Back to Journals » Risk Management and Healthcare Policy » Volume 15
COVID-19 Prevention Practices Among Prisoners, in Southern Ethiopia
Authors Chea Hankalo N ![]() , Alemayehu A
, Alemayehu A ![]() , Fikre R
, Fikre R ![]() , Shona E
, Shona E
Received 8 December 2021
Accepted for publication 8 March 2022
Published 20 March 2022 Volume 2022:15 Pages 521—528
DOI https://doi.org/10.2147/RMHP.S350257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Nana Chea Hankalo,1 Akalewold Alemayehu,1 Rekiku Fikre,2 Edilu Shona3
1School of Public Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2Departments of Midwifery, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 3School of Law, College of Law and Governance, Hawassa University, Hawassa, Ethiopia
Correspondence: Nana Chea Hankalo, School of Public Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia, Email [email protected]; [email protected]
Background: Coronavirus disease-19 (COVID-19) is a highly contagious disease with high attack and case fatality rate. Since WHO’s declaration of disease as pandemic in March 2020, the unprecedented global crises have been happening. To curb and reduce such crises, multi-dimensional international efforts have been made, particularly, infection prevention measures has been developed. However, there was a wide gap of implementing COVID-19 prevention measures from rural to urban, from institution to institution and from person to person. Therefore, the aim of this study was to measure the level of prevention practice towards COVID 19 and associated factors in prison, in Sidama National Regional State, Ethiopia.
Methods: A cross-sectional study using quantitative method of data collection was conducted in November, 2020 among 422 prisoners in two prisons. Data were collected by trained nurses using structured questionnaires. We analyzed data using SPSS version 24 software. Descriptive statistics and bivariable and multivariable logistic regression analyses were employed to identify factors associated with prevention practices of COVID-19.
Results: More than one-fifth (22%; 95% CI: 19%, 26%) of respondents had good preventive practice. Participants who had a history of alcohol intake were 1.79 times less likely to implement good preventive practice for COVID-19 (AOR = 1.79; 95% CI; 1.09, 2.93). The respondents who had negative attitude towards COVID-19 infection were 1.69 times more likely to have poor prevention practice (AOR = 1.69; 95% CI: 1.02, 2.81).
Conclusion and Recommendation: In this study, COVID-19 prevention practice among prisoners was very low. Negative attitude and previous alcohol taking history were factors associated with poor prevention practice. Accordingly, the researchers recommends to the concerned body to design educational intervention to change the attitude towards COVID-19 and other infectious diseases and behaviors of the prisoners.
Keywords: COVID-19, prevention practice, prison, Sidama, Ethiopia
Background
Coronavirus disease-19 (COVID-19) is a disease caused by a new strain of coronavirus. The virus is linked to the same family of viruses as severe acute respiratory syndrome (SARS) and some types of common cold. COVID-19 manifestation includes but is not limited to fever, cough and shortness of breath. In more complicated cases, the infection can cause pneumonia or breathing difficulties.1 Touching the contaminated surface and body of infected person, direct contact with the respiratory droplet of an infected person during and after coughing and sneezing is its means of transmission.2
As of February 3, 2022, globally there were 391,393,876 COVID-19 confirmed cases, 310,264,020 recoveries and 5,743,921 deaths.3 In Africa in the same period, there were 11,164,044 COVID-19 confirmed cases, 10,017,825 recoveries and 241,317 deaths.3 Similarly, as of February 3,2022 Ethiopia had 466,289 confirmed cases, 400,374 recoveries and 7355 deaths.4
Since COVID-19ʹs declaration as a Public Health Emergency of International Concern (PHEIC) in March, 2020, the virus has spread to almost all countries of the world. Among many factors, poor hand cleanliness, congestion in the same area, and bodily contacts like handshaking contributed for the fast spread of the virus within minimal period of time. The World Health Organization (WHO) recommends widely inform the public about the cause and, mode of transmission of the disease, and simple prevention methods such as hand washing with soap or use of hand sanitizers, maintaining social distance, and reducing social contact to slow down the fast spread of virus. Additionally, case detection, contact tracing, and quarantines and other community level measures are recommended actions to reduce wide spread COVID-19.2,5
Global surveillance system established by WHO with partners in January, 2020 contributed much in gathering standardized data at global, regional and country levels.6 It is also stated that the challenges to respond to COVID-19 in detentions like prisons requires collaborative actions of government and the whole society. This is because people in prisons are already affected of their freedom and may respond differently to further restrictive measures imposed upon them.7 WHO in its interim guideline recommends that all staff and people in prisons and other places of detention should have comprehensive awareness of COVID-19 prevention strategies, including adherence to hand hygiene measures, respiratory etiquette (covering coughs and sneezes), physical distancing (maintaining a distance of at least one meter from others), being alert to signs and symptoms of COVID-19, and staying away from ill people.7 Furthermore, since all regions of the world are at risk to COVID-19, each country is encouraged to be ready to respond in line with the global Strategic Preparedness and Response Plan.8
Ethiopia set up a Ministerial Committee led by the Prime Minister on March 16, 2020, to control COVID-19; the committee announced postponement of large gatherings and meetings including sporting events, wedding and funeral ceremonies, limiting religious institutions and places of worship to limit gatherings and a total closure of all public and private schools including the higher learning. Moreover, the federal government adopted a COVID-19 control implementation regulation and declared state of emergency (SoE) in April, 2020 which was approved by the House of Peoples Representative (HoPR).9 As a result, public and private institutions installed hand washing stations. At work area each individual obligated to use face mask using slogan “NO MASK, NO SERVICE”. More importantly, some individuals developed the behavior of sanitizer use before and after any procedure.
Despite efforts made to improve awareness and practice towards COVID-19 prevention, several studies showed that there are gaps in the implementation of prevention measures. A study conducted in Cameroon demonstrated that 61% of participants reduced their practice of avoiding crowded areas, using facemasks, keeping hand hygiene, using hand sanitizers and eating fruits.10 Similarly, study conducted in Malaysia reported that study participants have been avoiding crowded areas (83%), practiced proper hand hygiene (88%) and wearing of face masks (51%).11 Another study conducted in Pakistan revealed that study respondents wash hands frequently (85%), wash hands before eating (60%), wash hands after coming home (93%), cover their face when sneezing or coughing (50%), and practiced maintaining a safe physical distance (93%).12 Practice related evidence from Bangladesh also showed that 55% of participants increased hand hygiene, while 98% of them wore a face mask in crowded places, 99% of them agreed to inform a suspected case to health authorities, and 94% of them implemented washing hands with soap and water.13 As to Ethiopia, evidence showed that COVID-19 prevention practice was 16% in Gondar, 62% in Amhara regional online study, 49% in Addis Ababa online study, 41% among Dire Dawa residents, 42% among residents in Dessie.14–18
There is no study done on disease prevention practice among prisoners nationally in general and regional in particular. Thus, we aimed to measure the level of prevention practice and associated factors towards COVID 19 among prisoners in Sidama National Regional State, Ethiopia.
Methods
Study Design and Area
We conducted a cross-sectional study survey in November, 2020 in two Prisons (Yirgalem and Hawassa) of Sidama Region, Southern Ethiopia.
Sample Size and Sampling Procedure
A sample size formula to estimate a single population proportion was used to calculate sample size. After adding 10% of non-response rate on 384, the final sample size became 420.
Two major prisons (Yirgalem and Hawassa) were included purposively and study participants were selected randomly using prisoners register as a sampling frame.
Data Collection Tool and Procedure
Data was collected using structured questionnaire developed based on the review of the literature including WHO’s directives.4,5,7,11,12,16 The questionnaire sections on socio-demographic, behavioral including attitude and other features of the participants, and COVID-19 prevention measures practice. It was initially designed in English and then translated to local language (Sidamu Afoo and Amharic) and back to English to check the consistency. We checked the reliability of questionnaire related to attitude and practice using Cronbach’s Alpha test and values were 0.844 and 0.652 respectively. In addition it was also checked for its validity using Pearson’s correlation test and all items were significant. This value for each item was greater than critical value at 0.05. Finally, data were collected by four trained nurses using pretested and validated questioners and supervised by two trained supervisors. During data collection, the WHO’s recommendations to prevent COVID-19 (social distance and the use of personal protective equipment) was strictly implemented. To check consistency and accuracy of the collected data it was checked on daily basis.
Measurement and Operational Definition
The outcome variable was practice of COVID-19 Prevention measures (Good /Poor practice) which was measured using seven questions with dichotomous options (0=No, 1=Yes). Then, those participants who scored 3 and less of the seven were regarded as having poor practice of COVID-19 prevention measures, and those who scored 4 and more were considered as they have good practice.
The independent variable included were socio-demographic variables (age, sex, education, religion and marital status) and behavior factors such as history of alcohol consumption, history of chronic illness and attitude towards COVID-19.19 Three dichotomous questions (Yes/No) were used to assess the attitude of the respondents towards COVID-19. Each question given 0 and 1(0 =No and 1 = Yes). Then, those participants who agreed that COVID-19 is fatal, he/she is at risk of it and each individual should use prevention measure were considered as they had positive attitude and those disagree any one of these were considered as they had negative attitude.
Data Processing and Analyzing
After data entered in to Epi Data entry software, cleaning and analyzing was done using statistical package for the social sciences (SPSS) version 24. Statistical Parameters like frequency, proportion, mean, and standard deviation were computed to describe the socio-demographic and other characteristics of study participants. The multivariable logistic regression model was used to assess the factors associated with poor practice towards COVID-19 prevention measures. The variables under bivariable analysis with P-value < 0.25 were entered in multivariable logistic regression to control confounders and to identify predictors of COVID-19 prevention practice.19 Hosmer and Lemeshow’s goodness-of-fit was used to assess whether they fulfilled the assumption. Adjusted Odds Ratio (AOR) with 95% confidence interval (CI) at P-value <0.05 was used to report the predictors of COVID-19 prevention practices.
Result
Socio-Demographic Characteristics of the Respondents
Out of 422 study participants, 420 (99%) participated in the study and from which 403 (96%) were male. Regarding the ages of the participants, 324 (77%) was in the age group of 19–45 years old. Two hundred sixty-six (63%) participants can read and write while 27 (6%) had attended College and above. Regarding the religion and marital status of the study participants, 303 (72%) and 246 (58%) were protestant and married respectively (Table 1).
 |
Table 1 Socio-Demographic Characteristics of the Respondents, in Prison, Sidama, Ethiopia, November, 2020 |
Attitude Towards COVID-19 and Chronic Health Characteristics of the Respondents
From the total of 420 study participants, 57 (14%) had history of chronic illness. Three respondents reported having more than one chronic illness. The common chronic illness among the study participants was hypertension, 25 (6%). They were also asked for the history of alcohol drink and 122 (29%) had history of drinking alcohol and the remaining 298 (71%) had no history of drinking alcohol. Participants were assessed for how they perceive the COVID-19 and 165 (39%) responded had negative attitude.
Prevention Practice Towards COVID 19 Among the Respondents
From the all participants, 191 (45%), 106 (25%), 34 (8%), 9 (2%) reported as they wash their hands frequently, use face mask always, use disinfectants frequently and keep one meter of social distance respectively as to prevent COVID-19 infection in prison (Table 2).
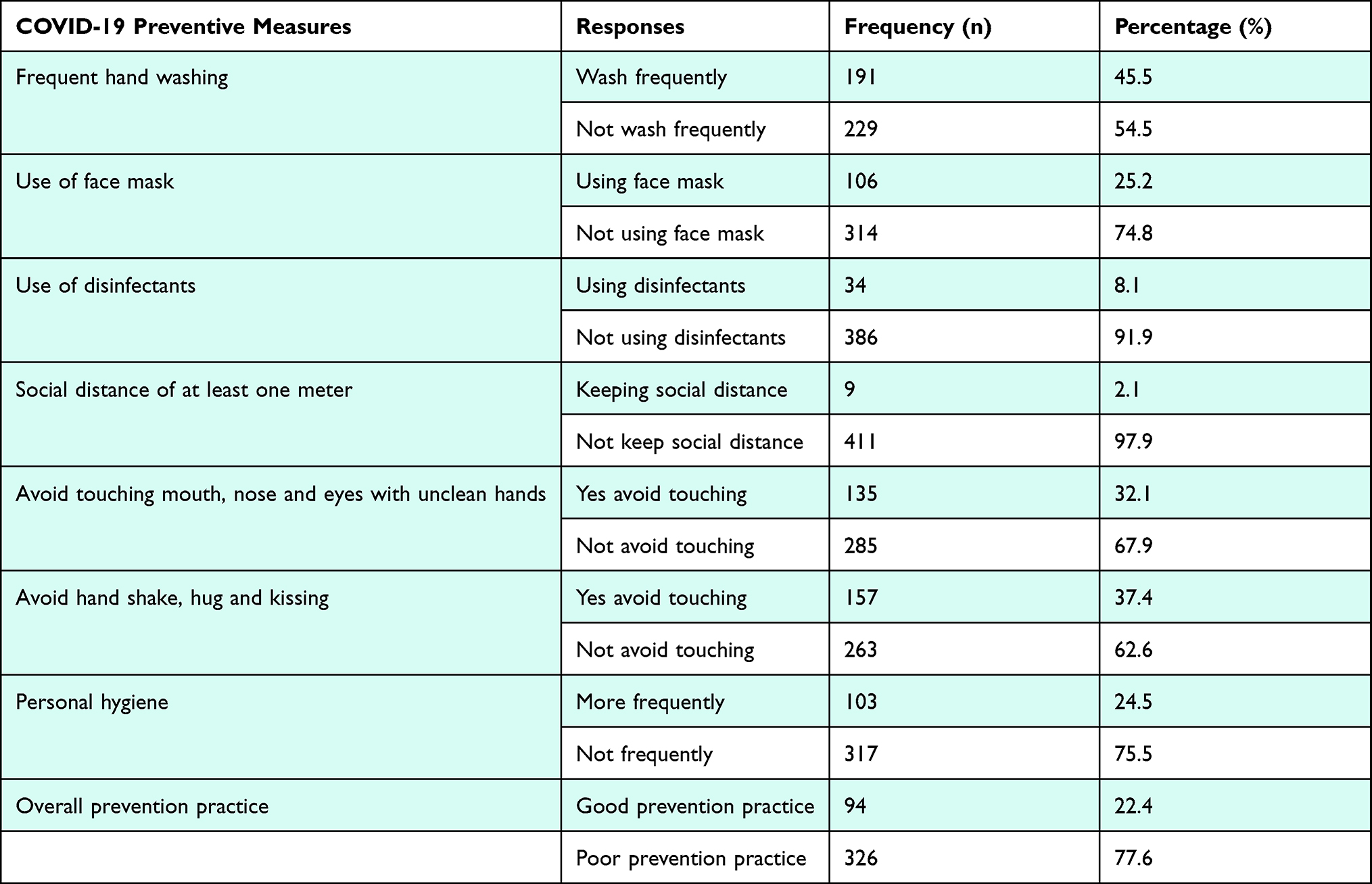 |
Table 2 Prevention Practice of Respondents to COVID-19 Prevention Measures, in Prison, Sidama, Ethiopia, November, 2020 |
Among all participants, while 326 (78%; 95% CI: 74%, 81%) participants had poor preventive practice to wards COVID-19, the 94 (22%; 95% CI: 19%, 26%) had good preventive practice.
Factors Associated with the COVID-19 Prevention Practices
Under binary logistic regression analysis; age, sex, marital status, attitude towards COVID-19, and history of alcohol intake of the participant were associated with prevention practice of the participants towards the infection.
In multivariable logistic regression analysis, history of alcohol taking (AOR= 1.79; 95% CI: 1.09, 2.93) and negative attitude (AOR= 1.69; 95% CI: 1.02, 2.81) towards COVID-19 were significantly associated with prevention practice of the respondents. However, all socio-demographic variables did not associated with COVID-19 prevention practices among the study participants (Table 3).
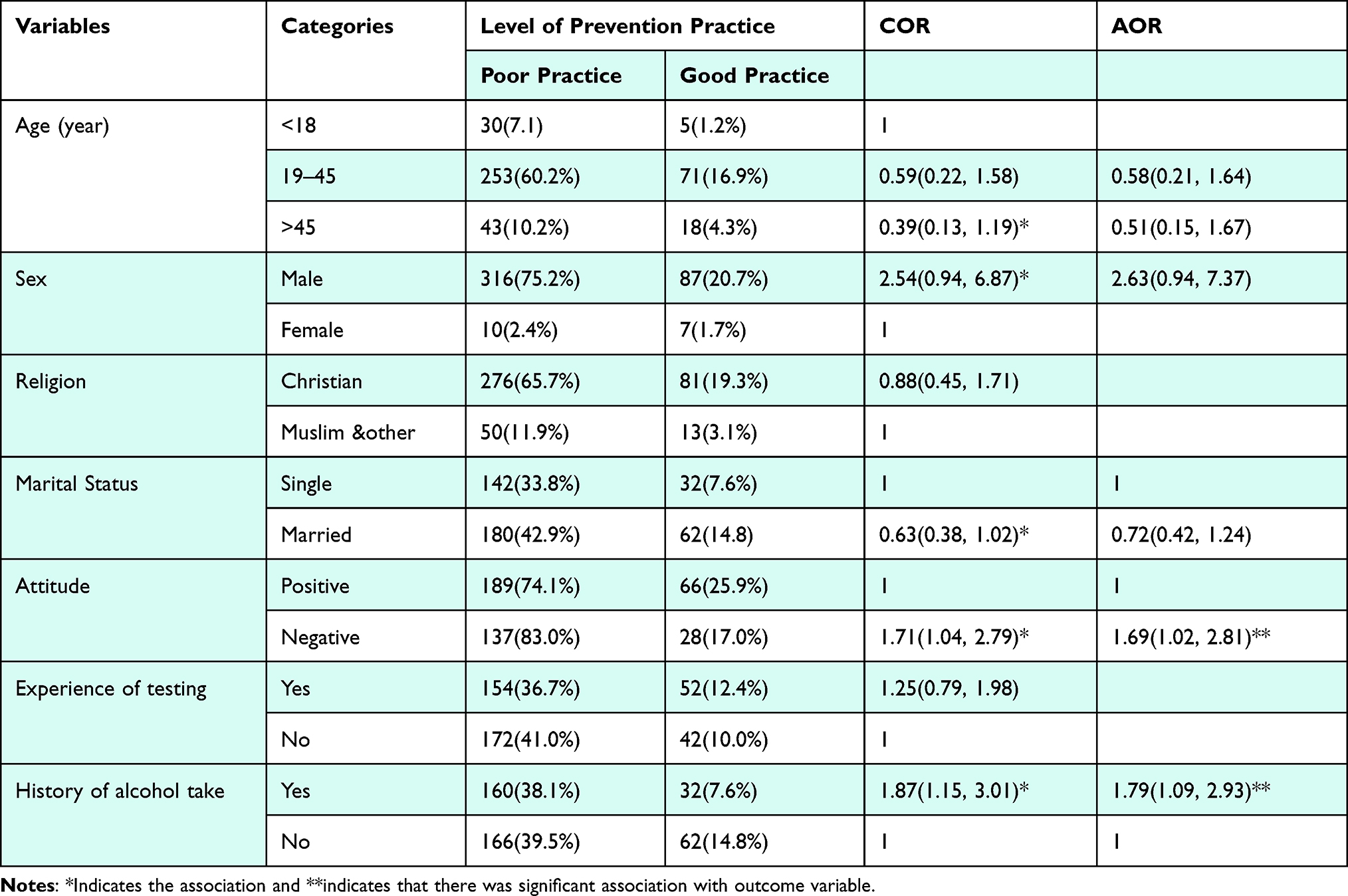 |
Table 3 Factors Associated with Prevention Practice Towards COVID 19 in Prison, Sidama Regional State, Ethiopia, November, 2020 |
Discussion
The prevalence of poor practice among respondents towards COVID-19 was found to be 78% (95% CI: 74%, 81%). This result was similar with findings of the study conducted among the residents of the southern region of the country.20 Similarly, it was in line with the findings of the study conducted in Gondar town (74%).14 More importantly, this finding is in support with statement of the WHO that inmates have poorer hygiene and weak immunity due to stress and poorer nutrition.21 Most prisoners are gathered from general populations which possibly justify the similarity of the study results. On the other hand, this finding was higher compared to the findings of the prevention practice related studies in Cameron (39%), Malaysia (26%), in Dessie (42%) in Addis Ababa (49%).10,11,16,18 The possible explanation for this could be study settings, current study conducted in Prison where the fully implementation of COVID-19 prevention measures likely difficult due to setting and the behavior of the prisoners. Our study indicated that only 22% of the study participants had practiced COVID-19 prevention measures correctly and consistently. In addition it was evidenced that the response to COVID-19 in such places like prison is challenging and requires whole-government-societal approach.7 Furthermore, healthcare service existing in prisons needs to be strengthening so that health education and counseling focused service could change the negative attitude and behavior of the prisoners.
This study reveals that the participant’s history of alcohol intake and their negative attitude towards COVID-19 was significantly associated with prevention practice of the respondents. Comparing the participants who have positive attitude, the respondents who had negative attitude towards Covid-19 infection were 1.69 times more likely to have poor prevention practice, (AOR= 1.69; 95% CI; 1.02, 2.81). This finding was supported by the finding of study conducted in north-east Ethiopia (among Dessie residents).18 Similarly study conducted in Egypt supports this finding as people with positive attitude towards COVID-19 prevention measures limits the spread of disease through good practice of its prevention measures.22 Another similar study conducted in Dire-Dawa (a city east of Addis Ababa) concluded that respondents with positive attitude towards COVID-19 prevention were 3.87 times more likely to practice COVID-19 prevention measures compared to their counterparts.17 Furthermore, study conducted in Bangladesh reveals those respondents with positive attitude were 1.4 times more likely to implement prevention practice than their counterparts.13 Therefore, the healthcare professionals and other concerned body of the prison should work to change the attitude of the prisoners.
In this study the respondents who had history of alcohol intake 1.79 times less likely implement the COVID-19 prevention practice correctly and consistently, (AOR=1.79 (1.09, 2.94). This result was similar with findings of the study conducted among Dire-Dawa residents.17 Additionally, this finding is in line with WHO statement that Alcohol alters one’s thoughts, judgment, decision-making and behavior. However, being cross-sectional nature of the study might affect the establishment of causal relationship of poor prevention practice and its associated factors.
Conclusion
In this Study, nearly three fourth of the participants had poor practice towards COVID-19 prevention measures. Negative attitude of the participant towards COVID-19 and participants’ previous history of alcohol intake were predicting factors for poor practice of COVID-19 prevention measures.
The researchers recommend to the government, nongovernment organization and other concerned body to design educational intervention to change the attitude towards COVID-19 disease and behaviors of the prisoners.
Abbreviations
AOR, adjusted odds ratio; CoM, Council of Ministers; COR, crude odds ratio; COVID-19, corona virus disease 19; IRB, Institutional Review Board; PHEIC, Public Health Emergency international Concern; PPE, personal protective equipment; SNNPRS, Southern Nation Nationalities Peoples Regional State; WHO, World Health Organization.
Data Sharing Statement
Data is not available for online access, however readers who wish to gain access to the data can write to the corresponding author Nana Chea at [email protected].
Ethical Approval and Informed Consent
Ethical clearance was obtained from Hawassa University College of Medicine and Health Science, Institutional Review Board (IRB) and supportive letter were obtained from the Sidama Regional Health Bureau and Sidama Region police Commission Department and participating prison administrators. All participants were informed about the purpose, risks, benefit and confidentiality issues related to the study. Informed consent was directly obtained from study participants after they were briefed about the objectives of the study. Participation in the study was on voluntary bases and informed about the right not to participate or withdraw at any time without compromising COVID-19 prevention rules. This indicates that our study complies with the Declaration of Helsinki.23
Acknowledgment
Firstly, our thanks goes to Hawassa University, Office of the Vice President for Research and Technology Transfer Research Programs Directorate, Police commission of the region and prison administrators for their support and providing necessary information. Moreover, we extend our thanks for the prisoners for the voluntarily participation in this study.
Author Contributions
All Authors made a significant contribution to the study work, reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article. They have agreed on the journal to which the article has been submitted, and have agreed to be accountable for all aspect of work.
Funding
Hawassa University.
Disclosure
The authors declare that they have no competing interests.
References
1. Culp WC. Coronavirus disease 2019: in-home isolation room construction. A&A Pract. 2020;14(6):e01218. doi:10.1213/XAA.0000000000001218
2. FMOH E. Covid19 management handbook, First edition. FMOH; April 2020:7–9. Available from: https://www.worldometers.info/coronavirus/?%3D%3D.
3. COVID Live - Coronavirus Statistics - Worldometer. htts://www.worldometers.info/coronavirus/. Accessed March 17, 2022
4. UNICEF. Situation in numbers cases 269 in critical condition Highlights Government announces the official re-opening of School starting from October 2020; 2020:1–10.
5. World Health Organization. Safe Ramadan practices in the context of the COVID-19: interim guidance. 2020:1–3. Available from: https://apps.who.int/iris/bitstream/handle/10665/331767/WHO-2019-nCoV-Ramadan-2020.1-eng.pdf?sequence=1&isAllowed=y.
6. World Health Organization. Who’s response to Covid-19. 2021.
7. World Health Organization. Preparedness, prevention and control of COVID-19 in prisons and other places of detention. Interim Guid World Heal Organ. 2020;2020. doi:10.13140/RG.2.2.26206.18245
8. World Health Organization. COVID-19 STRATEGIC PREPAREDNESS AND RESPONSE PLAN Country Preparedness and Response Status for COVID-19 Country Preparedness and Response Status for COVID-19. Geneva: World Health Organization. 2020:19–21.
9. Administrative F, Proclamation P. Federal Negarit Newspaper. Federal Negarit Gazette. 2020:35.
10. Ngwewondo A, Nkengazong L, Ambe LA, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. 2020;14:1–15. doi:10.1371/journal.pntd.0008700
11. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):1–15. doi:10.1371/journal.pone.0233668
12. Fatmi Z, Mahmood S, Hameed W, et al. Knowledge, attitudes and practices towards covid-19 among Pakistani residents: information access and low literacy vulnerabilities. East Mediterr Heal J. 2020;26(12):1446–1455. doi:10.26719/emhj.20.133
13. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15:1–17. doi:10.1371/journal.pone.0239254
14. Asmelash D, Fasil A, Tegegne Y, Akalu TY, Ferede HA, Aynalem GL. Knowledge, attitudes and practices toward prevention and early detection of COVID-19 and associated factors among religious clerics and traditional healers in Gondar town, northwest Ethiopia: a community-based study. Risk Manag Healthc Policy. 2020;13:2239–2250. doi:10.2147/RMHP.S277846
15. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48(1). doi:10.1186/s41182-020-00254-3
16. Defar A, Molla G, Abdella S, et al. Knowledge, practice and associated factors towards the prevention of COVID-19 among high-risk groups: a cross-sectional study in Addis Ababa, Ethiopia. medRxiv. 2020. doi:10.1101/2020.08.14.20172429
17. Amsalu B, Guta A, Seyoum Z, et al. Practice of COVID-19 prevention measures and associated factors among residents of Dire DAWA city, Eastern Ethiopia: community-based study. J Multidiscip Healthc. 2021;14:219–228. doi:10.2147/JMDH.S292409
18. Muluneh Kassa A, Gebre Bogale G, Mekonen AM. Level of perceived attitude and practice and associated factors towards the prevention of the COVID-19 epidemic among residents of Dessie and Kombolcha Town administrations: a population-based survey. Res Rep Trop Med. 2020;11:129–139. doi:10.2147/rrtm.s283043
19. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:1–8. doi:10.1186/1751-0473-3-17
20. Mola S, Aweke Z, Jemal B, et al. Magnitude and associated factors for attitude and practice of Southern Ethiopian residents toward COVID-19 and its preventions: a community based cross sectional study. 2020:1–14. doi:10.21203/rs.3.rs-36120/v1
21. Yordi Aguirre I, Ahalt C, Atabay T, et al. Prisons and health prisons and health. 2014:1–189. Available from: https://apps.who.int/iris/bitstream/handle/10665/128603/PrisonandHealth.pdf;jsessionid=9D8EB2F358676D0942F6EA53A5307F94?sequence=1.
22. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;45(5):881–890. doi:10.1007/s10900-020-00827-7
23. World Medical Association. Declaration of Helsinki, Ethical Principles for scientific requirements and research protocols. Bull World Health Organ. 2013;79(4):373.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.