Back to Journals » Journal of Pain Research » Volume 19
Cross-Cultural Adaptation and Validation for Central Aspects of Pain in the Knee Questionnaire: Based on Chinese Patients Undergoing Total Knee Arthroplasty for Knee Osteoarthritis
Authors Wu H, Wei Y, Wan D, Tang R, Guo Y, Yao S, Xu C, Ma J
Received 5 September 2025
Accepted for publication 23 December 2025
Published 8 January 2026 Volume 2026:19 565552
DOI https://doi.org/10.2147/JPR.S565552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Haodong Wu,1,2,* Yi Wei,3,* Dongping Wan,4,* Rui Tang,5 Yishun Guo,1 Shuxin Yao,1 Chao Xu,1,* Jianbing Ma1,*
1Department of Knee Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, 710061, People’s Republic of China; 2Department of Orthopedics, Medical College, Yan’an University, Yan’an, 716000, People’s Republic of China; 3Department of Anatomy, School of Medicine, Northwest University, Xi’an, 710069, People’s Republic of China; 4Department of Orthopedics, The First Affiliated Hospital, Guangxi University of Chinese Medicine, Nanning, 530023, People’s Republic of China; 5Department of Orthopedics, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, 610072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianbing Ma, Department of Knee Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, No. 555 E.Youyi Road, Xi’an, 710061, People’s Republic of China, Email [email protected] Chao Xu, Department of Knee Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, No. 555 E.Youyi Road, Xi’an, 710061, People’s Republic of China, Email [email protected]
Background: This study aimed to develop a simplified Chinese version of the Central Aspects of Pain in the Knee (CAP-Knee-CV) questionnaire and to evaluate its psychometric properties in patients with knee osteoarthritis (KOA).
Methods: The CAP-Knee-CV was developed using a standardized forward–backward translation procedure, followed by expert panel review to ensure cultural and linguistic equivalence. A total of 120 patients with KOA scheduled for total knee arthroplasty (TKA) were recruited from a tertiary orthopedic center in Xi’an, China. Among them, 50 participants were randomly selected to complete the questionnaire again after one week. Reliability and validity were assessed through exploratory factor analysis, internal consistency, test–retest reliability, and correlation analyses with established clinical measures.
Results: The CAP-Knee-CV consisted of 8 items loading on two factors, accounting for 66.1% of the total variance. Internal consistency was good (Cronbach’s α = 0.843), and test–retest reliability was excellent (intraclass correlation coefficient = 0.957). The CAP-Knee-CV showed significant correlations with the Central Sensitization Inventory (r = 0.610), pain intensity while walking (r = 0.697), the Western Ontario and McMaster Universities Osteoarthritis Index (r = 0.530), and the 5-level EQ-5D (r = 0.510).
Conclusion: The CAP-Knee-CV was successfully translated and cross-culturally adapted into simplified Chinese. It demonstrated satisfactory reliability, validity, and feasibility, making it a promising tool for assessing central sensitization in Chinese-speaking patients with KOA undergoing TKA.
Keywords: central sensitization, knee osteoarthritis, CAP-knee, cross-cultural adaptation, psychometrics
A Letter to the Editor has been published for this article.
Background
Knee osteoarthritis (KOA) is a prevalent age-related degenerative joint disorder, primarily characterized by knee pain and functional impairment.1 Its pathogenesis involves a complex interplay of peripheral pathological changes, which include articular cartilage degradation, synovial inflammation, subchondral bone sclerosis, and osteophyte formation.2 These changes initially trigger pain by activating peripheral nociceptors.3 Epidemiological studies have reported that between 2008 and 2017, the average crude prevalence of KOA among Chinese adults aged 55 years and older is approximately 13.2%.4 Although total knee arthroplasty (TKA) is the primary treatment for end-stage KOA and has proven efficacy in restoring joint function, approximately 10–20% of patients continue to experience persistent pain and overall dissatisfaction postoperatively, largely due to unexplained postoperative pain.5–7 This poor outcome is largely attributed to limitations of traditional treatments: most interventions, such as nonsteroidal anti-inflammatory drugs, physical therapy, or TKA itself, focus on resolving peripheral pathology while neglecting central nervous system (CNS) remodeling that sustains pain.8 In older patients, chronic knee pain not only results in diminished extensor strength, impaired walking ability, and reduced quality of life, but also markedly undermines satisfaction with surgical outcomes.9–11 With the acceleration of population aging, the effective management of knee pain in older patients has emerged as a pressing clinical challenge.
In recent years, the concept of central sensitization (CS) has gained increasing recognition, and clearly distinguishing CS from peripheral sensitization is critical for guiding targeted treatment.12 Peripheral sensitization refers to increased responsiveness of peripheral nociceptors to noxious or sub-noxious stimuli, triggered by local inflammation, tissue damage, or chemical mediators such as prostaglandins in KOA joints.13 It is a transient, localized process that resolves when peripheral pathology is controlled. In contrast, CS is defined as heightened responsiveness of nociceptive neurons in the CNS (such as spinal dorsal horn neurons and supraspinal brain regions) to normal or sub-threshold stimuli.12,14,15 It arises from plastic changes in the CNS induced by long-term peripheral pain input, including activation of N-methyl-D-aspartate (NMDA) receptors, hyperactivation of glial cells, and reduced descending pain inhibition.16–18 Importantly, CS has been identified as a major risk factor for persistent pain and dissatisfaction after TKA, as it perpetuates pain even when peripheral pathology is addressed by surgery.19,20 Interventions targeting CS, such as cognitive behavioral therapy and certain neuromodulators, can enhance treatment responses. These interventions complement traditional peripheral-focused strategies and provide more effective relief of knee pain.20,21
Current methods for assessing CS include quantitative sensory testing (QST), electroencephalography, functional magnetic resonance imaging (fMRI), and self-report questionnaires.12,22,23 QST quantifies sensory thresholds, such as heat and pressure pain thresholds, to reflect CNS excitability, but it is susceptible to subjective bias and operator variability, whereas fMRI visualizes CS-related brain activation, such as in the insula and anterior cingulate cortex, but is costly and not easily accessible in clinical settings.24,25 Among self-reported tools, the Central Sensitization Inventory (CSI) is the most widely used; it can predict pain outcomes associated with central mechanisms and evaluate treatment responses.26 However, the CSI lacks disease specificity: it does not account for knee-specific pain manifestations, such as weight-bearing-related central pain and post-TKA knee hypersensitivity.27 Thus, it may not adequately capture knee-specific central mechanisms in older patients with knee pain.
To address this gap, Akin-Akinyosone et al developed and validated the Central Aspects of Pain in the Knee (CAP-Knee) questionnaire.28 This questionnaire consists of 8 items covering dimensions closely linked to central mechanisms, including neuropathic-like pain, fatigue, cognitive impact, catastrophizing, anxiety, sleep disturbance, depression, and pain distribution.28 Evidence shows that higher total CAP-Knee scores are positively associated with greater pain intensity and poorer functional outcomes in KOA patients.28,29 As a concise, knee-specific tool, the CAP-Knee holds promise for screening and stratifying patients with knee pain in clinical practice. This could further facilitate the development of individualized treatment strategies, such as prioritizing CS-targeted interventions for patients with high CAP-Knee scores.
However, a simplified Chinese version of the CAP-Knee (CAP-Knee-CV) has not yet been developed. Therefore, the present study aims to translate and culturally adapt the CAP-Knee, and to evaluate its reliability, validity, and psychometric properties in Chinese KOA patients scheduled for TKA. The ultimate goal of this study is to lay a foundation for the clinical application of the CAP-Knee in China, particularly in its potential value for preoperative risk assessment, which helps identify patients at high risk of CS-related post-TKA pain, as well as for patient stratification in TKA.
Methods
Study Design and Ethical Approval
This prospective observational study was approved by the Medical Ethics Committee of Honghui Hospital, Xi’an Jiaotong University (Approval No. 202407008). All procedures conformed to the Declaration of Helsinki, and written informed consent was obtained from all participants prior to enrollment.30 Participants were informed of their right to withdraw from the study at any time without penalty, and all data were de-identified to protect privacy.
Translation and Cross-Cultural Adaptation
The translation and cross-cultural adaptation of the CAP-Knee into simplified Chinese followed internationally recognized guidelines, including three stages: forward translation, back translation, and cognitive debriefing.31,32 First, two native Chinese translators independently performed forward translations: one was an orthopedic surgeon proficient in English, and the other was a professional translator with medical translation experience. Their versions were synthesized under the supervision of a cross-cultural adaptation expert to form a preliminary consensus version. Next, two native English speakers without medical backgrounds independently back-translated the questionnaire to ensure semantic equivalence and identify potential ambiguities. Finally, a pilot test was conducted among 30 patients with end-stage KOA to assess comprehensibility, content integrity, and completion time. Based on participant feedback, revisions were made to generate the final CAP-Knee-CV (Figure S1).
Participants
From July 2024 to March 2025, patients with end-stage KOA scheduled for primary unilateral TKA were consecutively recruited from the Department of Knee Surgery, Honghui Hospital, Xi’an Jiaotong University. Inclusion criteria were: (a) age ≥18 years; (b) diagnosis of end-stage KOA with knee pain; (c) sufficient cognitive ability to complete questionnaires; (d) fluency in Mandarin; and (e) voluntary participation with signed informed consent. Exclusion criteria were: (a) inflammatory arthritis (eg, rheumatoid arthritis); (b) other conditions causing pain or impairing mobility (eg, hemiplegia, fracture, ligament injury, lower-limb vascular disease); (c) prior TKA; (d) comorbidities severely affecting daily life (eg, coronary heart disease, asthma, severe psychiatric disorders); and (e) inability to complete two CAP-Knee-CV assessments.
Demographic and clinical characteristics, including age, sex, BMI, Kellgren–Lawrence grade, education level, and living status, were obtained from the hospital medical records. All questionnaires were administered preoperatively under the supervision of trained interviewers. Missing items were completed with participants’ consent. To evaluate test–retest reliability, 50 patients were randomly selected to complete the CAP-Knee-CV again 7 days after the initial assessment, during which no additional intervention was performed.33
Questionnaires
CAP-Knee-CV
The CAP-Knee consists of eight items covering central mechanisms related to knee pain: neuropathic-like pain, fatigue, cognitive-impact, catastrophizing, anxiety, sleep disturbance, depression, and pain distribution.28,34–39 Items were scored as follows: “never” = 0, “sometimes” = 1, “often” = 2, and “always” = 2. To preserve measurement properties, the original four-level scoring was retained to avoid midpoint bias. Item 7 was reverse-scored (“never” = 2, “sometimes” = 1, “often” = 0, “always” = 0). For Item 8, pain distribution was scored as 0 if pain was localized to one knee and 2 if pain extended below the waist. All items were equally weighted, with a maximum score of 2 per item; total scores ranged from 0–16, with higher scores indicating greater central contributions to knee pain.
CSI
The CSI comprises Parts A and B; only Part A was used in this study.26 It includes 25 items scored on a 0 (“never”) to 4 (“always”) Likert scale, yielding a total score of 0–100. Higher scores indicate more pronounced features of central sensitization. The reliability and validity of the CSI have been previously validated in Chinese KOA populations.40
Pain Intensity While Walking
Pain intensity during walking was assessed using an 11-point Numerical Rating Scale (NRS, 0–10), where 0 represents no pain and 10 represents the worst imaginable pain.41 This tool has been widely validated as a simple and reliable pain measure.42
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC comprises 24 items divided into three subscales: pain (5 items), stiffness (2 items), and physical function (17 items).43 Each item is scored from 0 to 4, with higher scores indicating more severe pain, stiffness, and functional limitations. The simplified Chinese version has been validated in TKA patients.44
The 5-Level EQ-5D (EQ-5D-5L)
The EQ-5D-5L was used to assess health-related quality of life (HRQOL) across five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.45 Each dimension is rated on a five-level scale (no, slight, moderate, severe, or extremely severe difficulties). The Chinese version of the EQ-5D-5L was used, with established validity in KOA patients.46
Sample Size Determination
To calculate the required sample size, we adhered to established guidelines for factor analysis, which recommend having between 4 and 10 participants for each item, as well as a total sample size exceeding 100 participants. Based on these criteria, the sample size for this study was set to be at least 100 participants.47,48
Statistical Analysis
Descriptive statistics were used to summarize demographic and clinical characteristics. Continuous variables were presented as mean ± standard deviation (SD), and categorical variables as percentages. The Kolmogorov–Smirnov test was used to examine the distribution of CAP-Knee-CV, CSI, NRS, WOMAC, and EQ-5D-5L scores. All analyses were performed using SPSS version 26.0 (IBM, Chicago, IL), with a two-tailed significance threshold of p < 0.05.
Psychometric Evaluation
Structural Validity
Exploratory factor analysis (EFA) was conducted to examine the underlying factor structure of the CAP-Knee-CV. Suitability for factor analysis was assessed using the Kaiser–Meyer–Olkin (KMO) test and Bartlett’s test of sphericity. Factors were extracted using maximum likelihood estimation with promax rotation. Factors with eigenvalues >1.0 were retained, and loadings ≥0.40 were considered significant.49 A two-factor model was hypothesized for the CAP-Knee-CV, based on observed structural variability in cross-culturally adapted pain questionnaires. For example, the Japanese adaptation of the CAP-Knee exhibits a three-factor structure, which differs from the original English version’s unidimensional framework.28,29
Criterion Validity
Spearman correlation coefficients were used to assess relationships between CAP-Knee-CV and CSI, NRS, WOMAC, and EQ-5D-5L. Correlation strength was classified as follows: >0.81 = very strong; 0.61–0.80 = strong; 0.41–0.60 = moderate; 0.21–0.40 = weak; <0.20 = negligible.50 Based on content analysis, we hypothesized that CAP-Knee-CV would show moderate correlations with these measures.
Internal Consistency and Test–Retest Reliability
Internal consistency was assessed using Cronbach’s α (unacceptable <0.70, acceptable 0.70–0.79, good 0.80–0.89, excellent ≥0.90).51 Test–retest reliability was evaluated using the ICC: moderate (0.50–0.75), good (0.75–0.90), and excellent (>0.90).52 Following psychometric guidelines, a 2–14 days interval is recommended to minimize clinical change and recall bias; a 7-days interval was chosen in this study.33
Feasibility
Feasibility was assessed by recording participant difficulties, missing responses, and average completion time of the CAP-Knee-CV.
Results
Participants
A total of 120 patients completed the baseline survey, including 76 women (63.3%). The mean age was 65.2 ± 5.5 years, and the mean BMI was 25.7 ± 4.0 kg/m2. Most patients were classified as Kellgren–Lawrence grade IV (63.3%). Detailed demographic and clinical characteristics, including education level and living status, are presented in Table 1. The mean CAP-Knee-CV total score was 8.4 ± 3.9.
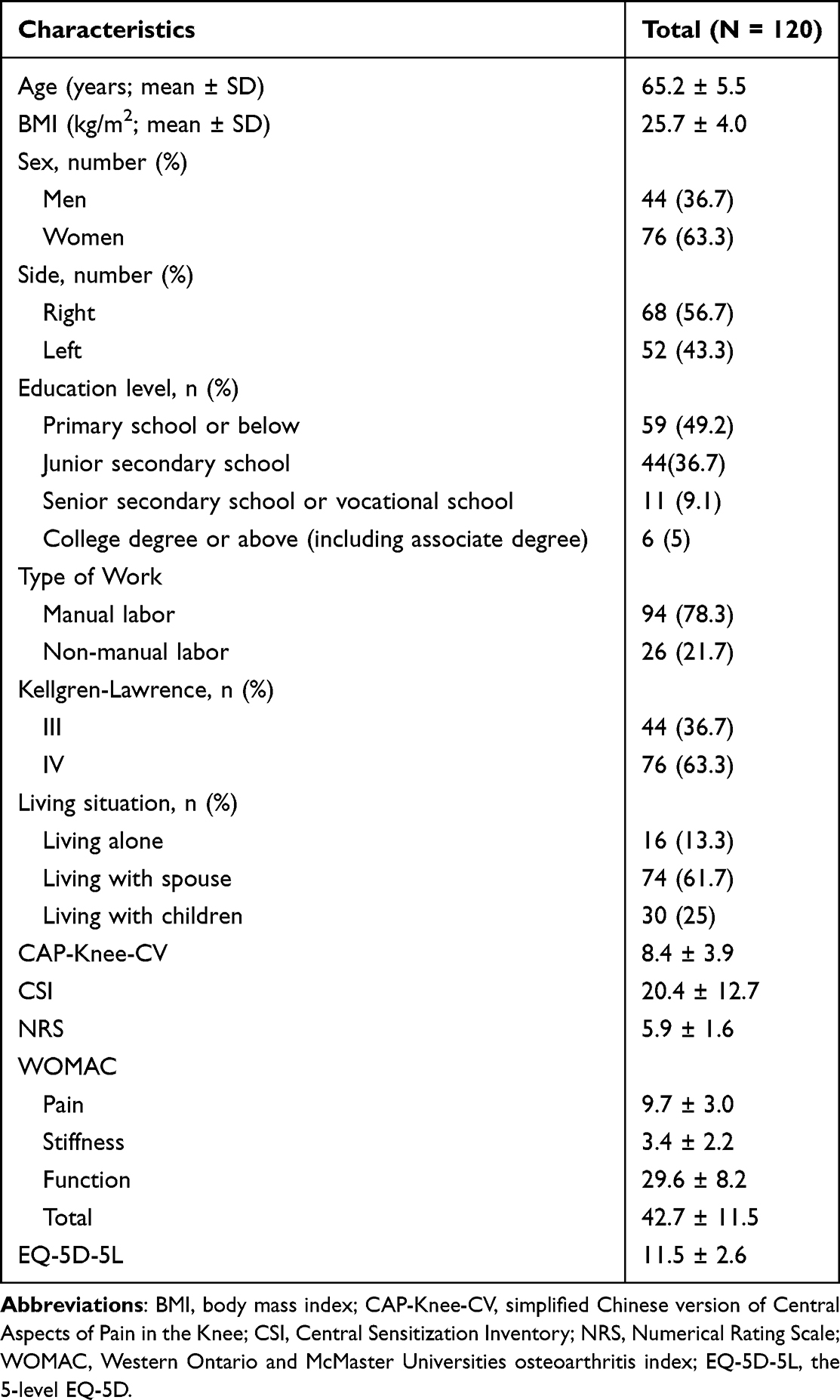 |
Table 1 Demographic Data of the Sample Group Population (n = 120) |
To further assess the statistical power of the sample size for factor structure validation, we conducted a post-hoc power analysis using G*Power 3.1 software. The analysis was based on two hypothesized models: a two-factor model and the original unidimensional model. The parameters for the analysis were set as follows: a medium effect size (f = 0.3), a significance level of α = 0.05, and the actual sample size of 120 participants.53 The number of predictors was set at 2 for the two-factor model and 1 for the unidimensional model. The results indicated that the statistical power for both the two-factor model and the unidimensional model was 0.99, suggesting that the sample size of 120 participants is sufficient to reliably detect the true effects of both factor structures. This power analysis supports the adequacy of the sample size for factor structure validation and subsequent reliability and validity assessments.
Structural Validity
The KMO value was 0.827, and Bartlett’s test of sphericity was significant (p < 0.001), indicating suitability for factor analysis. EFA with scree plot inspection (Figure 1) supported a two-factor model. The eigenvalues of Factor 1 and Factor 2 were 3.9 and 1.4, accounting for 33.3% and 32.8% of the variance, respectively, with a cumulative variance contribution of 66.1%. Factor loadings are shown in Table 2. Factor 1 comprised items 1, 5, 6, 7, and 8, representing patients’ emotional and physiological responses to knee pain, and was labeled the “psychological–physiological response factor”. Factor 2 included items 2, 3, and 4, reflecting cognitive impairment and fatigue, and was labeled the “cognitive–fatigue factor”.
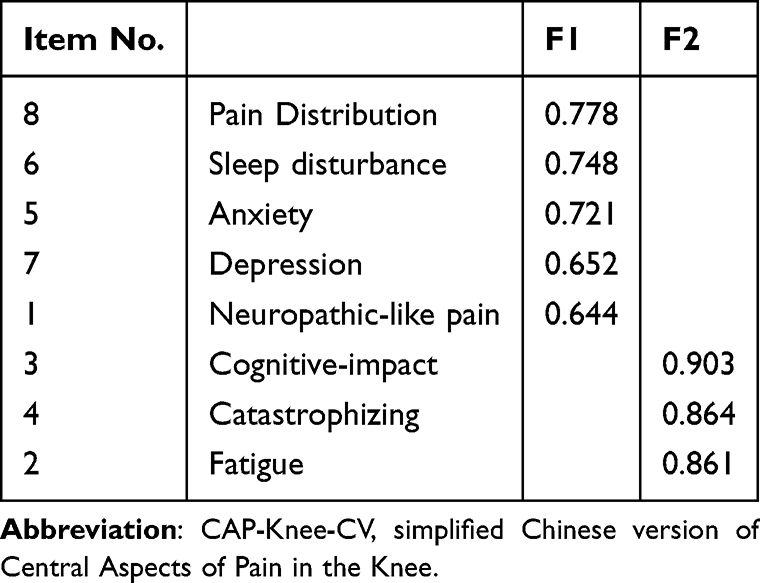 |
Table 2 Factors in Factor Analysis and Varimax Rotated Factor Matrix of the CAP-Knee-CV |
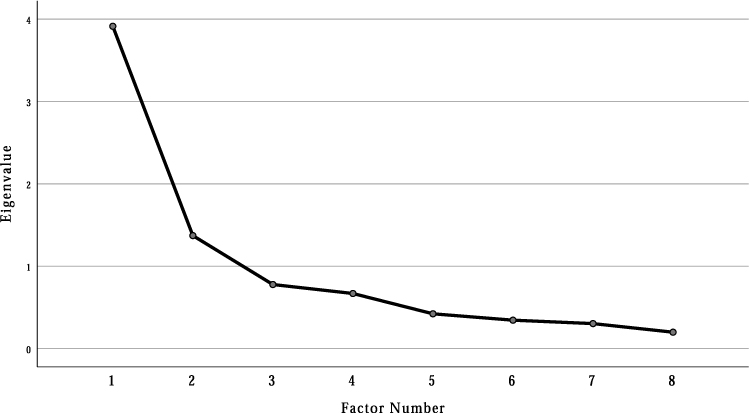 |
Figure 1 Scree plot of exploratory factor analysis. |
Criterion Validity
Correlations between the CAP-Knee-CV and other instruments are summarized in Table 3. The CAP-Knee-CV total score showed strong correlations with the CSI total score (r = 0.610, p < 0.001) and with NRS (r = 0.697, p < 0.001). Moderate correlations were observed with the WOMAC pain subscale (r = 0.526, p < 0.001) and total WOMAC score (r = 0.530, p < 0.001), as well as with the EQ-5D-5L total score (r = 0.510, p < 0.001).
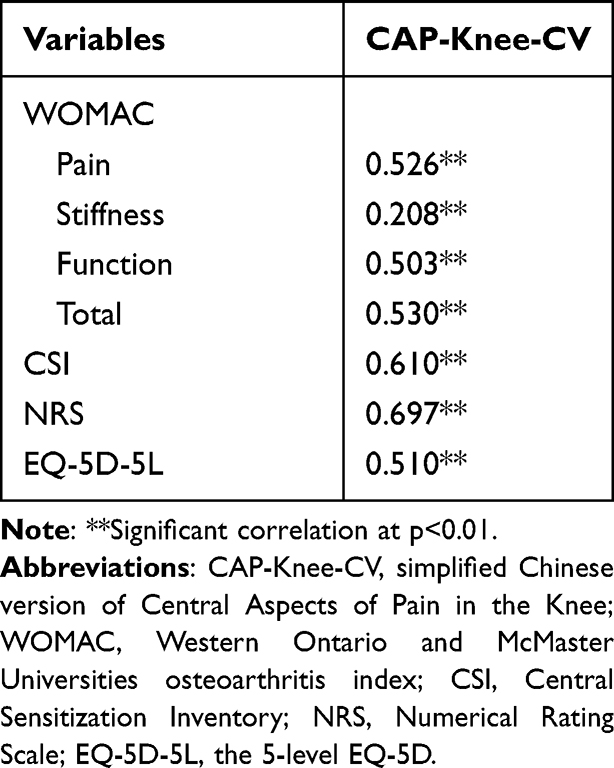 |
Table 3 Spearman Correlation Coefficients of CAP-Knee-CV, WOAMC, CSI, NRS and EQ-5D-5L |
Internal Consistency and Test–Retest Reliability
Reliability results are presented in Table 4. The CAP-Knee-CV demonstrated good internal consistency (Cronbach’s α = 0.843) and excellent test–retest reliability (ICC = 0.957, 95% CI: 0.924–0.976). All ICC values exceeded 0.90, confirming stable responses over 7 days.
 |
Table 4 Internal Consistency and Test–Retest Reliability of the CAP-Knee-CV |
Feasibility
All participants successfully completed the CAP-Knee-CV, with no missing data. The mean completion time was 3.6 ± 0.9 minutes, and no substantial difficulties were reported.
Discussion
This study aimed to develop and validate a simplified Chinese version of the CAP-Knee and to evaluate its psychometric properties in patients with KOA undergoing TKA. The findings demonstrated that the CAP-Knee-CV exhibited a clear two-factor structure, good internal consistency, excellent test–retest reliability, and significant correlations with pain-related outcomes (CSI, NRS, WOMAC, and EQ-5D-5L), indicating its clinical applicability in the Chinese patient population.
A key finding of our study was the two-factor structure of the CAP-Knee-CV, which diverges from the unidimensional model of the original English version.28 In our Chinese cohort, items clustered into two distinct domains: one reflecting emotional and physiological responses to pain (neuropathic-like pain, anxiety, depression, sleep disturbance, pain distribution) and the other indicating cognitive impairment and fatigue (fatigue, cognitive impact, catastrophizing). This structural difference likely reflects cultural variations in how pain-related symptoms are perceived and categorized.54 Consistent with cross-cultural pain research, Chinese populations often adopt a holistic “mind-body” framework that integrates emotional and physical experiences, whereas Western samples may conceptualize these domains as separate.55 This interpretation is further supported by comparisons with the Japanese version of the CAP-Knee, which exhibited a three-factor structure, with “sleep disturbance” and “fatigue” as independent dimensions, and some items failing to load adequately.29 Such cross-cultural variability underscores that direct translation of patient-reported outcome measures is insufficient. Rigorous cultural adaptation is necessary to ensure measurement equivalence and validity in diverse populations. For instance, Chinese participants in our study frequently described sleep disturbance as a consequence of pain or anxiety, justifying its inclusion in the “psychological–physiological response factor”.56 In contrast, Japanese patients in the prior validation study reported sleep disturbance as a standalone symptom.29
The CAP-Knee-CV’s reliability metrics are comparable to those of other international versions. Its Cronbach’s α (0.843) exceeds that of the original English version (α = 0.74) and is consistent with the Japanese adaptation (α = 0.86), indicating strong internal consistency.28 The excellent test–retest reliability (ICC = 0.957) aligns with the original study (ICC = 0.91), confirming the tool’s ability to stably capture CS features over time.28 These results indicate that the CAP-Knee-CV is a reliable instrument that can stably capture CS syndrome over time. Regarding criterion validity, the CAP-Knee-CV demonstrated strong positive correlations with the CSI (r = 0.610, p < 0.001), a gold-standard measure of general CS, confirming its convergence with core CS constructs. It also showed strong correlations with walking pain (NRS; r = 0.697, p < 0.001) and moderate correlations with KOA-specific function (WOMAC; total score: r = 0.530, p < 0.001) and HRQOL (EQ-5D-5L; r = 0.510, p < 0.001). These associations are consistent with the well-established link between CS and worse pain intensity, functional limitations, and HRQOL in KOA, further validating the CAP-Knee-CV as a clinically relevant measure of central pain mechanisms.19,20
Notably, the CAP-Knee-CV addresses a critical gap in personalized perioperative care by identifying patients at risk for iatrogenic modulation of central pain pathways, a concern highlighted in recent research on KOA.28 Iatrogenic inhibition, or the unintended alteration of central pain processing due to medical interventions, significantly contributes to persistent post-TKA pain.57,58 For example, overreliance on opioid analgesics during the perioperative period can exacerbate CS through NMDA receptor activation, while inadequate preoperative pain management prolongs nociceptive input, further amplifying CS.59–61 Preoperative CAP-Knee-CV assessment can stratify patients based on CS severity. Patients with high scores (indicating prominent central mechanisms) may benefit from multimodal perioperative analgesia, such as femoral nerve blocks combined with cognitive behavioral therapy, to mitigate iatrogenic exacerbation of CS, while patients with low scores may respond adequately to standard peripheral-focused care.58,60 This approach has the potential to reduce the 10–20% rate of persistent post-TKA pain linked to unaddressed central mechanisms, highlighting the CAP-Knee-CV’s relevance for clinical practice.57
Feasibility is another strength of the CAP-Knee-CV. With an average completion time of 3.6 ± 0.9 minutes and a 100% completion rate, it outperforms longer CS assessment tools, such as the CSI, which requires approximately 6.4 minutes to complete.40 This is a critical advantage in time-constrained clinical settings, such as preoperative TKA clinics.
This study has several limitations. First, we did not incorporate objective measures of CS, such as QST for pressure pain thresholds or fMRI to assess CS-related brain activation, such as in the insula or anterior cingulate cortex. Future studies integrating QST or fMRI would enable examination of concordance between the CAP-Knee-CV and objective CS biomarkers, further strengthening its validity. Second, recruitment from a single center in northwestern China may limit generalizability to patients from other regions with distinct cultural or socioeconomic profiles. Multicenter studies with geographically diverse samples are needed to confirm the CAP-Knee-CV’s performance across broader Chinese KOA populations. Third, our sample focused on moderate-to-severe KOA patients scheduled for TKA, and the tool’s validity in earlier-stage KOA or non-surgical patients remains untested. Expanding validation to these groups would confirm the CAP-Knee-CV’s utility across the full KOA disease spectrum. Finally, we did not evaluate the CAP-Knee-CV’s predictive validity for iatrogenic outcomes, such as opioid use or persistent post-TKA pain. Longitudinal studies tracking these endpoints would further establish the tool’s clinical value for risk stratification.
Conclusion
The CAP-Knee-CV demonstrates strong reliability and validity as a tool for assessing CS in Chinese patients with KOA awaiting TKA. It reveals a distinctive two-factor structure, consisting of the “psychological–physiological response factor” and “cognitive–fatigue factor”, which contrasts with the unidimensional structure of the original English version and the three-factor structure in the Japanese version. This underscores the importance of cultural adaptation in cross-cultural pain assessment. With robust psychometric properties and a short completion time of approximately 3.6 minutes, the CAP-Knee-CV is well-suited for use in preoperative TKA settings, such as screening for high-risk CS patients to guide personalized analgesia strategies. Future research should integrate objective measures like QST and conduct multicenter validations to broaden its applicability, while also exploring its potential in cross-cultural CS research.
Acknowledgments
We would like to express our sincere gratitude to all those who supported this project.
Funding
This study was supported by the Key Research and Development Program of Shaanxi Province (No.2023-YBSF-464), Cultivation Project for General Project of Xi’an Health Commission (No. 2024ms10), 2024 ministry of Education Humanities and Social Sciences Project (24YJAZH032) and the Program for Innovation Team of shaanxi Province (2023-CX-TD-73). We thank everyone who participated in the study and the individuals who helped with preparing the paper.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Litwic A, Edwards MH, Dennison EM, Cooper C. Epidemiology and burden of osteoarthritis. Br Med Bull. 2013;105(1):185–11. doi:10.1093/bmb/lds038
2. Mahmoudian A, Lohmander LS, Mobasheri A, Englund M, Luyten FP. Early-stage symptomatic osteoarthritis of the knee - time for action. Nat Rev Rheumatol. 2021;17(10):621–632. doi:10.1038/s41584-021-00673-4
3. Miller RE, Tran PB, Obeidat AM, et al. The role of peripheral nociceptive neurons in the pathophysiology of osteoarthritis pain. Curr Osteoporos Rep. 2015;13(5):318–326. doi:10.1007/s11914-015-0280-1
4. Chen H, Wu J, Wang Z, et al. Trends and patterns of knee osteoarthritis in China: a longitudinal study of 17.7 million adults from 2008 to 2017. Int J Environ Res Public Health. 2021;18(16):8864. doi:10.3390/ijerph18168864
5. DeFrance MJ, Scuderi GR. Are 20% of patients actually dissatisfied following total knee arthroplasty? A systematic review of the literature. J Arthroplasty. 2023;38(3):594–599. doi:10.1016/j.arth.2022.10.011
6. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57–63. doi:10.1007/s11999-009-1119-9
7. Klem NR, Smith A, O’Sullivan P, et al. What influences patient satisfaction after TKA? A qualitative investigation. Clin Orthop Relat Res. 2020;478(8):1850–1866. doi:10.1097/corr.0000000000001284
8. Wluka AE, Yan MK, Lim KY, Hussain SM, Cicuttini FM. Does preoperative neuropathic-like pain and central sensitisation affect the post-operative outcome of knee joint replacement for osteoarthritis? A systematic review and meta analysis. Osteoarthritis Cartilage. 2020;28(11):1403–1411. doi:10.1016/j.joca.2020.07.010
9. Muraki S, Akune T, Teraguchi M, et al. Quadriceps muscle strength, radiographic knee osteoarthritis and knee pain: the ROAD study. BMC Musculoskelet Disord. 2015;16(1):305. doi:10.1186/s12891-015-0737-5
10. Kitayuguchi J, Kamada M, Hamano T, et al. Association between knee pain and gait speed decline in rural Japanese community-dwelling older adults: 1-year prospective cohort study. Geriatr Gerontol Int. 2016;16(1):55–64. doi:10.1111/ggi.12432
11. Muraki S, Akune T, Oka H, et al. Association of radiographic and symptomatic knee osteoarthritis with health-related quality of life in a population-based cohort study in Japan: the ROAD study. Osteoarthritis Cartilage. 2010;18(9):1227–1234. doi:10.1016/j.joca.2010.06.001
12. Soni A, Wanigasekera V, Mezue M, et al. Central sensitization in knee osteoarthritis: relating presurgical brainstem neuroimaging and PainDETECT-based patient stratification to arthroplasty outcome. Arthritis Rheumatol. 2019;71(4):550–560. doi:10.1002/art.40749
13. O’Leary H, Smart KM, Moloney NA, Doody CM. Nervous system sensitization as a predictor of outcome in the treatment of peripheral musculoskeletal conditions: a systematic review. Pain Pract. 2017;17(2):249–266. doi:10.1111/papr.12484
14. Onu I, Matei D, Sardaru D-P, et al. Rehabilitation of patients with moderate knee osteoarthritis using hyaluronic acid viscosupplementation and physiotherapy. Appl Sci. 2022;12(6):3165. doi:10.3390/app12063165
15. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–s15. doi:10.1016/j.pain.2010.09.030
16. Baron R, Hans G, Dickenson AH. Peripheral input and its importance for central sensitization. Ann Neurol. 2013;74(5):630–636. doi:10.1002/ana.24017
17. Gold MS, Gebhart GF. Nociceptor sensitization in pain pathogenesis. Nat Med. 2010;16(11):1248–1257. doi:10.1038/nm.2235
18. Kılıçaslan H, Genç A, Tuncer S. Central sensitization in osteoarthritic knee pain: a cross-sectional study. Turk J Phys Med Rehabil. 2023;69(1):89–96. doi:10.5606/tftrd.2023.10470
19. Nijs J, Leysen L, Vanlauwe J, et al. Treatment of central sensitization in patients with chronic pain: time for change? Expert Opin Pharmacother. 2019;20(16):1961–1970. doi:10.1080/14656566.2019.1647166
20. Wylde V, Palmer S, Learmonth ID, Dieppe P. The association between pre-operative pain sensitisation and chronic pain after knee replacement: an exploratory study. Osteoarthritis Cartilage. 2013;21(9):1253–1256. doi:10.1016/j.joca.2013.05.008
21. Poenaru D, Sandulescu MI, Potcovaru CG, Cinteza D. High-intensity laser therapy in pain management of knee osteoarthritis. Biomedicines. 2024;12(8):1679. doi:10.3390/biomedicines12081679
22. Rankin J, Rudy-Froese B, Hoyt C, et al. Quantitative sensory testing protocols to evaluate central and peripheral sensitization in knee OA: a scoping review. Pain Med. 2022;23(3):526–557. doi:10.1093/pm/pnab285
23. Zafereo J, Wang-Price S, Kandil E. Quantitative sensory testing discriminates central sensitization inventory scores in participants with chronic musculoskeletal pain: an exploratory study. Pain Pract. 2021;21(5):547–556. doi:10.1111/papr.12990
24. Backonja MM, Attal N, Baron R, et al. Value of quantitative sensory testing in neurological and pain disorders: neuPSIG consensus. Pain. 2013;154(9):1807–1819. doi:10.1016/j.pain.2013.05.047
25. Harte SE, Harris RE, Clauw DJ. The neurobiology of central sensitization. J Appl Biobehav Res. 2018;23(2):e12137. doi:10.1111/jabr.12137
26. Mayer TG, Neblett R, Cohen H, et al. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012;12(4):276–285. doi:10.1111/j.1533-2500.2011.00493.x
27. Ten Klooster PM, Simoes JP, Vonkeman HE. Limited content overlap between commonly used self-report instruments for central (pain) sensitization in rheumatology. Rheumatol Adv Pract. 2024;8(3):rkae108. doi:10.1093/rap/rkae108
28. Akin-Akinyosoye K, James RJE, McWilliams DF, et al. The central aspects of pain in the knee (CAP-Knee) questionnaire; a mixed-methods study of a self-report instrument for assessing central mechanisms in people with knee pain. Osteoarthritis Cartilage. 2021;29(6):802–814. doi:10.1016/j.joca.2021.02.562
29. Oka T, Wada O, Matsuda S, Tanaka K, Mizuno K. Cross-cultural adaption, validity, and reliability of the Japanese version of the central aspects of pain in the knee (CAP-Knee-J) questionnaire in patients with knee pain: a validation study. BMC Musculoskelet Disord. 2024;25(1):365. doi:10.1186/s12891-024-07471-5
30. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
31. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417–1432. doi:10.1016/0895-4356(93)90142-n
32. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
33. Marx RG, Menezes A, Horovitz L, Jones EC, Warren RF. A comparison of two time intervals for test-retest reliability of health status instruments. J Clin Epidemiol. 2003;56(8):730–735. doi:10.1016/s0895-4356(03)00084-2
34. Hochman JR, Gagliese L, Davis AM, Hawker GA. Neuropathic pain symptoms in a community knee OA cohort. Osteoarthritis Cartilage. 2011;19(6):647–654. doi:10.1016/j.joca.2011.03.007
35. Ware J, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
36. Ferguson E, Daniel E. The illness attitudes scale (IAS): a psychometric evaluation on a non-clinical population. Pers Individ Dif. 1995;18(4):463–469. doi:10.1016/0191-8869(94)00186-V
37. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
38. Lacey RJ, Lewis M, Jordan K, Jinks C, Sim J. Interrater reliability of scoring of pain drawings in a self-report health survey. Spine. 2005;30(16):E455–8. doi:10.1097/01.brs.0000174274.38485.ee
39. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum. 1986;29(8):1039–1049. doi:10.1002/art.1780290816
40. Xu C, Yao S, Wei W, Zhang H, Ma J, Shang L. Cross-cultural adaptation and validation for central sensitization inventory: based on Chinese patients undergoing total knee arthroplasty for knee osteoarthritis. J Orthop Surg Res. 2023;18(1):960. doi:10.1186/s13018-023-04375-3
41. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798–804. doi:10.1111/j.1365-2702.2005.01121.x
42. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for pain (VAS Pain), numeric rating scale for pain (NRS Pain), McGill pain questionnaire (MPQ), short-form McGill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP). Arthritis Care Res. 2011;63 Suppl 11:S240–52. doi:10.1002/acr.20543
43. Clement ND, Bardgett M, Weir D, Holland J, Gerrand C, Deehan DJ. What is the minimum clinically important difference for the WOMAC index after TKA? Clin Orthop Relat Res. 2018;476(10):2005–2014. doi:10.1097/corr.0000000000000444
44. Xie F, Li SC, Goeree R, et al. Validation of Chinese western ontario and mcmaster universities osteoarthritis index (WOMAC) in patients scheduled for total knee replacement. Qual Life Res. 2008;17(4):595–601. doi:10.1007/s11136-008-9340-7
45. Luo N, Liu G, Li M, Guan H, Jin X, Rand-Hendriksen K. Estimating an EQ-5D-5L value set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
46. Lam CLK, Tse ETY, Wong CKH, et al. A pilot study on the validity and psychometric properties of the electronic EQ-5D-5L in routine clinical practice. Health Qual Life Outcomes. 2021;19(1):266. doi:10.1186/s12955-021-01898-3
47. Terwee CB, Mokkink LB, Knol DL, Ostelo RW, Bouter LM, de Vet HC. Rating the methodological quality in systematic reviews of studies on measurement properties: a scoring system for the COSMIN checklist. Qual Life Res. 2012;21(4):651–657. doi:10.1007/s11136-011-9960-1
48. DeVon HA, Block ME, Moyle-Wright P, et al. A psychometric toolbox for testing validity and reliability. J Nurs Scholarsh. 2007;39(2):155–164. doi:10.1111/j.1547-5069.2007.00161.x
49. Lin K, Bao L, Wang J, Fujita K, Makimoto K, Liao X. Validation of the Chinese (Mandarin) version of the Oxford knee score in patients with knee osteoarthritis. Clin Orthop Relat Res. 2017;475(12):2992–3004. doi:10.1007/s11999-017-5495-2
50. Cao S, Liu N, Li L, Lv H, Chen Y, Qian Q. Simplified Chinese version of university of california at Los Angeles activity score for arthroplasty and arthroscopy: cross-cultural adaptation and validation. J Arthroplasty. 2017;32(9):2706–2711. doi:10.1016/j.arth.2017.03.057
51. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
52. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
53. Kang H. Sample size determination and power analysis using the G*Power software. J Educ Eval Health Prof. 2021;18:17. doi:10.3352/jeehp.2021.18.17
54. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
55. Chan C, Ho PS, Chow E. A body-mind-spirit model in health: an Eastern approach. Soc Work Health Care. 2001;34(3–4):261–282. doi:10.1300/j010v34n03_02
56. Parmelee PA, Tighe CA, Dautovich ND. Sleep disturbance in osteoarthritis: linkages with pain, disability, and depressive symptoms. Arthritis Care Res. 2015;67(3):358–365. doi:10.1002/acr.22459
57. Luo D, Fan Z, Yin W. Chronic post-surgical pain after total knee arthroplasty: a narrative review. Perioper Med. 2024;13(1):108. doi:10.1186/s13741-024-00466-9
58. Fuller AM, Bharde S, Sikandar S. The mechanisms and management of persistent postsurgical pain. Front Pain Res. 2023;4:1154597. doi:10.3389/fpain.2023.1154597
59. Raja SN, Sivanesan E, Guan Y. Central Sensitization, N-methyl-D-aspartate receptors, and human experimental pain models: bridging the gap between target discovery and drug development. Anesthesiology. 2019;131(2):233–235. doi:10.1097/aln.0000000000002808
60. Chunduri A, Aggarwal AK. Multimodal pain management in orthopedic surgery. J Clin Med. 2022;11(21):6386. doi:10.3390/jcm11216386
61. Pogatzki-Zahn EM, Segelcke D, Schug SA. Postoperative pain-from mechanisms to treatment. Pain Rep. 2017;2(2):e588. doi:10.1097/pr9.0000000000000588
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Emotional Allodynia Questionnaire: Preliminary Validation and Clinical Phenotyping in Fibromyalgia
Corriero A, Giglio M, Pilolla A, Galdini F, Mucci O, Vurro M, Fornarelli F, Di Venosa C, Trerotoli P, Puntillo F
Journal of Pain Research 2026, 19:607309
Published Date: 3 June 2026