Back to Journals » Patient Preference and Adherence » Volume 17
Credentials That Matter While Selecting a Surgeon for Major Surgical Treatment
Authors Raza A, Furtado KM, Mathur D
Received 5 June 2023
Accepted for publication 7 September 2023
Published 5 October 2023 Volume 2023:17 Pages 2487—2494
DOI https://doi.org/10.2147/PPA.S404570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Arif Raza,1 Kheya Melo Furtado,1,* Devasheesh Mathur2,*
1Healthcare Management, Goa Institute of Management, Goa, India; 2Strategy and General Management, International Management Institute, New Delhi, India
*These authors contributed equally to this work
Correspondence: Arif Raza, Healthcare Management, Goa Institute of Management, Goa, 403505, India, Tel: +91 7566693564, Email [email protected]
Purpose: The credentials of surgeons, which include elements such as medical degree and length of practice, are vital information that forms a perception of their expertise in the patients’ minds. The specific credentials that matter to patients and how important they are have not been sufficiently studied. The objective of this study was to assess the relative importance that patients assign to the specific credentials of a surgeon while selecting one for surgical treatment.
Methods: This study was conducted using the constant-variable-value vignette (CVVV) method. Four credentials– medical degrees, duration of practice, medical college attended, and type of surgeries performed – were assessed for their relative importance to patients. The participants were provided with vignettes of medical situations that required major surgical intervention and profiles of surgeons who could perform the required surgery, each dominating the others in a specific credential. The participants allocated a total of 10 points across the four surgeons proportionate to their preferences. The response data were analyzed using descriptive statistics, ANOVA and t-tests.
Results: The highest mean score of 3.73 (SD 2.21) was observed for the surgeon with focused experience, followed by 2.55 (1.57) for the surgeon with the best medical degrees, 2.17 (1.65) for the surgeon with the longest practice experience, and 1.54 (1.47) for the surgeon from a higher-ranked medical college. The mean of the surgeon with focused experience was significantly higher than that of other surgeons, and the mean of the surgeon with the best medical degrees was significantly higher than that of surgeons with the longest practice experience and the surgeon from the topmost medical college (p < 0.05). Preference did not vary with respondents’ age or gender.
Conclusion: Patients seem to prioritize the focused surgical experience and superior medical degrees in their selection of surgeons.
Plain Language Summary: Undergoing major surgery is an incredibly critical situation for most patients, as it entails not only physical discomfort but also inherent risks. Given the specialized nature of medical care, patients rely heavily on their surgeons for advice and treatment. Therefore, selection of right surgeon becomes paramount for patients facing such decisions. Previous research has elucidated that the perceived level of expertise of a surgeon, significantly influence patients’ choice.
Medical practitioners typically display their credentials as a means of showcasing their expertise. However, specific credentials that hold the most significance in shaping patients’ perceptions of expertise remain unclear. In our study, we simulated various medical scenarios necessitating surgery and presented profiles of surgeons, each possessing distinct sets of credentials. We then solicited participants’ preferences for surgeons by allowing them to allocate points based on their perceived qualifications.
Our findings revealed that patients accord highest importance to a surgeon with relevant experience in the type of surgery required, followed by a surgeon with the most prestigious medical degrees. This indicates that, when it comes to surgical decisions, patients place a premium on focused practical experience over other aspects of a surgeon’s credentials.
Keywords: choice of doctors, preferred surgeon, doctor credentials, doctor qualifications, doctor experience
Introduction
Undergoing specialized medical treatment such as surgery is a critical event in a person’s life. Among various factors, the treating doctor is of paramount importance to the patient owing to the central role they play in the treatment. In healthcare systems that allow patients to choose their healthcare provider, patients tend to choose a doctor they think is the best within their resource constraints. The patients’ ability to make a choice enables them to “vote with their feet”, which is assumed to develop competition among healthcare providers to attract patients.1 In order to attract patients, the competing healthcare providers continuously make efforts to place themselves as the “doctor of choice” in minds of patients. However, to do this effectively, healthcare providers need to know what constitutes the perception of a “doctor of choice” in the minds of patients.
Several factors have been studied that influence the choice of patients to select a doctor. Convenience factors such as distance from home, cost, referral advice from the primary care provider, and quality of the doctor have been commonly reported.2,3 While the number of studies in this context is large, most focus on the behavioral features of doctors, such as communication, friendliness, and personal attention, and not on their technical capabilities. Doctors’ expertise has been identified as an important factor that patients consider.3 However, the credentials that predominantly determine expertise in the minds of patients have not yet been explored. Training or certification of doctors in a particular specialty is viewed as very important to patients.3 But how much patients differentiate between levels of qualification or the relative importance they place on certification over other parameters such as specialization and duration of experience have not been reported.
The number of years of practice, type of specialized training, and case load in a particular operation were identified as important factors for patients,4 but the relative importance of each of these credentials has not been studied.4
Most studies that explore patients’ choice of doctor have been conducted in developed economies.2,3 With socioeconomic, cultural, and healthcare market differences between developed and developing countries, the factors that influence patient choice could differ. Very few studies have been conducted in the context of developing economies. This study is based in India and explores the factors that influence decision-making in patients within developing economies.
Health care in the Indian healthcare system is provided by both public and private providers. Although public health care is offered at nil to nominal prices, the majority of patients (approximately 66.9%) are catered to by private providers.5 In urban regions of the country, 72.9% of people consult a private healthcare provider and 64.7% receive treatment in a private healthcare facility when hospitalization is required.5 While the overall doctor-to-population ratio is low in the country compared with the global average, the presence of doctors, especially specialists, is heavily skewed in urban areas.5 In the absence of any formal referral system and with a presence of multiple specialist doctors, patients in urban areas usually have a wide range of specialist doctors to choose from. An estimated 60–75% of visits to a specialist doctor are self-referred.6,7
Additionally, the influencing factors identified in most studies are generally related to the selection of general practitioners, primary care physicians, or doctors without any reference to the level of treatment involved.2 However, the factors that influence the choice of general practitioners cannot be generalized to the choice of doctors who provide higher-level treatment, such as surgery. The prognosis, risk to patients, side effects, and cost increase with the level and complexity of treatment required. Hence, it is possible that the factors that influence the selection of a doctor in cases of higher-level treatment could differ in type and intensity compared with the selection of a doctor for general or lower-level treatment.
The current literature provides sufficient insights into what determines a patient’s choice of a doctor. However, the role played by specific credentials, such as their level of education, the image of the medical college they attended, the duration and type of their experience, in patients’ decision-making is less explored.
Our study focuses on how much value patients or their family members place on each credential of a specialist doctor when selecting one to obtain a higher level of care. Some studies have identified individual conditions, such as literacy and economic status, as well as market conditions, such as availability and ease of access to healthcare providers, as discriminants of the level of influence that various factors have on making a choice.8 In our study, we specifically assessed the preferences of educated individuals with mid to high socioeconomic status and moderate to good access to healthcare. The reason for studying this group is based on the assumption that, owing to their education, they have better access to information about doctors from sources such as the Internet, and they are better placed to understand the information from a decision-making perspective. Second, for this population, the range of doctors to choose from is less restricted, owing to their better affordability. Finally, with the ongoing demographic transition of the country, it is expected that the number of educated middle-class people living in cities will increase. The urban population of India is currently 34.93%, and is expected to reach 40% by 2030.9 Seventy-three percent of the population are literate.5 Most Indians consider surgery a major or high-level treatment option. Surgery induces stress due to risks, long-term implications for health, and the cost involved. In such a scenario, selection of the right healthcare provider (in this case, the operating surgeon) becomes even more vital to the patient and their family.
Generally, the key credentials that indicate the technical competence of a doctor are their qualifications, the institutions from which their qualifications were obtained, their length of experience, and the type of experience. Private healthcare providers generally highlight doctors’ key credentials in attracting patients. In the provider market, doctors with various combinations of these credentials are available. For example, one doctor may have better qualifications than others, another may have more years of experience, and a third may have obtained their degrees from a reputed medical college. How does a patient reconcile the credential mix of available surgeons when selecting one for themselves or a family member? Very few studies have been conducted worldwide on this topic. Although not for the selection of surgeons, one study assessed the correlation between patient satisfaction and surgeon experience, and reported no such correlation.10 Another study that explored inequality between doctors in the UK based on their place of qualification stated that international medical graduates are treated unequally to those who graduated in the UK.11 Although the two pieces of literature cited here are not directly related to surgeon selection, they indicate that experience and place of qualification could matter in the views of patients. No studies were found in relation to a doctor’s qualifications or specificity of experience.
Materials and Methods
The study was conducted using “vignettes” as this method allows for manipulating variables, in this case the credentials of the doctors, which would not be possible using an observational method.12 Using the constant-variable-value vignette (CVVV) method,13 we created an instrument with hypothetical medical situations in which participants were required to select a surgeon for major surgical treatment of one of their family members. The decision must be made from a list of four surgeons based on the information provided in their profiles. The description of the surgeons consists of four credentials: their medical degrees, the medical colleges they attended, their number of years of practice, and the types of surgeries they perform. The credentials included in the study were selected based on the observation of the profiles of 40 specialist doctors from 5 private hospitals.
We created the profile in such a manner that each surgeon had one distinct credential that was clearly better than the others, whereas the remaining three credentials were basic and similar to the others. Thus, out of the four options of surgeons given to select from, one was best in medical degrees, the second had the longest duration of practice experience, the third completed medical education at the best medical college, and the fourth had most focused experience in the type of surgery required.
For medical degrees, the masters of surgery (MS) degree was considered basic and the M.Ch. considered higher. As per medical education in India, an MS degree requires a minimum of three years of education after the completion of six years of an MBBS degree. An MS degree can be obtained in various disciplines, including general surgery and orthopaedics. A holder of an MS degree is referred to as a surgeon and is entitled to perform surgeries related to their discipline. An M.Ch. degree requires an additional three years of education after completion of the MS degree. An M.Ch. degree is referred to as super-specialization and can be used in different fields of medicine, such as neurology, orthopedics and cancer surgery. This regulation allows an M.S. surgeon to perform any type of surgery within the discipline. We assumed that most patients preferred a surgeon with an M.Ch. degree over a surgeon with only an M.S. degree.
The basic level for medical college attended is kept as a college that ranked between 30 and 50 on the National Institutional Ranking Framework (NIRF) ranking of India, while a college that ranked among the top five was considered a higher-level college for this element. The NIRF ranking is conducted annually by the Ministry of Education, Government of India, in which educational institutions are ranked category-wise according to set criteria and methods, and is indicative of the quality of the institution. We assumed that patients would prefer surgeons who attended a top-ranked medical college.
For the length of practice experience, 6–7 years of experience was considered basic and 14–15 years of experience was used to differentiate surgeons with longer experience. This was to make the difference in the duration of practice experience apparent between the other surgeons and the experienced surgeon. Our assumption is that surgeons with more experience will be preferred by patients over surgeons with less experience.
Lastly, a surgeon with experience of multiple types of surgery in their discipline was considered to have basic experience, while a surgeon with focused experience in performing the specific kind of surgery needed by the patient was considered to have better experience. We assume that surgeons who have focused experience specific to the surgery needed will be preferred by patients over surgeons with generalized experience with multiple types of surgeries.
Table 1 presents the basic and higher credentials.
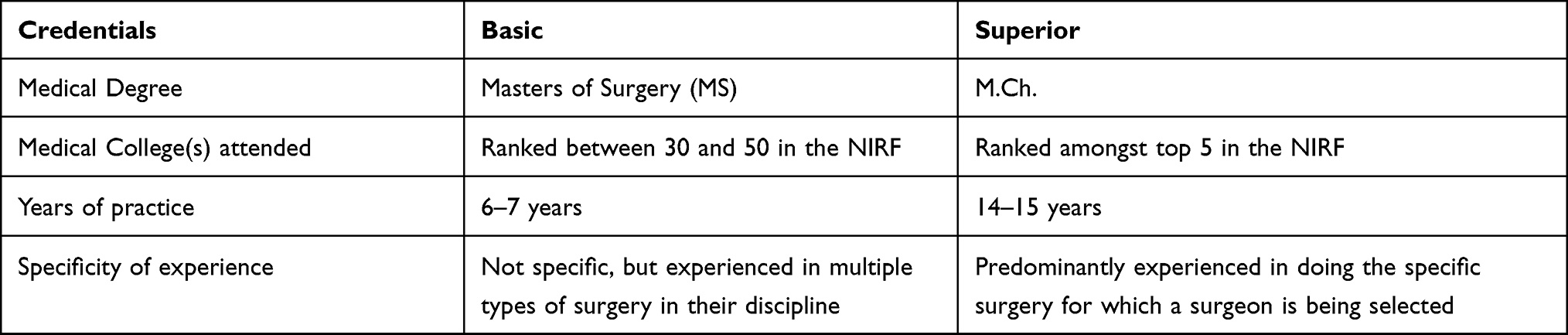 |
Table 1 Credentials Elements of the Surgeons Included in the Study |
To study the relative importance of each of these credentials, the participants were provided with a situation in which one of their family members had a medical condition that required major surgery. We created two medical situations for this purpose: one that required total knee replacement surgery (TKR), and another that required surgical removal of a tumor mass from the abdominal region. For each medical situation, we created a profile of four surgeons with specific credentials that matched the surgery requirements. Each surgeon was better than the other three on one specific credential.
The participants were required to indicate their relative preferences among the four surgeons based on the limited information provided. Relative preference was captured using a constant-sum scale, in which the participants were required to allocate a total of 10 points across the four surgeons in proportion to their level of preference. The participants were free to allocate points as long as the total score allocated across the four surgeons was exactly ten.
Information about the surgeon’s credentials was presented as bullet points. To avoid an effect of the order in which doctors’ credentials were presented, we kept the dominant credentials of each doctor at the top. To avoid bias arising from the surgeon’s gender, all surgeons were identified using their surname, which does not indicate their gender. To avoid bias from differences in surgeons’ religion, surnames indicative of a Hindu person (the dominant religion of the country) were assigned to all four groups.
Data Collection
The participants were students and staff at a postgraduate educational institution. To ascertain whether the respondents could relate to the medical situation, only those with a history of hospitalization (either self or a family member) were included in the study. After briefing participants, data were collected using Qualtrics, a software-based survey tool. To avoid bias due to the sequence in which the surgeons were listed, four versions were created for each situation. In each version, the sequence of doctors was changed to ensure that each surgeon was listed in 1st, 2nd, 3rd and 4th position in different versions of the forms. Immediately after the situation, a question on the realistic perception of the situation was included, and responses were collected on a 10-point scale, with 1 indicating not realistic at all and 10 indicating the most realistic.
Participants were requested to provide basic details, including gender, age, educational level, region of the country to which they belonged, annual household income, and whether they or any of their family members had been admitted to the hospital in the last five years. An open-ended question was also included, asking the respondents to state the basis of their decisions.
Validity
Pilot testing of the instrument was performed with 20 participants (not included in the final sample). The purpose was to ensure that the situation was conveyed effectively, and the participants were clear about what was expected of them. A debriefing meeting was conducted with those who participated in the pilot survey to receive feedback on the instrument and make modifications accordingly.
Analysis
The data were analyzed using descriptive statistics. The mean and standard deviation of the scores received by each surgeon were calculated. Because each surgeon represented a specific dominant credential element, the scores received by the surgeon indicated the scores given by the participant to the surgeon’s dominant credentials. For inferential statistics, ANOVA was used to determine whether the points attributed to a surgeon with specific credentials significantly differed from those of other surgeons. The null hypothesis considered for the statistical analysis was that patients who selected a specialist doctor for treatment ascribe similar importance to the doctor’s medical degree, medical college attended, years of practice, and experience specificity.
While the study explored patients’ preferences, two key limitations of this study must be kept into consideration while interpreting the findings. The first limitation is inherent to the method adopted by the study. Being a vignette study, the participants made decisions in a simulated situation and their decision-making in an actual situation can differ. The second limitation is a possibility of a bias that could be there in participants’ responses. While the study included only those participants who had a history of hospitalization (either self or family), their recall of experience could have varied owing to the difference of time elapsed since hospitalization, type of hospitalization and whether it was for self or a family member. These differences could have affected the responses of participants.
Results
A total of 315 responses were obtained. After filtering out incomplete forms and forms from participants who did not meet the inclusion criteria, data from 212 participants were collected for analysis. 45% of participants were females. All participants were graduates aged between 18 and 30 years, and 35.4% belong to the northern, 18.9% to the western, 30.7% to the southern, and 15% to the eastern and northeastern parts of India. Approximately 5% had graduate-level education in medicine or related fields.
The mean rating for the question “How realistic did the situation described above appear to you?” – was 7.47, with SD of 2.01. This indicates that the participants could relate to the situation to make a realistic decision.
The mean and standard deviation of the points allocated to each surgeon are presented in Table 2.
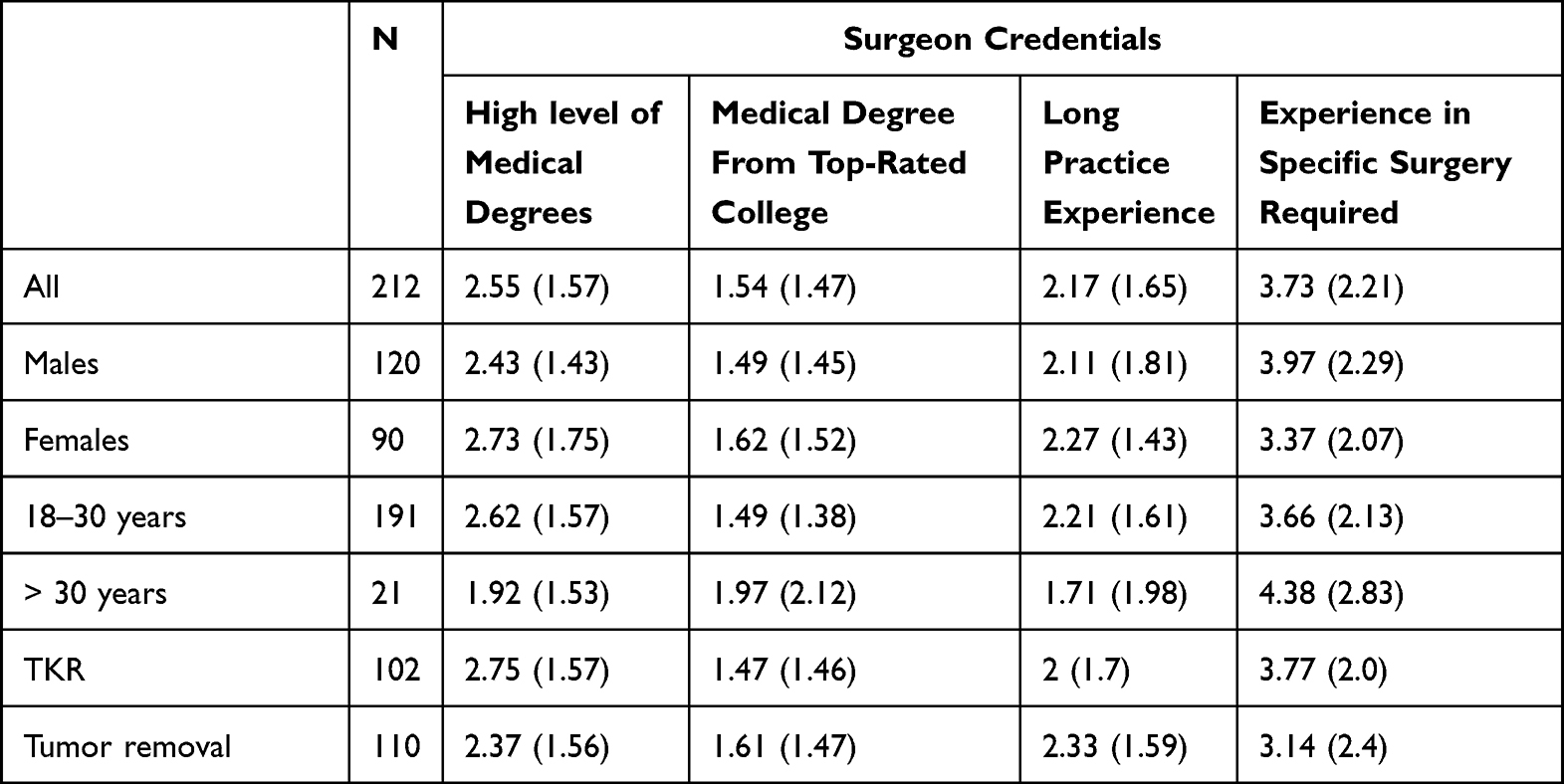 |
Table 2 Scores Allotted to the Surgeons |
Irrespective of the gender, age, or region of the participants, the surgeon with focused experience in the required surgery was the most preferred, followed by the surgeon with the best medical degrees. Surgeons with focused experience were most preferred in both types of medical situations presented to the participants.
The difference in scores attributed to the surgeons was statistically significant (p < 0.05). No significant difference was found between surgeons from the top-rated medical colleges and those with the longest practice experience. The scores awarded to the surgeon with the best medical degrees were significantly higher than those awarded to the surgeon from the top-ranked medical college and the surgeon with the longest practice experience, while the score awarded to the surgeon with focused experience in required surgery was significantly higher than that awarded to the other three surgeons (p < 0.05).
Discussion
Previous studies indicate that choosing a doctor is a complex process, and eventual choices are determined by the interplay between patient and provider characteristics. Various provider characteristics influence choices, such as image, interpersonal skills, trust, and competency. This study specifically focused on identifying the relative importance that patients attribute to different credentials that are usually present in a doctor’s profile when selecting a surgeon for major surgical treatment.
Respondents seemed to attribute differential importance to the credentials of individual surgeons. Of the four credentials studied, the specificity of experience in conducting similar surgeries earlier was given the highest importance. The dominance of this element was observed in participants, irrespective of gender, age group, or region. In the age groups, the older participants attributed even higher importance to the focused experience of the surgeon compared to younger participants. This aligns with the findings of a 2007 study, which observed that the satisfaction of breast cancer patients was highest with surgeons having practical experience specific to breast cancer treatment.14 In some cases where participants justified their choice, “better skills in performing the procedure”, “less likely to err”, and “better quality surgery” were the reasons stated for awarding higher points to surgeons with focused experience. It appears that the preference for experience specificity emanates from the participants’ concerns about the skills of a surgeon, even though the job of a surgeon requires both knowledge and skills. Since surgery is more skill-based than medicine, it needs to be seen whether experience specificity is attributed similar importance when the choice of a non-surgical specialist is to be made.
Surgeons with the highest level of medical degree were assigned the second highest importance. The remarks given by the participants indicate that superior qualifications reflect doctors’ deeper knowledge, which instills a sense of trust. Doctor qualifications have been reported as a significant factor in patient preference in several studies.11,15–17 Doctors with more relevant qualifications are generally preferred by patients.
Experience specificity and superior qualification as the top two preferred credentials indicate that for surgical intervention, the choice of surgeon is driven by their specific skills and knowledge, the perception of which is shaped by their experience specificity and qualifications.
The surgeon from the top-most-rated medical college was rated higher than the surgeon with the longest practice experience, although the difference was not statistically significant. It is evident that on the qualifications front, medical degrees were attributed a higher value than the college from which the degrees were obtained, and on the experience front, the specificity of experience was valued more than the overall length of the experience.
The two surgical situations used in this study belonged to different disciplines – one related to orthopedics and the other to oncosurgery – and in both cases the preference of surgeons was based on similar credential elements. This indicates that the relative importance that patients give to the credential elements of a surgeon may remain the same irrespective of the specialty of care required; this interpretation is limited, however, as only two specialties were undertaken in this study.
While the study explored patients’ preferences, two key limitations of this study must be kept into consideration while interpreting the findings. The first limitation is inherent to the method adopted by the study. Being a vignette study, the participants made decisions in a simulated situation and their decision-making in an actual situation can differ.18 The second limitation is a possibility of a bias that could be there in participants’ responses. While the study included only those participants who had a history of hospitalization (either self of family), their recall of experience could have differed owing to the difference of time elapsed since hospitalization, type of hospitalization and whether it was for self or a family member. The differences could have affected the responses of participants.
Conclusion
The study concluded that different credential elements in a doctor’s profile have different impacts on a patient’s decision when selecting a surgeon for major surgical treatment. While making their selection, the customer may place significantly higher importance on the focused experience of a surgeon on the specific type of surgery required by the patient.
Abbreviations
MBBS, Bachelor of Medicine Bachelor of Surgery; MS, Master of Surgery; M.Ch., Master of Chirurgiae; CVVV, constant-variable-value vignette; NSS, National Sample Survey; NIRF, National Institutional Ranking Framework; TKR, Total Knee Replacement.
Data Sharing Statement
The study was based on primary data, and the same data can be made available for verification. The identities of the study participants cannot be shared.
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the Board of Research Ethics (BORE)of Goa Institute of Management (Approval number: BH032202).
Informed consent was obtained from all participants. The informed consent form included the purpose of the study, the information to be collected, and a confidentiality statement. The participants were given time to read the form, and then accept or reject participation. The participants were also allowed to discontinue before completing their responses, if they wished.
Consent for Publication
The manuscript submitted to this journal has not been published elsewhere and is not under consideration for publication elsewhere.
Acknowledgments
We acknowledge and thank all the respondents of this study, who took time to participate and provide us with the data.
Funding
No financial assistance was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hirschman AO. ‘Exit, voice, and loyalty’: further reflections and a survey of recent contributions. Social Sci Information. 1974;13(1):7–26. doi:10.1177/053901847401300101
2. Victoor A, Delnoij DM, Friele RD, et al. Determinants of patient choice of healthcare providers: a scoping review. BMC Health Serv Res. 2012;12(1):272. doi:10.1186/1472-6963-12-272
3. Yahanda AT, Lafaro KJ, Spolverato G, et al. A Systematic Review of the Factors that Patients Use to Choose their Surgeon. World J Surg. 2016;40(1):45–55. doi:10.1007/s00268-015-3246-7
4. Ejaz A, Spolverato G, Bridges JF, et al. Choosing a Cancer Surgeon: analyzing Factors in Patient Decision Making Using a Best–Worst Scaling Methodology. Ann Surg Oncol. 2014;21(12):3732–3738. doi:10.1245/s10434-014-3819-y
5. NSS 75th round. Household Social Consumption on Education in India. June 2018.
6. Milind D. Socio-economic inequality and its effect on healthcare delivery in India: inequality and healthcare. Electronic J Sociol. 2004;11:25.
7. Godlee F. Put patients first and give the money back. BMJ. 2015;h5489. doi:10.1136/bmj.h5489
8. Wolinsky FD, Steiber SR. Salient issues in choosing a new doctor. Soc Sci Med. 1982;16(7):759–767. doi:10.1016/0277-9536(82)90229-5
9. About – NUDM. Available from: https://nudm.mohua.gov.in/about/.
10. Carty, M.J, Duclos A, Gu X, EleleN, Orgill D. Patient satisfaction and surgeon experience: a follow-up to the reduction mammaplasty learning curve study. Eplasty. 2012.
11. Oikelome F, Healy G. Gender, Migration and Place of Qualification of Doctors in the UK: perceptions of Inequality, Morale and Career Aspiration. J Ethn Migr Stud. 2013;39(4):557–577. doi:10.1080/1369183X.2013.745233
12. Gould D. Using vignettes to collect data for nursing research studies: how valid are the findings? J Clin Nurs. 1996;5(4):207–212. doi:10.1111/j.1365-2702.1996.tb00253.x
13. Cavanagh GF, Fritzsche DJ. Using vignettes in business ethics research. 1985. eweb:56639.
14. Waljee JF, Hawley S, Alderman AK, et al. Patient satisfaction with treatment of breast cancer: does surgeon specialization matter? J Clin Oncol. 2007;25(24):3694–3698. doi:10.1200/JCO.2007.10.9272
15. McGlone TA, Butler ES, McGlone VL. Factors Influencing Consumers’ Selection of a Primary Care Physician. Health Mark Q. 2002;19(3):21–37. doi:10.1300/J026v19n03_03
16. Wun YT, Lam TP, Lam KF, et al. How do patients choose their doctors for primary care in a free market? J Eval Clin Pract. 2010;16(6):1215–1220. doi:10.1111/j.1365-2753.2009.01297.x
17. Abghari MS, Takemoto R, Sadiq A, et al. Patient Perceptions and Preferences when Choosing an Orthopaedic Surgeon. Iowa Orthop J. 2014;34:204.
18. Matza LS, Stewart KD, Lloyd AJ, et al. Vignette-Based Utilities: usefulness, Limitations, and Methodological Recommendations. Value Health. 2021;24(6):812–821. doi:10.1016/j.jval.2020.12.017
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.