Back to Journals » Risk Management and Healthcare Policy » Volume 14
COVID-19 Knowledge, Attitude, Practices and Their Associated Factors Among Dessie City Residents, Northeast Ethiopia: A Cross-Sectional Study
Authors Alemu T ![]() , Amare S, Legesse S
, Amare S, Legesse S ![]() , Abera A, Ayalew M
, Abera A, Ayalew M ![]() , Bezabih B
, Bezabih B
Received 19 October 2020
Accepted for publication 17 December 2020
Published 4 February 2021 Volume 2021:14 Pages 439—451
DOI https://doi.org/10.2147/RMHP.S287600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Tefera Alemu,1 Semagn Amare,2,* Seid Legesse,2,* Abtew Abera,2,* Misganaw Ayalew,2,3,* Belay Bezabih2,4,*
1Amhara Public Health Institute, Public Health Emergency Management Directorate, Bahir Dar, Ethiopia; 2Amhara Public Health Institute Dessie Branch, Dessie, Ethiopia; 3ICAP Ethiopia, Bahir Dar Regional Office, Bahir Dar, Ethiopia; 4The World Health Organization (WHO), Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Tefera Alemu
Amhara Public Health Institute, P.O. Box 47764, Bahir Dar, Ethiopia
Tel +251 911598660
Email [email protected]
Background: Sufficient knowledge and favorable attitude are among the key determinants for people’s adherence to coronavirus disease (COVID-19) precaution measures. Hence, this study assessed Dessie city resident’s knowledge, attitude, and practice on COVID-19.
Methods: We used a facility-based cross-sectional study among 424 Dessie city residents from 17 to 21/05/2020. We dichotomized knowledge, attitude and practice scores based on the mean value. We entered the data into EpiData manager software 4.2 and exported to SPSS-20 for data analysis. We run three independent logistic regression analyses to determine factors associated with sufficient knowledge, a favorable attitude, and adequate practice. We defined significant association at a p-value of < 0.05.
Results: Among 424 participants, 92.7% have sufficient knowledge about COVID-19, while 96% have a favorable attitude to prevent and control the pandemic. However, the practice was adequate only in 44.6% of the participants. Increasing educational status (AOR: 6.5, 95% CI: 2– 21.4), availability of television (AOR: 3.8, 95% CI: 1.4– 10.5), having a telephone (AOR: 3.4, 95% CI: 1.3– 9.1) and radio (AOR: 4.2, 95% CI: 1.1– 15.5) are the factors associated with sufficient knowledge, while sufficient knowledge (AOR: 5.4, 95% CI: 1.7– 17.2), is the only predictor identified for favorable attitude. Similarly, being a farmer (AOR: 0.14, 95% CI: 0.047– 0.4), availability of telephone (AOR: 3.1, 95% CI: 1.2– 8.2), and sufficient knowledge (AOR: 15.2, 95% CI: 1.9– 118) are the predictors of adequate practice.
Conclusion: In the study area, the participant’s knowledge and attitude are found to be sufficient to halt coronavirus transmission. However, practice in the vast majority is not adequate to stop coronavirus transmission. Educational status, television, telephone, radio, occupation and knowledge are the significant factors for successful prevention and control of coronavirus. Despite escalating public knowledge, our finding suggests the government to follow some compulsory regulations for uniform implementation of preventive measures.
Keywords: attitude, COVID-19, knowledge, practice, Dessie city
Background
Coronavirus disease 2019 (COVID-19) is a respiratory tract infection caused by a newly discovered coronavirus, that was first recognized in Wuhan city, China, in December 2019. Its mode of transmission is through respiratory droplets, direct contact and feco-oral.1 So far, it has no proven antiviral to cure it, nor effective vaccine to prevent it.2 Since its first detection in China, the World Health Organization has been advising several preventive measures to curve the spread of the disease. These are, but not limited to, frequent hand-washing with soap, movement restrictions, keeping physical distancing, avoiding mass gatherings, utilization of personal protective equipment’s, alcohol-based sanitizers, case identification and contact tracing.3 Following these, an extraordinary measure has been taken by the government of Ethiopia to prevent the entrance of the disease. Community mobilization, public awareness creation and education campaigns have been central to the government’s effort.4 Despite this effort, the country has detected and notified its first COVID-19 case on 13th March 2020,5 reaching 112,740 cases and 1745 deaths as of December 6/2020.6 Since then, the government further strengthened its prevention and control strategies to halt the spread of the disease in the country. Among the essential strategies implemented are declaration of a state of emergency on April 8/2020, which contains compulsory components on COVID-19 precaution measures, strict regimen of rigorous contact tracing, isolation, compulsory quarantine, and treatment, concreted media campaign, strict passenger screening, house to house screening, scaling up diagnostic tests and treatment centers and local resource mobilization.
However, the success of such preventive and control measures is reliant on people’s adherence to it, which is affected by their knowledge and attitudes towards the disease. Therefore, it is better to assess individual’s knowledge, attitude and their practice on COVID-19, which enables to identify where the gap is and to take remedial actions, based on the identified gaps. Thus, to the best knowledge of the investigators, no published evidence assessed the knowledge, attitude and practices of urban residents through face-to-face interviews in the Amhara region, particularly in the study area. Previous studies conducted in the country have failed to assess the practices of COVID-19 preventive measures through an observational approach. Therefore, we assessed Dessie city resident’s knowledge, attitude and their practice on COVID-19. The result is important for public health authorities to redirect their anti-corona efforts towards the identified gaps. It also serves as an evaluation study of the existing community-based awareness creation campaigns.
Methods
Study Design and Period
We conducted a facility-based cross-sectional study from May 17–21/2020.
Study Setting and Population
We conducted the study in Dessie city administration health facilities, which is found in the northeast part of the country. It is 401 kilometers far from the capital city of Ethiopia, Addis Ababa. The city is divided into 5 sub-cities with 18 urban and 8 rural kebeles. According to the 2007 Central Statistical Agency report, the city has an estimated total population of 273,305 in 2019/20, of which 49.5% are men. There are 8 health centers, 8 health posts, 2 government hospitals, 3 private hospitals, 38 private clinics, 55 private drug stores, 4 private diagnostic laboratories. Besides, there are two governmental COVID-19 testing laboratories in the city, namely the Amhara Public Health Institute Dessie Branch and Wollo University laboratory center.
All Dessie city residents aged 18 years or more were the source populations. We included all individuals ≥18 years that come to the health facilities in the study period as study subjects. We excluded critically ill and health professionals from the study.
Sample Size and Sampling Technique
We determined the sample size using a single population proportion formula, by considering the following assumptions: 5% margin of error, 95% confidence level, and a prevalence of 50%, considering that it is not known previously. After adding a 10% non-response rate, we got a final sample size of 424 individuals who come from the community. Study participants who visited the selected health facilities in the study period for any reason were taken consecutively until we attained the final sample size.
Data Collection
We collected data through face-to-face interviews using pretested and a structured questionnaire (Supplementary Material 1). The questionnaire is first prepared in English language and then translated to Amharic version, which is the resident’s mother tongue and the national working language. We developed the questionnaire from different works of literature and the World Health Organization resources. The questionnaire addressed information on socio-demographic characteristics, knowledge, attitude and practice towards COVID-19. We assessed practice objectively using some observation items. We collected observational data after we prepared a handwashing facility for clients at the health facility entry site. We observed participants’ physical distancing and face mask utilization in their stay in the facility. Eight health professionals took part as a data collector.
Data Quality Assurance
Before the actual data collection period, we conducted pretesting of the questionnaire on 22 individuals and we made necessary modification before applying to the study participants and we excluded those who pretested from the actual study. Training was given for data collectors to enable them to have a common understanding of the objectives of the study and each of the questions in the questionnaire. The principal investigator did daily supervision. Four supervisors supervised the data collection process. We validated the questionnaire, and Cronbach’s alpha was estimated to assess the reliability of the questionnaire. We find the internal consistency estimate to be in the acceptable range.
Data Analysis
We entered data into EpiData manager version 4.2 and exported to SPSS 20 for data analysis. Before data analysis, we have done reverse scoring for negatively worded questions. We computed descriptive statistics to describe the data. We conducted logistic regression analyses to identify factors associated with knowledge, attitude, and practice on COVID-19. We defined a statistically significant association at a P-value of less than 0.05. We entered a variable with a P-value of ≤0.2 in the bivariate analysis into the multivariate logistic analysis. Finally, we used a backward stepwise regression method. Adjusted odds ratios with 95% confidence interval were computed to observe the strength of association between the dependent and independent variables.
Operational Definition
Sufficient Knowledge
Eighteen questions were used to measure the participant’s knowledge about COVID-19 and a score greater than the mean was considered sufficient. To compute the mean score, participants who answered “Yes” were considered as correct responses and we categorized those “No” and “I do not know” responses as incorrect responses.
Favorable Attitude
We measured attitude using 12 items, each graded as agree, disagree, and I do not know. Then, we dichotomize it into two categories. Finally, participants who positively reacted to at least seven questions were classified as having a favorable attitude. To calculate the mean score, participants who answered “agree/yes” were considered as correct responses while those who answered “disagree/no” and “I do not know” were taken as incorrect response.
Adequate Practice
We asked twelve questions about COVID-19 preventive measures and participants who scored above the mean were taken as having adequate practice.
Results
Socio-Demographic Characteristics of Participants
A total of 424 residents were interviewed. Their age ranges from 18 up to 90 years. The mean age was 34.4 (±13.4 SD) and 45.3% of them are in between 18–29 years. The proportions of female participants were 52.6%. Most participants are married (69.8%) and Muslims (61.8%) in religion. Seventy percent of them have a television in their house and 42.9% are social media users. Further socio-demographic information is available in Table 1.
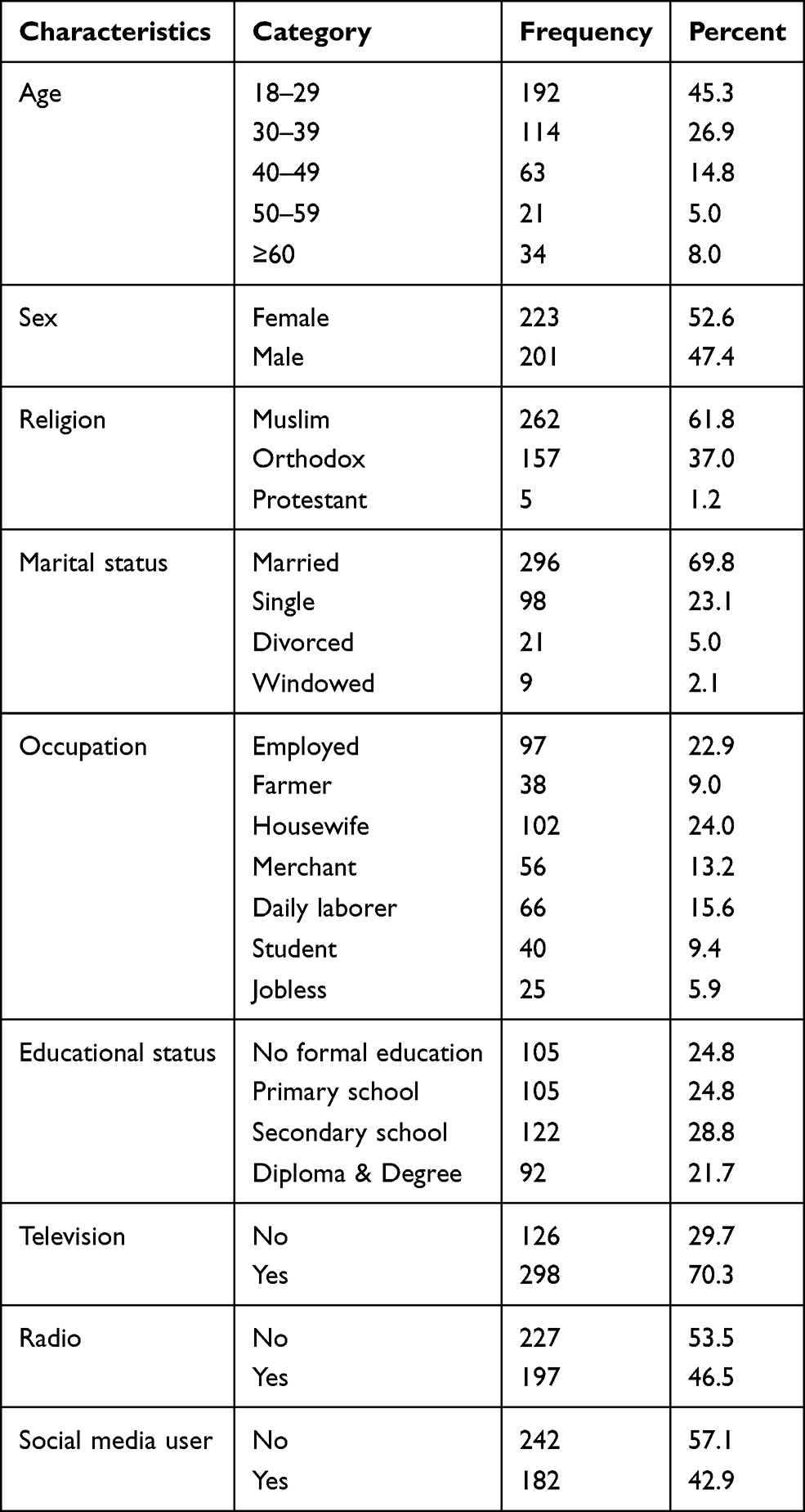 |
Table 1 Socio-Demographic Characteristics of Participants in Dessie City, Northeast Ethiopia (N=424) |
Knowledge About COVID-19
All participants have heard about the pandemic and 96% of them correctly mentioned its name. Even though the participants have got information from different sources, the most cited ones were television (79%), radio (37%) and social media/facebook (31.6%).
Regarding participant’s knowledge about COVID-19 symptoms, 78.8% mentioned fever while 68.9% and 23.6% told us dry cough and shortness of breathing, respectively. The most commonly listed modes of transmission were direct contacts like handshaking (94.3%), respiratory droplets (52.1%) and indirect contacts to contaminated inanimate objects (33.3%). Airborne way of transmission is also mentioned by 37.7% of the participants. The most frequently mentioned preventive measures were frequent hand washing (89.6%), physical distancing (82.8%), avoiding handshaking (54.7%), staying at home (44.6%) and face mask utilization (42.7%).
Eighty-seven percent of the participants mentioned that all age groups and both sexes are at risk of getting infected with the virus. Besides, the elderly (72.4%) and people with chronic diseases (60.6%) were specified as the most vulnerable groups to become severely ill or die. Concerning the activities following a single COVID-19 case detection, 97.6% mentioned isolation and treatment of the case, while 36.6% mentioned contact tracing and quarantining.
Out of eighteen knowledge items, participants score ranges from a minimum of 4 to a maximum of 18 knowledge scores, with a mean value of 13.96 ±2.6 SD. Half of the study participants have a knowledge score that lies in the 4th quartile, while 41% in the 3rd quartile (Table 2).
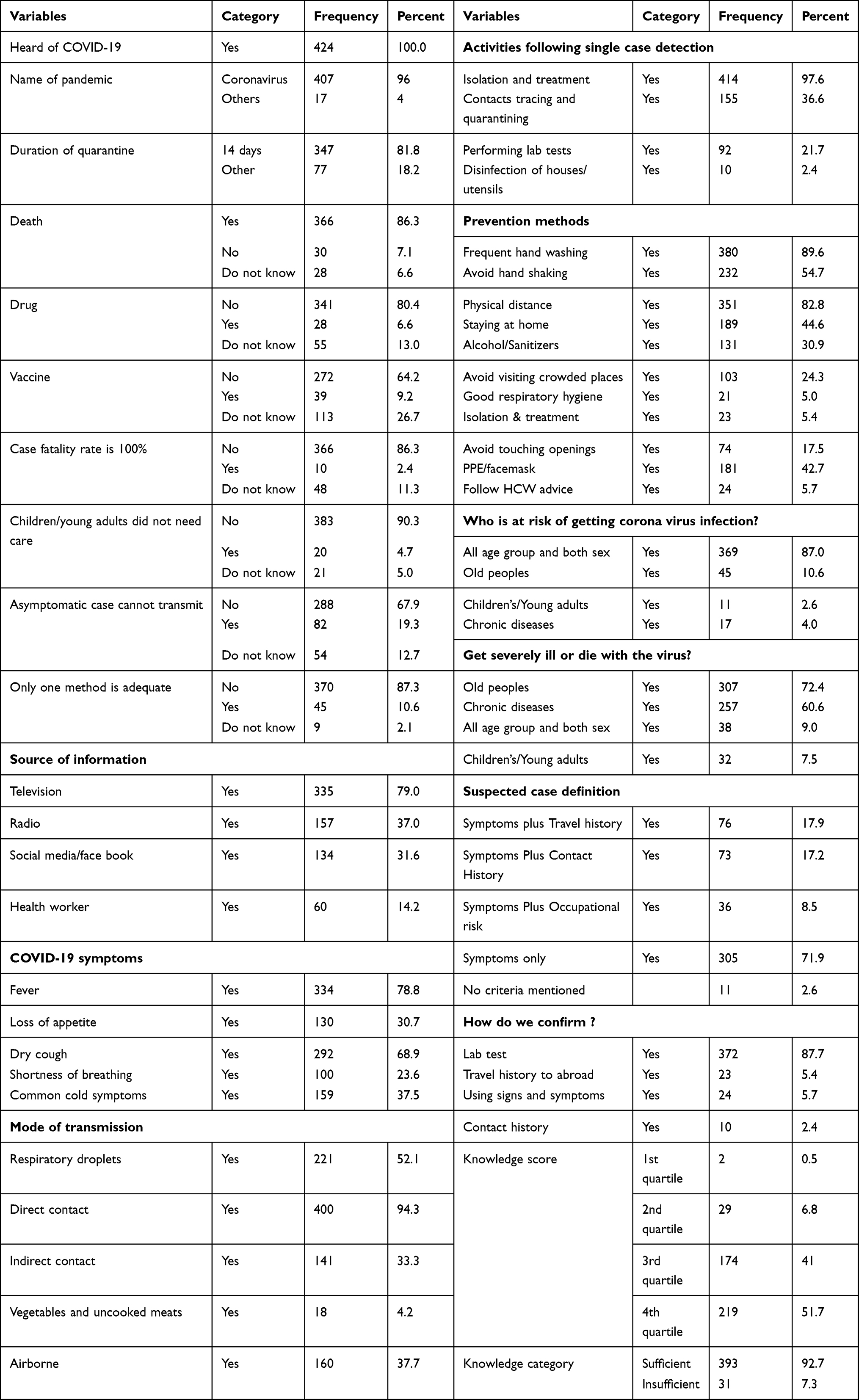 |
Table 2 Knowledge Items Mentioned by Participants About COVID-19 in Dessie City, Northeast Ethiopia (N=424) |
Attitude Towards COVID-19
We assessed the participant’s attitude using 12 questions. The mean attitude score was 10.8 (±1.8 SD), ranging from 2 up to 12 scores. Most participants (82.8%) score lie in the 4th quartile and 54% answered all the questions positively. Regarding specific attitude items, 91% agreed that the disease can infect African ethnic origins as well, while the remaining 5.7% believe that the disease cannot attack Ethiopians. In line with this, 12.3% of our participants also agreed on the issue that preventive measures are not important for Ethiopians. Besides, 22.2% of the participants agreed on the idea that cultural medications can prevent and/or cure coronavirus. Eighty-three percent of the participants advise their family members about coronavirus, and the same proportion of participants are ready to notify suspected COVID-19 cases to the nearby local authorities. Nine in ten participants (90.6%) have a firm commitment to purchase coronavirus prevention supplies, even at a high cost. The proportion of participants that agrees on the importance of handwashing, physical distancing, staying at home and avoiding mass gatherings in preventing coronavirus infection ranges from 94.6 to 97.6%. Eighty-four percent of the participants believe that coronavirus infection is preventable (Table 3).
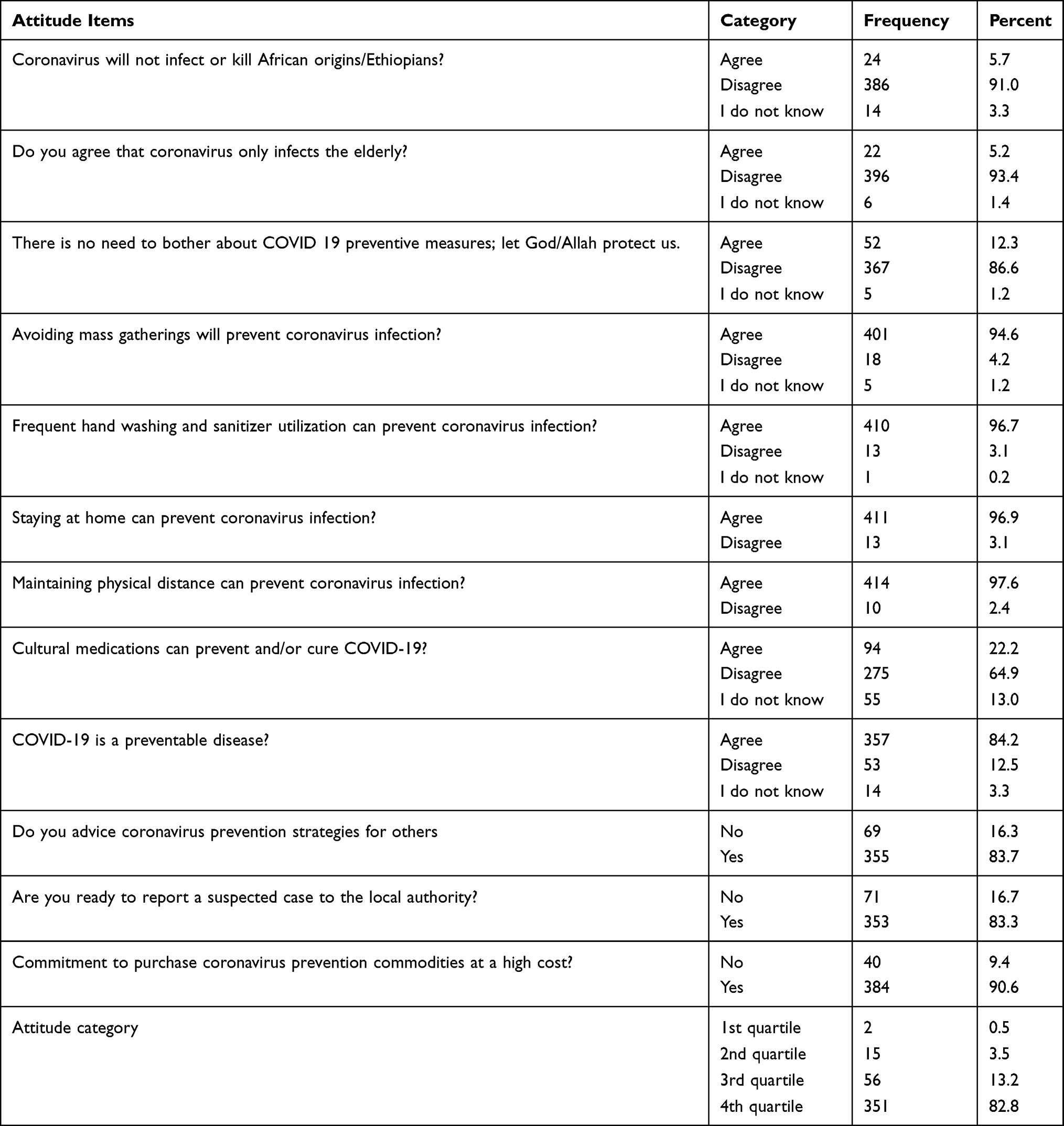 |
Table 3 Attitude of Participants Towards COVID-19 in Dessie City, Northeast Ethiopia (N=424) |
Practice on COVID-19 Preventive Measures
The proportion of participants who are washing their hands after touching any other objects was 87%. Meanwhile, 86.6% of the participants reported that their frequency of handwashing has increased with a minimum of two folds as compared to the era of no coronavirus infection. We found the estimated frequency of handwashing to be at least six times per day for 79.2% of the participants. Besides, 85.8% of the study participants were using soap at each handwashing events. Regarding direct contacts like handshaking, 93.2% of the participants have avoided it, while 79% avoided visiting crowded places. On the other hand, 34.7% were implementing staying at home as a prevention method and 89.4% are applying physical distancing strategy. Thirty-four percent of the participants reported that they are using face mask when leaving their home, but we observed that only 21% of the participants were using a facemask at the time of the interview. Similarly, forty-seven percent of our participants mentioned as if they have sanitizers in their home, while only 20% of them have sanitizers at hand during the time of interview. We observed that only 66.3% of the participants washed their hands at the entry to the health facilities. Of those, 95.4% have used soap to wash their hands, while 91.8% of them washed their hands appropriately. We observed that 72% of the participants have fully maintained their 2-meter physical distance in their stay to the health facility, while the rest 19.6% of the participants partially kept their physical distance in the facility.
Of the twelve practice items, we found the mean practice score to be 6.3 with ± 1.8 SD and ranging from 2 up to 11 scores. Most participants’ score falls in the 2nd (50.9%) and 3rd (38.9%) quartiles (Table 4).
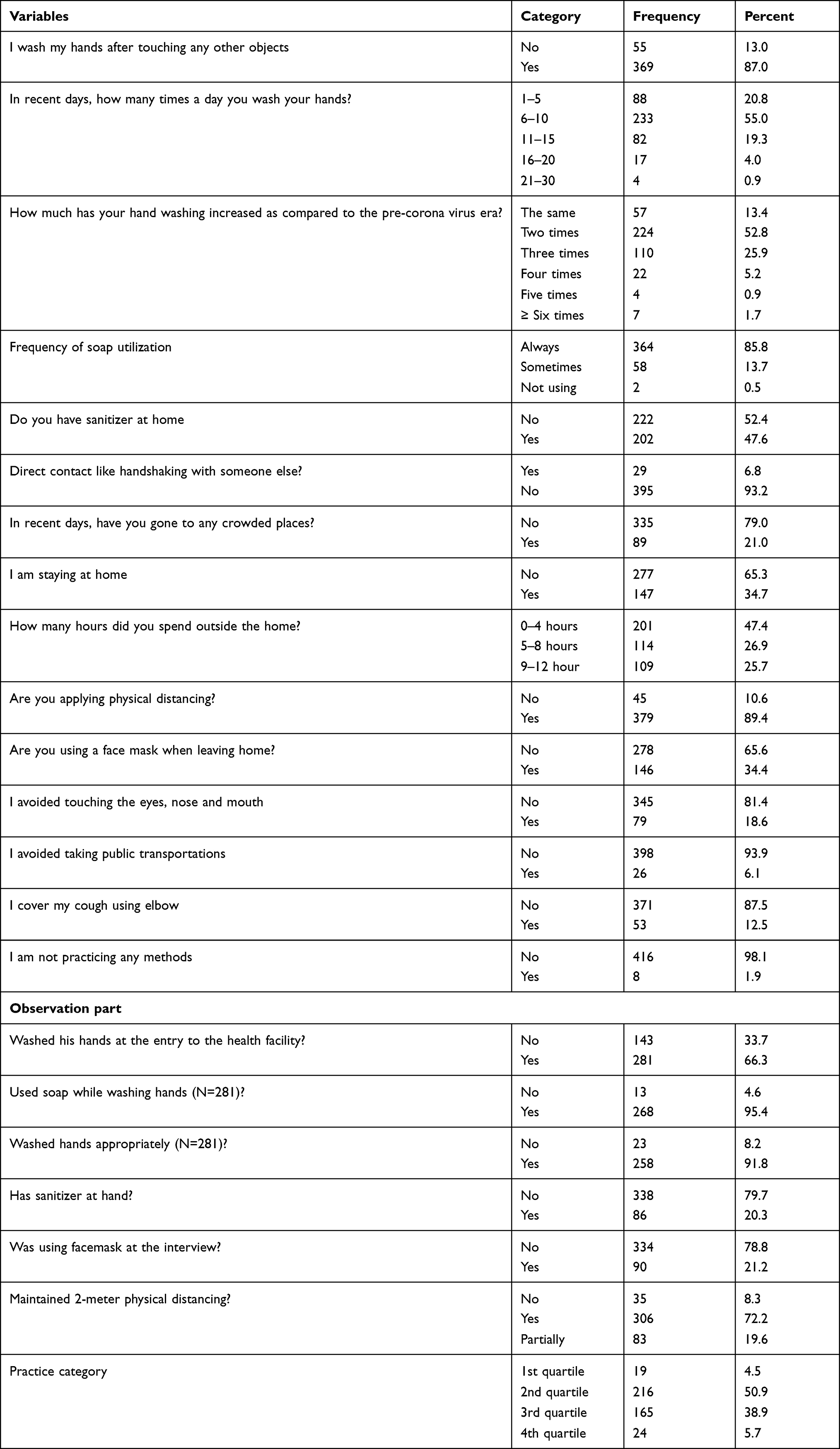 |
Table 4 Practice of Participants on COVID-19 Preventive Measures in Dessie City, Northeast Ethiopia (N=424) |
Factors Associated with Knowledge, Attitude and Practice
In the 1st regression model, participant’s religion, their educational status, occupation, availability of television, telephone, radio, their age category and social media utilization were found to be the predictors of sufficient knowledge about COVID-19 at a P-value of ≤0.2. However, in multivariate analysis, only participant’s educational status, availability of television, telephone and radio remains to be significant predictors of sufficient knowledge about COVID-19. Consequently, the odds of having sufficient knowledge are 6.5 times higher in participants with primary education as compared to participants without formal education (AOR: 6.5, 95% CI: 2.0–21.4). Likewise, participants who have a television in their house are 3.8 times more likely to have sufficient knowledge as compared to their counterparts (AOR: 3.8, 95% CI: 1.4–10.5). We also find the availability of personal telephone to increase participants’ knowledge with over three folds as compared to their counterparts (AOR: 3.4, 95% CI: 1.3–9.1). Similarly, participants who have a radio in their house are 4.2 times more likely to have sufficient knowledge about COVID-19 (AOR: 4.2, 95% CI: 1.1–15.5) (Table 5).
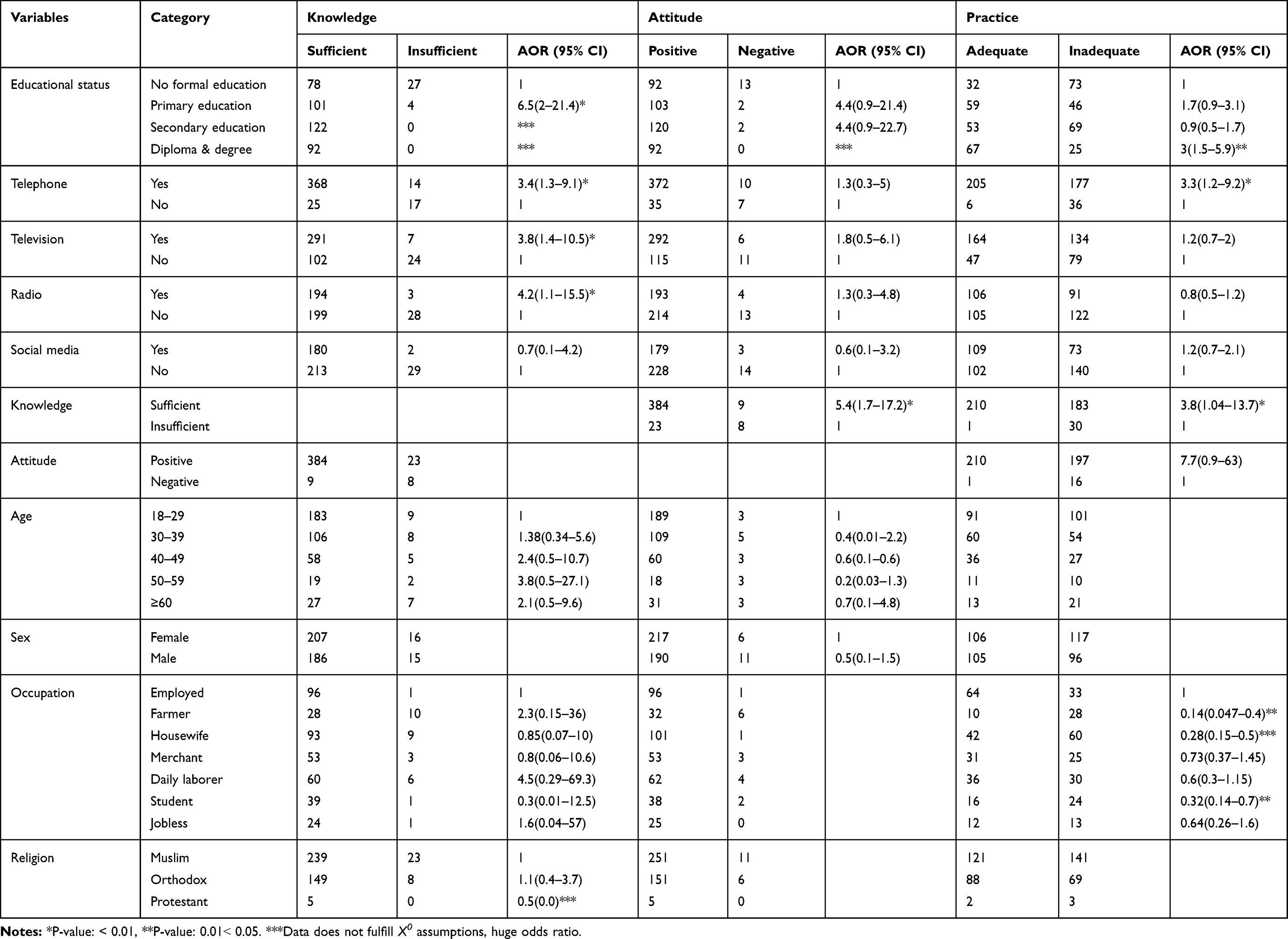 |
Table 5 Predictors of Sufficient Knowledge, a Favorable Attitude and Adequate Practice on COVID-19 in Dessie City, Northeast Ethiopia (N=424) |
In the 2nd regression model, participant’s educational status, their age category, television, telephone and radio availabilities, social media utilization and their knowledge status were found to be the predictors of a favorable attitude towards COVID-19 in bivariate analysis (P≤ 0.2). However, only the participant’s knowledge status remains significantly associated with a favorable attitude in the multivariate analysis model. Hence, participants who have sufficient knowledge about COVID-19 are 5.4 times more likely to have a favorable attitude towards COVID-19 prevention (AOR: 5.4, 95% CI: 1.7–17.2) (Table 5).
In the 3rd regression model, sex, religion, occupation, educational status, television, telephone, radio, social media utilization and knowledge status were the candidate variables (P-value ≤0.2) for multivariate regression. Thus, participants who have sufficient knowledge are nearly four times more likely to have adequate practice as compared to their counterparts (AOR: 3.8, 95% CI: 1.04–13.7). Similarly, participants who have personal telephone are three times more likely to implement COVID-19 preventive measures as compared to their counterparts (AOR: 3.3, 95% CI: 1.2–9.2). Conversely, farmer participants are seven times less likely to implement coronavirus prevention strategies as compared to an employed participants. Besides, housewife participants were 72% less likely to have adequate practice as compared to employed participants (AOR: 0.28, 95% CI: 0.15–0.5). Students are also 68% less likely to have adequate practice as compared to employed participants (AOR: 0.32, 95% CI: 0.14–0.7) (Table 5).
Discussion
Good knowledge and positive attitude towards an intervention or a new practice by a target group are among the key determinants for adoption. This study was interested in ascertaining the knowledge, attitude and practice of Dessie city residents on COVID-19. Therefore, when the participant’s knowledge was assessed, overwhelming majority (92.7%) showed having sufficient knowledge about COVID-19. This result shows that participant’s knowledge on COVID-19 is far broader than any time previously.7–11 and shows that coronavirus risk communication and awareness creation campaign across the country have made a positive impact on the public knowledge of the disease. This finding is much higher than other studies in the northern part of the country those reported 42.9% and 60.7% knowledgeable participants.12,13 The variation might be explained by the difference in the characteristics of study participants, change in the study period, inadequate access to COVID-19 information and different knowledge measurement tools used by researchers. Though our study reveals a high level of knowledge among participants, the knowledge varies from one coronavirus transmission and prevention method to another. For instance, the most popular prevention methods known by participants are frequent hand washing and physical distancing, which accounted for 89.6% and 82.8%, respectively. This is comparable with the finding from Addis Ababa city where 85% and 83% mentioned hand washing and social distancing as a COVID-19 prevention measures, respectively.7 Another online survey conducted in Ethiopia also documented a 90% prevention knowledge of maintaining social distance and frequent hand washing, which is in line with our finding.14 Avoiding handshaking is the third most popular prevention method cited by participants (54.7%), followed by staying at home (44.6%). In the meantime, the most commonly known mode of transmissions is direct contacts (94.3%), respiratory droplets (52.1%), airborne (37.7%), and indirect contacts (33.3%), which is also comparable with a previous study done in Addis Ababa.7 Furthermore, a good proportion of participants knew that being elderly (72.4%) and a concomitant chronic illness (60.6%) are among the poor prognostic factors. This result is higher than the finding from Kenya15 where 64% and 26% of the participants identified the elderly and peoples with weak immune systems as the most high-risk groups to develop severe illness. But our finding is comparable with the 66.6% and 56.6% study finding from northern Ethiopia.13 The study findings also revealed that television (79%), radio (37%) and social media (31.6%) are the major sources of COVID-19 information. A study from the southern part of the country16 also revealed that TV/radio is the major source (80.3%) of COVID-19 information. A large majority of study participants (96%) have a favorable attitude towards COVID-19 prevention and control measures. This is because of vast broadcasting about COVID-19 through private and public media and good knowledge of the participants. The result is much higher than previous studies conducted in the country,16 Uganda (72.4%) and Rivers state Nigeria (80.6%).17,18 Yet, 12.3% of the participants disagree on the importance of taking preventive measures, while another 22.2% has a trust in cultural medications to prevent and/or cure COVID-19. Interestingly, 83.7% of the study participants admitted that they could recommend the implementation of COVID-19 preventive measures to a friend; indicating their degree of willingness against the disease transmission. Furthermore, 84.2% of the participant’s belief that COVID-19 is a preventable disease provided that appropriate preventive measures are implemented uniformly. Generally, this finding suggests a high level of public willingness to stand with the government in combating the disease and the public acceptability of preventive and control measures.
Despite a high level of sufficient knowledge and favorable attitude towards COVID-19, this study found adequate practice only in 44.6% of the study participants; which shows inadequate practice in most participants to halt coronavirus transmission. Thus, the finding is lower when compared with previous studies carried out in the country9 and abroad,10,19 where the overall good practice was 52.7%, 88.1% and 67%, respectively.9,10,19 We might relate the reason to more practice questions (twelve) used in the present study and an observation part to measure practice objectively. Still, our finding is comparable with other studies conducted in the country that reported low practices of participants towards COVID-19 prevention.9,14,20 This implies that having adequate knowledge and favorable attitude will not always lead to the adoption of a new practice by a target group. These reminds the government to follow some compulsory regulations on COVID-19 preventive measures despite escalating public knowledge. Regarding specific practices, most participants are washing their hands with soap and water (87%), while 93.2% avoided handshaking, 79% stopped visiting crowded places, 89.4% maintain their physical distancing, and 34.7% staying at home. These specific practices seem high and adequate to prevent COIVD-19 as compared to our pooled practice prevalence which is 44.6%. Our findings are higher when compared with previous studies conducted in other parts of the country8 that reported a specific practice of 77.3%, 53.8%, 33.2%, 33.6% and 1.6%, respectively. The difference is more likely because they conduct the previous study in the early phase of the pandemic, where most preventive and control measures are not intensified by the government.
But even though our participant’s specific practice seems satisfactory, we found a big discrepancy between our point in time practice observation and participants’ self-report. For instance, the prevalence of handwashing is 87% as reported by participants, whereas the observed handwashing prevalence is 66.3%. Similarly, maintaining physical distancing and facemask utilization is self-reported to be 89.4 and 34.4%, respectively, but 72.2 and 21.2% as per our observation in the health facilities. Likewise, even though 47.6% of the study participants have sanitizers at home, only 20.3% of them were having it at hand. In our observation, we get a relatively low specific practice because of a point in time real data recording procedure or because of over-reporting by some participants on the counter.
To determine the predictors of sufficient knowledge, favorable attitude and adequate practice, we run three independent logistic regressions and each produced a unique combination of risk factors. In the first model, the odd of having sufficient knowledge is 6.5 times higher in participants with primary education as compared to participants with no formal education (AOR: 6.5, 95% CI: 2–21.4). This finding is consistent with other studies conducted in southwest Ethiopia21 and across the world.19,22 Similarly, the availability of television in the households resulted in a higher likelihood of having sufficient knowledge (AOR: 3.8, 95% CI: 1.4–10.5), which is also supported by our descriptive finding, where 79% of the participants mentioned television as the primary source of COVID-19 information. Likewise, the likelihood of sufficient knowledge is three to four times higher in participants who have telephone and radio. They also documented similar findings in a study conducted in Kenya.15 Nonetheless, this finding sounds more when we think of those rural residents that did not have formal education, television, radio and telephone and it implies the importance of choosing and designing appropriate communication media for each segment of the population.
Participants with sufficient knowledge are five and nearly four times more likely to have a favorable attitude and adequate practices, respectively, as compared to their counterparts. This tells us escalating public knowledge of COVID-19 is the cornerstone and the precursor for effective control of the pandemic. The finding is also evidenced in other similar studies carried out in central Nigeria.14 Also, even though not surprisingly, farmer participants are seven times less likely to exercise COVID-19 precaution measures as compared to employed participants. Likewise, students and housewives are also three times less likely to have adequate practice as compared to employed. We also find personal telephone utilization to increase the odds of implementing COVID-19 prevention precautions with over three folds. This is more likely explained because participants with telephone are more likely to use social media like Facebook and also receive short voice or text messages from the national telecom.
Finally, our study has its own strength and weakness that has to be known to the readers. First, we have tried to incorporate observation part to measure practice besides participants’ self-report. Second, this study has tried to avoid the possibility of social desirability bias by actively asking participants to mention the answer under each question rather than telling them the choices and recording their responses. Still, the possibility of false or over-reporting of preventive measures by some participants is not fully excluded from this study.
Conclusions
In the study area, the participant’s knowledge and attitude are sufficient to halt coronavirus transmission. However, practice in the vast majority is not adequate to combat the pandemic. Educational status, television, telephone, radio, occupation and knowledge are found to be significant factors for successful prevention and control of coronavirus. Despite escalating public knowledge, our finding suggests the government to follow some compulsory regulations to enable the uniform implementation of COVID-19 precaution measures. Furthermore, COVID-19 interventions should consider identified modifiable factors for successful prevention and control of the pandemic.
Abbreviations
APHI: Amhara Public Health Institute; COVID-19: coronavirus disease 2019.
Data Sharing Statement
We have deposited all relevant data on public data repositoriesAlemu, Tefera (2020), “Mr”, Mendeley Data, V1: http://dx.doi.org/10.17632/xk5hg4d5bg.1.
Ethics Approval and Consent to Participate
We got Ethical approval from Amhara Public Health Institute Ethical review committee (Protocol No: H/R/T/T/D/3/791) and a support letter from the research and technology transfer directorate of the institute to get the permission and cooperation of concerned bodies in Dessie city. We got an informed oral consent from each participant, which was approved by the ethical review committee. The interviewers took precautionary measures to prevent COVID-19 cross contaminations. The study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable.
Acknowledgments
We appreciate the study participants for their willingness to participate in the study. We are also grateful to acknowledge Amhara Public Health Institute Dessie Branch for covering data enumeration expenses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We did not receive funding from any organization, but the APHI_Dessie Branch has covered data enumeration expense.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Aylward B (WHO), Liang W (PRC). Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). WHO-China Jt Mission Coronavirus Dis 2019. 2020:16–24. Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
2. Available from: https://www.who.int/docs/default-source/coronaviruse/key-messages-and-actions-for-covid-19-prevention-and-control-in-schools-march-2020.pdf?sfvrsn=baf81d52_4.
3. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/.
4. COVID-19 prevention measures in Ethiopia: current realities and prospects. [cited November 6, 2020]. Available from: https://www.ifpri.org/publication/covid-19-prevention-measures-ethiopia-current-realities-and-prospects.
5. Ethiopian Ministry Of Health. Ethiopia confirmed the first case of COVID-19. [cited November 6, 2020]. Available from: http://www.moh.gov.et/ejcc/en/node/194.
6. Ethiopia coronavirus: 112,740 cases and 1745 deaths-worldometer. [cited November 6 2020]. Available from: https://www.worldometers.info/coronavirus/country/ethiopia/.
7. Defar A, Molla G, Abdella S et al. Knowledge, practice and associated factors towards the Prevention of COVID-19 among high-risk groups: a cross-sectional study in Addis Ababa, Ethiopia; 2020.
8. Yohannes Kebede,Yimenu Yitayih, Zewie Birhanu et al. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;77:1–15. doi:10.1371/journal.pone.0233744
9. Yonas Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at. Infect Drug Resist. 2020;Volume 13:1949–1960. doi:10.2147/IDR.S258736
10. Narayana G, Pradeepkumar B, Ramaiah JD, et al. Knowledge, perception, and practices towards COVID-19 pandemic among general public of India: a cross-sectional online survey. Curr Med Res Pract. 2020;10(4):153–159. doi:10.1016/j.cmrp.2020.07.013
11. Sima Rugarabamu MI, Garima T, Singh BM, Ram R, Tripti RP. Knowledge, attitudes, and practices towards COVID-19 among Nepalese residents: a quick online cross-sectional survey. Asian J Med Sci. 2020;11(3):6–11. doi:10.3126/ajms.v11i3.28485
12. Haftom M, Petrucka P, Gemechu K, et al. Knowledge, attitudes, and practices towards covid-19 pandemic among quarantined adults in Tigrai region, Ethiopia. Infect Drug Resist. 2020;13:3727–3737. doi:10.2147/IDR.S275744
13. Asmelash D, Fasil A, Tegegne Y, et al. Knowledge, attitudes and practices toward prevention and early detection of COVID-19 and associated factors among religious clerics and traditional healers in Gondar town, northwest Ethiopia: a community-based study. Risk Manag Healthc Policy. 2020;13:2239–2250. doi:10.2147/RMHP.S277846
14. Bekele D, Tolossa T, Tsegaye R et al. The knowledge and practice towards COVID-19 pandemic prevention among residents of Ethiopia. An online cross-sectional study. bioRxiv. 2020;06(01):127381. doi:10.1101/2020.06.01.127381
15. Austrian K, Pinchoff J, James B et al. COVID-19 related knowledge, attitudes, practices and needs of households in informal settlements in Nairobi, Kenya; 2020:1–21.
16. Fantaye T, Nassir N. Knowledge, attitude and practice towards COVID-19 among Arba Minch Town GSJ: volume 8, Issue 6, June 2020, Online: ISSN 2320-9186 Knowledge, attitude and practice towards COVID-19 among Arba. Glob Sci J. 2020.
17. Ssebuufu R, Katembo F, Mambo S, et al. Awareness, knowledge, attitude and practice towards measures for prevention of the spread of COVID-19 in the Ugandans: a nationwide online cross-sectional survey. medRxiv. 2020. doi:10.1101/2020.05.05.20092247
18. Kevin C, Anthony IVA. Knowledge, attitude and practice of clients towards COVID-19 at primary healthcare facilities in Rivers State, Nigeria; 2020. doi:10.21203/rs.3.rs-40966/v1
19. Al-hanawi MK, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. 2020;8:1–10. doi:10.3389/fpubh.2020.00217
20. Degu A, Nibret G, Gebrehana H et al. Knowledge and practice to prevent against corona virus disease (COVID-19) and its associated factors among pregnant women in Debre Tabor Town Northwest Ethiopia: a community based cross-sectional study; 2020:1–28. doi:10.21203/rs.3.rs-50212/v1
21. Feyissa D, Ejeta F, Abebe L et al. Community ’ s knowledge of COVID-19 and its associated factors in Mizan-Aman Town. 2020.
22. Alobuia WM, Nathan PD-B, Joseph D. Forrester et al. Racial disparities in knowledge, attitudes and practices related to COVID-19 in the USA. J Public Health (Bangkok). 2020:1–9. doi:10.1093/pubmed/fdaa069.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.