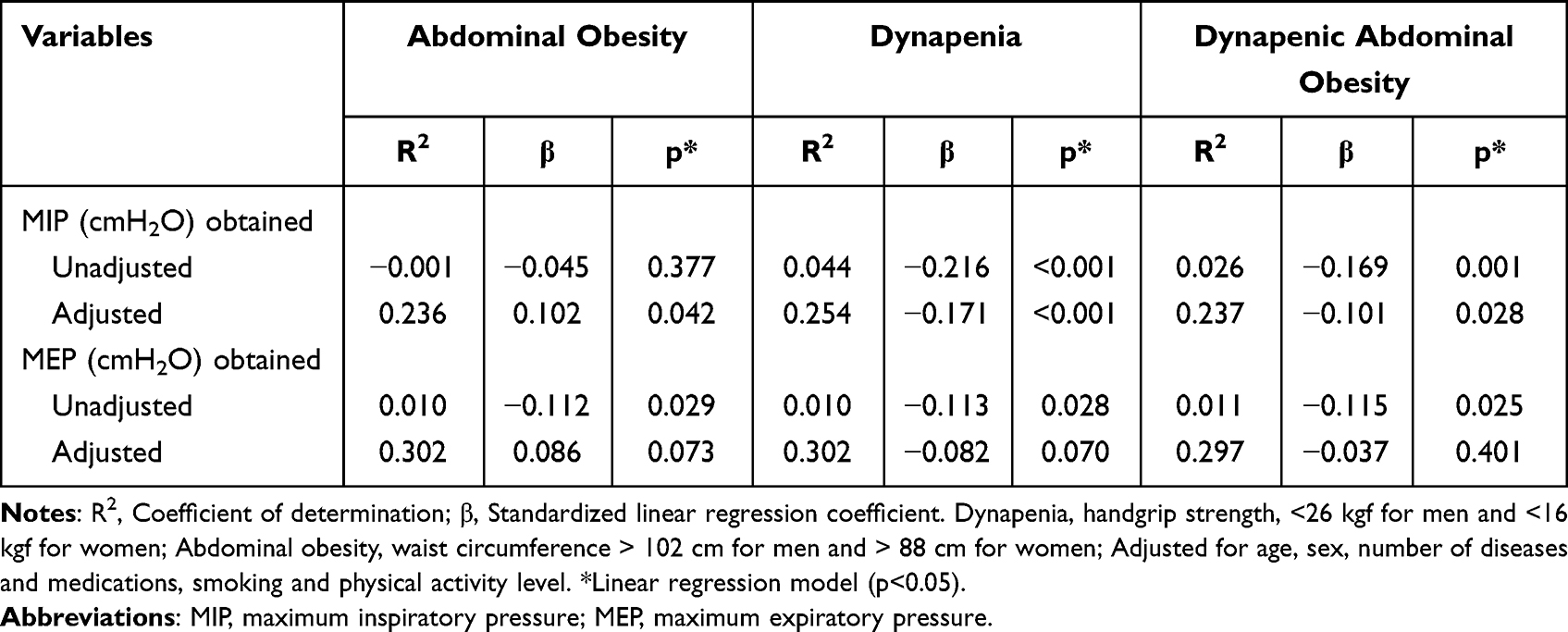 |
Table 3 Association of Maximal Respiratory Pressures According to Conditions of Abdominal Obesity, Dynapenia, and Dynapenic Abdominal Obesity. Macapá, AP, Brazil, 2017 (n= 382) |
Discussion
This is the first study to investigate possible associations between maximal respiratory pressure values and DAO in community-dwelling older adults. The results identified an inverse association between AO, dynapenia, and DAO and inspiratory muscle strength, even after adjustments. Additionally, older adults with AO, dynapenia, and DAO showed reduced inspiratory and expiratory muscle strength when compared to those without these conditions, demonstrating that respiratory muscle strength assessments may be important variables to be screened in dynapenic abdominal obesity in older populations.
The accumulation of adipose tissue, especially in the abdominal region (AO) may have consequences in several physiological systems, including the respiratory system. Previous studies demonstrated that AO may negatively influence, for example, lung function.10,28–30 Respiratory muscle weakness may be explained by the excess of adipose tissue, especially in the abdominal region, which leads to an increase in intra-abdominal pressure, and may result in changes in ventilatory mechanics, and in a mechanical disadvantage of the respiratory muscles, especially the diaphragm, which presents restricted mobility in this situation.14 During this process, the diaphragm may present functional impairment, such as in then generation of force and, consequently, suffer greater overload.4
Furthermore, excessive stretching of the diaphragm muscle fibers, and the accumulation of intra-abdominal fat may lead to the elevation of the diaphragmatic domes, reducing the contractile efficiency of the diaphragmatic muscle fibers, and leaving this muscle overloaded.4 This can result in muscle weakness in the long term and early diaphragmatic fatigue.31–33 Additionally, Souza et al34 showed in their study that inspiratory muscle weakness was found in 47.6% of subjects who presented a lower fat‐free mass percentage (p=0.017), smaller fat‐free mass index (p=0.001), greater fat mass percentage (p=0.029) and less diaphragmatic mobility (p=0.007) compared with the non-respiratory weakness group.
This hypothesis may support the results of the present study, which showed that older adults with AO presented respiratory muscle weakness (reduced MIP and MEP) when compared to those without this condition, therefore indicating that AO alone may negatively influence inspiratory and expiratory muscle strength.
On the other hand, a study by Sant’Anna35 and collaborators demonstrated that in individuals with grade 3 obesity (morbid obesity) there was no reduction in the values of either MIP or MEP when compared to non-obese individuals. However, it is noteworthy that the methodology used to measure obesity (body mass index), as well as the population were different from the present study, which may have caused these differences in the outcomes found.
Another condition frequently associated with adverse outcomes, such as functional disability, mobility decline, and deaths, is dynapenia.36,37 In recent years, dynapenia has also been associated with impaired lung function38 and reduced respiratory muscle strength.13 Ohara et al38 found an association (in the adjusted model) of dynapenia with a reduction in forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and peak expiratory flow (PEF). Mansour et al13 suggested an association between respiratory muscle strength and dynapenia, where dynapenic older adults with COPD presented significantly lower MIP and MEP values compared to non-dynapenic older adults. Our results are also in agreement with these findings, in which dynapenic older adults had lower MIP and MEP values compared to non-dynapenic older adults, suggesting that dynapenia may be associated with additional impairment of respiratory muscle strength.
Similarly, Ohara et al14 reported an association between respiratory muscle strength and sarcopenia. In that study, sarcopenic older adults had lower MIP values compared to non-sarcopenic older adults. In the present study we evaluated dynapenic, not sarcopenic, older adults. Both sarcopenia and dynapenia have loss of muscle strength as a diagnostic feature, however, unlike dynapenia, for sarcopenia, this decrease in strength is necessarily accompanied by a progressive decrease in muscle mass and is associated with poor physical performance in severe cases.39 In addition, the methods used to classify these conditions present divergences in the scientific literature, which can make comparisons between findings difficult. Despite this, we believe that there is an association between respiratory muscle strength and dynapenia, since one of the criteria for assessing sarcopenia is peripheral muscle strength.
In this sense, the study of Moon, Kong & Kim40 showed that obese older adults with low muscle mass (sarcopenic obesity) present compromised lung function (reduced FEV1 and FVC), when compared to those without this condition. Together, these findings suggest that elements related to the musculoskeletal system (muscle mass and strength) may influence respiratory variables. However, to date, no studies were found in the available literature that assess the existing relationships between respiratory muscle strength and DAO. Thus, the current study is probably the first to demonstrate these possible associations.
Some limitations of our study should be pointed out. There was a difference in the number of older males and females, which may have influenced the results, as it is known that obesity has a higher prevalence in females, and that females have lower respiratory muscle strength than males. We minimized this limitation, by adjusting the analyses not only for sex, but also for age, number of medications, number of diseases, smoking status, and physical activity level. Another limitation was that the assessment of abdominal obesity was not carried out using X-ray absorptiometry (DEXA), computed tomography (CT), and bioelectrical impedance analysis (BIA), and yes by to measure waist circumference. Therefore, in community-dwelling older adults, it is known that there are difficulties in using high-cost equipment. Thus, we chose to use a measure widely used in other studies, it is an easy, low-cost. Finally, the cross-sectional nature of our study. Therefore, it is not possible to determine any causal relationship between respiratory muscle strength and DAO and further longitudinal studies are still necessary.
Of note, our study presents a representative sample of older adults and provides information on the health condition of a population located in the Brazilian Amazon region. According to our findings, respiratory muscle strength should be included as an important component of clinical evaluations in older adult populations, as there are associations of AO, dynapenia, and DAO with negative health outcomes. This fact denotes the need for greater attention in the planning (screening, prevention, and treatment) of health care for older adults with AO, dynapenia, and DAO in order to aid early identification and treatment of decreases in respiratory muscle strength, as well as to prevent adverse health outcomes.
Conclusion
Older adults with AO, dynapenia, and DAO showed impaired respiratory muscle strength, with emphasis on inspiratory muscle strength, compared to older adults without these conditions. Furthermore, inspiratory muscle strength was associated with AO, dynapenia, and DAO.
The data may represent a starting point for investigating the impacts of dynapenia, AO and DAO on respiratory function, helping guide health professionals on the prevention and management of respiratory disorders among community-dwelling older adults. Given the clinical relevance of these factors, further longitudinal studies are needed to identify possible causal relationships between respiratory muscle strength and AO, dynapenia, and DAO.
Novelty Statement
The present study comprises the same sample and the variable of interest, which is DAO, as in another previously published study.41 However, the studies have different objectives, with different analyzes and results. For example, in the present study, the outcome of interest is respiratory muscle strength and we used some adjustment variables. In the other study, the outcome was DAO and we sought to investigate associated predictors.41
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Rossi AP, Urbani S, Fantin F, et al. Worsening disability and hospitalization risk in sarcopenic obese and dynapenic 287 abdominal obese: a 5.5 years follow-up study in elderly men and women. Front Endocrinol. 2020;288:11, 314.
2. Geirsdottir OG, Chang M, Jonsson PV, et al. Obesity, physical function, and training success in community-dwelling nonsarcopenic old adults. J Aging Res. 2019;2019:1–10. doi:10.1155/2019/5340328
3. da Cunha Leme DE. Dynapenia in middle-aged and older persons with and without abdominal obesity and the complex relationship with behavioral, physical-health and mental-health variables: learning Bayesian network structures. Clin Nutr ESPEN. 2021;42:366–372. doi:10.1016/j.clnesp.2021.01.006
4. Mafort TT, Rufino R, Costa CH, et al. Obesity: systemic and pulmonary complications, biochemical 296 abnormalities, and impairment of lung function. Multidiscip. Respir Med. 2016;11:28.
5. Manini TM, Clark BC. Dynapenia and aging: an update. J Gerontol Ser a Biol Sci Med Sci. 2012;67(1):28–40.
6. Máximo RO, Oliveira DC, Ramirez PC, et al. Combination of dynapenia and abdominal obesity affects long-term physical performance trajectories in older adults: sex differences. The. Am J Clin Nutr. 2022;115(5):1290–1299. doi:10.1093/ajcn/nqac023
7. Lee S, Sánchez GFL, Veronese N, et al. Dynapenic abdominal obesity increases risk for falls among adults aged ≥50 years: a prospective analysis of the Irish longitudinal study on ageing. J Gerontol. 2023;2023:glad104.
8. Ramírez PC, de Oliveira DC, de Oliveira Máximo R, et al. Is dynapenic abdominal obesity a risk factor for cardiovascular mortality? A competing risk analysis. Age Ageing. 2023;52(1). doi:10.1093/ageing/afac301
9. Dixon AE, Peters U. The effect of obesity on lung function. Expert Rev Respir Med. 2018;12(9):755–767. doi:10.1080/17476348.2018.1506331
10. Molani Gol R, Rafraf M. Association between abdominal obesity and pulmonary function in apparently healthy adults: a systematic review. Obes Res Clin Pract. 2021;15(5):415–424. doi:10.1016/j.orcp.2021.06.011
11. Choe EK, Kang HY, Lee Y, et al. The longitudinal association between changes in lung function and changes in abdominal visceral obesity in Korean non-smokers. PLoS One. 2018;13(2):1–10. doi:10.1371/journal.pone.0193516
12. Santos EPR, Silva CFR, Ohara DG, et al. Short Physical Performance Battery (SPPB) score as a discriminator of dynapenic abdominal obesity among community-dwelling older adults. Geriatr Nurs. 2021;42(2):467–472. doi:10.1016/j.gerinurse.2021.02.016
13. Mansour KMK, Goulart CL, de Carvalho-Junior LCS, et al. Pulmonary function and functional capacity cut-off point to establish sarcopenia and dynapenia in patients with COPD. J Bras Pneumol. 2018;45(6):1–7.
14. Ohara DG, Pegorari MS, Oliveira Dos Santos NL, et al. Respiratory muscle strength as a discriminator of sarcopenia in community-dwelling elderly: a cross-sectional study. J Nutr Health Aging. 2018;22(8):952–958. doi:10.1007/s12603-018-1079-4
15. Vidal MB, Pegorari MS, Santos EC, et al. Respiratory muscle strength for discriminating frailty in community-dwelling elderly: a cross-sectional study. Arch Gerontol Geriatr. 2020;89(January):104082. doi:10.1016/j.archger.2020.104082
16. Fiore Junior JF, Paisani DM, Franceschini J, et al. Maximal respiratory pressures and vital capacity: comparison mouthpiece and face-mask evaluation methods. J Bras Pneumol. 2004;30(6):515–520. doi:10.1590/S1806-37132004000600005
17. Souza RB. Maximal static respiratory pressures. J Pneumol. 2002;28:155–165.
18. Gibson GJ, Whitelaw W, Siafakas N, et al. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624.
19. Laveneziana P, Albuquerque A, Aliverti A, et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur Respir J. 2019;53(6):1801214. doi:10.1183/13993003.01214-2018
20. Macdermid J. ASHT - American Society of Hand Therapists. Clinical Assessment Recommendations.
21. Alley DE, Shardell MD, Peters KW, et al. Grip strength cutpoints for the identification of clinically relevant weakness. J Gerontol a Biol Sci Med Sci. 2014;69(5):559–566. doi:10.1093/gerona/glu011
22. Marucci MFN, Barbosa AR. Nutritional Status and Physical Capacity. In SABE - Health, well-being and aging. The SABE project in the city of São Paulo: an initial approach. OPAS. 2003;2003:95–117.
23. Clinical Guidelines on the Identification. Evaluation, and treatment of overweight and obesity in adults--the evidence report. National institutes of health. Obes Res. 1998;6(2):51S–209S.
24. Tavares DMS, Pelizaro PB, Pegorari MS, et al. Prevalence of self-reported morbidities and associated factors among community-dwelling elderly in Uberaba, Minas Gerais, Brazil. Cienc Saude Coletiv. 2019;24(9):3305–3313. doi:10.1590/1413-81232018249.31912017
25. Benedetti TRB, Antunes PDC, Rodriguez-añez CR. Reproducibility and validity of the International Physical Activity Questionnaire (IPAQ) in elderly men. Rev Bras Med Do Esporte. 2007;13(1):9–13.
26. Benedetti T, Mazo G, Barros M. Application of the International Physical Activity Questionnaire (IPAQ) for evaluation of elderly women: concurrent validity and test-retest reprodutibility. Rev Bras Ciên Mov. 2004;12:25–34.
27. World Health Organization. Global recommendations on physical activity for health; 2010. Available from https://www.who.int/publications/i/item/9789241599979.
28. Ishikawa C, Barbieri MA, Bettiol H, et al. Comparison of body composition parameters in the study of the association between body composition and pulmonary function. BMC Pulm Med. 2021;21:178. doi:10.1186/s12890-021-01543-1
29. Huang L, Ye Z, Lu J, et al. Effects of fat distribution on lung function in young adults. J Physiol Anthropol. 2019;38:7. doi:10.1186/s40101-019-0198-x
30. Sonpeayung R, Tantisuwat A, Janwantanakul P, Thaveeratitham P. Total and compartmental chest wall volumes, lung function, and respiratory muscle strength in individuals with abdominal obesity: effects of body positions. J Obes. 2019;2019:9539846.
31. Rossi AP, Watson NL, Newman AB, et al. Effects of body composition and adipose tissue distribution on respiratory function in elderly men and women: the health, aging, and body composition study. J Gerontol Ser a Biol Sci Med Sci. 2011;66(7):801–808. doi:10.1093/gerona/glr059
32. Dattani RS, Swerner CB, Stradling JR, et al. Exploratory study into the effect of abdominal mass loading on airways resistance and ventilatory failure. BMJ Open Respir Res. 2016;3(1):1–6. doi:10.1136/bmjresp-2016-000138
33. Manuel AR, Hart N, Stradling JR. Correlates of obesity-related chronic ventilatory failure. BMJ Open Respir Res. 2016;3(1):1–6. doi:10.1136/bmjresp-2015-000110
34. Souza RMP, Cardim AB, Maia TO, et al. Inspiratory muscle strength, diaphragmatic mobility, and body composition in chronic obstructive pulmonary disease. Physiother Res Int. 2019;24(2):e1766. doi:10.1002/pri.1766
35. Sant’Anna M, Carvalhal RF, Oliveira FDFB, et al. Respiratory mechanics of patients with morbid obesity. J Bras Pneumol. 2019;45(5):e20180311. doi:10.1590/1806-3713/e20180311
36. Clark BC, Manini TM. What Is Dynapenia? Nutrition. 2012;28:495–503. doi:10.1016/j.nut.2011.12.002
37. Máximo RO, Santos JLF, Perracini MR, et al. Abdominal obesity, dynapenia and dynapenic-abdominal obesity as factors associated with falls. Brazilian J Phys Ther. 2019;23(6):497–505. doi:10.1016/j.bjpt.2018.10.009
38. Ohara DG, Moreira YP, Silva CFR, et al. Impaired pulmonary function is associated with dynapenia, but not with abdominal obesity and 371 dynapenic abdominal obesity in older adults. Eur Geriatr Med. 2022;13:475–482. doi:10.1007/s41999-021-00560-x
39. Sampaio RAC, Sewo Sampaio PY, Uchida MC, et al. Management of dynapenia, sarcopenia, and frailty: the role of physical exercise. J Aging Res. 2020;2020:8186769. doi:10.1155/2020/8186769
40. Moon JH, Kong MH, Kim HJ. Implication of sarcopenia and sarcopenic obesity on lung function in 374 healthy elderly: using Korean national health and nutrition examination survey. J Korean Med Sci. 2015;375:1682–1688. doi:10.3346/jkms.2015.30.11.1682
41. Araújo FC, Silva KS, Ohara DG, et al. Prevalence of and risk factors for dynapenic abdominal obesity in community-dwelling older adults: a cross-sectional study. Ciênc Saúde Coletiva. 2022;27(2):761–769. doi:10.1590/1413-81232022272.01122021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.