Back to Journals » Infection and Drug Resistance » Volume 19
Critical Gaps in Infection Prevention and Control in Somalia: Insights from the 2024 Nationwide Harmonized Health Facility Assessment Data
Authors Adam AA ![]() , Mohamed MH, Osman NH
, Mohamed MH, Osman NH ![]()
Received 22 December 2025
Accepted for publication 24 February 2026
Published 3 March 2026 Volume 2026:19 581753
DOI https://doi.org/10.2147/IDR.S581753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Abdikarim Abdi Adam,1,2 Mohamed Hassan Mohamed,1 Nor Haji Osman1,3
1Department of Medicine and Surgery, Faculty of Medicine and Health Sciences, Jamhuriya University of Science and Technology, Mogadishu, Somalia; 2Department of Environmental Health and Climate, IPC Section, Federal Ministry of Health and Human Services, Mogadishu, Somalia; 3Department of Policy and Planning, HIS Section, Directorate of Health and Human Services, Banadir Regional Administration, Mogadishu, Somalia
Correspondence: Abdikarim Abdi Adam, Email [email protected]
Background: Preventing outbreaks, antibiotic resistance, and healthcare-associated infections (HAIs), infection prevention and control (IPC) is the cornerstone of safe, robust health systems. There is little data on IPC readiness across the country in Somalia due to its weak health system. The study aims to evaluate the preparedness of IPC systems in Somali healthcare facilities by looking at policies, fundamental procedures, and essential resources; to find gaps that guide focused interventions to improve patient safety and the resilience of the health system.
Methods: We carried out a cross-sectional secondary analysis of the 2024 Harmonized Health Facility Assessment (HHFA), which included 1,219 healthcare facilities of various categories spread over six states. Data were collected through structured interviews, observations, and facility record reviews. IPC indicators were presented using descriptive and inferential statistics. STATA Version 16 was used for the analyses, and a significance level of p < 0.05 was used.
Results: All Somali facilities have inadequate IPC readiness. Just 24% and 18%, respectively, have rules for standard precautions and healthcare waste management; 21% reported waste management training for workers. Hand hygiene supplies (39%), sterilizing equipment (26%), gloves (87%), masks (61%), and protective gowns (61%) were among the critical resources that differed in availability. There were significant regional differences (p < 0.001), with Benadir frequently having better resources than Southwest, Jubaland, Puntland, Galmudug, and Hirshabelle.
Conclusion: This study identifies significant gaps in the infection prevention and control (IPC) systems of Somali healthcare facilities, such as a lack of resources, procedures, and regulations that are critical to patient safety. Geographical disparities were apparent. These results underline the necessity of targeted, system-wide interventions to raise IPC readiness, increase resource accessibility, and guarantee uniform policy integration and training, all of which will contribute to the development of a more secure and robust healthcare system in Somalia.
Keywords: personal protective equipment, waste management, healthcare facilities, harmonized health facility assessments, Somalia, infection prevention and control
Introduction
Preventing healthcare-associated infections (HAIs), reducing antibiotic resistance, and ensuring patient safety all depend on infection prevention and control.1 Resilient health systems are built on strong IPC systems.2,3 Successful IPC implementation is extremely difficult in many low- and middle-income nations,4,5 including Somalia. Although IPC is widely acknowledged as a vital component of the health system, little is known about IPC readiness in Somalia due to the nation’s fragile healthcare system and persistent sociopolitical issues.6
The World Health Organization (WHO) developed a comprehensive, standardized tool, the Harmonized Health Facility Assessment (HHFA), to evaluate the performance and readiness of healthcare facilities. Service availability, service preparedness, care quality, and administration and finance are the four primary areas in which the instrument assesses important aspects of health system performance. Infrastructure, personnel, equipment, diagnostic capabilities, and quality assurance systems are among the areas that are the focus of its standalone questionnaires. Additionally, the HHFA incorporates combined questionnaires that answer fundamental and supplementary questions on management and finance, as well as service availability, preparedness, and quality. With the use of this tool, health systems may make sure that service delivery satisfies the necessary requirements for both organizational effectiveness and patient care.
This study utilizes data from the 2024 Harmonized Health Facility Assessment (HHFA). With its thorough analysis of vital health infrastructure, personnel, equipment, and IPC procedures, it offers insightful information for enhancing patient safety and system resilience. Knowing the gaps in service delivery and readiness is essential for directing policy decisions and interventions in Somalia, since IPC resources are frequently insufficient. Many low- and middle-income countries are still far from this goal, according to recent, high-quality data.7–9 Healthcare-associated infections (HAIs), infectious disease outbreaks, and the emergence of antimicrobial resistance (AMR) can be prevented through infection prevention and control (IPC), a fundamental component of safe, resilient health systems. For national and facility IPC programs, global guidance identifies a set of WHO “core components” that collectively determine program efficacy. These components include governance, guidelines, education and training, surveillance, multimodal improvement strategies, monitoring and feedback, workload/staffing, and built environment and supplies. In low-resource and fragile environments, where structural limitations, labor shortages, and restricted access to supplies often lead to suboptimal IPC program maturity and poor compliance with minimum IPC requirements, the implementation and sustained practice of IPC measures remain highly variable despite this established framework.10–14 A global study of 106 countries and their healthcare facilities found that only about 3.8% of the countries had fulfilled all minimum national Infection Prevention and Control (IPC) requirements, and only about 15% of the facilities met the standard. The study emphasizes the critical need for targeted investments and legislative actions to improve global health security by pointing out significant gaps in IPC readiness, particularly in low- and middle-income countries (LMICs).15,16 Similar studies show only around 55% of standard precaution items were regularly available, according to a multi-country study conducted across six low- and middle-income countries (LMICs), which included roughly 6,054 healthcare facilities. The survey also showed that important service sectors, such as neonatal healthcare and tuberculosis care, had especially poor readiness, with rural and NGO-run hospitals being disproportionately impacted. These results demonstrate the ongoing systemic deficiencies in Infection Prevention and Control (IPC) infrastructure, underscoring the necessity of focused interventions to guarantee fair access to critical IPC resources across institution types and geographical locations in LMICs.17 In the African Region, the outbreak assessment revealed 60.2%, with more than 30% of institutions scoring below 50% and crucial elements, including isolation, personal protective equipment, and staff training, continued to fall below 30%. Together, these results highlight enduring regional and worldwide IPC shortcomings, highlighting the critical need for focused funding, legislative changes, and fair resource distribution to improve patient safety and healthcare readiness.18 Significant differences in facility preparedness were found in a study on infection prevention and control (IPC) in primary care and hospitals among African nations. Only around 68% of primary healthcare (PHC) facilities have basic hand-hygiene facilities, compared to about 87% of hospitals. Additionally, just around 26% of PHC facilities in ten countries have official IPC rules in place. The study identifies significant gaps in primary care settings, including severe staff training and supply shortages, highlighting the pressing need for focused interventions to improve IPC at the front lines of healthcare delivery.19 An assessment of 25 healthcare facilities in Rwanda found that 96% of them lacked full-time IPC personnel and that IPC protocol implementation and training were seriously lacking. The vulnerability of healthcare settings to illnesses linked to healthcare was highlighted by the identification of critical deficiencies in human resources, staff capacity building, and infection-resistant protocols. This underscored the urgent need for improved workforce development and standard IPC practices.20 The IPCAF assessments of 307 facilities in Somalia revealed a mean score of 136/800 (“Inadequate”), with about 75% of facilities falling short of IPC criteria due to inadequate programs, policies, and training in the face of violence and unstable infrastructure. These results highlight the critical need for focused funding, staff development, and context-sensitive interventions to improve health system resilience and protect patient safety. They also parallel regional and global IPC shortages.21 There are still significant shortages in IPC programs, guidelines, training, monitoring, and staffing in Somali, African, and worldwide contexts. Particularly in low-resource and conflict-affected contexts, the evidence is primarily cross-sectional and provides no insight into relationships to HAI rates, longitudinal trends, or intervention impact. IPC performance is further hampered by metric variability and structural issues in Somalia, including weak systems, insecurity, and inadequate funding. These deficiencies demonstrate the critical necessity for all-encompassing, system-wide approaches that incorporate routine IPC procedures outside of epidemic response, leadership, surveillance, and training. This study provides a nationwide assessment of IPC readiness in Somalia, using standardized, harmonized health facility assessment data in 2024 to examine the availability of policies, core IPC practices, and critical resources across healthcare facilities in Somalia, highlighting gaps, and informing targeted interventions to strengthen health system resilience and patient safety in fragile settings
Methods
Study Design and Participants
This study used a cross-sectional analytical design and secondary data from the 2024 Harmonized Health Facility Assessment (HHFA). The HHFA is a standardized national survey instrument created by the World Health Organization (WHO) to assess the efficiency, accessibility, and readiness of healthcare institutions to deliver critical medical services. Every healthcare facility in Somalia, including hospitals, health clinics, primary health units, and facilities run by public, private, and community-based groups, was evaluated. Infrastructure, equipment, human resources, service delivery, and infection prevention and control (IPC) are just a few of the areas that the HHFA looks at. The HHFA supports evidence-based decision-making, identifies performance gaps in the health system, and influences the creation of national and subnational policies as well as the distribution of resources by offering uniform, comparable data.
Sampling Design
The HHFA used a sample strategy that was nationally representative and was based on the Ministry of Health’s master facility list. A stratified random sample technique was used to guarantee sufficient representation by ownership, facility type, and geographic area. Stratification made it possible for weighted analysis to represent national estimates and improved the comparability of results across regions. Excluded were facilities that were unavailable or not in use at the time of data collection. Banadir (n = 209), Galmudug (n = 146), Hirshabelle (n = 118), Jubaland (n = 160), Puntland (n = 316), and South West State (n = 270) comprised the final study of 1,219 facilities.
Data Collection Procedure
From March to August 2024, skilled field teams collected data under the direction of the Ministry of Health and WHO. To improve precision and consistency, standardized HHFA tools and online data gathering systems were used. Direct observation, a study of facility records, and structured interviews with facility management or assigned IPC focal points were all part of the assessment process. IPC guidelines and committees, hand hygiene facilities, waste management systems, staff training records, and the provision of personal protective equipment (PPE) were all important areas.
Data Quality Assurance
Several methods of quality control were used to guarantee the authenticity and trustworthiness of the data. Intensive training was given to data collectors on field methods, ethical issues, and data gathering instruments. Supervisors reviewed the supplied data every day to ensure it was comprehensive and logically consistent. The digital platform was utilized to implement real-time data validation, thereby reducing entry errors. Additionally, to confirm responses and guarantee adherence to established HHFA processes, periodic spot checks and back-checks were conducted. The Ministry of Health collaborated with the WHO and technical partners to clean and validate the final datasets before analysis.
Data Analysis
The IPC preparedness area of the HHFA framework was the main focus of the analysis. Before analysis, Microsoft Excel was used to arrange and clean the raw data. Facility characteristics and IPC indicators were compiled using descriptive statistics, such as percentages and frequencies. The Chi-square test was used for inferential analysis to evaluate relationships between categorical data. STATA Version 16 was used for every analysis, and a significance level of p < 0.05 was established.
Descriptive Analysis
The distribution of health facilities in Somalia by state, region, Type of facility, ownership, and management is shown in Table 1. With the highest percentage (25.9%) found in Puntland, followed by Southwest (22.2%) and Banadir (17.2%). Facilities were concentrated in Banadir (17.2%) and Bay (10.6%). Nearly half (48.2%) of the facilities were health centers, followed by private clinics (16.2%) and primary health units (19. 2%).In terms of management, public management accounted for the majority of facilities (51.9%), with private organizations and NGOs managing the remaining facilities (25.4% and 2.3%, respectively). Likewise, the government held around half of the facilities (50.0%), followed by facilities owned by NGOs (21.3%) and private companies (20.1%).
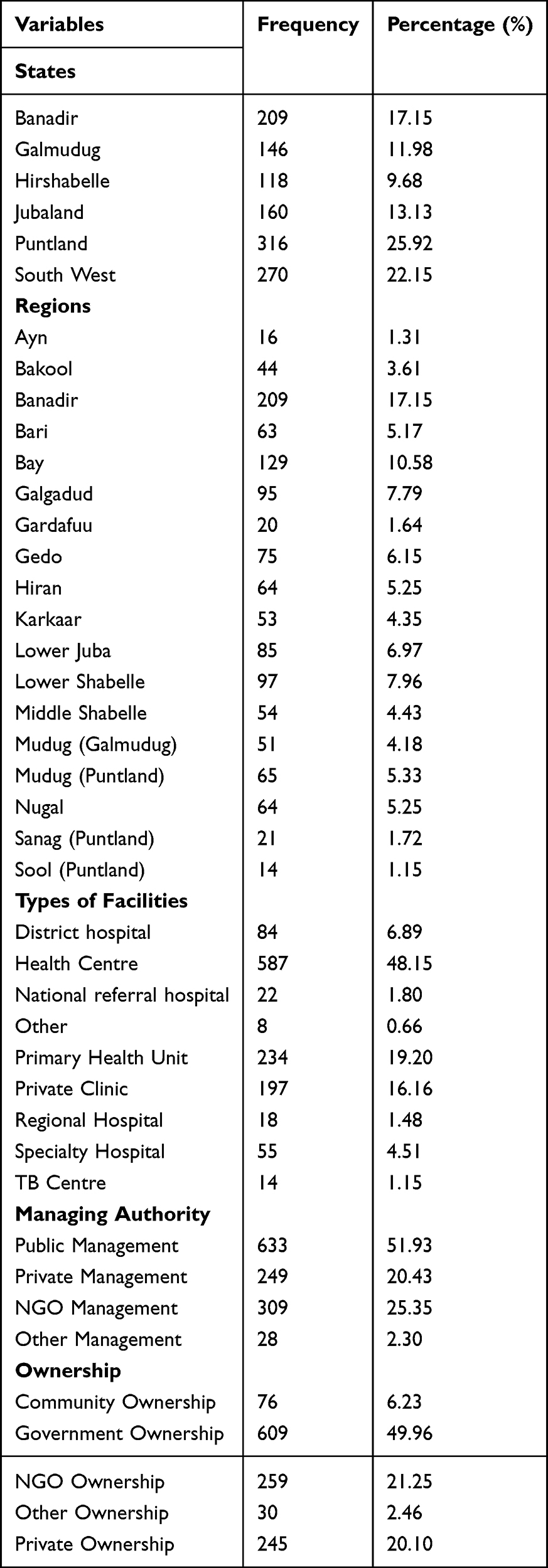 |
Table 1 Health Facility Distribution by State, Region, Type, Ownership, and Management |
The availability of guidelines, staff training, hand hygiene infrastructure, waste management systems, and personal protective equipment was among the many aspects of Infection Prevention and Control (IPC) preparedness that showed significant gaps, as Table 2 Illustrates. Critical deficiencies in policies, resources, and procedures were found when healthcare facilities’ Infection Prevention and Control (IPC) readiness was evaluated. Important infection prevention and control (IPC) guidelines and resources were absent from most facilities. Just 18.5% had waste management rules, and only 24.5% had instructions for standard precautions. There was little staff training on healthcare waste management (21.4%). 38.8% of facilities had hand hygiene supplies, whereas 79.6% had disposable items and 67.0% had latex gloves.
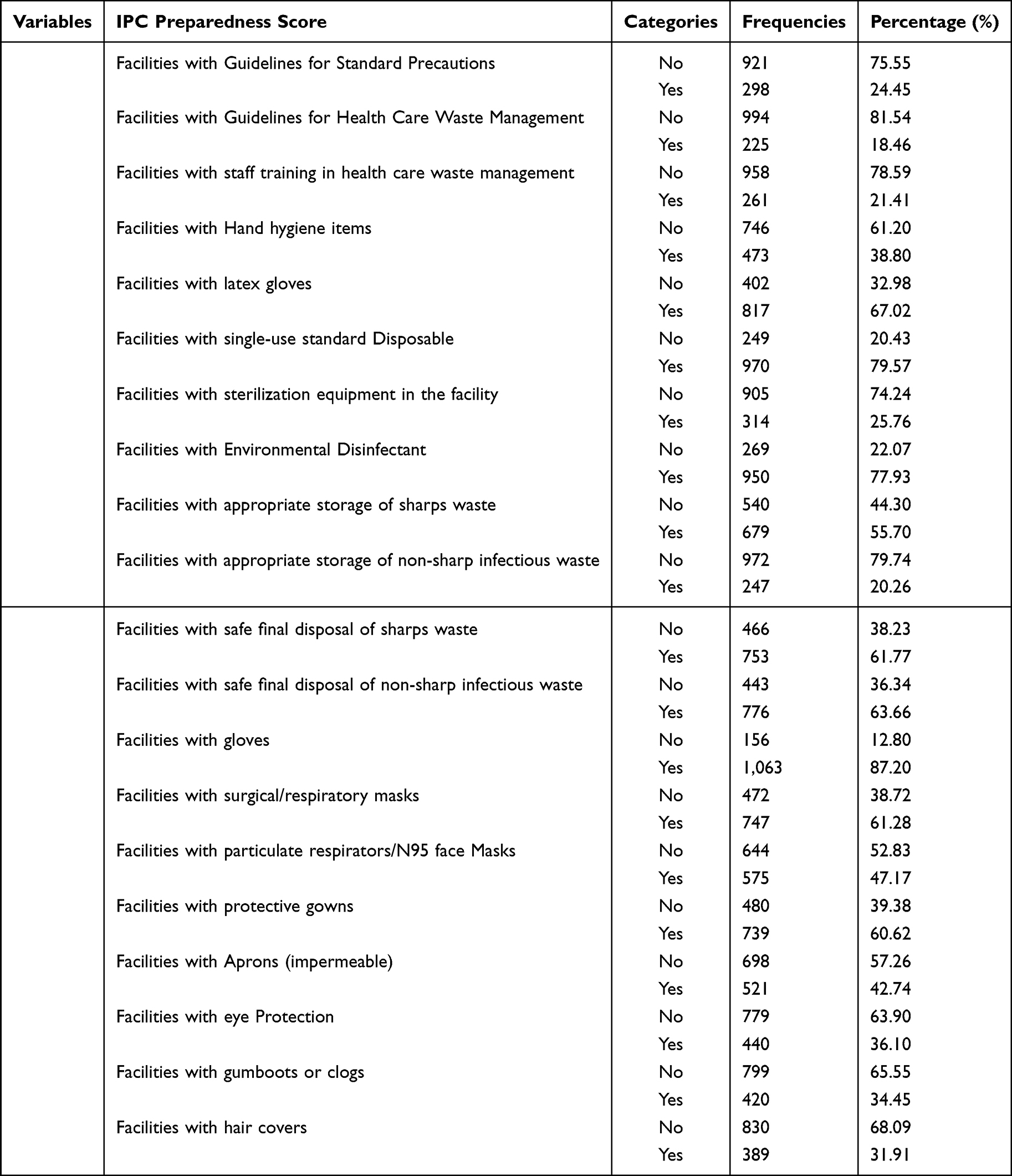 |
Table 2 Facility Indicators and Components of the IPC Preparedness Score |
There was a lack of essential IPC infrastructure: just 25.8% had sterilizing supplies, and 77.9% had disinfectants. Inconsistent safe waste management methods were observed; only 63.7% of respondents ensured safe disposal of non-sharp waste, whereas 55.7% had proper storage for sharps and 20.3% for non-sharp waste.
The availability of personal protective equipment (PPE) varied. Aprons (42.7%), eye protection (36.1%), gumboots (34.5%), and hair covers (31.9%) were less readily available than gloves (87.2%), masks (61.3%), gowns (60.6%), and N95 respirators (47.2%). Overall, the data shows significant gaps in IPC readiness across Somali healthcare facilities, including inadequacies in PPE coverage, staff training, policy execution, and the availability of necessary resources.
Inferential statistics were used to investigate the associations between facility characteristics and Infection Prevention and Control (IPC) preparedness indicators. In particular, the Chi-square (χ2) test of independence was employed to ascertain whether categorical variables, such as the existence of IPC guidelines, the accessibility of necessary PPE, staff training, and appropriate waste management practices, were significantly correlated across various healthcare facility types or geographical areas. When analyzing categorical data, the Chi-square test can be used to determine if observed frequency differences are likely the result of chance or point to a statistically significant association. For every comparison, the χ2 statistic and associated p-value were presented together with the frequency and percentage of facilities with and without a particular IPC metric. Statistical significance was defined as a p-value of less than 0.05, which indicated a significant relationship between the variables.
Table 3 above illustrates notable and statistically significant geographical disparities in IPC preparedness across Somali healthcare facilities. To determine the relationship between state and specific infection prevention and control (IPC) indicators across Somalia’s healthcare Facilities, the chi-square (χ2) test was employed. All IPC-related factors under investigation showed statistically significant differences (p < 0.001), suggesting that facility implementation and readiness varied significantly between states.
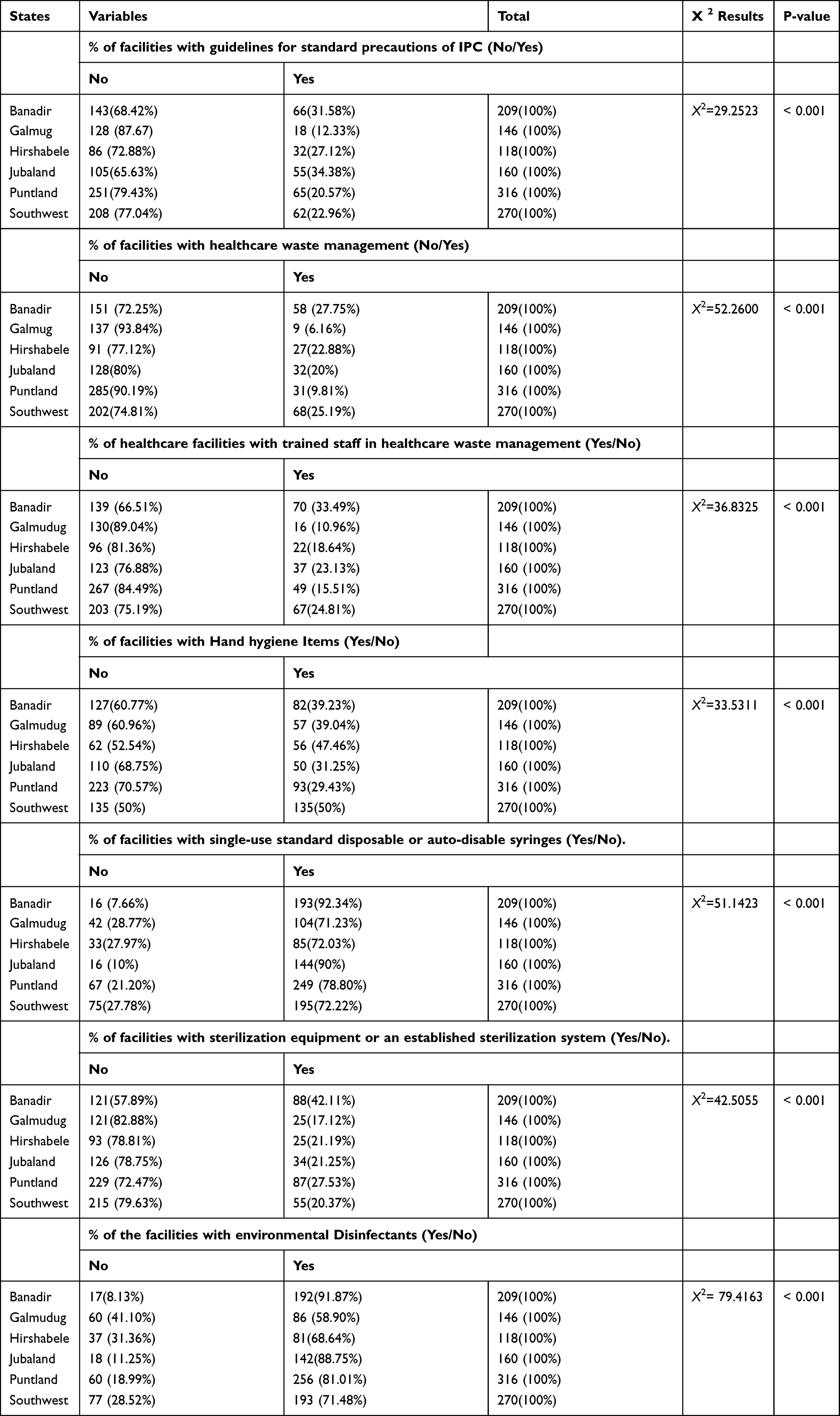 |
Table 3 Regional Differences in IPC Readiness Indicators Across Somali Healthcare Facilities |
All infection prevention and control (IPC) variables by state showed statistically significant differences (p < 0.001) according to chi-square analysis. These results reveal significant geographical disparities in the implementation and capacity of the IPC in the Somali states.
Discussion Section
This study assessed IPC readiness across Somali healthcare facilities using data from the 2024 Harmonized Health Facility Assessment (HHFA). It found important gaps in basic IPC materials, staff training, and policies that differed greatly by region, highlighting the need for focused interventions to improve infection prevention across the country.
These findings underscore the severe constraints in Somalia conflict-affected health system, which is characterized by significant regional disparities and severe resource constraints that cumulatively impede the uniform application of IPC standards across the country.
Our study is in line with the HHFA conducted in Ghana; there was significant regional variance in the application of Infection Prevention and Control (IPC) guidelines, with just 28% of health facilities. There are significant gaps in the workforce’s ability to implement IPC effectively, as evidenced by the fact that only about 25% of facilities reported having staff trained through accredited IPC programs. Higher-level hospitals generally demonstrated stronger IPC preparedness and compliance, whereas lower-level facilities fell behind, according to the assessment. This finding highlights structural and resource differences that threaten uniform IPC standards throughout the healthcare system15[1]. Ghana and Somalia both exhibit low IPC preparedness, with less than one-third of facilities having staff training and guidelines. They both have to deal with geographical differences. However, Ghana’s inequalities are primarily structural, with higher-level hospitals outperforming lower-level facilities, whereas Somalia’s shortcomings are caused by conflict and acute resource scarcity.
The majority of the 1,219 facilities included in the assessment were primary health units and health centers. Our study, consistent with other study conducted in Somalia which shows a high percentage of primary-level facilities (68.8%), which is consistent with the reported majority of primary health units and health centers, a dominant public (government) ownership, and greater representations, perhaps as a result of similar patterns of service delivery and health system structure that prioritize public primary care throughout the regions.1 in addition to Similar studies were found in Ethiopia,21 Uganda, and Bangladesh.22 Around 67% are Primary Health units and Health centers. This reflects proposals for similar health system architectures that prioritize preventive care and community-level service delivery. However, regional resource distribution techniques, investments in health infrastructure, and decentralization policies may differ slightly among nations. The majority of government ownership and public administration in Somali facilities is in line with research from Tanzania and Kenya.23,24 where the foundation of service delivery is made up of government facilities. However, compared to neighboring countries, where non-state players play a more significant role and frequently cover vital service gaps in rural and conflict-affected areas, private and NGO-operated facilities play a comparatively limited role. In our study, in line with other studies conducted in Somalia.1,25,26 The fact that our results are consistent with data at the national level indicates that the shortcomings noted, such as a lack of standards and regulations, gaps in training, and deficiencies in supply and infrastructure, are a component of Somalia’s systemic health system problems, which also include fragility, a lack of funding, a shortage of human resources, poor governance and oversight, and the legacy of conflict. However, compared with national waste management surveys reporting less than 50% safe disposal rates, our results showed slightly better performance in sharps storage (56%) and safe final waste disposal (62–64%).25 This could be because we concentrated on major tertiary and urban facilities, which typically have stronger logistical and donor support. These discrepancies most likely result from differences in the kind of facility, the extent of the sampling, and the exposure to treatments. However, the overall alignment highlights ongoing national IPC gaps, including weak governance in health facility management, insufficient infrastructure, and insufficient training. Our research shows that there are significant gaps in IPC preparedness across Somali healthcare facilities, as seen by the lack of environmental disinfectants, hand hygiene supplies, sterilization equipment, staff training, and guidelines. In order to improve infection control across the country, these findings underscore the ongoing systemic difficulties in IPC implementation and the pressing need for focused capacity-building, resource allocation, and consistent protocols. Poor healthcare waste management (HCWM), with low percentages of trained personnel and operational waste systems, is demonstrated by pooled evidence from sub-Saharan Africa. Training, policy, and resource limitations are identified as important determinants. Our findings, which show relatively poor staff training and HCWM system coverage throughout several Somali states, are consistent with these regional findings.25,27,28 Significant deficiencies were identified by our assessment in Somali healthcare facilities in several important IPC domains. Our study is consistent with the availability of basic infection control items and personal protective equipment.29
IPC readiness is consistently poor throughout the evaluated nations, especially in Ghana and Somalia, where staff training coverage is minimal and less than one-third of facilities have explicit IPC guidelines. Ghana shows more pronounced differences between higher- and lower-level facilities, whereas Somalia’s shortcomings are exacerbated by conflict and acute resource scarcity. Inadequate public reporting of IPC-specific metrics in Burkina Faso, Malawi, and Kenya restricts direct cross-country comparisons. The results point to important deficiencies in IPC procedures, such as the lack of sterilization equipment, waste management-trained staff, and standard precaution instructions. Progress is further hampered by inadequate infrastructure, inadequate governance, and inadequate training programs. Our findings highlight the necessity of strong waste management systems, better workforce development, and comprehensive national IPC policies.
Limitations
This study’s capacity to show causal correlations is limited by its cross-sectional methodology and dependence on secondary data. Furthermore, the situation in more remote or rural healthcare settings might not be adequately represented by the emphasis on urban and university facilities. To gain a better understanding of the long-term effects of IPC interventions, more primary data collection and longitudinal research are required.
Conclusion
The study’s findings highlight how urgently Somalia’s healthcare system needs to be strengthened by the implementation of IPC standards, more funding, and focused interventions. It will need a concerted effort from national and international partners to close these IPC gaps, with an emphasis on governance, infrastructure, and training to increase patient safety and health system resilience.
Abbreviation
HHFA, Harmonized Health Facility Assessments; IPC, Infection prevention and control; HAI, Healthcare-associated infections; AMR, antimicrobial resistance; WHO, World Health Organization; LMICs, low- and middle-income countries; PHC, primary healthcare; PPE, personal protective equipment.
Data Sharing Statement
All the data and its supporting files are within the manuscript and are available. The dataset used in this research is openly accessible and available online at https://somalia-platform.netlify.app/.
Ethics Approval and Consent to Participate
Verbal informed consent was obtained from all participants prior to data collection. The consent process and all study procedures were reviewed and approved by the National Institute of Health and Somalia’s Ethics and Research Committee. The National Institute of Health and Somalia’s Ethics and Research Committee gave the study ethical approval (Approval No. NIH/IRB/126/Dec/2025), and it was carried out in compliance with relevant institutional rules and the Declaration of Helsinki’s tenets. Additionally, the Ministry of Health’s Health Information System (HMIS) Section in Mogadishu, Somalia, authorized data access after a formal request outlining the goal of the study, the particular secondary data needed, and its intended use for scholarly research was submitted.
Acknowledgments
We are really appreciative of the Ministry of Health and Human Services, Somalia, for granting access to the data and making this study possible.
Author Contributions
Each author contributed significantly to the work reported, whether it was in the areas of conception, study design, execution, data acquisition, analysis, and interpretation, or all of these; participated in the article’s drafting, revision, or critical review; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no competing interests in this work.
References
1. Adam AA, Mohamed HD, Anyiam FE. Assessment of infection prevention and control in somali healthcare facilities using the WHO infection prevention and control assessment framework. Antimicrob Resist Infect Control. 2025;14(1):103. doi:10.1186/s13756-025-01584-9
2. Saravanos GL, Islam MS, Huang Y, et al. Infection prevention and control programme priorities for sustainable health and environmental systems. BMC Global Public Health. 2024;2(1):6. doi:10.1186/s44263-023-00031-4
3. Debie A, Nigusie A, Gedle D, Khatri RB, Assefa Y. Building a resilient health system for universal health coverage and health security: a systematic review. Glob Heal Res Policy. 2024;9(1):2. doi:10.1186/s41256-023-00340-z
4. Asghar S, Atif M, Masood I, Khan M. A comprehensive review of current status of infection prevention and control program in low- and middle-income countries. Infection Disease Health. 2025;30(3):260–11.
5. Shamas N, Stokle E, Ashiru-Oredope D, Wesangula E. Challenges of implementing antimicrobial stewardship tools in low to middle income countries (LMICs). Infect Prev Pract. 2023;5(4):100315.
6. Id BB, Scambler S, Najwa A, Khairuddin M, Gallagher E. Health system strengthening in fragile and conflict-affected states: a review of systematic reviews. PloS one. 2024;19(6):1–33. doi:10.1371/journal.pone.0305234
7. World Health Organization. Global report on infection prevention and control. Who. 2022. 1–182 p.
8. Tomczyk S, Twyman A, de Kraker MEA, et al. The first WHO global survey on infection prevention and control in health-care facilities. Lancet Infect Dis. 2022;22(6):845–856. doi:10.1016/S1473-3099(21)00809-4
9. Maki G, Zervos M. Health care-acquired infections in low- and middle-income countries and the role of infection prevention and control. Infect Dis Clin North Am. 2021;35(3):827–839. doi:10.1016/j.idc.2021.04.014
10. Guidelines Review Committee IHS. Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level [Internet]. World Health Organization. 2016. Available from: http://apps.who.int/bookorders.
11. Storr J, Twyman A, Zingg W, et al. Core components for effective infection prevention and control programmes: new WHO evidence-based recommendations. Antimicrob Resist Infect Control. 2017;6(1):6. doi:10.1186/s13756-016-0149-9
12. Tomczyk S, Storr J, Kilpatrick C, Allegranzi B. Infection prevention and control (IPC) implementation in low-resource settings: a qualitative analysis. Antimicrob Resist Infect Control. 2021;10(1):113. doi:10.1186/s13756-021-00962-3
13. Abbas S. The challenges of implementing infection prevention and antimicrobial stewardship programs in resource-constrained settings. Antimicrob Stewardship Healthcare Epidemiol. 2024;4(1):e45.
14. Access I, Services I, Outcomes BH. USAID medicines, technologies, and pharmaceutical serviceS (MTAPS) program strengthening infection prevention and control (IPC) at the national and health care facility levels in Bangladesh. 2024.
15. Hinson C, Kilpatrick C, Rasa K, et al. Global surgery is stronger when infection prevention and control is incorporated: a commentary and review of the surgical infection landscape. BMC Surg. 2024;24(1):397. doi:10.1186/s12893-024-02695-7
16. Dempsey K. Exploring the context of governance, structure and evaluation of australian infection prevention and control exploring the context of governance, Structure and Evaluation of Australian Infection Prevention and Control. 2026.
17. Biswas MAAJ, Adams SJ, Xing L, Mondal P, Szafron M. Exploring healthcare facilities’ readiness for standard precautions in infection prevention and control: a cross-country comparative analysis of six low- and middle-income countries using national cross-sectional surveys. J Glob Health. 2025;15:4205. doi:10.7189/jogh.15.04205
18. Kabego L, Balde T, Barasa D, et al. Analysing the implementation of infection prevention and control measures in health care facilities during the COVID-19 pandemic in the African Region. BMC Infect Dis. 2023;23(1):824. doi:10.1186/s12879-023-08830-8
19. Deeves M, Bancroft E, Lessa FC, Godfrey C, Allegranzi B. The case for strengthening infection prevention and control in primary care. J Infect Dis. 2025;232Supplement_2:S140–4. doi:10.1093/infdis/jiaf371
20. Irakiza JJ, Mazimpaka C, Ndatimana D, et al. Status of infection prevention and control programs in 25 facilities of Rwanda: results from the WHO infection prevention and control assessment framework. Public Health Challenges. 2024;3(2):e183. doi:10.1002/puh2.183
21. Tiruneh MG, Fenta ET, Delie AM, Masresha SA. Service availability and readiness to provide comprehensive emergency obstetric and newborn care services in post–conflict at North Wollo Zone hospitals, Northeast Ethiopia: mixed survey. BMC Health Serv Res. 2023:1–10. doi:10.1186/s12913-023-09165-5
22. Thapa DK, Acharya K, Karki A, Cleary M. Health facility readiness to provide antenatal care (ANC) and non-communicable disease (NCD) services in Nepal and Bangladesh: analysis of facility-based surveys. PLoS One. 2023;18(3):e0281357. doi:10.1371/journal.pone.0281357
23. Sriram V, Yilmaz V, Kaur S, Andres C, Cheng M, Meessen B. The role of private healthcare sector actors in health service delivery and financing policy processes in low-and middle-income countries: a scoping review. BMJ Glob Heal. 2024;8(Suppl 5).
24. Peck R, Mghamba J, Vanobberghen F, et al. Preparedness of Tanzanian health facilities for outpatient primary care of hypertension and diabetes: a cross-sectional survey. Lancet Glob Heal. 2014;2(5):e285–92.
25. Adam AA, Anyiam FE, Shube MA, Mohamed HD, Ahmed HA, Osman NH. Assessment of Medical Waste Segregation, Disposal Practices for Infectious and Sharps Waste in Healthcare Facilities in Somalia: implications for Infection Prevention and Control. Infect Drug Resist. 2025;18:3605–3615. doi:10.2147/IDR.S525134
26. Janay AI, Kilic B, Unal B. Healthcare workers’ compliance with COVID-19 2 preventive and control measures at De Martino. medRxiv. 2024. doi:10.1101/2024.03.29.24305060
27. Berihun G, Walle Z, Desye B, et al. Healthcare waste management practices and associated factors among healthcare workers in Sub-Saharan Africa: a systematic review and meta-analysis. PLoS One. 2025;20(10 October):1–25. doi:10.1371/journal.pone.0334290
28. Mugambe RK, Wanyenze RK, Ssekamatte T, et al. Infection prevention and control and water, sanitation, and hygiene status of healthcare facilities in the Greater Kampala Metropolitan region during the COVID-19 pandemic in Uganda. PLOS Water. 2025;4(1):1–24. doi:10.1371/journal.pwat.0000189
29. Hakim S, Chowdhury MAB, Uddin MJ, Leslie HH. Availability of basic infection control items and personal protection equipment in 7948 health facilities in eight low- and middle-income countries: evidence from national health system surveys. J Glob Health. 2024;14:1–12. doi:10.7189/jogh.14.04042
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Medical Waste Segregation, Disposal Practices for Infectious and Sharps Waste in Healthcare Facilities in Somalia: Implications for Infection Prevention and Control
Adam AA, Anyiam FE, Shube MA, Mohamed HD, Ahmed HA, Osman NH
Infection and Drug Resistance 2025, 18:3605-3615
Published Date: 22 July 2025