Back to Journals » Pragmatic and Observational Research » Volume 11
CPAP Therapeutic Options for Obstructive Sleep Apnea
Authors Hooper RG
Received 17 April 2020
Accepted for publication 12 June 2020
Published 13 July 2020 Volume 2020:11 Pages 67—76
DOI https://doi.org/10.2147/POR.S258632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Robert G Hooper
Center for Sleep Medicine, Mayo Clinic, Phoenix, Arizona, USA
Correspondence: Robert G Hooper P.O. Box 4100, Scottsdale, Arizona 85261-4100, USA
Tel +1-480-342-1019
Fax +1-480-342-1012
Email [email protected]
Introduction: There are many options available to patients who are placed on constant positive airway pressure (CPAP) for obstructive sleep apnea. Despite the success of CPAP in correcting apnea, a significant number of patients have difficulty with the therapy. A large number of those patients who have difficulty stop therapy and are often labeled as “CPAP Failure”. Non-sleep specialists may view CPAP therapy as a singular course of treatment, but there are many ways CPAP may be ordered for a patient. Each patient experiences a unique set of options that constitute a unique order set.
Methods: In order to demonstrate the magnitude of the possible options, estimates of the number of unique order sets were calculated. The author chose individual order options and the number of selections possible within each option. The calculated sets included a “Generous, Limited and Minimal” number of selections for each option. Calculations were done separately for standard CPAP and for auto-adjusting CPAP. Additional calculations were performed using the number of commercially available masks in the United States.
Results: The maximum number of unique order sets was seen using a standard CPAP combined with commercially available masks: 49,152 unique order sets. The fewest number of unique order sets were seen with the auto-adjusting CPAP and the “Minimal” selections: 288 unique order sets.
Discussion: There are a large number of unique CPAP orders that a patient may experience. CPAP treatment is not a singular or simple therapy. When evaluating obstructive sleep apnea patients with histories of CPAP failure or prior difficulty with CPAP, paying close attention to the patient’s treatment experiences may help explain a significant number of those patients’ CPAP therapy problems.
Keywords: obstructive apnea, apnea treatment failure, CPAP, CPAP failure, CPAP orders, CPAP compliance
Introduction
Constant Positive Airway Pressure (CPAP) is considered the most effective therapy for moderate to severe obstructive sleep apnea (OSA).1–4 It is widely prescribed and used. Although CPAP is the most effective therapy, clinicians are often faced with patients who experience difficulties or have stopped therapy for some reason. The duration of nightly use, even among regular users, is disappointing. CPAP intolerance and CPAP failure are terms clinicians hear frequently and may use themselves. What exactly is “CPAP” therapy?
CPAP therapy involves sleeping while breathing air that is at mildly increased pressures over the ambient atmospheric pressure. As the name implies, the air pressure is maintained at a constant level on a breath-to-breath basis.5–7 This simple concept remains the basis for CPAP therapy. However, technologic innovations over the last 35 years have added optional pressure modifications when CPAP is prescribed. These include ramping up of pressure at treatment onset, pressure drops on exhalation and machine selected therapeutic pressures (auto adjusting). Additional types of pressure interactions, interfaces or modes have been developed and are in common use in the United States (USA). Examples of these positive airway pressure (PAP) therapies include bi-level pressure machines (a different set pressure for inspiration and expiration), pressure support machines (a set expiratory pressure with a machine selected variable inspiratory pressure designed to achieve appropriate tidal volumes) and others. Furthermore, each of these machine types is available in auto-adjusting formats. Technological advancements lead to more considerations when selecting therapy for a patient. The indications for these technologies continue to evolve, but the majority of newly diagnosed OSA treated with positive airway pressure therapy will be initially placed on CPAP.
CPAP is often considered as a single modality by those who are not familiar with the field or by patients being treated for OSA. CPAP therapy represents a wide spectrum of possible options when ordered for an individual patient. The purpose of this report is to present calculated estimates of the number of unique order options available to a provider when selecting CPAP therapy for a patient. These calculations demonstrate the variability and complexity of ordering just the CPAP form of positive airway pressure. More advanced forms of pressure therapies will have their own sets of unique order options.
These calculations demonstrate that CPAP is not a single or simple therapy. The calculations demonstrate a wide range of results that depend upon the arbitrary choices made of which and how many options to include in a single order. However, even a minimal number of included options results in a large number of potential patient experiences. The methods section describes what options were chosen to include in these calculations.
Methods and Assumptions
In determining estimates of possible order options, CPAP therapy and auto-adjusting CPAP therapy were calculated independently, as there are major differences in the approach to ordering the pressure settings for those two types of machines. For each machine type, the components of a typical order need to be addressed to assess the available number of order options.
A typical order in the USA will include machine type, pressure setting(s), the use of an expiratory pressure drop, pressure ramping, mask, mask sizing, and humidifier settings and usage. For these calculations, the number of possible selections for each of these variables was selected for each machine type. Three sets of selections for each variable were determined. First is a ‘generous’ set of option choices. The second set is a reduced or “limited” set of options that would represent more closely those that a typical clinician might routinely use. The last set of numbers would represent a “minimal” number of options. The results of the calculation for each set of option choices – generous, limited and minimal – were calculated for both standard and auto-adjusting CPAP. All option choices were made by the author and are arbitrary.
The Mayo Clinic Institutional Review Board (IRB) acknowledged this activity and that it did not require IRB review. No patients or patient data was utilized in this study. The author knows no ethical conflicts.
The results of the calculations are presented in four groups. One based upon using a standard CPAP machine and a second based upon using an auto-adjusting CPAP machine with the ordering options for each as described above. A third and fourth sets. of calculations, one for each machine type, are presented with a change in the numbers of mask options used for calculating results. For those last two sets of calculations, the mask options are based upon the number of masks available in December 2019 in the USA from the three largest manufacturers of CPAP masks.
Selection of Standard CPAP Machine Order Options
Therapeutic Pressures
On standard CPAP machines, a single therapeutic pressure is selected to control the patient’s OSA. Available pressures depend upon the manufacturer of the equipment. The lowest setting is at 4 cm H2O and the higher settings may range from 20 to 30 cm H2O. The pressure is selected and ordered by the provider. For these calculations, an available pressure range of 4 to 20 was used. Sixteen selection options were used in the generous set. Most clinicians will utilize fewer selections. For the limited estimate, four options were considered in the calculations, while only 2 options were used for the minimal category.
Relief of Pressure on Expirations
This setting is available on most manufacturers’ CPAP machines. The settings briefly lower the pressure on exhalation to provide a more normal feel to breathing on positive airway pressure. The setting can be turned off or set for a drop of 1, 2 or 3 cm H2O. Four selection options are available and were used for the generous calculations. For the limited and minimal estimates, two options (used or not used) were employed in the calculations.
Mask Types
Masks were considered to be of three major types (nasal pillow, over the nose nasals, and full face). Three selection options are available. For generous, limited and minimal estimates, three options were used in the calculations.
Mask Designs or Models
Multiple manufacturers provide masks for the CPAP market. There are many masks available. For these calculations, a number of four different designs were considered to be available within each mask type. Four selection options were used for the generous calculations. For the limited and minimal estimates, two options were used in the calculations.
Mask Size
Masks come in multiple sizes. In some situations, the headgear to hold mask in place is available in different sizes. For the calculations, an assumption was made that each mask was available in three sizes. Three selection options are available. For the generous, limited, minimal and commercially available mask estimates, three options were used in the calculations.
Humidification
Most CPAP machines have available humidification systems with some designs having the humidifier built into the CPAP machine. Humidifier systems can have multiple settings and the type of settings available vary between machines and manufacturers. For these calculations, the humidification options were simplified to “off” and “on”. Two selection options were used for the generous, limited, minimal and commercially available mask options calculations.
Pressure Ramping
A feature that permits the user to experience a gradual increase in pressure over a fixed period of time till it reaches the prescribed treatment pressure. It can start at a preselected pressure ending at the treatment pressure. It increases over a selected period of time (usually 5 to 30 mins). For these calculations, the ramp options were considered to be two, used or not used. Two selection options were used for the generous, limited, minimal and commercially available mask options calculations.
Selection of Auto-Adjusting CPAP Machine Order Options
Therapeutic Pressure
On auto-adjusting CPAP machines, the machine can be set to be used as a standard CPAP machine or it can be used in the auto mode. When used as an auto-adjusting machine, it will gradually change the therapeutic pressure to control apnea events that it identifies. Upper (maximum) and lower (minimum) pressure levels are set and the machines will operate within those limitations.
These machines have similar pressure capabilities as standard CPAP machines and for these calculations, a range of 4 minimum and 20 maximum for the machines was assumed. A large number of pressure ranges can be selected. However, for these calculations four pressure ranges were chosen; 1) full, 2) large – difference between minimum and maximum pressure of >10 cm of H20, 3) medium – difference between minimum and maximum pressure of 6–10 cm H2O and 4) small – difference between minimum and maximum pressure of <-6 cm H2O. The full range would be minimum 4 and maximum 20 for one option. The assumptions of the number of possible options for a large range – 2 options, medium range – 3 options, and small range – 4 options.
Total selection options chosen above and used in the generous calculations were 10 options. For the limited calculations, four options were used. For the minimal calculations, two options were used.
Additional Order Options for Auto-Adjusting CPAP
Auto-adjusting CPAP orders will have all the options described above for standard CPAP machines. The orders will differ only in the selection of therapeutic pressures.
Positive Airway Pressure Masks Commercially Available in USA
The web sites of Fisher/Paykel, ResMed and Phillips Respironics were reviewed on December 17, 2019.8–10 The types and designs of adult CPAP masks offered for sale were reviewed and are presented in Table 1–3. The masks available were then used to recalculate the potential order options.
 |
Table 1 Fisher Paykel Mask Options Available (United States – December 2019) |
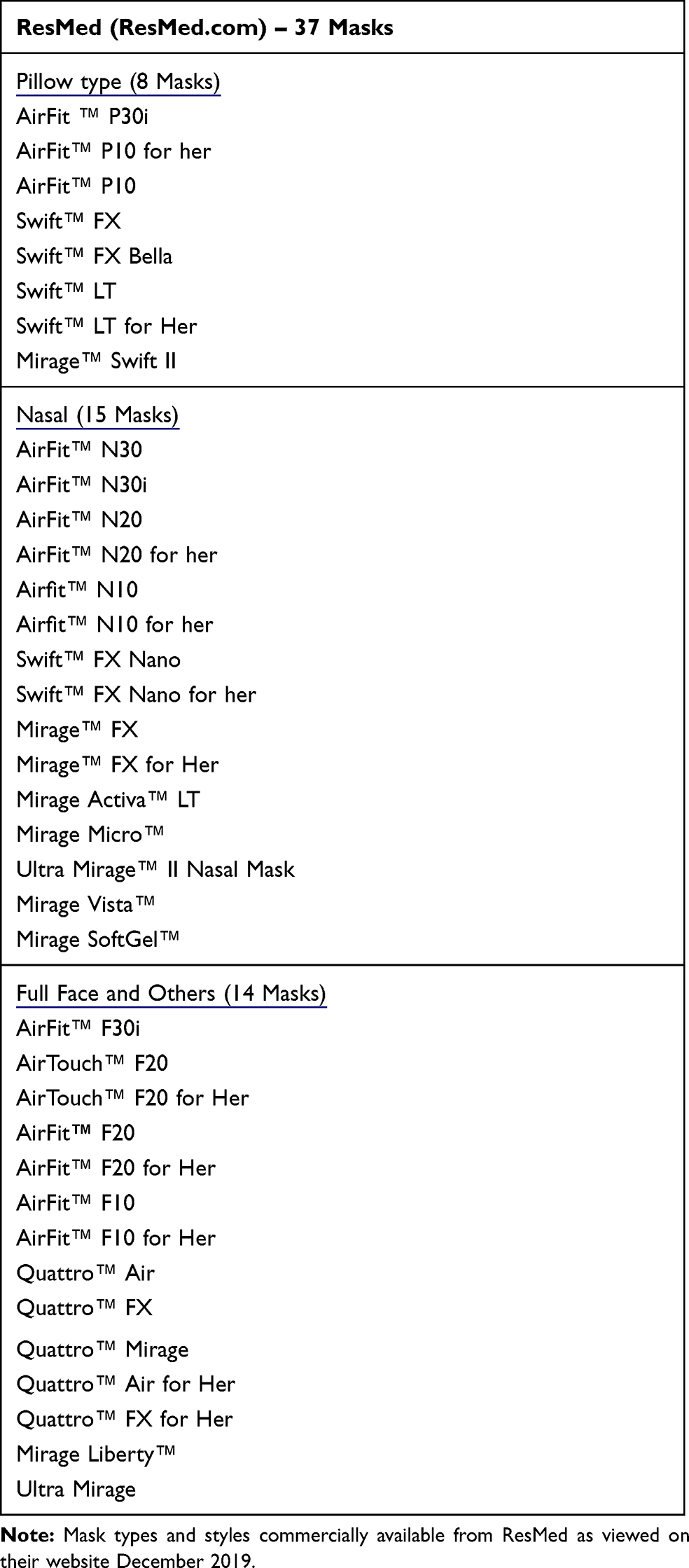 |
Table 2 ResMed Mask Options Available (United States – December 2019) |
 |
Table 3 Respironics Mask Options Available (United States – December 2019) |
A review of the web sites showed that in total, these manufacturers offered 24 full face masks, 27 nasal masks and 15 pillow type masks. For calculations using the commercially available masks, the total number of 66 masks was substituted for the types and designs numbers used for the other calculations.
Results
For standard CPAP orders, the unique order options ranged from a low of 288 unique options with the minimal assumptions and a high of 9,216 with the generous assumptions (Table 4). The calculations for auto-adjusting CPAP showed a low of 288 and a high of 5,760 (Table 5).
 |
Table 4 Ordering Options for Standard CPAP Machines |
 |
Table 5 Ordering Options for Auto-Adjusting CPAP Machines |
The number of options increased dramatically when the calculations were repeated substituting the number of commercially available CPAP masks (66 – Table 1–3) in place of the style and design mask assumptions used above. The high was 49,152 with standard CPAP (Table 6) and the low was 3027 with both standard and auto-adjusting CPAP (Tables 6 and 7).
 |
Table 6 Ordering Options with Commercially Available CPAP Mask and Standard CPAP |
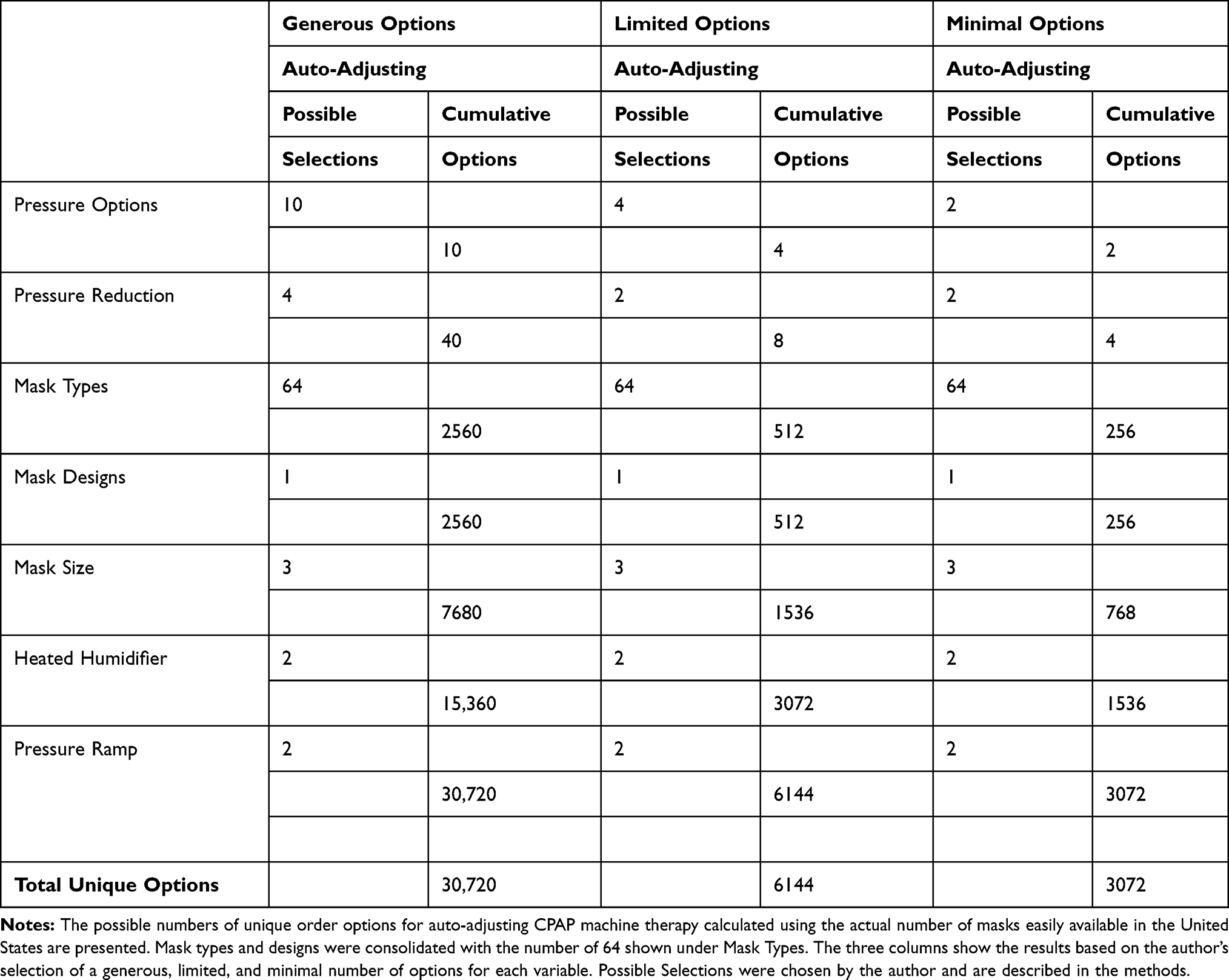 |
Table 7 Ordering Options With Commercially Available Cpap Mask And Auto-Adjusting CPAP |
Discussion
It will not surprise sleep clinicians that many options exist for ordering CPAP. The calculations based upon the above assumptions demonstrate that even with a conservative selection of options there is a significant number of independent unique orders. As a result, there are many ways that a patient may experience CPAP. Certainly, sleep clinicians have standard practices that limit how they choose CPAP orders and those orders are limited in type and number. The numbers calculated here serve to demonstrate that CPAP is far from a simple or singular therapy, but rather one that is unique for the individual patient.
The physician may or may not make all the decisions regarding the options used in these calculations. Midlevel providers, sleep technicians and respiratory therapists may help the patient with mask selection and other options. The patient’s input to the decisions also plays a role in the ultimate set of unique orders that defines the therapy that the patient will experience. The purpose of this report is not who chooses the options or how they are chosen. The point of these calculations is to demonstrate the large set of unique options that the patient may experience when CPAP therapy is initiated. It is that unique situation which needs to be considered if trouble with therapy occurs or has previously been encountered. These calculations demonstrate that because of the large set of possible unique orders, many technical factors need to be reviewed when trouble with CPAP therapy is encountered.
CPAP pressure orders in the United States traditionally were directed by testing performed in sleep centers while on CPAP therapy. During the period of time when only standard CPAP machines were available, testing was routinely performed to select the pressure needed. For approximately a quarter of a century after the introduction of positive airway pressure, the process remained the same. The process, by its nature, limited the number of options by having therapeutic pressures and an appropriate mask identified at the time of testing. Clinicians recognize that even with the guidance of testing, pressure settings often needed adjustment and initial mask selections were not the best. A large number of patients did well, but a significant number did not.4,11,12
Two factors changed the approach to the diagnosis of OSA and the ordering of CPAP therapy in the US and both occurred at approximately the same time (2011 to 2014). Home sleep apnea testing was approved by government and by commercial insurance payers to be a covered item for the diagnosis and as proof of the diagnosis of OSA so that the therapy would also be a covered item. The change led the commercial insurance payers to move rather quickly to restrict payments for diagnostic sleep center testing. Auto-adjusting CPAP machines had been developed and were commercially available several years earlier. Work demonstrated that auto-adjusting machines could be utilized in place of facility-based CPAP polysomnograms (PSG) to determine the best therapeutic pressures.4,13–16 The payers rapidly began to require the use of auto-adjusting equipment as the initial step for treatment with PAP therapy and to deny payments for sleep center-based CPAP testing. Fortunately, during the same time period, a significant drop in the cost of auto-adjusting CPAP equipment occurred. The result of the insurance restrictions has been that most patients who need evaluation for OSA are limited to home sleep apnea testing and the ordering of auto-adjusting CPAP for titration by the machine. The benefit of knowing an appropriate pressure and mask based on sleep testing with CPAP has been taken away from the ordering physician. Interestingly, the reported compliance achieved is the same as it was for those who were managed after CPAP PSGs.4,15,17 Nor do other outcomes seem to differ.4,18
The lack of U.S. insurance payment for CPAP PSGs for pressure titrations has led to modifications in the practice of sleep medicine. Empiric selection of initial pressure or pressure range is now standard practice for most patients depending on their healthcare insurance.
The changes in how positive airway pressure therapy are reimbursed by insurance in the US have led to modifications in the practice of sleep medicine. The cost of diagnosis and treatment is reduced by the use of home-based testing and treatment with auto-adjusting CPAP units.15 These calculations indicate that changing to auto-adjusting CPAP machines will reduce the possible number of different unique orders that are placed. However, the number of unique order options remains large. It has been argued that fewer issues develop on the auto-adjusting technology, but it is not known if that is or is not true. Neverthe less, there is a large number of patients who will not do well on the initially ordered therapy with auto-adjusting technology.4,18
Probably the most common problems encountered with patients on CPAP are with the masks employed. When CPAP PSGs were common, mask selection at the time of the test helped reduce the number of mask problems encountered. Now, mask fitting is more of a problem. The number of masks available commercially is amazingly large. A single manufacturer, ResMed, lists a total of 37 masks offered (14 full face masks, 15 nasal masks, and 8 nasal pillow masks). All masks come in different sizes and some have headgears that differ in size. The masks available from three manufacturers are listed in Table 1–3.
Selection of a mask is difficult. Best results are obtained when a patient is able to sleep with the mask and be able to assess its comfort and seal (no inappropriate air leakage). In the US, government regulations limit these items to single patient use. As a result, it is hard for patients to try on multiple masks, as providers are not legally able to reuse a mask after it has been tried on. The single-use-only requirement financially limits the number of masks available for fitting and trials. There is no easy solution in view for this problem.
The choices for mask selection options used for the calculations are conservative. The wide number of types, designs and sizes make it difficult at best to determine an appropriate number of choices to use. The large number of commercially available masks serves to demonstrate the unique features of each CPAP order and the problems faced with assessing issues when patients have problems with CPAP or report prior failure of CPAP therapy.
Technical problems with CPAP therapy also include the options that are often considered comfort features. These include humidity setting, expiratory pressure release and ramp features. These features along with the mask and pressure selections define the unique order the individual patient experiences. When a patient experiences problems with their therapy, all of these technical factors need to be reviewed. Identifying problems that patients experience with their CPAP therapy represents a continuing clinical challenge. Patients become frustrated and adjustments to therapy can be difficult to implement.
The selection of options and the choice of the number used for calculations were the author’s personal selections. Other curious clinicians might choose differently. By choosing a generous, limited and minimum set of order options, it was hoped to demonstrate the possible and the commonly used range of options. It may be that even the set of minimum selections chosen are considered too many by some. Further limiting the number or options for each detail will reduce the results accordingly. Some readers may not consider factors such as humidity, ramp or pressure release worthy of inclusion. Reducing the possible options to a minimum still leaves a significant number of unique order sets.
Experienced sleep physicians and providers initiating CPAP therapy limit the number of ordering options they use on a regular basis. The author uses only five or six ordering options excluding mask choices. However, the evaluation of a patient with a history of CPAP failure requires consideration that other providers may employ different therapeutic programs.
This report is not a call for reducing the available options for CPAP therapy. The large number of pressure forms, mask options and comfort features available enrich the ability of the clinician to provide a therapy that is comfortable and successful for the patient. This report’s purpose is to bring to attention that an individual’s CPAP treatment can take many forms depending on the options selected for the patient. In assessing problems with ongoing therapy or histories of CPAP failure, attention to the patient’s prior CPAP experience is important.
Conclusion
Therapy with CPAP represents a wide range of unique order options. These calculations, based on real but arbitrarily selected options, demonstrate one fact. CPAP therapy is not a simple or singular therapy. CPAP therapy includes a large number of unique order options that a patient may experience. Patients benefit from a wide variety of available options. Correcting obstructive apnea requires their utilization. Many modifications can be made within those options to improve compliance and acceptance.
Patients who experience difficulty with using CPAP may do so because of many reasons.11,12 In addition to the unique technical options each patient experiences, other reasons include: a lack of, or ineffective, obstructive apnea control; a lack of improvement in the patient’s symptoms; an incorrect apnea diagnosis; the presence of an additional (second or third) sleep disorder; medical conditions that make using CPAP difficult; anxiety, claustrophobia, psychological or psychiatric problems; a lack of understanding of the reasons for the CPAP treatment; problems with the patient’s healthcare delivery system; personal and family perceptions and attitudes; and personal choice. Knowing the unique technical factors an individual experiences will explain many patient problems.
Acknowledgments
The author expresses his gratitude to Skye A. Buckner-Petty MPH, Biostatistician, Division of Health Sciences Research, Mayo Clinic for his assistance and guidance of this project.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Marin JM, Agusti A, Villar I, et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA. 2012;307(20):2169–2176.
2. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053.
3. Campos-Rodriguez F, Pena-Grinan N, Reyes –nunez N, et al. Mortality in obstructive sleep apnea hypopnea patients treated with positive airway pressure. Chest. 2005;128(2):624–633.
4. Paul SP, Ayappa IA, Caplies SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American academy of sleep medicine systematic review, meta-analysis and GRADE assessment. J Clin Sleep Med. 2019;301.
5. Sullivan CE, Issa FG, Ferthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nose. Lancet. 1981;1(8225):862–865.
6. Jordan AS, McSharry DG, Malhotra A. Adult Obstructive sleep apnoea. Lancet. 2014;383(9918):736.
7. Qaseem A, Holty JE, Owens DK, Dallas P, Starkey M. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159(7):471.
8. https://www.fphcare.com/us/products/homecare-products/masks/.
9. https://www.resmed.com/en-us/sleep-apnea/cpap-parts-support/sleep-apnea-full-products-list/#mask.
10. https://www.usa.philips.com/healthcare/solutions/sleep.
11. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173–178.
12. Bakker JP, Weaver TE, Parthasarathy S, Alola MS. Adherence to CPAP: what should we be aiming for, and how can we get there? Chest. 2019;155(6):1272–1287.
13. Masa JF, Jimernez A, Duran J, et al. Alternative methods of titrating continuous positive airway pressure: a large multicenter study. Am J Respir Crit Care Med. 2004;170(11):1218.
14. Ayas NT, Patel SR, Malhotra A, et al. Auto-titrating versus standard continuous positive airway pressure for the treatment of obstructive sleep apnea: result of a meta-analysis. Sleep. 2004;27(2):249.
15. Planes C, D’Orthro MP, Foucher A, et al. Efficacy and cost of home-initiated auto-nCPAP versus conventional nCPAP. Sleep. 2003;26(2):156–160.
16. Hukins C. Comparative study of autotitrating and fixed –pressure CPAP in the home: a randomized, single-blind crossover trial. Sleep. 2004;27(8):1512–1517.
17. Vennelle M, White S, Riha RL, Mackay TW, Engleman HM, Douglas NJ. Randomized controlled trial of variable-pressure versus fixed-pressure continuous positive airway pressure (CPAP) treatment for patients with obstructive sleep apnea/hypopnea syndrome (OSAHS). Sleep. 2010;33(2):267.
18. Pepin JL, Tamisier R, Baguet JP, et al. Fixed-pressure CPAP versus auto-adjusting CPAP comparison of efficacy on blood pressure in obstructive sleep apnonea, a randomized clinical trial. Thorax. 2016;71(8):726–733.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.