Back to Journals » Patient Preference and Adherence » Volume 17
COVID-19 Vaccine Hesitancy and Its Associated Factors Among Adolescents
Authors Alemu D, Diribsa T, Debelew GT ![]()
Received 17 December 2022
Accepted for publication 9 May 2023
Published 16 May 2023 Volume 2023:17 Pages 1271—1280
DOI https://doi.org/10.2147/PPA.S400972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Dawit Alemu, Tujuba Diribsa, Gurmesa Tura Debelew
Department of Population and Family Health, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Tujuba Diribsa, Department of Population and Family Health, Jimma University, Jimma, Ethiopia, Tel +251 925270679, Email [email protected]; [email protected]
Background: Currently, COVID-19 disease is a major public health issue that affects a large number of people worldwide. The COVID-19 vaccine is one of the best preventative measures. Adolescents between the ages of 12 and 17 are eligible to get the COVID-19 vaccine. The COVID-19 pandemic cannot be stopped if people are reluctant to use this vaccine. However, the extent of COVID-19 vaccine hesitancy and related variables among adolescents are not well understood.
Objectives: To assess the magnitude of COVID-19 vaccine hesitancy and its associated factors among adolescents in Seka Chekorsa town, Jimma, Ethiopia.
Methods: Institutional-based cross-sectional study employing both qualitative and quantitative methods were used. The study participants were selected using a simple random sampling technique. Data were collected using interviewer-administered questions. Data collected was checked for completeness and entered into EPI data version 3.1. Finally, data were exported to SPSS version 25 for further analysis. The bivariate analysis was used to identify variables eligible for multivariate logistic regressions. In a multivariable analysis to identify factors that have statistically significant association, a p value less than 0.05 and a 95% confidence interval were used. The qualitative data were triangulated with quantitative data.
Results: In this study, 379 adolescents were participated, yielding a response rate of 95.2%. The magnitude of COVID-19 vaccine hesitancy among adolescents was 29% (95% CI: 24.3– 33.5%). Being female (AOR = 1.89, 95%, 1.81– 3.56), primary education (AOR = 2.99, 95% CI: 1.26– 3.56), source information from social media (AOR = 2.42, 95% CI: 1.06– 5.57), poor knowledge about COVID-19 disease (AOR = 3.18, 95% CI: 1.66– 6.12), unfavorable attitude (AOR = 5.2, 95% CI: 2.76– 9.79) and poor knowledge towards COVID-19 vaccine (AOR = 5.66, 95% CI, 2.91– 11.0) were associated with COVID-19 vaccine hesitancy among adolescents.
Conclusion: This study shows that COVID-19 vaccine hesitancy among adolescents is very high. Being female, poor knowledge towards COVID-19 disease and the vaccine, an unfavorable attitude and social media were factors significantly associated with COVID-19 vaccine hesitancy.
Keywords: COVID-19 disease, adolescent, COVID-19 vaccine hesitancy
Introduction
A plague known as severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) that led to COVID-19 disease was declared as an outbreak on March 11, 2020, by WHO. Severe acute respiratory syndrome coronavirus 2 (SARS CoV 2) is a strain of coronavirus that causes COVID-19 (coronavirus disease 2019), the respiratory illness responsible for the ongoing COVID-19 pandemic. Initially, it was thought that respiratory droplets from coughs and sneezes within a 1.8-meter radius were the main source of transmission. Recent evidence has revealed that the virus may also be airborne, with the possibility that aerosols could spread the disease.1
As of February 2023, there have been 757,264,511 confirmed cases of COVID-19 worldwide, with 6,850,594 fatalities reported by WHO.2 According to WHO, there were 7572 deaths and 499,833 confirmed cases of COVID-19 in Ethiopia between 3 January 2020 and 21 February 2023.2 According to a UNICEF report, 17,200 people died from COVID-19 were people under the age of 20, of which adolescents aged 10 to 19 account for 53% of these deaths.3
The World Health Organization has set up COVID-19 vaccination strategies through prioritization. First, older people and highly risk groups are vaccinated with a goal of reducing the highest risk of mortality. Second, all adults are vaccinated with a goal of risk mitigation, lowering disease burden, lowering the burden of the health system and returning to socioeconomic interests. Lastly, widespread immunization of adolescents is needed to significantly minimize disease burden and the probability of novel variant formation, possibly by preventing viral transmission.4
Ethiopia deployed around 6.2 million doses of COVID-19 vaccines on November 25, 2021, including those from Sino Pharma, AstraZeneca, Johnson & Johnson, and Pfizer-BioNTech, immunizing 5.4 million people, with Pfizer-BioNTech vaccinations only valid for adolescent aged 12 to 17.5 However, the challenge of COVID-19 vaccine hesitancy causes this strategy to be difficult to achieve. According to the World Health Organization definition, vaccine hesitancy is defined as a delay to accept or resistance to a vaccine in spite of the presence/accessibility of a vaccine carrier.6 According to several research findings, young people, particularly students, are more likely to contract COVID-19 and spread the infection to others.7
According to a USA report, only 53% of adolescents aged 12 to 17 had received all recommended vaccinations by the beginning of January 2022. On January 8, 2022, the complete COVID-19 vaccine vaccination rate in Africa was 9.6%, with an estimate that fifty-two countries had less than 10% coverage, which is contrary to WHO targets of 40% by the end of 2021 and 70% by the end of June 2022.8 According to research conducted in China, the majority of adolescents between the ages of 12 and 17 were hesitant to receive the COVID-19 vaccine at a rate of 58%.9
There is a limited study and report regarding the impact of COVID-19 among adolescents. According to a UNICEF report, 12,800 children and adolescents died from COVID-19, and of those, 58% were adolescents owing to both direct and indirect causes.10 According to a systematic review on adolescents aged 10 to 19 years, of the 3788 global deaths caused by COVID-19, 3394 (91.5% of deaths) occurred in low- and middle-income countries.11 According to a study conducted in the Oromia region, Ethiopia, 10.7% of cases of COVID-19 were found in people aged 10 to 19 years, with cases occurring at rates of 44.9 and 22.1 for people in the 20 to 29 and 30–39 age groups, respectively.12
Determinants of COVID-19 vaccine hesitancy among adolescents were not clearly identified in Ethiopia. According to a study done on vaccine uptake in Ethiopia, only 31.4% of the general public are interested in accepting COVID-19 vaccines.13 In Ethiopia, a few studies were conducted regarding COVID-19 vaccine acceptance among adults, university students and the health profession. However, as far as the investigators know, there is no study conducted on COVID-19 vaccine hesitancy and its associated factors among adolescents in Ethiopia.
Methods
Study Setting and Design
This study was conducted in Seka Chekorsa town, Jimma, Ethiopia. Seka Chekorsa town is located 20km away from Jimma town and 370 km from Addis Ababa. Seka Chekorsa Woreda has a total population of 310,721, the youth 93,240 and total adolescents resides in town are 2456. There are three governmental primary schools which teach around 1402 from grade 5–8 students and two secondary schools which serve around 4152 students from grade 9 to 12. Woreda has 9 health centers and one primary hospital. An institutional-based cross-sectional study was conducted on school adolescents’ age group of 12–17 years, from June 20, 2022, to July 15, 2022.
Study Population and Sampling Procedures
This study was conducted on school adolescents in the age group of 12–17 years attending their education at Seka Chekorsa town. Study participants were selected from primary and secondary schools. This study was conducted after COVID vaccine has been started to be offered for adolescents. Samples were calculated using a single proportioned formula. Since there is no prior similar study on adolescents about the COVID-19 vaccine among adolescents in Ethiopia and also to get the maximum sample size for the study proportion of 50%, 5% margin of error and 95% confidence of interval were used. Accordingly, the final sample size was 398 used for quantitative study. Then, the sample size was proportionally allocated to both primary and secondary education and the study participants were selected by a simple random technique using a computer-generated lottery method. For qualitative study, adolescents from different schools, local community leaders and health workers who participated in the COVID-19 vaccine campaign period were involved.
Data Collection Tools and Procedures
The structured questionnaire was developed after reviewing relevant literature. The questionnaire was prepared in English, translated to the local language (Afaan Oromo and Amharic) and then back to English to check its consistency. Two weeks before actual data collection, a pretest was conducted at Shebe town, which is about 50km away from the study area. Before beginning the task, two supervisors and four data collectors were hired and instructed on how to collect the data and elucidate the questionnaire. Data were collected using an interviewer administered questionnaire. For qualitative data, an interview guide was developed after reviewing different related literature. In-depth interviews were made by the principal investigator with purposely participants.
Data Processing and Analysis
Data was collected, verified as complete, cleansed, coded, entered into EPI Data statistical software version 3.1, and then exported to SPSS Windows version 23 for additional analysis. The study population was described in relation to relevant variables using frequencies, proportions, and summary statistics, and then presented using text, tables, and figures. The bivariate analysis was employed to identify candidate variables for multivariable analysis. Then, to control potential confounding effects, variables with p-values less than 0.25 were included in the multivariable logistic regression. Finally, variables which had significant associations were identified at p value <0.05 and Adjusted OR with 95% CI was determined to see the strength of the associations.
The Hosmer and Lemeshow test was used to check the fitness of the model. For qualitative data, in-depth interviews were audio-recorded, transcribed, and translated to English. After reading the text several times, codes were given and related codes were categorized. Then, categories were merged to form themes. Finally, the findings were presented in narrations and triangulated with quantitative findings.
Data Quality Assurance and Ethical Issues
Quality of data was assured through careful design, translation and retranslation of the questionnaire. A pre-test was conducted to ensure clarity, logical sequence and skip pattern of the questionnaire. Training was given to data collectors and supervisors, and the overall supervision was carried out by researchers. Supervisors evaluated and verified the questionnaire daily for accuracy and consistency, and the next morning they provided the necessary feedback. The trustworthiness of qualitative data was ensured by triangulation of findings, taking field note, careful transcription and translation, and rich description of the study methods.
This study was approved by the institutional review board of Jimma University. The official letter to undertake the study was obtained from the Seka Chekorsa Woreda education office. Informed verbal consent was undertaken from parents or guardians, and assent was got from study participants.
Results
Socio-Demographic and Economic Characteristics of the Study Participants
In this study, a total of 379 adolescents participated, yielding a response rate of 95.2%. Out of total respondents, 210 (55.4%) of them were found in the age group of 16–17 years and 197 (52%) were females. Among study participants, 60.4% and 77.6% were Muslims and Oromo ethnicities, respectively (Table 1).
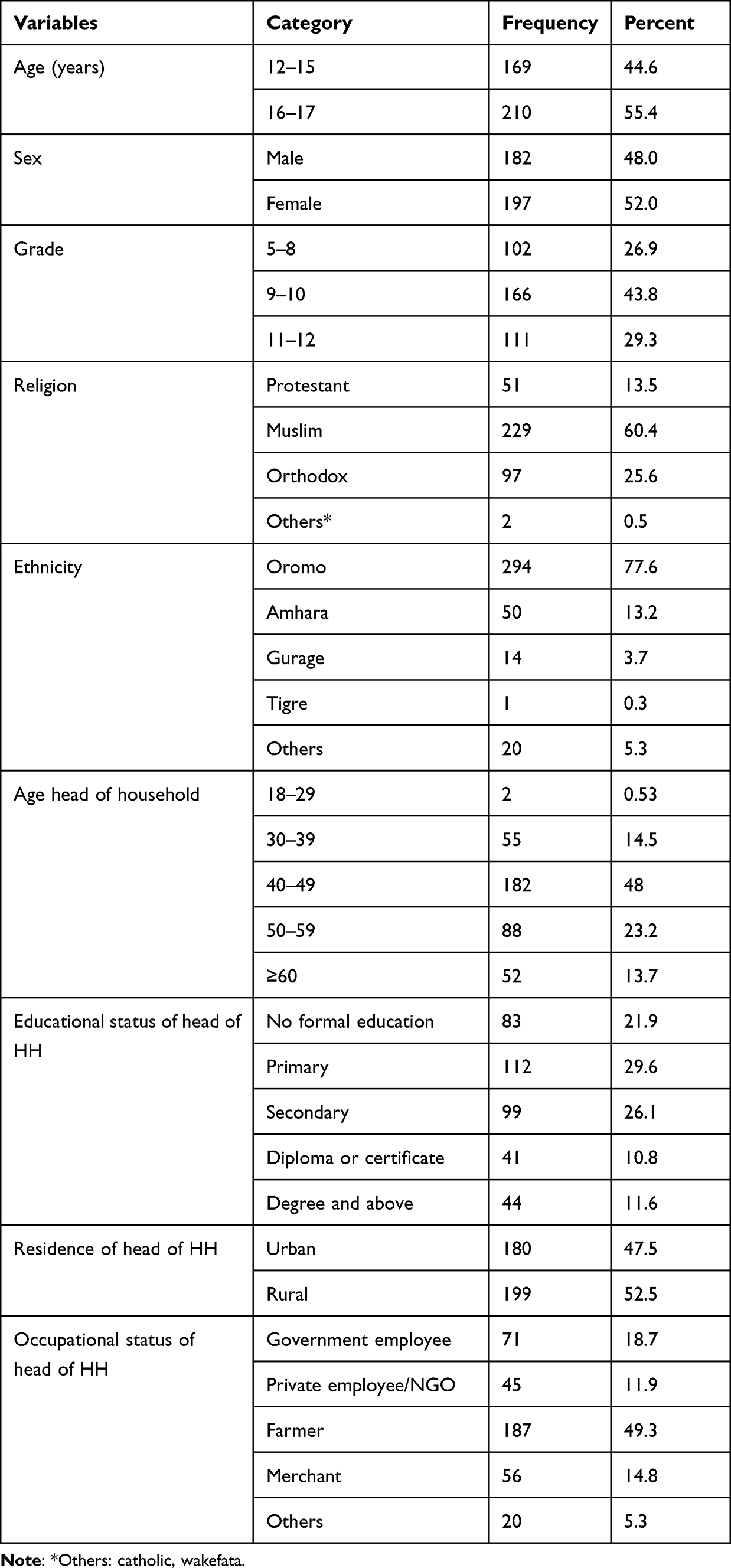 |
Table 1 Socio-Demographic Characteristics of Adolescents in Seka Chekorsa Town, Jimma Zone, Southwest Ethiopia, 2022 |
Knowledge About COVID-19 Disease
This study assessed knowledge related to the COVID-19 disease and the mean score of 4.96 (SD = 1.53) used for categorization. The score below the mean is used as the cut-off point for poor knowledge and above or equal to 4.96 is the cut-off point for good knowledge about COVID-19 disease. Accordingly, 68.3% of the adolescents had good knowledge about COVID-19 disease (Figure 1).
 |
Figure 1 Knowledge about COVID-19 disease among school adolescents in Seka town Jimma zone, southwest Ethiopia, 2022. |
Knowledge, Attitude and Perception Towards COVID-19 Vaccine
Knowledge, attitude and perception towards COVID-19 vaccine are classified based on their respective mean scores. A mean score below 4.7 is considered as poor knowledge and a mean score equal or above is considered as good knowledge. Accordingly, 40.4% of study participants had poor knowledge of the COVID-19 vaccine (Figure 2).
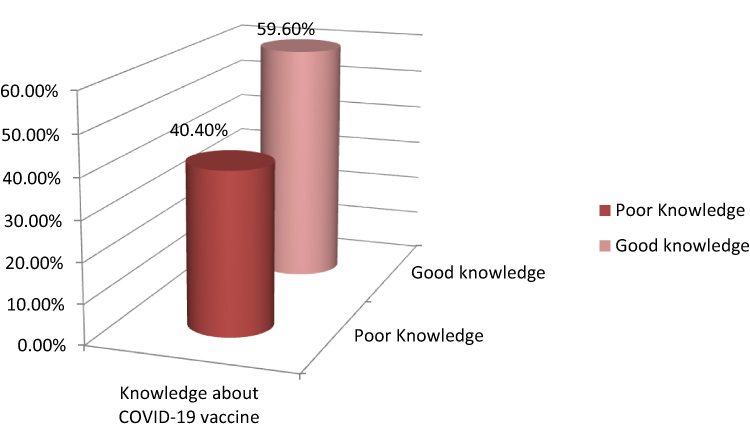 |
Figure 2 Knowledge about COVID-19 vaccine among school adolescent study participant Seka town, Jimma zone, southwest Ethiopia, 2022. |
Regarding the attitude towards vaccines, a mean score below 28.7 is considered as an unfavorable attitude and a score equal or above means considered as having a favorable attitude. Accordingly, 38.3% of study participants had an unfavorable attitude towards the COVID-19 vaccine (Figure 3).
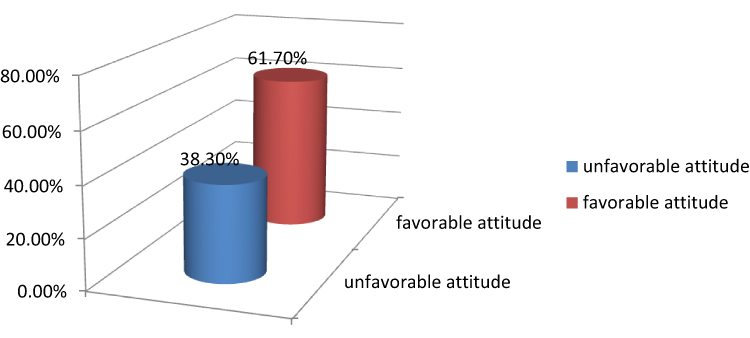 |
Figure 3 Attitude towards COVID-19 vaccine among school adolescents Seka town, Jimma Zone, southwest Ethiopia, 2022. |
Regarding perception of the COVID-19 vaccine, the mean score of 11.20 (SD = 1.93) was used. Accordingly, among the study participants, 60.2% of them had a negative perception towards the COVID-19 vaccine.
The finding from a qualitative study also shows:
…I’m at low risk of COVID-19 disease and I don’t want to get a vaccine against COVID-19….I don’t trust the COVID-19 vaccine. It is a means to transmit COVID-19 disease and spread the illuminati religion or Satanism. ….My religion also doesn’t permit you to take this vaccine…… (A 16-years old student)
…I have seen information about the COVID-19 vaccine from Facebook that it has severe side effects……. (A 17-year- old student 11th male student)
…. Most of the time, this disease affects old and adult individuals and I don’t think that it is important to vaccinate children or adolescents…. (48-year-old religious leader)
Magnitude of COVID-19 Vaccine Hesitancy Among Adolescents
According to this study, COVID-19 vaccine hesitancy among school adolescents was 110 (29.0%) (95% CI: 24.3–33.5%) (Figure 4).
 |
Figure 4 Magnitude of COVID-19 vaccine hesitancy among adolescents in Seka Chekorsa town, Jimma, Ethiopia. |
Factors Associated with COVID-19 Vaccine Hesitancy
Bivariate analysis was performed to identify candidate variables for multivariate analysis at p value <0.25. Age, sex, education levels, the number of children in the family, the parents’ vaccination status, the information source, knowledge of the COVID-19 disease, knowledge of the COVID-19 vaccine, perception of the COVID-19 vaccine, and attitude toward the COVID-19 vaccine were candidate variables for multivariable analysis.
In multivariable analysis, sex, educational level, source of information, knowledge about COVID-19 disease, knowledge about COVID-19 vaccine and attitude towards COVID-19 vaccine showed statistical significant association with COVID-19 vaccine hesitancy at p-value <0.05 with 95% CI.
Accordingly, the odds of vaccine hesitancy among female adolescents were 2 times (AOR = 1.89, 95% CI, 1.81–3.56) higher than the odds among male adolescents. The odds of vaccine hesitancy among adolescents in primary education were 3 times (AOR = 2.998, 95% CI, 1.26–7.13) higher than those in preparatory school.
The odds of vaccine hesitancy among adolescents who obtained information from social media about the COVID-19 vaccine were 2.42 higher than adolescents who obtained information from friends (AOR = 2.42, 95% CI, 1.06–5.57). These findings also supported the qualitative findings:;
….I heard a lot of information about the COVID-19 vaccine from social media that it has serious side effects and is suspected of…….I don’t allow my children to vaccinate for COVID-19 because of its serious side effects which may harm my children….(A 42 years old male participant)
The odds of vaccine hesitancy among adolescents who had poor knowledge of COVID-19 disease were 3.18 (AOR = 3.18, 95% CI, 1.66–6.12) higher than students who had good knowledge of COVID-19.
In this study, the odds of vaccine hesitancy among adolescents who had poor knowledge of the COVID-19 vaccine were 5.66 times (AOR = 5.66, 95% CI, 2.91–11.0) higher than adolescents who had good knowledge.
….Coronavirus vaccine is less protective from corona virus ….I couldn’t understand coronavirus as safe for children. (A 52 years old male)
In the present finding, the odds of vaccine hesitancy among adolescents who had an unfavorable attitude were 5.2 times (AOR = 5.2, 95% CI, 2.76–9.79) higher than their counterpart (Table 2).
 |
Table 2 Multivariable Logistic Regression of Factors Associated with COVID-19 Vaccine Hesitancy Among Adolescents in Seka Town, Jimma Town, Southwest Ethiopia, 2022 G.C |
Discussion
One crucial tactic to combat the spread and burden the COVID-19 disease imposes on society is the COVID-19 vaccine. Additionally, it is a means to mitigate the risk of new variant emergence. However, the strategies concerning COVID-19 vaccination have been challenged by vaccine hesitancy.
According to this study, the magnitude of COVID-19 vaccine hesitancy among adolescents was 29% (24.3–33.5%). This result is consistent with a study done in China, whereby 31.6% of teenagers refused to receive COVID-19 immunization.14 Also, the finding is consistent with a study conducted in Nigeria, in which 25% of adolescents were hesitant to take a vaccine.15 However, this finding is much greater than studies conducted in Germany, which was 68.3%.16 This discrepancy might be due to socioeconomic differences, which determine accessibility to health services and health information.
In this study, female students were 1.89 times higher in COVID-19 vaccine hesitation than male students. The finding is comparable with studies conducted in America,17 Addis Ababa18 and China.14 This possible justification behind the findings could be due to the difference in accessibility to information between females and males, which is associated with the status of women in the community. Additionally, there was widespread misinformation about the COVID-19 vaccine as the vaccine causes women to be infertile, which could increase the hesitation among females.17
In this study, adolescents in primary education are 3 times more likely to be hesitant to use a vaccine than those attending preparatory education. This finding is in line with a study conducted in South Africa19 and a study conducted in Canada.20 The possible justification of the findings is that those at a lower grade are less accessible to sufficient information about vaccines.
Regarding source of information, odds of vaccine hesitancy among social media users were 2.42 higher than friends. Similarly, findings from a study conducted in Addis Ababa show that information from social media increases hesitancy. Social media users were highly exposed to misperception and overestimation of side effects of the vaccine.21 On the other hand, those adolescents who obtained information from health professionals were 80% less likely to have vaccine hesitancy when compared with those getting information from friends. Qualitative findings also support this
….I heard a lot of information about the COVID-19 vaccine from social media that it has serious side effects…….I restrict my family to vaccinating COVID-19 vaccine…. (A 42 years old male participant)
Moreover, the present study revealed that adolescents who had poor knowledge about COVID-19 disease, poor knowledge about the vaccine, and unfavorable attitude towards the vaccine were 3 times, 5 times and 5 times more likely to have vaccine hesitancy than their counterparts, respectively. These findings are similar to other studies conducted in Addis Ababa and China a.18,22,23 The possible justification of the findings could be explained by the fact that good knowledge of COVID-19 disease, good knowledge of the vaccine, and a positive attitude toward the vaccine result in fewer false beliefs and misinformation about the vaccine, which may reduce resistance to the COVID-19 vaccine. The finding is also supported by the qualitative data.
…I’m at low risk to COVID-19 disease and I don’t want to get a COVID-19 vaccination… (A 16-year-old, grade 10 student)
Furthermore, this study showed that the attitude of COVID-19 vaccine is significantly associated with vaccine hesitancy. Those adolescents with an unfavorable attitude about the COVID-19 vaccine were 5 times more likely to have vaccine hesitation than those with a favorable attitude. Similar findings from studies in Addis Ababa and China showed that individuals with attitudes were more prone to the COVID-19 vaccine than their counterparts.18 The findings from qualitative support these findings
…I don’t trust COVID-19 vaccine and it is also a means to transmit COVID-19 disease and spread illuminati religion or Satanism… My religion does not allow me to take this vaccine…… (A 17 years old, grade 11 student)
As a limitation of these study variables like having at least one parent vaccinated and history receiving the influenza vaccine was not included.
Conclusions
In general, the finding from this study shows that the magnitude of COVID-19 vaccine hesitancy among adolescents is very high. Being female, information sources from social media, an unfavorable attitude to the COVID-19 vaccine, and poor knowledge about COVID-19 disease and the vaccine were the factors that have an association with vaccine hesitancy. Therefore, it is essential to work on providing enough information about the vaccine and minimizing the negative view of the vaccine in order to scale up the COVID-19 vaccine uptake among adolescents.
Abbreviations
AOR, Adjusted Odds Ratio; COR-Crudes Odds Ratio; COVID-19, Coronavirus Disease 2019; SAGE, Strategic Advisory Group of Experts (on Immunizations); SARS-COV-2, Severe Acute Respiratory Syndrome Coronavirus 2; UNICEF, United Nations International Children’s Fund; WHO, World Health Organization.
Data Sharing Statement
All data generated or analyzed during this study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical clearance was obtained from the institutional review board of Jimma University, Institute of Health. Permission to conduct the study was obtained from all necessary authorities. Study participants received full details about the purpose, advantages, and right to decline, as well as assurances of confidentiality. Before the interview, written informed consent was obtained from study participants. For minors (<18 years), written informed consent from their parent/guardian and assent from the children was obtained. Information that has been collected is kept private and confidential.
Acknowledgments
We would like to pass our thanks to Jimma University for the financial support for this study and the Department of Population and Family Health for its mentorship. We are also thankful to the study participants, data collectors and supervisors for their willingness and commitment to participate in this study.
Author Contributions
All authors contributed significantly to the conception, design, implementation, collection, analysis, and interpretation of the data, as well as the writing, editing, and critical review of the article. They also agreed on the journal to which the article should be submitted and gave final approval of the version to be published. All authors also agreed to be responsible for all aspects of the work.
Funding
Sponsored by Jimma University.
Disclosure
The authors declare that they have no competing interests.
References
1. Riley T, Sully E, Ahmed Z, Biddlecom A. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low- and middle-income countries. Int Perspect Sex Reprod Health. 2020;46:73–76. doi:10.1363/46e9020
2. WHO,COVID 19 Weekly Epidemiological Update ; 2023. Available from https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—1-february-2023
3. UNICEF. Child mortality and COVID-19 - UNICEF DATA. Unicef Data; 2020. Available from: https://data.unicef.org/topic/child-survival/under-five-mortality/.
4. Document T. Global COVID-19 vaccination – strategic vision for 2022 technical document; 2022:1–92.
5. World Health Organization. Ethiopia launches a COVID-19 vaccination campaign targeting the 12 years and above population; 2022.
6. Sage, World Health Organization. Strategies for addressing vaccine hesitancy – a systematic review; 2014.
7. Tavolacci MP, Dechelotte P. COVID-19 vaccine acceptance, hesitancy, and resistancy among university students in France; 2021:1–13.
8. Sam NA. Children and adolescents in African countries should also be vaccinated for COVID- - 19; 2022:1–6.
9. Willis DE, Presley J, Williams M, Zaller N, Pearl A. COVID-19 vaccine hesitancy among youth ABSTRACT. Hum Vaccin Immunother. 2021;17(12):5013–5015. doi:10.1080/21645515.2021.1989923
10. UNICEF. Child Mortality and COVID 19 report; 2022. Available from: https://data.unicef.org/topic/child-survival/covid-19/.
11. Id TK, Kitano M, Krueger C, et al. The differential impact of pediatric COVID-19 between high-income countries and low- and middle-income countries: a systematic review of fatality and ICU admission in children worldwide. PLoS One. 2021;394(Lmic):1–12.
12. Gudina EK, Gobena D, Debela T, et al. COVID-19 in Oromia Region of Ethiopia: a review of the first 6 months’ surveillance data. BMJ Open. 2021;11(3):1–9. doi:10.1136/bmjopen-2020-046764
13. Belsti Y. Willingness of Ethiopian population to receive COVID-19 vaccine; 2021:1233–1243.
14. Rehati P, Amaerjiang N, Yang L, et al. COVID-19 vaccine hesitancy among adolescents: cross-sectional school survey in four Chinese cities prior to vaccine availability. Vaccines. 2022;10(3):452. doi:10.3390/vaccines10030452
15. Adebisi YA, Alaran AJ, Bolarinwa OA, Akande-Sholabi W, Lucero-Prisno DE. When it is available, will we take it? Social media users’ perception of hypothetical covid-19 vaccine in Nigeria. Pan Afr Med J. 2021;2021:38.
16. Zychlinsky Scharff A, Paulsen M, Schaefer P, et al. Students’ age and parental level of education influence COVID-19 vaccination hesitancy. Eur J Pediatr. 2022;181(4):1757–1762. doi:10.1007/s00431-021-04343-1
17. Waters AR, Kepka D, Ramsay JM, et al. COVID-19 vaccine hesitancy among adolescent and young adult cancer survivors. JNCI Cancer Spectr. 2021;5:1–4. doi:10.1093/jncics/pkab049
18. Dereje N, Tesfaye A, Tamene B, et al. COVID-19 vaccine hesitancy in Addis Ababa, Ethiopia: a mixed-method study. BMJ Open. 2022;12(5):e052432. doi:10.1136/bmjopen-2021-052432
19. Engelbrecht M, Heunis C, Kigozi G. COVID-19Vaccine hesitancy in South Africa: lessons for future pandemics. Int J Environ Res Public Health. 2022;19(11):6694. doi:10.3390/ijerph19116694
20. Lavoie K, Gosselin-Boucher V, Stojanovic J, et al. Understanding national trends in COVID-19 vaccine hesitancy in Canada: results from five sequential cross-sectional representative surveys spanning April 2020-March 2021. BMJ Open. 2022;12(4):1–12. doi:10.1136/bmjopen-2021-059411
21. Puri N, Coomes EA, Haghbayan H, Gunaratne K. Social media and vaccine hesitancy: new updates for the era of COVID-19 and globalized infectious diseases. Hum Vaccin Immunother. 2020;16(11):2586–2593. doi:10.1080/21645515.2020.1780846
22. Cai H, Bai W, Liu S, et al. Attitudes toward COVID-19 vaccines in Chinese adolescents. Front Med. 2021;8:1–6. doi:10.3389/fmed.2021.691079
23. El-Elimat T, AbuAlSamen MM, Almomani BA, Al-Sawalha NA, Alali FQ. Acceptance and attitudes toward COVID-19 vaccines: a cross-sectional study from Jordan. PLoS One. 2021;16(4April):1–15. doi:10.1371/journal.pone.0250555
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.