")
Back to Journals » International Journal of Women's Health » Volume 15
COVID-19 Vaccine Uptake, Acceptance, and Reasons for Vaccine Hesitancy: A Cross-Sectional Study Among Pregnant Women in Trinidad, West Indies
Authors Khan S , Sohan K, Mohammed ZCM, Bachan V
Received 26 November 2022
Accepted for publication 22 February 2023
Published 28 February 2023 Volume 2023:15 Pages 343—354
DOI https://doi.org/10.2147/IJWH.S396884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Marleen van Gelder
Shane Khan,1 Karen Sohan,2 Zada CM Mohammed,3 Vishal Bachan4
1Department of Clinical Surgical Sciences, University of the West Indies, St. Augustine, Trinidad and Tobago; 2Diagnostic Mother and Baby (Private Sector), Chaguanas, Trinidad and Tobago; 3Office of the Directorate of Women’s Health, Ministry of Health, Port-of-Spain, Trinidad and Tobago; 4Department of Obstetrics and Gynaecology, San Fernando General Hospital, San Fernando, Trinidad and Tobago
Correspondence: Shane Khan, Department of Clinical Surgical Sciences, University of the West Indies, St. Augustine, Trinidad and Tobago, Tel +1 868 735 5162, Email [email protected]
Purpose: Pregnant women are at greater risk for severe COVID-19 disease and are a priority group for vaccination. Trinidad and Tobago (TTO) introduced COVID-19 vaccination for pregnancy in August 2021, however uptake is presumed to be low. The objective was to determine the COVID-19 vaccine acceptance and uptake rates among pregnant women in TTO and reasons for vaccine hesitancy.
Patients and Methods: This was a cross-sectional study on 448 pregnant women conducted at specialized antenatal clinics within the largest Regional Health Authority in TTO, and at one private institution from February 1 to May 6, 2022. Participants completed an adapted WHO questionnaire on reasons for COVID-19 vaccine hesitancy. Logistic regression was used to assess factors affecting vaccination decisions.
Results: The vaccine acceptance and uptake rates in pregnancy were 26.4% and 23.6%, respectively. The main reason for vaccine hesitancy was lack of research on the COVID-19 vaccine in pregnancy (70.2%), where 75.5% of women believed the vaccine would harm their babies and 71.2% believed there was not enough data. Women seeking care in the private sector (OR: 5.24, 95% CI: 1.41– 19.43) and who had comorbidities (OR: 3.72, 95% CI: 11.57– 8.83) were more likely to take the vaccine, while Venezuelan non-nationals (OR: 0.09, 95% CI: 0.01– 0.71) were less likely to take the vaccine. Older women (OR: 1.80, 95% CI: 1.12– 2.89), women with tertiary education (OR: 1.99, 95% CI: 1.25– 3.19), and women seeking care in the private sector (OR: 9.45, 95% CI: 4.36– 20.48) were more likely to accept the vaccine.
Conclusion: Lack of confidence in the vaccine was the main reason for hesitancy, which may reflect paucity of research, lack of knowledge or misinformation of the vaccine in pregnancy. This highlights the need for more targeted public education campaigns and promotion of the vaccine by health institutions. The knowledge, attitudes, and beliefs of pregnant women obtained from this study can guide the development of vaccination programs in pregnancy.
Keywords: COVID-19, vaccine, pregnancy, hesitancy, uptake, Trinidad
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Tampake has been published for this article.
Introduction
On March 11, 2021, the World Health Organization (WHO) officially declared the SARS-CoV-2 (COVID-19) infection a pandemic.1 Since then, there has been a fast-track to develop vaccines against COVID-19. As of September 2022, there are 47 approved vaccines rolled out in 201 countries, of which 11 have WHO Emergency Use Listing.2
WHO has designated pregnant women as a high priority-use group for vaccination because pregnant women with COVID-19 are at higher risk of developing severe disease,3 with increased risk of ICU admission and invasive ventilation, compared to non-pregnant women of reproductive age.4 Additionally, COVID-19 in pregnancy is also associated with an increased risk of preterm birth and neonates requiring neonatal intensive care.4
Trinidad and Tobago received its first doses of COVID-19 vaccines on March 30, 2021.5 Since then, four vaccines – BNT162b2 (Pfizer-BioNTech), ChAdOx1-S [recombinant] vaccine (Oxford/AstraZeneca), Janssen Ad26.COV2.S (Johnson and Johnson) and BIBP (Sinopharm) – have been offered. The Ministry of Health, Trinidad and Tobago (MoH) approved the use of the Pfizer vaccine in pregnant women during the second and third trimesters on 25th August 2021.
However, despite the global and national campaigns to promote vaccination, there has been a relatively low uptake rate among the Trinidad and Tobago population, with only around half of the population of Trinidad and Tobago has been fully vaccinated.6,7 Further, as there are no available data on vaccine coverage in pregnant women, it is presumed that the uptake rate is even lower in this vulnerable group.
This study therefore seeks to determine the uptake and acceptance rates of COVID-19 vaccines among pregnant women in Trinidad and Tobago as well as to identify reasons why pregnant women may be hesitant to take a COVID-19 vaccine. As far as we are aware, this is the first study reporting on reasons for COVID-19 vaccine hesitancy in pregnancy in the Caribbean.
Materials and Methods
Ethics Approval and Informed Consent
Ethical approval was obtained from both the University of the West Indies (UWI), St Augustine and the South-West Regional Health Authority (SWRHA) prior to commencement of the study.
Participants were informed about the purpose of the study in accordance with the Declaration of Helsinki. Written informed consent was then obtained from all participants, after which they were given a questionnaire to complete. The survey did not capture any patient identifiers and participants were free to omit any questions they were not comfortable answering. The data was stored on a password protected computer which was only accessible to the Principal Investigator.
Study Design and Sample Size
This cross-sectional study was conducted at the main secondary care antenatal clinic at the San Fernando General Hospital (SFGH) and four specialist-led antenatal clinics in the community under the purview of the SWRHA from February 1, 2022 to May 6, 2022. As a comparison, a second dataset was collected from a single private antenatal clinic in central Trinidad. A public participant is one who seeks care in the public health sector where health care is free at the point of service, while a private participant is one who self-funds their care. In Trinidad and Tobago, approximately 90% of deliveries occur in the public health sector and 10% occur in the private health sector.8
Convenience sampling was employed, where all patients attending these clinics for their regular antenatal appointments during the study period were offered the questionnaire and they chose whether to opt-in or opt-out. The questionnaire was administered by the nurse-in-charge of the clinics who had been briefed by the Principal Investigator.
As accurate figures of the number of pregnant women in the catchment area of the SWRHA were unavailable, the CDC estimate that pregnant women represent approximately 1% of the total population at a point in time9 was used to determine that there would be approximately 6000 pregnant women at the time of the study, given that the catchment population of the SWRHA is approximately 600 000. Therefore, assuming a population size of 6000, a margin of error of 5%, a sample proportion of 50% and a confidence level of 95%, the calculated sample size was 362 using the population proportion sample size calculation. The actual number of pregnant women who participated in the study was 448.
Survey Design and Outcome Ascertainment
The questionnaire that was used for this study was based on the survey tool developed by the WHO SAGE Working Group on Vaccine Hesitancy in 2015 to assess the nature and scale of vaccine hesitancy issues. The WHO tool was adapted to the local setting and for COVID-193,10 informed by a similar study undertaken by Goncu Ayhan et al.11 The adapted questionnaire was offered in the primary language of Trinidad and Tobago, Standard English, and a translated version in Spanish for the refugee population from nearby Venezuela.
Survey questions focused on demographics, medical comorbidities, perception of COVID-19 infection and risk of infection, barriers to vaccination, preferred source of medical information, vaccine acceptance, vaccine uptake, and reasons for unwillingness to receive the COVID-19 vaccine decision. Participants responded to a series of yes or no and Likert scale questions and multiple-choice to collect quantitative and qualitative data on vaccine perceptions. A copy of the study questionnaire is provided in the Supplementary Data section.
The outcome variables were COVID-19 vaccine uptake and acceptance during pregnancy. To assess vaccine uptake, respondents were asked whether they had received any doses of COVID19 vaccine while pregnant. Respondents who indicated that they received at least two doses prior to pregnancy, ie, were fully vaccinated before pregnancy, were not considered when determining vaccine uptake in pregnancy. To assess vaccine acceptance, respondents were asked whether they would be willing to take the COVID-19 vaccine in pregnancy. Respondents who indicated that they received three doses of a COVID-19 vaccine prior to pregnancy were not considered when determining vaccine acceptance.
Statistical Analysis
Baseline characteristics of participants and survey responses were presented as counts and percentages for categorical variables, while continuous variables were presented as mean and standard deviation. Categorical and continuous data were compared by Pearson’s chi-squared and ANOVA, respectively. As a sub-group analysis, responses of pregnant women who sought care in the public health system were compared to those who sought care in the private health system. Univariate logistic regression was used to assess potential factors associated with vaccine acceptance and uptake. Odds ratios (OR) and 95% confidence intervals (CI) were calculated, with statistical significance set at p < 0.05, and were used to describe the odds of COVID-19 vaccine acceptance and uptake for all variables. Statistical analyses were completed using Stata 13 (College Station, TX).
Results
In total, 448 pregnant women participated in the study. As participants were not required to answer every question, there was missing data. Generally missing data for the demographic variables was around 5%, except for occupation (10.3%), gestational age (39.7%), trimester (39.7%), children in the household (24.3%), and elderly in the household (31.7%). There were also high proportions of missing data for questions on the perception of vaccine safety (10.9–12.7%), sources of information (17.0%), wait times (33.9%), trimester for taking the vaccine (36.8%), and vaccination during breastfeeding (19.4%). Missing data for the questions used to determine vaccine uptake and vaccine acceptance ranged from 9 0.2–14.5%.
The baseline characteristics of the participants are shown in Table 1. Generally, the majority of participants were nationals accessing care in the public health-care system, had completed secondary or tertiary education, were in their 3rd trimester of pregnancy, and almost one quarter of women surveyed had a comorbidity, the most common being diabetes. Additionally, almost one quarter of pregnant women surveyed reported that they were previously infected or diagnosed with COVID-19.
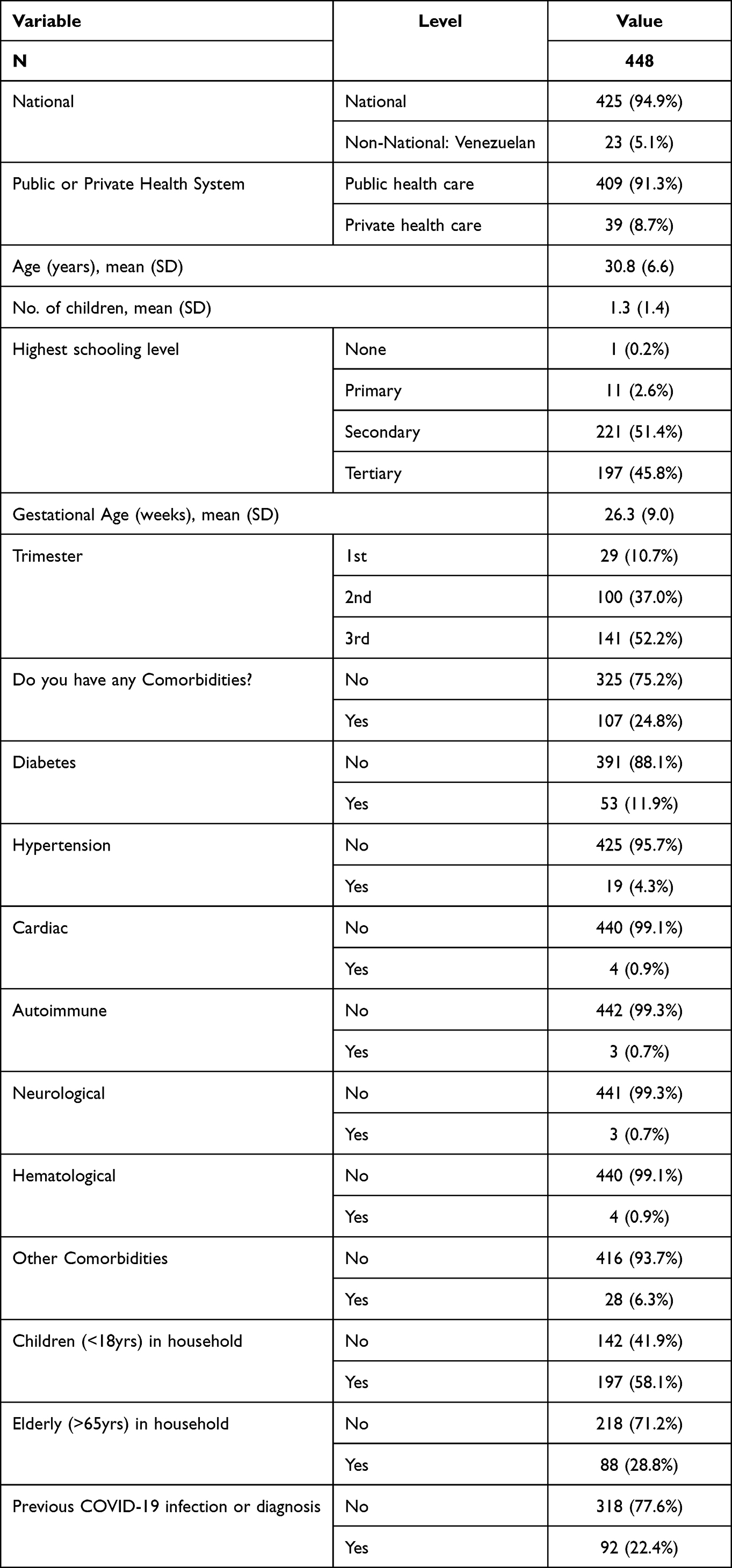 |
Table 1 Baseline Characteristics of the Study Population |
Table 2 shows participants’ response to receiving the COVID-19 vaccine and willingness to receive the vaccine. Of the 448 participants, 404 responded to the question on receiving the COVID-19 vaccine prior to pregnancy. Of those, 115 were considered fully vaccinated, giving a pre-pregnancy COVID-19 fully vaccinated uptake rate of 28.5%. Having removed the women who were fully vaccinated prior to pregnancy, the remaining 296 participants who responded to the question of how many COVID-19 vaccine doses they received in pregnancy, 70 reported receiving at least one dose of a COVID-19 vaccine in pregnancy, resulting in a 23.6% vaccine uptake in pregnancy. Of the 379 participants who responded to the survey question on willingness to take the COVID-19 vaccine in pregnancy and had not received three doses of the vaccine, 100 reported they were willing to take the vaccine in pregnancy, resulting in a 26.4% vaccine acceptance in pregnancy.
 |
Table 2 Vaccine Uptake Prior to and in Pregnancy and Vaccine Acceptance in Pregnancy |
Table 3 shows the reasons for unwillingness to accept the vaccine, amongst women who indicated that they were not willing to accept the vaccine in pregnancy. The most common reason given for not being willing to take the vaccine was that there was not enough research on the COVID-19 vaccine in pregnancy (70.2%), followed by having received the vaccine prior to pregnancy (24.5%). Only a few women indicated that they believed they were unlikely to be affected by COVID-19 (4.2%) and that it was difficult to access the vaccine (1.1%). When looking at reasons for vaccine hesitancy, the three most common reasons given were that the women believed that the vaccine would harm their babies (75.5%), there was not enough data on the COVID-19 vaccine in pregnancy (71.2%), and the vaccine would harm their bodies (61.9%).
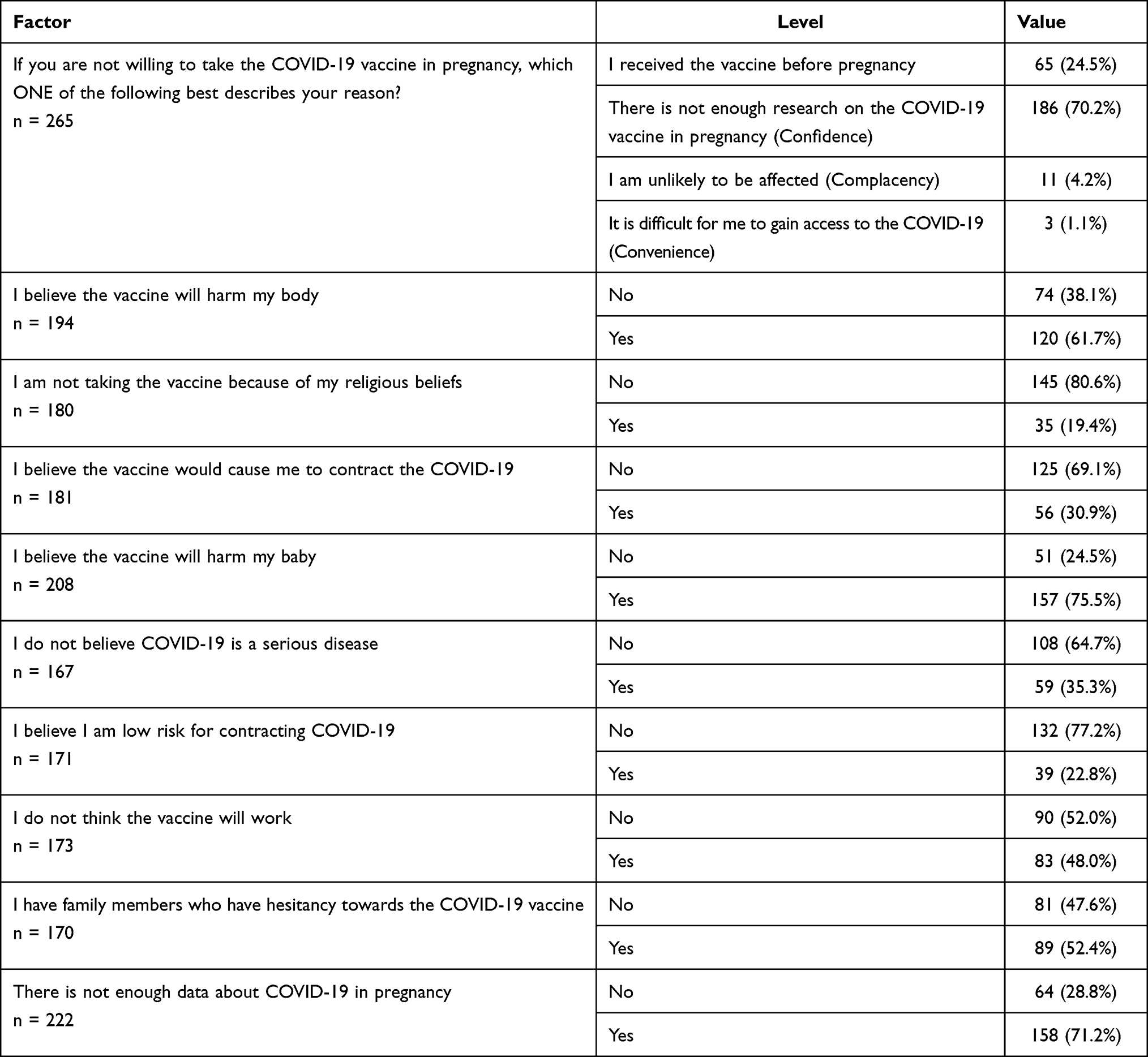 |
Table 3 Reasons for COVID-19 Vaccine Hesitancy in Pregnancy Amongst Women Who Indicated That They Were Not Willing to Take the Vaccine in Pregnancy |
Though 1.1% of women who were unwilling to accept the vaccine indicated that the vaccine was difficult to access, Table 4 shows that amongst all participants, the general opinion was that the vaccine was in fact easy or very easy to access (85.4%) and that the process of being immunized was generally a positive experience (64.9%).
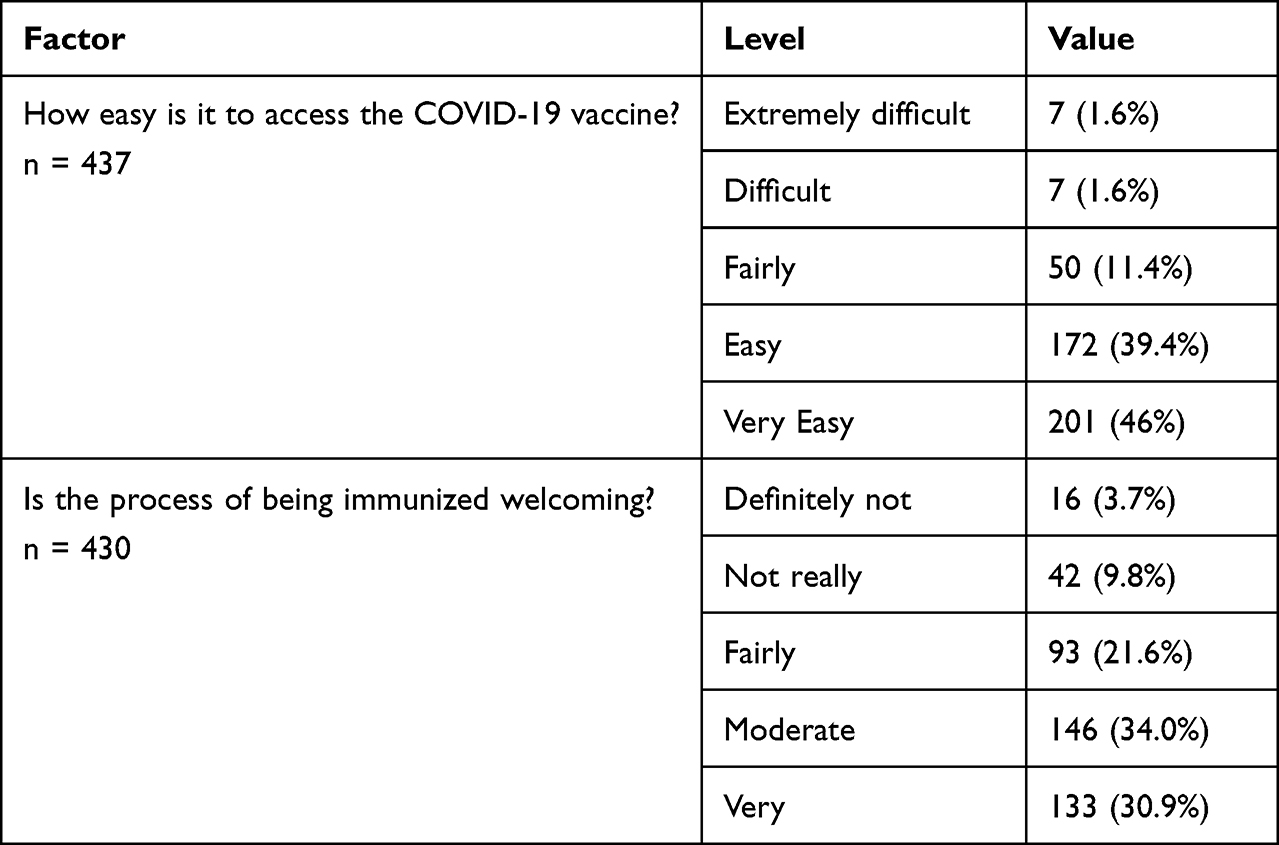 |
Table 4 Responses to Access and Process of the COVID-19 Vaccine |
Participants’ knowledge and awareness of the COVID-19 vaccine in pregnancy were also examined as shown in Table 5. While the majority of pregnant women (78.3%) were aware that the COVID-19 vaccines are recommended in pregnancy by both national and international authorities, most women (64.9%) were unaware that pregnancy increased their risk of more severe outcomes if infected with COVID-19 and that most adverse outcomes in pregnancy were in unvaccinated women (62.7%). Most women (46.9%) indicated that they felt comfortable receiving the vaccine in the 3rd trimester.
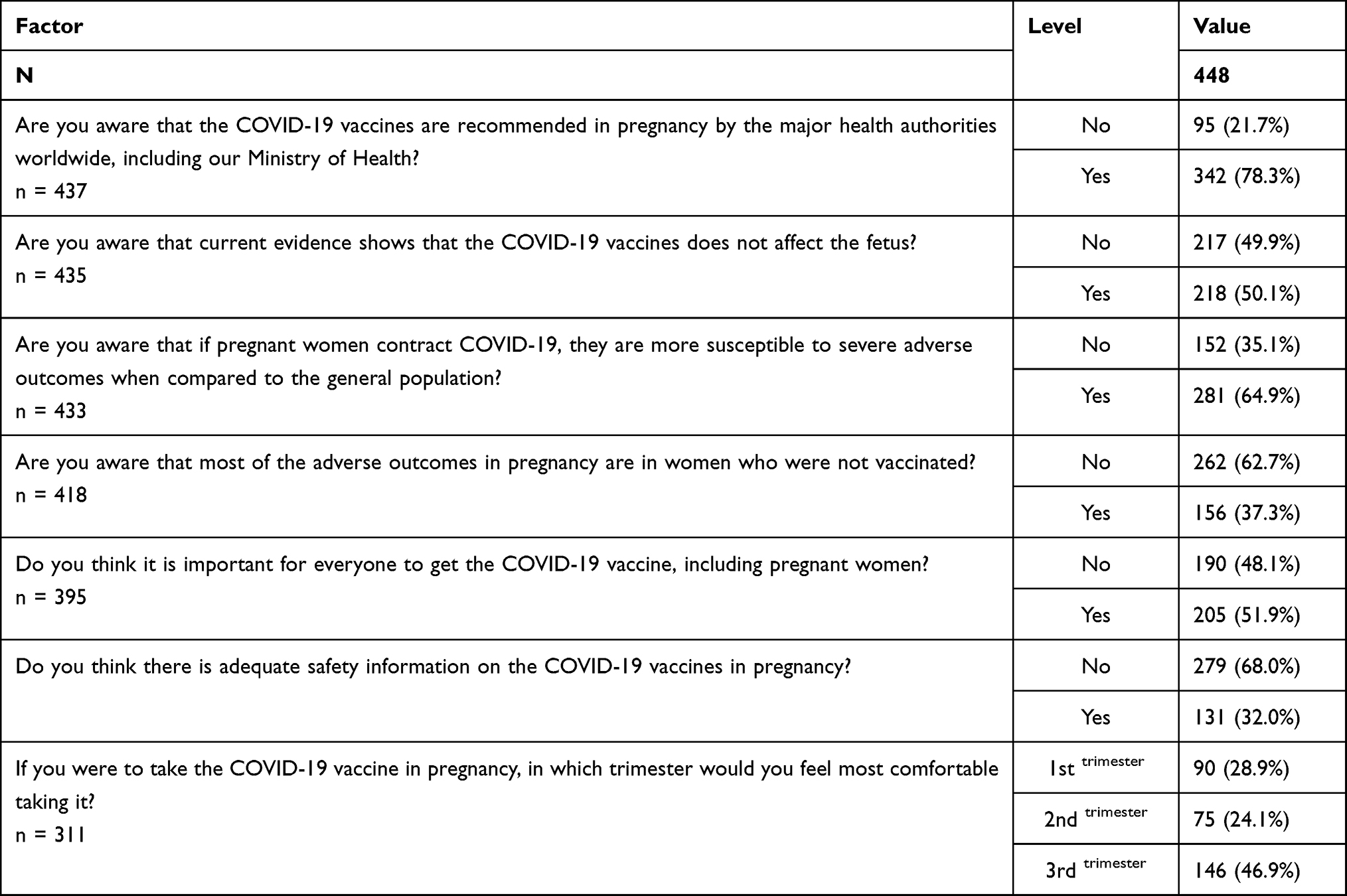 |
Table 5 Participants’ Knowledge and Awareness on the COVID-19 Vaccine |
Table 6 shows participants’ responses to questions related to their trust of the health system and newer vaccine technology. Generally, participants trusted the information emanating from health systems – health care professionals (61.6%) and health organizations (41.7%) – more than information from social media (3.0%) and pharmaceutical companies (1.6%) were the most trusted sources for information on the COVID-19 vaccine in pregnancy. As it pertains to newer vaccine technologies, the majority of participants (61.7%) trusted the older tetanus and influenza vaccines more than newer vaccines, with 67.8% of participants indicating that they did not believe the new COVID-19 vaccines were as safe as older vaccines. When asked if they would be willing to take the vaccine after delivery, less than half of participants (47.6%) were willing to take the vaccine while breastfeeding.
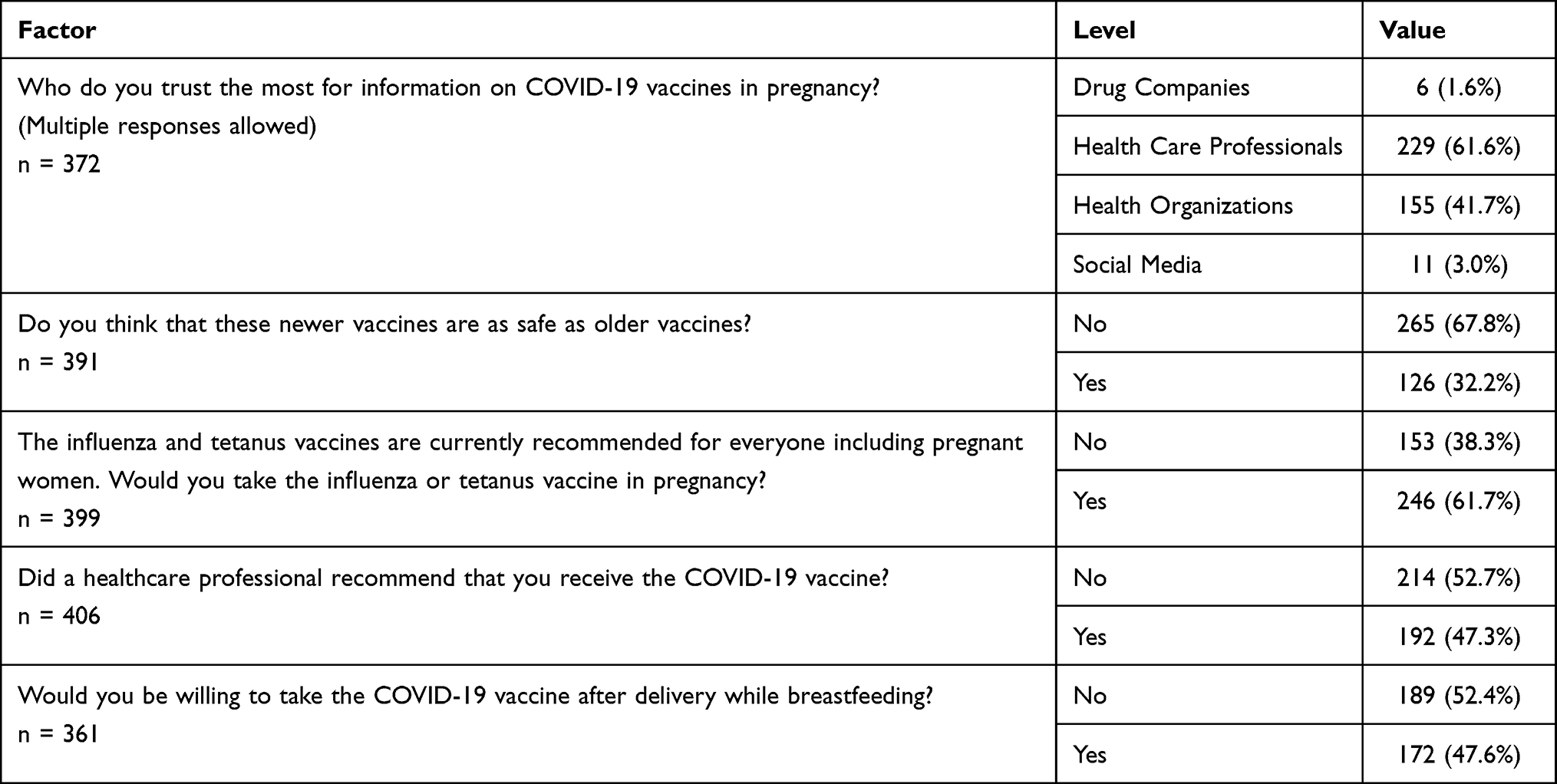 |
Table 6 Trust of the Participants in the Health Care System and the New COVID-19 Vaccine |
Table 7 shows the results of univariate logistic regression analysis to determine predictors of vaccine uptake and vaccine acceptance. When looking at uptake, persons seeking care in the private health sector had 5.24 (95% CI: 1.41–19.43) times the odds of receiving the COVID-19 vaccine in pregnancy, compared to women seeking care in the public sector and women who had a comorbidity had 3.72 (95% CI: 1.57–8.83) times the odds of receiving the vaccine in pregnancy compared to women who did not have a comorbidity. Conversely, the Venezuelan non-nationals had 0.09 times the odds of taking the vaccine, compared to non-nationals. When looking at vaccine acceptance, older women were more likely to accept the vaccine, with women with advanced maternal age pregnancies (≥35 years) having 1.80 (95% CI: 1.12–2.89) times the odds of accepting the vaccine compared to women less than 35 years, and women ages 30–39 years having 2.5 (95% CI: 1.44–4.36) times the odds of accepting the pregnancy compared to women 20–29 years old. Women with tertiary education had 1.99 (95% CI: 1.25–3.19) times the odds of accepting the vaccine compared to women with secondary level education or lower, and women who sought care in the private health sector had 9.45 (95% CI: 4.36–20.48) times the odds of accepting the vaccine compared to women who sought care in the public health sector.
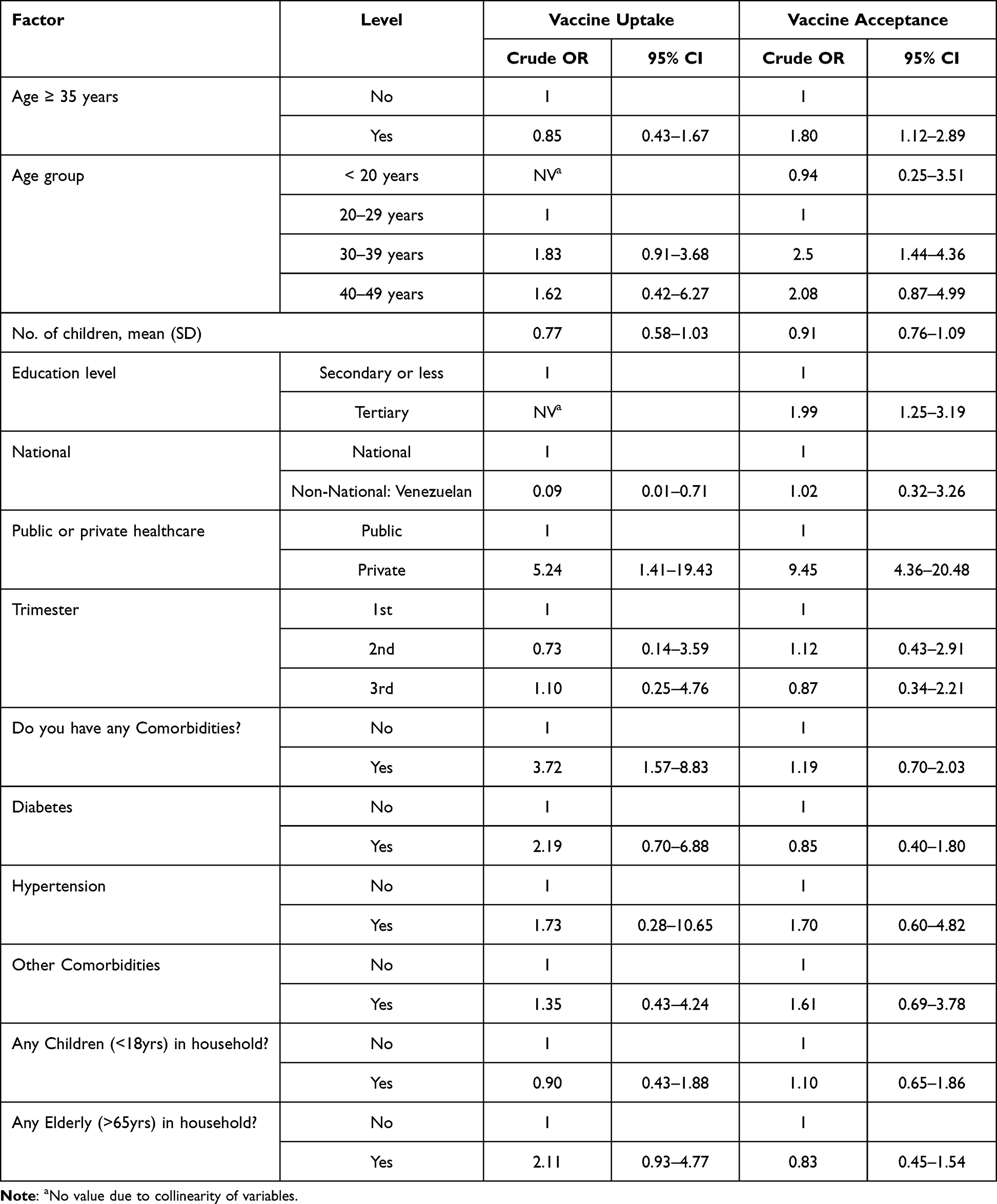 |
Table 7 Univariate Logistic Regression Analysis of Baseline Demographics as Predictors of COVID-19 Vaccine Uptake and Acceptance in Pregnancy |
As a subgroup analysis, responses of women seeking care in the public health sector and women seeking care in the private health sector were compared, as shown in Table 8. In terms of demographics, the public and private health sector participants only differed significantly by age (p = 0.009), number of children (p = 0.001), and education level (p < 0.001), where private health sector participants were older, had less children, and were more likely to have tertiary education as compared to the public health sector participants. The public and private health sector participants also had statistically significant differences in vaccine uptake (p < 0.001) and vaccine acceptance (p < 0.001). As shown in Table 8, 56.8% of the private sector participants were fully vaccinated prior to pregnancy compared to 25.2% in the public health sector. There was also a higher uptake in pregnancy in the private health sector participants (70.6%) compared to the public health sector participants (20.8%). Private sector participants were also more willing to accept the COVID-19 vaccine in pregnancy (71.1%) as compared to the public health sector participants (22.4%).
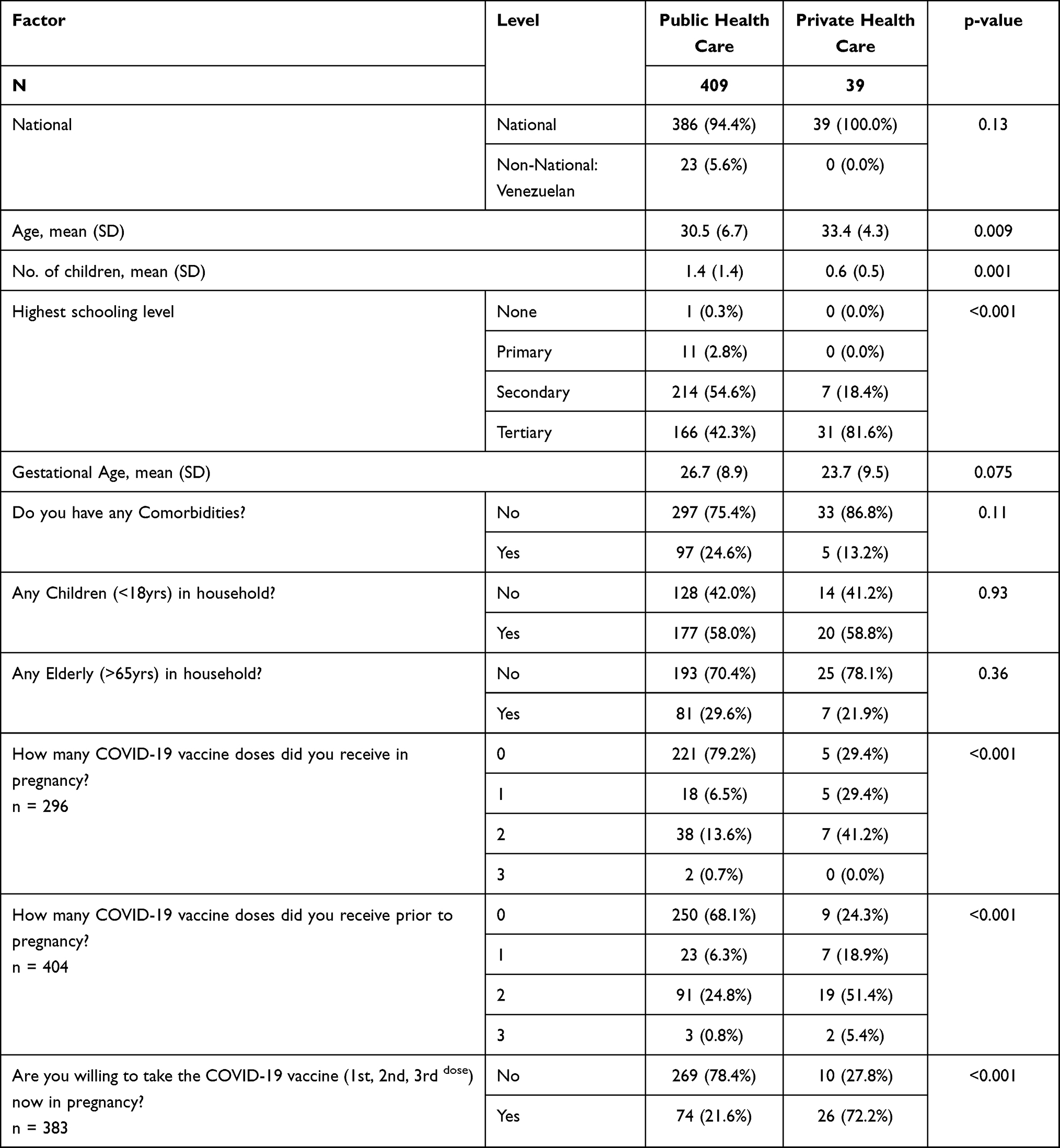 |
Table 8 Comparison of Demographics and Vaccine Uptake and Acceptance in Pregnancy in Women Seeking Care in the Public and Private Health Sectors |
Discussion
This study was the first regarding COVID-19 vaccine uptake, acceptance, and hesitancy in pregnancy in Trinidad and Tobago. It provided useful insights into the attitudes, beliefs, and knowledge of our pregnant population as it relates to the COVID-19 vaccine. It also highlighted the areas that need addressing when rolling out a vaccination program for pregnant women and where improvements can be made.
It is interesting that only 28.5% of our sampled pregnant population were fully vaccinated (2 or 3 doses of a COVID-19 vaccine) prior to pregnancy (Table 2) even though at the time of the survey, 50% of the general population of Trinidad and Tobago were fully vaccinated.6,7 This discrepancy between pregnant women and the general population may be due to the fact that the COVID-19 vaccines were initially only offered to the elderly, health-care workers, and persons with noncommunicable diseases.12 As a result, pregnant women had a shorter time-period to access and receive the vaccine. In addition, as shown in our study, vaccine hesitancy was more common in the younger age group, in keeping with the findings of Robertson et al, Battarbee et al and Hosokawa et al.13–15
In our study, lack of confidence in the safety of the vaccine in pregnancy proved to be the main reason why patients were hesitant in taking the vaccine. Complacency and convenience did not seem to play any significant role in the vaccine hesitancy in our pregnant population (Table 3). It was reassuring that the majority of participants found that the process of accessing and acquiring the vaccine was relatively easy and welcoming (Table 4).
Communication may have been an attributable factor for vaccine hesitancy as 61.6% of participants trusted health-care professionals the most for information on the COVID-19 vaccine in pregnancy. However, only 47.3% said they were advised by a health-care professional to take the vaccine (Table 6). Promotion of the COVID-19 vaccine by health-care professionals may need to be addressed if we are to improve vaccine acceptance and uptake. An interesting find was that the Venezuelan participants were 91% less likely to take the vaccine as compared to nationals. This suggests that separate strategies must be utilized to increase awareness in this vulnerable populations such as production of health information in Spanish, as the communication materials developed by the MoH during the COVID-19 pandemic were primarily in English. This is applicable not just to vaccination, but other health interventions as the Venezuelan migrants and asylum seekers constitute most of the non-national population in Trinidad and Tobago.16
The majority of pregnant women believed that the vaccine would harm their babies, or that there was not enough data on the COVID-19 vaccine in pregnancy (Table 3). These findings are again similar to the aforementioned studies.11,14,15 Understandably, pregnant women feel an overwhelming sense of protection to their unborn babies, and it may be that the time from development to implementation of the COVID-19 vaccine was just too short to be acceptable by this group.
There was a statistically significant difference in the COVID-19 vaccine acceptance rate between the public and private sectors. The difference in tertiary level education between the two groups is in keeping with the socioeconomic status of the patients who access the two types of care. It is likely that in the private setting, patients can spend more time with medical health personnel so that their questions can be answered and fears addressed, whereas in the busy public health antenatal clinics with 80–100 patients a day, it was not possible to provide the same attention to concerns about the COVID-19 vaccine. This again suggests that public health officials may need to alter current strategies to improve counselling and awareness in the public. It is clear that lack of awareness played a major part in vaccine hesitancy as over 60% of participants were unaware that the majority of adverse outcomes in pregnancy were in the unvaccinated (Table 5).
Although current MoH guidelines in Trinidad and Tobago recommend the Pfizer-BioNTech vaccine after 12 weeks of gestation, patients were most comfortable receiving the vaccine in the first trimester as compared to the second and third trimesters (Table 5). This suggests that more needs to be done to educate and publicize current evidence and recommendations. This can be in the form of television advertisements, posters in clinics and public counselling. Although only 3% of our participants trusted social media for information, social media can still be utilized, perhaps through different approaches and strategies, to disseminate relevant information via social media (Table 6).
Almost twice as many participants were willing to take the COVID-19 vaccine while breastfeeding compared with during the antenatal period (Table 6). This may suggest that patients are more worried about teratogenic side effects of the COVID-19 vaccine as opposed to the potential effects via transfer through breastfeeding. However, a follow-up study would be required to determine the actual uptake of the vaccine while breastfeeding.
Our findings should be considered within the context of its limitations. The sampling strategy used in this study was convenience sampling. Additionally, accurate data on the population of the catchment area of the clinics and the number of pregnant women were not available. Both these factors could have resulted in underrepresentation of some groups in the study. This study was cross-sectional in nature, and as such, participants were not followed up to determine if they did follow through with the vaccine or if their attitudes changed as more information became available. A larger sample size is needed to examine the differences between the public and private health sector participants, and the national and Venezuelan non-nationals. It was recognized that it would have been useful to enroll patients from private practices in other parts of the island, but this was met with a lack of support. There is selection bias as the study was limited to pregnant women who sought antenatal care, and the findings may not be reflective of pregnant women who do not seek antenatal care. The results of the study also may not be generalizable to other regions, who differ by demographics such as age and education level which were found to be significant predictors of vaccine acceptance.
Despite these limitations, our study provides new information on the attitudes, beliefs, and knowledge of COVID vaccination in pregnancy, which remains a critical public health issue.
Conclusion
Overall, the COVID-19 vaccine uptake and acceptance rates were relatively low, 23.6% and 26.4%, respectively. The main reason for hesitancy was due to a lack of confidence in the COVID-19 vaccines. This was attributed to the vaccine being harmful to the baby and the lack of research on the COVID-19 vaccine in pregnancy. Although lack of confidence in the vaccine was the main reason for hesitancy, lack of awareness with respect to specific facts on the vaccine may have contributed as well. Promotion and public education by health-care professionals and institutions may need to be improved to address these issues.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID19 -March 2020 [Internet]. Geneva: World Health Organization; 2020. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-The-media-briefing-on-COVID-19---11-march-2020#:~:text=WHO%20has%20been%20assessing%20this,be%20characterized%20as%20a%20pandemic.
2. Basta NE and Moodie EMM on behalf of the VIPER (Vaccines, Infectious disease Prevention, and Epidemiology Research) Group COVID-19 Vaccine Development and Approvals Tracker Team. COVID-19 vaccine development and approvals tracker; 2020. Available from: https://covid19.trackvaccines.org.
3. World Health Organization. WHO SAGE Roadmap for Prioritizing Use of COVID-19 Vaccines [Internet]. Geneva: World Health Organization; 2022. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-Vaccines-SAGE-Prioritization-2022.1.
4. World Health Organization. Questions and Answers: COVID-19 Vaccines and Pregnancy [Internet]. Geneva: World Health Organization; 2022. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-FAQ-Pregnancy-Vaccines-2022.1.
5. Pan American Health Organization. Trinidad and Tobago Receives the First COVID-19 Vaccines Through the COVAX Facility [Internet]. Pan American Health Organization; 2021. Available from: https://www.paho.org/en/news/31-3-2021-trinidad-and-tobago-receives-first-COVID-19-vaccines-through-covax-facility.
6. Johns Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) [Internet]. Johns Hopkins University. Available from: https://coronavirus.jhu.edu/vaccines/international.
7. Live Covid-19 vaccination tracker. Available from: https://covidvax.live/location/tto.
8. Matroo C. Joy at POSGH. Available from: https://newsday.co.tt/2019/05/12/joy-at-posgh/.
9. CDC Division of Reproductive Health. Estimating the number of pregnant women in a geographic area. Available from: https://www.measureevaluation.org/resources/publications/sr-03-12/at_download/document.
10. Larson HJ, Jarrett C, Schulz WS, et al. Measuring vaccine hesitancy: the development of a survey tool. Vaccine. 2015;33(34):4165–4175. doi:10.1016/j.vaccine.2015.04.037
11. Goncu Ayhan S, Oluklu D, Atalay A, et al. COVID-19 vaccine acceptance in pregnant women. Int J Gynecol Obstet. 2021;154:291–296. doi:10.1002/ijgo.1371
12. Ministry of Health Government of the Republic of Trinidad and Tobago. Covid-19 vaccine frequently asked questions. Available from: https://health.gov.tt/covid-19/covid-19-vaccine/faqs.
13. Robertson E, Reeve KS, Niedzwiedz CL, et al. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav Immun. 2021;94:41–50. doi:10.1016/j.bbi.2021.03.008
14. Battarbee AN, Stockwell MS, Varner M, et al. Attitudes toward COVID-19 illness and COVID-19 vaccination among pregnant women: a cross-sectional multicenter study during August-December 2020. Am J Perinatol. 2022;39:75–83. PMID: 34598291. doi:10.1055/s-0041-1735878
15. Hosokawa Y, Okawa S, Hori A, et al. The prevalence of COVID-19 vaccination and vaccine hesitancy in pregnant women: an internet-based cross-sectional study in Japan. J Epidemiol. 2022;32(4):188–194. PMID: 35095091; PMCID: PMC8918615. doi:10.2188/jea.JE20210458
16. Thomas-Hope E. Migration in Trinidad and Tobago: current trends and policies. United Nations Development Programme; 2022. Available from: https://www.undp.org/latin-america/publications/migration-trinidad-and-tobago-current-trends-and-policies.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.