Back to Journals » Risk Management and Healthcare Policy » Volume 15
COVID-19 in Veterans: A Narrative Review
Authors Chuang YC ![]() , Tsai HW, Liu SA, Wu MJ
, Tsai HW, Liu SA, Wu MJ ![]() , Liu PY
, Liu PY ![]()
Received 19 December 2021
Accepted for publication 9 April 2022
Published 26 April 2022 Volume 2022:15 Pages 805—815
DOI https://doi.org/10.2147/RMHP.S354814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Yu-Chuan Chuang,1 Hung-Wen Tsai,2 Shih-An Liu,3 Ming-Ju Wu,1 Po-Yu Liu4
1Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 2Medical Administration Department, Taichung Veterans General Hospital, Taichung, Taiwan; 3Center of Quality Management, Taichung Veterans General Hospital, Taichung, Taiwan; 4Division of Infection, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
Correspondence: Po-Yu Liu, Division of Infection, Department of Internal Medicine, Taichung Veterans General Hospital, No. 1650, Sec. 4, Taiwan Blvd., Xitun Dist., Taichung City, 407219, Taiwan, Tel +886 4 2359 2525, Email [email protected]
Abstract: Veterans are a special population that has been largely ignored during the corona virus disease 2019 (COVID-19) pandemic. Veterans with COVID-19 not only suffered symptoms from the disease but also had a higher risk of further development of in-hospital complications involving multiple organs. This article aims to review the current literature on the epidemiology, risk factors, diagnosis, clinical presentation, treatment, and outcome in veterans who contracted COVID-19 during the pandemic, using papers published between January 1, 2020 and August 1, 2021. Forty published papers were considered relevant to this review study. The COVID-19 pandemic not only caused a burden on health-care facilities but also affected the veterans population. Veterans with COVID-19 not only suffered symptoms from the disease but also had a higher risk of further development of in-hospital complications involving multiple organs. The dismal outcome might be attributed to old age and multiple comorbidities among veterans. Symptoms that may be seen in veterans with COVID-19 are comparable to those in the general population with fever, cough, and dyspnea, the most commonly reported. There are several approaches, such as self-assessment tools and virtual or telephone triage strategies, that can initially provide adequate evaluation of the symptoms related to COVID-19 in veterans. Adequate risk stratification could be carried out using the VA COVID-19 (VACO) Index, which predicts the risk of 30-day all-cause mortality after COVID-19 infection. There are several COVID-19 specific treatments that have been given to veterans; however, none of them have been proven to reduce the overall mortality in veterans. The overall mortality rate among veterans showed a declining trend. However, veterans suffering from chronic COVID-19 are at risk of dependence on activities of daily living after recovering from the illness. In summary, veterans are a special population that requires more attention especially during the COVID-19 pandemic.
Keywords: SARS-CoV-2, COVID-19, veterans, pandemic
Introduction
Veterans represent a special population that may suffer not only from physical illness but also from mental problems, such as mental health issues, behavioral adjustment disorder, substance use disorders, and post-traumatic stress disorders, disproportionately compared to the general population.1 There is also evidence showing that veterans who have been previously injured in combat are at higher risk of developing hypertension, coronary artery disease, diabetes mellitus, and chronic kidney disease.2 Moreover, veterans seem to suffer from a poorer health status and have more chronic medical conditions. A previous study in the United States analyzed patients in the Veterans Affairs (VA) health system, and the results showed that veterans are 14 times more likely to have more than 5 medical conditions compared with the general population.3 As a result, it is essential to take veterans into special consideration in the global pandemic of coronavirus disease 2019, which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).4
Veterans are a group of individuals, mainly male, who are older compared to the general population. The COVID-19 pandemic not only caused a burden on health-care facilities but also affected the veterans population. Reduced hospitalizations, delayed surgeries, and even rising numbers of cases with serious mental illnesses were reported during the pandemic. Veterans with COVID-19 not only suffered symptoms from the disease but also had a higher risk of further development of in-hospital complications involving multiple organs.5–7 The case fatality rate in veterans aged 65 and older was 20%, which exposed the fact that the majority of the veterans population was at risk of COVID-19 related mortality.8 In veterans with COVID-19, even after recovery from the acute phase, they faced sequelae involving pulmonary and extrapulmonary systems; additionally, they had a higher risk of death.9
Currently, there are few data on the impact of COVID-19 on veterans, even though it is apparent that taking veterans into special consideration is crucially important. In this study, we conduct a thorough review of the current data on SARS-CoV-2 infection in veterans, from epidemiological, clinical, and laboratory perspectives, including data on the disease course, treatment, and prognosis.
Materials and Methods
We organize the current evidence related to epidemiology, risk factors, diagnosis, clinical presentation, treatment, and outcomes in veterans suffering from COVID-19. Accordingly, we performed a thorough literature search using PubMed. The available data were identified by searching PubMed, current contents, and references from relevant articles. For the bibliographic search, MeSH terminology was used with the following search strategy: [(“COVID-19”[Mesh]) AND (“Veterans”[Mesh])]. The search period was January 1, 2020 to August 1, 2021. All retrieved records (including original articles, letters to editor, editorials, and case reports) in English and records with English translation were downloaded and evaluated. Afterwards, the abstracts were evaluated for eligibility. All duplicates were eliminated. Finally, all of the data were analyzed.
Results
In total, there were 84 published papers found with contents related to COVID-19 and with a specific population of veterans. All full-text articles were published between January 1, 2020 and August 1, 2021. After a thorough review, 40 published papers were considered relevant to this study.
Impact of COVID-19 in Veterans
The COVID-19 pandemic not only placed a burden on health-care facilities but also affected the veterans population. Reduced hospitalizations, delayed surgeries, and even a rise in cases of serious mental illnesses were reported during the pandemic. Veterans with COVID-19 not only suffered symptoms from the disease but also had a higher risk of further development of in-hospital complications involving multiple organs.5–7 During the COVID-19 pandemic, the overall number of VA hospitalizations due to emergency conditions, including stroke, myocardial infarction, heart failure, chronic obstructive pulmonary disease (COPD), appendicitis, and pneumonia, decreased. Aaron et al showed a decrease in hospitalizations of up to 41.9%.4 This reduction might have a major impact on public health. In addition, the severity of illness during the COVID period seemed to be more intense. For example, Nadim et al showed fewer hospitalizations with increased inpatient severity, such as higher admission MELD (Model for End-Stage Liver Disease) Score among veterans patients with cirrhosis.10 The phenomenon in the aforementioned study was largely due to the fact that most of the patients, avoided the visiting hospital so as to minimize the risk of SARS-CoV-2 infection, even when their condition required emergency treatment.
Fortunately, Linda et al determined that the delay in elective surgical cases did not have a definite impact on the short-term mortality of veterans.11 This might be due to appropriate clinical decision-making. For example, most of the canceled elective surgical procedures were in those who were healthier with the majority of the cases related to ophthalmology and orthopedics. However, there were still several serious impacts on the overall health care system; one of which was that the surgical delays were likely to increase the overall costs.6 In addition, the consequences of cancellation may have had a deleterious psychosocial impact, including disappointment, anger, unhappiness, and stress, on the patients.7 Moreover, in some circumstances, the postponement of an intervention could have resulted in delayed definite diagnosis and even treatment.
Another critical issue in veterans with COVID-19 was the increase in mental illnesses, including anxiety, depression, and posttraumatic stress disorder (PTSD), during the pandemic. A recent study revealed around half of veterans reported symptoms of anxiety and depression; and at least 20% of veterans reported symptoms of PTSD.12 The rates of veterans suffering from these mental health disorders in the pre-COVID-19 era were approximately 23% for anxiety and 33% for depression, with the rate of PTSD remaining at nearly the same level. Based on these findings, the necessity for adopting an adequate strategy to tackle mental illness among veterans should not be underestimated.12 Indeed, psychiatric comorbidities might lead to long-term mental health sequelae. Apart from the physical and mental conditions that put veterans at risk, financial issues, limited access to medical resources, and lack of information on COVID-19 prevention are also important factors that resulted in veterans’ greater vulnerability during the pandemic.13
Epidemiology of COVID-19 in Veterans
Currently, most COVID-19 studies on veterans have been conducted in the United States. In the United States, the proportion of veterans in the population is approximately 7% with over 9 million enrolled in the VA health care system.14 The National Center for Veterans Analysis and Statistics published a report in 2018 showing that United States veterans were predominantly male and white; nevertheless, minority veterans accounted for up to 22% of the overall veterans population.14 The two largest minority groups in that year were African-Americans (11%) and Hispanics (7%). Female members comprised about 8.7% of whom 34.4% were from minority groups, namely African-Americans (19.5%) and Hispanics (8.3%).15
From the outbreak of COIVD-19 to October 17th, 2021, the VA identified 356,777 COVID-19 cases. The known COVID-19-related deaths totaled 15,591 cases. At the same time, there were 44,909,023 confirmed COVID-19-positive cases in the United States cases and 723,072 COVID-19-related deaths.16 In a previous study, the percentages of veterans with COVID-19 were 19%, 28%, and 52% in the 18–49 years, 50–64 years, and ≥65 years age group, respectively.14 Patient aged ≥65 years comprised the largest group of veterans with COVID-19 disease. With respect to gender, the ratio between male and female with COVID-19 disease was around 9 to 1, which is largely attributable to the baseline composition of the veterans population, which was predominantly male.14,17 The distribution of COVID-19 cases based on ethnicity is also an important issue. Around half of the patients were white, with blacks comprising 40% of cases. Hispanics accounted for 15%, and the remaining groups accounted for less than 1%, which included Asians, Native American, Alaskan natives, Hawaiian native, and Pacific islanders.14,17 Of those who tested positive for COVID-19, the percentage of reported deaths in the veterans population was about twice that of the general population, ie, 11.9% versus 5.2%.14,17 This difference may be due to the fact that veterans are older with higher prevalence of multiple comorbidities. In summary, veterans were a group of older individuals, compared to the general population, and were mostly male.
Risk Factors of Severe COVID-19
Veterans are at risk of severe illness, particularly due to old age (65 years of age and older), obesity, and multiple comorbidities. Table 1 summarizes the common risk factors for developing severe COVID-19 in veterans. Older adults were more likely to develop severe COVID-19 disease. That is to say, they were at greater risk of having SpO2 <94% on room air, a ratio of arterial partial pressure of oxygen to a fraction of inspired oxygen (PaO2/FiO2) <300 mm Hg, respiratory frequency >30 breaths/min, or lung infiltrates >50%, according to the National Institutes of Health (NIH).18 In comparison to veterans aged <65 years old, those who were aged ≥65 years old had up to 4.5-fold increased mortality rates after hospitalization from COVID-19.19 Moreover, veterans aged ≥85 years old had a 14-fold risk of hospitalization after contracting COVID-19 compared to those aged 18–29 years old.15 Based on age categories of veterans patients, the percentages of mortality in the 18–49 years, 50–64 years, and ≥65 years old age groups were 0.5%, 9.5%, and 89.9%, respectively.19 An analysis of the overall rates of COVID-19 based on ethnicity revealed rates of 0.10% and 0.38% for white and black veterans. Black veterans were more likely to have COVID-19 disease, with a rate 3.7 times higher than that of white veterans. As for mortality, black veterans had a 2.8 times higher rate than white veterans.14 With respect to minority veterans, Hispanic or Latinos were reported to have a 4.6 times higher rate of hospitalization compared with non-Hispanic White veterans.14,19 However, whether race is a risk factor for developing severe COVID-19 disease remains a question and requires further studies.
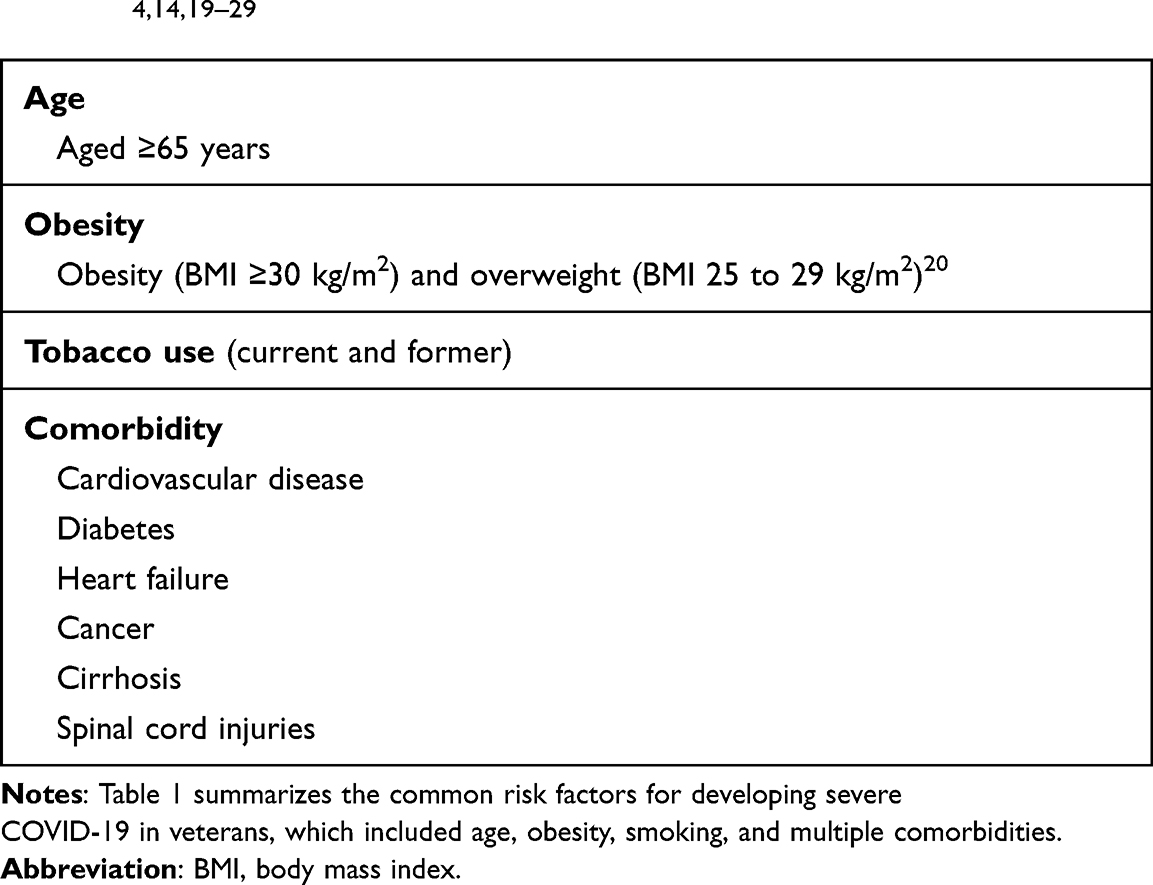 |
Table 1 Documented Risk Factors for Severe COVID-19 in Veterans4,14,19–29 |
Obesity is a well-known risk factor in developing severe COVID-19 in general population as well as in veterans. Veterans with a higher BMI were reported to be more likely to test positive for SARS-CoV-2; moreover, the rate of using mechanical ventilation or even mortality were also higher.20 It was estimated that up to 44% of veterans with COVID-19 were obese.14 Indeed, Oda et al concluded that the BMI values between 30 and 39 kg/m2, but not BMI values between 23 and 30 kg/m2 in veterans were associated with increased rates of hospitalization due to COVID-19, ICU admission, and mortality.21
Smoking is a risk factor that may contribute to higher rates of COVID-19-related mortality. Amanda et al found a positive relation between lifetime tobacco use and the rate of testing positive for SARS-CoV-2, as well as the likelihood of COVID-19 mortality.22 Social and behavioral risk factors are common in veterans; however, surprisingly in veterans with COVID-19, housing issues, financial difficulty, alcohol use, and substance use were not associated with higher mortality.23
Veterans with positive test results of SARS-CoV-2 had higher rates of coexisting comorbidity. Ioannou et al revealed that only 31% of veterans had no comorbid conditions; therefore, most veterans were at a considerable risk of developing severe COVID-19.24 It is believed that veterans with COVID-19 and concomitant cardiovascular disease (CVD) had adverse outcomes. Roughly, 66% of veterans suffering from COVID-19 had a medical history of CVD. Of those who died of COVID-19, 87% of veterans were reported to have a history of CVD.14 Heart failure is another common complication in COVID-19, which confers a higher risk of mortality. In addition, veterans with pre-existing heart failure were also at increased risk of 30-day mortality and hospital admissions.25
A previous study showed that 43% of veterans suffering COVID-19 had diabetes mellitus.14 Diabetes mellitus is linked to a higher risk of severe COVID-19 in veterans because of diabetes-related problems, such as hyperglycemia, metabolic abnormalities, altered immune status, and coagulation abnormalities.26 Nevertheless, in veterans with diabetes, CVD-related factors also, in part, play an important role in developing adverse outcomes from COVID-19. Cancer itself is known to put populations, including veterans, at higher risk of SARS-CoV-2 infection and developing severe COVID-19.27 Cirrhosis in veterans is another important issue as it is a risk factor that increases the likelihood of contracting SARS-CoV-2 compared with veterans without cirrhosis. In veterans with COVID-19, if the patient had cirrhosis, the percentages of hospitalization, mechanical ventilation, and mortality were all higher than those without cirrhosis.28 Veterans who have suffered a spinal cord injuries (SCIs) are at higher risk of community-acquired pneumonia associated death, as well as COVID-19 associated medical condition. The case fatality rate in SCI veterans with COVID-19 was 2.4 times higher than that in non-SCI veterans.29 Aside from the aforementioned comorbidities, Rebecca et al also listed several conditions in veterans that the physician should be alert to. These conditions include respiratory failure, congestive heart failure, cardiac dysrhythmias, ischemic heart disease, hypertensive heart and/or renal disease, renal failure, and electrolyte or acid-base disorders.4 All of these conditions put veterans at a higher risk of developing severe COVID-19.
Clinical Presentation of COVID-19 Illness in Veterans
There is a wide spectrum of symptoms in veterans with a positive result of SARS-CoV-2. A patient may present with asymptomatic infection or even life-threatening illness, including respiratory and non-respiratory complications.30 Around half of veterans reported symptom of fever, and although it is a critical symptom, it is not the only initial symptoms of COVID-19. Among veterans who contracted COVID-19 illness, the top three most common symptoms were fever, cough, and dyspnea.24 Nevertheless, the ratio of symptoms varied. Another study showed that the most common symptoms in veterans with COVID-19 was cough, which occurred in 60% of patients, followed by fever and dyspnea in more than half of the patients. Furthermore, malaise, chills, myalgias, headache, gastrointestinal complaints, and loss of smell or taste were also common in veterans.31 In contrast, about 80% of the general population only experienced mild respiratory symptoms with approximately 15% of patients suffering moderate-to-severe pneumonia.32 Table 2 summarizes the common symptoms among veterans with COVID-19 in comparison with the general population.33–35 With the limited data on COVID-19 related symptoms in veterans, the interpretation of the results could be biased. Further study should be carried out to better define the clinical characteristic in this special population.
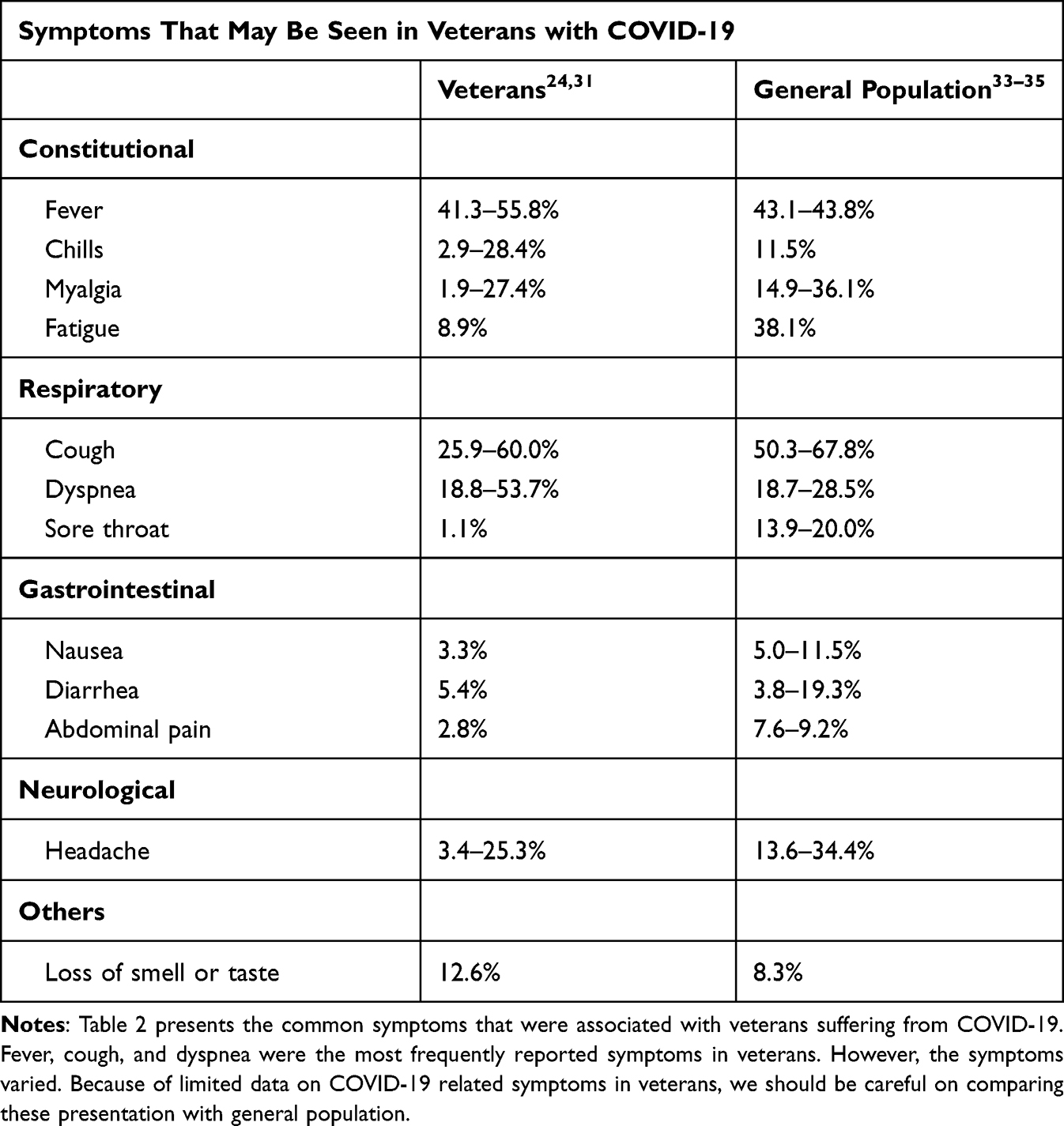 |
Table 2 Symptoms Associated with COVID-19 in Veterans and the General Population |
Complications resulting from COVID-19 in veterans were common. It is estimated that around 24% of COVID-19 veterans patients had involvement of more than three organ systems with respiratory complications being the most common.36 The most commonly involved organ was the respiratory system. More than 70% had respiratory complications and pneumonia was the most common, followed by respiratory failure and acute respiratory distress syndrome (ARDS). Regarding non-respiratory complications, the most commonly involved organ was the renal systems.36 Benjamin et al conducted a national cohort of US veterans hospitalized with COVID-19. The study found that around 30% of veterans developed acute kidney injury (AKI) and 12% eventually received renal replacement therapy. Most veterans with COVID-19 suffered from AKI on the first day of admission and in almost half of them, renal function did not return to baseline on discharge.37 There were several important factors that had a significant association with AKI during admission, which included old age, male gender, obesity, Black race, hypertension, diabetes mellitus, and impaired baseline kidney function. Compared to veterans with and without AKI, AKI appeared to confer a higher risk of mechanical ventilator use, longer hospitalization, and death.37 Other commonly involved organ systems included cardiovascular, hematologic, and neurologic systems.36 In general, veterans with COVID-19 not only suffered symptoms of the disease but also had a higher risk of further development of in-hospital complications. In addition, minorities seemed to be more vulnerable to the development of these complications.36 Although further study is needed to confirm the relationship between races and multi-organ complications, it is crucial to take these patients into special consideration.
Laboratory abnormalities are also common in veterans with COVID-19, including lymphopenia (generally corresponding to <1000 lymphocytes/microL in adults), impaired renal function test, impaired liver function tests, decreased albumin level, and coagulation abnormalities. Lymphopenia is particularly common, which is seen in almost half of the veterans with COVID-19, even though the total white blood cell count can vary. As an example, in a series of 10,131 US Veterans with SARS-CoV-2 Infection, 71.2% had a lymphocyte count <1400/microL, and a white blood cell count of <4770/microL was reported in 24.5% of the patients.24 In conclusion, there were many laboratory abnormalities that were associated with mechanical ventilation and death, and these included impaired renal function test, liver function test, total white blood cell count elevation, lymphopenia, and low albumin level.
Comparisons Between COVID-19 and Seasonal Influenza in Veterans
After the emergence of the COVID-19 pandemic, the similarities and differences between COVID-19 and seasonal influenza were widely discussed. For veterans who required further admission, COVID-19 patients had a more than five times higher risk for respiratory and non-respiratory complications, mechanical ventilator use, ICU admission, and mortality, as well as incurring higher health costs, compared with those who contracted seasonal influenza.36,38 In summary, compared with influenza, COVID-19 had a strong association with risk of COVID-19-related complications and mortality. These differences warrant further research on the development of management strategies for veterans with COVID-19.
Co-Infection with Other Respiratory Pathogens in Veterans
The actual prevalence of co-infection with other respiratory pathogens is not well known. Bradley et al revealed that bacterial coinfection in COVID-19 is not frequent. Among COVID-19 patients requiring hospitalization, the rate was less than 10%.39 Patricia et al conducted a study, which included 174,746 veterans, and found that the rate of respiratory co-infection in veterans was around 1.5%.40 The most common pathogens for causing co-infection were rhinovirus and enterovirus, which was similar to other studies in the general population. However, the low prevalence of respiratory co-infection in COVID-19 may have been underestimated because not all of the patients who were positive for SARS-CoV-2 receive the test for other respiratory pathogens.
Approach to COVID-19 in Veterans
Appropriate Triage
The approach to COVID-19 in veterans requires greater caution as this population is at risk of severe illness, particularly those with risk factors, such as old age (65 years of age and older), obesity, and multiple comorbidities. The definite treatment approach to veterans should be based on local and national strategies; however, herein we have presented several strategies used in the United States that can be applied in other regions. Even in cases with mild symptoms, once the patient has been confirmed positive for SARS-CoV-2, he or she will probably first contact the VA health system for help. Self-assessment tools and virtual or telephone triage strategies are both helpful in this situation. The assessment includes several questions that can provide adequate evaluation for symptoms related to COVID-19. The VA has developed many ways for veterans to access help when needed; for instance, adequate medical information and assistance are available via VA websites, VA application software, call centers, and scheduled virtual visits, which include video- and phone-based care.30 The VA system responded to the pandemic immediately by shifting the inpatient service to virtual care for all veterans. The VA launched a digital self-screening tool for COVID-19 in June, 2020. This enabled the identification of veterans at risk of contracting COVID-19 and facilitated the arrangement of further screening for these veterans.41 For veterans who were at risk of developing COVID-19, these strategies had several benefits including maintaining adequate social distance and allowing the management of increasing numbers of infected veterans in a safer way. Nevertheless, there were also disadvantages. For example, the elderly, homeless people, and veterans living in rural areas had limited access to the virtual service.42 When veterans experienced symptoms that suggested respiratory compromise, such as hypoxia or dyspnea at rest, they were referred for in-person evaluation at either the outpatient clinic or emergency department.30 After proper triage, the patient may be sent home for isolation, to an alternate site of care, or to the emergency department. If veterans who need further medical resource can be identified quickly, the proper medical resource can be allocated accordingly.
Risk Stratification
Proper evaluation of the risk of developing severe COVID-19 disease in veterans should be conducted in order to provide better management of care. According to the NIH, once a patient suffers SpO2 of <94% on room air, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mm Hg, respiratory frequency >30 breaths/min, or lung infiltrates >50%, hospitalization is indicated.18 However, these criteria may not be appropriate for veterans. Veterans are at a higher risk of severe COVID-19 due to the high prevalence of multiple comorbidities, old age, and obesity. Therefore, Joseph et al developed a risk score, using data from the VA health system, to evaluate the short-term mortality in both inpatients and outpatients with COVID-19 disease. The VA COVID-19 (VACO) Index predicts the risk of 30-day all-cause mortality after COVID-19 infection using a formula consisting of age, gender, and pre-existing conditions.43 The VACO index can help clinicians make better treatment decisions for veterans with COVID-19, such as determining who should be managed as inpatients who require close clinical follow-up, and even determining who is a priority for COVID-19 vaccination.44
Mental health in veterans with COVID-19 is an issue that has often been underestimated. Compared to the general population, veterans had a higher prevalence of psychiatric disorders and psychosocial stressors.45 Veterans with existing mental problems, such as post-traumatic stress disorder, anxiety and depression, substance use disorders, and sleep disorders, were more vulnerable to mental health issues during the COVID-19 pandemic.46 Suicide rates also increased during the pandemic among veterans. Accordingly, enhancing social support and suicide prevention should be just as important as managing COVID-19 disease itself, particularly in vulnerable populations like veterans.
Universal screening for SARS-CoV-2 was beneficial in limiting the spread of the disease in veterans. For instance, success in controlling the COVID-19 outbreak in a VA nursing facility was achieved using the universal screening approach.47,48 Not only veterans but also staff members at VA nursing facilities may benefit from screening of SARS-CoV-2, as this allows the health system to determine whether those infected with SARS-CoV-2 were actually asymptomatic or pre-symptomatic.48 Whether there is a benefit or not in screening for SARS-CoV-2 for all veterans requires further investigation.49 However, in a veterans facility, the screening is necessary so as to reduce the overall risk, especially during outbreaks in local region.
COVID-19 Treatment in Veterans
In general, the overall treatment of COVID-19 in veterans is conducted in accordance with the NIH COVID-19 treatment guidelines.18 For patients, including veterans, with mild symptoms, which refer to oxygen saturation >94% without the need for oxygenation or ventilatory support, management can be provided in the outpatient setting with close monitoring for COVID-19 disease progression. However, as mentioned previously, it is essential to pay close attention to veterans even in those who have only developed mild symptoms due to the high risk of progressing to severe COVD-19. Nonetheless, for veterans requiring inpatient management, oxygen supplementation, low-dose dexamethasone, and remdesivir are suggested. Administration of tocilizumab added to dexamethasone should be considered in patients with markedly elevated inflammatory markers, mechanical ventilator use, or extracorporeal membrane oxygenation.18 Herein, we review the efficacy and safety of several COVID-19-specific treatments carried out in veterans.
Remdesivir
Remdesivir is a nucleotide analog that was approved by FDA for treatment in hospitalized COVID-19 patients. Its precise role remains uncertain. In veterans, its efficacy may be limited. Michael et al conducted a cohort study in US veterans and found routine use of remdesivir showed no benefit. In fact, the use of remdesivir did not improve survival or reduce the 30-day mortality, but prolonged the length of hospitalization.50 The longer hospital stays could be partially attributed to the treatment course of remdesivir, which lasted for several days.
Antibody-Based Therapies with Convalescent Plasma
It has been hypothesized that convalescent plasma, which contains potentially therapeutic antibodies from individuals who have recovered from COVID-19, has a clinical benefit for hospitalized patients suffering from COVID-19. However, research on veterans showed that convalescent plasma did not actually reduce the death rate in veterans with non-severe COVID-19. Approximately, 8% of 4755 VA patients had received convalescent plasma therapy in the study. The 30-day mortality rates of patients who received and did not receive convalescent plasma were 6.5% and 6.2%, respectively.51 In summary, the results showed no benefits on mortality rates in veterans with non-severe COVID-19.
Hydroxychloroquine
Hanna et al investigated 64,000 VA patients, among whom more than 7000 tested positive for SARS-CoV-2, and found hydroxychloroquine had no clear clinical benefit.52 In total, 657 veterans were prescribed hydroxychloroquine; however, use of either hydroxychloroquine alone or in combination with azithromycin was not shown to be effective. Conversely, in veterans using hydroxychloroquine with azithromycin, there was a higher risk of mechanical ventilator use.52 Consequently, the decision to use hydroxychloroquine in veterans should be weighed carefully.
Antibacterial Agents
Since there are few data on bacterial co-infection and it is relatively uncommon, routine administration of empiric antibiotic therapy is not recommended in the current clinical practice.53 However, more than 50% of hospitalized patients received empiric antibiotic therapy without definitive identification of the pathogens.54 Nevertheless, it is reasonable to prescribe antibacterial agents in severe clinical situations. Laboratory findings that are suggestive of bacterial co-infection include leukocytosis and elevated inflammatory markers and chest roentgenogram may reveal patchy areas of consolidation. Also, recurrent fever after initial defervescence is another feature. For patients requiring mechanical ventilator support and for critically ill patients, empirical antibiotic treatment is also recommended.53 Antibiotic de-escalation strategy is necessary with close evaluation according to the microbiological evidence and the patient’s condition.
Thrombosis and Venous Thromboembolism Prevention
Prompt evaluation and prevention of venous thromboembolism is suggested in the current literature. A study of veterans with COVID-19 showed that baseline aspirin use is associated with lower mortality rates.55 In addition to antiplatelet medications, the use of anticoagulants lowered the mortality from COVID-19 according to data from the VA health system, which included about 4200 patients admitted due to COVID-19. Compared with patients not receiving anticoagulants, patients on anticoagulation therapy had a 27% lower risk of 30-day mortality from COVID-19. Moreover, its use was not apparently associated with serious bleeding events.56 In conclusion, veterans may benefit from the prophylactic use of anticoagulants, which prevent venous thromboembolism in hospitalized patients with COVID-19.
The Role of Palliative Care in Managing Veterans with COVID-19
The high burden of coexisting comorbidities in veterans means that they are more vulnerable than the general population. Palliative care may play an important role in veterans with COVID-19.57 In such patients, several pharmacological and non-pharmacological management for breathlessness, agitation, and anxiety are crucial. Withholding non-beneficial treatment should also be considered. Jordana et al demonstrated the benefits of palliative care in veterans. Palliative care intervention provides critically ill patients with relief from discomfort, which in turn is beneficial to the patient’s family.58
Outcomes in Veterans with COVID-19
In veterans, more than 80% of COVID-19-related deaths were seen in patients older than 65 years of age, which was higher than in the general population.8,19 Nevertheless, the overall mortality rate in veterans showed a declining trend. The initial 30-day mortality rate was 19.2%, which dropped significantly to 16.8% over the first 10 months of the COVID-19 pandemic. The decline might be due in part to increased utilization of personal protective equipment and proper social distancing, as well as better management of patients suffering from COVID-19.8 However, even though there was a substantial improvement in the overall mortality among veterans, there is still a relatively high risk of severe disease and death in these patients compared to the general population.
The functional status at discharge is important in patients who have recovered from COVID-19 infection, especially in the elderly. Functional disability in veterans with COVID-19 increased with age and severity of COVID-19 as well as related complications, including respiratory failure, delirium, cardiac disease, and thromboembolic disease. These data provide health systems with useful information, which may help inform decisions related to arrangements of discharge plans for veterans and conducting a proper transition to other care facilities for veterans with dependence on activities of daily living after recovering from the illness.59
Chronic COVID-19, also known as “long COVID”, has no formal diagnostic criteria.60 However, veterans who have recovered from acute symptoms of COVID-19 disease are at higher risk of mortality and further consumption of medical resources at one-month post-recovery. Moreover, veterans may suffer from several symptoms for a prolonged period after the acute phase of the illness. Prolonged symptoms place an excess burden on veterans. The most commonly involved organ is the respiratory system with presentation of cough, hypoxemia, and shortness of breath. The extrapulmonary systems that are affected include the cardiovascular, hematologic, endocrine, dermatological, gastrointestinal, renal, and neurological systems, as well as mental health.9
Conclusion
In this review, we conducted a thorough analysis of studies in the literature that related to veterans with COVID-19. In the United States population, the proportion of veterans is approximately 7%; however, due to old age, obesity, and multiple comorbidities, veterans are at higher risk of developing severe COVID-19, compared with the general population. During the COVID-19 pandemic, reduced hospitalizations, delayed surgeries, and even a rise in cases with serious mental illnesses were reported in veterans, which could have a major impact on public health. The symptoms and signs in veterans with COVID-19 are similar to those in the general population, and complications resulting from COVID-19 in veterans are common. Overall, several COVID-19-specific treatments have been carried out in veterans, but none of them have been shown to reduce the mortality rate. Further research on veterans with COVID-19 is necessary. Moreover, governments should pay more attention to this vulnerable population.
Acknowledgments
The authors did not receive any financial support for conducting this review or publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Olenick M, Flowers M, Diaz VJ. US veterans and their unique issues: enhancing health care professional awareness. Adv Med Educ Pract. 2015;6:635–639. doi:10.2147/AMEP.S89479
2. Stewart IJ, Sosnov JA, Howard JT, et al. Retrospective analysis of long-term outcomes after combat injury: a hidden cost of war. Circulation. 2015;132(22):2126–2133. doi:10.1161/CIRCULATIONAHA.115.016950
3. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at veterans affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21):3252–3257. doi:10.1001/archinte.160.21.3252
4. Song RJ, Ho YL, Schubert P, et al. Phenome-wide association of 1809 phenotypes and COVID-19 disease progression in the veterans health administration million veteran program. PLoS One. 2021;16(5):e0251651. doi:10.1371/journal.pone.0251651
5. Baum A, Schwartz MD. Admissions to veterans affairs hospitals for emergency conditions during the COVID-19 pandemic. JAMA. 2020;324(1):96–99. doi:10.1001/jama.2020.9972
6. Fu SJ, George EL, Maggio PM, Hawn M, Nazerali R. The consequences of delaying elective surgery: surgical perspective. Ann Surg. 2020;272(2):e79–e80. doi:10.1097/SLA.0000000000003998
7. Soreide K, Hallet J, Matthews JB, et al. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. Br J Surg. 2020;107(10):1250–1261. doi:10.1002/bjs.11670
8. Seligman B, Charest B, Gagnon DR, Orkaby AR. Trends in 30-day mortality from COVID-19 among older adults in the Veterans Affairs system. J Am Geriatr Soc. 2021;69(6):1448–1450. doi:10.1111/jgs.17127
9. Al-Aly Z, Xie Y, Bowe B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature. 2021;594(7862):259–264. doi:10.1038/s41586-021-03553-9
10. Mahmud N, Hubbard RA, Kaplan DE, Serper M. Declining cirrhosis hospitalizations in the wake of the COVID-19 pandemic: a national cohort study. Gastroenterology. 2020;159(3):1134–1136 e3. doi:10.1053/j.gastro.2020.05.005
11. Tran LD, Rose L, Urech T, Dalton A, Wu S, Vashi AA. Short-term effects of canceled elective procedures due to COVID-19: evidence from the veterans affairs healthcare system. Ann Surg. 2021;274(1):45–49. doi:10.1097/SLA.0000000000004809
12. Amsalem D, Lazarov A, Markowitz JC, Gorman D, Dixon LB, Neria Y. Increasing treatment-seeking intentions of US veterans in the Covid-19 era: a randomized controlled trial. Depress Anxiety. 2021;38(6):639–647. doi:10.1002/da.23149
13. Gerber MR. The things they carry: veterans and the COVID-19 pandemic. J Gen Intern Med. 2020;35(10):3093–3094. doi:10.1007/s11606-020-06048-x
14. Luo J, Jeyapalina S, Stoddard GJ, Kwok AC, Agarwal JP. Coronavirus disease 2019 in veterans receiving care at veterans health administration facilities. Ann Epidemiol. 2021;55:10–14. doi:10.1016/j.annepidem.2020.12.003
15. Affairs USDoV. Office of research & development. internet. U.S. Department of Veterans Affairs; 2021. Available from: https://www.research.va.gov/topics/health_equity.cfm.
16. Affairs USDoV. Department of veterans affairs COVID-19 national summary. U.S. Department of Veterans Affairs; 2021. Available from: https://www.accesstocare.va.gov/Healthcare/COVID19NationalSummary.
17. Rentsch CT, Kidwai-Khan F, Tate JP, et al. Patterns of COVID-19 testing and mortality by race and ethnicity among United States veterans: a nationwide cohort study. PLoS Med. 2020;17(9):e1003379. doi:10.1371/journal.pmed.1003379
18. National Institutes of Health (US). Coronavirus disease 2019 (COVID-19) treatment guidelines. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570371/.
19. Cardemil CV, Dahl R, Prill MM, et al. COVID-19-related hospitalization rates and severe outcomes among veterans from 5 veterans affairs medical centers: hospital-based surveillance study. JMIR Public Health Surveill. 2021;7(1):e24502. doi:10.2196/24502
20. Eastment MC, Berry K, Locke E, et al. BMI and outcomes of SARS-CoV-2 among US veterans. Obesity. 2021;29(5):900–908. doi:10.1002/oby.23111
21. Oda G, Sharma A, Lucero-Obusan C, Schirmer P, Sohoni P, Holodniy M. COVID-19 infections among healthcare personnel in the United States veterans health administration, March to August, 2020. J Occup Environ Med. 2021;63(4):291–295. doi:10.1097/JOM.0000000000002109
22. Raines AM, Tock JL, McGrew SJ, et al. Correlates of death among SARS-CoV-2 positive veterans: the contribution of lifetime tobacco use. Addict Behav. 2021;113:106692. doi:10.1016/j.addbeh.2020.106692
23. Kelly JD, Bravata DM, Bent S, et al. Association of social and behavioral risk factors with mortality among US veterans with COVID-19. JAMA Netw Open. 2021;4(6):e2113031. doi:10.1001/jamanetworkopen.2021.13031
24. Ioannou GN, Locke E, Green P, et al. Risk factors for hospitalization, mechanical ventilation, or death among 10131 US veterans with SARS-CoV-2 infection. JAMA Netw Open. 2020;3(9):e2022310. doi:10.1001/jamanetworkopen.2020.22310
25. Rumery K, Seo A, Jiang L, et al. Outcomes of coronavirus disease-2019 among veterans with pre-existing diagnosis of heart failure. ESC Heart Fail. 2021;8(3):2338–2344. doi:10.1002/ehf2.13291
26. Wander PL, Lowy E, Beste LA, et al. Risk factors for adverse outcomes among 35 879 veterans with and without diabetes after diagnosis with COVID-19. BMJ Open Diabetes Res Care. 2021;9(1):e002252. doi:10.1136/bmjdrc-2021-002252
27. Fillmore NR, La J, Szalat RE, et al. Prevalence and outcome of COVID-19 infection in cancer patients: a national veterans affairs study. J Natl Cancer Inst. 2021;113(6):691–698. doi:10.1093/jnci/djaa159
28. Ioannou GN, Liang PS, Locke E, et al. Cirrhosis and severe acute respiratory syndrome coronavirus 2 infection in US veterans: risk of infection, hospitalization, ventilation, and mortality. Hepatology. 2020;73:204–218. doi:10.1002/hep.31649
29. Burns SP, Eberhart AC, Sippel JL, Wilson GM, Evans CT. Case-fatality with coronavirus disease 2019 (COVID-19) in United States Veterans with spinal cord injuries and disorders. Spinal Cord. 2020;58(9):1040–1041. doi:10.1038/s41393-020-0529-0
30. Administration VH. COVID-19 response plan. Incident-specific annex to the VHA high consequence infection (HCI) base plan. Version 2. Available from: https://www.publichealth.va.gov/docs/n-coronavirus/COVID-19_Response_Plan_07Aug2020_signed_final.pdf.
31. Ebert TJ, Dugan S, Barta L, Gordon B, Nguyen-Ho C, Pagel PS. Clinical features of COVID-19 infection in patients treated at a large veterans affairs medical center. WMJ. 2020;119(4):248–252.
32. Tsai P-H, Lai W-Y, Lin -Y-Y, et al. Clinical manifestation and disease progression in COVID-19 infection. J Chin Med Assoc. 2021;84(1):3–8. doi:10.1097/JCMA.0000000000000463
33. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
34. Cheung KS, Hung IFN, Chan PPY, et al. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from a Hong Kong cohort: systematic review and meta-analysis. Gastroenterology. 2020;159(1):81–95. doi:10.1053/j.gastro.2020.03.065
35. Stokes EK, Zambrano LD, Anderson KN, et al. Coronavirus disease 2019 case surveillance - United States, January 22–May 30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(24):759–765. doi:10.15585/mmwr.mm6924e2
36. Cates J, Lucero-Obusan C, Dahl RM, et al. Risk for in-hospital complications associated with COVID-19 and influenza - veterans health administration, United States, October 1, 2018–May 31, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(42):1528–1534. doi:10.15585/mmwr.mm6942e3
37. Bowe B, Cai M, Xie Y, Gibson AK, Maddukuri G, Al-Aly Z. Acute kidney injury in a national cohort of hospitalized US veterans with COVID-19. Clin J Am Soc Nephrol. 2020;16(1):14–25. doi:10.2215/CJN.09610620
38. Xie Y, Bowe B, Maddukuri G, Al-Aly Z. Comparative evaluation of clinical manifestations and risk of death in patients admitted to hospital with covid-19 and seasonal influenza: cohort study. BMJ. 2020;371:m4677. doi:10.1136/bmj.m4677
39. Langford BJ, So M, Raybardhan S, et al. Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin Microbiol Infect. 2021;27(4):520–531. doi:10.1016/j.cmi.2020.12.018
40. Schirmer P, Lucero-Obusan C, Sharma A, Sohoni P, Oda G, Holodniy M. Respiratory co-infections with COVID-19 in the veterans health administration, 2020. Diagn Microbiol Infect Dis. 2021;100(1):115312. doi:10.1016/j.diagmicrobio.2021.115312
41. Affairs USDoV. COVID-19 screening tool. U.S. Department of Veterans Affairs; 2021. Available from: https://www.va.gov/covid19screen/.
42. Ferguson JM, Jacobs J, Yefimova M, Greene L, Heyworth L, Zulman DM. Virtual care expansion in the veterans health administration during the COVID-19 pandemic: clinical services and patient characteristics associated with utilization. J Am Med Inform Assoc. 2021;28(3):453–462. doi:10.1093/jamia/ocaa284
43. King JT
44. King JT, Yoon JS, Bredl ZM, et al. Accuracy of the veterans health administration COVID-19 (VACO) index for predicting short-term mortality among 1307 Yale New Haven Hospital inpatients and 427,224 medicare patients. medRxiv. 2021. doi:10.1101/2021.01.01.20249069
45. Levine J, Sher L. The prevention of suicide among military veterans during the COVID-19 pandemic. Eur Arch Psychiatry Clin Neurosci. 2021;271(2):405–406. doi:10.1007/s00406-020-01217-9
46. Murphy D, Williamson C, Baumann J, Busuttil W, Fear NT. Exploring the impact of COVID-19 and restrictions to daily living as a result of social distancing within veterans with pre-existing mental health difficulties. BMJ Mil Health. 2020. doi:10.1136/bmjmilitary-2020-001622
47. Psevdos G, Papamanoli A, Barrett N, et al. Halting a SARS-CoV-2 outbreak in a US veterans affairs nursing home. Am J Infect Control. 2021;49(1):115–119. doi:10.1016/j.ajic.2020.10.022
48. Dora AV, Winnett A, Jatt LP, et al. Universal and serial laboratory testing for SARS-CoV-2 at a long-term care skilled nursing facility for veterans - Los Angeles, California, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(21):651–655. doi:10.15585/mmwr.mm6921e1
49. Viswanathan M, Kahwati L, Jahn B, et al. Universal screening for SARS-CoV-2 infection: a rapid review. Cochrane Database Syst Rev. 2020;9:CD013718. doi:10.1002/14651858.CD013718
50. Ohl ME, Miller DR, Lund BC, et al. Association of remdesivir treatment with survival and length of hospital stay among US veterans hospitalized with COVID-19. JAMA Netw Open. 2021;4(7):e2114741. doi:10.1001/jamanetworkopen.2021.14741
51. Cho K, Keithly SC, Kurgansky KE, et al. Early convalescent plasma therapy and mortality among US veterans hospitalized with non-severe COVID-19: an observational analysis emulating a target trial. J Infect Dis. 2021;224:967–975. doi:10.1093/infdis/jiab330
52. Gerlovin H, Posner DC, Ho YL, et al. Pharmacoepidemiology, machine learning and COVID-19: an intent-to-treat analysis of hydroxychloroquine, with or without azithromycin, and COVID-19 outcomes amongst hospitalized US veterans. Am J Epidemiol. 2021;190:2405–2419. doi:10.1093/aje/kwab183
53. Lai CC, Yu WL. Appropriate use of antimicrobial therapy for COVID-19 co-infection. Immunotherapy. 2021;13(13):1067–1070. doi:10.2217/imt-2021-0134
54. Vaughn VM, Gandhi TN, Petty LA, et al. Empiric antibacterial therapy and community-onset bacterial coinfection in patients hospitalized with coronavirus disease 2019 (COVID-19): a multi-hospital cohort study. Clin Infect Dis. 2020;72(10):e533–e541. doi:10.1093/cid/ciaa1239
55. Osborne TF, Veigulis ZP, Arreola DM, Mahajan SM, Roosli E, Curtin CM. Association of mortality and aspirin prescription for COVID-19 patients at the veterans health administration. PLoS One. 2021;16(2):e0246825. doi:10.1371/journal.pone.0246825
56. Rentsch CT, Beckman JA, Tomlinson L, et al. Early initiation of prophylactic anticoagulation for prevention of coronavirus disease 2019 mortality in patients admitted to hospital in the United States: cohort study. BMJ. 2021;372:n311. doi:10.1136/bmj.n311
57. Ting R, Edmonds P, Higginson IJ, Sleeman KE. Palliative care for patients with severe covid-19. BMJ. 2020;370:m2710. doi:10.1136/bmj.m2710
58. Meyerson JL, McNamara LA, Nathan SN, Skarf LM. Complexities of corona virus disease-19: the role of palliative care at a veterans affairs hospital. J Palliat Med. 2021;24:1375–1378. doi:10.1089/jpm.2021.0020
59. Leigh AE, McCall J, Burke RV, Rome R, Raines AM. Predictors of functional dependence after COVID-19: a retrospective examination among veterans. Am J Phys Med Rehabil. 2021;100(1):34–38. doi:10.1097/PHM.0000000000001614
60. Alwan NA, Johnson L. Defining long COVID: going back to the start. Med. 2021;2(5):501–504. doi:10.1016/j.medj.2021.03.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.